جامعة البصرة
–
ة الطبٌلك
...
مكتب المنتظر للحاسباتًف ةعابطلا تمت
(
البصرة
–
رٌوهلا
–
السوق
)
Summary Of
Common
Surgical Cases
Prepared By:
أنور قيس سعدون
2
" Reading without contemplation is like eating without digestion "
Chinese byword
بسم اهلل الرمحن الرحيم
ة متواضعةٌدهك رٌسٌلا لمعلا اذه مدقأ نأ ًنرسٌ
كمٌلإ
ًإخوت
وأ
خ
ـ
ًوات
ة الطب جامعة البصرةٌلك ةبلط
والتمس منك
م ال
ةٌعابط ءاطخأ يأ نع رذع
ةٌملع وأ
قد تكون وقعت
دون
مٍملع
أو
قصد
وال
ًفوتنٌ
ان
أقدم
جزي
ل
ال
ِ
ِكر
واالمتنان
لإلخوة
:
ّممك اللم
ري
ًعمء الزك
ً القحطانًلع
ًف العلٌان
محمد قاسم
نٌذلا
ًكان لهم الفضل ف
جمع و
كتا
بة
هذهًف عٌضاوملا مظعم
الملزمة
.
س
ـائ
كمٌلعو انٌلع َّنُمٌَ نا ىلاعتو هناحبس الله ًلا
ر والمنفعة لناٌخلا هٌف امل مكاٌإو انقفوٌ نأو ةٌفاعلاو ةحصلاب
ولكم
إ
ب الدعاءٌجم عٌمس هن
.
قٌفوتلا الله نمو
سٌق رونأ
25
/
8
/
2012
3
" Reading without contemplation is like eating without digestion "
Chinese byword
Index
The subject Page number
History 3
Examination 10
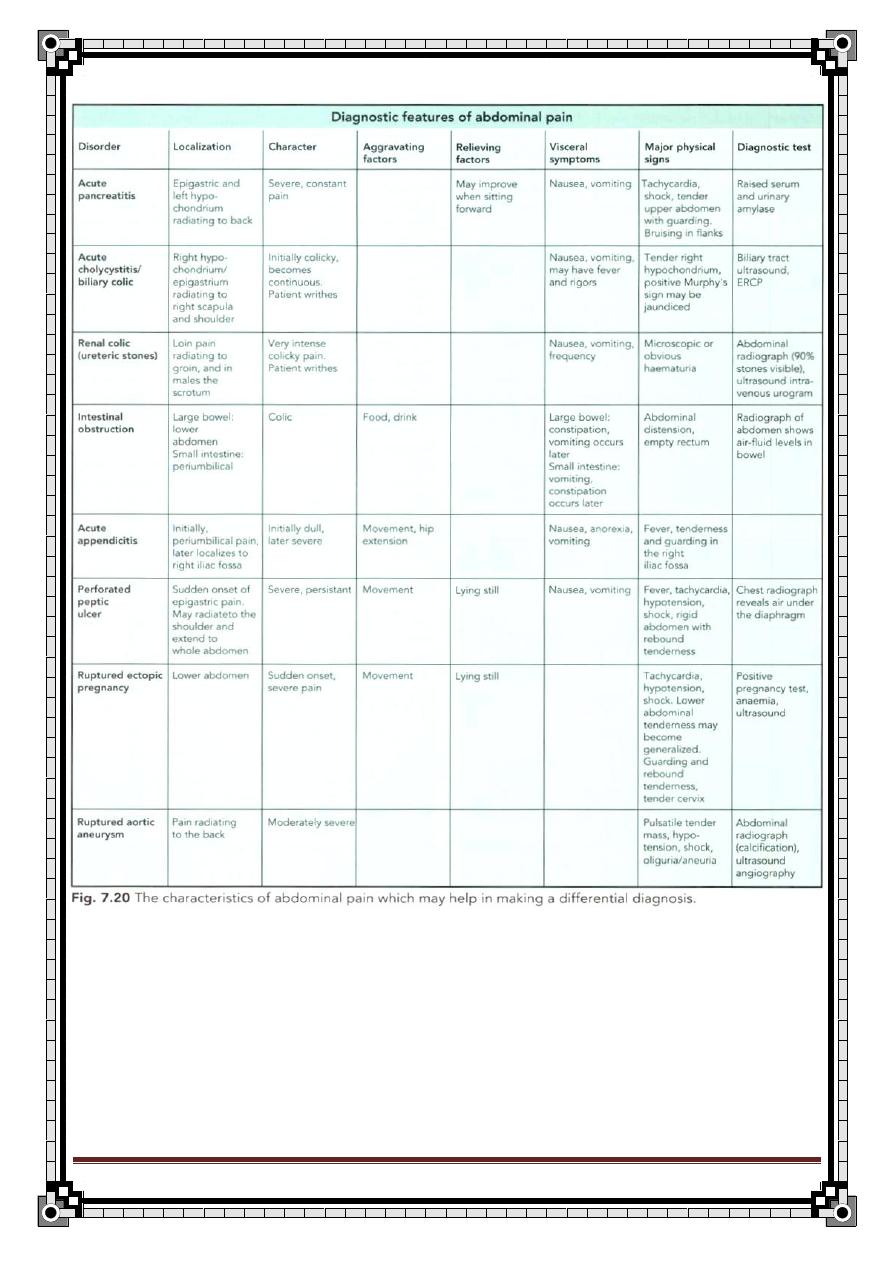
Abdominal Pain and The acute abdomen 14
Acute appendicitis 22
Peptic ulcer 35
Pancreatitis 53
Intestinal obstruction 66
Hernia 76
Gall bladder and bile ducts 100
Hydatid liver disease 115
History and examination of lumps and ulcers 119
Diabetic foot 129
Jaundice 140
Anorectal diseases 160
Thyroid gland diseases 190
Breast diseases 217
Chest trauma 238
Venous thrombosis 249
Urology
Haematuria 257
Renal stone 260
Urine retention 262
4
" Reading without contemplation is like eating without digestion "
Chinese byword
History
Identity
1-
Name
2-
Age
3-
Sex
4-
Nationality
5-
Religion
6-
Address
7-
Marital status
8-
Occupation
9-
Blood group
10-Next of kin
11- date of admission & Time
12-Source of referral
Chief complaint:
Symptom & duration
History of Present illness
For most symptoms ask about:
1. Onset
2. Timing
3. Course
4. Frequency
5. Analysis of the symptom:
For example:
Site of the pain
5
" Reading without contemplation is like eating without digestion "
Chinese byword
Diffuse or localize
Character
Severity
Radiation
6. Aggravated and relieving factors
7. Associated symptoms
8. Review the involved systems & exclude other differential diagnosis
9. Patient reaction
Review of systems
CNS
1- Headache
2- Dizziness
3- Vertigo
4- Visual disturbance
5- Syncope
6- Loss of consciousness
7- Limb weakness
8- convulsion
9- Tremor
10-Paresthesia
6
" Reading without contemplation is like eating without digestion "
Chinese byword
CVS:
1- Chest pain
2- Dyspnea
3- Claudication
4- Orthopnea
5- PND
6- Palpitation
7- Syncope
8- Fatigue
9- Ankle edema
Respiratory system:
1- Chest pain
2- Dyspnea
3- Cough
4- Sputum
5- Haemoptysis
6- Wheeze
7- Stridor
GIT:
1- Anorexia
2- Abdominal pain
3- Altered bowel motion (diarrhea or constipation)
4- Flatulence
5- Nausea & vomiting
6- Weight loss
7- Haematemesis
8- Jaundice
9- Dysphgia
10- Melaena
11- Bleeding per rectum
7
" Reading without contemplation is like eating without digestion "
Chinese byword
GUT:
1- Dysuria
2- Frequency
3- Nacturia
4- Urgency
5- Urine retention
6- Polyuria
7- Haematuria
8- Incontinence
9- Loin pain
10-Intermittent stream
11-Post micturition dripping
Locomotor system:
1- Joint pain
2- Joint swelling
3- Joint Stiffness
4- Joint locking
5- Muscle weakness
6- Deformity
7- Myalgia
Skin:
1- Petechiae
2- Echymosis
3- Itching
4- Skin rash
8
" Reading without contemplation is like eating without digestion "
Chinese byword
Past medical & surgical history
1- Pervious same symptoms or similar attack
2- Previous hospitalization (when, why)
3- Previous operation(when ,why name of hospital)
4- Previous blood transfusion(NO. of unit ,reason, complication)
5- Previous investigations and screening tests
6- Previous vaccinations
7- Parity
8- childhood Illnesses
9- Chronic illnesses
Family history
1-
Marital status (married, divorced ,separated ,widow)
2-
partner : name ,age, occupation
3-
children : No. ,age, sex, condition
4-
father : name ,age, occupation
5-
mother : name ,age, occupation
6-
consanguinity: relative or not
7-
Brothers & sisters(age ,sex, illnesses)
8-
same symptoms in the family
9-
Hx of surgery in the family
10-History of death in the family :cause ,date
11-Diseases affect more than one member of the family
9
" Reading without contemplation is like eating without digestion "
Chinese byword
Social history
1-Jop , duration
2-Alcohol drinking
Type
Amount
duration
3- Smoking:
No. of cigarette/20 x years of smoking
4- housing:
Own or rented house
Water and electrical supply
Number of rooms
Sanitary condition
Safety measures
5- Animal relationship & Pet rearing
6-hobbies
7-traveling
8-worris or stresses
9-contact with patient with same symptoms
Drug history
:
1- chronic drug use: of contraceptive , steroid, others
2- Allergy to drug & food
3- previous significant drug side effect
4- Hx of Warfarin or Heparin, Aspirin use
10
" Reading without contemplation is like eating without digestion "
Chinese byword
Examination
Headlines of general examination
1-General look (ABOPE)
A=Age
B=Built
O=Orientation
P=Position
E=Expression(Anxious , depressed)
2-General signs (JACCOL)
Jaundice
Anemia
Cyanosis
Clubbing
Oedema
LAP(lymph Adenopathy )
3-Eamination of Head Neck, Hand & foot
1- Head :
1-Skin 2-Hair 3-Orifices
2- Neck:
1-Thyroid 2-Tracheal deviation 3-Neck veins4-Cervical LN
3- Hand &Foot
1) Skin
2) Nail
3) Muscle
4) Oedema
4-Vital signs
a. Pulse
b. Temperature
c. Respiratory rate
d. Blood pressure
11
" Reading without contemplation is like eating without digestion "
Chinese byword
Headlines of abdominal examination
Inspection:
1-From the foot of the bed
Symmetry
Shape
2- kneeling from side of the bed
Movements
Move with respiration
Visible pulsation
Visible Peristalsis
3- from the side of the bed look for any:
1. skin
Dilated veins
Scars (site, describe it)
Any discoloration , pigmentation
Sign of liver diseases
stria
2. Umbilicus (position, shape ,discharge<amount, color, type>)
3. Ask the pt. to cough to examine hernial orifice
Palpation
a. Superficial and deep
b. palpation for tenderness or masses
c. palpation for organomegaly ( for any organomegaly look for
span, edge , surface , consistency)
12
" Reading without contemplation is like eating without digestion "
Chinese byword
13
" Reading without contemplation is like eating without digestion "
Chinese byword
Percussion
Tympanic (Normal)
Dull(fluid , Mass)
Auscultation
For aortic bruit
For renal artery bruit
For bowel sound
Then
Inspect the abdomen from behind and do renal angle
tenderness
Examine
1. The genitalia
2. Supra claviclar lymph node
3. Do PR examination
4.
do succession splach
14
" Reading without contemplation is like eating without digestion "
Chinese byword
Abdominal pain and the acute
abdomen
History of the Present Illness
1.
onset (sudden or gradual)
2.
Timing (Day or night)
3.
Severity
4.
Localized OR diffuse
5.
Site
6.
character at onset and at present (burning, crampy, sharp dull);
constant or intermittent (“colicky”)
7.
radiation (to shoulder, back, groin)
8.
pattern of progression
9.Aggrevating & relieving factors Effect of eating, vomiting, defecation,
flatus, Urination, inspiration, movement, position on the pain,
Drugs
Aspirin
NSAID's,
Narcotics
Anticholinergics
Laxatives
antacids.
relation to last menstrual period. Food (Fatty food intolerance)
11.Associated Symptoms:
Fever
Chills
Nausea
vomiting (bilious, feculent, blood, coffee ground-colored material); vomiting
before or after onset of pain
jaundice
constipation
change in bowel habits or stool caliber
obstipation (inability to pass gas)
chest pain, diarrhea
hematochezia (rectal bleeding)
melena (black, tarry stools)
dysuria, hematuria
anorexia, weight loss
15
" Reading without contemplation is like eating without digestion "
Chinese byword
dysphagia
odynophagia (painful swallowing)
early satiety
trauma.
Past Medical History:
1. History of abdominal surgery (appendectomy, cholecystectomy), hernias,
gallstones
2. coronary disease
3. kidney stones
4. alcoholism
5. cirrhosis
6. peptic ulcer
7. dyspepsia
8. Endoscopies
9. X-rays
10.upper GI series.
Physical Examination
1-
General Appearance
:
Degree of distress
body positioning to relieve pain
nutritional status
Signs of dehydration
septic appearance
Note whether the patient appears ill
well, or malnourished.
2-
Vitals:
Temperature (fever), pulse (tachycardia), BP (hypotension),
respiratory rate (tachypnea).
3-
Regional examination
HEENT:
Pale conjunctiva, scleral icterus, atherosclerotic retinopathy, “silver
wire” arteries (ischemic colitis); flat neck veins (hypovolemia).
Lymphadenopathy, Virchow node (supraclavicular mass).
4-
Specific examination
Abdomen Inspection:
Scars
Ecchymosis
visible peristalsis (small bowel obstruction)
16
" Reading without contemplation is like eating without digestion "
Chinese byword
distension
Scaphoid
Flat
Auscultation:
Absent bowel sounds (paralytic ileus or late obstruction)
high-pitched rushes (obstruction)
bruits (ischemic colitis)
Palpation:
Begin palpation in quadrant diagonally opposite to point of maximal pain
with patient's legs flexed and relaxed
Bimanual palpation of flank (renal disease)
Rebound tenderness
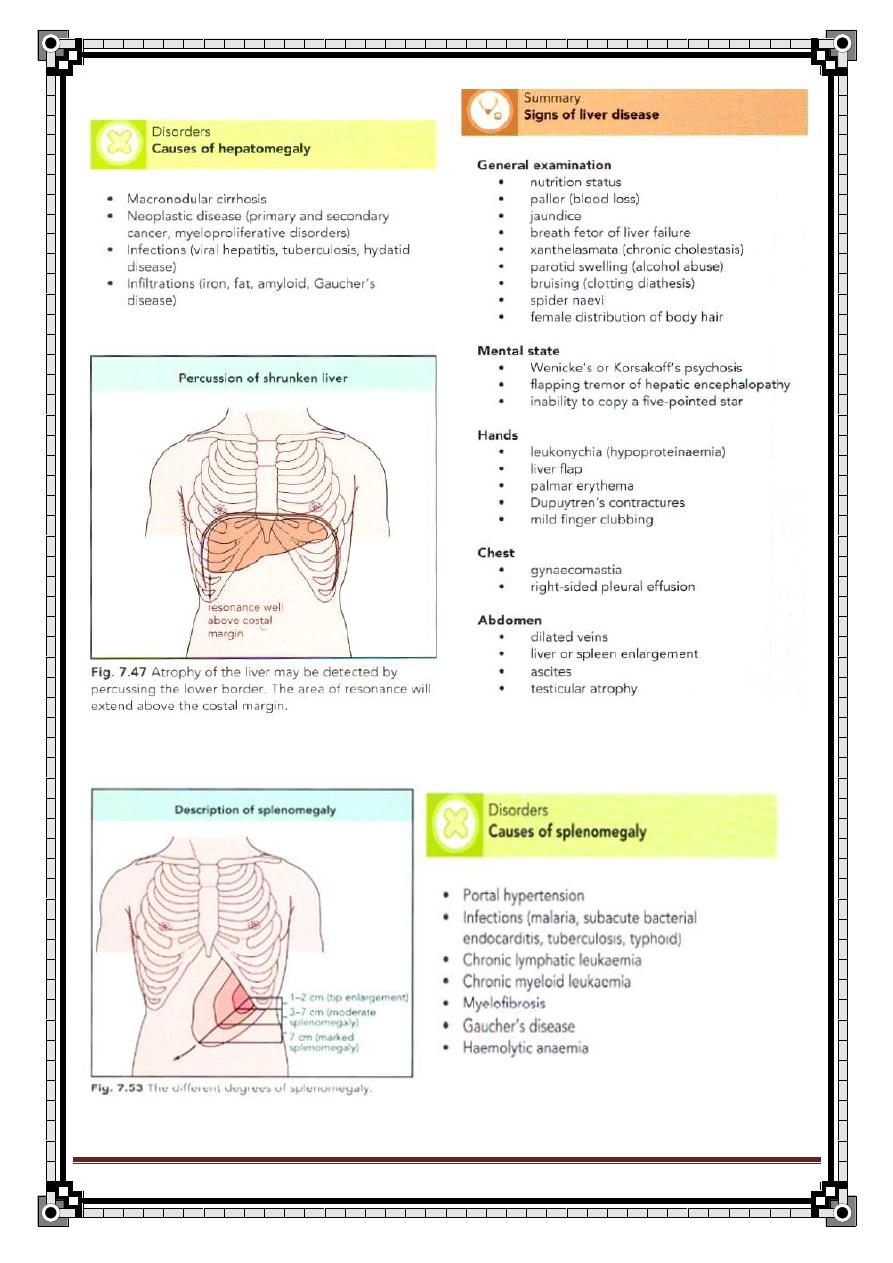
hepatomegaly
splenomegaly
masses
hernias (incisional, inguinal, femoral)
Pulsating masses
costovertebral angle tenderness
Bulging flanks
shifting dullness
fluid wave (ascites)
Specific Signs on Palpation
Murphy's sign:
Inspiratory arrest with right upper quadrant palpation,
cholecystitis
Charcot's triad
:
Right upper quadrant pain, jaundice, fever& rigor
=Ascending suppurative cholangitis .
Courvoisier's low :
Palpable, non tender gallbladder with jaundice;
pancreatic head malignancy
McBurney's point tenderness:
Located two thirds of the way between
umbilicus and anterior superior iliac spine; appendicitis.
Iliopsoas sign:
Elevation of legs against examiner's hand causes pain,
retrocecal appendicitis.
Obturator sign
:
Flexion of right thigh and external rotation of thigh
causes pain in pelvic appendicitis.
Rovsing's sign
:
Manual pressure and release at left lower quadrant colon
causes referred pain at McBurney's point; appendicitis.
Cullen's sign:
Bluish periumbilical discoloration; peritoneal hemorrhage.
Grey Turner's sign:
Flank ecchymoses ; retroperitoneal hemorrhage.
17
" Reading without contemplation is like eating without digestion "
Chinese byword
Percussion:
Loss of liver dullness (perforated viscus, free air in peritoneum); liver and
spleen span by percussion.
Rectal Examination:
Masses, tenderness, impacted stool; gross or occult blood.
Genital/Pelvic Examination:
Cervical discharge, adnexal tenderness, uterine size, masses, cervical motion
tenderness.
Extremities:
Femoral pulses
popliteal pulses (absent pulses indicate ischemic colitis)
edema.
Skin: Jaundice, dependent purpura (mesenteric infarction),
petechia (gonococcemia).
Stigmata of Liver Disease:
Spider angiomata
periumbilical collateral veins (Caput medusae)
gynecomastia
ascites
hepatosplenomegaly
testicular atrophy.
Labs:
CBC, electrolytes, liver function tests, amylase, lipase, UA, pregnancy
test. ECG.
Chest X-ray:
Free air under diaphragm
infiltrates
effusion (pancreatitis).
X-rays of abdomen (acute abdomen series
): Flank stripe,
subdiaphragmatic free air
distended loops of bowel
sentinel loop
air fluid levels
thumbprinting
mass effects
calcifications
fecaliths
portal vein gas
pneumatobilia.
18
" Reading without contemplation is like eating without digestion "
Chinese byword
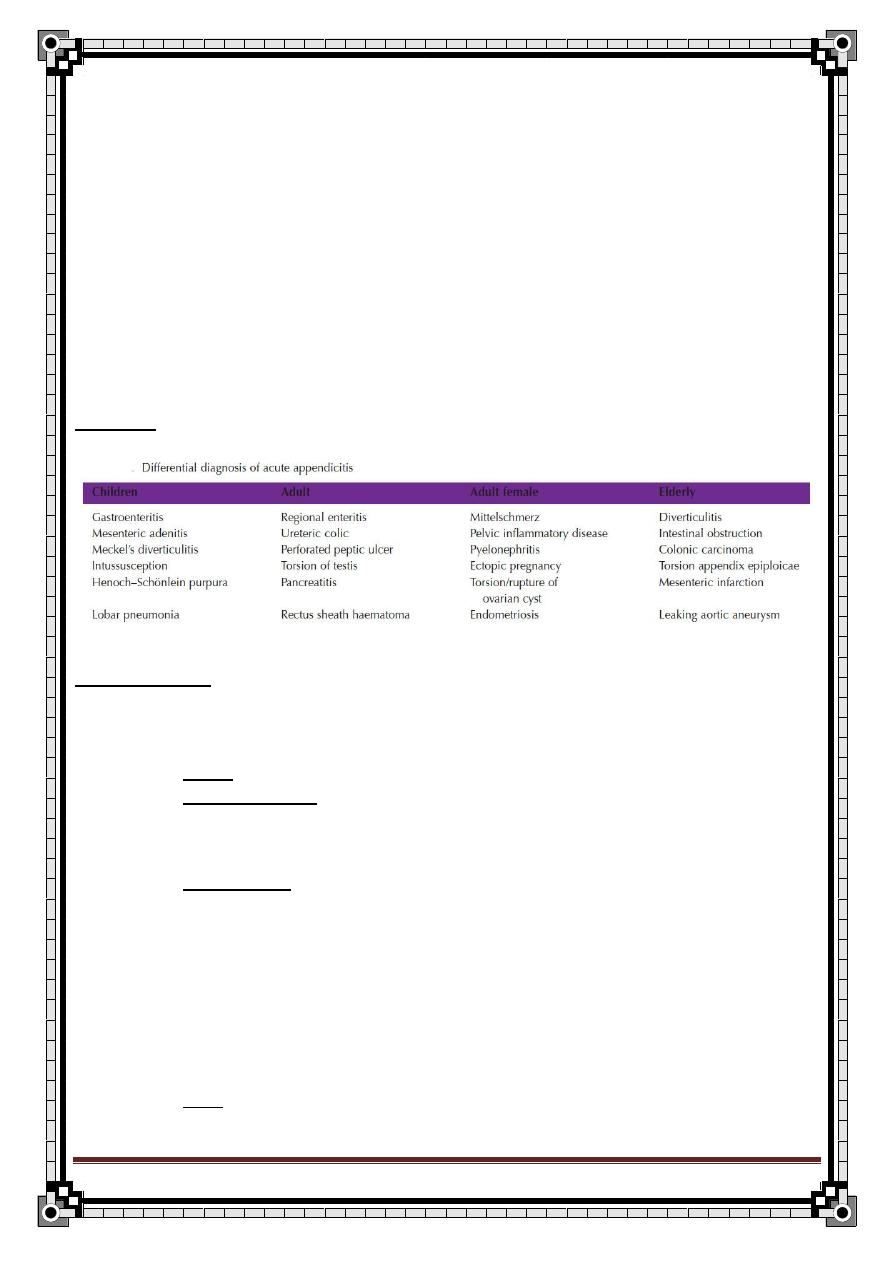
Differential Diagnosis
Generalized Pain:
1.
Intestinal infarction
2.
Peritonitis
3.
obstruction
4.
diabetic ketoacidosis
5.
sickle crisis
6.
acute porphyria
7.
penetrating posterior duodenal ulcer
8.
psychogenic pain.
Right Upper Quadrant:
1.
Cholecystitis
2.
Cholangitis
3.
Hepatitis
4.
Gastritis
5.
Pancreatitis
6.
hepatic metastases
7.
gonococcal perihepatitis (Fitz-Hugh-Curtis syndrome)
8.
retrocecal appendicitis
9.
pneumonia
10.
peptic ulcer.
Epigastrium:
1.
Gastritis or gastroenteritis
2.
peptic ulcer
3.
gastroesophageal reflux disease
4.
esophagitis
5.
pancreatitis
6.
perforated viscus
7.
intestinal obstruction
8.
ileus
9.
myocardial infarction
10.
aortic aneurysm
19
" Reading without contemplation is like eating without digestion "
Chinese byword
Left Upper Quadrant:
1.
Peptic ulcer
2.
Gastritis
3.
Esophagitis
4.
gastroesophageal reflux
5.
pancreatitis
6.
myocardial ischemia
7.
pneumonia
8.
splenic infarction
9.
pulmonary embolus.
Left Lower Quadrant:
1.
Diverticulitis
2.
intestinal obstruction
3.
colitis
4.
strangulated hernia
5.
inflammatory bowel disease
6.
gastroenteritis
7.
pyelonephritis
8.
nephrolithiasis
9.
mesenteric lymphadenitis
10.
mesenteric thrombosis
11.
aortic aneurysm
12.
volvulus
13.
intussusceptions
14.
sickle crisis
15.
salpingitis
16.
ovarian cyst
17.
ectopic pregnancy
18.
endometriosis
19.
testicular torsion
20.
psychogenic pain.
20
" Reading without contemplation is like eating without digestion "
Chinese byword
Right Lower Quadrant:
1.
Appendicitis
2.
Terminal ileitis
3.
Uretric colic
4.
Right sided acute pyelonephritis
5.
Perforated peptic ulcer
6.
Testicular torsion
7.
Rectus sheath hematoma
8.
diverticulitis (redundant sigmoid)
9.
salpingitis
10.
intussusceptions
11.
Mittelschmerz
12.
endometritis
13.
endometriosis
14.
ectopic pregnancy
15.
hemorrhage or rupture of ovarian cyst
Hypogastric /Pelvic:
1.
Cystitis
2.
Salpingitis
3.
ectopic pregnancy
4.
diverticulitis
5.
strangulated hernia
6.
endometriosis
7.
appendicitis
8.
ovarian cyst torsion
9.
bladder distension
10.
nephrolithiasis
11.
prostatitis
12.
malignancy
.
21
" Reading without contemplation is like eating without digestion "
Chinese byword
22
" Reading without contemplation is like eating without digestion "
Chinese byword
Acute Appendicitis
Anatomy:
It is a warm shaped tube containing large amount of lymphoid tissue.
Length 8-13 cm.
It has a complete peritoneal covering called Mesoappendix.
The base is attached to the posteriomedial surface of the cecum, about 1
inch below the iliocecal junction and this coincides with
Mc Burney’s point
N.B. the base is easily identified by following the tenia coli at the point of
convergence.
The other end is freely moving and usually found in
Retrocecal 74% (most common / give localized inflammation bcoz
cecum is covered with peritoneum from front and both 2 sides)
Pelvic 21%
Postileal 0.5%
Subcecal 1.5%
Preileal 1%
Paracaecal 2%
The Blood Supply of the appendix is by appendicular artery a branch of the
posterior cecal artery which is a branch of iliocecal
Iliocecal artery posterior cecal artery appendicular artery
Venous drainage through appendicular vein to the posterior cecal vein
Appendiclar vein posterior cecal vein
Lymphatic drainage through one or two nodes lying in the mesoappendix
into mesenteric nodes superior mesenteric nodes
Nerve Supply is derived from sympathetic and parasympathetic (vagus) nerves
from the superior mesenteric plexus
23
" Reading without contemplation is like eating without digestion "
Chinese byword
Causes:
Faecolith (the commonest).
Foreign body. E.g. fruit seeds
Kink from inflame adhesion.
Lymphoid hyperplasia within the wall.
Lesion in the cecum e.g. carcinoma.
Warm (rare).
Coarse (according to presence Bacteria)
Present absent
Bacteria proliferate in the Mucocel
Obstructed appendix and Due to continues
Invade the wall that was Secretion of mucous
Damaged by pressure necrosis from goblet cell
Inflammation
Bacteria are:
E.coli 85%
Pseudomonas
Normal flora of the appendix.
Bacteroid.
Afferent fiber conducting visceral pain of appendix enter through the 10
th
thoracic segment (this explains the referred pain at the umbilical level)
Acute appendicitis
It is the most common surgical emergency, more common in the western
countries d/t their diet.
Appendicitis is a disease of young adults and children but can occur in
elderly patient.
Peak age of the disease is 15 years (adolescence).
Types of appendicitis
Obstructed Appendicitis Non Obstructed Appendicitis
causes:
Direct infection of
lymphoid follicle
from appendicular
lumen.
Hematogenous.
E.g. strept
(rare)
24
" Reading without contemplation is like eating without digestion "
Chinese byword
Inflammation:
May resolve.
If not treated within 12 hours progressive infection and
obstruction which lead to
impairment of blood supply
gangrene
If perforation has occurred the outcome depend on the ability of the omentum
to contain the infection
History Taking
Age: can occur at all, but more common in the adolescence age group.
Sex: same incidence.
Symptoms:
1)
Pain: the main symptom.
Site:
it starts central pain around the umbilicus (visceral pain)
and it is a referred pain because the visceral innervation
of the appendix comes from the 10
th
thoracic spinal
segment, the corresponding dermatome encircle the
abdomen at the umbilicus.
A-If adequate omentum
there will be:
Appendicular mass.
Appendicular abscess
B- if the omentum is not
adequate there will be
Generalized
peritonitis
25
" Reading without contemplation is like eating without digestion "
Chinese byword
This central pain will shift to the right iliac fossa RIF after
few hours, to 2-3 days and then it is Somatic pain (d/t
irritation of the inflamed appendix to the sensitive parietal
peritoneum).
Onset: gradual and then becomes sudden.
Severity: sever.
Pattern:
Colicy pain obstructed appendix.
Constant painnon obst appendix.
Duration: usually few hours but it can be 2-3 days.
Progression: increases with time.
Relieving: by bending the leg to the abdomen(flexion) or by lying
down
Association: with other symptoms:
2)
vomiting:
vomiting after the onset of pain because vomiting before pain suggests
gastroenteritis.
3)
anorexia
4)
constipation:
majority of cases state that they have been constipated for few days
before the attack of pain.
5)
diarrhea:
few of the patients especially when it is pelvic appendicitis (d/t irritation to
the rectum)
6)
low grade fever: (37.2
– 37.7 C )
if higher fever think about complicated appendicitis ( by peritonitis and abscess)
in the Hx you have to exclude other GIT symptoms.
26
" Reading without contemplation is like eating without digestion "
Chinese byword
symptoms of DDx.
Physical Examination
General examination:
patient locks ill & unwell
pale (esp. in children)
tachycardia ( d/t spread of infection)
low grade fever
tongue: white and furred
foetor oris ( bad breath)
flushing of the face
Neck:
palpate glands and look at the tonsils to exclude mesenteric adenitis
Chest:
Examine the lung for right basal pneumonia
Abdomen:
inspection: normal, the abdomen is slowly moving with respiration due to
pain.
palpation:
right iliac fossa is tender with or without guarding
(voluntary contraction of abdominal muscle when palpate)
Rebound tenderness: +ve in McBurney’s point.
Signs:
Rovsing’s Sign:
Pain in the Right iliac fossa RIF d/t pressing or palpating the Left
iliac fossa LIF.
Because either - transmission of air
Or: - by pressing on the left side you are moving the
intestine to touch the inflammed organ
Psoas Sign:
27
" Reading without contemplation is like eating without digestion "
Chinese byword
Pain when extending the right hip joint d/t spasm of the psoas
muscle.
So, you observe hip flexing slightly by patient to decrease the pain.
Obturaror internus sign:
Pain with passive internal rotation of the flexed Rt. Thigh
it indicates inflammation overlying the muscle.
positive with pelvic
abscess and appendicitis
Blumberg’s sign:
Pressing and releasing suddenly in LIF feels pain in the RIF [
crossed rebound tenderness]
Straight leg raising sign:
+ve with retrocecal appendix.
Rectal Examination;
Tenderness ( in the pelvic position, or when there is pus in Douglas Pouch).
DDx:
(according to the location of pain)
I - RIF pain & tenderness II- Central abd. Colic
(Discussed below)
A)
Intra abdominal diseases:
1-Mesenteric adenitis:
Especially in children following upper
respiratory tract infection URTI.
28
" Reading without contemplation is like eating without digestion "
Chinese byword
It looks like appendicitis in their symptoms.
You must ask about previous Hx of URTI tonsillitis or enlarged L.N.
2-
Meckel’s diverticulitis:
Often indistinguishable from appendicitis, you have to look for Meckle’s
when you do appendectomy.
3-Acute
crohn’s ileitis:
Affect young adult & usually there is Hx of recurrent pain.
Mass of inflamed ilieum can be felt.
4-Acute cholecystitis:
Sometimes pain of inflamed Gall bladder descends into RIF.
Murphy’s sigh (+ve in cholecystitis).
Vomiting & jaundice may be present.
5-Perforated peptic ulcer:
Hx. Of dyspepsia.
Sudden pain on epigastrium shifted to RIF.
Gas under diaphragm on X-ray.
6-Pancreatitis: (rare)
Diffuse abd. Pain & sometimes central or RIF pain.
Associated with copious vomiting & back pain.
B)
The urinary tract diseases:
1-Renal colic & acute pyelonephritis:
You should ask about hematuria or loin pain which radiate to the groin
region.
Ask if there is any change in (color / frequent / volume) of urine.
2-Testicular torsion or undescended testis:
Very rare.
29
" Reading without contemplation is like eating without digestion "
Chinese byword
C)
Gynecological diseases (females):
1-Acute salpingitis:
Hx of vaginal discharge, menstrual irregularities and dysmenorrhea or
dysuria.
Hx of contact with venereal dis.
On PR or PV examination, enlarged fallopian tubes may be palpable.
Confirm Dx by Laparoscopy
2-Ectopic pregnancy:
Hx. Of missed period.
Pain on constant site.
Sever pain.
N.B. In female pt you should ask about:
3-Mid cycle pain: (esp. in youngs) d/t rupture of ovarian follicle
o Pain
o Bleeding
Ectopic pregnancy (missed period)
4- complicated overaian cyst
5- pelvic inflammatory disease
D)
Chest:
Pneumonia and pleurisy:
Rt basal pneumonia.
Associated with tachycardia and cheat pain.
Chest examination added sound and friction rub.
Chest X-ray may be helpful.
II- DDx of Central abd pain:
In the early stages of appendicitis may suggest:
30
" Reading without contemplation is like eating without digestion "
Chinese byword
1-Gastroenteritis:
Nausea, vomiting and diarrhea precedes the pain.
2-Intestinal obstruction:
High level obstruction characterized by profuse vomiting and little
abdominal distension.
Low level obstruction causes mark distention & late onset vomiting.
On X-ray you will see fluid level.
Noisy bowel sounds.
Summary
Investigation:
Lab investigation
1) CBC: leukocytosis esp. neutrophils.
2) Urine Analysis: to exclude urinary tract disease
Pyourea may indicate Rt.pyelonephritis.
Imaging
3) Plain X-ray:
Related to appendicitis:
May show faecolith in RIF.
Loss of Rt psoas shadow.
Others to exclude:
Acute intestinal obstruction.
Peptic ulcer perforation.
Uretric stone.
4) U.S:
To exclude or verify:
31
" Reading without contemplation is like eating without digestion "
Chinese byword
Ovarian pathology.
Or mesenteric adenitis.
Or carcinoma of the cecum.
Or appendicular mass.
Laparoscopy:
In doubtful diagnosis.
Management:
A. Direct operative management:
If you doubt it is appendicitis or not you can admit the patient for few
hours:
If still fever then operate.
If it improves
don’t operate & he may not have appendicitis.
If the patient did not under go appendectomy there will be:
1. He may improve give him antibiotics.
2. in some cases there will be adhesions of the omentum and
adjacent viscera to the inflamed appendix and then there will
be formation of
Appendicular mass.
Localized abscess.
To differentiate between the two, do U.S. & treat both of them by antibiotic if it
is:
Mass: will improve, mass will decrease in size, fever will decrease [can be
treated by antibiotics alone]
Abscess: will not improve(confirm by U.S) [need drainage under
ultrasonograpgy guidance]
N.B:
we Don’t operate and remove the mass b/c there will be inflammation
around the whole area & you may injure the bile or blood vessels or renal
strucrure.
B. Appendectomy:
32
" Reading without contemplation is like eating without digestion "
Chinese byword
Types of incisions:
* You can do Laparoscopic appendectomy
Paramedian incision:
It is a vertical incision lying
parallel to the mid line just
1.25-2.5 cm
Commonly 2.5 cm below
the umbilicus and just
above the pubis.
Advantage:
Done when the Dx is doubt
and you should operate.
It gives a good access to the
pelvic organs in females.
It can extend upward to deal
with a perforated duodenal
ulcer or other
intraabdominal pathology.
Disadvantage:
Give limited access to
retrocecal appendix.
High incidence of infection.
High Chance of incisiona
hernia
May injure the bladder.
Grid Iron incision:
When the Dx is certain,
an incision is made aright
angle to a line joining the
superior iliac spine to the
umbilicus. Its center
being the line at
McBurney’s point
Has less
postoperative
complication
Superficial
circumflex artery
usually need ligation
Lanz incision:
Transverse incision made
approximately 2 cm
below the umbilicus
centered in the
midclavicular line.
The external oblique
aponeurosis,internal
oblique and transverses
muscles are split in the
direction.
The exposure is
better and extension
if needed is easier
Recently this incision
became so popular
and it is performed
in most of the
patients.
33
" Reading without contemplation is like eating without digestion "
Chinese byword
Complications:
Complications of the operations:
1.
Bleeding.
2.
wound infection:
anaerobic bacteria (flagyl)
gram
–ve bacteria (gentamycine)
gram +ve bacteria (ampicilline)
3.
residual abscess:
local.
Pelvic.(common)
Paracolic.
4.
Intestinal obstruction from adhesions.
5.
Incisional hernia ( esp. Para median incision)
6.
Rt. Inguinal hernia (following the grid iron incision)
Complications of the appendicitis:
1.
localized peritonitis or generalized after perforation:
symptoms include:
generalized abdominal pain.
Nausea and vomiting.
Sweating and sometimes rigors.
With pyrexia.
2.
appendicular mass:
pt. present with Hx. Of 4-5 days abd. Pain with localized mass in the
RIF.
No signs of general peritonitis.
Conservative ttt( 80% will resolve) :
Antibiotic:
Anaerobesflagyl.
G-ve gentamycine.
G +ve ampicillin.
Analgesia.
Observe vital signs.
The remaining 20% :
Deterioration.
Abscess formation.
No change.
3.
appendicular abscess: Need drainage.
34
" Reading without contemplation is like eating without digestion "
Chinese byword
May give pelvic abscess or portal pyemia through ilio colic vein.
N.B:
In 20% of the cases the appendix is found to be normal
You look for other causes and remove the appendix as prophylaxis.
DDx of a mass in the RIF:
1. appendicular mass or abscess.
2. carcinoma of the cecum :
not tender.
Blood in stool.
Deterioration in health over month
Pt. usually old.
Signs of metastasis e.g. to the liver [ enlarged/ tender]
3.
Crohn’s disease:
Diarrhea.
Wt. loss.
Abdominal pain, rectal bleeding.
Occult blood in stool.
Increased ESR.
4. Ovarian carcinoma.
5. Iliocecal T.B.
6. Iliac L.N enlargement.
7. Iliac artery aneurysm.
8. psoas abscess.
9. distended gall bladder.
35
" Reading without contemplation is like eating without digestion "
Chinese byword
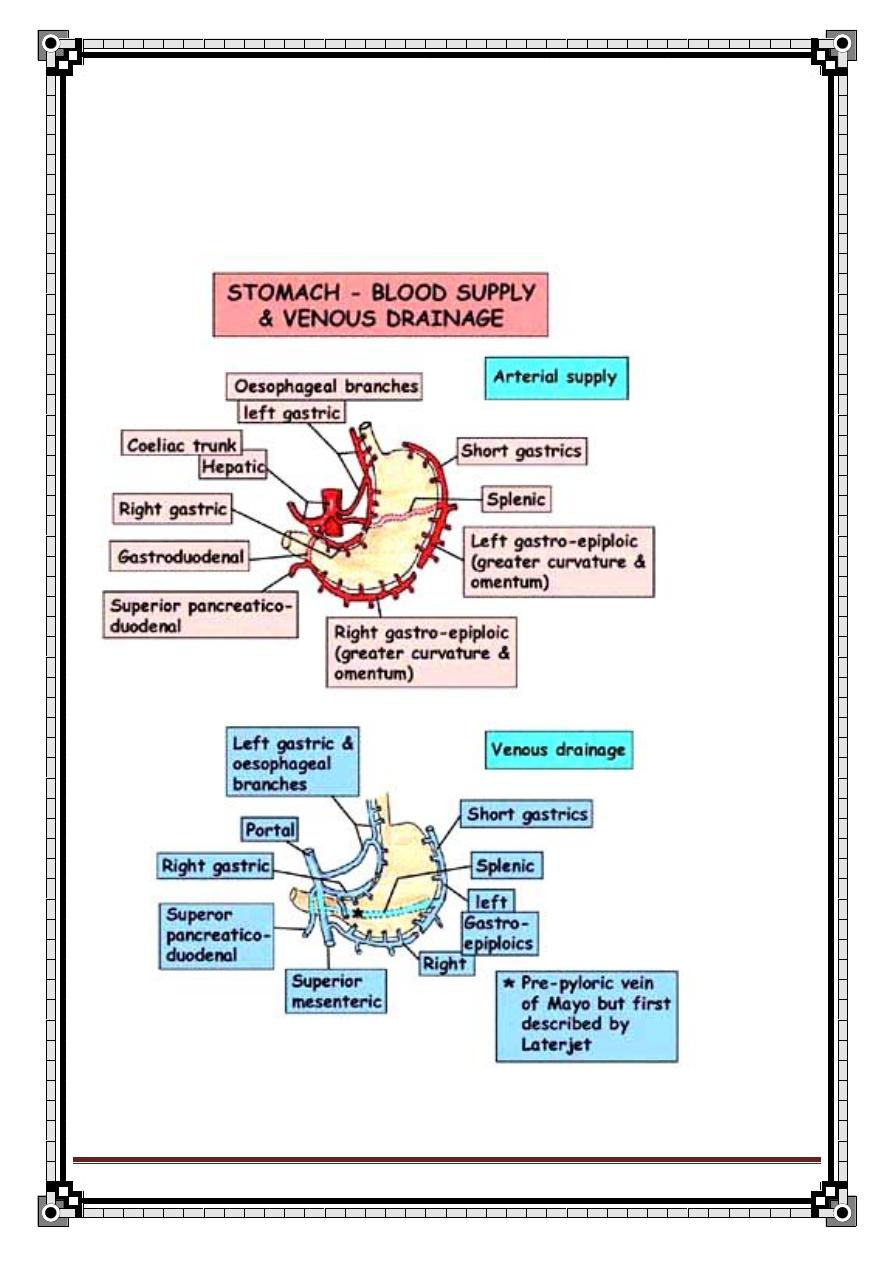
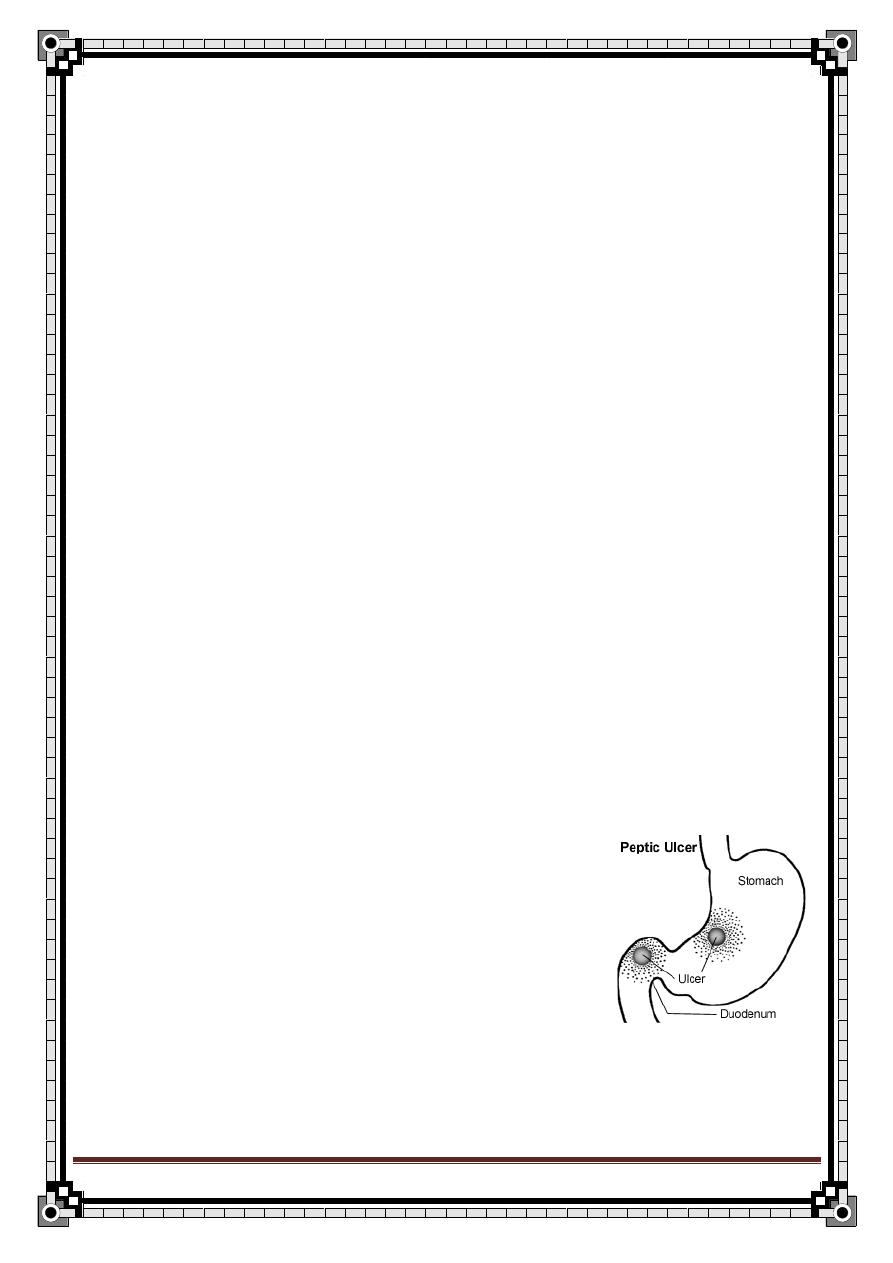
Peptic Ulcer
Blood supply & venous drainage of stomach:
36
" Reading without contemplation is like eating without digestion "
Chinese byword
37
" Reading without contemplation is like eating without digestion "
Chinese byword
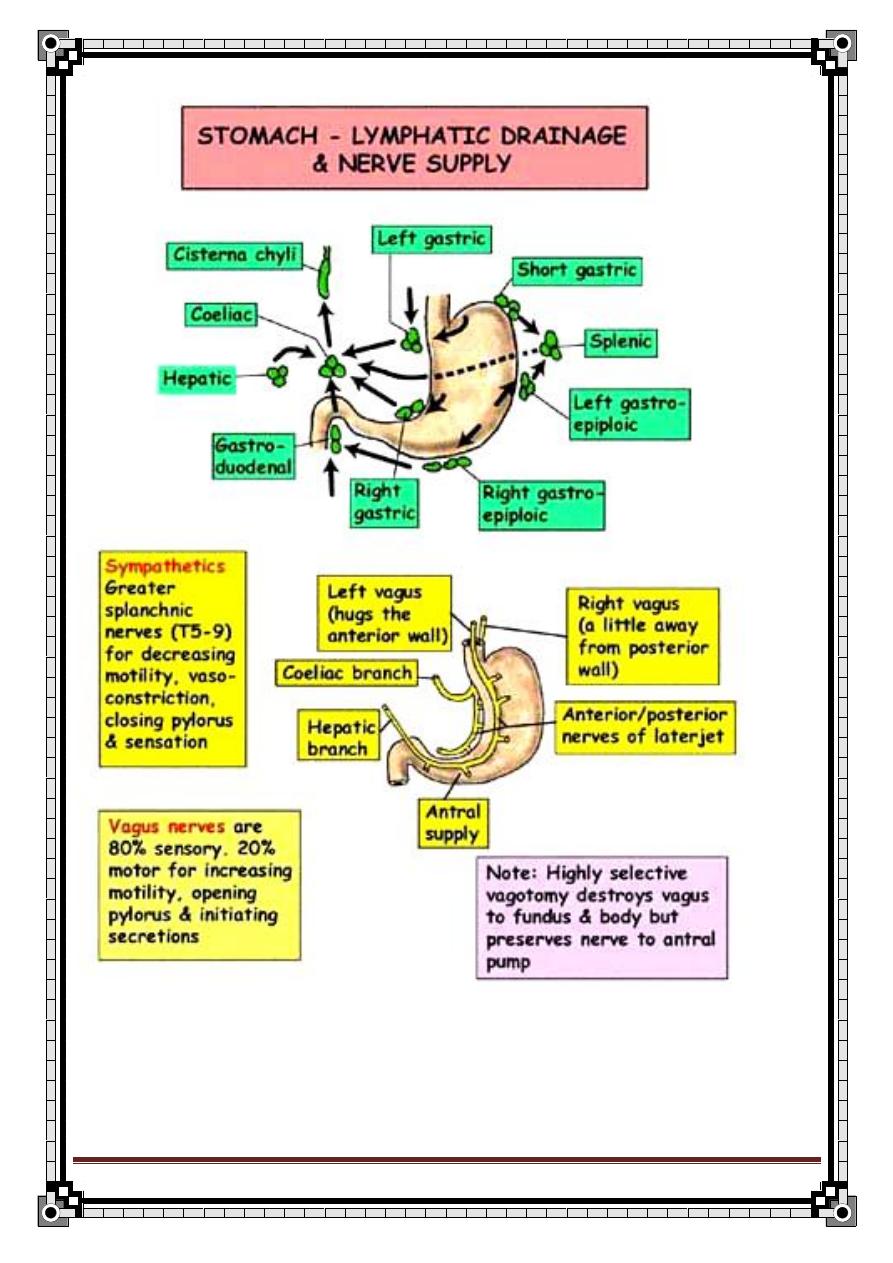
Nerve supply of stomach:
1/ Sympathetic
2/ Parasympathetic:
-
ant.vagal trunk → hepatic branch
→ descend along lesser curvature &
supply ant. wall of stomach
-
post.vagal trunk → coelic branch
→ supply back wall of stomach
Vagus
⅔ ⅓
Ant & Post vagus hepatic branch celiac b.
Stomach liver & gall bladder -pancreas
-S.Intestine
-transverse
colon
Histology:
1/ Columnar epith :
Lines the whole stomach
2/ Cardiac gland:
Secrete mucous and electrolytes
Occupy a small ring around the oesophagogastric junction
38
" Reading without contemplation is like eating without digestion "
Chinese byword
3/ Oxyntic glands:
Occupy the fundus and body of stomach
a- parietal cells:
produce H+ & intrinsic factor
it is double its # in duodenal ulcer & 4х in Zollinger Ellison syndrome
its # is ↓ in gastric ulcer
b- peptic (chief) cells:
in the fundus &
produce pepsinogen
4/ Pyloric glands:
In the antrum
Secrete mucous & electrolytes
5/ G-cells:
In the antrum
Secrete gastrin
Its # increase only in duodenal ulcer
Surgical Physiology:
1/ Gastric motility:
Body & fundus act as a reservoir for food.
39
" Reading without contemplation is like eating without digestion "
Chinese byword
Antrum acts as a mill, mix & grind the food & expel it to the duodenum.
Gastric motility is controlled by intrinsic neural plexus which are regulated by
the extrinsic nerve supply (vagus)
Truncal vagotomy affects & reduces gastric motility.
Also, sympathetic n. inhibit gastric motility.
2/ Gastric secretion:
Mucus is secreted in all regions of stomach & protects surface epith.
against acid and pepsin.
Acid & pepsin secretion is regulated by a neurocrine, endocrine &
paracrine factors.
Neurocrine: Ach from vagus
Endocrine: Gastrin from antrum
Paracrine: Histamine from cells near to parietal or peptic cells
Parietal (w secrete H+) & pepsin (w secrete pepsin) cells has specific
receptor for each of the 3 stimulants.
The action of each stimulant is potentiated by the other two. Eg;
Gastrin & Ach release histamine from mucosal stares.
Ach stimulate secretion by inhibit the release of somatostatin.
In truncal vagotomy not only Ach stimulation is affected, but also gastrin &
histamine efficacy is reduced.
Phases of gastric secretion:
1/ Cephalic (neural) phase:
Sight, smell, taste or though stimulate vagal center
Vagus → stimulate peptic & parietal cells (direct)
→ stimulate gastrin release from antrum (indirect)
2/ Gastric Phase:
Distention of gastric antrum & products of protein digestion stimulate
gastrin release from antral mucosa.
3/ Intestinal Phase:
40
" Reading without contemplation is like eating without digestion "
Chinese byword
Food in small bowel release enteroxyntin (duodenal gastrin) that
increases acid release.
Pathology:
Due to imbalance between gastric acid
– pepsin secretion and the ability of the
GI mucosa to define against them.
This imbalance occurs due to:
a. Hyper secretion of acid and pepsin. (D.U)
b. Defect in mucosal defense. (G.U)
c. H.pylori infection.
Special Forms of Peptic Ulceration:
1/ Stress ulcer:
Occur after major surgery, trauma or sever illness.
Multiple small superficial ulcers in the stomach or duodenum.
2/ Curling’s ulcer:
In patient with sever burns.
In the duodenum.
3/ Cushing’s ulcer:
In patient with neuro-surgical illness or head injury.
In both stomach or duodenum.
Sites:
1) Duodenum:
o The 1
st
part of the duodenum is the commonest.
o If it is in the Ant.
surface → perforation.
o
If it is in the Post. surface → He by erosion of arteries.
2) Stomach:
41
" Reading without contemplation is like eating without digestion "
Chinese byword
o Type 1 (1ry GU): often in the lesser curvature.
o Type 2: same as type 1 plus a D.U.
o Type 3: in pyloric channel or prepyloric area.
3) Esophagus:
o At the lower end.
o Due to reflux of acid and pepsin from the stomach.
4) Jejunum:
o Zollinger-Ellison syndrome.
o After gastro-jejunostomy.
5) Meikle’s diverticulum:
o Due to the presence of ectopic gastric mucosa.
N.B
G.U in Post. wall → erode to pancreas
G.U in Ant. wal
l → erode to liver
Etiology:
1/ Acute peptic ulcer:
May be without apparent cause.
Or associated with ingestion of alcohol, NSAID or steroidal therapy.
Also it can be associated with stress ulcer, curling’s ulcer or cushing’s
ulcer.
2/ Chronic peptic ulcer:
42
" Reading without contemplation is like eating without digestion "
Chinese byword
I. Genetic & blood group
Blood group O 3x likely to get D.U
α¹- antitrypsine deficiency
II. Neurogenic therapy
Vagal stimulation → hyper secretion & hyper motility ←
Stress & anxiety +→ vagus
III. Accessory causes (factors)
Alcohol
Excessive smoking
Vitamine deficiency
IV. Endocrine
Z-
E syndrome →↑gastrin →↑acid secretion
Multiple adenoma syndrome
Hyper parathyroidism →↑Ca² →↑gastrin
V. Infection
Helicobacter pylori
H-pylori:
A Gm -ve spirochetal bacteriam
Found in the antral and duodenal mucosa
Mechanism:
It is u
rease +ve → split urea & lead to formation of ammonia → alkaline
media around the pacteria → 2ry ↑ in acid → ulcer
Also it affects the cells through cytotoxin
Diagnosis:
43
" Reading without contemplation is like eating without digestion "
Chinese byword
1) Histology
Spiral bacterial rod adjacent to gastric epith.
2) Direct culture
Only done when an Atb resistant organism is suspected.
3) CLO (urease) test
4) Serology
High anti
– H.pylori IgA & IgG titer
Treatment:
Triple therapy
Bisthmus
Metronidazole
Tetracycline or Ampicillin
History:
H.P.I:
D.U
G.U
Age
30’s – 40’s
50’s – 60’s
Sex
♂:♀ 4:1
♂>♀
Occupation
Highly professional & managers
Pain
epigastrium
Epigastrium & can
radiate to the back
Onset
2-3 hrs after eating or at
midnight (empty
stomach)
Soon after eating
(15-30min)
Aggravated by Hunger (missing meal),
anxiety, stress
Eating (pt afraid to eat)
Relieved by
Eating (milk, biscuits),
anti-acid
Vomiting or by lying
down flat, anti-acid
Periodicity
More prominent features
4-6 mth (spring & fall)
Comes & goes in a 2-3
months cycle
Duration of
attack
1-2 months
Few weeks
Vomiting
Uncommon
Common to relieve the
pain
Appetite
Good
Pt is afraid to eat
Diet
Eat every thing
Avoid fried food &
curries but like milk, fish
44
" Reading without contemplation is like eating without digestion "
Chinese byword
Weight
No wt loss
Loss wt
Hematemesis
&
Melena
Hematemesis:Melena
40:60
Hematemesis:melena
60:40
Ratio of all Hge is more in D.U than G.U
Drug Hx:
NSAID, steroid
Social Hx:
Smoking, alcohol intake
Examination:
General examination is likely to be normal.
Usually there is only mild to moderate epigastric tenderness.
If complications develop:
Bleeding → anemia
Pyloric
stenosis → epigastric fullness & visible peristalsis
Malignant changes → wasting
Differential Diagnosis:
1. uncomplicated hiatal hernia
2. atrophic gastritis
3. chronic cholecystitis
4. irritable bowel syndrome
5. pancreatitis
6. functional indigestion
7. reflux esophagitis
Investigation:
1) Barium meal: (not used anymore)
a- gastric ulcer:
A niche will be seen projecting from the stomach outline.
J-shaped stomach & hangs low in the pelvis.
b- duodenal ulcer:
45
" Reading without contemplation is like eating without digestion "
Chinese byword
Ulcer crater filled with Barium wich indicate active ulcer.
Folds of scar tissue coverage on the ulcer site (rugal
convergence).
2)
CBC:↓ Hb in chronic blood loss.
3) Stool:
Occult blood.
4) Gastroduodenoscopy: (the best one)
a- especially in G.U to roll out malignancy
b- take biopsy.
c- View the esophagus, stomach, 1
st
& 2
nd
part of duodenum.
5) Serum gastrin level:
Specially done in pt with recurrent ulcer or multible ulcers or
suspected to have Z-E syndrome.
Level > 200 pg/ml is high.
In Z-E syndrome > 500 pg/ml
6) Gastrin function studies:
a- Measurement of acid production without stimulating the
stomach
(Normal basal acid input = 1.5
– 2.5 mEq/hr)
b- Measurement of acid production in stimulated stomach, done
by histamine or pentagastrin
(Maximal acid output = 20
– 30 mEq/hr)
Complications:
1. Hemorrhage.
2. Perforation.
3. Obstruction (pyloric stenosis/ D.obst)
4. Malignant transformation (only in G.U)
5. Pancreatitis.
6. Biliary obstruction.
46
" Reading without contemplation is like eating without digestion "
Chinese byword
Surgical Pathology:
G.U
D.U
Site
Single, in lesser curvature Single, in the 1
st
part,
sometimes double
Edges
Punched out
Punched out
Associations Atrophic gastritis
Duodinitis
Malignancy
May become malignant
Never become malignant
Penetration
To near structure like
pancreas or liver
Liver, pancreas or post.
abdominal wall
Hge
Minor → from mucosa
Sever → from large art.
Gastroduodenal art.
Erosion
Perforation
To lesser sac → abscess
To peritoneum→peritonitis
Anteriorly → peritonitis
Obstruction
If there is ulcer in pylorus
or large ulcer
Pyloric stenosis by
edema & fibrosis
Duodenal Ulcer Treatment:
Indications for surgery:
1/ Failure of medical ttt:
Break through of symptoms during medical ttt.
Endoscopy fails to confirm ulcer healing.
2/ Development of complication:
Perforation
Bleeding
Pyloric stenosis
3/ Other:
Combined duodenal & gastric ulcer.
Highly level of gastric secretion.
47
" Reading without contemplation is like eating without digestion "
Chinese byword
Principle of surgery:
It is to reduce acid & pepsin secretion to certain levels no longer associated with
ulceration.
Operations for D.U:
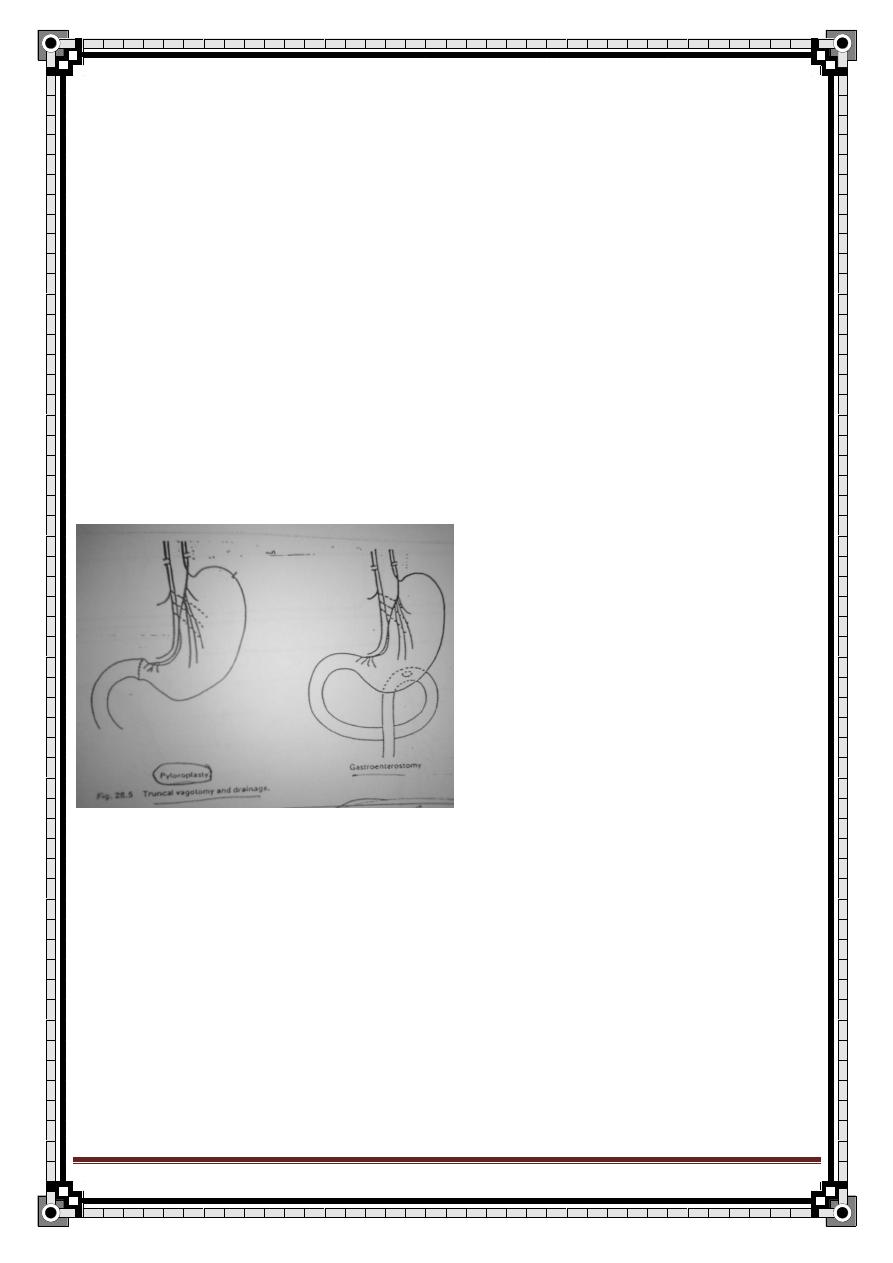
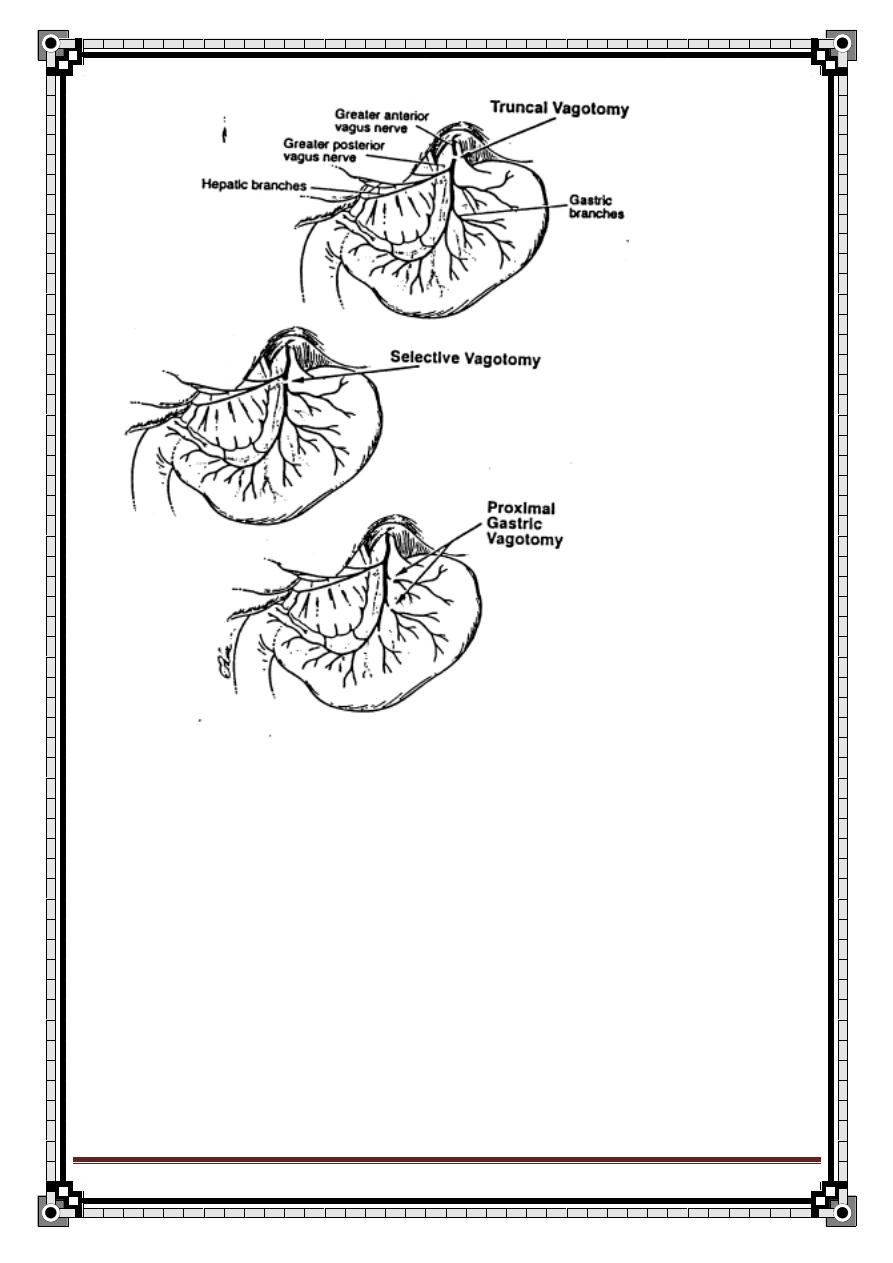
1/ Truncal vagotomy & drainage:
The aim of vagotomy is to reduce gastric acidity.
We cut the major trunk of vagus to the stomach to;
a- reduce acid & pepsin secretion.
b- Impair antral motility & draiage.
So we have to drain by either:
a- pyloroplasty
b- gastrojejunostomy
2/ Highly selective vagotomy: (parietal cells vagotomy)
With or without drainage.
We cut the branch of vagus to the body & fundus ( where more parietal
cells are located) → ↓ HCl secretion.
Here the antrum & the pylorus branches are intact, so we may not need
drainage.
Many surgeons consider it the procedure of choice, although its
recurrence rate is higher than truncal vagotomy.
48
" Reading without contemplation is like eating without digestion "
Chinese byword
3/ Truncal vagotomy + Anterectomy:
Combination of vagal denervation & emoval of the major area of gastric
production.
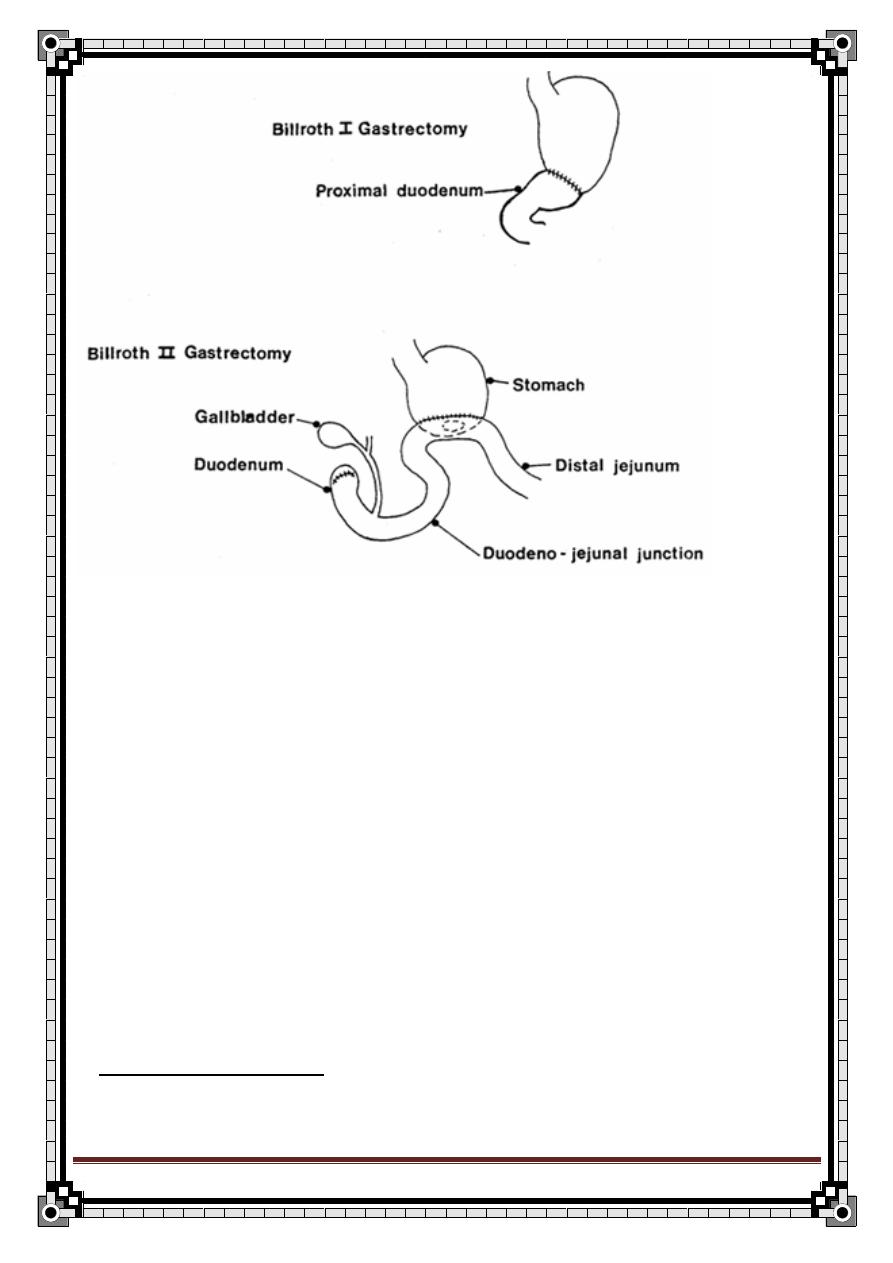
Gastrointestinal continuity is restored by gastroduodenal (Billroth 1)
anastomosis OR gastrojejunal (Billroth 2) anastomosis.
49
" Reading without contemplation is like eating without digestion "
Chinese byword
4/ Partial gastrectomy:
We remove the antrum & proportion of the body of the stomach.
GI continuity was usually restored by closing the duodenal stump &
anastomosing the gastric remnant to the jejunum.
Complication of vagotomy:
Esophagus → Post. vagotomy stricture
Gall bladder → Gall stones
Small bowel → Post. vagotomy diarrhea
Vagus nerve → failed vagotomy
1) Post vagotomy stricture:
o The lower part of esophagus gets narrowed.
o The cause is not known but may be due to:
50
" Reading without contemplation is like eating without digestion "
Chinese byword
i.
Peri-esophagus hematoma.
ii.
Excessive denervation of lower esophageal end.
iii.
Prolong nasogastric intubation → hiatal hernia
iv.
Mucosal edema.
o Pt comes with sever dysphagia.
o Diagnosis: by Barium meal & endoscopy.
o ttt: Bougie nage (dilater).
2) Gall stones:
o Due
to denervated gall bladder which will loose its contraction → biliary
stasis → gall stone
3) Post-vagotomy diarrhea:
o It is passage of watery stool up to 20x a day with the fallowing character:
a- expulsive b- urgent c- watery
o Occur in 2% of truncal vagotomy.
o Can be controlled by cholesteramine.
4) Failed vagotomy:
o It will lead to recurrent ulceration either stomal ulcer or anastomatic ulcer.
Gastric Ulcer Treatment:
Indication for surgery:
1/ Failure of medical ttt:
A benign G.U which fails to heal clinically or endoscopically after 1 mth of
adequate ttt.
2/ Development of complication:
Perforation, bleeding or stenosis (hourglass stomach).
3/ Suspicion of malignancy.
51
" Reading without contemplation is like eating without digestion "
Chinese byword
Operations for chronic gastric ulcer:
Type 1 & 2:
Partial gastrictomy OR truncal vagotomy & drainage.
Partial gastrectomy:
Fallowed by gastroduodenal anastomosis or gastrojejunal anastomosis (Billroth
1, 2)
Complication of gastrectomy:
(1) Immediate (1
st
day):
a- Bleeding:
Usually from the gastric side of anastomosis.
Can be sever & require re-exploration.
(2) Early (1
st
week):
a- Anastomotic leak with its complication:
Sub-phernic abscess.
Pelvic abscess.
Abdominal collection.
Jaundice.
b- Obstruction:
Afferent loop → bilious vomiting
Efferent loop → food vomiting
c- Internal herniation:
Usually fallows gastrojejunal anastomosis.
(3) Late (1
st
month):
a- Dumping syndrome:
52
" Reading without contemplation is like eating without digestion "
Chinese byword
Feeling of epigastric fullness after food, associated flushing, sweating.
Pt feels faint after the meal.
b- Intestinal hurry (diarrhea):
2
– 4% of pt.
c- Iron def. anemia:
Due to post operative anemia, inefficient absorption of dietry Iron post
operative or chronic blood loss from gastritis.
d- Stomal (anastomotic) ulcer:
Recurrence may occur in duodenum or jejunum.
e- Reactive hypoglycemia:
Due
to rapid glucose absorption from the upper small bowel →
hyperglycemia → ↑↑ insulin secretion → reactive hypoglycemia.
Usually 90
– 120 min after meal.
f- Small stomach syndrome:
Vomiting → loss wt
53
" Reading without contemplation is like eating without digestion "
Chinese byword
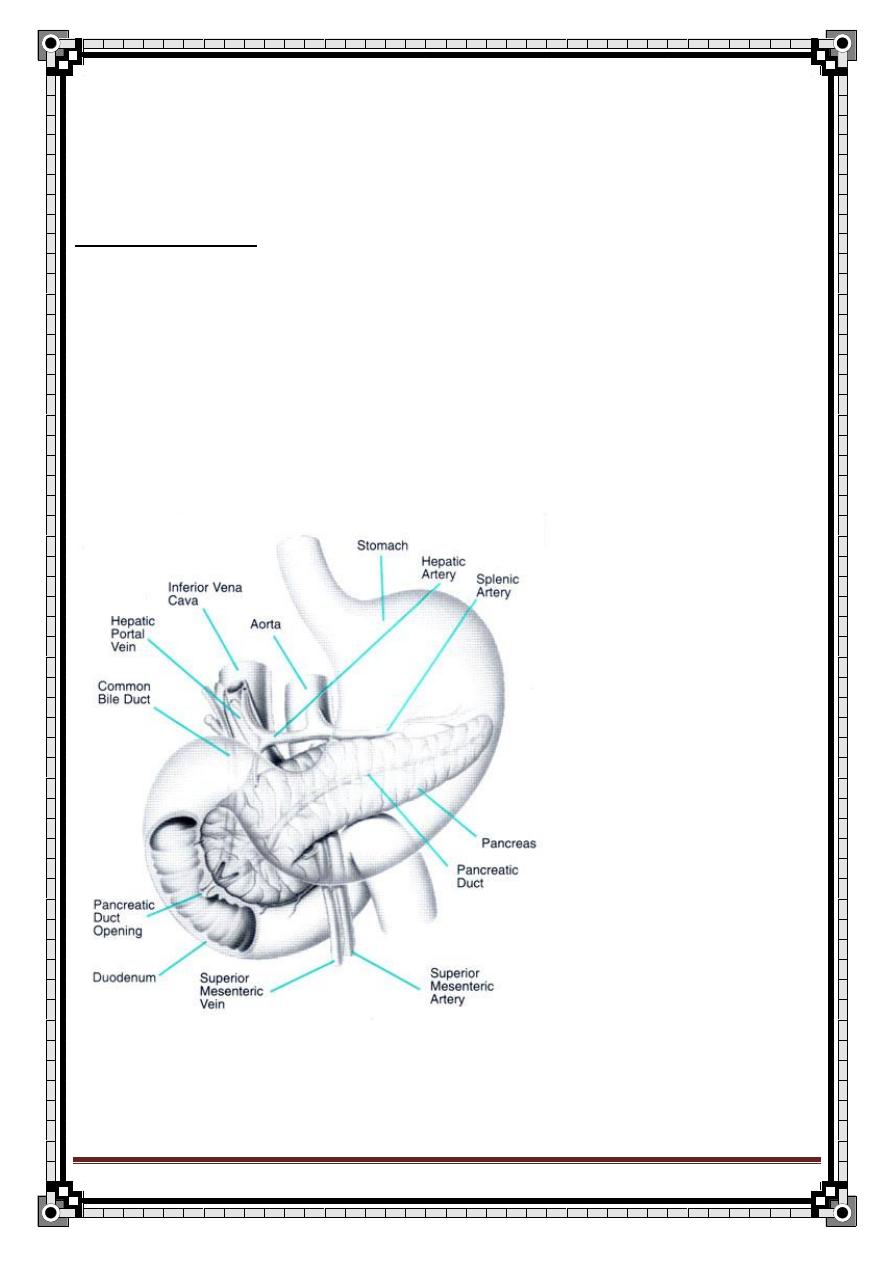
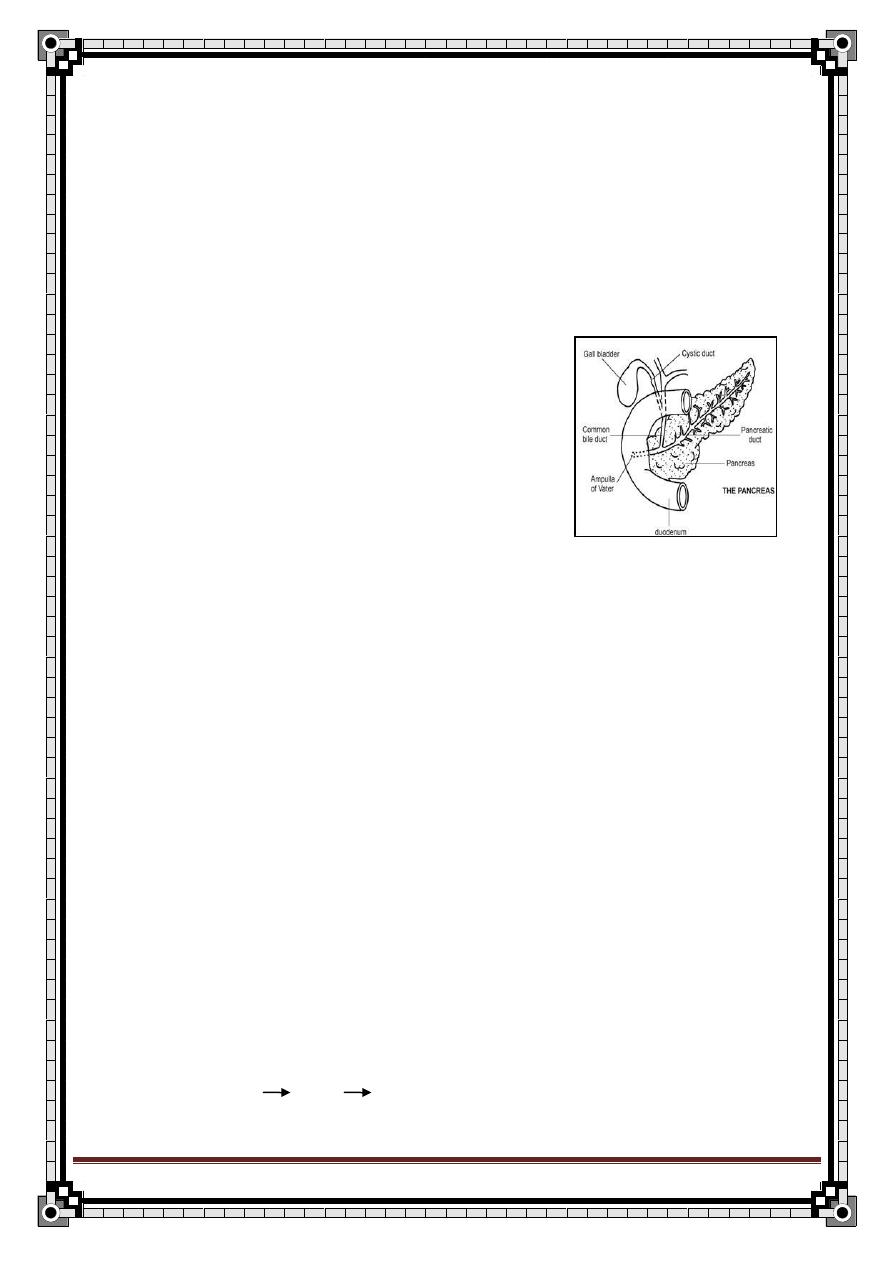
Pancreatitis
Surgical anatomy:
-retroperitoneal organ
-lies behind the lesser sac and stomach
-the head lies within the curve of the duodenum
-the main duct of pancreas begins in the tail and opens into the 2
nd
part of the
duodenum on the major duodenal papilla
-the intimate relationship between the friable pancreas and the major blood
vessels explains why bleeding is a major problem after pancreatic trauma
54
" Reading without contemplation is like eating without digestion "
Chinese byword
-Arterial & venous supply:
o splenic artery
o superior and inferior pancreaticoduodenal artery
o the corresponding veins drain into the portal system
-Lymphatic drainage:
o lymph nodes situated along the arteries that supply the pancreas
o they all drain into the celiac and superior mesenteric L.N.
-Nerve supply:
o sympathetic and parasympathetic nerves
-the close association b/w the common bile duct and the head of pancreas
explains why obstructive jaundice is so common in cancer of the head of the
pancreas, and why gallstones frequently give rise to acute pancreatitis
-Surgical physiology:
-acinar cells synthesize and secret => digestive enzymes
while duct cells secretes => bicarbonate
-pancreatic secretions stimulated by:
P.sympathetic (vagus)
Hormones (secretine, gastrin, CCK, vasoactive intestinal peptide VIP)
pancoenzymes
-it also has 3 secretory phases:
cephalic, gastric, intestinal
-food in duodenum
CCK + pancreas secretions
55
" Reading without contemplation is like eating without digestion "
Chinese byword
-acid in duodenum
secretine + pancreas to secrete watery alkaline
juice
-Digestive enzymes in pancreas:
trypsin proteolytic
lipase lipolytic
amylase starch splitting
ribonucleas nucleic acid splitting
-
don’t forget islet of Langerhans INSULINE
Classification of Pancreatitis:
1- Acute pancreatitis
2- Relapsing acute pancreatitis
Recurrent attacks, and pt. is normal in between the attacks.
3- Chronic pancreatitis
There is a remaining functional or structural damage (irreversible).
Etiology:
o gallstones: billiary pancreatitis
o alcoholism (ethanol) 80
– 85 %
o post-operative (spleenectomy)
o trauma
blunt trauma to the back
ERCP
o distortion of ampulla of vater (carcinoma)
it will lead to stenosis of pancreatic duct pressure in duct
pancreatitis
Other classification:
1- simple
2- hemorrhagic
3- necrotizing
Ampullary stenosis
Tumor pancreatic Duct obst.
Car. Mustation
56
" Reading without contemplation is like eating without digestion "
Chinese byword
o penetrating peptic ulcer
o hypercalcemia
hyperparathyroidism
multiple myeloma
o hyperlipidemia
o drugs
steroids
estrogens
thiazide
o D.M.
o Viral
Mumps, CMV, Coxsackie virus
o Hypoxic
PAN
Shock
5
– 10% are idiopathic
Microscopic Pathology:
- the pancreas is damaged by autodigestion by it own (liberating) digestive
enzymes
1- auto digestion of pancreas (trypsin)
2- fat necrosis (lipase)
3- B.V. necrosis
interstitial hemorrhage
4- association of acute inflammatory rxn
History Taking
Sex:
Male = Female
Age:
Any age
with peak incidence 40’s – 50’s
Symptoms:
1- pain:
site: epigastric
onset: sudden, usually after heavy meal
severity: sharp
nature: vague
progression: steadily increase in severity
radiation: to the back
57
" Reading without contemplation is like eating without digestion "
Chinese byword
duration: variable
aggravating factors: increase by sitting up or movement
relieving factors: by bending forward
association: anorexia, N&V
2- anorexia: b/c eating will aggravate pain
3-N&V
Nausea is persistent b/w the attacks but not nauseated before pain
4-muscle twitches, cramps, or spasm:
in late stages d/t hypocalcemia
Past history:
Hx. Of biliary tract disease
Social History:
Alcohol intake
Contact with a pt. with a mumps
Examination
General:
- Pt. lie still b/c of pain
- In late stages, pale & sweaty (hypovolaemia)
- Dyspnea, cyanosis d/t respiration b/c of pain
- Jaundice 10% (if it is 2ry to gallstones)
- Tachycardia 60%
- Fever 60%
- Tachypnea 50%
Abdominal Examination:
Inspection:
- abdominal movement
- mild abdominal distention (if paralytic ileus develops)
-
Grey turner’s sign
-
Cullen’s sign
5% (hemorrhagic pancreatitis)
Palpation:
- tenderness & guarding in upper abdomen, but guarding is less sever
- epigastric fullness (pseudocyst or lesser sac abscess)
58
" Reading without contemplation is like eating without digestion "
Chinese byword
Percussion:
- resonant (d/t gas collection in the bowel as in P.ileus)
- pseudocyst in the epigastrium will be dull
Auscultation:
- normally present
- may disappears later when bowel movement is paralyzed
SYMPTOMS:
1- Pain
Sudden, sharp, epigastric pain
Radiates to the back
Relieved by sitting and leaning forward
Associated with:
2- Anorexia
b/c eating will pain
3- N/V
SIGNS:
Mild-moderate:
-tachycardia
-fever (low)
60%
-epigastric tenderness & guarding
-tachypnea 50%
-jaundice 10%
-Grey-Turner sign 5%
-
Cullen’s sign
indicate hemorrhagic pancreatitis
(on the flanks & periumbilical, respectively, sign of intra-abdominal hemorrhge)
- or absent bowel sounds in paralytic ilius
59
" Reading without contemplation is like eating without digestion "
Chinese byword
Sever:
or signs of complication:
shock
acute renal insufficiency
anemia
carpopedal spasm
-spiking fever
-sweating if abscess present
-signs of shock if present ( B.P)
-signs of anemia if present (pallor, tachycardia)
=> d/t hemorrhagic pancreatitis
-signs of hypocalcemia if present, e.g. carpopedal spasm
=> d/t consumption of Ca++ in pancreatitis & pseudocytes formation
-signs of pseudocyst, e.g. epigastric fullness
Differential Diagnosis:
1- mesenteric infarction or ischemia
2- acute cholecystitis
3- perforated P.U
4- high small bowel obstruction (duodenal obstruction)
5- acute appendicitis
6- aortic aneurysm
Investigations:
-CBC
leukocytosis
Hg initially normal, but when the progress, it drops
HCT indicating the severity
-electrolytes
K+, Na+ (d/t vomiting)
Ca++
-RFT (renal function test)
60
" Reading without contemplation is like eating without digestion "
Chinese byword
creatinine
BUN with dehydration
-blood glucose
hyperglycemia (d/t islets destruction)
-LFT (liver function test)
abnormal in pt. who still have obstruction in the ampulla of vater
-serum amylase:
elevation > 1000 IU pancreatitis
b/c other diseases may cause elevated S.amylase level but to a lesser
extent
Abdominal causes:
-acute pancreatitis*
-perforated P.U.
-acute cholecystitis
-intestinal obstruction
-afferent loop obstruction following
partial gastrectomy
-ruptured abdominal aortic
aneurysm
-ruptured ectopic pregnancy
-mesenteric infarction
-trauma, open or blunt
The causes of raised serum amylase
(only those marked with an asterisk
cause a marked increase in amylase
(five fold or more))
Impaired renal excretion
-renal failure*
-macroamylasaemia (amylase not
cleared by kidneys d/t complexing or
protein binding)
Salivary gland disease
-salivary calculi
-parotitis
Metabolic causes
-sever diabetic ketoacidosis*
-acute alcoholic intoxication
-morphine administration (causing
sphincter of Oddi spasm)
61
" Reading without contemplation is like eating without digestion "
Chinese byword
-Serum lipase:
more specific than amylase
remains elevated in blood after serum amylase level have retained to
normal after 4-5 days
-Urine amylase:
it takes longer time to come to normal levels than S.amylase
-ABG:
hypoxia in ARDS
the enzymes secreted by pancreas can affect the capillary endothelium
in the lung and causes permeability leading to ARDS
(hypoxia)
-X-ray:
CXR: for ARDS
Abdominal x-ray:
Air under diaphragm (perforated P.U.)
Calcification
Dilated loop of intestine in obstruction
Stone in CBD
-U/S:
looking for gallstones
abscess or pseudocyst
pancreas is
not seen well d/t it’s retroperitoneal position
-CT scan:
to visualize the pancreas and its surrounding
-ERCP:
diagnostic: visualize the bile duct & pancreatic duct
therapeutic: relief the impacted stone by sphincterectomy or
papillotomy
one of the most common complication of ERCP is pancreatitis
Complications:
-shock
d/t pancreatic hemorrhage & release of vasodilator agents (bradykinin)
62
" Reading without contemplation is like eating without digestion "
Chinese byword
-Anemia
b/c of massive hemorrhage
-ARDS
d/t surfactant loss
-Acute renal failure
d/t either:
direct effect of pancreatic enzymes on kidney
b/c of shock causes decrease in renal perfusion
-Carpopedal spasm
d/t hypocalcaemia
-Pancreatic
P.abscess
P.pseudocyst
Fat necrosis
-D.M.
-Paralytic ileus
-Jaundice
d/t bile duct obstruction or portal vein thrombosis
-Intra-abdominal sepsis (i.e. peritonitis)
Treatment:
Mild to moderate:
1- NPO: (i.e. non per oral)
To vomiting
Mild jaundice if:
Pancreatitis caused by gallstones
If edema in head of pancreas is
causing compression on the bile
duct
63
" Reading without contemplation is like eating without digestion "
Chinese byword
To pancreatic stimulation
2- IVF: (i.e. intravenous fluid)
L.R or N.S. 0.5-1 ml/Kg/hr
If pt. in shock give a larger amount
3- Analgesia:
Pethidine
Don’t give morphine b/c it leads to contraction of sphincter of Oddi
=> pain
4- Anti-spasmodic:
To decrease G.bladder & duct contraction
Buscapan
- if pt. have fever & leukocytosis, give Atb
- this is the standard ttt
5- NG tube: (i.e. nasogastric tube)
Suction of acid from stomach
Acid in stomach + secretion production it + pancreas action, so
when you do suction of the acid pancreatic activity
6- Cimitidine:
to H+ secretion
7- Atb:
Some Dr. give it to every pt. with pancretitis
Others only give it if there is fever or leukocytosis
Treatment of complications:
1- shock: IVF
2- ARDS (hypoxia): O2 mask
3- Hypocalcemia: Ca++ glucanate I.V.
4- Hyperglycemia: insulin
5- Abscess: drain
Other measures:
1- peritoneal lavage:
to early systemic complications of sever disease
2- ERCP:
Endoscopic sphincterotomy (papillotomy)
64
" Reading without contemplation is like eating without digestion "
Chinese byword
Widening of the sphincter of Oddi, so the stone pass out to the
duodenum
3- elective cholecystectomy
Treatment of complications:
1- Pancreatic abscess:
-epigastric pain
-spiking fever
-sweating
always in abscess
-leukocytosis
ttt:
-drainage & Atb
2- Pancreatic pseudocyst:
-pain
-NO fever or leukocytosis
-if large we can palpate it
ttt:
-wait for 6 weeks, the majority will disappear, if not resolved:
1. external drainage
2. internal drainage
pseudocystogastrostomy
drain pseudocyst to the stomach
Prognosis:
Factors which determine the severity of acute pancreatitis,
65
" Reading without contemplation is like eating without digestion "
Chinese byword
Ranson’s Criteria is used to determine the severity, other indices used like
Glascow critetia.
On admission:
-age > 55 y
-blood glucose > 200 mg/dl
-WBC > 16,000 /mm3
-LDH > 700 IU
-SGOT (AST) > 250 franke U/dl
After initial 48 hr:
-HCT decrease more than 10%
-serum Ca++ < 8 mg/dl
-BUN > 5 mg/dl
-base deficit > 4 mEq / L
-fluid sequestration > 6,000 ml
-Po2 < 60 mmHg
-presence of 3 factors or less
Mild Pancreatitis
(mortality rate 1%)
-presence of > 3 factors
Sever Pancreatitis
(mortality rate 30%)
-serum Amylase has nothing to do with prognosis.
66
" Reading without contemplation is like eating without digestion "
Chinese byword
Intestinal Obstruction
History
Identity
Age: imp. To reach the nearest cause.
History of present illness
:
1)pain:
1
– onset depend on the type of obs.
2- site centrally S.bowel
suprapubic L.bowel
3-severity mild to moderate
awake him from sleep
Interfere With pt live
force the pt to roll around
4-nature coicky : Intermittent, Hollow viscous, contraction against
resistance S.bowel
discomfort L.bowel
5-progression fluctuating
6-duration
7-relieving factors
8-agg. Factors
9-radiation
10-associated symptoms :Non specific fever, sweating , weakness,
Related to system involved: vomiting
2) abd. Distention: time ( early, late)
degree of the distention (progression)
how was it noticed? (by himself or the dr.)
does it relieved by vomitimg or bleching?
Slight pain
Raise and fall irregular in
severity
67
" Reading without contemplation is like eating without digestion "
Chinese byword
3)Vomiting: time (early, late, delayed or absent)
content
color
smell
volume
4-Constipation: Time (early, late)
if he passed stool of flatus? When?
** ask about other GIT sym.
** ask about fever infection or strangulation
Past Hx : -previous operation or illness.
Continue the rest of Hx points.
Examination
General signs:
Signs of dehydration if the pt had copious vomiting
1) tachycardia
2) hypotension
3) dry skin
4) dry mouth
5) loss of skin turgor
6) oliguria
Local abdominal Signs
:
Inspection scar of previous operation
distention (central S.bowel, peripheral L.bowel)
68
" Reading without contemplation is like eating without digestion "
Chinese byword
visible peristalsis ( in thin people)
irreducible or strangulated swelling at hernial orifices
Palpation abd. Mass suggesting hernia, CA or intussusceptions.
obs. hernia.
tenderness, rebound tenderness, rigidity indicating
generalized peritonitis.
Percussion resonance b/c of gas filled bowel.
tenderness on percussion indicate peritonitis or early
strangulation.
Auscultation Metalic click as the pressure is raised if much gas is
present in the bowel.
gurgling borborygmi if gas & fluid are present in the bowel
Rectal Ex:
fécal impaction
rectal tumor
bl. On finger may indicate mesenteric a. occlusion
sigmoid volvulus
intussusceptions
Investigation:
1)
plain abdominal X-ray
(erect and supine ) distended (gas)
fluid
–filled-coils
S.bowel obs. centrally located
a ladder pattern of the dilated loop.
69
" Reading without contemplation is like eating without digestion "
Chinese byword
striations that pass completely across the width of
the distended loop produced by the circular mucosal folds called
valvulae conniventis.
N.B:
- Jejunum valvulae conniventis
- Ilium featureless
- cecum round gas in the RIF
L.bowel obs. peripherally located
show haustration of the taenia coli, which do not
extend across the whole width of the bowel.
2) Baruim follow-through
series of X-rays taken following ingestion
of barium sulphate
used in suspected cases of S.bowel obs.
3) Water soluble contrast enema
in L.bowel obs. d.t CA or
diverticulum
Gastrografin is used instead of barium
4) Sigmoidoscopy :
in the L.bowel may reveal CA
sigmoid volvulus
inflame. Stricture
** can be therapeutic in sigmoid volvulus
5) CT scan:
useful to Dx obstructing lesions & colonic CA.
6) Non specific Investigation:
1- CBC
increase WBC in inflame.
70
" Reading without contemplation is like eating without digestion "
Chinese byword
// Hb, PCV d.t dehydration & hemoconcentration
2 - electrolyte decrease especially Na & Cl d.t vomiting.
The pt may have hypokalamia d.t vomiting ( loss of HCl, so the
kidney will correct this by secrete K+ & reabsorb H+
Others important Information
Classification:
1- Paralytic obstruction.
2- Mechanical obstruction which is further classified according to:
1) Speed of onset acute (rapid onset & severe symptoms)
chronic (slowly progressive & insidious )
acute on chronic (as the obs. Suddenly become
complete)
2) Site high (small bowel)
low (large bowel)
3) Etiology:
In the small intestine:
1- Extramural strangulated hernia (external or internal)
volvulus
adhesion
bands
intussusception
tumor
71
" Reading without contemplation is like eating without digestion "
Chinese byword
2- Intramural stricture ,congenital atresia
inflame. (chron’s dis.)
tumor
diverticulitis of the colon
3-Intralumenal fecal impaction
gall stone
food bolus
pedunculated tumor
swallowed foreign body
((The commenest causes in the s.bowel are adhesions & hernia))
In the large intestine cancer (commonest)
sigmoid volvulus
sigmoid diverticulitis
** age & the common causes of the alimentary tract obs.
72
" Reading without contemplation is like eating without digestion "
Chinese byword
Browse p.413
Age
Cause
Neonate
Atresia
Meconium obs.
Volvulus neonatorum
3 wks
Congenital hypertrophic pyloric stenosis
6-9 mon.
Intussusceptions
Teenage
Inflame. Mass (appendicitis)
Intussusceptio
ns of Meckel’s diverticulum or
polyp
Young adult Hernia
Adhesion
Adult
Hernia
Adhesion
Inflame. (app., Chron’s)
CA
Elderly
Ca
Inflame.
Sigmoid volvulus
4) surgical pathology
a) MECHANICAL OBS. (dynamic):
Mechanical obs. occur in which there is a bowel capable of
contracting normally proximal to the local site of obs.
More common in the s.bowel
3 main types:
73
" Reading without contemplation is like eating without digestion "
Chinese byword
1-
Simple occlusion:
When the bowel is occluded w/out damage to the bl. Supply
The intestine distal to the site of occlusion rapidly empties & become
collapsed
The bowel above the obs. Become dilated d.t accumulation of
a)
gas swallowed air OR
putrefaction within the lumen
b)
fluid poured out by the intestinal wall together w/ gastric,
biliary & pancreatic secretion.
This will lead to fluid & electrolyte loss
There will be increase in the peristalsis colic
Another cause for the fluid depletion is the distention of the bowel
which leads to impairment of the bl. Supply. The mucosa is th 1
st
part of the bowel wall to show the effect of the ischemia, leading to a
net excretion of the water & electrolyte into the lumen decrease
the extracellular fluid & hypovolemia.
Part of this fluid will be lost by vomiting the rest may accumulate in
the gut.
So, - 2 L of ECF
ــــlost ـــ> prior to vomiting
- 4 L w/ vomiting & dehydration occur
- 6 L circulatory collapse w/ hypovolemic shock
** in simple obs., the development of shock occur d.t depletion of ECF
2-
Closed loop obs. (special type of simple obs.):
The occlusion occur at both ends of the loop of the bowel
Mechanism: obs. In distal part & valve like mechanism proximally that
allow the entry of the food and prevent the exit, most commonly in Lt
colon (cecum) w/ competent iliocecal valve.
Also can occur in torsion of the small bowel.
obs. External hernia.
sigmoid volvulus.
74
" Reading without contemplation is like eating without digestion "
Chinese byword
3-Strangulation:
Initially, there will be venous occlusion edema in the bowel wall
Arterial bl. Continues to enter the bowel until prevented by the
increasing back pressure ischemia infarction gangrene
perforation.
** the development of shock is accelerated by the bacteria & toxins which
pass from the ischemic wall ( which no longer can act as a barrier) to the
peritoneal cavity 2ry peritonitis to the bl. Stream bacteremia.
The Cardinal symptoms:
1) Pain:
Usually the 1
st
sym.
In S.bowel colicky
centrally located (peri-umbilical)
accompanied by hyperperistelatic rushes
every 2-20 min.
In L.bowel more discomfort
suprapubic
Every 30 min.
2) abd. Distention:
Absent or late in high obs.
Marked & delayed in low obs.
3) Vomiting:
Early in high obs.
Late or even absent in low obs.
In S.bowel obs. the vomitus is initially clear & contain food (if in pylorus)
fluid bilious feculent (later d.t bacterial decomposition of the stagnant
contents of the bowel
75
" Reading without contemplation is like eating without digestion "
Chinese byword
4) Absolute constipation:
Is failure to pass either flatus or faeces.
Early in L.bowel obs.
Late in S.bowel obs.
The pt may have bowel motion at the onset of the mech, obs. as the distal
part of the bowel empties its content.
Constipat
ion may be absent in partial obs, Richter’s hernia & pelvic mass.
How to diff. btw mech. & non-mech. Obs.?
Diff. btw these 2 types is imp. Since paralytic ileus (p.i) is ttt conservatively while
mech. Obs. usually calls for urgent op.
p.i
Mech.obs
Duration
3-4 days
>4 days
Bowel sounds Silent (Dxtic)
Noisy
Pain
- ve
+ ve
X-ray
Diffuse app. Of gas
Distended loops w/out gas
shadows in the colon or
rectum
There are 3 imp. Points to remember about intestinal obs.:
1) it is diagnosed by the presence of: (cardinal sym. Of in. obs.)
colicky abd. Pain
distention
absolute constipation
vomiting
2) Ex. Should always include a search for hernias
3) Is it simple or strangulated? Feature suggesting strangulation are:
Tachycardia
Pyrexia
Peritonism
Bowel sounds are absent or reduced
leukocytosis
76
" Reading without contemplation is like eating without digestion "
Chinese byword
Hernia
Hernia is the protrusion of an organ through its containing cavity wall.
Could be either congenital or acquired.
Divided into:
External abd. Hernias inguinal
femoral
umbilical & paraumbilical
incisional
epigastric
Internal abd. Hernias diaphragmatic
paraduodenal
paracaecal
iatrogenic internal
Varieties:
Reducible when the contents of the sac of the hernia can be replaced
completely into the peritoneal cavity either spontaneously or manually.
Irreducible
when the contents of the sac of the hernia can’t be replaced
into the abd.
Incarcerated the contents are literally imprisoned in the sac of the
hernia (usually by adhesions) but are alive & functioning normally and is
NOT tender.
Obstructed a loop of the bowel is kinked or trapped w/in the sac of the
hernia in such a way that the lumen but not the bl. Supply is obstructed.
Strangulated the bl. Supply to the content of the sac has been cut 7
they are dead or dying. It is acutely tender.
femoral hernia is more likely to be str. b/c the narrowness of the
Neck & its rigid wall.
clinical features include sudden pain
vomiting
77
" Reading without contemplation is like eating without digestion "
Chinese byword
tenderness
complications paralytic ileus
toxic shock
Ri
chter’s hernia only part of the circumference of the bowel is
strangulated. So, there will be signs of strangulation (tenderness) but there
are no signs of ints.obs.
Aetiology
:
Predisposing factors:
Congenital defect:
1- Persistence of the processes vaginalis allowing ing.H formation
2- Patent canal of Nuck in female ing.H
3- Incomplete obliteration of the umbilicus umbilical.H
4- Persistence of the communication btw the abd. & the thoracic cavity
diaphragmatic.H
Acquired defect:
1- Weakness of the ant.abd. wall can result from surgical incision
incisional.H
2- M. weakness d.t streatching of the abd. m. as a result of obesity,
pregnancy or n. damage (e.g. ingury to the ilioinguinal n. following
appendectomy Rt ing.H)
Precipitating factors:
d.t increase in the intra-abd. pressure b/c of:
chr. cough
straining at defecation
chr. constipation
urethral or bladder neck obs.
pregnancy
asctis
78
" Reading without contemplation is like eating without digestion "
Chinese byword
severe muscular efforts or lifting heavy objects
Composition of Hernia:
Hernia consists of 3 parts:
1- The sac: usually has mouth, neck, body, fundus
- Absent in direct & incisional H.
- Narrow in femoral & umbilical H. more liable to be strangulated
- N.B: indirect H is narrower then the direct
2- The covering: derived from abd. Wall layers:
Skin subcut. Tissue external.oblique.m in.ob.m. transversus
Abdominis fascia transversalis extraperitoneal fat peritoneum
3- The contents: fluid:the most common,derived from the peritoneal exudate
Omentum: omentocele
int.: enterocele (usually s.bowel)
part of the large bowel
part of the bladder: diverticulum of the bladder
Meckel’s div. Littr’s H
Inguinal hernia
Anatomy:
Inguinal ligament: is the Aponeurosis of the external oblique m. when folded
back & attached btw 2 bony points medially to the pubic tubercle
laterally to ant.sup.iliac spine
Inguinal canal: it is an oblique passage through the lower part of the ant. Abd.
Wall which allow structure to pass to & from the testis in the male and allow the
passage of the round lig. Of the uterus in the female.
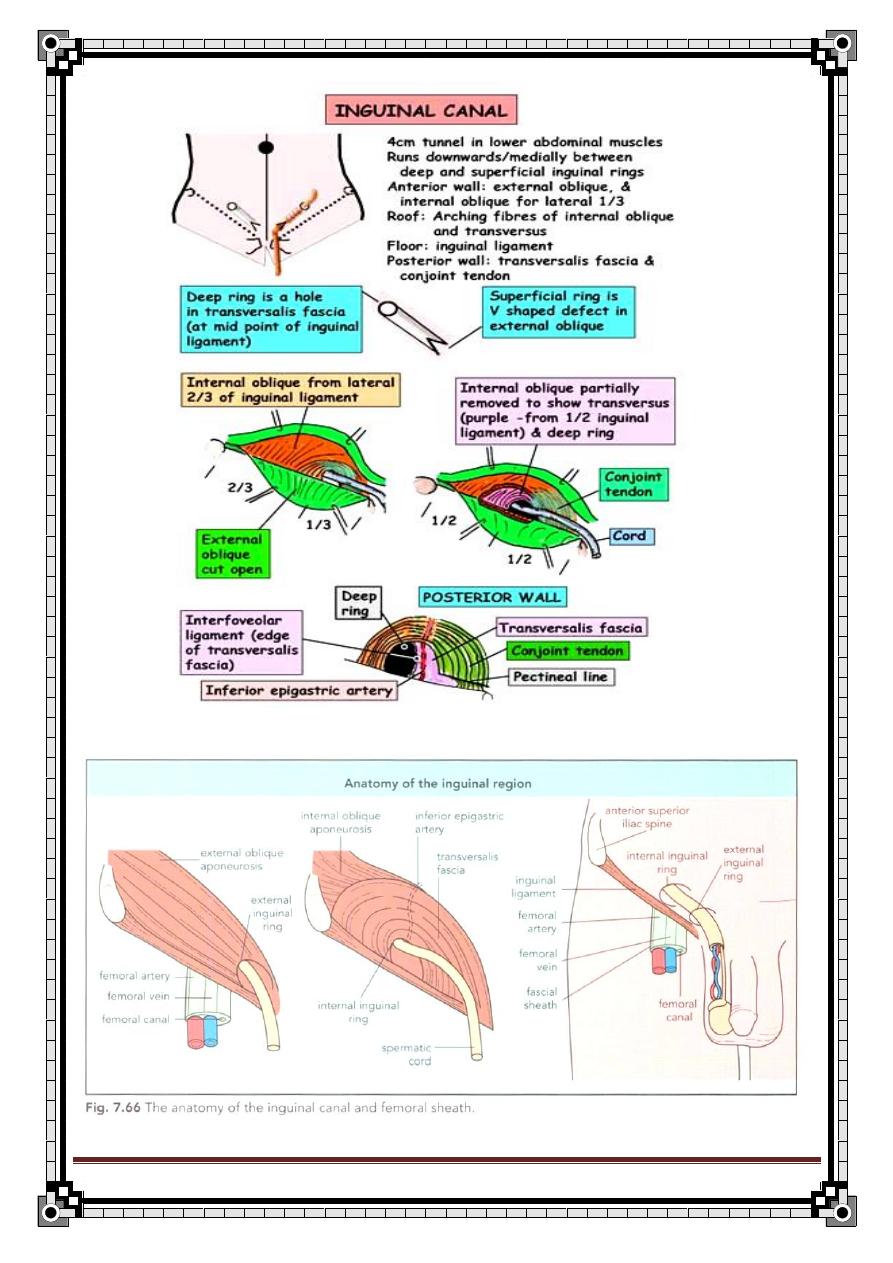
79
" Reading without contemplation is like eating without digestion "
Chinese byword
80
" Reading without contemplation is like eating without digestion "
Chinese byword
Deep ing. Ring: an oral opening in the fascia transversalis ½ inchs (1.3cm)
above the ing.lig. midway btw the A.S.I.S & the symphysis pubis.
lateral to inf. Epigastric vessels.
How to find the site of the deep ing.ring??
By 2 way:
1-by bony promenance: mid-point btw Ant.sup.iliac spine & symphysis pubis
Then 1cm above it.
2- by feeling the femoral a. & following it above until it disappears, then feel 1
cm above it.
Superficial ing. Ring: is a triangular defect in the aponeurosis of the ex.ob.m.
lying just above & medial to the pubic tubercle.
How to find site of the sup. Ing. Ring??
Just above & medial to the pubic tubercle
You can find the pubic tubercle byflexion of the hip + external rotation &
follow the adductor longus m.
or feeling the sym.pubis & then 2cm lat.To it
Contents of the ing.canal:
1- ilioinguinal nerve.
2- Spermatic cord & its content:
Vessels testicular a.
// v.
a. to the vas deferanse
cremastric a.
Nerves genitofemoral
autonomic n.
Reminants of the processus vagianalis
L.N
Vas deferense
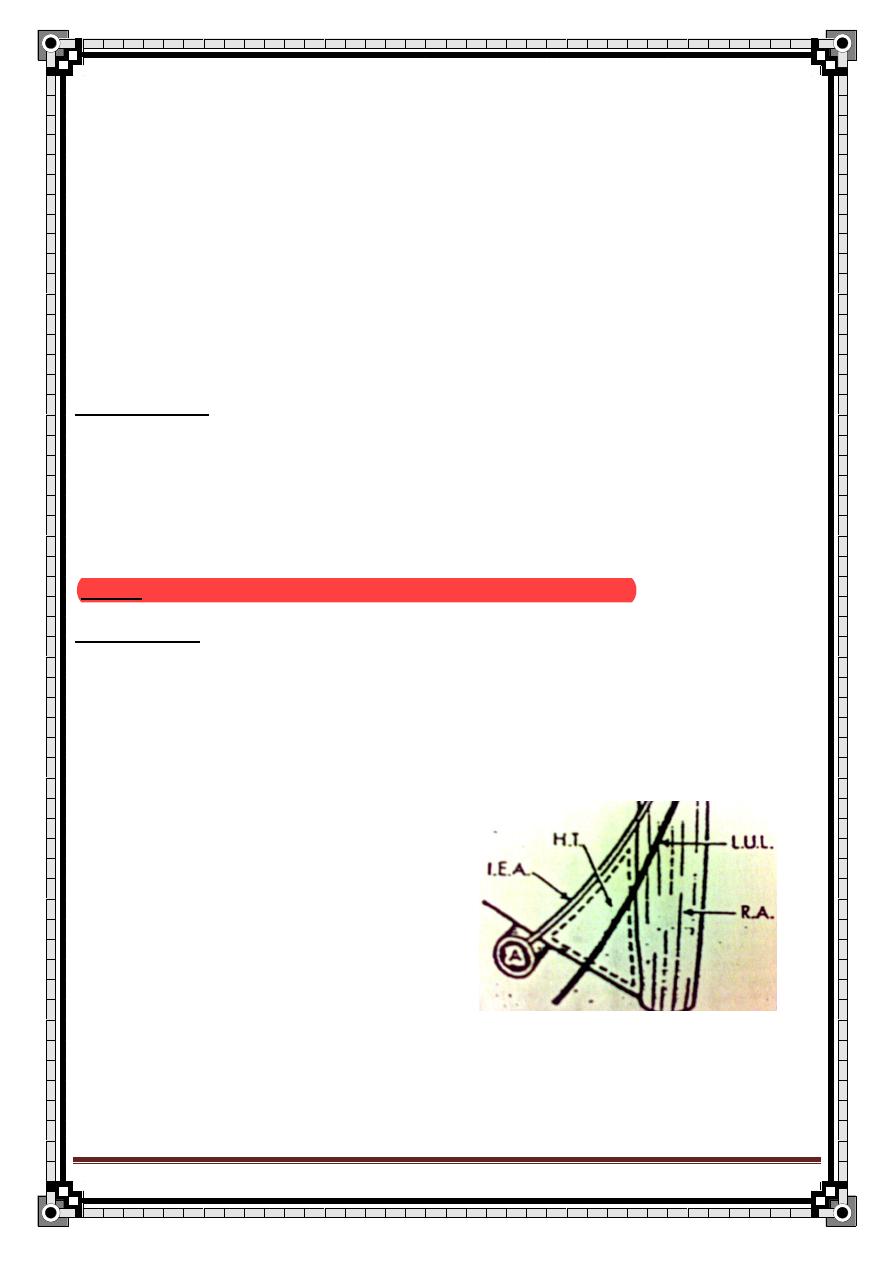
81
" Reading without contemplation is like eating without digestion "
Chinese byword
Inguinal H.:
Def.: protrusion of part of the abd. contents through the ing. Region of the
abd. wall.
80% of the abd. H is groin H & of 3 types indirect ing.H (60%)
Direct ing.H (25%)
femoral H (15%)
♂ > ♀ & the COMMONEST is the indirect H.
Femoral H is more common in ♀ BUT still the MOST COMMON in ♀ & ♂ is
the indirect ing.H.
Indirect ing.H:
- descends along the line of the processus vaginalis & the vas deferens,
entering through the in.ing.ring & traversing the ing. Canal & lies w/in the all
covering of the spermatic cord & can reach down to the scrotum in ♂.
-Cause: Failure of the obliteration of the processus vaginalis.
Direct ing.H:
- pushing through the post. Wall of the ing. Canal medial to the internal ring.
-
it protrudes through a ▲ known as Hesselbach’s ▲ which is bounded by:
Medially lat. Border of the
rectus abdominis m. (R.A)
Laterally Inf. Epigastric a (I.E.A)
Base ing.lig.
82
" Reading without contemplation is like eating without digestion "
Chinese byword
Differentiation btw indirect & direct hernia:
indirect
direct
Origin
Pass through the
in.ring lat. to the I.E.
vessels
Pass through the
post. Wall of the ing.
Canal med. To the
I.E. vessels
Etiology
May be congenital
Always acquired,
rare in childhood &
adolscence
Control by pressure
over the in.ing.ring
Yes
No
Direction of
reduction
Reduces upward, then
lat. & backward
Reduces upward &
then straight
backward.
Reappearance
after reduction
In the middle of the
ing. Region then flows
medially & downward
Exactly where it was
before
Palpation
NOT palpable as it is
behind the fibers of the
ex.ob.m
Can be felt in the
abd.wall above the
pubic tubercle
strangulation
Commonly, b/c of the
narrow neck
Rarely, b/c usually it
has a wide neck
Extending to the
scrotum
Often
Rarely
Reduction on lying
NOT redialy
spontanously
Recurrence after
op.
uncommon
More common
How to diff. btw indirect ing.H & hydrocele:
83
" Reading without contemplation is like eating without digestion "
Chinese byword
Special varities of the ing. H:
- Pantaloon H.=dull H.=Saddle bag H.: both direct & indirect ing.H. are found
in the same groin.They appear as 2 sacs which are straddled by the I.E.A
- Sliding H.: a H. of a piece of the extra-peritoneal bowel ( caecum, terminal
ileum on the Rt & sigmoid colon in the Lt.) which slides down into the ing.
Canal, pulling a sac of the peritoneum on its surface.
-
Maydl’s H.: (rare) tow loops of the bowel in the sac, w/ strangulation of the
loop of the bowel in the abd. which connects them.
- Recurrent H.: more likely to present w/ more pain than a new H.
- bubonocele: the H. is limited to the ing. Canal
- Funicular: the processus vaginalis is just closed above the epididymis. The
contents of the sac can be felt separately from the testis.
- Complete (scrotal): the testis appear to lie w/in the lower part of the H.
Indirect ing.H
hydrocele
Palpation of the
neck of the scrotum
You can’t get above it
(feel the upper edge)
You can rech above
it
Tranillumination
- ve
+ ve
Cough impulse
+ve
- ve
84
" Reading without contemplation is like eating without digestion "
Chinese byword
How to take Hx from pt w/ ing.H?
I.D:
Age: indirect ing.H young
Direct ing.H old age
Occupation:heavy works,especially lifting,puts a great strain on the abd.m
C.C: pt usually complains from:
1- Swelling in the groin or in the scrotum + the duration
2- Discomfort or pain in the groin or in the scrotum
OR the pt may present w/ the sym of intestinal obstruction:
Colicky abd. pain
Vomiting
abd. distension
Absolute constipation
Or sym of strangulation becoming very painful & tender
Or toxic sym d.t perforation peritonitis
HPI: according to the C.C:
If the pt compilan of a lump
1- Ask the routine Q for any lump.
1- Site: is on Rt, Lt, or bilateral?
2- First symptom: how did it start(the onseton straining,coughing or lifting
heavy wt)?
85
" Reading without contemplation is like eating without digestion "
Chinese byword
3- Progression: where did it 1
st
appear & what was its size at that time?
4- Extension: does it extend after that (to the scrotum)?
5- Disappearance: does it disappears automatically, on lying down or
reduced by hand?
6- Multiplicity: there is any other mass
7- Pain: Is it ass. W/ pain or not?
2- Sym. Of strangulation tender & v.painful & the pt become febrile
tense & irreducible
change of its color & ↑ in size
3-Sym. Of int.ob as mentioned before
4-Ask about the predisposing: factors as mentioned before
Past Hx:
1.
a previous op. incisional H
2.
Hx of appendectomy d.t injury to the ilioinguinal n. intraop. Which
leads to weakness of the abd. m. Rt direct ing. H
3.
Hx of H repair in the same side recurrent H
4.
// // // opp. Side Rt ing.H generally proceeded by Lt
Social Hx:
1.
Is these sym affects the ability to work?
2-Hx of heavy smoking chr.cough
86
" Reading without contemplation is like eating without digestion "
Chinese byword
How to Ex a pt w/ ing.H?
Aims: to determine the Dx signs of H. position
expansile cough impulse
reducibility
- Prepare the pt expose both groins (from umbilicus to mid-thigh)
1
st
on standing position then on supine position.
always examine & compare both ing.region
A) Inspection:
from the front & back
1- Site: swelling in the groin (is it Lt, Rt or bilateral?)
2- state of over lying skin:Color of the skin should be normal
the skin will turn to red color if the H is strangulated.
notice if there is a scar Recurrent H
3- Shape Indirect susage shaped or oval.
Direct rounded
4- Size: variable
5- Cough impulsethe H. become larger & more tense in all directions
(expansile)
6- Involvement of the scrotum.
7- Position of the penis pushed to the other side.
B) Palpation: from the front & the sides
1- Temperature normal
if warm strangulated
2- Tenderness if +ve strangulated
87
" Reading without contemplation is like eating without digestion "
Chinese byword
3- Position to diff. btw the ing. & femoral H palpate from the pubic tubercle:
if the swelling is above & medial to it Ing.
below & lateral femoral
4- Surface smooth
5- Composition soft, resonant & fluctuant bowel.
firm(rubbery), granular, dull & non-fluctuant omentum.
6- Cough impulse compress the lump firmlt w/ your fingers, ask the pt to turn
his head to the opp. Side & cough, if the swelling expends & become more
tense +ve
- the presence of it is Dxtic BUT its absence does NOT rule out the Dx.
7- Involvement of the scrotum: determine if the swelling is:
Pure ing.
Ing.scrotal
Pure scrotal
By palpation of the neck of the scrotum btw your finger as (mentioned before)
8- Testis if can be felt separately or not
9- Compressibility & reducibility +ve, but unlike vascular tumors it will not
expand or reappear immediately unless some force, such as gravity of cough
forces it out.
10- Ring occlusion test if the swelling is reduced only by pressure on the
ex. Ing. Ring direct ing.H
if it can be controlled by pressure on the in.ing. ring
indirect ing. H
11- remove your hand & watch the H reappear slides obliquely indirect
directly forward direct
12-exam of the back for psoas abscess
88
" Reading without contemplation is like eating without digestion "
Chinese byword
C) Percussion: resonant bowel
Dull omentum
D) Auscultation: presence of thr bowel sounds enterocele
E) PR Ex: constipation tone of the anal sphincter
Anal fissure
Any mass
Urine retention enlarged prostate
-
Don’t forget general Ex.
DDx of ing.H:
1- Femoral H.
2- Vaginal hydrocele.
3- Hydrocele of the cord or of the canal of Nuck.
4- Undescended testis.
5- Lipoma of the cord.
DDx of a lump in the groin
In the hernial orifices: - inguinal hernia
- Femoral hernia
In the testicular apparatus: - hydrocele of the cord
- spermatocele
- undescended testis
Vein: saphena-varix
Artery: femoral aneurysm
LN: lymphadenopathy which could be either infection,lymphoma or
secondary neoplasm.
In the psoas sheath: -psoas abscess
- psoas bursae
89
" Reading without contemplation is like eating without digestion "
Chinese byword
In the skin or subcutaneous; lipoma
ttt
:
ttt of the cause of H. 1
st
(e.g. Chr.cough, constipation, …..)
ttt of indirect ing.H:
In the past conservative ttt was used (truss),but now the ttt of choice is the op.
In infants: Herniotomy is enough (excision of the H. sac only). b/c the abd. m.
is normal & the in.ring is not dilated.
In older children & adults: abd. m. is normal & the in.ring is dilated. So, the ttt
is herniotomy + narrowing of the ring around the cord.
In older pt: the post. Wall of the canal is weak. So, we need to tight the in.ring
& strength the opst. Wall herniotomy + herniorrhaphy (repair)
This op. consists of:
1- excision of the H. sac & ligation of the neck of the sac.
2- Repair of the stretched in. ring & fascia transversalis
3- Then, one of the following choices can be done:
- Shouldice repair- this is a double breasted repair of the
transversalis fascia followed by suturing of the conjoint tendon
to the inguinal ligament with non-absorbable suture.
- Lichtenstein repair- tention free mesh repair using polypropylene
mesh (hernioplasty)
- Laproscopic- this may be via an extraperitonial or intraperitonial
technique.
ttt of direct ing.H
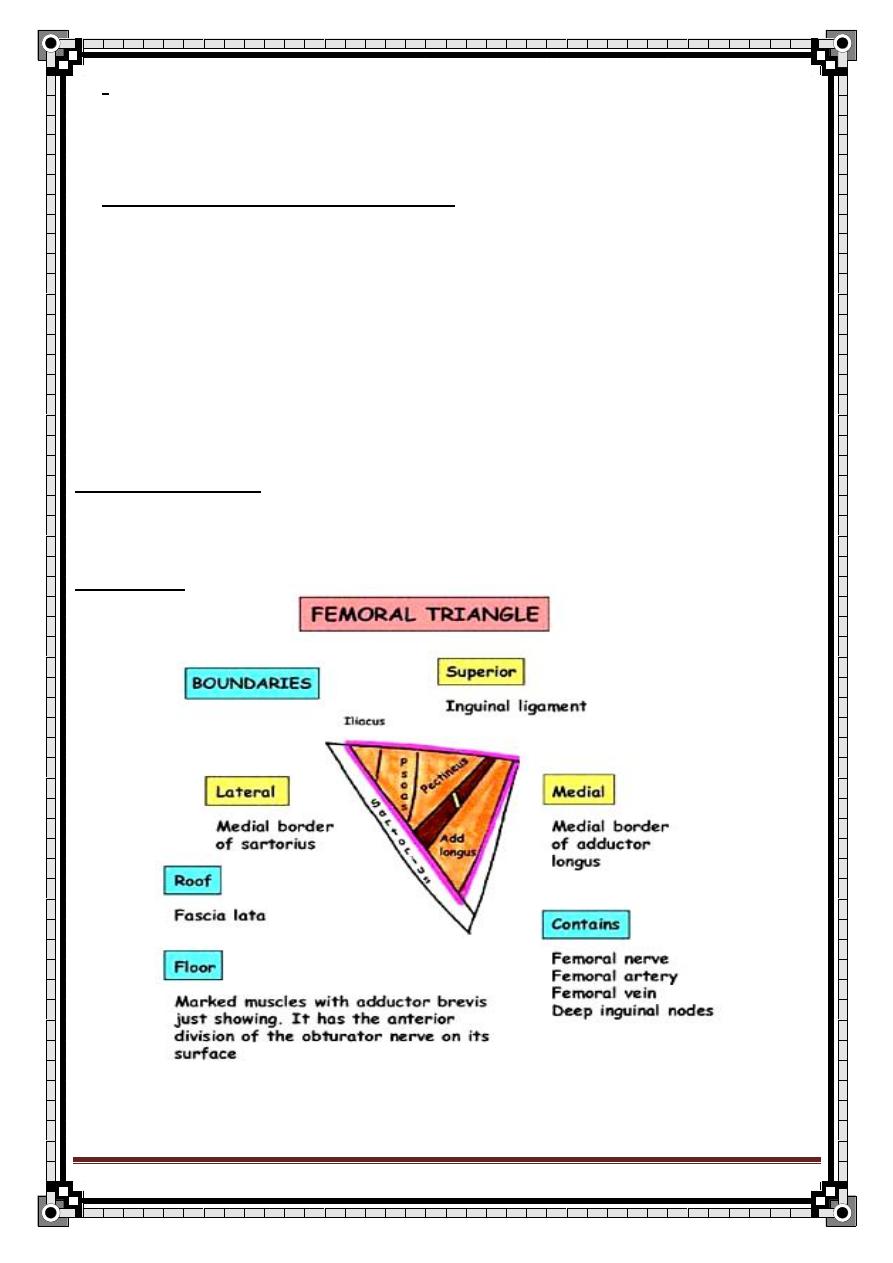
90
" Reading without contemplation is like eating without digestion "
Chinese byword
:no need to excise the sac b/c of widening of the neck. Simply invaginate the
sac inside+few sutures in the fascia transversalis.
Complication of the Herniorrhaphy:
1- wound infection (5-8%)
2- Hematoma
3- Acute urinary retention
4- Respiratory complication
5- Bleeding to the ing;. Canal or the scrotum (may predispose to infection)
6- Chr. Pain d.t trapping of the ilioinguinal n.
7- Tightening /compression of the testicular a.testicular atrophy &/or pain
8- Recurrence in 5% of the pt.
Femoral Hernia
Anatomy:
Femora
l ▲:
Femoral canal:
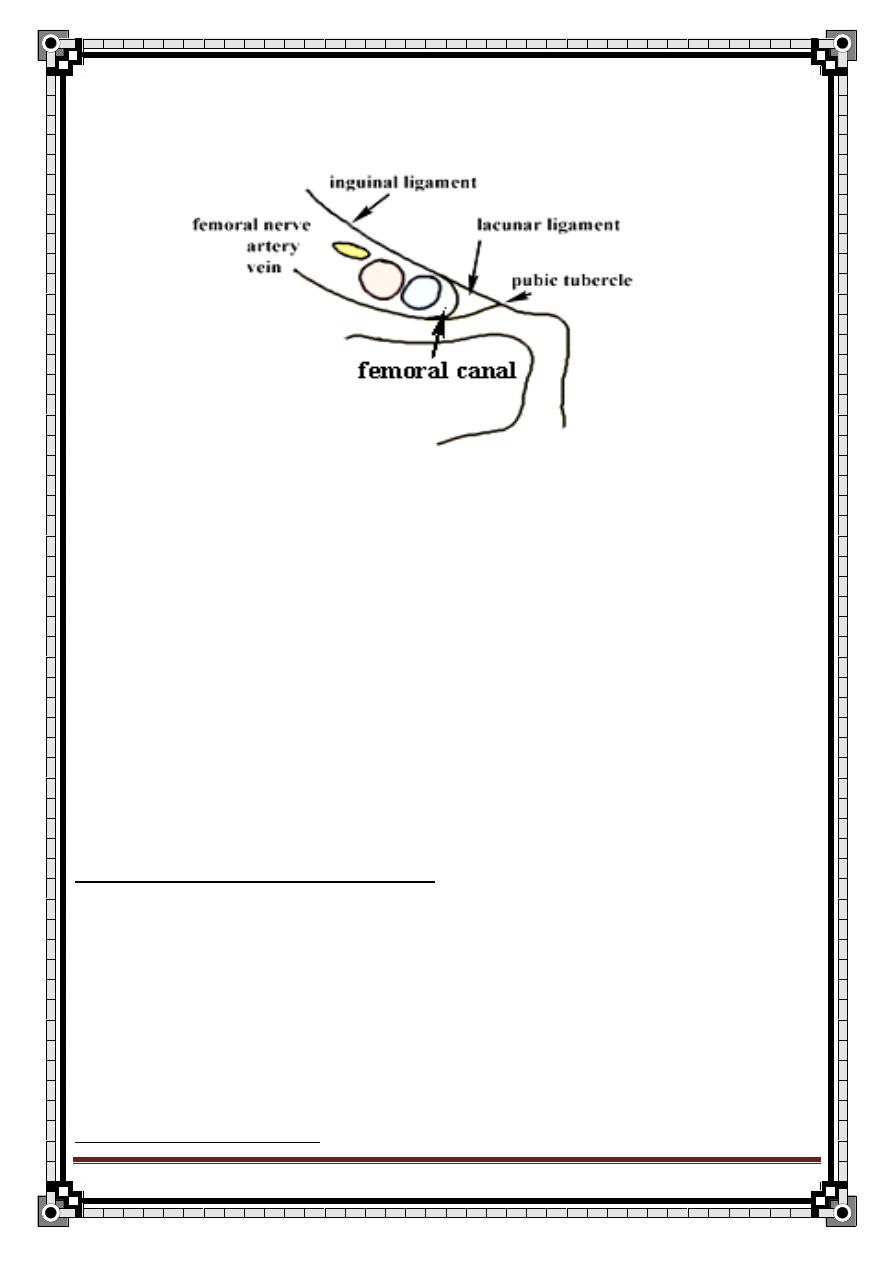
91
" Reading without contemplation is like eating without digestion "
Chinese byword
Short gap (1.5 cm), coincide the compartment of the femoral sheath.
- Its abd. end is called femoral ring.
So, it has a rigid wall more prone to strangulation.
The contents of the canal L.N + fat
Femoral (F.) H.:
Def.: protrusion of the extra-peritoneal fat, peritoneum or sometimes abd.
contents through the femoral ring & down the femoral canal.
The majority of the femoral H. are acquired
♀ > ♂
middle or old age.
Richter’s H. is more likely to occur in the F.sac.
How to take Hx from a pt w/ F.H.?
Same as the ing.H
- Age: over the age of 50, rare in children.
-
Gender: more in ♀.
- Usually bilateral.
How to Ex a pt w/ F.H?
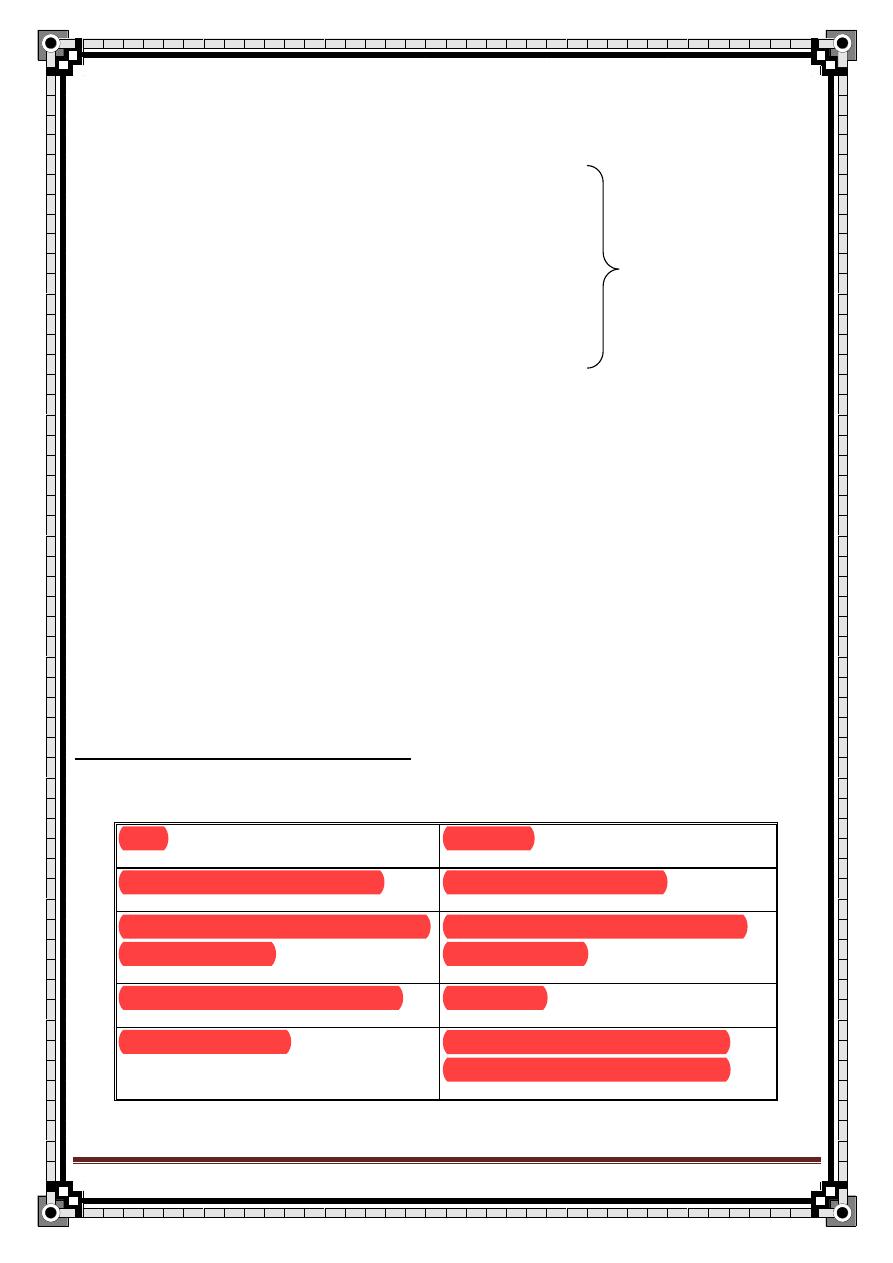
92
" Reading without contemplation is like eating without digestion "
Chinese byword
1- site: lateral to the body of the pubis & inferior to the tip of the pubic tubercle.
The bulge appear to be directly behind the skin creases.
2- color
3- size
4- shape spherical
5- cough impulse may be
–ve same as ing.H
6- temp.
7- tenderness
8- surface smooth
9- composition majority are firm & dull omentum.
10- reducibility
11- relations Dx depends primarily on the site
12- state of local tissue weak area either naturally or by injury
-
Don’t forget General Ex.
Differentiation btw ing. & femoral H.:
Ing.
Femoral
-arise from the ex. Ing. ring
-arise from the F.canal
- reduced above & medial to the
pubic tubercle.
- reduced below & lateral to the
pubic tubercle
- above the groin skin crease
- below it
- soft & reducible
- thick wall & remain palpable
even if it is empty (Dxtic clue)
93
" Reading without contemplation is like eating without digestion "
Chinese byword
**The majority of F.H. passes through the F.ring, where it is usually irreducible
& need surgical intervention EXCEPT rare types which don’t pass through the
canal, e.g.:
-Prevascular femoral H.: bulge down underneath the ing. Lig. In front of the F.
a. & v. usually ass. w/ congenital dislocation of the hip.
-Pectineal H.: passes behind the femoral vessels btw the pectineal m. & fascia.
-Laccunar H.: through the lacunar lig.
DDX of the femoral H.:
is the same as for a lump in the groin.
ttt.:
Truss is contraindicated b.c the risk of strangulation
can’t be fitted to control the F.ring.
So, op. is best ttt.: its principles:
Complete excision of the sac & repair of the defect (obliteration of F. ring):
a) Below the ing. Lig.
b) Through the post. wall of the ing. Canal.
c) From above the ing. Canal best access to the F.ring.
After excistion of the F. sac, F.ring is obliterated by suturing Conjoint
tendon to the pectineal lig.
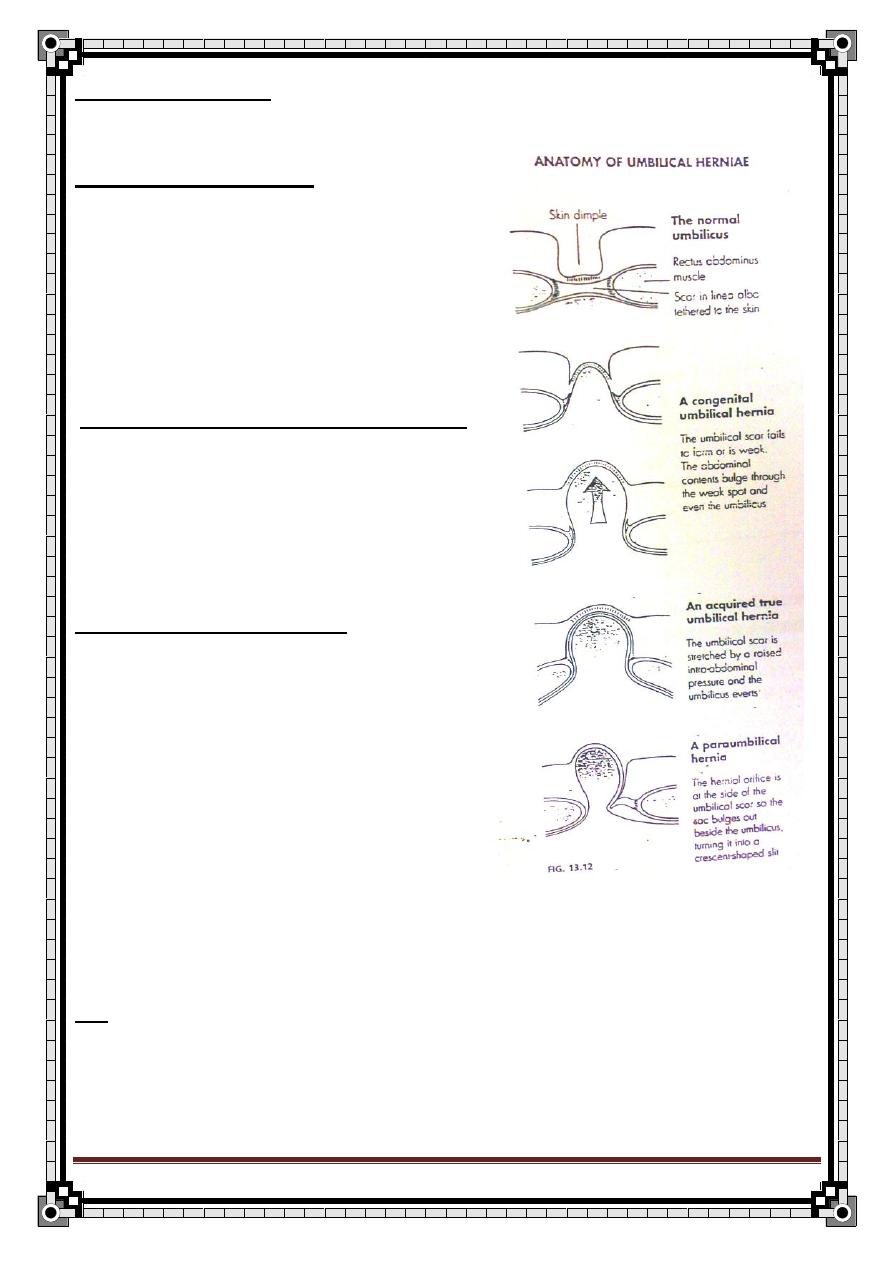
94
" Reading without contemplation is like eating without digestion "
Chinese byword
Umbilical Hernia
Congenital umbilical H.:
- appears at this site if the process by which
scar tissue closes the gap, once the umbilical
vessels have atrophied after birth, fails.
How to take Hx from a pt w/ C.U.H.?
- age: after the separation of the cord
- sym.: rare. ints.obs. is extremely rare
- natural Hx: disappear spontaneously during
the 1
st
few years of life.
How to Ex a pt w/ C.U.H?
1- site: centrally in the umbilicus.
2- shape: hemispherical.
3- size: v.small v.large.
4- cough impulse: variable.
5- composition: soft, compressible & easy to
Reduce. Usually contain bowel resonant on
Percussion.
ttt.:
- surgery is not recommended before the age of
5 b/c 90% of it will disappear spontaneously
During the 1
st
5 ears of life.
95
" Reading without contemplation is like eating without digestion "
Chinese byword
-if persist beyond 5 years H. repair is done.
Umbilical H. in adults (acquired U.H.):
- it comes through the umbilical scar & has the
Umbilical skin tethered to it.
-
2ry to ↑ in the intra-abd. pressure. Commonly d.t pregnancy & ascitis.
Para-umbilical H.:
- appears through a defect that is adjacent to the umbilical scar (in the linea
alba) just above or beside the umbilicus.
-It is clinically apparent b/cit does NOT bulge into the center of the umbilicus
the umbilical skin is NOT atteched to the center
Of the sac.
How to take Hx from a pt w/ P.U.H.?
- Age: middle & old age.
- Gen
der: more common in ♀ than ♂ especially parous & obese ♀
- Sym.: swelling + pain (discomfort or tenderness around the umbilicus) which
are made worse by standing & heavy exercise
- Strangulation is common in U.H.
How to Ex a pt w/ P.U.H?
1-Site: beside the umbilicus.
2-Shape: crescent-shaped (pushed to one side)
3-size: variable
4-Surface & edge: smooth & the edge is easy to defined.
5-Composition: usually firm omentum
If contain bowel soft & resonant.
96
" Reading without contemplation is like eating without digestion "
Chinese byword
6-cough impulse: +ve
7-reducibility: most are reducible.
ttt:
Mayo’s operation
the sac is excised & the edges of the rectus sheath are
overlapped above & below the H.
Epigastric Hernia
Def.: A protrusion of extra-peritoneal fat, and sometimes a small peritoneal sac
through a defect in the linea alba somewhere btw the xiphisternum & the
umbilicus.
C.C: epigastric pain (mistaken w/ ulcer that can be diff. by Hx. & superficial
palpation).
Ex. firm
-ve cough impulse
Irreducible
DDx.: - peptic ulcer.
- lipoma.
ttt.: if there are sym. op. transverse incision exposing the linea alba
excision of the extra-peritoneal fat repair of the defect in the linea alba.
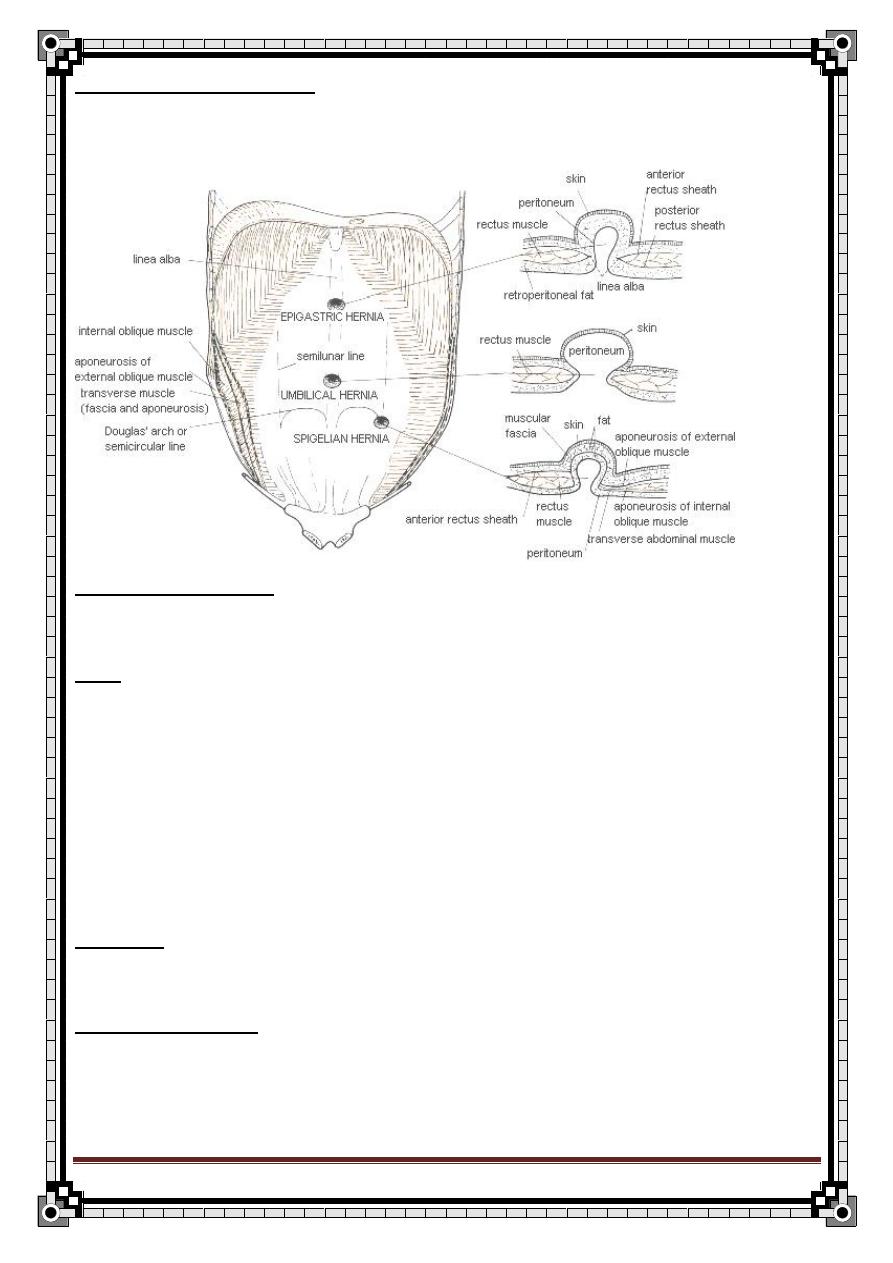
97
" Reading without contemplation is like eating without digestion "
Chinese byword
Epigastric H. in children:
- common in children ass. w/ divarication of the rectus abdominis m.
Incisional Hernia
Def.: a H. through an acquired scar in the abd. wall, caused by a previous
surgical op. or injury.
N.B: scar tissue is inelastic & stretches progressively if subjected to pressure
- commonly occur w/ the lower midline incision.
Kocher’s incision.
Etiology:
a) causes in the pt.:
1- age: healing is slower & weaker in elderly.
2- Obesity: predispose to seroma, hamatoma & infections.
98
" Reading without contemplation is like eating without digestion "
Chinese byword
3- Gen. debilitating dis.: diabetes, uremia, hypoproteinemia
b) op. causes:
1- Inadequate closure: e.g. using absorbable suture.
2- Bad op. technique: e.g. rough handling, inadequate heamostasis.
3- injury to n. supply.
c) post op. causes:
1- post op. ileus (distension), cough.
2- post op infection
3- early resuming of heavy works.
Prevention of incisional H.:
a) pre- op:
1- treat the pul. Dis. Before surgery
2- wt reduction
3- correct anaemia or any nutritional or vit. Deficiency.
4 in case of
huge H., try to ↑ the intra-abd. Volume by gradual injection of air in
the peritoneal cavity.
b) op.:
1- use non-absorbable suture to close aponeurotic layers.
2- gentle handling of tissue, proper haemostasis.
3- avoid tention in wound closure.
99
" Reading without contemplation is like eating without digestion "
Chinese byword
c) post- op:
1-early graded ambulation
2- avoid heavy works for several months after surgery.
Hx.: - age: all ages
- sym.: lump + pain , sym of ints.obs. may occur.
- ask about past surgical Hx.
- ask if there was any complication after the op. (infections, hematoma)
- factors causing weakness of the abd. m. chr.cough, obesity, steroid
Therapy.
Ex.: - reducible lump
- +ve cough impulse
- local tissue state thin & weak m.
ttt.: -H. repair by dissecting out & suturing the affected layers of the abd. wall.
- if large H. synthetic palstic mesh is used.
Rare abd. Herniae
-
spigelian H.:
occur at the lat. border of the rectus sheath (area of linea
semilunaris) below the umbilicus & above the inguinal area.
- Opturator H.:
come through the opturator foramen, and the small sac is
concealed among the area. The sac may compress the opturator n. & cause
pain in the medial side of the thigh
- Lumbar & gluteal H.:
are extreamly rare. Ass w/ previous surgery near to
the defect such as a loin incision or an excision of the rectum.
-
Interstitial H.:
a variety of the ing.H. in which the sac spreads btw the m.
that forms the ing. Canal, above the groin, and emerges through a defect in
the in. ob. & transverse m. rather than the ex. Ing. Ring.
100
" Reading without contemplation is like eating without digestion "
Chinese byword
Gall bladder and bile ducts
Anatomy:
Biliary tree consist of fine interhepatic biliary radiator, which drain liver
segments forming right and left hepatic ducts.
Right and left hepatic ducts join to form common hepatic duct.
This join with cystic duct and end at papilla of vater ( in the second part of
duodenum ). It is joined by pancreatic duct just before entering the duodenum.
The gall bladder supplied by the cystic artery, a branch of the right hepatic
artery.
Common bile duct has 4 parts:
1- supradudenal
2- reterodudenal
3- pancreatic part
4- intradudenal
Bile composition and function:
Bile is combination of cholesterol, phospholipids (lecithin), bile salt (
chenodeoxycholic acid and cholic acid) and water.
Bile also contains conjugated bilirubin, the breakdown product of hemoglobin.
Cholesterol is not water soluble and is carried in the bile in water soluble
micelles.
Bile acid synthesized by the liver from cholesterol ( primary bile acid).
101
" Reading without contemplation is like eating without digestion "
Chinese byword
Primary bile acids ( cholic and chenodeoxycholic acid ) conjugated with glycin to
increase there solubility in water.
In small intestine the bacterial action produce secondary bile acid ( deoxycholic
and lethocholic acid).
Bile salt act as a detergent, breaking up and emulsifying fats to facilitates theirs
absorption.
The bile salt themselves are resorbed in the distal ileum, 95% of the bile are
reabsorbed, transported back to the liver and passed once again in to the
biliary system ( enterohepatic circulation).
The gall bladder contract in response to cholecystokinin (CCK) which is
released by duodenal mucosa by presence of food
(especially fatty acids).
***Disease or resection of terminal ileum is associated with high incidence of
cholesterol gall stone.
Gall stones:
The most common case.
There are 3 common varieties of stone;
1- cholesterol stone (20%).
2- pigmented stone (5%).
3- mixed (75%).
1- cholesterol stone;
This occur as
Solitary, oval, yellowish green, regular shape and rough stone.
102
" Reading without contemplation is like eating without digestion "
Chinese byword
These may be associated with elevated blood cholesterol.
Causes of cholesterol gall stone:
1- 5f (fat, female, fair, forty and fertile).
2- oral contraceptive use but not pregnancy.
3- family history, obesity and low dietary fibers.
4- removal of terminal ileum or
crohn’s disease >>> interruption of
enterohepatic circulation >>>>>> bile become supersaturated with cholesterol
due to deficiency of the bile salts >>>> cholesterol gall stone.
N.B. When cholesterol precipitate on the gallbladder wall ( choleterosis), it
forms yellow sub mucous aggregations with an appearance similar to a
strawberry skin ( strawberry gall bladder).
2- pigment stones:
Pigment stones are composed of calcium bilirubinate, with some calcium
carbonate. On X- ray it appeare as radiolucent.
They occur in hemolytic anemia, eg spherocytosis and sickle cell disease,
where excess of circulating bile pigment is deposited in the biliary tract.
N.B. If such stone are found in the gallbladder of children or adolescents,
haemolytic anaemia should be suspected.
3-Mixed stone;
The majority have the same metabolic origin as cholesterol stone.
103
" Reading without contemplation is like eating without digestion "
Chinese byword
Pathological effects of gall stone:
1- silent : gall stone lying free in the lumen of the gall bladder.
- it produce no pathological disturbance of the wall (asymptomatic) ( majority of
cases ).
- no need for surgery except in:
DM, sickle cell disease and pilot.
2- impaction in gallbladder:
Gall stone impact either in Hartmann's pouch or in the cystic duct>>>>> water is
absorbed from the contained bile.
>>>> concentrate bile in the gallbladder.
>>>> chemical irritation
>>>> inflammation and secondary infection
>>>> cholecystitis.
Or, if stone impact in hartmman pouch when the gallbladder is empty, the
gallbladder may continue to secrete mucous and the gallbladder distended to
form a mucocele.
3- choledocholithiasis;
- gall stone migrate into the common bile duct.
- these may be silent, or produce an intermittent or complete obstruction of the
common bile duct with pain and jaundice
( ascending cholengitis)
4- gall stone ileus;
104
" Reading without contemplation is like eating without digestion "
Chinese byword
This occurs when there is ulceration through the wall of the gallbladder into the
duodenum.
The large gallstone may pass per rectum or produce gallstone ileus >>> result
in intestinal obstruction.
N.B. a key feature in such case is the presence of air in the biliary tree that can
be readily seen on a plain abdominal radiograph.
5- acute and chronic pancreatitis
6- carcinoma of the gall bladder.
So, what are the complication of the gallstone? ( important question)
1-5 >>> the effect of gall stone is on the gallbladder
1- cholecystitis
2- mucocele
3- empyema
4- abscess
5- peritonitis >>> septic shock
6- cholangitis and obstructive jaundice >>> the effect is on the biliary tree.
7- pancreatitis.
8- liver abscess and secondary biliary cirrhosis.
6-7 are the common complications.
N.B. if the patient is diabetic>>> decrease the sensitivity to the pain >>>> more
prone to get complication.
105
" Reading without contemplation is like eating without digestion "
Chinese byword
Clinical features:
1- biliary colic
2- acute cholecystitis
3- chronic cholecystitis
4- obstruction or infection of the common bile duct ( the most common).
1- BILIARY COLIC:
This is produced by impaction of the stone in hartmann pouch or cystic duct for
a short periods, following which the calculus either fall back or is passed along
the duct.
Contraction of the smooth muscle in the wall of the gallbladder and the cystic
duct produce severe pain
** Characters of pain:
Site; at right subcostal region but may be epigastric.
Onset: suddenly
Character; it is background of constant pain with exacerbation between the
attack ( due to contraction of GB ). It is not true colic.
Radiation: radiate to the tip of the shoulder
Reliving factors : analgesic.
Associated symptoms: vomiting, sweating.
Deferential diagnosis is from the other acute colic;
- uretric colic due to stone .
- bladder colic in acute retention due to enlarged prostate
-mechanical obstruction
- apendicular colic
106
" Reading without contemplation is like eating without digestion "
Chinese byword
- menstruation
- parturition
- ectopic pregnancy
2-Acute cholecystitis
-if the stone remain impacted in gallbladder outlet >>>> the gallbladder wall
become inflamed due to inflammation irritation from concentrated bile and from
secondary infection >>> empyma>>>gangrenouce >>>> perforation
>>>>peritonitis .
,The common organisms responsible secondary infection are E.coli
klebsiella aerogenes and strept.faecalis
criteria for diagnosis of acute cholecystitis:
a- symptoms
b- signs
c- investigation
A-symptoms:
1-pain: persist pain in right hypochondrium that is not relived by analgesic. it
radiate to the back or to the angel of scapula. The pain is aggravated by
movement and breathing.
2-The pain associated with nausea , vomiting and fever.(38-39C)
The appetite is completely lost, bowel habit is unchanged.
3- flatulent dyspepsia ( feeling of fullness after food associated with blenching
and heart burn).
107
" Reading without contemplation is like eating without digestion "
Chinese byword
Deferential diagnosis of pain in the right hypochondrium;
Cholycystitis
Hepatitis
Liver abscess
Ascending bacterial cholangitis
HCC
Peptic ulcer
Pancreatitis
Pyelonephritis
Reterocecal appendicitis
B-Signs;
General; pyrexia and tachycardia
Local;
1- tenderness over the right hypochondrium
2- gurding and rigidity;
Indicate involvement of the inflammatory process of peritoneum.
If rigidity present >>> generalize peritonitis.
3- positive murphys sign:
Pain on taking a deep breath while a hand is placed below the right costal
margin ( medial to midclavicular line at the tip of 9
th
rib) and pressed onto the
gallbladder.
4- if empyma develop:
Palpable mass beneath the right costal margin, move with respiration.
108
" Reading without contemplation is like eating without digestion "
Chinese byword
N.B. acute cholecystitis can be acalculous due to typhoid fever or gas
gangrene infection.
Abdominal examination of patient with acute cholecystitis:
- inspection:
Diminished movement of the abdomen with respiration.
- palpation:
1- tenderness and gurding in right hypochondriumn.
2- Murphy sign
3- boas sign: area of skin below the scapula which is hyperesthesia.
- percussion:
- auscultation; no bowel sound mean general peritonitis
PR: normal.
c- investigation:
1-CBC: leukocytosis ( shift to the left >>> neutrophillia).
Acute cholecystitis may associated with moderate leukocytosis and raised
inflammatory marker e.g. C reactive protein.
2-A plain abdominal X-ray may provide evidence of gall bladder disease in
form of radio-opaque stone( in only 10% of cases).
Occasionlly, the gallbladder may be seen to be calcified ( porcelain gallbladder).
3-Ultrasound
It is single most useful investigation for the diagnosis of gall stone disease.
Cholesterol
109
" Reading without contemplation is like eating without digestion "
Chinese byword
This is non invasive technique gives 3 pieces of information;
a- the presence of stones as clear acoustic shadow.
b- the thickened and edematous wall of the gall bladder
c- the dilated diameter of the common bile which, if over 7mm, is suggestive of
the presence of stones within.
N.B stone produce acoustic shadow.
Other investigations:
4-Oral cholecystogaraphy
Iodine- containing prepration is given by mouth and is excreted by the liver into
the bile and then concentrated in the gall bladder.
( a disease gall bladder, being unable to concentrate the dye, will give no
shadow on X- ray.)
5-IV cholangiography
6- upper GI endoscopy is available in cases to exclude an associated peptic
ulcer or hiatus hernia.
7- magnentic resonance cholangiopancreatography (MRCP) Permit
visualization of the billary tree, and contained calculi can be detected. This is
non invasive procedure produce the same diagnostic information as can be
obtained with ERCP but without important risk of complication ( perforation,
bleeding, pancreatitis) associated with ERCP.
8-Endoscopic reterograde cholangiography (ERCP)
Endocopic intubations of the bile ducts through the ampulla of vater is more
invasive than ERCP, but in addition to visualizing the duct and contained stone
110
" Reading without contemplation is like eating without digestion "
Chinese byword
it also permit their extraction. So, it is diagnostic and therapeutic but, it has
complication ( perforation, bleeding, pancreatitis)
9-Precutaneous transhepatic cholangiography
Investigation to exclude deferential diagnosis:
1- CBC: Hb level to exclude peptic ulcer
2- pancreatic tests:
Serum amylase and lipase to exclude pancreatitis.
3- renal function tests:
Blood urea and creatinin. Urin analysis to exclude renal disease.
Treatment of acute cholecystitis:
1- 90% resolved by bed rest, NPO, analgesic and antibiotic (2
nd
or 3
rd
generation cephalosporin).
2- then, elective cholecystectomy after 6 weeks.
3-If the patient comes in golden period (24-48hr), emergency surgery.
4-If the diagnosis is uncertain >>>> laprotomy.
5-If empyma develop >>> emergency cholecystectomy.
Chronic cholecystitis:
This is almost invariably associated with the presence of gallstones.
Repeated episodes of inflammation result in chronic fibrosis and thickening of
the entire gallbladder wall.
History of chronic cholecystitis:

111
" Reading without contemplation is like eating without digestion "
Chinese byword
Age: from 30-60
Sex: more in female.
There are recurrent bouts of abdominal pain at right hypochondrium
Discomfort is experienced after fatty meals since they stimulate release of
CCK which cause the gallbladder to contract on the stone; there is often
flatulence. The pain relived by analgesic. It is associated with N AND V.
Deferential diagnosis:
duodenal ulcer
-
chronic pacreatitis
-
- other colicky pain (renal colic )
- GI neoplasia
- MI
- hiatus hernia
EXAMINATION OF CHRONIC CHOLECYSTITS:
Almost 5f : female, fats, fertile, fair and fourty.
Abdominal examination:
Inspection:
Usually looks normal
Palpaption:
Tenderness in the right hypochondrium.
Percussion, auscultation and PR are normal
112
" Reading without contemplation is like eating without digestion "
Chinese byword
Stone in the common bile duct (
choledocholithiasis ):
This may be symptomless. More often, there are attacks of biliary colic
accompanied by obstructive jaundice with clay- cooured stool and dark urine.
If the obstruction is not relived either spontaneously or by operation, the
chronic back- pressure in the biliary system might result in secondary biliary
cirrhosis and liver failure.
Ascending cholangitis
If infection of the common bile duct supervenes, this result in
Charcot triad:
Biliary colic, obstructive jaundice and fever ( chills and rigors).
Deferential diagnosis of stone in CBD without jaundice
;
Renal colic, intestinal obstruction or MI
Deferential diagnosis of stone in CBD with jaundice;
Carcinoma of the pancreas, acute hepatitis and other causes of jaundice.
Courvoisier low;
If in the presence of jaundice the gallbladder is palpable, then the jaundice is
unlikely to be due to stone. ( because obstructive jaundice is associated with a
small, contracted and fibrotic gallbladder).
Complication of obstructive jaundice:
1- ascending cholangitis
2- malabsorbtion, espically fat soloube vitamin ( vit. K).
113
" Reading without contemplation is like eating without digestion "
Chinese byword
3- coagulopathy and hypovolemia
4- pruritis.
5- stricture
6- hepatorenal syndrome >> due to accumulation of bile salt in renal tube and
bacterial overgrowth.
Treatment":
Impacted stones are removed using a balloon at ERCP. Subsequent
cholecystectomy is performed as soon as possible.
Important preparation is IV vitamin K.
What are the complication of cholecystectomy?
1- leakage of bile which may result from
a- injury to bile canaliculi, or
b- injury to common hepatic duct or common bile duct.
c- slipping of the ligature or clip from the cystic duct.
2- jaundice, this may be due to the following:
a- missed stone in the common bile duct.
b- inadvertent injury to the common bile duct.
c- cholangitis or associated pancreatitis.
114
" Reading without contemplation is like eating without digestion "
Chinese byword
Important question:
What is the different between acute and chronic cholecystitis?
chronic cholecystitis
Acute cholecystitis
-
+
guarding
-
+
rigidity
+
+
tenderness
-
+
murphy
-
+
leukocytosis
What is the different between biliary colic and acute cholecystitis?
Acute cholecystitis
Biliary colic
+ Murphy sign
-ve Murphy sign
Fever 38-39C
No fever
+ leukocytosis
-ve leukocytosis
The stone may or may not
present.
On US >> there is stone
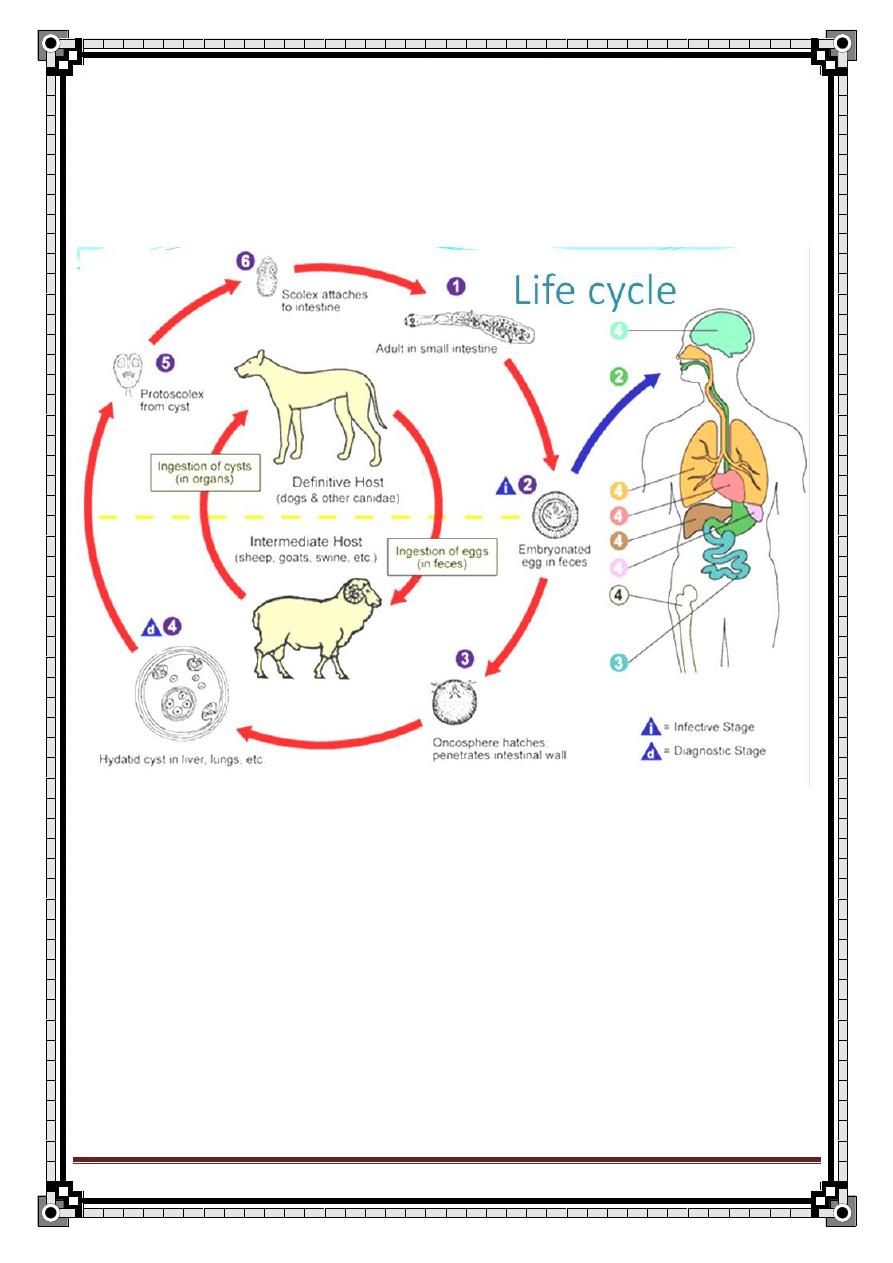
115
" Reading without contemplation is like eating without digestion "
Chinese byword
Hydatid liver Disease
The causative agent is Echinococcus granulosus.
It's widespread in sheep-rearing area of the world.
Life cycle
Organs involvement
Liver (52-77%)
Lungs (8.5-44%)
Abdominal cavity (8%)
Kidneys (7%)
CNS (0.2-2.4%)
Bone (1-2.5%)
116
" Reading without contemplation is like eating without digestion "
Chinese byword
Clinical features
Asymptomatic:
Incidental finding in postmortem examination.
Radiologic examination for other purposes e.g. ultrasound scan.
Local effects of enlarging cyst, according to the cyst site:
Local swelling
Symptoms of raised intra-cranial pressure with focal neurological
signs in brain disease.
Pathological fracture of long bones.
Collapsed vertebrae.
Complicated cyst
Acute anaphylaxis due to cyst rupture.
Liver or lung abscess due to secondary bacterial infection.
Children with hydatid cyst of the liver usually complain of right upper
abdominal pain and abdominal mass.
Pulmonary hydatid usually presented with:
Fever
Cough & expectoration.
Dyspnoea
Renal hydatid cysts:
Isolated renal cyst is rare condition, as it is usually a part of
multiple hydatid disease.
Commonly causes lumber pain.
Very rarely presents with hydatiduria.
Diagnosis
Pulmonary hydatid:
Plain radiograph
CT scan confirmation
117
" Reading without contemplation is like eating without digestion "
Chinese byword
Brain hydatid:
CT scan
MRI
Liver hydatid:
Ultrasound scan
MRI
ERCP (Endoscopic Retrograde Cholangio Pancreaticography):
Shows any cysto-billiary relationship
Permits evacuation in cases of intra-billiary rupture of the cyst.
Serology: ELISA, CFT,……etc.
Treatment
Medical treatment
— The drug regimen used is as follow:
3 months Albendazol (40-50mg/kg/day) along with
Praziquantel (40mg/kg/day in 2 divided doses) for the first 2 weeks.
— Then reassessment to decide one of two:
1. Proceed with surgery
2. Continue with chemotherapy for one year course.
— Post-operatively, 2 weeks of Praziquantel plus Albendazol should be
given to deal with material possibly spilled at operation.
118
" Reading without contemplation is like eating without digestion "
Chinese byword
Surgical treatment
Many surgical procedure for the treatment of hepatic hydatid cyst, including:
1. CT or ultrasound- guided PAIR (Puncture Aspiration Injection Re-
aspiration).
2. Laparoscopic cystotomy, deroofing and omentoplasty.
3. Partial resection.
4. Marsupialisation and tube drainage or omentoplasty.
5. Radical surgical resection (total cysto-pericystectomy).
6. Partial hepatectomy
Scolicidal agents used in hydatid surgery:
20% hypertonic saline
— 0.5% silver nitrate (PAIR)
— 95% sterile ethanol (PAIR)
— Absolute alcohol
— Albendazol
Formaldehyde is not used
Complications of surgical resection of liver hydatid
1. Billiary leak
2. Billiary fistula
3. Infection of the residual cavity
4. Cholangitis
5. Heamorrhage
6. Missing of deep seated cyst
7. Damage to the liver
8. Damage surrounded tissue

119
" Reading without contemplation is like eating without digestion "
Chinese byword
HISTORY AND
EXAMINATION OF
LUMPS AND ULCERS
HISTORY OF LUMPS:
1- Duration
2- First symptom
3- Associated symptoms
a-pain
b-disfiguring
c-interfering with movement, respiration, or swallowing.
4- Progression
when did they notice the change
bigger or smaller
fluctuated in size
more tender
5- Persistence
on lying down
during exercise
irreducible
6- Other lumps
7- Caused the lump?
EXAMINATION:
Inspection:-
6S
1- Site: exact position
120
" Reading without contemplation is like eating without digestion "
Chinese byword
2- size height by width by depth
3- shape three dimensions (eg: spherical, hemispherical , pear ,
kidney shaped )
4- surface smooth or irregular
5- state of the overlying skin: 1-color 2-Dilated veins
6- scar
On inspection
There is lump in the anteromedial part of the lower third of the
leg about 2 cm superolateral side of medial malleolus 2 by 3 by 1
cm in dimension spherical in shape with smooth surface the color
of overlying skin is red no dilated veins no visible scar or
pulsation.
On palpation
it's not tender of normal temperature the edge is indistinct firm in
consistency of cystic composition
Palpation
1-Temperature assessed by the dorsum of the fingers.
2-Tenderness
3-Edges either clearly defined or indistinct.
4-Composition
a- calcified tissues such as bonehard
b- tightly packed cellssolid
c- extra vascular fluid such as urine, serum, CSF, synovial fluid, blood
cystic
d- gas
e- intravascular blood
121
" Reading without contemplation is like eating without digestion "
Chinese byword
5-consistency can vary from very soft to very hard
1. very soft like jelly
2. soft
like relaxed muscle
3. firm
like contracted muscle
4. Hard
like contracted biceps of boxer
5. stony hard
like bone or calcification
others
rubbery
slightly squashable like a rubber ball
spongy soft and very squashable but with some resilience
the consistence of a lump depends not only on the structure but also on the tension
within it.
1-fluctuation
pressure on one side of a fluid filled cavity makes the other
surfaces protrude.
-It can only be elicited by feeling at least two other areas of the lump while pressing on
a third.
-This exam is best done in two directions, the second at right angle to the first.
2-fluid thrill
a percussion wave is easily conducted across a large fluid collection
–cyst- but not across a solid mass.
3-transillumination
light will pass easily through clear fluid but not through
solid tissues.
-fluids that transilluminate are water, serum, lymph or plasma or highly refractile fat.
-transillumination requires a bright pinpoint light source and a dark room.
5-pulsatility
lumps may pulsate because they are near to an artery and are moved
by its pulsations.
122
" Reading without contemplation is like eating without digestion "
Chinese byword
-expansile pulsations if the two fingers are pushed outwards and upwards. Eg:
aneurysm and very vascular tumors.
-transmitted pulsations if the two fingers move in the same direction.
6-compressibility
it is a feature of very vascular malformations and fluid
collections. A lump that is reducible such as a hernia can be pushed away into another
place but will often reappear spontaneously without the stimulus of coughing or gravity.
7-bruits
vascular lumps with AV fistulas can have a systolic bruit.
8-resonace
solid and fluid filled lumps sound dull when percussed. A gas filled
lump sound hollow and resonant.
8-reducibility
lumps can be reduced by gentle compression. If the lump
reappears as the patient coughs, this is called
9-cough impulse
and is a feature of hernia.
10-relations to the surrounding structures
-lumps attached to bone move very little.
- lumps attached to vessels or nerves move sideways not up and down
-lumps in the abdomen arising from mesentry or omentum moves freely
11-Slipping: for subcutaneous lipoma
12- Indentation for sebaceous cyst
123
" Reading without contemplation is like eating without digestion "
Chinese byword
For every lump
12-state of the regional lymph glands
13-state of the local tissue
skin, SC, bone, muscle, local circulation and
nerve supply
14-general examination
always examine the whole patient.
Hints to remember the examination method
:
1-
5S:
Site
Size
Shape
Surface
state of surrounding tissue and LN.
2-
4C:
composition-and all the points under it
described above
consistency
color
cough impulse
3-
2R:
Reducibility
relation to surroundings
4-
2T:
Temperature
Tenderness.
124
" Reading without contemplation is like eating without digestion "
Chinese byword
DDX of lumps:
1-skin:
sebaceous cyst (obvious punctum +indentation +ve), dermoid cyst (Indentation),
furuncle, carbuncle, hidr adenitis suppurtina. Wart, naevi secondary carcinomatous
nodule, malignant melanoma
2-under the skin:
LN
Lipoma above the facia slipping +ve with lobulation or under the facia or muscles
If multiple and tender = dercum's dz or adiposis dorsalis
liposarcoma , fibroma
3-Nerves:
neuroma,neuro fibromatosis
4-BV:
angioma, aneurysm, AVM
5-soft tissue:
fibrosarcoma
6-muscle:
myosarcoma: 1-leiomyosarcoma 2-rhabdomyosarcoma
7-bones:
osteosarcoma, chondrosarcoma
8-swelling near the joints:
ganglion, bursae, cystic production of the synovial
cavity of the arthritic joints.
you have to look up all of these structures.
INVESTIGATIONS:
1. US: cystic or solid
2. Biopsy
3. FNA
4. CxR
125
" Reading without contemplation is like eating without digestion "
Chinese byword
HISTORY OF ULCERS:
an ulcer is a solution or a break of the continuity of an epithelium (i.e. an epithelial
deficit, not a wound). Unless it is painless and in an inaccessible part of the body,
patients notice ulcers from the moment they begin and will know a great deal about
their clinical features.
The history taking is the exact same thing done as when taking the history of a lump –
mentioned above-
EXAMINATION OF ULCERS:
it follows the same pattern as above plus the following:
1-shape
(round, oval, irregular, serpiginous)
2-size
3-floor:
usually consists of slough or granulation tissue but also bones or tendons may
be visible. The nature of the floor may give some indication of the cause:
*solid brown or grey dead tissue full thickness skin death
*yellow grey wash leather slough syphilitic ulcers.
*bluish unhealthy granulation tissue tuberculous ulcers
*poor granulation tissue with tendons or other structures that may lie bare in the base
ischemic ulcers.
The redness of the granulation tissue reflects the underlying vascularity and indicates
the ability of the ulcer to heal. Healing epidermis is seen as a pale layer extending in
over the granulation tissue from the edge of the ulcer.
4-base of the ulcer :
what you are palpate either indurated or attached to the deeper
stractures
5-edge:
there are 5 types of edges
*a flat, gently sloping edge shallow, superficial ulcer. Mostly venous ulcers. This
healing ulcer has a pale pink almost transparent edge.
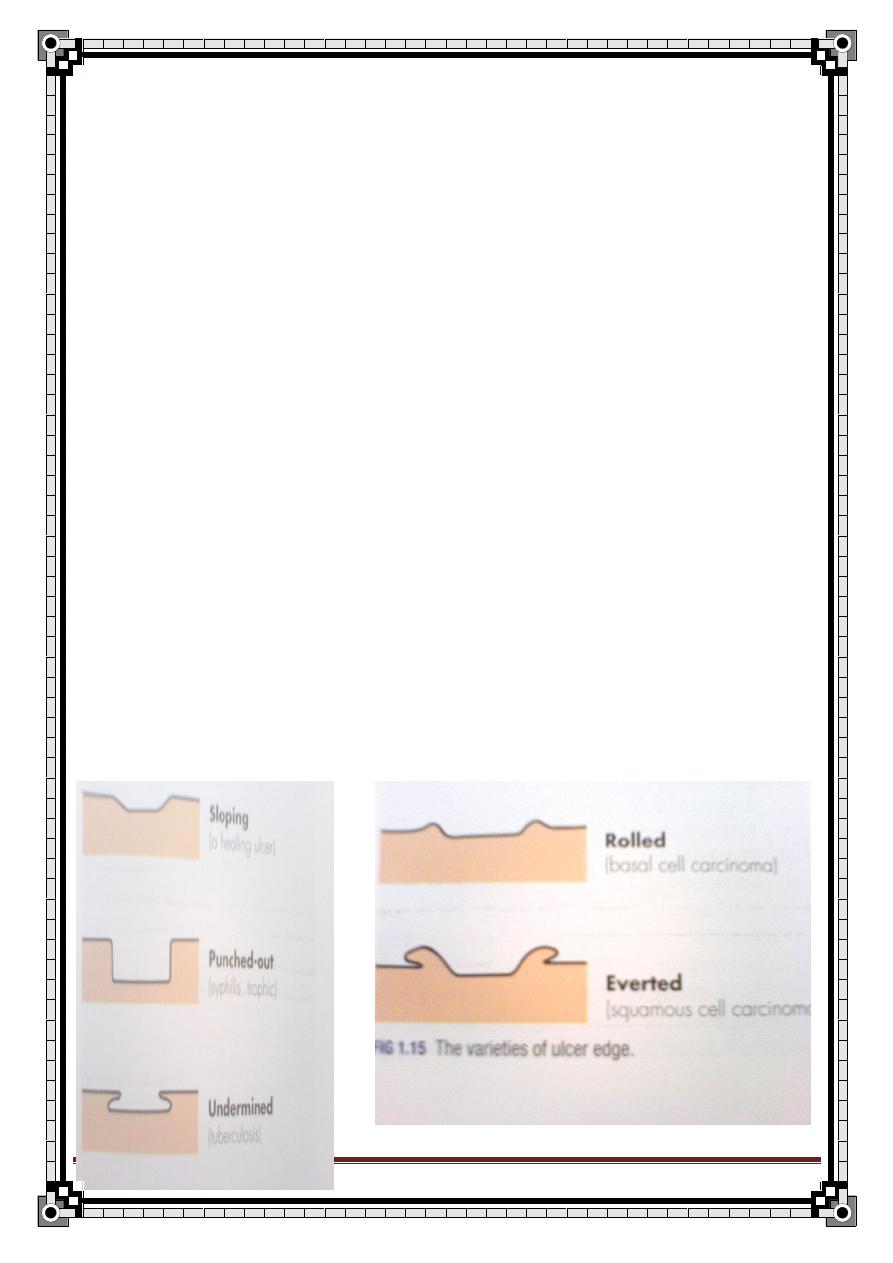
126
" Reading without contemplation is like eating without digestion "
Chinese byword
*a square-cut or punched out edge rapid death and loss of whole thickness of the
skin without attempts to repair. This happens in tertiary syphilis, neuropathic lesions of
DM or ischemia and leprosy. Mostly occur in the legs.
*an undermined edge infection of an ulcer involving the SC tissue more then the
skin. Mostly happens in the buttock area. Happens in tubercoulus ulcers.
*a rolled edge slow growth of the tissue in the edge of the ulcer. Diagnostic of rodent
ulcers – Basal Cell Carcinoma - where telangiectases are seen in the pearly edges.
*an everted edge the tissue in the edge of the ulcer is rapidly growing that it spills
out of the ulcer to overlap the normal skin. This is typical of carcinoma.
6- depth
7-state of surrounding tissues: inflammation, pigmentation, varicosity
8-discharge
Serous
Sanguinous
serosanguinous
purulent.
127
" Reading without contemplation is like eating without digestion "
Chinese byword
CAUES OF LEG ULCERS :
1-venous stasis ulcer most common
Site : around malleoli
Associated pigmentation, stasis, eczema
2-ischemic ulcers:
*large artery disease (atherosclerosis, obliterations) usually lateral side of the leg with
an absent pulse.
*small vessel disease
3-malignant ulcer: BCC, Sq.CC.
4-infections
5-neuropathic : painless penetrating ulcer on the sole of foot
6-underlying systemic disease:
*DM: vascular disease, neuropathy or necrobiosis lipodica (front of leg)
*pyoderma gangrenosum
*rheumatoid arthritis
*lymphoma
*haemolytic anemia (small ulcers over the malleoli) as in SCA
INVESTIGATIONS:
1-fasting B.S. and R.B.S.
2-urin analysis
3-CBC
4-plain X-ray
5- swap for culture.
6-Biobsy for malignancy. It is taken from the edge of the ulcer.
7-arterio and angiogram.
128
" Reading without contemplation is like eating without digestion "
Chinese byword
MANAGEMENT:
1. clean the wound
2. dressing
3. Abx
4.
skin grafting.
COMPLICATIONS OF ULCERS:
1-keloid: hypertrophic persistence scar
2-hypertrophic scar
3-hyper- or hypo – pigmentation
4- chronic benign ulcer sq. cc
129
" Reading without contemplation is like eating without digestion "
Chinese byword
Diabetic foot
Definition:
A spectrum of foot disorders ranging from ulceration to gangrene in diabetic pt
as a result of peripheral neuropathy or ischemia or both.
WHO definition..
It is the foot of the diabetic pt that has the potential risk of pathological
consequences, including infection, ulceration, and /or destruction of deep tissue
associated with neurological abnormalities, various degrees of peripheral
vascular disease, and/or metabolic complication of diabetis in lower limbs.
Classification:
i.
Neuropathic foot.
ii.
Neuroischemic foot.
iii.
Diabetic foot infection.
i. The Neuropathic foot..
Pathogenesis:
Vascular hypothesis:
by occlusion of the vasovasorum.
Metabolic hypothesis:
Hyperglycemia → accumulation of sugar in schwan cells →disruption of their
function& structure and delayed nerve conduction lead to neuropathy.
Types of neuropathy:
1. autonomic neuropathy..
- loss of sweating.
- Callous formation.
-
2. sensory neuropathy..
- extrinsic foot lesion.
- Symmetrical.
- Loss of vibration sense (1
st
to occur).
- Loss of temperature & pain sensation.
- Loss of proprioception &joint position sense.
130
" Reading without contemplation is like eating without digestion "
Chinese byword
3. motor neuropathy
-
intrinsic lesion → subluxation.
→ charcot’s joint.
Clinical manifestation of neuropathic foot:
- warm.
- Numb.
- Dry.
- Painless.
- Palpable pulse.
- Presence of granulation tissue (good sign of healing).
Complication:
1. unrecognized trauma lead to ulceration, infection.
2.
charcot’s joint.
3. neuropathic edema(rarely).
Neuropathic ulcer..
- Site: the planter surfaces of the metatarsal heads and toes.
- Could be infected with staph/ strept. If untreated.
- Causes: 1.peripheral nerve lesions e.g. diabetes, nerve injury, leprosy.
2.spinal cord lesions e.g. spina bifida, tabès dorsalis, syringomyelia.
- Ttt: remove callous, swap, oral AB and special foot wear.
Charcot’s joint..
- precipitating usually by minor traumatic episode.
- Presented as swollen, erythematous, hot, painful(sometimes) joint.
- Most commonly involved: metatarsal- tarsal joint.
- Management: immobilization.
131
" Reading without contemplation is like eating without digestion "
Chinese byword
Neuropathic edema..
- uncommon.
- Sever peripheral neuropathy.
- Swelling of feet and lower leg.
ii. The Neuroischemic foot..
The purely ischemic foot with no concomitant neuropathy is rarely seen in
diabetic pts and its management is the same as for Neuroischemic foot.
Pathogenesis:
Ischemia as a result of angiopathy.
Diabetic angiopathy classified into two types:
1. microangiopathy
affects the small blood vessels throughout the body but it is particularly
dangerous in
*retina → blindness.
*renal glomeruli → end stage renal disease(ESRD).
*nerve sheath → neuropathy.
2. macroangiopathy
affects large BV like
*coronary artery →ischemic heart disease.
*cerebral artery→ stroke.
*peripheral artery → acute / chronic→ intermittent claudication/ trophic
changes.
Atherosclerosis of the vessels of the leg & neuropathy predisposing to
minor trauma.
The atherosclerosis is multi-segmental, bilateral, and distal.
Involves: popliteal, tibial, peroneal arteries.
Smoking, hypertension, and hyperlipidemia commonly contribute.
132
" Reading without contemplation is like eating without digestion "
Chinese byword
Clinical signs &symptoms:
- pain.
– claudication.
- Absent pulses.
– ulceration.
- Thinned or shiny skin.
– thickened nails.
Absence of hair.
– gangrene.
Vascular ulcer..
- The wounds heal poorly.
- Minor trauma cause ulcer present as area of necrosis surrounded by a
rim of erythema, often painful, cold, no callous, at edge of foot or toes.
- Investigation:
Transcutaneous oxygen measurement
The ankle
– brachial index(ABI)..
Not accurate (false +ve), because of calcification of arterial walls in
diabetic foot (arteries are stiff, not squashed by the pressure cuff.
normal ABI=1, if 0.8→ischemia, if 0.5→rest pain, if less than that
gangrene/ ulcer.
Absolute toe systolic pressure..
More accurate.
-
management
:
1.
if ulcer is small, shallow, recent →medical ttt (insulin, anti-coagulant,
opiate).
2. remove necrotic tissue, ulcer swap, clean, dressed.
3. if infected: drainage, specific antibiotic therapy.
4. sever sepsis: emergen
cy admission →Iv AB, surgical debridement,
angioplasty or bypass surgery.
* if the ulcer is acute there will be granulation tissue & bleeding, if ulcer is
chronic there will be slough in the floor, thickening of the edge, and
pigmentation around the ulcer.
* if any lesion however small, in the pulse less foot has not respond to
conservative ttt within 4 weeks then the pt should be considered for
arteriography & revascularization.
133
" Reading without contemplation is like eating without digestion "
Chinese byword
* other causes of ischemic ulcer:
Large artery obliteration:
- atherosclerosis.
- embolism.
Small artery obliteration:
- scleroderma.
– Buerger’s disease.
- embolism.
– diabetes.
- physical agents e.g. pressure necrosis, radiation, trauma, electrical
burns.
Gangrene..
- it is the end point of Neuroischemic foot due to macroangiopathy.
- Mainly the big toe is involved.
- Manifested as black discoloration and deeper tissue necrosis.
-
If only the artery is blocked →
dry gangrene
(dark, dry, hard,
shrunken with clear line of demarcation) → wait for auto- amputation
then reconstruct.
- If both artery and vein are blocked, the blood will remain in the vessels
→
wet gangrene
(soft, swollen, infected, malodorous without clear
line of demarcation) → amputation.
*atherosclerosis cause slow &progressive blockage of the arte
ry → dry
gangrene.
* diabetic gangrene is often associated with gas in the tissue (tissue
crepitus) and foul smell.
- there will be loss of pulse, sensation, temp &function and changes in
color.
- The dead tissue will rotten & invite anaerobic infection (gas gangrene)
→ crepitation on palpation& air bubbles on x-rays.
134
" Reading without contemplation is like eating without digestion "
Chinese byword
Characteristics
Neuropathic foot
Neuroischemic foot
Skin temp.
Warm
Cold
Pain.
Painless
Painful
Skin color.
No change
Dependent rubor(red)
Callous.
Thick at pressure
points
May or may not
present
Ulcer
Planter ulceration at
pressure points
At tips of toes/over
pressure areas
Peripheral pulse
Bounding
Not palpable
Beside ulcer and gangrene diabetic foot can also present as diabetic foot
infection, which ranges from simple superficial cellulites to chronic
osteomyelitis.
Cellulites..
- tender erythematous non-raised skin lesions on the lower extremity
that may or may not be accompanied by lymphangitis.
- No ulcer or wound exudates.
- Caused by group A streptococcus.
Deep skin& soft tissue infection..
- Acutely ill, with painful indurations of the soft tissues in the extremity.
- Common in thigh area, but they may be seen any where on leg or foot.
- Wound discharge usually not present.
- In mixed infection that may involve anaerobes, crepitation may be
noted over the afflicted area.
-
Extreme pain &tenderness→ compartment syndrome, closteridial
species i.e. gas gangrene.
Osteomyelitis..
- Results from contiguous spread of deep tissue infection through
cortex to bone marrow.
- Associated with deep long standing foot infection.
- no lymphangitis.
- pain may or may not present.
135
" Reading without contemplation is like eating without digestion "
Chinese byword
- usually are located between toes or on the planter surface of the
foot.
- diagnostic feature: chronic discharging sinus or sausage like
appearance of toe.
-
early osteomyelitis doesn’t show up on x-ray so, we use CT/ MRI
and bone biopsy to confirm.
- ttt of choice: resection.
Differential diagnosis of diabetic foot:
1. wet gangrene.
2.
arterial (atherosclerosis, burger’s disease, aretritis)
3. venous (DVT, varicose veins(venous ulcer).
4. neuropathy (leprosy, tabes dorsalis, DM).
5. lymphatic obstruction.
6. malignancy (squamouse cell carcinoma).
7. systemic disease (Sickle cell disease, rheumatoid arthritis).
8. mycetoma, leshmania.
History taking of diabetic foot:
Diabetic history.
Ulcer history:
1. Duration.. when was it 1
st
diagnosed?
2. 1
st
symptom.. what brought it to pt notice?
3. other symptoms.. what symptoms does it cause?
4. progression.. how has it changed since it was it 1
st
noticed?
5. persistence.. has it ever disappeared or healed?
6. multiplicity.. has the pt had any other ulcers?
7. causes.. what does the pt think cause it?
Ask about symptoms of the differential diagnosis.
SCA: bone pain Rh.Arthritis stiffness joint pain Rh. nodule
Ask about risk factors e.g. hyperlipidemia, smoking.
136
" Reading without contemplation is like eating without digestion "
Chinese byword
Examination :
General.. systemic.
Local .. before you start ..
1. expose both limbs.
2. compare both limbs.
3. examine lower limbs as a whole then examine the ulcer.
I.
inspection:
a. signs of chronic ischemia(pallor, cold, atrophy):
- atrophy of muscles.
- hair loss.
- atrophic nail.
- shiny skin.
b. Color.. white, pale, blue, black.
c. Swelling.
d. Pressure points.. base of 5
th
metatarsal, lateral side of the foot, head of
1
st
metatarsal, heel, malleoli.*look between toes and tips of toes.
e. Ulcer..
- site, size, shape.
- Edge, depth, floor.
- Discharge, granulation/ necrotic tissues, surrounding tissues.
II.
palpation:
- Tenderness.
- Temperature.
- Base of the ulcer.
- Pulsation of:
1. dorsalis pedis.
2. posterior tibial.
3. popliteal.
4. femoral.
- sensation : touch, vibration and position sense is the 1
st
to be lost in
DM.
- Inguinal LN.
- If the foot is swollen; may be an abscess so, look for fluctuation,
discharge sinuses and widening of space between the toes due to bus
collection.
- If there is a sinus near the ulcer; look for deep infection; infection of
bone or tendons.
137
" Reading without contemplation is like eating without digestion "
Chinese byword
Investigations:
1. CBC.. leukocytosis.
2. Random& fasting blood sugar(RBS/FBS).
3. X-ray of the foot; to rule out:
Osteomyelitis.
Gas gangrene.
Atherosclerosis.
4. Swab for culture& sensitivity.
5. check blood vessels by:
Doppler U/S.
Angiography.
Arteriogram.
* look for site &length of the block and presence of collateral.
Management..
a. prevention
foot care:
-
feet kept clean.
-
Inter-digital space dry.
-
Remove calluses.
-
Toenails trimmed.
-
Frequent inspection.
-
Properly fitting shoes.
-
Check water temperature before bathing.
b. specific management
1. Control diabetes..
Any diabetic pt will be on insulin when he/she develops
infection.
2. Antibiotic..
Ampicilin → Gram +ve.
Gentamycin → Gram –ve.
Metronidazole/ flagyl → Anaerobes.
138
" Reading without contemplation is like eating without digestion "
Chinese byword
3. Local debridment..
Remove necrotic tissue in the foot, because it is infected&
good medium for infection.
*if there is abscess → incision & drainage.
4. Dressing..
Every day or every other day, use dry dressing.
5. In vascular abnormality..
-
small abnormality→ dilate by balloon.
-
large abnormality→ bypass surgery.
* in angiopathy we need both medical &surgical ttt.
* in neuropathy we need to educate the patient &control the
infection.
Indication of amputation:
Uncontrolled infection.
Osteomyelitis.
Extensive tissue destruction.
139
" Reading without contemplation is like eating without digestion "
Chinese byword
How to describe an ischemic ulcer?
-Site:
tips of toes & over pressure areas.
-Size: any size.
-Shape:
elliptical(oval), irregular.
-Edge:
punched out
, but if healing begin→ sloping edge. The skin at the edge is
usually blue-grey color.
-floor:
Contains grey yellow slough covering flat, pale-pink granulation tissue.
-Depth: often deep.
-Discharge:
either clear fluid, serum or pus.
-Temperature:
surrounding tissue usually COLD because they are ischemic (warm, healthy
tissue suggest another cause for ulceration).
-Tenderness:
the ulcer& surrounding tissue are very tender.
-Relation:
the base may be stuck to underlying tissue. Bare bone, ligaments, and tendon
may be exposed.
-Lymph drainage:
the infection usually localized to the ulcer, so LN are not involved.
-Local tissues:
pallor, cold, atrophy, absent pulses.
140
" Reading without contemplation is like eating without digestion "
Chinese byword
Jaundice
Definition:
Yellowish discoloration of skin and mucous membranes due to staining
with bilirubin
Normal bilirubin = 0.3
– 1.3 mg/dl
Conjugated (direct) = 0.1
– 0.3 mg/dl
unconjugated (indirect) = 0.2
– 0.7 mg/dl
jaundice detected clinically at level of > 3 mg/dl
Physiology of bilirubin:
1. Break down of old RBCs in the RET releases HB
2. Released HB is converted to unconjugated bilirubin (UB)
3. UB is transported in plasma bound to albumin to liver
4. UB is transported through liver cells after been taken up by two proteins
5. In liver: UB converted to conjugated (H2o soluble), this is mediated by
bilirubin UDP glucuronyl transferase
6. Conjugated bilirubin passes via biliary tree to duodenum
7. In small bowel:
conjugated bilirubin is deconjugated by bacterial glucuronidase
unconjugated bilirubin is reduced to urobilinogen
8. Most of urobilinogen is excreted in faeces as stercobilinogen. Some is
reabsorbed and partly excreted by liver (enterohepatic circulation)
and rest is excreted by kidneys
141
" Reading without contemplation is like eating without digestion "
Chinese byword
Bile Pigment Metabolism
Defects
85%
15%
Uncojugated Bilirubin
(Water-Insoluble, Lipid-Soluble)
Conjugated Bilirubin
O2 + stercobilin
Liver haem
destruction
RBC
precursor
destruction
Mature
RBC
destructi
on
Minimal
colonic
absorption
(in colon)
bacterial
deconjugation
sterocobilinogen
kidney
Disturbed excretion of bilirubin
a. Intrahepatic cholestasis
b. Extrahepatic cholestasis
or obstructive jaundice
Increased bilirubin load
Haemolytic jaundice
Disturbed uptake and
conjugation of bilirubin
Familial hyperbilirubinaemias
Viral/toxic/infective hepatitis
(in liver)
liver cell microsomes
conjugation
(water-soluble, bilirubin)
urobilinogen
142
" Reading without contemplation is like eating without digestion "
Chinese byword
Causes of jaundice (Hyperbilirubinaemia):
The bilirubin present in serum represents a balance between input from
production of bilirubin and hepatic/biliary removal of bilirubin.
Hyperbilirubinamia Jaundice
Hyperbilirubinaemia result from:
Over production of bilirubin (haemolysis) PREHEPATIC
Impaired uptake, conjugation or excretion of bilirubin HEPATIC
Regurgitation of unconjugated or conjugated bilirubin from damaged
hepatocytes or bile ducts POSTHEPATIC
Causes of unconjugated hyperbilirubinaemia:
Either overproduction (haemolysis)
Or impairment of uptake
Or impairment of conjugation
Causes of conjugated hyperbilirubinaemia:
Either decreased excretion into bile ductules
Or backward leakage of the pigment (bilirubin)
NOTE
-Unconjugated bilirubin is not filtered by kidneys b/c it is bound to albumin, so it
is not found in urine.
-Conjugated bilirubin is filtered, so any bilirubin in urine is conjugated (direct).
143
" Reading without contemplation is like eating without digestion "
Chinese byword
Some Causes of Unconjugated Hyperbilirubinaemia:
Haemolysis
Inherited disorders
impaired conjugation Crigler-Najjar syndrome
Gilbert’s syndrome
Drugs
Impaired uptake Rifampicin
By the liver Probenecid
Ribavirin
Others
Pyruvate kinase def.
Extra vascular
Sickle cell
Thalassemia
Hereditary spherocytosis
eleptocytosis
Intra vascular
G6PD def.
Malaria
Septicemia
DIC
Prosthetic valve
Hb. Uria
(tea color urine)
due to haem
not due to bilirubin
b/c unconjugated
bilirubin is not found in
urine
144
" Reading without contemplation is like eating without digestion "
Chinese byword
Microangiopathic hemolytic anemias
Paroxysmal nocturnal hemoglobinuria(PNH)
Immune hemolysis
Ineffective erythropoiesis due to cobalamine, folate, and iron def.
Some Causes of Conjugated Hyperbilirubinaemia:
Hepatocellular
condition
Cholestatic
conditions
-viral hepatitis
hepatitis A,B,C,D
EBV
CMV
Herpes simplex
-Drugs
isoniazed
-alcohol
-autoimmune hepatitis
-others
INTRAHEPATIC
-viral hepatitis
hepatitis A,B,C
EBV
CMV
-Drugs
contraceptive pills
-alcohol
-1ry biliary cirrhosis
EXTRAHEPATIC
-Malignant
cholangio ca.
pancreatic ca.
gall bladder ca.
ampullary ca.
-Benign
CBD stone
(choledocholithiasis)
chronic pancreatitis
145
" Reading without contemplation is like eating without digestion "
Chinese byword
Hepatocellular conditions that may produce jaundice:
-viral hepatitis
hepatitis A,B,C,D and E
EBV
CMV
Herpes simplex
-Drug toxicity
Predictable, dose-dependent, e.g., acetaminophen
Unpredictable, idosyncratic, e.g., isoniazid
-alcohol
-Environmental toxins
vinyl chloride
Jamaica bush tea
– pyrrolizidine alkaloids
Wild mushrooms
– amanita phalloides or verna
-
Wilson’s disease
-autoimmune hepatitis
146
" Reading without contemplation is like eating without digestion "
Chinese byword
Cholestatic conditions that may produce jaundice:
1- INTRAHEPATIC
-viral hepatitis
fibrosing cholestatic h2epatitis B and C
hepatitis
EBV
CMV
-Drug toxicity
pure cholestasis
– anabolic and contraceptive steroids
cholestatic hepatitis
– chlorpromazine, erythromycin estolate
chronic cholestasis
– chlorpromazine and prochlorperazine
-alcoholic hepatitis
-1ry biliary cirrhosis (AMA in 90%)
-1ry sclerosing cholangitis
-vanishing bile duct syndrome
chronic rejection of liver transplants
sarcoidosis
drugs
-inherited
benign recurrent cholestasis
-cholestasis of pregnancy
-total parenteral nutrition
-nonhepatobiliary sepsis
-benign postoperative cholestasis
-paraneoplastic syndrome
147
" Reading without contemplation is like eating without digestion "
Chinese byword
-venoocclusive disease
-graft-versus-host disease
2- EXTRAHEPATIC
A- Malignant
cholangio ca.
pancreatic ca.
gall bladder ca.
ampullary ca.
malignant involvement of the porta hepatis lymph nodes
B- Benign
CBD stone (choledocholithiasis) [the most common]
1ry sclerosing cholangitis
chronic pancreatitis
AIDS cholangiopathy
Hydatid cyst
Primary sclerosing cholangitis:
Destruction and fibrosis of large bile ducts.
Dx. is made by ERCP => multiple strictures of bile ducts.
75% have IBD.
You can differentiate b/w hepatocellular causes and cholestatic causes by liver
enzymes ALT, AST, ALP
148
" Reading without contemplation is like eating without digestion "
Chinese byword
HOW??
The first steps in evaluating a pt. with jaundice are to determine:
1- what is predominant:
conjugated bilirubin OR unconjugated??
2- whether other liver biochemical tests are normal (isolated elevation of
bilirubin) OR increased??
The other liver biochemical tests are:
- ALT or GPT => alanine aminotransferase
- AST or GOT => aspartate aminotransferase
- ALP => alkaline phosphatase
In pt. with conjugated bilirubin due to hepatocellular conditions ALT/AST will be
elevated out of proportion to ALP.
While in cholestatic conditions ALP will be elevated out of proportion to
ALT/AST.
Blood
Urine
Stool
Radiological
1- BLOOD
a) serum bilirubin:
conjugated or unconjugated
Investigations
ALT/AST in cytoplasm of
hepatocytes
ALK in cells of biliary
tree
149
" Reading without contemplation is like eating without digestion "
Chinese byword
b) liver enzymes:
o ALT
o AST
o ALP
-normal in hemolytic jaundice
- in hepatocellular causes of jaundice but mainly for ALT/AST
and ALT is more specific for hepatitis
while AST is more specific for alcoholics
-
in cholestatic causes of jaundice but mainly alkaline phosphatase (ALP)
c) CBC:
-
Hb
in hemolytic jaundice
-
Reticulocytes
-
Leucopenia
viral hepatitis esp. HBV aplastic anemia
-
Lymphocytes
-
thrombocytopenia hyperspleenism
(as a complication of portal HTN)
alcohol BM suppression
d) coagulation profiles:
PT (factor I, II, V, VII, IX)
-
normal in hemolytic jaundice
-
prolonged in cholestatic (obstructive) jaundice, due to vit. K malabsorption,
corrected by I.V. vit.K, factor II, XII, IX
-
prolonged in hepatocellular jaundice, due to hepatocellular injury, not
correctable
e) serum antigens (hepatitis profile):
-
HBs Ag, HBe Ag ,…..
-Ig M, Ig G
(read about hepatitis)
150
" Reading without contemplation is like eating without digestion "
Chinese byword
f) LDH (lactate dehydrogenase):
-
found in muscles and RBCs
-
in hemolytic jaundice (RBCs are one of the sources of LDH)
-
in hepatitis
g) albumin:
-
in chronic process in the liver:
cirrhosis
cancer
-
normal in acute process in the liver:
viral hepatitis
choledocholithiasis
h) immunological tests:
- autoantibodies,
e.g.:1ry biliary cirrhosis (antimitochondrial AB <MAM>)
2- URINE
-
urobilinogen
in hemolytic jaundice
or absent in obstructive jaundice (no more bile)
-
conjugated bilirubin
in obstructive (cholestatic) or hepatocellular jaundice
-
Hb urea: intravascular haemolysis
3- STOOL
-
Pale stool in obstructive jaundice
-
stercobilinogen
o in hemolytic jaundice
o or absent in obstructive jaundice (pale stool)
-
occult blood
o carcinoma of GI (metastasis to liver)
o esophageal varices (2ry to liver cirrhosis)
151
" Reading without contemplation is like eating without digestion "
Chinese byword
4- RADIOLOGICAL INVESTIGATION:
-US
Gall stones
Intrahepatic or extrahepatic biliary dilation (due to obstruction by
stone, stricture, or tumor)
Rarely identify site or cause of the obstruction
the distal common bile duct is difficult to be visualized by US (d/t
overlying bowel gas) => so, do CT scan
-CT
assessing the head of pancreas (if there is Ca.)
identify stones in the distal CBD
-ERCP
-PTC
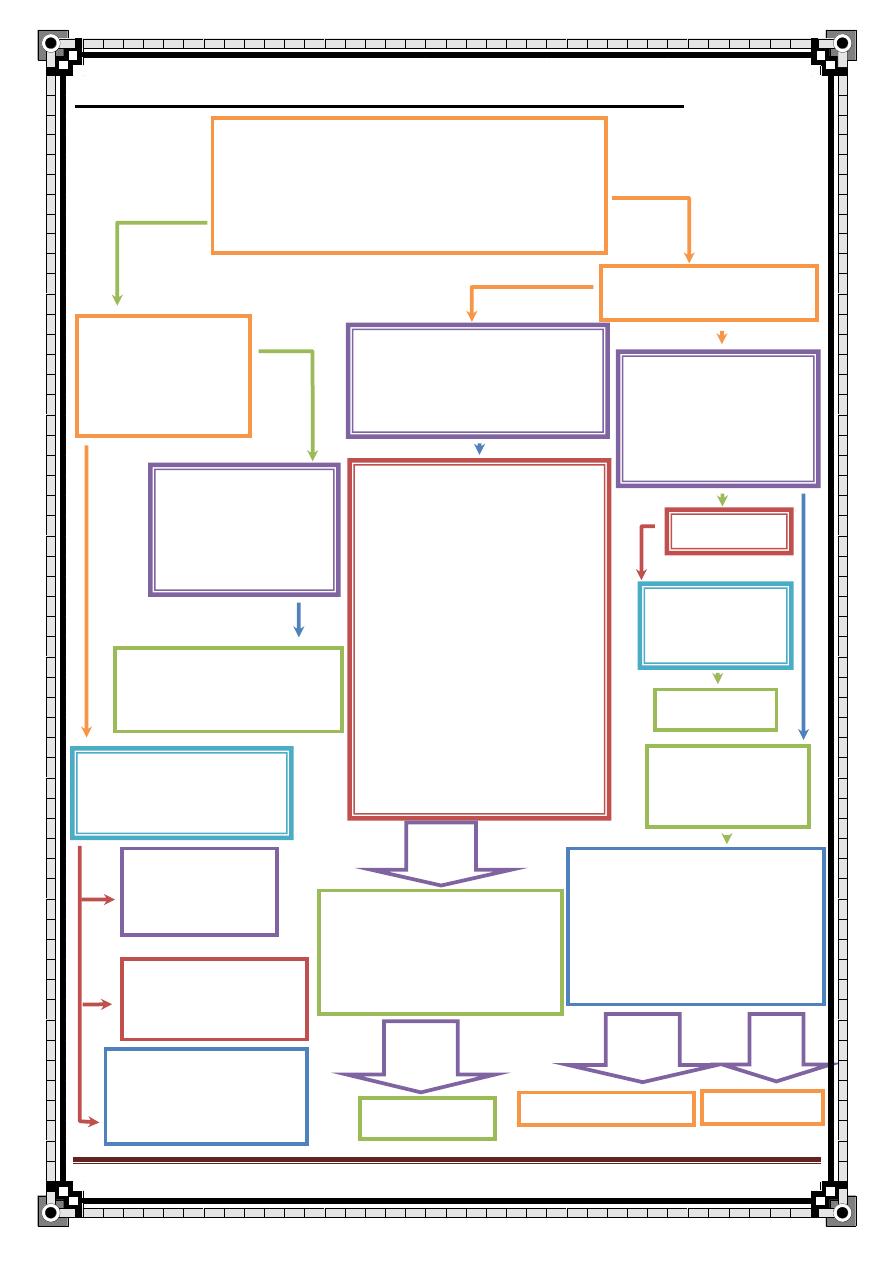
152
" Reading without contemplation is like eating without digestion "
Chinese byword
evaluation of the Patient with Jaundice
Inherited disorders
Dubin-Johnson syndrome
Rotor’s syndrome
Direct (rare)
Hyperbilirubinemia
(direct> 15%)
Serologic Testing
AMA*** (1ry biliary cirrhosis)
Hepatitis serologies
Hepatitis A, CMV, EBV
Review drugs
Ducts not dilated
(intrahepatic
cholestasis)
Liver biopsy
ERCP/liver biopsy
Hemolytic disorders
Ineffective
erythropoiesis
Inherited disorders
Gilbert’s syndrome
Crigler-Najjar
syndromes
Drugs
Rifampicin
probenecid
Indirect (mainly)
Hyperbilirubinemia
(direct< 15%)
Liver biopsy
Additional virologic testing
CMV,
DNA, EBV capsid antigen
Hepatitis D antibody (if
indicated)
Hepatitis E IgM (if indicated
)
Dilated ducts
(extrahepatic
cholestasis)
CT/ERCP
ultrasound
viral serologies:
hepatitis A IgM
hepatitis B surface antigen
and core antibody
hepatitis C RNA
toxicology screen
paracetamol level
ceruloplasmin* (if pt. less
than 40 yrs of age)
ANA, SMA, LKM, SPEP**
Bilirubin and other liver
tests elevated
Isolated
elevation of
the bilirubin
History (focus on medication/drug exposure)
Physical examination
Lab tests: bilirubin with fractionation, ALT, AST,
alkaline phosphatase, prothrmbin time, and albumin
Hepatocellular pattern:
ALT/AST elevated out of
proportion to ALP
AMA
+ ve
Results
- Ve
Results
- Ve
Cholestatic pattern:
ALP elevated out of
proportion to ALT/AST
Results
- Ve
153
" Reading without contemplation is like eating without digestion "
Chinese byword
* ceruloplasmin decrease in Wilson’s disease
** ANA=
antineuclear antibodies
SMA= smooth muscle antibody
LKM= liver-kidney microsomal antibody
SPEP= serum protein electrophoresis
[testing for autoimmune hepatitis]
*** AMA= antimitochondrial antibodies
for Dx of 1ry biliary cirrhosis
Primary biliary cirrhosis:
-disease of middle aged women
-progressive destruction of interlobular bile ducts
-AMA found in 95% of cases
HISTORY TAKING
ID:
Occupation (hydatid cyst in farmers)
HPI:
1-duration of the jaundice
2-onset:
Sudden: CBD stone, viral hepatitis
gradual: cirrhosis, pancreatic Ca.
3-pattern:
154
" Reading without contemplation is like eating without digestion "
Chinese byword
fluctuating: CBD stone, ampullary Ca, hemolytic episodes
progressive: pancreatic Ca, cholangiocarcinoma
4-pain:
painful: CBD stone, pancreatic disease
painless: malignancy, viral hepatitis (although there is dragging subcostal pain)
5-history of:
blood transfusion
tattoos
viral hepatitis
contact with jaundiced pt.
serum sickness like syndrome
(arthalgia, myalgia, urticaria, malaise)
anorexia
wt. loss malignancy
abdominal pain (RUQ)
6-fever
CBD stone (ascending cholangitis)
7-Pruritis => in obstructive jaundice and hepatitis
8-Dark urine (or tea color) & pale stool
in conjugated hyperbilirubinaemia
9-fatty dyspepsia
10-steatorrhea
obstructive jaundice
11-bleeding disorder
Fever can be due to:
1-
cholangitis
2-
viraemia due to hepatitis
3-
septicemia
4-
hepatic abscess
155
" Reading without contemplation is like eating without digestion "
Chinese byword
12-Symptoms of anemia:
Dyspnea, palpitation, dizziness, fatigue, ….. hemolytic jaundice
Hx of SCD & G6PD
Hx of malaria
Hx of IBD => 1ry biliary cirrhosis
Past Hx:
Biliary surgery (stricture, residual stone)
Social Hx:
- alcohol
frequency
quantity
alcoholic liver cirrhosis
type: wine, whisky, bear
-drug abuse (I.V.)
-sexual activity (homosexuality)
-recent travel
viral hepatitis
-blood transfusion
Family Hx:
-SCD & G6PD
-spherocytosis
(gall stone, anemia, spleenectomy)
-Hx of jaundice in the family
Drug Hx:
-hx of any hepatotoxic drug
-hx of contraceptive pills
156
" Reading without contemplation is like eating without digestion "
Chinese byword
Physical Examination
General appearance:
Cachexia (muscle wasting => in malignant disease)
General examination:
-stigmata of chronic liver disease:
palmer erythema
clubbing (in cirrhosis) in the hand
flapping tremor (in hepatic failure)
Duputren’s contracture
Ecchymosis
spider nevi
Gynecomastia
Testicular atrophy
(these are commonly seen in advanced alcoholic liver cirrhosis)
-
enlarged left supraclavicular lymph node (Virchow’s)
=> in abdominal malignancy
-
JVP (RSHF => congested liver)
-scratch marks
(in obstructive jaundice d/t irritation of nerve endings by bile salts)
157
" Reading without contemplation is like eating without digestion "
Chinese byword
Abdominal examination In Jaundiced Pt:
Inspection:
Caput medusa (dilated periumblical veins d/t liver cirrhosis & portal HTN)
-scratch marks
Abnormal hear distribution
Palpation
1-heptomegaly
o grossly enlarged & hard nodules => in malignancy
o slightly enlarged & smooth => in chronic cholestasis
o enlarged tender liver => in viral & alcoholic hepatitis
2-spleenomegaly
o in hemolytic anemia
o in portal HTN
3-RUQ tenderness
o in hepatitis
o in cholecystitis
o in ascending cholangitis
4-
Murphy’s (+ve)
in acute cholecystitis & ascending cholangitis
5-palpable gall bladder
158
" Reading without contemplation is like eating without digestion "
Chinese byword
Courvoisier’s low:
Palpable gall bladder + jaundice means the jaundice is unlikely to be d/t gall
stones (think about Ca. of head of pancreas)
6-abdominal masses: malignancy
7-abdominal scars: previous operation on biliary tree
8-ascitis: cirrhosis or malignancy
9-PR: color of stool, malignancy
Surgical Treatment
Depends on the cause:
-CBD stones:
ERCP & sphincterotomy followed by laparoscopic cholecystectomy
Failure of ERCP: open cholecystectomy and CBD exploration or
laparoscopic CBD exploration
-Traumatic damage to CBD:
if early end-to-end reconstruction over a T-tube
late stricture requires excision and Roux-en-Y hepaticojejunostomy
-Pancreatic carcinoma:
operable: pancreatoduodenectomy (Whipple’s operation)
inoperable: bypassed by hepaticojejunostomy (Roux-en-Y)
endoscopic expandable metallic stent
-Ampullary and duodenal carcinoma:
Whipple’s operation
-Extrahepatic cholangiocarcinoma:
excision and hepaticojejunostomy
159
" Reading without contemplation is like eating without digestion "
Chinese byword
Surgical ttt of obstructive jaundice:
preoperative preparation:
adequate hydration: 5% dextrose / -500 mls of 10% Mannitol
maintain good urinary output: to avoid hepato-renal syndrome
antibiotics: to avoid sepsis
correction of prolonged PT: vit.K injections
DVT prophylaxis: external intermittent pneumatic calf compression
Cross match blood
160
" Reading without contemplation is like eating without digestion "
Chinese byword
ANO-RECTAL
DISEASES
APPLIED ANATOMY:
Rectum
12–15 cm in length.
Rectum has distinct peritoneal covering.
Fascia:
Waldeyer’s fascia: Rectosacral fascia that extends from S4 vertebral body to rectum.
Denonvilliers’ fascia: Anterior to lower third of rectum.
Pelvic floor: Levator ani (composed of pubococcygeus, iliococcygeus,
and puborectalis muscles); innervated by S4 nerve.
Anus
Anal canal runs from pelvic diaphragm to anal verge (junction of ano-
derm and perianal skin).
Dentate line: A mucocutaneous line that separates proximal, pleated
mucosa from distal, smooth anoderm (1–1.5 cm above anal verge).
Anal mucosa proximal to dentate line lined by columnar epithelium;
mucosa distal to dentate line (anoderm) lined by squamous epithelium
and lacks glands and hair.
Columns of Morgagni: 12–14 columns of pleated mucosa superior to
the dentate line separated by crypts. Perianal glands discharge their secretions at the
base of the columns.
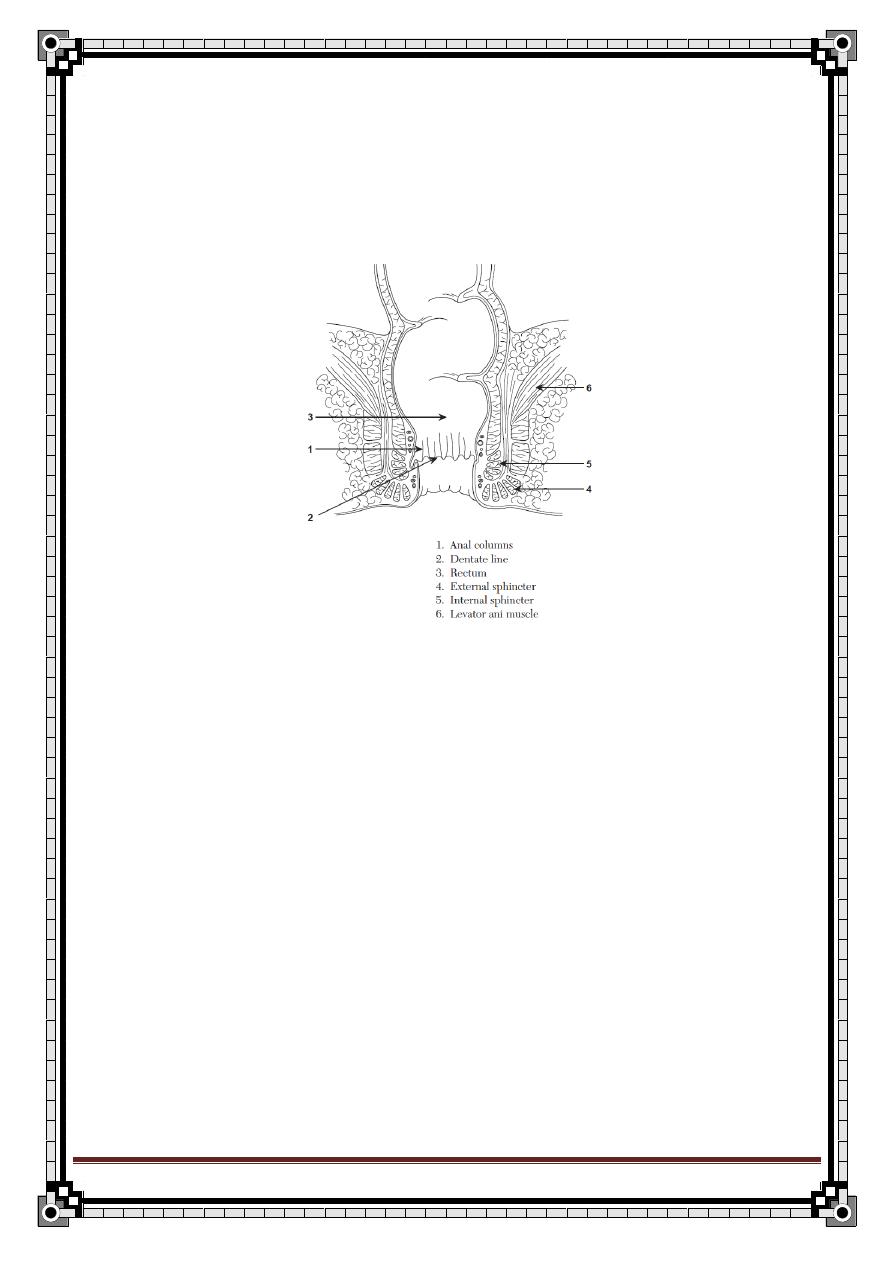
161
" Reading without contemplation is like eating without digestion "
Chinese byword
Anal sphincter:
Internal: Consists of specialized rectal smooth muscle (from inner circular layer);
involuntary, contracted at rest, responsible for 80% of resting pressure.
External: Consists of three loops of voluntary striated muscle; a continuation of
puborectalis muscle; responsible for 20% of resting pressure and 100% of
voluntary pressure.
Blood Supply of (colon , rectum , anus)
Arterial
Superior mesenteric artery (SMA): Supplies the cecum, ascending colon, and
proximal two thirds of the transverse colon via the ileocolic,
right colic, and middle colic arteries, respectively.
Inferior mesenteric artery (IMA): Supplies the distal two thirds of the
transverse colon, sigmoid colon, and superior rectum via the left colic,
sigmoidal, and superior rectal (hemorrhoidal) arteries, respectively.
Internal iliac artery: Supplies the middle and distal rectum via the
middle rectal and inferior rectal arteries, respectively (the inferior rectal
artery is a branch of the internal pudendal artery).
Internal pudendal artery: Supplies the anus; is a branch of the internal iliac artery.
162
" Reading without contemplation is like eating without digestion "
Chinese byword
Venous drainage
Rectum
The superior haemorrhoidal veins which draining the upper half of the anal canal
above the dentate line pass upwards to become the rectal veins: these unite to form
the superior rectal vein, which later becomes the inferior mesenteric vein.
This forms part of the portal venous system and ultimately drains into the splenic vein.
Middle rectal veins exist but are small, unimportant channels unless the normal paths
are blocked.
anus
The anal veins are distributed in a similar fashion to the arterial
supply. The upper half of the anal canal is drained by the superior
rectal veins, tributaries of the inferior mesenteric vein and thus
the portomesenteric venous system, and the middle rectal veins,
which drain into the internal iliac veins. The inferior rectal veins
drain the lower half of the anal canal and the subcutaneous
perianal plexus of veins: they eventually join the internal iliac vein on
each side.
Lymphatic Drainage
Lymphatics of the colon, rectum, and anus generally follow the arterial sup-
ply, with several levels of nodes as one moves centrally toward the aorta (e.g.,
ileocolic nodes, superior mesenteric nodes, etc.).
Innervation
Derives primarily from autonomic nervous system.
Sympathetic nerves: Inhibit peristalsis.
Parasympathetic nerves: Stimulate peristalsis.
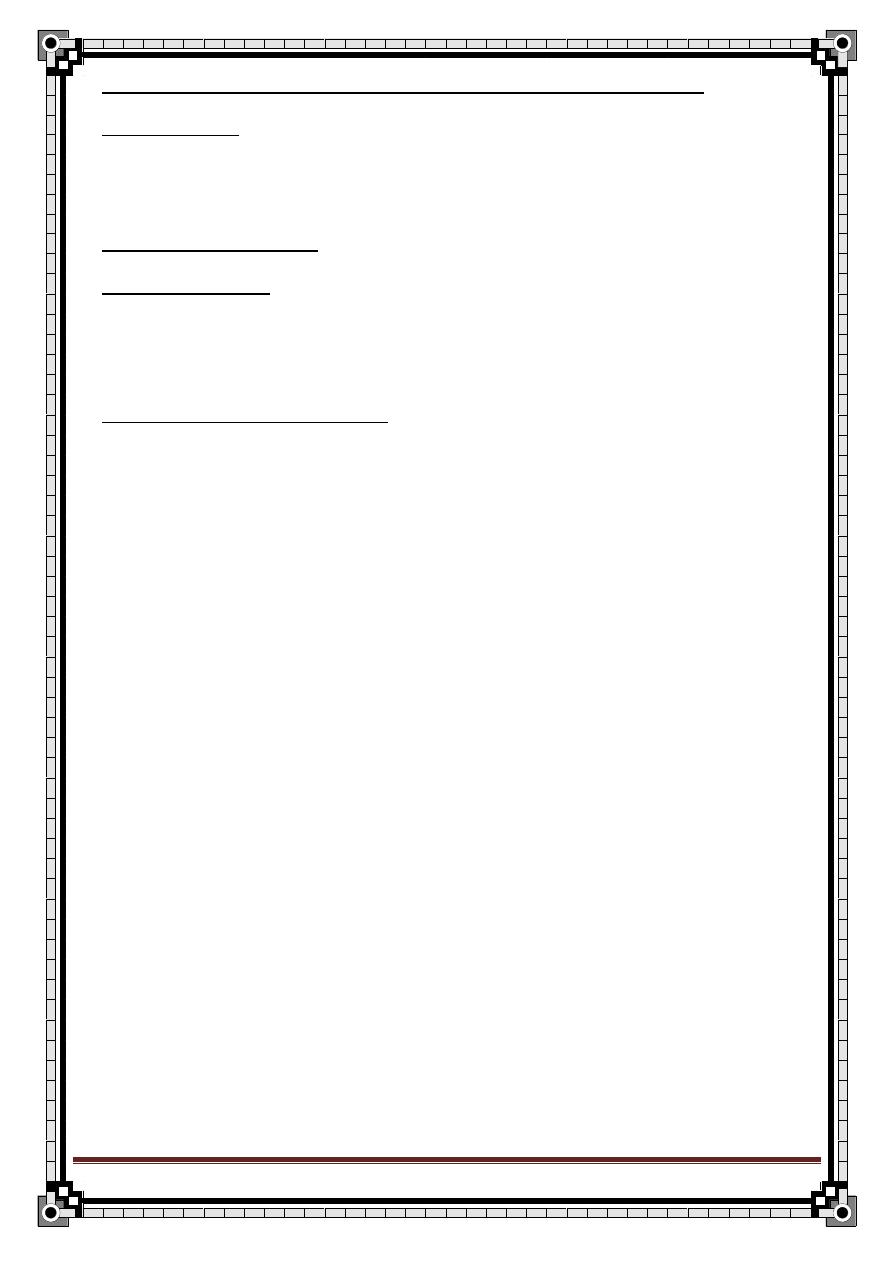
163
" Reading without contemplation is like eating without digestion "
Chinese byword
DIAGNOSIS OF ANAL CONDITIONS WHICH PRESENT WITH:
PAIN ALONE:
1- fissures
2- proctalgia fugax
–pain spontaneously at night-
3- anorectal abscess
PAIN AND BLEEDING: fissures
PAIN AND LUMP:
1-perianal hematoma
2- anorectal abscess
PAIN, LUMP AND BLEEDING:
1- prolapsed haemorrhoids
2- carcinoma of the anal canal
3- prolapsed rectal polyp or carcinoma
4- Prolapsed rectum
DIAGNOSIS OF CONDITIONS PRESENTING WITH RECTAL BLEEDING
BUT NO PAIN:
Blood mixed with stool colon carcinoma
Blood streak on stool rectal carcinoma
Blood after defecation haemorrhoids
Blood and mucus colitis
Blood alone diverticular disease
Melaena peptic ulcer
Bleeding and pain fissure or anal carcinoma
HEMORRHOIDS (PILES)
Heme = blood , Rhoids= flowing , Piles= ball
* it is the commonest cause of rectal bleeding
ANATOMY:
Within the anal canal there are anal cushions which contain blood vessels
(arterioles, venues, A-V fistula) muscles and connective tissues.
These cushions are found at the ano-rectal junction above the dentate line.
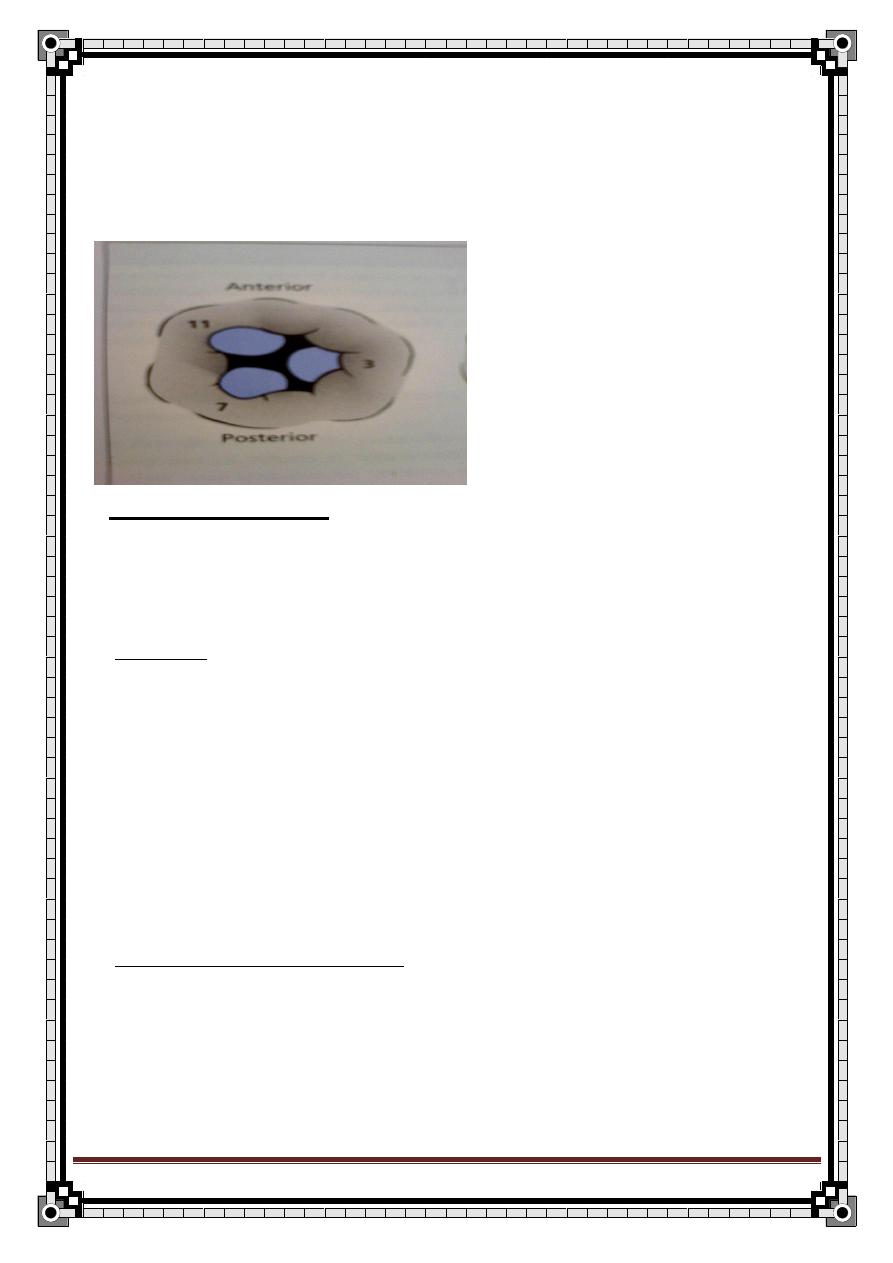
164
" Reading without contemplation is like eating without digestion "
Chinese byword
They lie in the left lateral, right anterior and right posterior positions relative
to the anal canal (3, 7, 11 o’clock position) when the pt. lies in the lithotomy
position.
In-between these 3 primary haemorrhoids (cushions) there may be smaller
secondary ones.
PATHOPHYSIOLOGY:
Anal cushions may become congested as a result of increased intra-
abdominal pressure (straining) or by compression of superior rectal vein by
a carcinoma in the rectum or by the uterus of a pregnant women.
CAUSES:
1- carcinoma of the rectum: may compress or cause thrombosis of the
superior rectal vein piles
2- pregnancy: pregnant uterus compress superior rectal vein also
progesterone causing an increase in the pelvic circulating volume.
3- Chronic constipation: straining increases intra-abdominal pressure. Hard
stool passage traumatizes the cushion’s wall.
4- Also, heart failure, excessive use of laxatives and portal HTN are
causes.
*internal and external hemorrhoids are differentiated by their anatomical
origin in the anal canal.
INTERNAL HAEMORRHOIDS:
-develops above the dentate line.
-covered by anal mucosa.
-lacks sensory innervation (painless)
-bright red or purple in color.
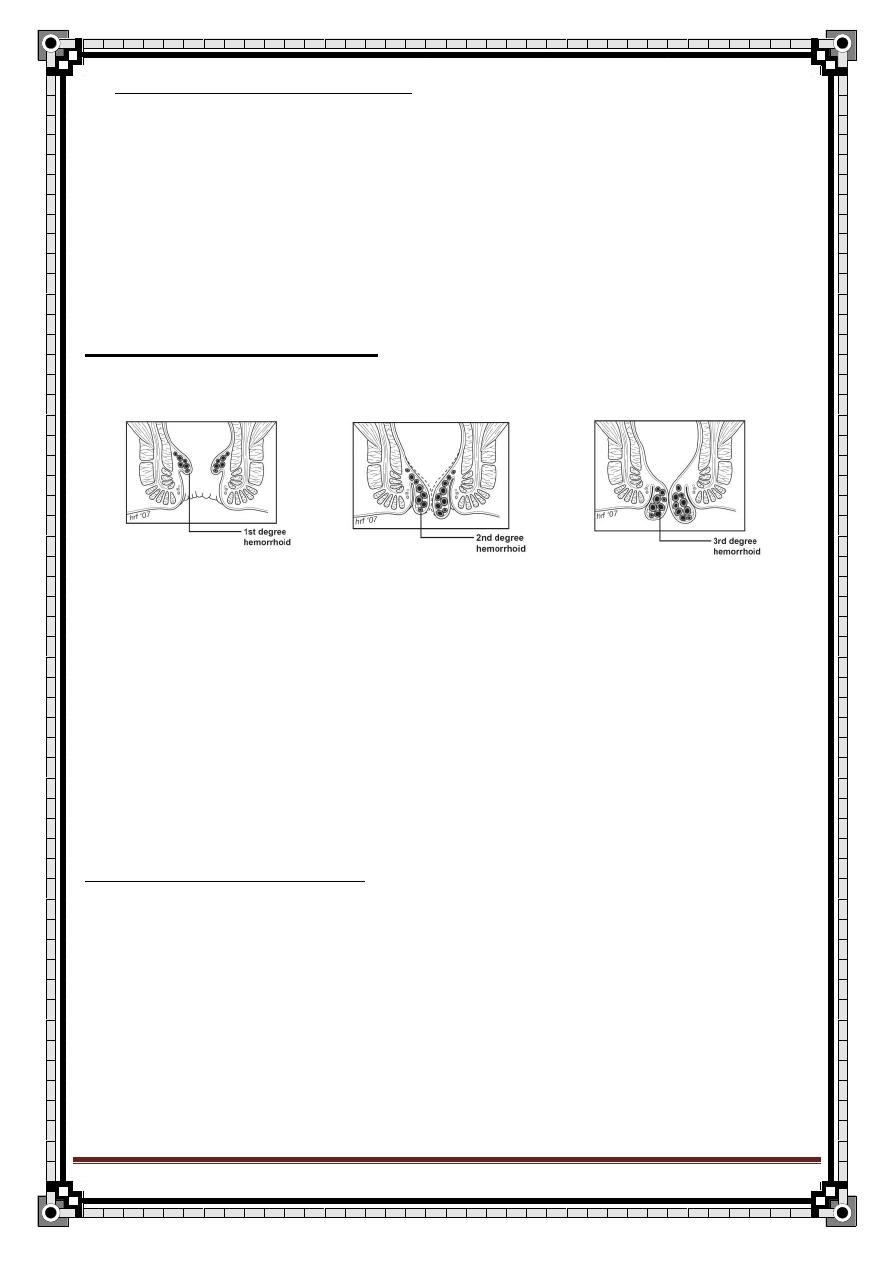
165
" Reading without contemplation is like eating without digestion "
Chinese byword
EXTERNAL HAEMORRHOIDS:
-arise below the dentate line.
-Covered by St. sq. epith.
-innervated by the inferior rectal nerve.
Internal H. drains into sup. Rectal veins portal system
External H. drains into inf. Rectal veins I.V.C.
GRADING HAEMORRHOIDS :
Internal H. are classified by the degree of tissue prolapse into the anal canal.
GRADE 1: they are confined to the anal canal with minimal bleeding or maybe
asymptomatic but do not prolapse.
GRADE 2:they prolapse on defecation or straining then reduce spontaneously.
GRADE 3: prolapse with or without straining and require manual reduction.
GRADE 4: chronically prolapsed and if reducible fall out again. Others fall out
of the anus and are irreducible (strangulated) surgical emergency.
PREDESPOSING FACTORS:
Most H. are idiopathic, but they may be precipitated by factors that produce
sup. Rectal vein congestion.
1- Compression by any pelvic tumour or pregnant uterus.
2- Cardiac failure or portal HTN.
3- Chronic constipation.
4- Use of purgatives (laxatives) excessively.
5- Rectal carcinoma.
166
" Reading without contemplation is like eating without digestion "
Chinese byword
SYMPTOMS:
Grade 1 usually are asymptomatic or with minimal bright red bleeding on
defecation.
1-bleeding:
-the main and earliest symptom
-starts as bright red bleeding on the surface of the stool or on the toilet paper.
-it may continue intermittently for years or months.
-it often increases in frequency and severity until a steady drip of blood
accompanies defecation.
2-prolapse:
-a much later symptom
-starts transiently on defecation, but occurs with increasing frequency until 3
rd
degree H. develop.
3-discharge:
-a mucous discharge accompanies a prolapsed pile.
-occurs when the columnar mucosa of the upper anal canal is exposed.
4-pruritis: this will follow the discharge.
5-pain: they are painless unless if they are complicated by a thrombus to a
thrombosed pile.
167
" Reading without contemplation is like eating without digestion "
Chinese byword
SIGNS: the pt. should be in the left lateral position.
INSPECTION:
-1
st
degree H. show no outward abnormality
-2
nd
degree H. may show the skin covered components when the buttocks are
separated or piles may prolapse when the pt. strains.
-3
rd
degree H. shows the red anal mucosa in their position (3,7,11)
DIGITAL EXAMINATION: internal H. can’t be felt unless they are thrombosed
or in the long standing thickened piles.
Proctoscopy: it is the key investigation.
- When the proctoscope is slowly withdrawn just below the anorectal
ring the H. will bulge into the lumen of the proctoscope.
- The pt. is asked to strain during the withdrawal so the vascular
engorgement is produced and the degree of prolapse can be
determined.
*don’t forget abdominal examination.
Thrombosed piles: the skin around the anus is swollen and edematous
in relation to the pile bearing areas.
INVESTIGATIONS:
1-Sigmoidoscopy : essential to exclude co-exclude rectal pathology as
carcinoma or polyps.
2-barium enema: indicated when Sigmoidoscopy and Proctoscopy
can’t
explain the symptoms.
3-CBC: anemia, rarely happen in longstanding piles
168
" Reading without contemplation is like eating without digestion "
Chinese byword
DDx:
1- Anal or rectal cancer.
2- pedunculated polyps.
3- Rectal prolapse.
4- Anal fissures or fistula or hematoma
– if painful-
COMPLICATIONS:
1- anemia: rarely may follow a sever or continuous bleeding
2- Strangulation: when a prolapsing pile become gripped by the external
anal sphincter.
3- Thrombosis: results from an occlusion of the venous return by a
strangulated pile. It is swollen, painful, tense and dark.
4- Ulceration: superficial ulceration of the exposed mucous membrane.
5- Gangrene: when strangulation is so tight to constrict the arterial supply
of the H.
6- Suppuration: uncommon. Due to infection of the thrombosed pile.
7- Fibrosis: after the thrombosis, the H. may be converted into fibrous
tissue.
8- Profuse hemorrhage
9- Ulceration
10- Portal pyaemia
TREATMENT:
1-first degree H.: bulk laxatives and high dietary fibers maybe enough to
decrease the constipation
2-injection therapy (sclerotherapy):
-for the 1
st
degree and early 2
nd
degree H.
-3-5 ml of 5% phenol in almond oil is injected through a special syring to the
base of the pile or just above the anorectal ring.
-It is a painless procedure if done properly because the high anal canal area
is painless.
-Bleeding should stop within 24-48 hours.
169
" Reading without contemplation is like eating without digestion "
Chinese byword
-Procedure may be repeated after a few weeks if necessary.
3- Rubber band ligation:
-effective with 1
st
and 2
nd
degree H.
-a small o-ring rubber band applied to constrict the mucosa at the base. This
will lead to strangulation of the pile and subsequent sloughing of the pile over
a period of 10 days or so.
4-infra-red photocoagulation.
5-cryotherapy: a cryoprope is applied to the overlying mucosa.
6-stretching of the anal sphincter: decrease the need for straining.
Overstretching may lead to anal incontinence.
7-haemorrhoidectomy:
Necessary for
1-failure of conservative treatment
2-the 3
rd
& 4
th
degree Hemorrhoids.
2-prolapsed thrombosis or fibrosed or combined internal and external
hemorrhoids .
Post operative complications:
Early:
1- Severe pain
2- Urine retention
3- Reactionary hemorrhage
Late:
1- Bacterial infection
2- Secondary hemorrhage
3- Anal stricture
4- Anal fissure
5- Fecal incontinence
170
" Reading without contemplation is like eating without digestion "
Chinese byword
CARCINOMA OF THE RECTUM
Carcinoma of the rectum accounts for approximately one third of all
tumours of the large intestine.
Predisposing factors are:
1- pre-existing adenomas
2- familial adenomatous polyposis
3- ulcerative colitis.
Diagnosis is made on the basis of: the history, rectal examination,
Sigmoidoscopy and biopsy finally.
75% occur in the lower part of the rectal ampulla A simple ulcer with
everted edges or papilliferous.
25% in the upper part of the rectum annular in shape.
90% of rectal cancers can be felt with a finger during PR.
MACROSCOPIC APPEARANCE:
It may be as follows:
papilliferous
ulcerating commonest
stenosing at rectosigmoid
colloid
MICROSCOPIC APPEARANCE:
*90% are adenocarcinoma
*9% are colloid
– adenocarcinoma with mucous production-
*1% highly anaplastic carcinoma simplex
*at the anus, sq. cc can occur but, a malignant tumour protruding through
the anal canal is more likely to be an adenocarcinoma of the rectum invading
the anal skin.
Rectal ca is common in middle and old age (50-70 yrs) but can occur in
young adults.
It is equally common in both sexes.
171
" Reading without contemplation is like eating without digestion "
Chinese byword
SYMPTOMS:
Rectal bleeding: small dark red streak on the stool. If a lot of blood
accumulates it can pass as such but this is uncommon.
The surface of the tumour produces mucous which is expressed in a
more liquid motion
– diarrhea like- but if it pools it can be passed as liquid
faeces. Specially at morning
There may be change in bowel habit usually towards constipation.
High annular cancers at the rectosigmoid junction may cause partial
obstruction presenting as alternating constipation and diarrhoea.
Tenesmus tumour in the lower part of the rectum is large to fool the
sensory mechanisims into thinking it is faeces.
Wight loss: this is common even if there is no any metastasis.
Small primary lesions maybe symptom less but associated with multiple
metastasis especially to the liver. Here the pt. has upper abdominal pain,
malaise and a palpable mass.
Pain is an uncommon symptom, but if present it could be:
1- Colic, with distension and vomiting. Caused by high annular tumours
obstructing the lumen.
2- Local pain in the rectum, perineum or lower abdomen. Caused by direct
spread of the tumour to the surrounding structures especially the sacral
nerves.
3- Pain on defecation, occurs if the tumour has spread downwards below the
mucocutanious junction into the sensitive anal canal. It can mimic a fissure.
Any pt. complaining of passing water through the rectum, usually has rectal
carcinoma or villous adenoma.
In the past history, the pt. may have a long standing or extend for long
sigment Ulcerative colitis increases the risk of rectal ca after 10 or more
years of the disease.
Also, the symptoms of cancer may be thought as a recurrence of UC and
could lead to late presentation.
In the family Hx, polyposis
– in which the entire colon and rectum are
carpeted by polyps one of which could turn malignant at any time.
SIGNS ON EXAMINATION:
on rectal examination:
Usually nothing abnormal to see around the anus, but you can see a low
tumour protruding through the anus.
What can be felt depends upon the site of the lesion.
If the tumour is low in the ampulla, the finger can feel the whole lesion.
More commonly, only the lower edge of a malignant ulcer can be felt. It feels
hard and bulges into the lumen of the rectum, the edges are everted and the
base is irregular and friable.
172
" Reading without contemplation is like eating without digestion "
Chinese byword
Upon withdrawal of the finger, you will have blood and mucous on the gloved
finger.
If the tumour is in the upper part of the rectum, only the lower edge is felt.
This position of the lesion makes it hard to decide if the tumour is in the
rectum or out of it Sigmoidoscopy is the answer.
PR is not reliable in fat people.
On general examination: the liver is the most common site for metastasis.
Other sites for metastasis are: supraclavicular lymph glands, the lungs and
the skin.
Lung metastasis is uncommon but because it is small and peripheral not
producing symptoms or signs, a chest x-ray is mandatory.
Lymph drains to the mesenteric LN then to the pre-aortic LN which are rarely
palpable. Meso-colic glands are occasionally palpable on PR.
The inguinal LN are involved only if the tumour is below the Hilton's line to
involve the skin.
If the pt. has palpable inguinal LN, the tumour is most likely to be sq. cc. of
the anal skin.
SPREAD OF THE CANCER:
1-local:
a- circumferentially around the lumen of the bowel
b- Invasion through the muscles
c- Penetration into adjacent organs as prostate, bladder, vagina, uterus,
sacrum, sacral plexus, ureters and lateral pelvic wall.
2-lymphatic: to regional LN along the inferior mesenteric vessels. At a late
stage, there is invasion of the iliac LN and of the groin LN
–retrograde- and
involvement of the supraclavicular nodes via the thoracic duct.
3-blood: via the superior rectal venous plexus then the portal vein to the liver
and then to the lungs.
4-trans-coelmic: seeding of the peritoneal cavity.
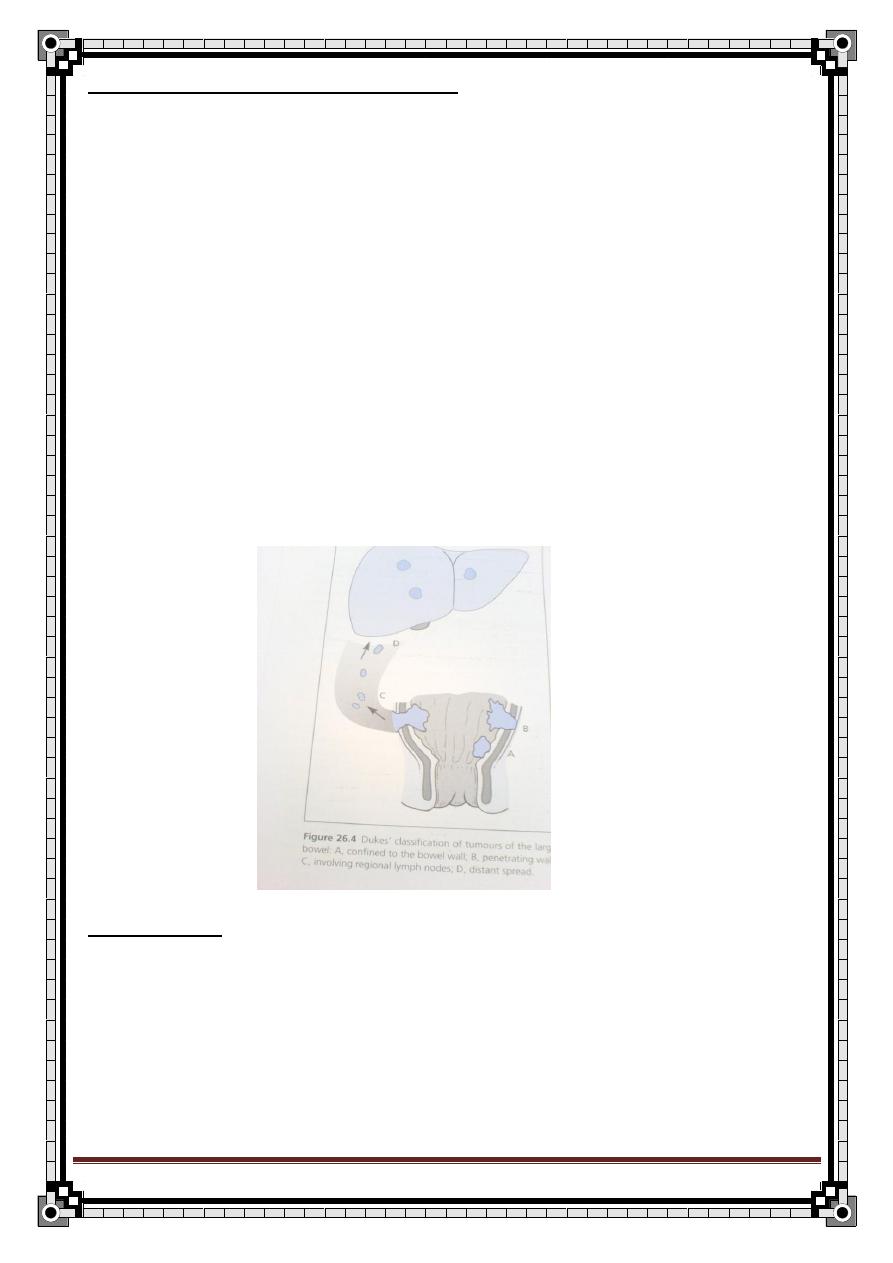
173
" Reading without contemplation is like eating without digestion "
Chinese byword
STAGING OF RECTAL CARCINOMA:
by Duke’s staging:
A-
The growth is limited to the rectal wall (15%): prognosis
excellent.
B-
The growth is extended to the extrarectal tissues, but no metastasis
to the regional lymph nodes (35%): prognosis reasonable.
C -There are secondary deposits in the regional lymph nodes
(50%). These are subdivided into C1, in which the local
pararectal lymph nodes alone are involved, and C2, in which
the nodes accompanying the supplying blood vessels are implicated
up to the point of division. This does not take into
account cases that have metastasised beyond the regional
lymph nodes or by way of the venous system: prognosis is poor
.
D- Distant metastasis has occurred eg: the liver, invasion of the bladder.
PROGNOSIS:
Depends on the stage of progression of the tumour and on the histological
degree of differentiation. The more advanced the spread and the more
anaplastic its cells, the worse the prognosis.
174
" Reading without contemplation is like eating without digestion "
Chinese byword
SPECIAL INVESTIGATIONS:
1-Sigmoidoscopy : to inspect and take a biopsy.
2-barium enema: the indications for this procedure are:
1)
The growth isn’t visualized by Sigmoidoscopy
2) if a second tumour is suspected
3) ulcerative colitis
4) familial polyposis
3-ultrasound of the abdomen to check liver metastasis and ascites.
DDx OF RECTAL TUMOUR:
Benign growth Adenoma
Inflammatory stricture
Carcinoid tumor
Ovarian or uterine tumours
Extension of a carcinoma in the prostate or cervix
Diverticular disease
Endometriosis
Lymphogranuloma inguinale
Amoebic granuloma
Faeces
– known by indentation on examination-
TREATMENT:
Curative:
Surgery depends on the distance of the tumour from the anal verge.
Upper third tumours high anterior resection with anastomosis between
the sigmoid and lower rectum
Lower third tumours less than 5 cm from the anal verge are ttt by
abdominoperineal excision of the rectum + terminal colostomy +
adjunctive radiotherapy to reduce recurrence.
Mid third tumours low anterior resection if distal clearance can be
obtained. This easier in women due to the wide pelvic
Palliative procedure: Even if secondary tumours are present, palliation is best
achieved when the primary is resected. Colostomy is necessary for
intestinal obstruction. But this doesn’t relieve the bleeding, discharge and
sacral pain. In inoperable cases, deep x-ray therapy, diathermy, or laser of
the tumour may give temporary relief as may cytotoxic drugs.
175
" Reading without contemplation is like eating without digestion "
Chinese byword
DIVERTICULAR DISEASE
this disease may present in one of the following manners:
1-chronic left sided abdominal pain + change in bowel habits
2-acute abdominal symptoms
3- Rectal bleeding: acute, massive and fresh blood
Elderly pt. with this disease present with a little faint, lower abdominal
pain, and a desire to defecate that when emptied pass large volume of
fresh blood and clots.
The patients are rarely shocked and don’t require transfusion.
It is diagnosed via barium enema or colonscopy
Causes of bleeding are:
1- eroded artery in the mouth of the diverticulum
2- the disease is incidental and the bleeding is due to angiodysplasia of the
chronic mucosa
surgery is very rarely needed
PERI-ANAL HEMATOMA
It is not a true hematoma but a thrombosis of a vein in the subcutaneous
plexus.
There are no presepitating factors usually but causes could be:
1-injury to the venous wall during anal stretching with defecation
2-after straining and stretching of the perineum during the second stage of
labour in child birth.
An inflammatory reaction is present in the area with pain and oedema.
It can occur at all ages and in both sexes equally.
It can occur any where in the anal area, be multiple or be recurrent.
SYMPTOMS:
176
" Reading without contemplation is like eating without digestion "
Chinese byword
1- pain: usually due to the tension
*it begins gradually increasing in severity over a few hours and subsiding
gradually over few days
*it is continuous.
*made worse by sitting, moving and defecating
*localized to the lump
2-swelling:
*appears at the same time as the lump
*First it is small and spherical
* Then it may enlarge and become more painful
3-bleeding: this happens only if:
*the lump bursts
*the skin over the lump ulcerates
4- The skin around the lump is itchy and moist due to the leakage of the
mucous because the lump doesn’t allow the anus to close properly.
SIGNS ON EXAMINATION:
*Colour: if it is close to the overlying skin which is not edematous, it is deep
red-
purple. But if the skin is edematous then its colour can’t be seen.
*The lump is tender especially if it ulcerates.
*shape and size: initially the lump is spherical and up to 1cm in diameter. If
the skin is lax or edematous then the lump is polypoid.
*surface: covered by skin and the surface beneath it is smooth
177
" Reading without contemplation is like eating without digestion "
Chinese byword
*composition: solid, hard hemispherical mass
*relations: the lump is superficial to the external sphincter. Not fixed to the
skin or other structures. Cannot be reduced to the anal canal.
TREATMENT:
The symptoms may subside spontaneously after 2-3 days during which
analgesia is given. If it is in the acute phase and the patient doesn’t want to
wait, incision under local anaesthesia is the way to go.
FISSURE-IN-ANO
*anal fissure is a longitudinal split in the skin of the anal canal
PATHOPHYSIOLOGY:
178
" Reading without contemplation is like eating without digestion "
Chinese byword
An acute tear is common and usually heals quickly. Re-opening of the tear
when the pt. next defecates will cause more pain causing an increase in
the tone of the anal sphincter spasm the tear is more likely to open at
each defecation vicious circle of tear-pain-spasm- and more tear then
the base of the lesion becomes fibrous no healing chronic ulcer.
*acute fissures are common in children who pass bulky stool quickly
*chronic fissures are most common in the age group 20 and 40 years.
*chronic fissures are common in women after childbirth.
*anal fissures are more common in men than in women.
*multiple fissures may complicate Crohn’s disease.
SYMPTOMS:
1-Pain:
fissures are the commonest cause of pain in the anal verge
both acute and chronic fissures are very painful
it begins at defecation and is described as tearing
it persists for minutes to hours after defecation
it is throbbing or aching in nature
2- Bleeding:
acute fissures may streak the stool with blood and stain the toilet paper
Chronic fissures bleed less and may produce little blood stain of the
toilet paper if any.
3-a small skin tag called sentinel tag or sentinel pile may form at the
lower end of a chronic fissure. This tag may be felt by the pt.
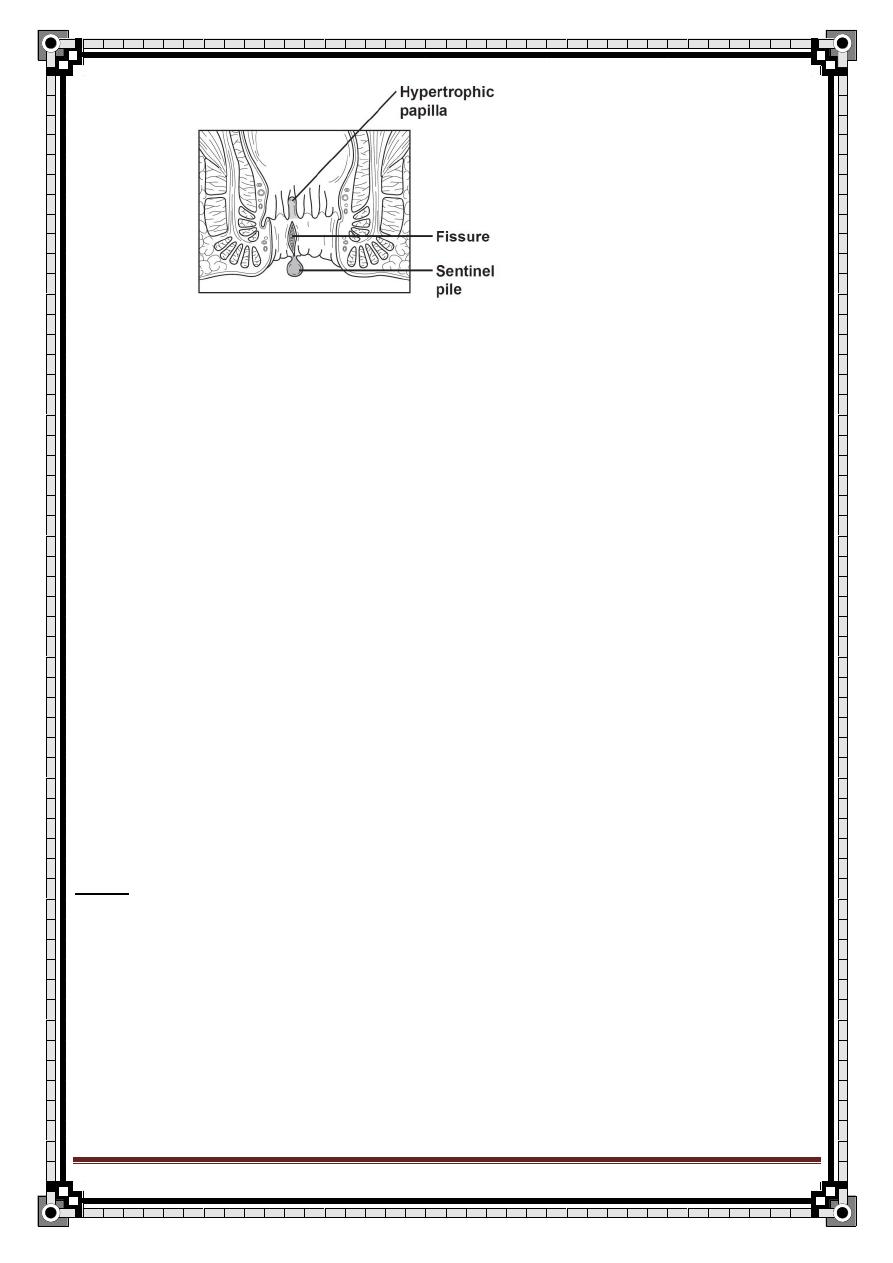
179
" Reading without contemplation is like eating without digestion "
Chinese byword
4- Because of the pain, the pt. is usually constipated.
5-the fibrosis around the chronic fissure prevents a good seal around the
anus leading to small amounts of mucous leak on the peri-anal skin
pruritus
–could be the presenting symptom of a chronic fissure-
6-the symptoms are slow to develop and become long standing, there may
be periods of remission
The majority of the fissures are in the midline posteriorly, but some are
anterior and a few are lateral.
The diagnosis is made by inspection of the area after gently parting the
skin of the anus and seeing a split.
The anal sphincter is in spasm and any attempt to open it or doing PR is
very painful this is contraindicated
You can do PR only if the pain is not sever detecting the defect in the anal
canal skin. There will be a streak of fresh blood on the gloved finger after
withdrawal
Never attempt to do Sigmoidoscopy or Proctoscopy without anaesthesia.
When done under an anaesthetic, the raw base of the fissure will be seen
as the instrument is withdrawn.
DDx:
crohn’s disease
trauma (abuse of children)
carcinoma
TB
syphilis
psoriasis.
180
" Reading without contemplation is like eating without digestion "
Chinese byword
TREATMENT:
Acute fissures:
*if early and small may heal spontaneously.
*local anaesthetic ointment + lubricant laxative relief
*application of GTN cream or ca+2 chanal blockers like diltiazem relaxes the
anal sphincter healing of the epithelium.
*chemical sphincterotomy using an injection of botulinum toxin into the internal
sphincter
*advantages of the chemical method are:
1-sphincter paralysis is short lived
2-gives a more sustained effect than GTN cream
*more intractable cases respond to dividing the internal sphincter submucosally
under general anaesthetic.
Chronic fissures: require excision
FISTULA-IN-ANO
DEFENITION:
A fistula is a track lined with epith. Or granulation tissue, connecting two
epithelial surfaces. It may connect two body cavities or one cavity and the
body’s external surface.
A fistula-in-ano connects the lumen of the rectum or anal canal with the external
surface. It is usually lined by granulation tissue.
181
" Reading without contemplation is like eating without digestion "
Chinese byword
CAUSES:
1-abscess:
In most cases, it is caused by an abscess in the inter-sphenteric space
bursting in two directions internally into the anal canal and externally to the
skin.
2-
IBD: Crhon’s disease causes multiple painless fistulas. Here the disease is
primarily involving the terminal ileum.
3-low rectal carcinoma
CLASSIFICATION:
There are high level fistulas and low level fistulas. It is important to differentiate
between them as the surgical management of both is completely different.
LOW LEVEL FISTULAS:
The internal opening is below the anorectal ring
This ring is the point where the puborectalis muscle sling fuses with the
external sphincter
The ring is the major muscle involved in maintaining continence fistulas
below it (low level) may be opened without impairing continence.
They could be of the following:
1-trans sphincteric
2-inter sphinteric
3-subcutaneous or submucous
HIGH LEVEL FISTULAS:
The internal opening is above the anorectal ring.
If opened, it may divide the ring and make the pt. incontinent
More complex surgery is required
They could be of the following:
1-extra sphincteric (pelvirectal supralevator)
2-trans sphincteric
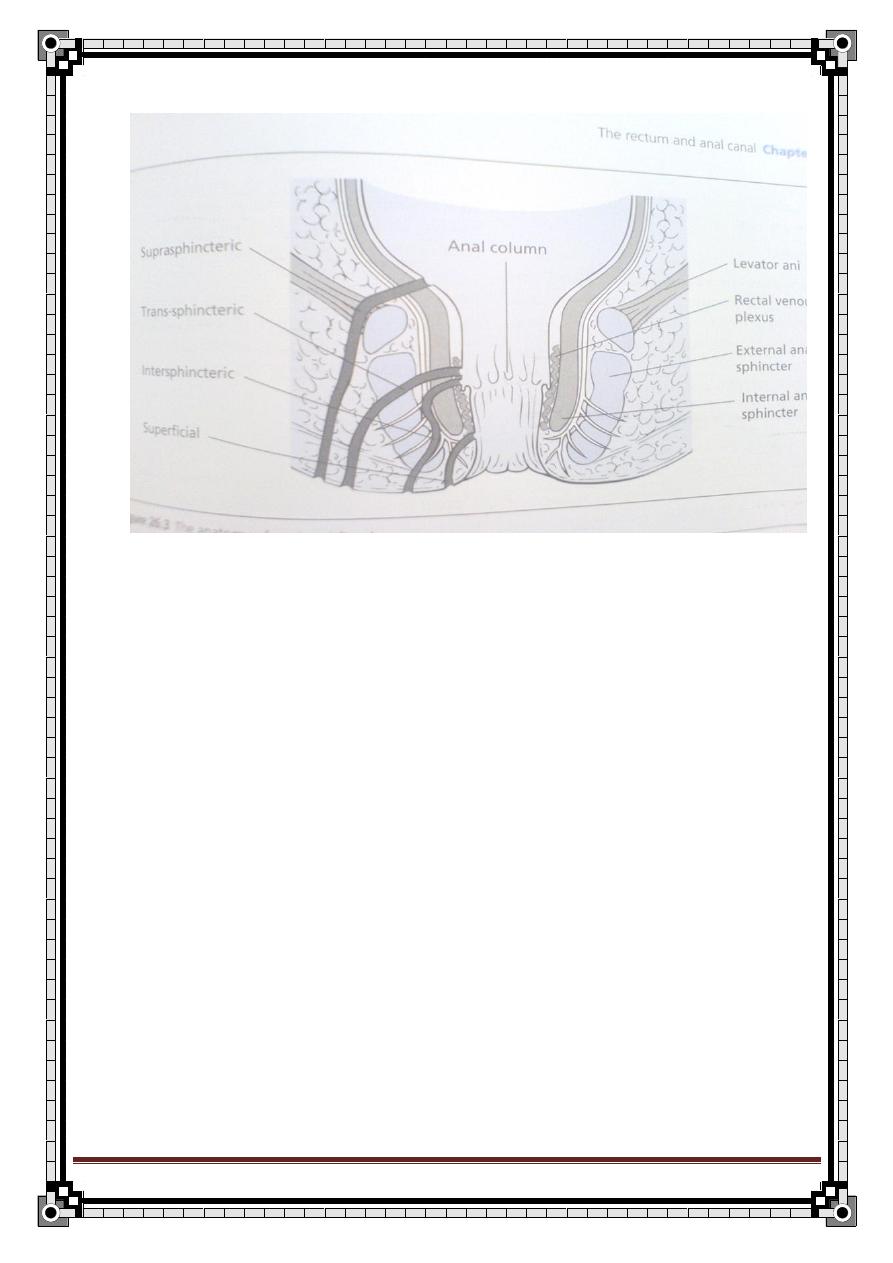
182
" Reading without contemplation is like eating without digestion "
Chinese byword
3-inter sphincteric
SYMPTOMS:
1-
purulent discharge or Watery from the external opening of the fistula. The
pt. may notice bubbling on defecation as mucous is forced through the
fistula stop the fistula from healing.
2-
Pain is episodic as the fistula fills with pus.
If the pus doesn’t discharge
pain is more intense and throbbing
3-
pruritus ani caused by the discharge.
4-
bleeding may be minor from the external opening
5-
There is no difficulty with defecation
6-
The symptoms in general are episodic but the condition hardly ever cures
itself
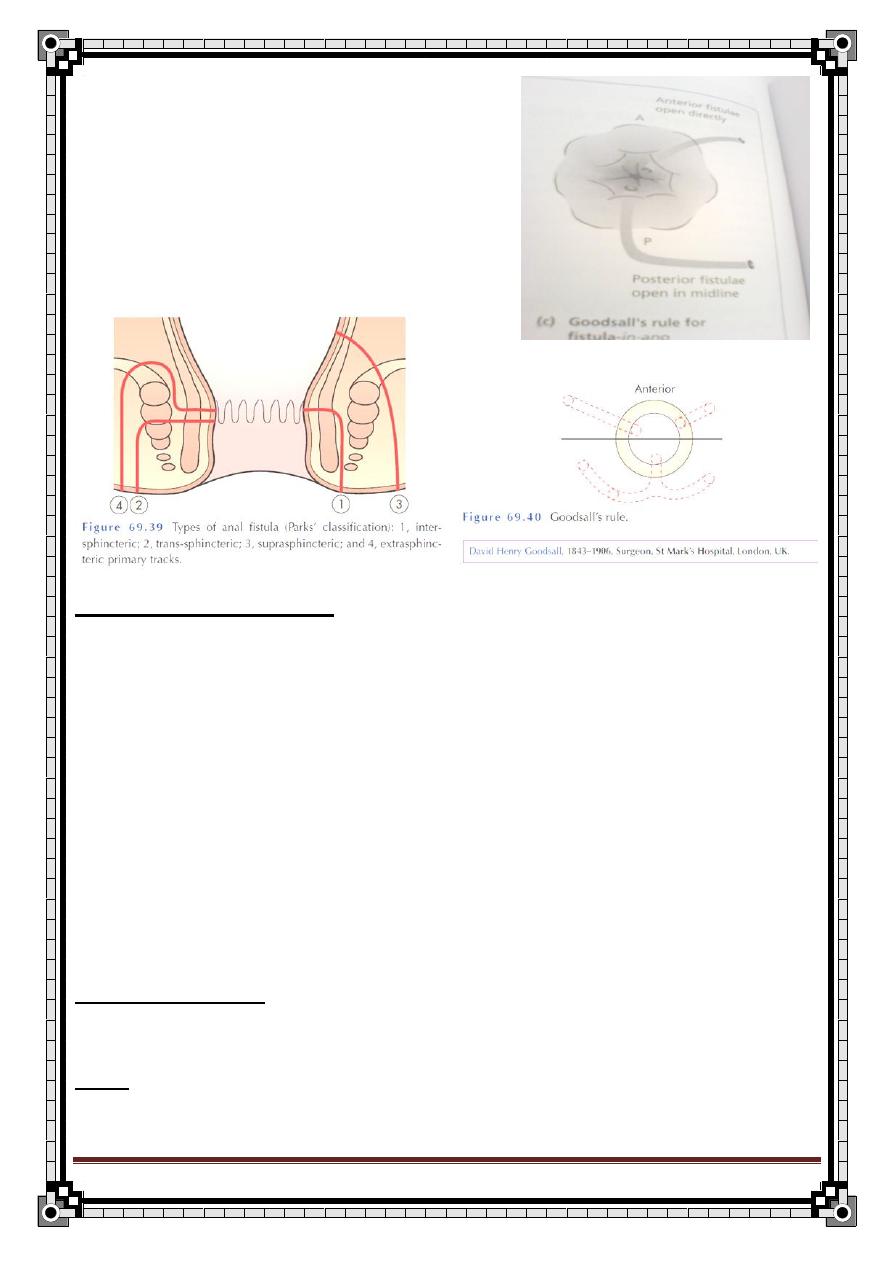
183
" Reading without contemplation is like eating without digestion "
Chinese byword
GOODSALL’S RULE:
The internal opening of an anterior fistula lies
along a radial line drawn from the external
opening to the anus, whereas the internal
opening of a posterior fistula lies in the mid
line posteriorly.
ON PR EXAMINATION:
The external opening is visible anywhere around the anus usually close
to the anal margin but sometimes a few centimetres away.
The opening is not tender but the thickened tissue around it may be.
The serous or purulent discharge may be visible.
Rectal examination is not painful.
The internal opening may be felt. 2/3 are posterior, 1/3 are anterior.
Sigmoidoscopy and proctoscopy are essential to exclude underlying
disease as croh
n’s or carcinoma or TB.
The inguinal LN are not enlarged except if there is inflammation or
secondary infiltration by carcinoma.
Don’t forget general examination if there is a suspected systemic
underlying cause
INVESTIGATIONS: fistulogram, endoanal ultrasound, MRI
DDx: pilonidal sinus, hidradenitis, incontinence, croh
n’s disease, trauma.
184
" Reading without contemplation is like eating without digestion "
Chinese byword
TRAETMENT:
Superficial and low level fistulas are laid open and allowed to heal by
granulation. There is no loss of continence This is only done if the
fistula lies below the anorectal ring
High fistulas (suprasphincteric, trans-sphincteric) only the lower part of
the fistula is laid open a non-absorbable ligature (eg.: nylon) termed a
seton is passed through the upper part of the fistula left for 2-3
weeks the sphincter is fixed by scar tissue subsequent division of the
upper part of the track either by a second operation or by tightening of the
ligature. To avoid incontinence
ANORECTAL ABSCESSES
CLASSIFICATIONS:
1.
Peri-anal (subcutaneous) :
The swelling is at the anal margin which it distorts.
It results from infection a hair follicle, a sebaceous gland or a peri-anal
haematoma.
Pain and tenderness are greater here than in other classes, as the space
in which it expands is confined.
The painful area could be any where around the anal margin.
2- Submucous: infected fissure or laceration of the anal canal
3- Pelvirectal: spread from pelvic abscess
–rare-
4- Ischiorectal:
From infection of the anal gland leading from the anal canal into the
submucosa, spread of infection from a peri-anal abscess or penetration
of the ischiorectal fossa by a foreign body.
The abscess may track as a horse shoe behind the rectum to the opposite
fossa.
It lies lateral to the anus and occupies a much larger space.
The patient with this class of abscess is much more likely to be
systematically unwell.
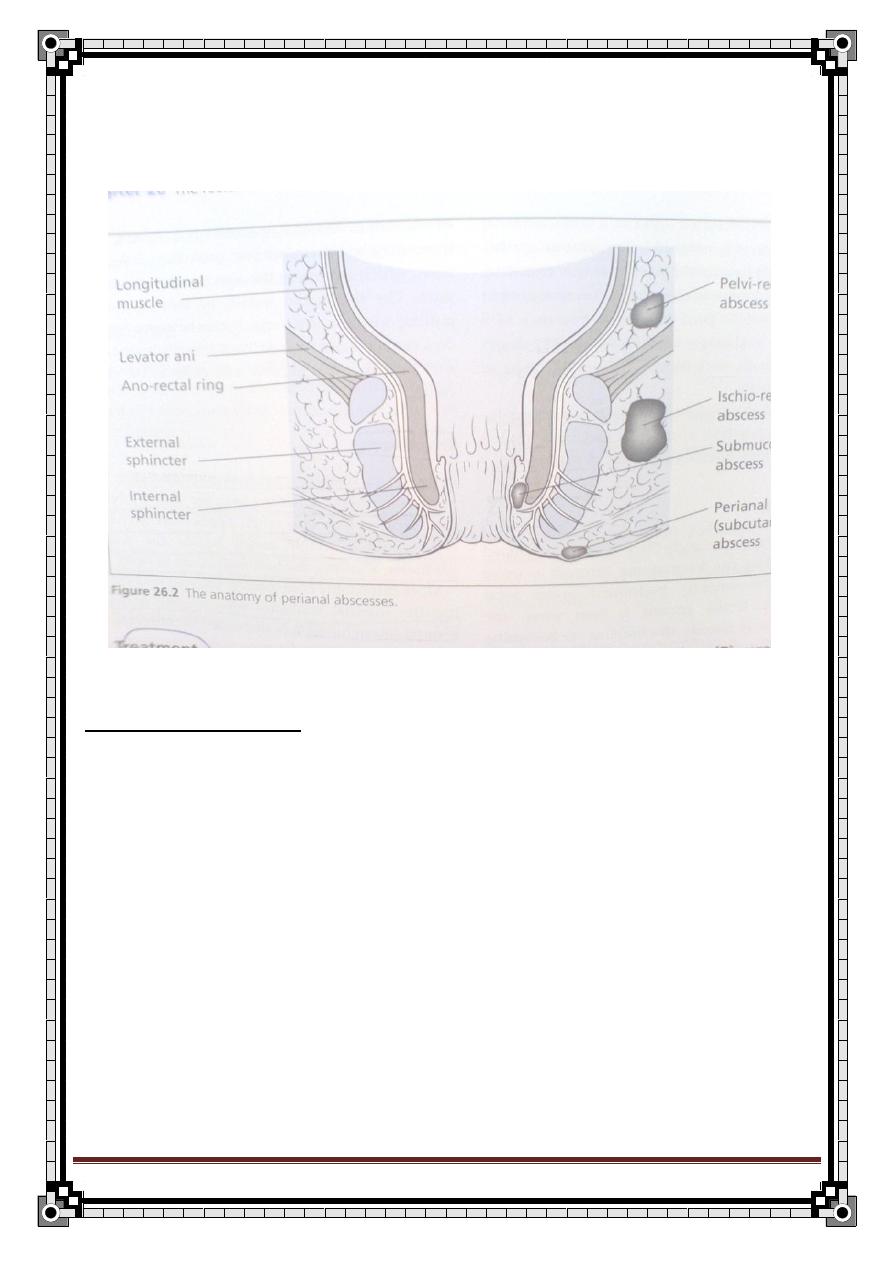
185
" Reading without contemplation is like eating without digestion "
Chinese byword
It is not always possible to decide which sort of an abscess it is, as the
land marks can't be detected.
Abscesses are commonest in patients between 20-50 yrs, but occurs at
any age even in children although rarely.
It is more common in men.
PATHOPHYSIOLOGY:
Infection at anal gland pus either:
1-tracks down to the perineum between the sphincters perianal abscess
2-penetrates the external sphincter to reach the ischiorectal fossa
If the abscess is drained externally or bursts the anal gland is destroyed.
If the abscess continues to secrete a fistula will develop.
186
" Reading without contemplation is like eating without digestion "
Chinese byword
SYMPTOMS AND SIGNS:
1-sever throbbing pain which makes sitting, moving, defecation difficult and is
exacerbated by them all.
2-a tender swelling close to the anus may be felt
3-the general symptoms of abscesses may be present- malaise, loss of
appetite, sweating, rigors.
4-the overlying skin is hot and red and tender
5- it is not possible to define the features of the mass
6- the size is assessed by palpation, the mass is too tender to elicit fluctuation.
7-PR is possible but very painful anesthesia
8- the abscess may bulge into the side of the lower part of the rectum.
9-the inguinal LN are sometimes enlarged and tender.
10- on general exam
1.
tachycardia
2.
pyrexia
3.
sweating
4.
dry furred tongue
5.
foetor oris.
TREATMENT: early surgical drainage to prevent rupture and fistula formation
Abx if immunocompromised, Dm *30% of patients develop it
STRICTURE OF THE ANAL CANAL
CLASSIFICATION:
1-conginital
2-traumatic: as postoperative after too radical excision of the skin and
mucosa in haemorrhoidectomy
3-inflammatory: lymphgranuloma inguinale
–mostly female-, CD, UC
4-post-irradation
5-infiltrating neoplasm
187
" Reading without contemplation is like eating without digestion "
Chinese byword
TREATMENT: depends on the cause and may call for repeated dilatation,
plastic reconstruction, defunctioning colostomy, excision of the rectum if
malignancy is the cause.
PRURITIS ANI
CAUSES:
1- local causes within the rectum or the anus. Any factor that causes
moisture of the area: poor hygiene, sweating, mucous from haemorrhoids,
proctitis, colitis, fistulas.
2- Skin disease: scabies, pediculosis, fungal infection: candida
3-
General diseases associated with pruritis: DM, hodgkin’s lymphoma,
obstructive jaundice.
4- Idiopathic
TREATMENT: according to the cause. The idiopathic group responds to
hydrocortisone ointment and attention to hygiene.
PROLAPSE OF THE RECTUM
1-PARTIAL PROLAPSE:
Confined to the mucosa that prolapses an inch or two from the anal verge.
Palpation of the prolapseno muscular wall in the prolapse.
Happens in infants who are otherwise healthy.
Treatment of these babies requires reassuring the parents as the condition
is self limiting
If happens in adults, it is associated with prolapsed piles or sphincter
incontinence or pruritis ani.
Treatment in adults is to excise the redundant mucosa, or a submucosal
phenol-in- oil injection in order to produce sclerosis.
2-COMPLETE PROLAPSE:
All layers of the rectal wall.
Usually in elderly women that have naturally delivered children.
There is discomfort and incontinence due to the stretching of the
sphincter and the mucous discharge from the prolapsed surface.
188
" Reading without contemplation is like eating without digestion "
Chinese byword
Treatment:
1-Thiersch wire operation where a wire is passed around the anal orifice to
narrow it and reduce the prolapse. OR
2- fixation of the rectum in the pelvic by an abdominal operation
wrapping the rectum in sponge fibrous reaction fixation.
3-
Delorme’s procedure less traumatic perineal approach excision of
the mucosa and bunching of the bowel muscle to form a doughnut-like
ring holds the rectum in the pelvis rather as a ring pessary may control
vaginal prolapse.
PILONIDAL SINUS
PILONIDAL= nest of hairs
It is a sinus that contains a tuft of hairs. However, it can occur without
hairs.
*it is found in the midline skin covering the sacrum and the coccyx.
*they are sometimes also found between the fingers in hairdressers, and in
the umbilicus.
*it is lined by granulation tissue not by skin and there isn’t hairs growing
within it.
* The hairs are short, broken pieces that often come from the scalp.
PATHOPHYSIOLOGY:
While walking, the motion of the buttocks on either side results in hairs
getting sucked into a pre-existing dimple in the skin or actually piercing the
normal skin. Then they act as foreign bodies and cause chronic infection.
The end result is a chronic abscess which contains hair and flares up
frequently into an acute abscess.
*it is rare before puberty and in people over 30 years of age.
*it is a self limiting condition.
*it is more common in men, especially dark haired hirsute men.
189
" Reading without contemplation is like eating without digestion "
Chinese byword
SYMPTOMS AND SIGNS:
Pain and discharge are common when an abscess forms in the tract.
The pain varies from dull aching pain to acute throbbing pain.
The discharge varies from little serum to sudden gush of pus.
An acute abscess may be the first sign of the disease.
In between the acute exacerbations, it produces few symptoms and the
patient may think it has disappeared.
The acute exacerbations happen at irregular intervals.
If the sinus becomes chronic, it may discharge continually.
It could be misdiagnosed as a fistula due to its proximity to the anus.
The sinuses are always at the midline of the natal cleft and lie over the
lowest part of the sacrum and coccyx.
It is very rare for a sinus or an abscess to be closer to the anus then to
the tip of the coccyx.
There could be more than one
Sinuses could have edges that are: epitheliazed edges puckered
scarred edges, granulation tissue if the sinus is discharging.
The skin around the sinus is normal except if it is inflamed.
If the sinus is infected, it is indistinguishable from other SC abscess.
A patient with pilonidal abscess finds some relief from the throbbing pain
by lying prone, in contrast to patients with ano-rectal abscesses who
prefer to lie on their side.
The inguinal LN does not enlarge.
The underlying sacrum, the skin of the perineum the anal canal and the
ischiorectal fossa should be normal.
190
" Reading without contemplation is like eating without digestion "
Chinese byword
Thyroid Gland Diseases
Anatomy:
The gland consist of right & left lobes connected by a narrow isthmus, both
lobes lies on the front & sides of the trachea & larynx at the level of 5
th
-7
th
cervical vertebra and the isthmus overlay the 2
nd
-3
rd
tracheal rings.
I. Blood supply:
a. Arteries:
1.Superior thyroid a. from external carotid a. it runs with external laryngeal
nerve.
2.Inferior thyroid a. from subclavian a. it runs with recurrent laryngeal nerve.
3.Thyroid ima a. (if present it arise from bracheocephalic a. or arch of aorta).
b. Veins:
1. Superior thyroid v. drains to internal jugular vein.
2. Middle thyroid v. drains to internal jugular vein.
3. Inferior thyroid v. into left bracheocephalic v.
II. Lymphatic drainage:
*From Sub capsular pluxes To the juxtathyrid LN( Delphian node)
Paratrachial LN
* Laterally into deep cervical LN. either direct or indirect
*Downward into pretracheal & mediastinal LN.
191
" Reading without contemplation is like eating without digestion "
Chinese byword
Physiology:
The thyroid follicles secretes tri-iodothyronine (T3) & thyroxine (T4).
Synthesis involves combination of iodine with tyrosine group to form mono & di-
iodotyrosine which are coupled to form T3 & T4.
The hormones are stored in the follicles bound to thyrogolbulin.
When hormones released in the blood they are bound to plasma proteins (TBG)
and small amount remains free in the plasma.
The metabolic effects of thyroid hormones are due to the free (unbound)
T3&T4.
90% of the secreted hormones is T4 BUT T3 is the active hormone So, T4 is
converted to T3 peripherally.
Physiological control of secretion:
Synthesis & liberation of T3&T4 is controlled by thyroid stimulating hormone
(TSH) secreted by anterior pituitary gland.
TSH release is in turn controlled by thyrotropin releasing hormone(TRH) from
hypothalamus.
Circulating T3&T4 exert
–ve feedback mechanism on hypothalamus &anterior
pituitary gland.
So, in hyperthyroidism where hormone level in blood is high , TSH production
is suppressed & vice versa.
192
" Reading without contemplation is like eating without digestion "
Chinese byword
Goitre..
Goitre is an enlargement of thyroid gland regardless of its function.
Classification:
1. simple (non toxic):
*simple hyperplastic goitre (colloid).
*multinodular goitre.
2.toxic goitre:
*diffuse (grave’s disease).
*toxic nodule.
*toxic multinodular.
3.inflammatory:
*deQuervain’s thyroiditis (sub acute).
*Riedel’s thyroiditis.
4.autoimmune:
*Hashimoto’s thyroiditis.
5.neoplastic goitre :
*
adenoma (benign).
*papillary Ca (malignant).
*follicular Ca.
193
" Reading without contemplation is like eating without digestion "
Chinese byword
*anaplastic Ca.
*medullary Ca.
Causes:
1.Physiological: puberty& pregnancy.
2.Iodine deficient ( endemic).
3.1ry hyperthyroidism (Grave’s).
4.Adenomatous (nodular) goitre.
5.Thyroiditis.
6.Malignancy.
7.Ingestion of goitregens (phenylbutazone , lithium).
Symptoms of goitre:
1. Lump or swelling in the neck.
Cc: swelling in the anterior lower part of the neck for 2 years duration
The condition start when the pt notice a small swelling in the anterior lower part
of the neck it was painless but cause discomfort during swallowing and
shortness of breath when the neck moved laterally or foreword ,at the previous
one year the swelling gradually get increment in its size and become larger in
size. there is no other swelling in the pt's neck or any other part of his body the
pt think that the lump is due to previous trauma
The pt has increment in appetite but ass. with weight loss.
heat intolerance and sweating , Palpitation, nervousness, irritability, Insomnia
attacks of Depression, Hyperesthesia, Headache ,vertigo, tremors of hands
&tongue also mild diarrhea
194
" Reading without contemplation is like eating without digestion "
Chinese byword
2. Discomfort during swallowing
Large swellings cause tugging sensation in the neck & rarely obstruct the
esophagus. it is not true dysphasia, it is because the thyroid is pulled upward
with the trachea during swallowing.
3. Dyspnea
due to deviation or compression of trachea & the symptoms become worse if
the neck flexed laterally or forward.
If trachea is narrowed, a whistling sound (stridor) can be heard during
inspiration.
4. Pain
Not a common feature of goitre, found in acute & sub acute thyroditis and
Hashimoto’s disease.
*anaplastic Ca can cause local pain & pain referred to the ear if it infiltrate
surrounding structures.
5. Hoarseness
A very significant symptom because it may be caused by a paralysis of one of
the recurrent laryngeal nerve i.e. the lump is a neoplastic Ca invading the nerve.
General symptoms:
Hyperthyroidism
1.Metabolic symptoms:
-increase appetite. - weight loss.
195
" Reading without contemplation is like eating without digestion "
Chinese byword
-heat intolerance. - exx sweating.
2.CVS:
- palpitation. - shortness of breath on exertion.
- extra systole & Atrial fibrillation.
- tiredness.
*CVS symptoms are often the presenting symptoms of 2ry thyrotoxicosis.
3.Neurological:
1) nervousness
2) irritability.
3) insomnia
4) depression.
5) Hyperesthesia
6) headache
7) vertigo.
8) tremors of hands &tongue.
4. GIT:
mild diarrhea.
5.Others..
- oligomenorrhea/ amenorrhea.
- wasting& weakness of small muscles of hand, shoulder& face.
Hypothyroidism
1.Metabolic symptoms:
Tiredness & weakness.
196
" Reading without contemplation is like eating without digestion "
Chinese byword
Physical & mental lethargy.
Always feels cold (pt like hot weather & dislike cold weather).
Wight gain but poor appetite.
2.CVS:
Breathlessness and ankle swelling indicate the onset of heart failure due to
myxoedematous infiltration of the heart.
3. Neurological :
Slow & unclear thoughts, speech, action.
Deep, hoarse voice.
Hallucination, dementia (myxoedema madness).
Carpal tunnel syndrome.
4.Others..
- Anemia. - Menorrhagia.
- Constipation. -
↓sweating.
Neck examination:
1- exposure up to the nipple
2- sitting position
I. inspection:
General inspection
Distended neck veins may indicate retrosternal extension
From the front:
1- visible lump
197
" Reading without contemplation is like eating without digestion "
Chinese byword
a- 4S
Site
Size
Shape (Irregular, oval ,spherical)
State of over lining skin ( redness ,discharge or Scar)
b- ask the Pt. 3 things
1-to swallow if thyroid it will move except
neoplasm
riedl's thyroiditis
scar
2-to protrude his tongue if it does it is a thyroglossal cyst
3- to elevate his hand pemberton's sign => retrosternal goitre Pemberton’s
sign when the patient lifts both arms as high as possible, venous congestion of
the face & neck occurs after a few minutes if a retrosternal goitre is present.
II. Palpation:
From front:
3T
Tracheal displacement
Tenderness = thyroiditis
Temperature hot = inflammation
From behind:
1) surface (smooth/bosselated (nodular)
198
" Reading without contemplation is like eating without digestion "
Chinese byword
2) Edge (lower edge)(Ask the pt to swallow)
3) Consistency
4) Thrill
5) Attachment to over lying skin or under lying muscles
6) Attachment to deep muscles & Mobility
7) Carotid pulsation (berry's sign)
8) Lymph nodes : pretrachial LN
III. Percussion:
Percuss the manubrium
along the clavicles
over the sternum
upper chest from one side to the other for dullness indicating a retrosternal
extension.
IV. Auscultation:
A systolic bruit may be heard over each lobe in thyrotoxicosis.
Specially superior lobe Because superior thyroid artery pass superficial
General examination:
Pay particular attention to the cardiovascular &nervous systems for any
evidence of hyper or hypothyroidism.
Signs of hyperthyroidism:
1. In the neck:
Thyrotoxicosis can be present with out any enlargement of the gland..
Enlargement can be diffuse, nodular, or tender depending on the cause.
199
" Reading without contemplation is like eating without digestion "
Chinese byword
A diffusely enlarged hyperemic gland usually has a systolic bruit, audible over
the lobes.
2. In the eyes:
a- lid retraction:
due to over activity of the involuntary part of levator palpebrae superioris
muscle.
The upper lid is raised, lower lid is normal.
Stellwag's sign
b- lid lag:
the upper lid lags behind the moving down eyeball while the head is fixed (the
upper lid does not keep pace with the eyeball as it follows a finger moving from
above downwards).
c- exophthalmos:
the eyeball is pushed forwards by an increase in retro orbital fat, edema &
cellular infiltration.
Sclera become visible below the lower edge of the iris(the inferior limbus) or
both lids moved away from the center with sclera visible all around.
Patient can look up without wrinkling the forehead 1-
( Joffrey’s sign).
Patient has difficulty in converging 2-( Moebios sign)
**normally, the upper lid rest halfway between pupil and the superior limbus of
iris.
3-Naffziger's sign
d- ophthalmoplegia:
the cause of the weakness of ocular muscle is edema & cellular infiltration of
the muscles themselves& of the oculomotor nerves.
The muscles mostly affected are the superior and lateral rectus and inferior
oblique.
Paralysis of these muscles prevents patient from looking upwards &outwards.
200
" Reading without contemplation is like eating without digestion "
Chinese byword
e- chemosis:
it is edema of the conjunctiva which become thickened, crinkled, edematous
and slightly opaque.
Caused by the obstruction of normal venous& lymphatic drainage of the
conjunctiva by the increased retro-orbital pressure.
3. Metabolic signs:
Patient looks thin and their face hands may be wasted.
They may look hot and be sweating, even in cold room.
4. CVS:
- tachycardia of 90 beats/min persist during sleep.
- pulse is irregular if there is exrasystole or atrial fibrillation.
- there may be rales at the bases of the lungs & edema of the ankles if heart
failure developed.
5. Neurological:
Patient looks worried, nervous & agitated.
Fine tremor demonstrated when they stretch out their hands with their fingers
spread, also present in protruded tongue.
6. Musculoskeletal:
The muscles of the hands ,shoulders and face may be wasted & weak and the
finger tips enlarged (thyroid acropathy/ clubbing).
7. Skin:
Pretibial myxoedema : red, blotchy, raised areas seen over the shins in patients
with grave’s caused by deposits of myxoid tissue within the skin.
8-Hand signs
1) Hot
2) Moist
3) Palmer erythema
4) Atrophy of the muscles
201
" Reading without contemplation is like eating without digestion "
Chinese byword
5) Chek the Pulse (incease)
6) Reflexes( hyperreflexia )
7) Tremor
8) Clubbing
9) Nail changes
9- legs
1) Clubbing
2) Pretepial myxedema
3) Reflexes
4) Atrophy
Then examine for myopathy
hypothyroidism
1.In the neck:
In many cases the neck is normal..
2.In the eyes:
The eye is normal.
The eye lid
is swollen &heavy → periorbital puffiness (edema).
The hair in the lateral ⅓ of the eyebrows falls out.
3.General signs:
Dry, coarse skin & thin hair. In white skinned pt the skin is smooth & pale while
the cheeks are often slightly flushed resemble peaches & cream.
The skin is dry, inelastic and does not sweat. it looks edematous but does not
pit after prolonged pressure.
The patient is overweight with exx CT &fat in the supraclavicular fossae, across
the back of the neck and over the shoulders.
The hands are puffy & spade like.
The tongue enl
arges →interfere with articulation of the words.
202
" Reading without contemplation is like eating without digestion "
Chinese byword
4.CVS:
The pulse rate is slow (40-60 beats/ minutes).
Blood pressure is low.
* these changes reversed if heart failure develops.
The hands are cold & the finger tips blue.
5. Neurological :
Mental alertness and the ability to respond to questions are retarded.
Slow deliberate movements (Brady kinesis).
Refluxes are sluggish with slow recovery phase (hang up refluxes).
Investigations:
1.serum free T3&T4:
T4 level will usually establish whether the gland is overactive or not. Elevation
suggest hyperthyroidism.
2.serum TSH: (most sensitive)
Raised in hypothyroidism (myxoedema), suppressed in hyperthyroidism where
the gland secrets T4 autonomously.
It is used with TRH level to determine the level of failure of production of thyroid
hormones.
3.serum LATS:
The presence of LATS is a diagnostic of Grave’s disease.
203
" Reading without contemplation is like eating without digestion "
Chinese byword
LATS: long acting thyroid stimulating factor, it is an IgG and they activate TSH
receptors on follicular membrane & has much longer t1/2 in circulation then
TSH.
4.thyroid antibodies:
Like anti-thyroglobulin & anti-mitochondrial antibodies which indicate
autoimmune etiology e.g. Hashimoto’s or Grave’s disease.
5.Isotope scan:
By I¹³¹ or technetium. The injected isotope is taken by
*thyroid gland & distributed uniformly in a normal thyroid.
*a nodule in the thyroid gland that is hyper active so called hot nodule.
A nodule that is not producing T4 will not take up the isotope (hypoactive) it is
called cold nodule & it indicates a cyst or tumor.
6. Ultrasound:
To know if the lump is cystic or solid & the general shape &outline of the gland.
7.fine needle aspiration cytology:
It is the principal investigation for all solitary nodules.
8.plain X-ray of the chest & thoracic inlet:
Determine if there is tracheal displacement & compression.
To see if there is a retrosternal extension of the gland.
9. excision biopsy with frozen section
Alternative way for FNA.
10.ECG:
204
" Reading without contemplation is like eating without digestion "
Chinese byword
In hypothyroidism: low electrical activity with small complexes.
In hyperthyroidism: to confirm atrial fibrillation.
11.serum cholesterol:
Usually raised in hypo &normal or slightly low in hyperthyroidism.
Clinically:
Patient with goitre either is :
Euthyroid.
Hyperthyroidism(thyrotoxicosis).
Hypothyroidism (myxoedema/ cretinism).
Euthyroidism..
Causes:
1.Physiological e.g. puberty, pregnancy where there is increase in demand.
2.Iodine deficiency (endemic).
Hypothyroidism..
Causes:
1.With goitre..
*Chronic lymphocytic thyroiditis (
Hashimoto’s).
*Drugs e.g. lithium, amiodarone, iodide.
*Iodine deficiency.
205
" Reading without contemplation is like eating without digestion "
Chinese byword
2.Without goitre..
*idiopathic atrophy.
*after thyroidectomy.
*after radio active therapy I¹³¹.
*thyroid agenesis.
*pituitary disease (2ry) ↓TSH.
*hypothalamic disease (3ry) ↓TRH.
Investigations:
Thyroid function test:
-
↓T3,T4.
-
↑TSH (except in pituitary failure)
-
in case of autoimmune disease → ↑ titer of anti-thyroid antibodies.
Treatment:
Oral thyroxin (0.1- 0.2) as a single daily dose.
Hyperthyroidism..
Causes:
1. exogenous causes:
Exx thyroid hormone ingestion.
2.pituitary causes:
pituitary adenoma.
3.thyroid causes:
Grave’s disease(exx stimulation of thyroid).
Sub acute thyroiditis (exx release hormone).
4.iodine deficiency.
206
" Reading without contemplation is like eating without digestion "
Chinese byword
Investigation:
1. Ultrasound:
Defined the shape & outlines of the gland.
2. X-ray:
Of the chest& thoracic inlet.
3. serum test:
↑T3,T4
↓TSH
LATS
(diagnostic for grave’s disease)
4. Isotope scanning..
5. FNA..
Treatment:
1.antithyroid:
a. carbimazole: (15 t.d.s)
-patient should remain on a maintenance dose up to 2 years
-SE: joint pain, skin rash, fever, agranulocytosis.
b. propylthiouracil :
(300-600mg/day).
c. propranolol : (symptomatic treatment)
2. radioactive iodine:
-I¹³¹ is given orally, it takes 8-12 weeks before pt becomes euthyroid so,
antithyroid drugs are given during this period.
-It is appropriate for middle aged pt who
failed with medical ttt & can’t do the
operation.
-Most of the pt will develop hypothyroidism later on.
-It is contraindicated in pregnancy & childhood.
207
" Reading without contemplation is like eating without digestion "
Chinese byword
3. surgery:
Indications:
a. failure of medical ttt.
b. drug sensitivity in young pt.
c. large goitre with compression symptoms.
d. malignancy.
e. cosmetic.
Preoperative preparation:
-Pt should become euthyroid before surgery to prevent thyroid crisis.
-assessment of vocal cords condition(direct laryngoscope).
Operations:
-
solitary bengin nodule → lobectomy.
-
cancer → total thyroidectomy.
-
thyrotoxicosis → subtotal thyroidectomy.
Complications:
1.hemorrhage/hematoma..
In the first 24hrs post operation.
2.recurrent laryngeal nerve damage..
-
if unilateral → hoarseness.
-
if bilateral → air way obstruction & emergency tracheostomy is required in 2-3
%.
3.superior laryngeal nerve damage..
Low pitch voice &inability to make explosive sounds.
Usually transient.
208
" Reading without contemplation is like eating without digestion "
Chinese byword
4. hypoparathyroidism..
- may lead to tetany.
- within the 1
st
week of surgery.
- manifested by tingling sensation& carpopedal spasm.
- symptoms relieved by injection of Ca+2.
5. hypothyroidism..
- in 15%of cases.
- ttt is by hormonal replacement therapy.
6. thyroid storm..
- Very rare nowadays due to preoperative care
- pt may have pyrexia, agitation, exx sweating, tachycardia& atrial fibrillation.
- ttt is by rapid administration of:
*antithyroid drugs.
*IV fluid.
*cooling for pyrexia.
*barbiturate.
*digoxin.
7.wound infection.
8.recurrent thyrotoxicosis.
9.keloid scar.
209
" Reading without contemplation is like eating without digestion "
Chinese byword
Different forms of goitre
…
1.simple hyperplastic goitre..
Caused by exx stimulation by TSH which is stimulated by low level of circulating
level of thyroid hormones e.g.
- relative iodine deficiency is the commonest pathological cause.
- pregnancy &puberty (physiological states require increased activity of thyroid
gland).
History:
-In endemic areas it appears in childhood.
-Sporadic physiological hyperplasa appeas in puberty& early adult life.
-Common in area with low iodine content in the drinking water.
-It is 5 times more common in women than in men.
-an exx dietary intake of goitreogen e.g. cabbage can cause goitre by interfering
with hormone synthesis.
Symptoms:
Locally:
- swelling in the neck that appears slowly without pain.
- if it enlarged it may cause pressure symptoms such as Dyspnea, venous
engorgement, and mild discomfort during swallowing.
Generally:
- pt usually euthyroid.
- long standing simple colloid goitre often becomes nodular goitre &
occasionally 2ry thyrotoxicosis (Plummer’s syndrome) or myxoedema may
develop.
210
" Reading without contemplation is like eating without digestion "
Chinese byword
Signs:
* neck examination..
- the swelling occupies the anatomical site of the gland.
- not tender.
-has 2 lobes &isthmus.
- 2-3 larger than a normal gland.
- surface is smooth, if it turns colloid, surface become nodular.
- feels firm and dull to percussion.
-the gland moves upon swallowing.
-LN& eyes are normal.
Treatment:
- addition of iodine to diet (iodized salt).
- thyroxin to suppress TSH.
-Partial thyroidectomy if the gland very large& causing pressure effects.
N.B. in late stage when the acini are distended by colloid it is called colloid
goitre.
2. Multinodular goitre..
- it develops spontaneously and in glands subjected to prolonged stimulation i.e.
hyperplastic gland.
- it could be endemic( in I def. areas) or sporadic.
-it results from disorganized response to stimulation and contains areas of
hyperplasia & areas of hypoplasia.
- when the nodules are hyperplastic the pt may develop 2ry thyrotoxicosis.
211
" Reading without contemplation is like eating without digestion "
Chinese byword
- in long standing nodular goitre, most of the nodules becomes inactive so,
hormone production is inadequate and myxoedema develops.
History:
Age:
-Endemic(15-30years).
-Sporadic(25-40 years).
-
♀:♂ = 6:1.
Symptoms:
-The commonest presenting symptoms is enlarging painless swelling which
may cause stridor and other pressure symptoms.
- Sudden enlargement and pain occur if there is hemorrhage into necrotic
nodule
- Thyrotoxicosis occur in25%of pt with long standing nodular goitre.
Signs on examination:
-
The swelling in the lower ⅓ of the neck.
- only tender if there is recent hge .
- usually asymmetrical, nodules in the isthmus are prominent , may extend
below the clavicles and the sternal notch, into the superior mediastinum.
- surface is smooth but nodular. Frequently only one nodule is palpable
(dominant nodule).
-
the composition varies some feel hard, others feel soft. The nodules don’t
fluctuate or transilluminate and are dull to percussion.
- moves with swallowing .
- LN and eyes are normal.
- trachea may be compressed or deviated (bilateral nodules will compress the
trachea into a narrow slit, causing Dyspnea and stridor especially during lateral
flexion of the neck. Large unilateral nodules will push the trachea laterally).
212
" Reading without contemplation is like eating without digestion "
Chinese byword
- there may be signs of thyrotoxicosis especially the cardiovascular signs.
- it is unusual to get neurological signs or eye changes with 2ry thyrotoxicosis
associated with nodular goitre. These systems are affected more often in 1ry
thyrotoxicosis.
Treatment:
- if the pt is clinically euthyroid & the goitre is small, no ttt is required.
- if the goitre is large & cause symptoms of compression or if thyrotoxicosis
occur, partial thyroidectomy is indicated.
3.Solitary nodule..
-Although only one nodule is palpable, approximately ½ of the pts who present
with a solitary nodule actually have a Multinodular goitre i.e. a clinically
dominant nodule in a macroscopical Multinodular goitre.
- majority are benign but all have to be differentiated from Carcinoma by FNA.
- thyrotoxicosis is rare to occur.
Causes:
a. dominant nodule in a multinodular goitre.
b. hemorrhage into a nodule or necrosis of hyperplastic nodule.
c. adenoma.
d. carcinoma (papillary or follicular).
e. enlargeme
nt of the whole of one lobe(usually Hashimoto’s disease).
213
" Reading without contemplation is like eating without digestion "
Chinese byword
4. Diffuse toxic goitre
..(Grave’s)
-Diffuse vascular goitre, appearing at the same time with the symptoms of
hyperthyroidism.
-
Usually occur in young ♀& associated frequently with eye signs.
-Thyroid stimulating antibodies (TSAB) stimulate TSH receptors causing
hypertrophy & hyperplasia.
-Signs &symptoms are same as for pt with thyrotoxicosis.
5. Toxic Multinodular goitre..
-Not all the nodules are active.
-There are several nodules functioning independently of TSH stimulation.
-Signs &symptoms are like thyrotoxicosis.
-Isotope scan shows cold& hot nodules.
-Rarely associated with eye symptoms.
-Affects middle age and elderly.
6.Toxic nodule..
-A solitary over active nodule, which may be a part of generalized nodularity or
a true toxic adenoma.
-It is called autonomous toxic nodule.
-
It’s hypertrophy & hyperplasia are not due to TSAB.
214
" Reading without contemplation is like eating without digestion "
Chinese byword
Thyrotoxicosis Examination…
1.general appearance..
- wt. loss.
– anxiety.
-restless.
– sweating.
2.hands..
-pulse(tachycardia, bounding/collapsing pulse, atrial fibrillation).
-moisture.
– fine tremor.
-palmar erythema.
– onycholysis.
-warmth.
– clubbing (thyroid acropathy).
3.arms..
-proximal myopathy. - exaggerated reflexes.
4.eyes..
-lid retraction.
– lid lag.
-exophthalmus(pt looks upward without wrinkling /difficult converging).
-ophthalmoplegia.
– chemosis.
5.chest..
-gynecomastia.
– murmur. -signs of CHF.
6.abdomen..
-splenomegally.
7.legs..
- pretibial myxoedema: red, thickened swelling above the lateral malleoli, which
progress to thickened non pitting edema of the feet.
*test for proximal myopathy & hyper reflexia in the legs.
215
" Reading without contemplation is like eating without digestion "
Chinese byword
8.Neck..
Inspection:
-swelling.
-movement of the swelling(tongue protrusion/swallowing).
-scars of surgery. -
pemberton’s sign.
Palpation:
-the gland(site, size, shape, surface, tenderness, temperature, thrill,
consistency, relation to surrounding tissue)
-Lymph nodes.
– tracheal deviation. -carotid arteries.
Percussion:
- retrosternal extension.
Auscultation:
- bruit over the thyroid &carotid arteries.
216
" Reading without contemplation is like eating without digestion "
Chinese byword
Correlation between clinical state of the thyroid gland, endocrine
function and pathological diagnosis:
Hyperthyroidism
Euthyroidism
Hypothyroidism
- 1ry
hyperthyroidism
(Grave’s disease)
-I deficiency.
-enzyme defects
-goitrogen
-thyroiditis
-amyloid
-physiological
Pregnancy/puperty
- thyroiditis
Diffuse
enlargement
- 2ry
hyperthyroidism
(Plummer’s
syndrome)
-multinodular goitre
-lymphoma
-anaplastic Ca
-medullary Ca
- Multinodular
goitre with gross
degeneration
Multinodular
enlargement
- autonomous
toxic nodule
-cyst
-dominant nodule
-adenoma
-follicular or papillary
Carcinoma
-coincidental
nodule with
myxoedema
Solitary
nodule
- 1ry
hyperthyroidism
- thyroxin
overdose
-normal gland
-thyroiditis
-1ry myxodema
-post
thyroidectomy
-post radioactive
iodine
No palpable
goitre
217
" Reading without contemplation is like eating without digestion "
Chinese byword
Breast diseases
Anatomy of breast
Blood supply:
- medial mammary branches of perforating branches and anterior intercostals
branches of the internal thoracic artery, originating from subclavian artery.
- lateral thoracic and thoracoacromial arteries, branches of the axillary artery.
- posterior intercostals arteries, branches of the thoracic artery in the second,
third and 4
th
intercostals space.
Venous drainage
Mainly to the axillary vein but there is some drainage to internal thoracic vein.
Lymphatic drainage
Lymph passes from the nipple, areola and lobule to the subareolar lymphatic
plexus .
Then from subareolar plexus:
Most lymph (>75%) especially from the lateral quadrant of the breast, drain to
the axillary lymph node, initially to the pectoral ( anterior) node.
Most of the remaining lymph especially from the medial quadrant, drain to the
parasternal node.
218
" Reading without contemplation is like eating without digestion "
Chinese byword
Lymph from the axillary node drain into infraclavicular and supraclavicular node
and from them into subclavian lymphatic trunk.
Lymph from parasternal nodes drain into bronchomediastinal trunk.
These 2 trunks + jugular lymphatic trunk form right lymphatic duct on the right
side, or entering the termination of the thoracic duct on the left. Then open into
the junction of the internal jugular and subclavian vein.
N.B. skin of the breast ( exept the nipple and areola which drained by
subareolar node ) drain into the axillary, inferior deep cervical, infraclavicular
and also parasternal nodes of both sides.
in sagittal suction :
- the breast composed of glandular tissue and fat.
Its secretions draining on to the surface of the nipple through 5-7 main duct
orifice.
The primary secreting unit is a group of secular alveoli draining into a ductile.
The alveoli and ducts are lined by single layer of epithelial cells.
The shape of the female breast is due to fat containing within fibrous septa,
and not to the glandular tissue.
Presentation of breast disease:
Breast disease present in 3 main ways:
-lump, which may or may not be painful
-pain
-Nipple discharge or change in appearance.
219
" Reading without contemplation is like eating without digestion "
Chinese byword
1-Lump
Painful lump
d.dx;
fibroadenosis ( common)
matitis ( redness )
absecess ( usually
postpartum or lactational)
cyst and rarely carcinoma
questions to ask:
Q1: is it associated with
menstrual period or not?
Q2: is the female
lactating?
Q3; is it associated with
redness, sweeling or
itching?
Painless lump
d.dx:
fibroadenoma ( breast mouse)
beast cancer
cyst and some times adenosis
questions to ask:
Q1; Is it mobile or fixed?
Q2: is there any nipple
changes?
Q3: dose the patient have back
pain or headache?
( carcinoma)
2-pain and tenderness without lump
DDX:
cyclical breast pain
non cyclical breast pain
very rarely carcinoma
220
" Reading without contemplation is like eating without digestion "
Chinese byword
3- nipple discharges;
a- red, pink or clear pale yellow >>> duct papilloma or
carcinoma or duct ectasia.
b- brown, green or black >>>> duct ectasia or cyst
c- creamy white yellow >>>> duct ectasia or lactation
questions to ask;
Q1; is it come spontaneously?
Q2; is it unilateral ?
Is it persistence?
Is the female lactating or not?
4- nipple changes:
Duct ectasia
Carcinoma
Paget disease
Eczema
5- change in breast size
Pregnancy
Carcinoma
Benign hypertrophy
Rare large tumor
If you have breast case, you have to
cover all these symptoms.
221
" Reading without contemplation is like eating without digestion "
Chinese byword
Examination of breast
The patient must be fully undressed to the waist, resting comfortably on an
examination couch with her body raised at 45 degree to the leg. This position is
the best compromise between lying flat , which makes the breasts full sideways,
and sitting upright, which makes the breasts pendulous.
Ask the patient to slowly raise her arms above her head>>>> skin change may
then become more apparent, particularly tethering to the skin.
Ask the patient to press her hand against her hip to tense pectoral muscle.
- inspection
Inspect area from clavicle upward to the 6
th
intercostals space downward, and
from midline to anterior axillary line.
Do not forget, inspect the axillae, arm and supraclavicular area for dilated vein
or LN enlargement.
You have to inspect:
1-breast size
2-Symmetry
3-skin:
3 - the skin
- Peau, d orange, ( there may be edema caused by
obstruction of skin lymphatics by cancer cells, which mark the opening of hair
follicle and sweat glands result in orange - peel appearance).
Look for any visible scar ,dilated veins, tethering
may be fixed by underlying cancer.
222
" Reading without contemplation is like eating without digestion "
Chinese byword
4-Nipples and areola
The color of the nipple change with age, and there is darkening during
pregnancy.
Nipple inversion or eczematous changes.
Duplication: accessory nipple
Palpation:
Palpate with flat of the fingers and not with the palm of the hands.
If you find a lump, ascertain its site, size, shape…………etc
For example: there is a lump in left upper outer
quadrant, 2*3cm, spherical, smooth not Fixed to skin, not tender…..etc
You have to palpate the axillae, and axillary lymph node.
***Normal breast is firm, fibrous and easily palpable nodule.
**There is different between skin fixed and tethering
If a lump can not be moved without moving the skin, it is fixed.
If a lump can move independently, it is skin tethering.
A tethering lesion is one which is more deeply situated.
Triple assessment:
1-history and examination
2- diagnostic imaging ( US <30 and mammogram >30 ) >>> important for
screening.
3- cytology or histology ( fine needle aspiration FNA) >>> Most reliable.
223
" Reading without contemplation is like eating without digestion "
Chinese byword
Breast disease:
Breast carcinoma
cancer of the breast is an adenocarcinoma and the commonest cancer in
women.
The cut surface of a carcinoma is classically concave, gritty and pale grey
with prominent yellow and white flecks.
Etiology
:
1-genetic factors;
**Family history >>>>> premenopausal first-degree relative with breast
cancer confers a lifetime risk of 25%, which reduce to 14% if the same
relative is postmenopausal.
If both mother and sister develop premenopausal BC, the risk is 33%.
**Gene carriage >>> BRCA1 AND BRCA2 ( AUTOSOMAL DOMINENT)
present in 80-90% of the cases.
An individual whose mother carries a mutation in one of these genes has a
50% chance of inheriting that mutation, which will confer a lifetime risk of 80-
90%.
The presence of mutation in BRCA1 also increase risk of ovarian cancer.
2- hormonal factors:
Gender>>>> women are 100 times more likely to have BC than men.
Menarche and menopause>>>> early menarche and late menopause are
associated with high risk.
224
" Reading without contemplation is like eating without digestion "
Chinese byword
Parity >>> nulliparous and late age at first pregnancy (35yr) have high risk.
Hormonal replacement therapy also slightly increase the risk.
3- benign breast disease ( lobular or ductular hyperplasia) increase the risk
of 4-5 times.
4- radiation exposure in adolescences or early childhood increase the risk.
The commonest type of BC (85%) is invasive ductal carcinoma or (no
special type NST).
SPREAD:
1- direct extension to skin >>>> skin dimpling and nipple retraction
2- by lymphatic >>> blockage of lymphatic >>> edema >>>
pea, d orange.
The main lymph channels pass directly to the axillary and internal thoracic
LN. later spread to the supraclavicular, abdominal, mediastinal, groin and
opposite axillary node.
3- blood >>>> to lung, liver, brain and bone.
Prognostic factors:
1- axillary node status >>>> the greater the number of ipsilateral node>>>
the worse the prognosis.
2- tumor grade ( histology)
Well differentiated(1), poor differentiated(2) or plemorphic (3).
3- tumor size >>>> large size more prone to metasis.
225
" Reading without contemplation is like eating without digestion "
Chinese byword
NPI (Nottingham prognostic index):
The above 3 prognostic factors combined to form a prognostic index which
allocate patient to 5 different groups with variable 10 yr survival rate.
The NPI is calculated as follows:
0.2* DIAMETER+ GRADE+ NODAL STATUS.
(see table 35-1 lecture note)
TNM classification:
T >>>> TUMOR
T IS >>> CARCINOMA IN SITU
T0 >>>> no primary tumor located
T 1 >>>> tumor less than 2 cm >>>> 80% 5 year survival
T2 >>>> tumor 2-5 cm >>>> 50% 5 year survival
T3 >>>> tumor more than 5 cm >>>> 15% 5 year survival
T4 >>>> extension to chest wall >>>> 5% 5year survival
N >>>> NODE
N1 >>>>> no palpable axillary node
N2 >>>> MOBILE palpable axillary node
N3 >>>>> palpable supraclavicular nodes.
M >>>> metasis
M0>>>> no metasis
M1 >>>> distance metasis
226
" Reading without contemplation is like eating without digestion "
Chinese byword
History of breast carcinoma;
Age>>> rare in teenager and 20.
from 30 onward there is progressively increase incidence to which peak in
late 50.
Clinical pictures:
1-Majority of patients with invasive BC have painless lump.
2-Other features are nipple changes, blood stained nipple discharge and
unilateral nipple eczema (paget disease).
3-The nipple may become retracted, or even destroyed.
4-Swelling of the arm, caused by lymphatic or venous obstruction in the
axilla.
5-Backache, caused by secondary infiltration and collapse of lumbar
vertebrae, with nerve root pain radiating down the back of legs, is a common
symptoms of advanced disseminated disease.
6-Cerebral metaplasia may cause a fit.
7-Pathological fracture may be the first indication of the presence of the
disease.
The general symptoms commonly associated with cancer, such as malaise,
weight loss and cachexia, are rare in patient with breast cancer. Even those
with disseminated fatal disease usually feel well in themselves until the final
stages.
227
" Reading without contemplation is like eating without digestion "
Chinese byword
Examination;
Site; half of carcinomata of the breast occur in upper outer quadrant, which
include the axillary tail.
Colour:
If the tumor is close to the surface, the overlying skin may be discolored.
Tumor fixed to the skin first give the skin a smooth, redness appearance, but
as the process advance and ulceration is imminent, the skin becomes paler.
Tenderness: most carcinomata are not tender, but palbation may produce
mild discomfort.
Temperature: only the very rare ' inflammatory type' of breast carcinoma feel
warm.
Shape; in early stages, it is roughly spherical.
Surface: the surface is usually indistinict, which makes it difficult to define the
shape. Few cancer are encapsulated and have smmoth surface, mimicking
cysts and fibroadenoma.
Composition: carcinomas are solid, so they do not fluctuate, transilluminte or
have a fluid thrill.
Their consistency is normally quit firm.
Some are soft as a lipoma.
Fixation of a lump to the skin is almost diagnostic of a carcinoma. The only
other condition producing fixation is traumatic fat necrosis or pointing
abscess.
228
" Reading without contemplation is like eating without digestion "
Chinese byword
Peau d, orange ( already mentioned)
Lymph gland containing metastases are usually hard and discrete. Ulceration
in the axilla is rare.
General examination:
Essential to detect the metastasis;
The skeleton; especially the lumbar spine, causing back pain and reduced
spinal movements.
The lung: plural effusion, lung parenchyma, in the form of diffuse lymphatic
involvement known as lymphangitis carcinomatosa, may cause severe
dyspnea.
The liver; making it palpable and causing jaundice and ascities.
The skin; producing multiple hard nodules within the skin.
Condition mimicking breast cancer;
1-Fat necrosis; fat necrosis occur in the elderly after an injury or trauma.
There may be focal necrosis of subcutaneous fat with local scaring which
causes skin tethering.
2-Mondor,s disease; it is thrombophlebitis of the lateral thoracic vein which
produce a cord like, linear skin puckering. It rexsolve spontaneously.
Treatment;
Early breast cancer:
1- wide local excision >>> removal of the lump with margin of normal breast.
2- simple mastectomy involve excising the breast tissue ( it usually combined
with reconstructive surgery) + axillary node clearance. By this combination
we avoid the needs of postoperative radiotherapy in most cases.
3- adjuvnt therapy;
229
" Reading without contemplation is like eating without digestion "
Chinese byword
Pt. with early BC should be considered for chemotherapy with or without
antiestrogen (tamoxifin).
Antiestrogen therapy should be given only in females who have estrogen
receptors are positive.
In Stage 4 ( palittation)
1- local radiotherapy for fungation
2- radiotherapy to bone metastasis.
3- aspiration of pleural effusion.
4- tamoxifine
5- chemotherapy.
N.B. patients with bone metastasis>>> hormonal therapy is better than
chemotherapy.
While patients with liver metastasis>>> chemotherapy is better.
Complication of mastectomy:
1- wound seroma
2- stiffness of the shoulder
3- lymphedema of the arm.
4- psychological.
the cardinal signs of a late cancer of breast:
1- hard, non tender, irregular lump.
2- tethering or fixation of lump
3- palpable axillary lymph gland.
230
" Reading without contemplation is like eating without digestion "
Chinese byword
Benign breast tumor
1- fibroadenoma ( breast mouse):
The commonest breast tumor in young women.
A fibroadenoma is a benign neoplasm of the breast in which fibromatous
element is the dominant feature.
There are 2 histological varieties of fibroadenomata, pericanalicular, which
mainly consist of fibrous tissue, and intracanlicular, which contain more glands.
Most fibroadenomata present in young women, age between 15 and late 20.
History:
The patient present with painless lump, that it is highly mobile.
Examination:
Will demarcated, spherical, painless, smooth, firm swelling that can present
anywhere in the breast.
It is the most mobile of all breast lesions.
Deferential diagnosis:
Breast cyst, but cysts are found in a different age group and are not usually
mobile.
all fibroadenoma must be investigated by triple assessment.
The largest lump should undergo core biopsy.
Surgery should be avoidable in the majority of cases but should be considered
in the following circumstances;
1- lump increase in size
2- symptomatic lump- pain or tenderness
3- patient preference.
231
" Reading without contemplation is like eating without digestion "
Chinese byword
Phylloides tumor ( cystsarcoma phyllodes or brodie tumor):
This is rare, large and massive, irregular, bosselated tumor that dose not
metastasis. LN enlargement is rare.
It present as a slow- growing, smooth swelling in the middle age>40.
It can be big enough to cause skin necrosis.
Treatment:
Removal of the tumor with a wide margin of normal breast.
If massive tumor>>>> total mastectomy with axillary node sampling.
Intraduct papilloma:
This due to hyperplasia of the duct epethelia lining.
Predispose to malignant >>>> ductal carcinoma- in situ.
It is the only benign breast disease that may lead to malignancy.
The most common cause of Bleeding from nipple.
Papilloma can be felt as a small nodule at the areolar margin, pressure at that
point >>> discharge.
Treatment:
Surgical excision of the involved duct.
Lipoma of the breast:
Lipoma may occur anywhere in the body where there is fat, which include the
breast, both SC and more deeply seated between the lobule.
232
" Reading without contemplation is like eating without digestion "
Chinese byword
Lumps and nodularity:
The symptoms of lumps and nodularity occur during the years of ovarian
activity, from early menarche to menopause, beginning in the early 20 and
reaching the peak in the 30.
Symptoms:
Pt. present with more than 1 lump in the breast which are commonly tender.
The pain is Intermittent related to menstrual cycle, mostly in premenstrual
phase and resolving when the menses begin.
On examination:
Benign breast lump vary from a diffuse nodularity to quite discrete lesion.
Nodular lumps tend to be in the upper outer quadrants and have moderate
hardness, sometimes describe as rubbery.
They are not fixed or tethered to skin or muscle.
Breast pain;
Cyclical breast pain
Non- cyclical breast pain
1- cyclical breast pain:
Cyclical breast pain is very common.
It comes on during the second half of the cycle.
It is quite commonly unilateral, it may be felt through out the breast, or more in
the upper outer quadrent.
The pain is usually reduced by oral contraceptive.
On examination, there may be tenderness but no discrete lump. Diffuse
nodularity is common particularly in upper outer quadrant
The pain is never a symptom of cancer.
233
" Reading without contemplation is like eating without digestion "
Chinese byword
Treatment: If the pain is so severe:
- bromcriptin ( dopamine antagonist).
- danazol ( gonadotropin antagonist).
- tamoxifen.
- firm supporting brassiere may help.
2- non- cyclical breast pain:
This is less common.
It occur at these condition:
- at puberty
- at menopause due to cessation of hormone ( usually unilateral).
- tietze syndrome ( this is uncommon condition in which pain and tenderness
arise from costochondral junction lateral to the sternum). The pain is
exacerbated by movement.
- duct ectasia
- mondors disease.
- inflammatory disease.
Breast cyst:
Breast cyst is probably the commonest of the discrete breast swelling.
Breast cyst is fluid filled cavity appears in the breast, without a demonstrated
endothelial lining or a capsule.
This condition occur at times when the pt. hormone environment is changing,
usually around the menopause ( before the age of 40, the peak incidence is in
the late in 40 and early 50).
234
" Reading without contemplation is like eating without digestion "
Chinese byword
Presentation:
They may develop sudden swelling, moderate pain and tenderness are
common.
Examination;
Solitary cyst is smooth, spherical swelling.
If it is large cyst, it may be visible and even appear blue or green through the
skin, but there will never be tethering or fixation to skin or muscle.
It is rarely possible to elicit fluctuation or fluid thrill or to transilluminate the
lesion.
The clinical diagnosis of a cyst, will processed immediately to needle aspiration,
the appropriate treatment.
The fluid that emerges is variable in color and clarity, varying from very dark
green to clear yellow.
Galactocele
It is milk containing cyst and occur during or after lactation. It presents as above
and the physical signs are similar.
Aspiration produces milk, but the cyst rapidly refills and resolution must await
cessation of breast feeding.
Paget disease of then nipple:
Paget disease of the nipple is caused by cancer cells migrating or spreading
along the duct system from a carcinoma situated deeply in the breast, which in
the early stages is usually confined to the epithelium (DCIS).
THE presence of carcinoma cells in the skin of the nipple produce a clinical
appearance similar to that of eczema. patches of skin first become red and
235
" Reading without contemplation is like eating without digestion "
Chinese byword
then encrusted and oozy. The edges of these lesions are distinict, unike
eczema, and they do not itch.
In time the nipple is destroyed, and replaced by a malignant ulcer.
Paget disease of the nipple always indicated underlying malignant process in
the breast itself.
The different between eczema and paget disease of the nipple;
Paget disease
eczema
unlateral
Bilateral
Occur at menopause
Commonly occur at lactation
Dose not itch
No vesicles
Nipple may be destroyed
Itches
Vesicles
Nipple intact
May be underlying lump
No lump
Duct ectasia:
This is common of unknown etiology.
It is dilatation of the mammary ducts, which are full of inspissated material
containing macrophages and chronic inflammatory debris.
It has the following presenting features:
- nipple inversion, which is at first mild and readily everted.
There is characteristic transverse slit appearance. In many pt. this is the only
feature.
- difficulty in breast feeding.
- nipple discharge
236
" Reading without contemplation is like eating without digestion "
Chinese byword
- chronic low grade infection of the peri- areolar area, with tender thickening
around the nipple, going on abscess formation, known as periductal mastitis.
- periductal abscess that may rupture and stay in communication with the duct
system. This result in mammillary fistula.
Supernumary breast/ nipple;
Extra nipple or breast develope along the primitive milk line as a congenital
anamolies.
Breast absess
Acute breast abscess is often associated with lactation.
S. aureous is the commonest organism.
Bacteria may gain access to the engorged breast lobules, an excellent medium
for bacterial culture.
The pt. develop malise and fever accompanied by an ache in the breast which
progresses to throbbing pain.
On examination:
Signs of inflammation which are:
Pain, redness, swelling….
It is safe to continues breast feeding even from the breast containing the
abscess.
When a breast abscess occurs in a women who is not lactating there is often a
predisposing risk factor such as diabetes mellitus or immunocompromise.
Recurrent and chronic breast abscess;
It is usually associated with duct ectasia.
Tuberculosis remain common in some part of the world.
Mycobacterial infection is rare cause.
237
" Reading without contemplation is like eating without digestion "
Chinese byword
** the breast changes of pregnancy:
- fullness and pricking sensation
- enlargement and distended subcutaneous vein.
- increase nipple and areolar pigmentation with clear, expressed
secretion( colostrums).
- hypertrophy of subareolr sebaceous glands ( montogomery tubercle).
The male breast:
There are 2 causes of enlargement of the male breast.
1- gynecomastia ( benign)
The causes of gynecomastia are;
The pt. complain of painless, or slightly tender, enlargement of one or both
breast.
There is clearly palpable disk of firm breast tissue behind and attached to the
areolar.
General examination, especially of liver and scrotum (testes), may yield
information that indicate the likely cause.
2- carcinoma of the male breast;
It is uncommon, usually of elderly men.
Its symptoms and signs are identical to those of carcinoma of female breast.
There is little public awareness of the condition.
Because the male breast is small and not covered by a thick layer of SC fat, the
disease spread rapidly.
Physical signs such as skin and muscle fixation, ulceration and axillary
lymphadenopathy are often present by the time of presentation.
238
" Reading without contemplation is like eating without digestion "
Chinese byword
Chest trauma
Thoracic injuries can be divided into those that are immediately life
threatening and those that are potentially life threatening .
Immediately life-threatening injuries can be remembered
by
” ATOM FC”:
Airway obstruction
Tension pneumothorax
Open pneumothorax
Massive haemothorax
Flail chest
Cardiac temponad
Potentially life-threatening injuries can be remembered
by
“ATOM PD”:
Aortic disruption
Tracheobronchial injury
Oesophageal injury
Myocardial contusion
Pulmonary contusion an pneumothorax
Diaphragmatic rupture
For more info:
refer to churchill’s pocket book of surgery
Pneumothorax
Definition:
Air in the pleural cavity (i.e. between visceral and parietal pleura)
239
" Reading without contemplation is like eating without digestion "
Chinese byword
Types:
I-
Spontaneous:
Entrance of air into the pleural cavity through the pulmonary tissue
either
1- Primary( simple):
Due to rupture of a small localized bulla, usually in the apex of the
upper lobes.
The bulla may rupture spontaneously without any cause or it might
be triggered by exertion like high altitude ,flying or during diving
It usually occurs in Young Thin & Tall males
2-Secondary (complicated):
Due to lung disease which breaches the pleura
Common causes are: bullous emphysema rupture, pneumonia,
asthma, cystic fibrosis , T.B , alpha-1 anti trypsine deficiency ,
eosinophilic granulomata.
II-
Traumatic:
Due to a blunt or penetrating injury that disrupt the parietal or visceral pleura
Either
1-open pneumothorax:
Occurs when a penetrating chest wound produces a persistence
communication between the outside and the pleura, space that allows outside
air to enter the pleura e.g. srabbing , shooting.
2- closed pneumothorax:
The chest wall become airtight after penetration e.g. thoracocentesis
needle, central vein catheter, fractured rib, liver or lung biopsy.
May be due to leakage of air from a ruptured bronchus or perforated
eosophagus into mediastinum and then into pleural space
Pulmonary barotraumas can cause pneumoturax in patient on mechanical
ventilators.
240
" Reading without contemplation is like eating without digestion "
Chinese byword
Types of pneumothorax according to the degree of the collapse:
1) Small (simple) pneumothorax:
There is a small rim of air around the lung
The rim best seen on X-ray almost 3 cm or < 20% of radiographic
volume
Does not inhibit respiratory activity
No ttt , spontaneously resolves within weeks.
2) Moderate pneumothorax:
The lung is collapsed toward the heart border
Large enough to inhibit respiratory activity
Needs drainage of air
3) Tension pneumothorax:
Very sever complicated condition
pneumothorax
Spontaneous
Primary
Secondary
Traumatic
Open
close
Do You Know?
Marfan Syndrom is associated with an increased risk of pneumothorax
241
" Reading without contemplation is like eating without digestion "
Chinese byword
Symptoms of pneumothorax:
Unilateral chest pain (usually sudden)
Dyspnea
Anxiety
Fatigue
Dry cough ( may occur at onset)
Pain may be referred to the corresponding shoulder, across the
chest or over the abdomen
.So DDx: angina pectoris
Cholecystitis
Signs of pneumothorax:
In simple pneumothorax there may be no detectable signs or only diminution of
breath sounds
A. Inspection:
Decreased chest wall movement on the affected side
B. Palpation:
Decreased chest expansion at the affected side
Decreased tactile vocal fremitus at the affected side
There may be subcutaneous emphysema
C. Percussion:
Hyper resonance
D. Auscultation:
Decreased air entry
Breath sounds absent or decreased
Vocal resonance absent or decreased
There is no added sounds
242
" Reading without contemplation is like eating without digestion "
Chinese byword
Investigation:
Usually the diagnosis is established from the history and physical examination
A. Chest X-ray:
Better to be taken on expiration
Small pneumothorax may not be observed on inspiratory X-ray (bcause the
size and density of the lung is less than expiration)
1) Absence of peripheral lung marketing laterally
2) The line of pleura is more medially and separated from the chest wall
or mediastinum by air.
3) Absence of vessels shadow outside this line Nage9
B. ABG:
Hypoxia
Management:
A) Simple pneumothorax:
<20% radiographic volume or <3cm on X-ray
Only admit the patient for 48 hrs under observation
It usually heals (air is reabsorbed) within few days
We give the patient analgesic if needed
Rarely, small needle aspiration is needed. It is inserted in the 2
nd
intercostal space at the midclavicular line.
B) Moderate pneumothorax:
If it is >30% RGV or in Bronchopleural fistula
1
st
line ttt: aspirate air by simple needle in the second intercostals
space.
2
nd
line ttt:
Insertion of underwater seal drainage tube.
In very sever cases a suction device is added.
Follow up the patient by X-ray to evaluate the re-expansion.
243
" Reading without contemplation is like eating without digestion "
Chinese byword
C) Recurrent pneumothorax:
a. Pleurodesis:
By inserting a sclerotic material (Talc or doxycycline)
intrapleurally.
It will cause inflammation which heals by fibrosis and
adhesion between the two pleura no space for air.
Usually avoided in patient with cystic fibrosis.
b. Thoracotomy:
Usually indicated after 2 spontaneous pneumothorax on
the same side
Other indications for thoracotomy:
1. Massive air leak with failure of lung expansion.
2. small air leak persist for >9 weeks
3. Previous contralateral pneumothorax.
4. Presence of large apical bulla in CXR.
5. Complication like Emphysema, Hemothorax.
Procedure:
Bullae are excised and the pleura roughened
by rubbing with gauze or partial pleurectomy
when the bullae are extensive.
Tension Pneumothorax
Is the accumulation of air underpressure in the pleural space; displacing
mediastinal structures and compromising cardiopulmonary function.
It develops when injured tissue forms a 1-way valve, allowing air to enter pleural
space on inspiration and preventing it from escaping during expiration
It is an emergency condition which may lead to death if untreated.
Causes:
1) Trauma ( blunt or penetrating) usually associated with rib fracture
2) Barotrauma , 2ry to positive pressure ventilation
3) Central venous catheter( subclavian or internal jugular)
244
" Reading without contemplation is like eating without digestion "
Chinese byword
4) Conversion of idiopathic, spontaneopus, simple pneumothorax to tension
pneumothorax.
5) Chest compression during CPR.
6) High positive end-expiratory pressure(PEEP)
Pathophysiology:
1) When a 1-way valve forms due to disruption involving the visceral pleura,
parietal pleura or tracheobronchial tree allows air to enter into the
pleural space and inhibit air exit.
2) As the volume of the intrapleural air increases with each inspiration the
pressure increases within the affected hemithorax.
3) As the pressure increases ipsilateral lung collapse.
Mediastinal shift to the other side.
Symptoms:
Pain.
Anxiety.
Palpitation.
Dyspnea.
Grasping respiration.
Signs:
Early findings:
1) Tachypnea
2) Tachycardia
3) Decreased chest movement and expansion in the affected side
4) Decreased tactile vocal fremitus in the affected side or absent
5) Decreased breath sounds or may be absent
6) Hyperresonance
Late findings:
1) Decreased level of consciousness
2) Tracheal deviation to the contralateral side
3) Jugular venous distension
4) Hypotension
5) Cyanosis
6) Displacement of apex beat to the contralateral side
245
" Reading without contemplation is like eating without digestion "
Chinese byword
Investigation:
A. CXR:
1) Mediastinal shift to the other side , also trachea.
2) Flattening or inversion of the hemidiaphragm
3) Widening intercostals spaces > normal
4) Ipsilateral lung collapse at the hilum
B. ABG:
1) Hypoxia
2) Hypercapnea
3) Respiratory acidosis
Treatment:
Once diagnosed clinically, immediate ttt is necessary
Don’t delay ttt to do X-ray
Remember it is a life threatening condition
1) Place the patient on 100% oxygen
2) Emergency needle decopresion
Not the definitive ttt but to stop the progression and restore
cardiopulmonary function slightly
Done by inserting a large-bore needle with a catheter into the
2
nd
ICS just above the 3
rd
rib at the midclavicular line,
1-2 cm from sternal edge ( to avoid internal thoracic artery
injury)
3) Tube thoracostomy
The definitive ttt for tension pneumothorax
Immediately done after needle decompression
Create a 3-cm horizontal incision in the skin, over the 5
th
ICS
midaxillary line
Insert a chest tube and connect it to underwater seal apparatus
and suction
4) Follow up X-ray.
To asses for lung re-expansion
Thoracostomy tube positioning
Mediastinal deviation
5) Follow up ABG
246
" Reading without contemplation is like eating without digestion "
Chinese byword
Haemothorax
Blood in pleural cavity
Causes:
I. Traumatic:
The most common cause and can be due to
a) Blunt chest trauma: This may lead to rib fracture, pulmonary
laceration, great vessels injury and cardiac rupture.
b) Penetrating chest trauma: This may result in intercostals laceration,
great vessels and cardiac perforation or injury to diaphragm and
abdominal vescera.
II. Iatrogenic:
Central venous catheter placement, thoracocentesis( surgical puncture to
the chest wall for removal of fluid), needle biopsy, chest wall or lung injury
during thoracostomy or postoperative bleeding after thoracic or cardiac
operation.
III. Spontaneous:
In intrapleural malignancy or patient with coagulation disorders also can be
due to spontaneous pneumothorax with tern vascularized adhesions.
Rib fracture is the commonest type of blunt chest trauma
Intercostals vessels commonly lacerated by fractured ribs, also by
stab wounds, aspirating needles or chest drains.
Symptoms:
Pain (due to pleural irritation or/and trauma).
Dyspnea.
Shock in massive bleeding.
Signs:
Similar to pleural effusion:
A. Inspection:
247
" Reading without contemplation is like eating without digestion "
Chinese byword
Reduced chest movement.
B. Palpation:
Reduced chest expansion.
Mediastinal and tracheal deviated to the contralateral side if side.
Reduced or absent tactile vocal fremitus.
In rib fracture there may be tenderness and chest wall deformity
C. Percussion:
Stony dull
D. Auscultation:
Reduced or absent breath sounds.
Absent vocal resonance.
No added sounds.
Investigation:
A. CXR:
Pleural effusion.
Chest wall fracture may be present.
B. Thoracocentesis:
To aspirate blood.
Haematocrite > 50%.
Complication:
A) Short term effects:
Blood loss (if massivedeath)
Lung compression reduce gas exchange.
B) Long term effects:
Thickening of pleural surfaces.
Infection empyma.
Compression of the lung by a fibrous case made
of the organized clotted blood.
Treatment:
A. Chest tube:
In the 6
th
ICS in midaxillary line and connected to a suction( -20 cm
h2o)
Aim:
1. Re-expand collapsed lung.
248
" Reading without contemplation is like eating without digestion "
Chinese byword
2. Remove blood, so it decrease the risk of fibrothorax from the
organized blood clot and decrease risk of empyema.
3. Reduce further bleeding by
–ve pressure of pleural space.
4. Provide accurate rate of blood loss.
If residual hemothorax is minor or even moderate, it may
be ignored (no chest tube) b/c it will be resorbed later
on.
B. Thoracostomy:
For massive haemothorax.
In the 5
th
lateral ICS.
Blood clot is evacuated and bleeding is sought.
Indications for sx:
1. Pt in shock and fails to respond to resuscitative measures.
2. if continue bleeding at a rate > 500ml/8 hrs
3. Rate of bleeding increasing rather than decreasing.
4. Inability to empty the chest of large amount of blood clots.
5. If suspected rupture of aorta.
Chylothorax
Lymph in pleural cavity (milky coloy)
Causes:
Thoracic duct injury
Complication:
Systemic loss of protein rich fluid
Space occupying effect in pleural space
If persist fibrothorax
Risk of secondary infection
Diagnosis:
Aspiration of milky fluid which is sterile on culture
Lymphocyte > polymorph cells.
DDx: empyema
Treatment:
Thoracic duct ligation
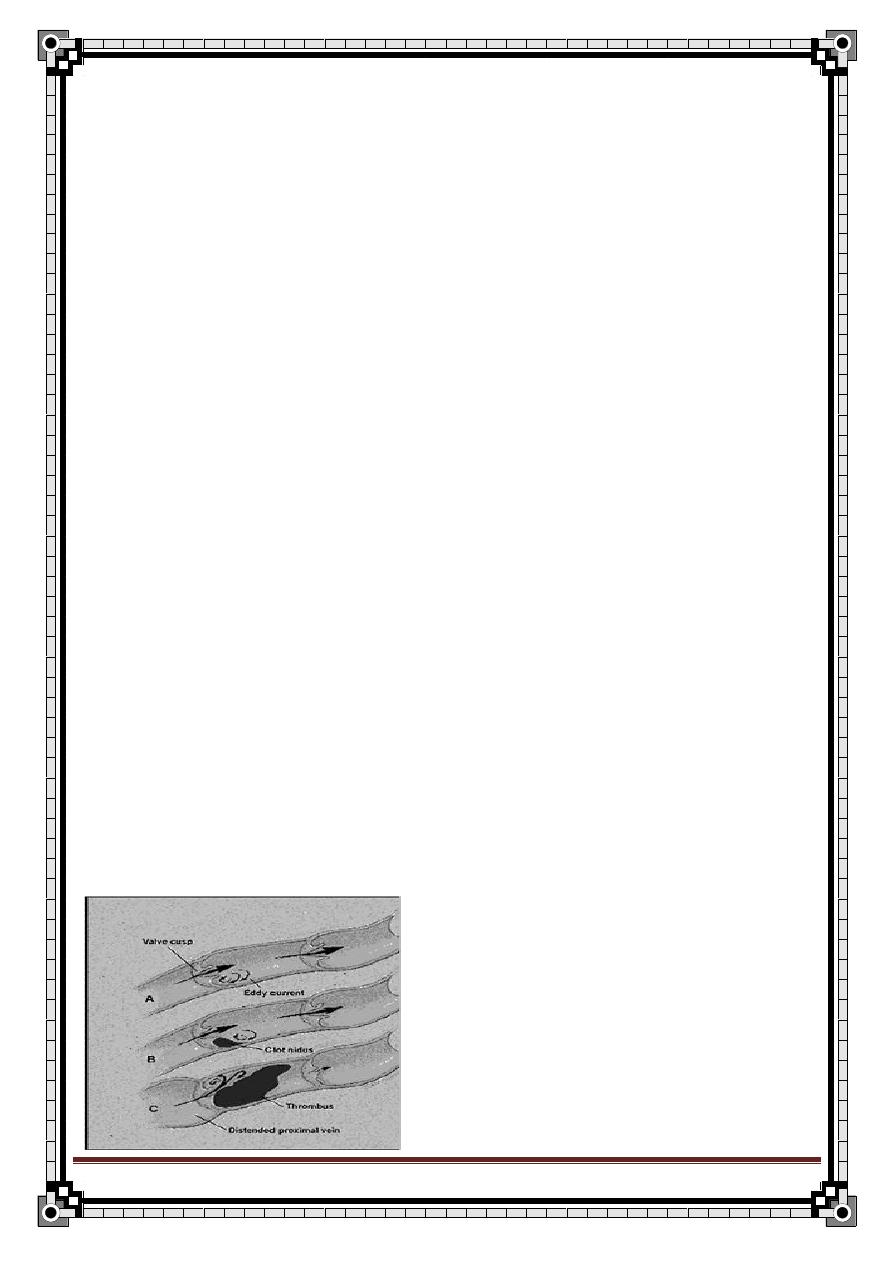
249
" Reading without contemplation is like eating without digestion "
Chinese byword
Venous Thrombosis
Classification:
1/ Superficial venous thrombosis:
Causes:
Hidden malignancy (eg; bronchus, pancreas), the vein is apparently
normal.
Burger’s disease.
Trauma.
Irritant from IV.
2/ Deep venous thrombosis:
Very common.
30% of legs after operations.
Commonly asymptomatic esp. in first few days.
(A) Sites:
Upper limbs: -superior vena cava
-axillary & subclavian vein
Lower limbs: - calf vein
- superficial femoral
- iliofemoral
Usually start at the valve sinus in the deep vein of the calf.
250
" Reading without contemplation is like eating without digestion "
Chinese byword
(B) Predisposing factors for DVT: (Virchow’s triad)
1. Stasis:
I.
Immobility (↓muscle pump activity)
II. Obesity.
III. Pregnancy.
IV. Heart failure.
V. Pelvic mass (compression to iliac vein)
2. Endothelial trauma:
I. IV therapy (canula, needle).
II. Injection associated with inflammation to the wall.
III. Trauma (esp. involving fractures).
IV. Pressure from operation table.
3. Altered constituent of blood: (hypercoagulability)
I. Increase viscosity & platelets by a- Loss of water (dehydration), b-
Increase cellular elements (polycythemia, leukemia, malignancy)
II. Decrease protein C, S & antithrombin
׀׀׀. ( if pt. with recurrent
thrombotic episodes, these factors should be suspected esp. in young
person or person with strong family Hx. Of thrombotic episodes).
III. Activated clotting factors
׀х, x, ׀x after operation.
IV. Drugs, eg; contraceptive pills.
(C) Stages of DVT:
1/ Stage of phlebothrombosis:
No local signs indicate its presence.
Clot is propagated & not attached to the vein wall.
Can be detected by Doppler ultrasound, Duplex us, venography.
2/ Stages of thrombophilibitis:
Clot release substances or f
rom bacterial break down products → inflammatory
reaction in the wall of the vessels. (the clot become adherent, so it is less
dangerous)
251
" Reading without contemplation is like eating without digestion "
Chinese byword
Clinical features of vein thrombosis:
In superficial thrombosis:
Tender.
Redness. Over the line of the vein.
Cord like thickening.
↑ temp.
In DVT:
Symptoms & clinical features of a lower limb DVT are;
1- Swelling. The most significant findings
2- Pain.
3- Redness.
4- Dilated superficial veins.
5-
Calf tenderness “Homan’s sign”. (no longer be used)
6- Low grade fever.
These features can be found in other conditions like: (DDx)
o Lymph edema.
o Arterial occlusion.
o Mechanical or tumor obstruction.
o Cellulitis.
o
Ruptured Baker’s cyst.
o Haematoma.
So, ttt with anticoagulants should not be started until a definite diagnosis of DVT
has been made, and the only reliable way to detect venous thrombosis is using
investigations like Duplex us or ascending venography.
In case of massive DVT → phlegmasia caerulea dolens
(painful swelling & blue)
“not only the main vein is occluded but
also the collaterals"
OR → phlegmasia alba dolens
252
" Reading without contemplation is like eating without digestion "
Chinese byword
(swelling, pale & pulseless)
“b/c of arterial compression by massive
edema"
Invetigations:
CBC: thrombocytosis, ↑ Hb in case of polycythemia.
PT & PTT: to start anticoagulant therapy.
LFT: mainly albumin → b/c warfarine is metabolized by liver.
Venography: (the most accurate & widely available), will define filling
defect in deep veins.
Doppler us: (hand held Doppler).
Doplex us: (us + flow measurement).
Radioactive
– Labeled Fibrinogen.
Treatment:
1/ For superficial venous thrombosis:
Prophylaxis: - treat varicose vein
- careful IV therapy technique
Curative: treat the cause as hidden tumor or varicose vein.
2/ For deep venous thrombosis:
Prophylaxis: to the pt. on RISK to thromboembolism.
Table (1): Risk factors for venous thromboembolism
Pat
ient’s factors
Disease or surgical procedure
Age
Trauma or surgery, esp. of pelvis,
hip, lower limb
Obesity
Malignancy esp. pelvic,
abdominal metastatic
Varicose veins
Heart failure
Immobility (bed rest > 4 days)
Recent myocardial infarction
Pregnancy
Paralysis of lower limb(s)
Puerperium
Infection
High-dose estrogen therapy
Inflammatory bowel disease
253
" Reading without contemplation is like eating without digestion "
Chinese byword
Previous DVT, or pul.embolism
Nephrotic syndrome
Thrombophilia
Polycythemia
Deficiency of antithrombin III,
protein C or protein S
Paraproteinaemia
antiphospholipid
Paroxysmal nocturnal
haemoglobinuria antibody, or
lupus anticoagulant
Behget’s disease (disease ccc by
mouth ulcer, genitalia ulcer, iritis,
uvitis, thrombophlibitis
Homocystinaemia
Table (2): Risk categories for thromboembolism in surgical patients
High risk
General and urological surgery in patients over 40 years with a recent
history of DVT or PE
Extensive pelvic or abdominal surgery for malignant disease
Major orthopedic surgery of lower limbs
Moderate risk
General surgery in patients over 40 years lasting 30 minutes or more
General surgery in patients below 40 years on contraceptive pills
Low risk
Uncomplicated surgery in patients under 40 years without additional
risk factors
Minor surgery of less than 30 minutes duration in patients over 40
years without additional risk factors
General prophylaxis for DVT:
1/ Pre-post operative compression stocking for all patients undergoing major
surgery, esp.
– pt with past Hx of DVT
– pt with varicose vein
– pt with myocardial disease
2/ Protection of leg vein during the operation (padded operation table)
3/ Post-operative elevation of the foot 9 inches (23cm).
4/ Early ambulation after operation.
254
" Reading without contemplation is like eating without digestion "
Chinese byword
Specific prophylaxis for DVT:
o Subcutaneous heparin during & after operation.
o Pre-operative intermittent electrical stimulation of the calf muscle or
pneumatic calf compression.
Conservative ttt:
Elastic stocking.
Foot elevation (23cm).
Anticoagulant: heparin or streptokinase (in major DVT).
Operative ttt:
Caval umbrella filter:
Under local anest
hesia, expose internal jugular, insert the umbrella → sup.
Vena cava → Rt heart → IVC (under x-ray control), then the umbrella opened
out.
Thrombectomy:
If the thrombosis is in the iliofemoral segment, it can be sucked out or pulled out
with balloon catheter through a groin incision.
Inferior vena caval application:
It is an old operation.
Complications of DVT:
1. Pulmonary embolism (the most important one).
2. Gangrene.
3.
Valve incompetence → varicose vein.
4. Venous claudication.
5.
Stroke → in pt who has patent foramen ovale or VSD (ventricular septal
defect with reverse Rt to Lt shunt).
Other Forms of DVT:
1) Inferior vena cava thrombosis:
255
" Reading without contemplation is like eating without digestion "
Chinese byword
Causes: - extension of iliofemoral thrombosis
- abdominal malignancy
Typical sign: - bilateral leg & scrotal edema.
- distended abdominal wall veins.
2) Superior vena cava thrombosis:
Causes: - mediastinal tumors.
- enlarged L/N (from breast or bronchial Ca.).
The pt complains of unpleasant bursting feeling in the head, neck, and
upper limbs.
There are edema, cyanosis, and venous distension.
3) Axillary & subclavian thrombosis:
Causes: - enlarged axillary L/N (from malignant disease)
- may fallow exercise in y
oung adult → axiilary
thrombosis.
- narrow space b/n the clavicle & 1
st
rib →
constrict the vein → subclavian thrombosis.
- central venous catheter.
The pt complains of uncomfortable heavy arm.
There are edema, cyanosis, and venous distension.
Venous collaterals develop over the shoulder and in the anterior chest
wall.
HISTORY OF DVT:
HPI:
Sudden pain (describe) + swelling.
Ask about risk factors:
o Malignancy (esp. pelvic and abdominal)
o Recent operation
o Immobility (bed rest > 4 days)
o HF & MI
o Trauma or surgery (esp. pelvic, hip, lower limbs)
o Dehydration
256
" Reading without contemplation is like eating without digestion "
Chinese byword
o Hx of previous DVT
o Pregnancy & Puerperium
Ask about symptoms of pulmonary embolism:
o Pleuritic chest pain (describe)
o Dyspnea
o Haemoptysis
o Collapse
Do not forget to ask about symptoms of DDx.
Family Hx:
Thrombotic episodes in the family (thrombophilia).
Drug Hx:
Contraceptive pills.
EXAMINATION OF DVT:
(1) General examination:
Vital signs
CVS: JVP, auscultation
Respiratory: pleural friction rub (pulmonary embolism)
Abdomen: palpation of any mass
Pelvis: PR & PV for any masses
(2) Local examination:
A. Inspection:
Swelling
Color of the skin (pale, blue, other)
Prominent veins
Hair loss
Cyanosis
B. Palpation:
Muscle texture (in DVT become hard)
Tenderness
Pitting edema
Measurement (magnitude of difference) (measure the
circumflex of the leg 10cm above and below the tibial tubrisity,
compare both legs)
Peripheral pulsation & capillary filling
Temperature
Sensation (touch, vibration, joint position sense)
Homan’s sign (just mention, do not do it)
257
" Reading without contemplation is like eating without digestion "
Chinese byword
Urology
Haematuria
Chief Compliant :bloody urine for 4 days.
History of the Present Illness
:
1- Duration
2- Onset of change in color
3- Timing (intermittent or continous)
4- amount
5- pattern of hematuria: Initial Haematuria (anterior urethral lesion);
terminal hematuria (bladder neck or prostate lesion); hematuria
throughout voiding (bladder or upper urinary tract)
6- clot
7- bleeding between voidings
8- Associated symptoms
Frequency,Dysuria,Suprapubic pain,flank pain (renal colic),perineal
pain,joint pain, weight loss, fever, palpitation
9- Aggravated factors : Recent exercise, menstruation
7- Recent sore throat, streptococcal skin infection
(glomerulonephritis)
8- Quantity of RBCs found on urinalysis
9- Hx of trauma
10- prior stone passage
11- Foley catheterization
12-Patient reaction
Past Medical History:
Prior Pyelonephritis
occupational exposure to toxins.
258
" Reading without contemplation is like eating without digestion "
Chinese byword
DDx.
Drug Hx:
Medications Associated with Hematuria:
Warfarin, aspirin,
ibuprofen, naproxen, phenobarbital, allopurinol, phenytoin,
cyclophosphamide.
Causes of Red Urine: Pyridium, phenytoin, ibuprofen, cascara laxatives,
levodopa, methyldopa, quinine, rifampin, berries, flava beans, food coloring,
rhubarb, beets, hemoglobinuria, myoglobinuria.
Family History:
Hematuria
renal disease
sickle cell
bleeding
deafness (Alport's syndrome)
hypertension.
Physical Examination
General Appearance: Signs of dehydration. Note whether the patient
appears ill, well, or lethargic.
Vital Signs: BP (hypertension), pulse (tachycardia), respiratory rate,
temperature (fever).
Skin: Rashes.
HEENT: Pharyngitis, carotid bruits.
Heart: Heart murmur; irregular rhythm (atrial fibrillation=> renal emboli).
259
" Reading without contemplation is like eating without digestion "
Chinese byword
Abdomen: Tenderness, masses, costovertebral angle tenderness (renal
calculus or pyelonephritis), abdominal bruits, nephromegaly, suprapubic
tenderness.
Genitourinary: Urethral lesions, discharge, condyloma, foreign body,
cervical malignancy; prostatetenderness, nodules, or enlargement (prostatitis,
prostate cancer).
Extremities: Peripheral edema (nephrotic syndrome), arthritis, ecchymoses,
petechiae, unequal peripheral pulses (aortic dissection).
Labs: UA with microscopic exam of urine, CBC, KUB, intravenous
pyelogram, ultrasound, ANA, INR/PTT.
Indicators of Significant Hematuria: (1) >3 RBC's per high-power field on
2 of 3 specimens; (2) >100 RBC's per HPF in 1 specimen; (3) gross
hematuria
The patient should abstain from exercise for 48 hours prior to urine
collection, and urine should not be col-
lected during menses.
Differential Diagnosis
A. Medical Hematuria is caused by a glomerular lesion; plasma proteins
filter into urine out of proportion to the amount of hematuria. It is
characterized by glomerular RBCs that are distorted with crenated
membranes and an uneven hemoglobin distribution and casts. Microscopic
hematuria and a urine dipstick test of 2+ protein is more likely to have a
medical cause.
B. Urologic Hematuria is caused by a urologic lesion, such as a urinary
stone or carcinoma; it is characterized by minimal proteinuria, and protein
appears in urine proportional to the amount of whole blood present. RBCs
are disk shaped with an even hemoglobin distribution; there is an absence of
casts.
260
" Reading without contemplation is like eating without digestion "
Chinese byword
Renal Stone
Chief Compliant:
The patient is a 40 year old white female who complains of
flank pain for 8 hours.
History of the Present Illness:
Pain analysis
1) Onset: acute
2) Severity: Severe
3) Character: colicky
4) Pattern: intermittent
5) Site: lower abdominal pain or flank pain
6) Radiation: may radiate laterally around abdomen to groin or to scrutum if upper
ureter stone while lower radiate to tip of glans penis or glitoris
7) Associated symptoms
Haematuria, fever, Dysuria ,incontinence, polyurea , nacturia ,urgency
,frequency. intermittent stream ,symptoms of uremia( headache, restlessness
,twitching, fits convulsion, drowsiness, coma,) wt loss malaise generalize
weakness
8) Aggravated or relieving factors: movement, medications
9) Others
low fluid intake
urinary tract infection
prior history of renal stones
parenteral nutrition
Excessive calcium administration
Immobilization
Furosemide
10)Patient reaction
Past Medical History:
1- Chemotherapy
2- inflammatory bowel disease
3- ileal resection
4- Diet high in oxalate: Spinach, rhubarb, nuts, tea, cocoa.
Drug Hx:
Excess vitamin C, hydrochlorothiazide, indinavir, unusual dietary habits.
Family History:
Kidney stones
261
" Reading without contemplation is like eating without digestion "
Chinese byword
Physical Examination
General Appearance:
Signs of dehydration, septic appearance. Note whether the patient appears ill, well, or
lethargic.
Abdomen:
Costovertebral angle tenderness, suprapubic tenderness; enlarged kidney.
Gyn:
Cervical motion tenderness, adnexal tenderness, cysts.
Labs:
Serum electrolytes, calcium, phosphorus, creatinine, uric acid. Urine cystine, UA
microscopic (hematuria), urine culture, KUB, intravenous pyelogram. PTH levels (if
hypercalcemia), 24-hour urine calcium, phosphate, urate, oxalate, citrate, Cr, sodium,
urea nitrogen, and cystine.
Differential Diagnosis:
1) Nephrolithiasis
2) Appendicitis
3) Cystitis
4) Pyelonephritis
5) Diverticulitis
6) torsion of hernia
7) ovarian torsion
8) ovarian cyst rupture or hemorrhage
9) bladder obstruction
10) prostatitis
11) prostate cancer
12) endometriosis
13) ectopic pregnancy
14) colonic obstruction
15) carcinoma (colon, prostrate, cervix, bladder).
Causes of Nephrolithiasis:
1- Hypercalcemia
2- Hyperuricosuria
3- Hyperoxaluria
4- cystinuriarenal tubular acidosis
5- Proteus mirabilis urinary tract infection (stag horn calculi)
262
" Reading without contemplation is like eating without digestion "
Chinese byword
Urine retention
Acute urinary retention is defined as the sudden inability to pass urine.
May be caused by obstruction, neurogenic causes, or medications .
Causes
Bladder
1. Bladder stone
2. Bladder cancer
3. Bladder infection
4. Neurogenic bladder
5. Detrusor instability
Prostate
1. BPH
2. Prostatic inflammation
3. Prostatic cancer
Post Prostatic
1. Urethral stricture
2. Polyps
3. Stone
4. Meatal stenosis
Other
1. DM
2. Parkinson Dz
3. MS
4. Previous CVA
5. Drug : Anticholinergics , Diuretics
263
" Reading without contemplation is like eating without digestion "
Chinese byword
Symptoms
■
Abdominal discomfort and distention (unless neurogenic)
■
Hesitancy, decreased force of stream, straining with voiding, sensation of
incomplete emptying in patients with obstructive etiology
■
Dysuria, urgency, frequency, or discharge with infection
Associated symptoms:
1. Wt loss
2. Loss of Appetite
3. Malaise generalize weakness
4. Fever
5. Leg or back pain
6. Nausea vomiting
7. Abdominal distension
Examination:
■
Findings vary with cause of obstruction (eg, enlarged prostate BPH).
■
Abdominal tenderness
■
Palpable bladder (if containing > 150 mL)
Diagnosis
■
UA to evaluate infection, tumor, calculi
■
BUN and creatinine to evaluate renal function
Treatment
■
Supportive care with analgesia
■
Placement of a 16- or 18-inch French urethral catheter or Coude catheter
■
Do not clamp catheter.
■
Bladder aspiration if Foley catheter cannot be placed
■
Observation of patients with chronic retention for the development of postobstructive
diuresis (4–6 hours)
■
Discharge with catheter in place and follow up with urology.
■
Antibiotics for infection, as needed
مت
ت
حبمد اهلل