ماده سنيه د. رنا
ثاني اسنان موصل31 / 3 / 2016
ماده سنيه د. رنا
ثاني اسنان موصل
31 / 3 / 2016
Dental metaral
Temporary Filling Materials
Indications
1. During treatment of root canal fillings.
2. It should be placed after inlay and onlay preparation until the final restoration is placed.
3. After pulp capping in case of traumatic exposure, to give time for pulp healing process
and production of dentin.
4. Pedodontic practice.
Requirements
1. Should be easily removed from the cavity
2. Should have sedative effect to the tooth and promote pulp healing
3. Reasonable strength and abrasive resistance
4. Radiopaque
5. Reasonable setting time and has low flow after setting
Types
1. Zinc oxide eugenol
2. Zinc phosphate
3. Zinc silico phosphate
4. Gutta-percha
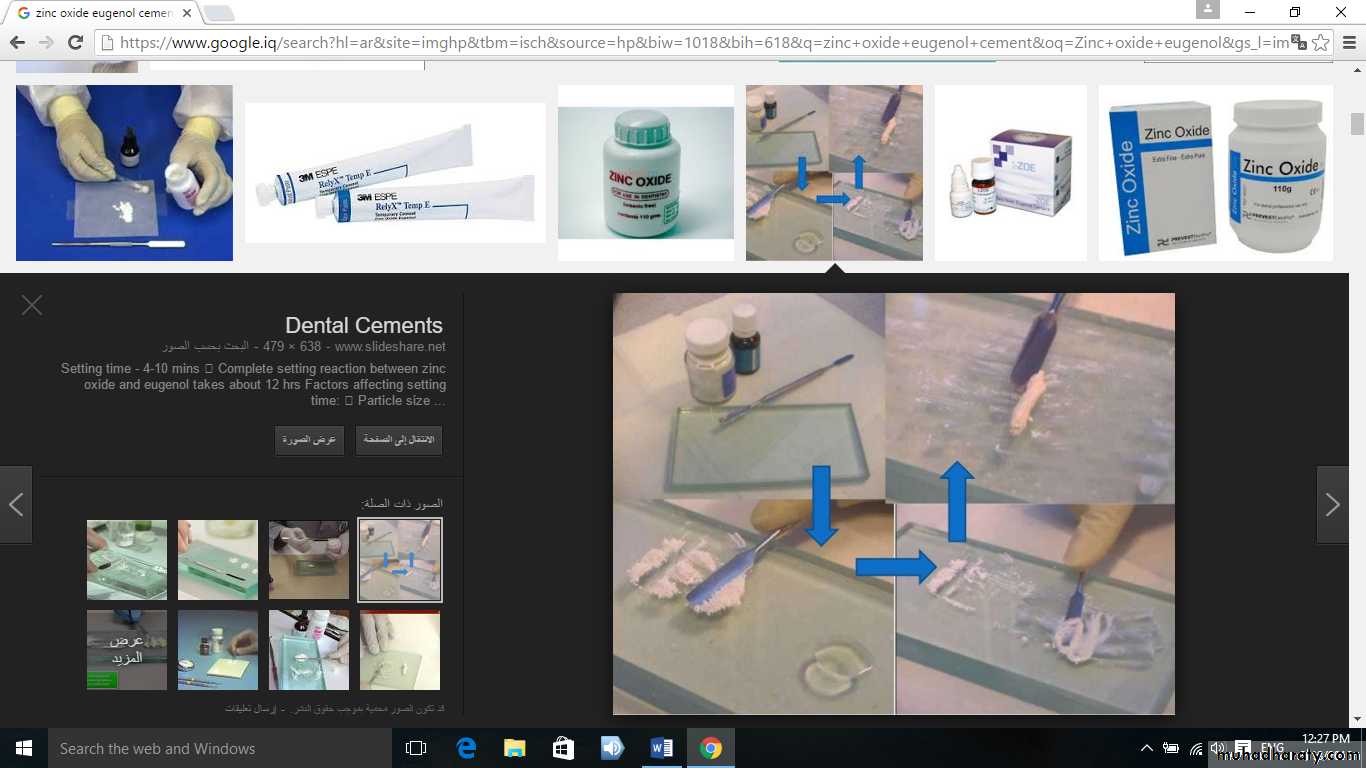
1. Zinc oxide eugenol
It's the material of choice as temporary filling.
Powder: zinc oxide, zinc acetate
Liquid: olive oil
Mixing is according to manufacture instruction or pastes.
Properties:
It has sedative effect on the tooth; reasonable sealing of the cavity, but it has low
strength, low abrasive resistance, and low flow after setting.
The strength and abrasive resistance could be improved by adding 20-40% of fine
polymer particles and treating the surface of zinc oxide particles with carboxylic acid reinforced
type. Sufficient powder should be added to the liquid to achieve putty consistency.
2. Zinc phosphate
It is powder and liquid.
Properties:
Has higher strength and abrasive resistance than ZOE and has relatively low solubility
in oral fluids but still has low abrasive resistance in area subjected to high load of
mastication.
Higher powder/liquid is required to decrease acidity and increase strength.
Reinforced zinc phosphate is more durable and could be used when longer time is
required.
3. Zinc silico phosphate
Powder: zinc oxide and silicate glass
Liquid: phosphoric acid
Properties:
it cause fluoride release
it has superior strength and more translucent than zinc phosphate
not promotes healing of the pulp.
used when longer time is required for temporary filling.
4. Gutta-percha
It is composed of natural gutta-percha, zinc oxide, wax, resin, metal salts to give radiopacityIt is applied by softening the gutta-percha on the flame and put it inside the cavity.
Disadvantages
1. Lack the ability to seal the cavity lead to micro leakage
2. Heat cause pain to the patient
3. Low strength, so reinforced zinc phosphate is more durable and could be used when
longer time is required.
5- Hybrid ionomer cements
Resin-modified (hybrid) glass ionomers (RMGIs) are versatile materials with a variety of applicationsthey are available in self-, light-, or dual-cured forms and are supplied as powder–liquid systems, as paste–paste systems, and in automix cartridges and syringes as well as pre-dosed capsules.
RMGIs may have three setting mechanisms: acid–base reaction, light-activated polymerization, and chemically activated polymerization.
Bonding to dentin is comparable to that of GICs but RMGIs bond better to resin-based restorations. Initial pH is low (3.5) but increases over time.
Applications: RMGIs are used for luting of cast metal and porcelain restorations, posts, and orthodontic appliances, and as adhesive liners for amalgam restorations. They are also used for bases and provisional restorations
6- Resin cements are essentially low-viscosity composite filling materials having a resin matrix containing silane-treated inorganic fillers (silica, glass, or ceramic particles and/or colloidal silica). The polymer systems of resin cements include PMMA or methacrylate copolymers, bis-GMA resins, and urethane dimethacrylate resins with diluents such as triethylene glycol dimethacrylate (TEGMA);
Most resin cements require a bonding agent to promote adhesion to tooth structure.
Resin cements have greater strength and lower solubilities than inorganic cements, GICs, and hybrid ionomers , they form thinner films,but set faster.
The disadvantages of resin cements are technique sensitivity, radiolucency with some materials, difficulty in removing excess material, and higher cost
periodontal dressing material
Periodontal surgery involves surgical manipulation of soft tissue to alleviate various problems but, during the histological tissue turnover process, the mucosa requires protection for 6–7 days. In particular, postoperative healing wounds require protection against insult from saliva, trauma, food impaction, and stagnation. Periodontal dressing materials or “packs” are used for this purpose. They also alleviate pain, reduce hemorrhage, facilitate healing, and prevent overgrowth of granulation tissue.Properties of an ideal periodontal dressing material:
Slow setting, Smooth, non irritant, Flexibility ,Good adhesion, Bacterial growth inhibition ,Dimensional stability, Non allergenic, Resistant to plaque accumulation, Acceptable taste.
The properties of an ideal periodontal dressing Traditionally, periodontal dressing materials were eugenol-containing systems derived from ZOE temporary cement, based on the belief that the eugenol had anodyne and antiseptic properties. However, studies indicate that eugenol possesses little antimicrobial activity and, in fact, has toxic side-effects that may delay healing and elicit allergic reactions. Accordingly, noneugenol materials are now used in periodontology; in particular, postsurgical dressing materials are placed in and around surgical sites to promote wound healing and epithelial growth.
Two ZnO-based periodontal materials are in widespread use: the paste–paste Coe-Pak® system and paste–gel PerioCare®; their principal components are indicated inTable 37.1. Compared with the amounts of luting agent used for provisional cementation, comparatively large volumes of material have to be mixed for periodontal use and, accordingly, slower setting rates are required. In the case of these two self-curing products, setting occurs within 15–20 minutes. In order that the dressings have a suitable degree of plasticity and reduced brittleness compared with that required for luting or provisional restorations, these materials also have relatively high oil contents. The latter ensures that the mixed material has a smooth texture and is cohesive, so that these dressings are readily form ropes to facilitate placement and contouring to promote good adaptation. The absence of eugenol eliminates the unpleasant taste, odor, and burning sensation found with ZOE materials.
Polymeric periodontal dressings A single-component, light-activated periodontal dressing material, Barricaid®, has been introduced for routine periodontal packing and protection following surgery as well as for use as a protective pack for extraction sites. It is also used to seal in antimicrobial agents placed in periodontal pockets.
The components of this gel material are indicated in Table 37.1. This VLC material gives the clinician total control over the placement and setting of the periodontal dressing and, when cured, the material forms an elastic protective covering over the wound. Further, incremental additions can be made since the material bonds adhesively to itself. Because Barricaid is light-cured.
Antimicrobials such as antibiotics and chlorhexidine can be incorporated into the unset gel such that these agents are delivered in situ with sorption of oral fluids into the cured polymer Such additions, however, do reduce the elastic modulus of the material and its elastic recovery after strain.
Dressing properties: All three dressing materials are in widespread use and each has certain advantages and drawbacks and, as stated, none contains eugenol. All three materials show some solubility. The solubility of PerioCare is greater at mouth temperature than room temperature but this is not the case for Coe-Pak and Barricaid. Likewise, the three materials show sorption behavior at mouth temperature. However, whereas water sorption over time actually improves adhesion for PerioCare and has a small but progressive negative effect on Coe-Pak, fluid sorption by Barricaid decreases its already lower adhesion compared with that of the two inorganic materials. Whereas Coe-Pak and PerioCare exhibit good adhesion to hard tissue, their solubility (particularly for PerioCare) suggests that their durability in the mouth may be limited. The polymeric Barricaid shows little solubility but does sorb fluids and this appears to reduce adhesion. Thus, Coe-Pak and PerioCare may be applied directly to the soft and hard tissues, where they appear to anchor well. Barricaid, although easier to manipulate, may require placement such that it encircles the teeth along the arch and extends through embrasures to ensure mechanical locking in position.