1
Fifth stage
Pediatric
Lec-7
.د
رواء
1/1/2014
TTN , Meconium aspiration , IVH
Objectives:
• To know the clinical features and management of newborn baby with transient
tachypnea of newborn baby and meconium aspiration syndrome
• To recognise the clinical features of congenital diaphragmatic hernia and
tracheoesophageal fistula
• To know the features of other complications of preterm baby like intraventricular
hemorrhage, apnea, and necrotizing enterocolitis
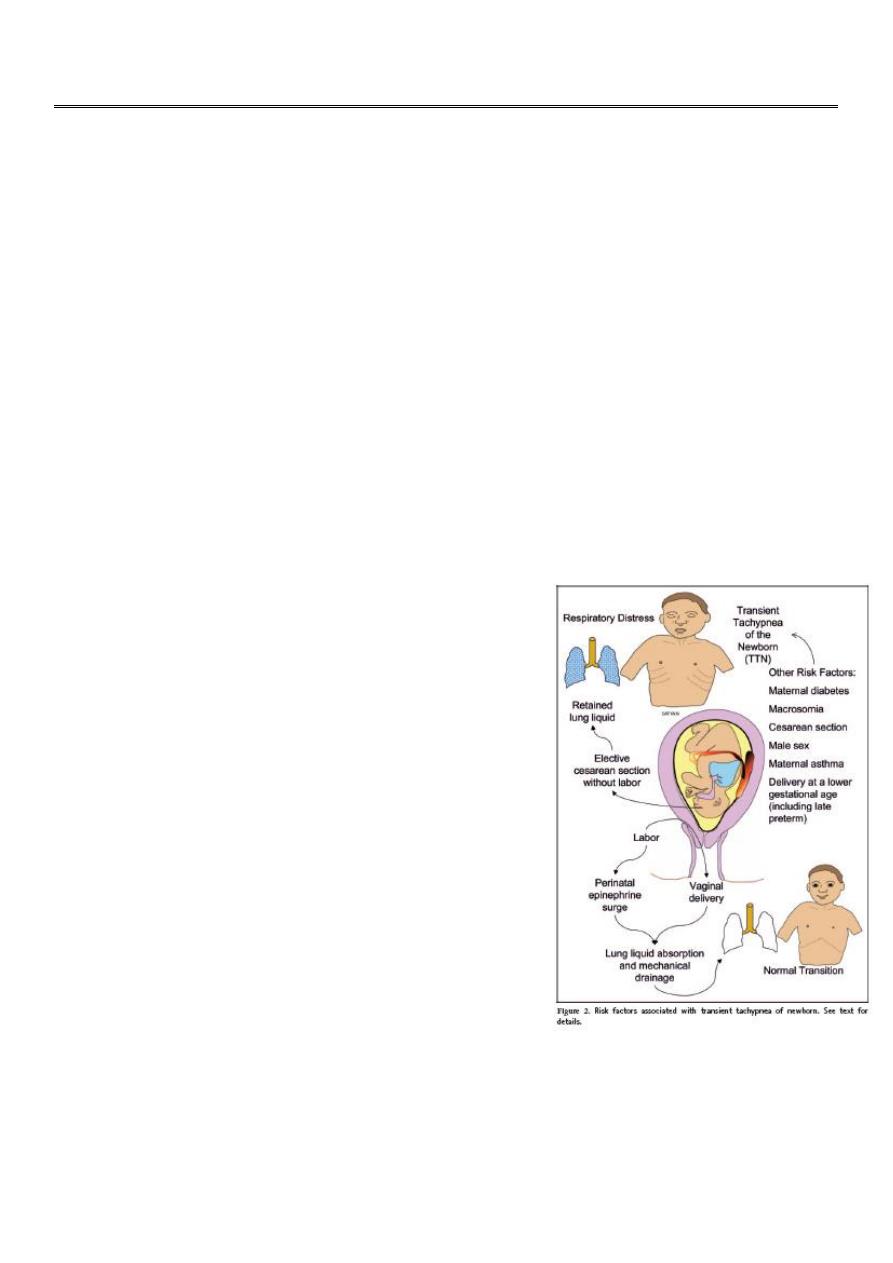
Transient Tachypnea of Newborn [TTN]
• TTN is self limited condition characterized by
tachypnea,mild retraction, and occational
grunting,usually with out signs of severe
respiratory distress. Cyanosis when present,
usually requires no more than 40% O2.
Patients usually recover rapidly within 3 days.
The lungs are generally clear without rales or
rhonchi
• TTN is noted in large premature infants& term
infants born by cesserian section with out prior
labour. Also infants of diabetic mother.
• TTN may be caused by retained lung fluid or slow
resorption of lung fluid.
• Chest x-ray:Prominent central vascular marking,
fluid in lung fissure, overaereation, occasionaly
small pleural effusion.
Meconium Aspiration Syndrome
Meconium is the first intestinal discharge from newborns which is a viscous, dark green
substance composed of intestinal epithelial cells, lanugo, mucus, and intestinal secretions,

2
such as bile.
Meconium stained amniotic fluid is seen in 10% of predominantly term, growth retarded,&
post term deliveries& should be considered a sign of fetal distress& suggest in utero
asphyxia, hypoxia, acidosis.
Meconium inactivates surfactant
Meconium aspiration syndrome deveops in 5% infants with meconium stained amniotic
fluid.
Meconium. A typical, sticky, greenish-black meconium stool consists of accumulated
intestinal cells, bile, and proteinaceous material formed during intestinal development
Aspiration of amniotic fluid contaminated with meconium may occur in utero& more often
after delivery leading to high incidence of pneumonia& pneumothoraces.
Clinical features:
Meconium aspiration pneumonia characterized by tachypnea, hypoxia, hypercapnia,& small
airway obstruction that produce air trapping,& extra-alveolar leaks. Complete small airway
obstruction produces atelectasis within 24-48 hr, chemical pneumonitis develops in
addition mechanical effect of airway obstruction.
Chest x-ray:
- Patchy infiltrates, overdistention , flattening of diaphragm, increase anteroposterior
diameter& high incidence of pneumomediastinum& pneumothorax.
Prevention
The risk of meconium aspiration may be decreased by rapid identification of fetal distress
and initiating prompt delivery in the presence of fetal acidosis, late decelerations, or poor
beat-to-beat variability.
Treatment
• Routine intubation to aspirate the lungs of vigorous infants born through meconium-
stained fluid is not recommended.
• Depressed infants (those with hypotonia, bradycardia, fetal acidosis, or apnea) may
undergo endotracheal intubation, and suction applied directly to the endotracheal
tube to remove meconium from the airway .
• Treatment of meconium aspiration pneumonia includes supportive care and standard
management for respiratory distress.
• Administration of exogenous surfactant to infants with MAS requiring mechanical
ventilation decreases the need for ECMO support
3
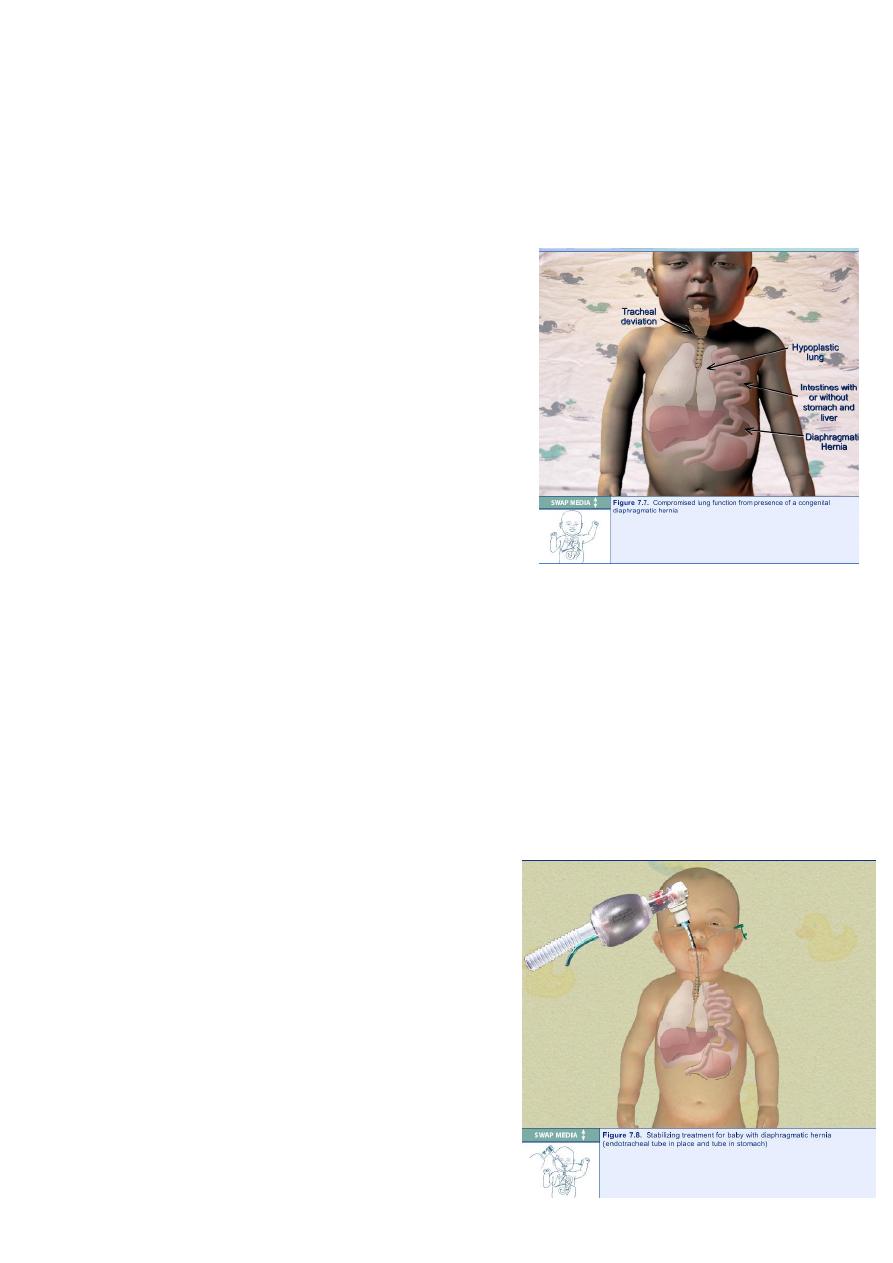
Congenital Diaphragmatic Hernia
Etiology:
Herniation occurs most often in posterolateral segment of diaphragm more often in left
side due to failure of pleuroperitoneal canal to close[foramen of Bochdalek].
Less frequently the herniation in the retro sternal area[foramen of Morgagni].
Pathology:
Protrusion of abdominal viscera
[stomach,intestine,spleen …] through diaphragmatic
hernia in to thoracic cavity displace the lungs and heart
to opposite side.
The lung on affected side is compressed and
hypoplastic,this lead to increase pulmonary vascular
resistance and pulmonary hypertension.
Clinical Manifestations:
Severe respiratory distress,including dysopnea and cyanosis is frequently present at birth or
later.
The abdomen is usually small and scaphoid.
The infant is cyanotic and have respiratory retraction.
Breath sounds may be absent on the affected side,and occasionally sounds of intestinal
peristalitic movement can be heard over the chest.
Diagnosis: by x-ray.
Antenatal diagnosis may be made by ultrasound.
Treatment:
Resuscitation of newborn is mandatory prior to
surgery
1-position head and thorax higher than abdomen to
facilitate downward displacment of abdominal
organs.
2-nasogastric intubation with intermittent suction
decrease air and fluid in herniated viscera.
4
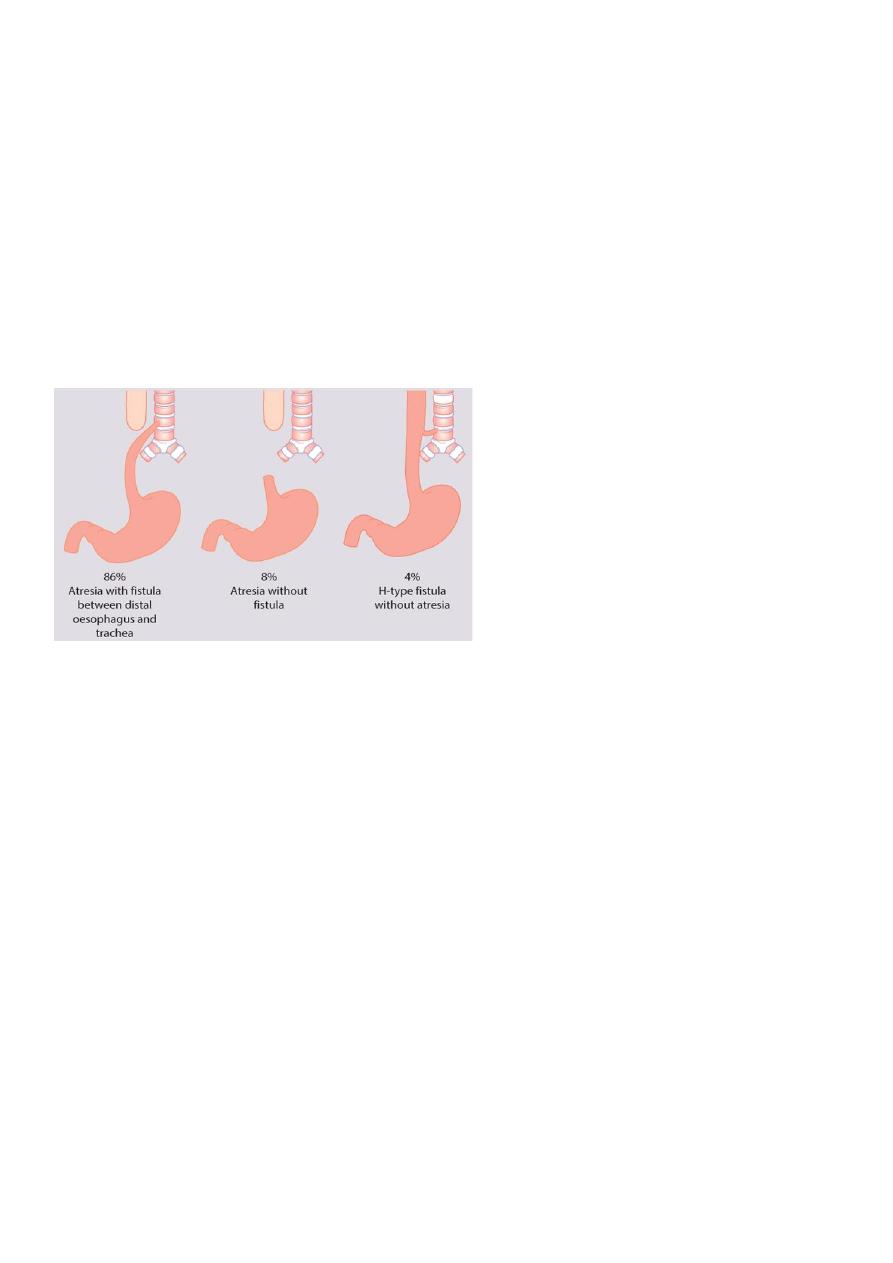
Esophageal Atresia&Tracheoesophageal Fistula
In 85% of cases fistula between trachea and distal esophagus accompanies atresia. Less
commonly, EA or TEF may occur alone.One third of affected infants are born premature.
Clinical manifestations:
Atresia of esophagus should be suspected:
1-In cases of maternal polyhydromnias.
2-If catheter used at birth for resuscitation cannot be inserted in to the stomach.
3-If infant has excessive oral secreations.
4-If choking, cyanosis,or coughing occurs with an attempt of feeding.
In infant with fistula with out atresia [H type] the usual sign is recurrent aspiration
pneumonia.
At least 30% of infant with EA have associated congenital anamolies like VATER anomalad.
Diagnosis:
Inability to pass catheter in to the stomach confirms the suspicion,and x-ray shows coiled
catheter in to upper esophageal pouch.
Treatment: by surgery.
Periventricular Hemorrhage [PVH]& Intraventricular Hemorrhage[IVH]
Are common among VLBW ,and the risk decrease with increasing gestational age.
50% of infants under 1500gm have evidence of intracranial hemorrhage.
Pathogenesis: unknown
Initial site of bleeding may be the weak blood vessels in the periventricular germinal matrix.
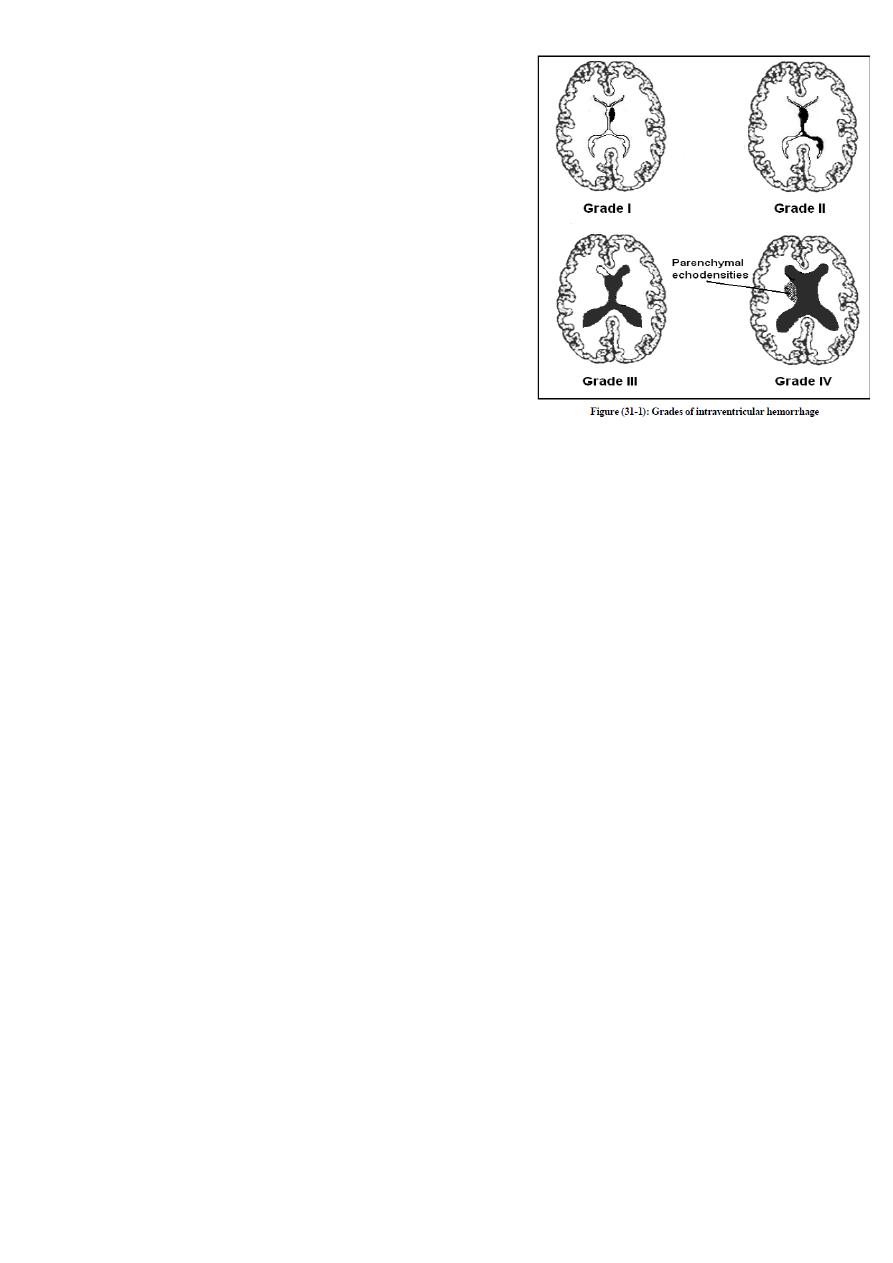
5
These vessels in this area have poor structural
support.
Main risk factor is passive changes in cerebral flow
with variation of blood pressure.Factor effect blood
pressure or interfere with venous return from head
increase risk of IVH includes: asphyxia, pneumothorax,
mechanical ventilation, hypercapnia, hypoxemia,
prolonged labor, breach delivery, PDA, heart failure,
I.V.therapy with albumin& hypertonic solution such as
sodium bicarbonate.
Clinical manifestations:
Most PVH&IVH occur in the first 3 days of life, it is
unusual after 5th day of life.
Seizure, apnea, bradycardia, lethargy,coma,
hypotension, metabolic acidosis, anemia not corrected by blood transfusion,bulging
anterior fontanel,& cutanous mottling.
Small hemorrhage are asymptomatic, large hemorrhage may progress to shock &death.
Later complications includes posthemorrhagic hydrocephalus, periventricular leukomalacia,
which may be precursor to cerebral palsy.
Diagnosis:
By CT scan or ultrasound through anterior fontanel
Treatment: of acute hemorrhage
Standard supportive care including ventilation for apnea, and blood transfusion for shock.
Post hemorrhagic hydrocephalus may be managed by serial lumbar puncture, external
ventriculostomy tube or permanent ventricular peritoneal shunt.
Apnea
Apnea is defined as the cessation of pulmonary air flow for a specific time interval, usually
longer than 10-20 seconds. Bradycardia often accompanies prolonged apnea.
Types:
1-Central apnea: refers to complete cessation of airflow and respiratory efforts with no
chest wall movement.
2-Obstructive apnea: no airflow is exhibited but the chest wall movements continue.
3-Mixed apnea: a combination of these two events and is most frequent type.

6
Pathogenesis:
-Idiopathic apnea: a disease of premature infants appears in the absence of any other
identifiable disease,it occurs during the first week of life and resolve by 36 weeks of post-
conceptional age. It is usually due to process of regulating respiration.
Premature infants respond paradoxically to hypoxia by apnea rather than by increasing
respiration as mature infant.
Potential causes of neonatal apnea:
-CNS disease, respiratory disease, infectious disease,GIT disease, cardiovascular disease,
metabolic disease.
Treatment of apnea of prematurity:
1-Adminstration of oxygen to hypoxic infants.
2-Transfusion of anemic infants.
3-Cutanous stimulation for infants with mild apnea.
4-Persistent apnea with bradycardia can be treatd with methylxanthine[ caffeine or
theophylline]. Theophylline act as CNS stimulant.
5-Nasal CPAP of 3-5 cm H2O is effective method of treating obstructive or mixed apnea.
Necrotizing Enterocolitis [NEC]
Higher incidence in very low birth weight baby.
Etiology: unknown, but it is likely multifactorial with super infection with gas forming
bacteria and failure of the mucosal barrier in the immature gut.
Precipitating factors:
-Hyperosmolar feeds
-Perinatal asphyxia
-Polycythemia
-Umblical catheritization
-PDA
Breast milk is partly protective
Clinical features:
The onset of symptom is usually in the first week of life.
Increasing aspirate usually bile stained from stomach or vomiting usually bilious but
occasionally blood stained.Diarrhea follows the failure to tolerate feeds and may be watery
or contain mucus and visible blood and pus.The baby often unwell, lethargic and having
apneic episodes.

7
Examination: reveals a tense distended tender abdomen which is silent if perforation has
taken place.Septic or hypovolemic shock may be a complication and infant may collapse
and die.
Diagnosis:
-Blood culture.
-Plain abdominal x-ray: initially shows separation of bowel loops due to ascitis& fluid levels.
Periluminal tramlines indicating intramural gas [pneumatosis intestinalis].
Later signs include gas in the portal tree& gas under the diaphragm following perforation.
Management:
• Initially medical & conservative.
• Oral feeding should be stopped& nasogastric tube put.
• Septic screen is performed.
• Intravenous antibiotics[penicilline,gentamicin,& metonidazole].
• I.V feeding through central line for 10 days& bowel rest.
• Surgery is indicated if there is perforation or failure to improve on medical therapy.