
1
Fifth stage
Pediatric
Lec-1
.د
رواء
1/1/2014
Infant feeding
Objectives
1.To know about nutritional requirements in infancy
2.To know about the process of breast feeding .
3.To know the advantages of breast feeding
Nutritional requirements
The aim of infant feeding
1. is to achieve optimal physical ,neural ,and mental growth as the maximum brain
growth occur in the first two years of life .
2. Good nutrition prevents acute and chronic illnesses results from macro and micro
nutrients deficiency or exces
Water
Forms about (70-75 )% of body weight ,and the daily consumption of fluid by the healthy
infant is equivalent to (10-15 )% of body weight .
Water balance depends on :
1.fluid intake
2.protein and mineral contents of diet
3.solute load for renal excretion
4.metabolic and respiratory rate
5.body temperature
Calories
Kilo calorie :is the amount of heat required to raise the temperature of 1 kg of water
from (14.5-15.5 C ) .
The daily requirements of calories in infants is (80-120 )Kcal for the first year of life with
subsequent decrease of about 10 Kcal /Kg for each succeeding 3 years period .
Approximately (9-15 )% are derived from protein
(35-45 )%from fat
(45-55 )% from carbohydrate
As 1gm of protein and carbohydrate give 4 Kcal and 1gm of fat give 9 Kcal

2
Proteins
It constitute about 20% of body weight ,it’s amino acids are essential in forming cell
protoplasm ,we have 24 amino acids 9 of them are essential for infants ,those are
(Threonine ,valine ,leucine ,isoleucine ,lysine ,Tryptophan ,phenyl alanine ,Methionine
and Histidine ) .
Arginine ,Cystine ,and Taurine are essential for low birth wt.infants .
Carbohydrates
It constitute about 1% of body weight ,it is stored as glycogen in the liver and muscle, it
is the major source of calories (45-55 )%,it has 3 various forms :
1.monosaccharides (glucose ,fructose ,galactose )
2.Disacchrides (lactose ,sucrose ,maltose ,isomaltose)
3.Polysaccharides (glycogen ,starches ,gums,cellulose and dextrin's )
Fats
Fats form 30-40% of the total energy intake for children (1-3 )yr of age and 25-35% for
children (4-18 yr) of age. Dietary fats are composed of a various mix of saturated fats,
monounsaturated fat, PUFA, trans fat, and cholesterol. In addition to being energy-
dense macronutrients, fats play significant structural and functional roles; cholesterol
moieties are precursors for cell membranes, hormones, and bile acids. Fat intake also
facilitates absorption of the fat-soluble vitamins A, D, E, and K.
Humans are incapable of synthesizing the precursor ω3 (α–linolenic; ALA) and ω6
(linoleic; LA) PUFAs and are dependent on dietary sources for these essential fatty acids.
Micronutrients
1.Minerals :the principle cations are (calcium,magnesium ,potassium and sodium ) and
The principle anions are (phosphorus ,sulphur and chloride ).Iron,iodine and cobalt
appear in important organic complexes,and the trace element floride,copper,zink
,manganese ,and chromium have important metabolic rule .
2.Vitamines :are organic compounds required in minute amounts to catalyze cellular
metabolism ,there are 3vitamines synthesized by the intestinal flora which are
(vit.K,pantothenic acid andBiotin )

3
Feeding of infants
Feedings should be initiated soon after birth unless medical conditions preclude them.
The American Academy of Pediatrics (AAP) and World Health Organization (WHO)
strongly advocate breast-feeding as the preferred feeding for all infants. The success of
breast-feeding initiation and continuation depends on multiple factors, such as
education about breast-feeding, hospital breast-feeding practices and policies, routine
and timely follow-up care, and family and societal support ,the AAP recommends
exclusive breast-feeding for a minimum of 4 mo and preferably for 6 mo.
Preparation of the lactating mother
The mother should be prepared from the mid trimester of pregnancy :
1.Psychologically
2.Physically :by promoting good health and nutrition and balanced rest and exercise with
treatment of any illness ,and if the mother has retracted nipples she will benefit from
manual or electric breast pump traction during latter weeks of pregnancy .
Establishment and maintenance of breast feeding
Breast feeding: should start as soon as possible after delivery as the condition of the
mother and the baby permits ,practically after drying ,checking under heater source and
if normal to put the baby on the breast even before delivery of the placenta as sucking
stimulate oxytocin hormone secretion from the posterior pituitary and leads to rapid
separation of the placenta .
Breast fed infants who cant feed on demand should be put on the breast every 3-4 hours
Care to the nipples
Any pain and tenderness in the nipples should be prevented to promote successful and
continuous breast feeding by :
1.exposing the nipples to air
2.Applying pure lanoline emollient (panthenol )
3.Avoiding soaps and shampoos for cleaning
4.Frequent changing of nursing pads
5.Nursing more frequently by proper position of the baby
Physiology of breast feeding
1.Babies use rooting , sucking ,swallowing reflexes to locate the nipple and feed
2.Tactile receptor in nipples are activated

4
3.Hypothalamus sends efferent impulses to anterior and posterior pituitary
4.Anterior pituitary prolactin secretion stimulate milk secretion by cuboidal cells in the
acini of the breast
5.Posterior pituitary oxytocin secretion result in contraction of myoepethelial cells in the
alveoli forcing milk into the larger ducts the so called (let down reflex )
Problems of breast feeding which affect initiation &maintanance of breast
feeding
1.Truly retracted nipples (inverted nipples ) :
Breast shells, also referred to as milk cups, breast cups, or breast shields, take advantage
of the natural elasticity of the skin during pregnancy by applying gentle, but constant
pressure to the areola in an effort to break the adhesions under the skin that prevent
the nipple from protruding. The shells are worn inside the bra, which may need to be
one size larger than normal to accommodate the shell. Ideally, shells should be worn
starting in the third trimester of pregnancy for a few hours each day. As the mother
becomes comfortable wearing the shells, she can gradually increase the amount of time
she wears them during the day. After the baby is born, these same shells can be worn
about 30 minutes prior to each feeding to help draw out the nipple even more. They
should NOT be worn at night
2.Breast engorgement :
In the 2nd stage of lactogenesis day 3 or 4, physiological fullness of the breast occurs. If
the breasts are firm, overfilled, and painful, the cause may be incomplete removal of
milk due to poor breast-feeding technique or other reasons such as infant illness.
Frequent breast-feeding or, in some cases, manual milk expression before breast-
feeding may be required .
3.Mastitis :
Mastitis occurs in 2-3% of lactating women and is usually unilateral, manifesting with
localized warmth, tenderness, edema, and erythema after the 2nd post delivery week.
Sudden onset of breast pain, myalgia, and fever with fatigue, nausea, vomiting, and
headache can also occur. Organisms implicated in mastitis include Staphylococcus
aureus, Escherichia coli, group A streptococcus, Haemophilus influenzae, Klebsiella
pneumoniae, and Bacteroides spp. Diagnosis is confirmed by physical examination. Oral
antibiotics and analgesics, while promoting breast-feeding or emptying of the affected
breast, usually resolve the infection. A breast abscess is a less-common complication of
mastitis, but it is a more serious infection that requires intravenous antibiotics as well
as incision and drainage, along with temporary cessation of feeding from that breast
5
4.Breast abscess :
A breast abscess is a serious and painful complication of mastitis that occurs when there
has been inadequate treatment or where treatment has been delayed. Breast abscess
occurs in approximately 0.1–0.5% of breastfeeding women
and in approximately 3–10% of breastfeeding women with inflammatory symptoms of
the breast
Ultrasound examination is useful in confirming the presence of an abscess if suspected
because of localised mass and fever.
Breastfeeding should continue on the unaffected breast.
the abscess may be managed with needle aspiration or surgical incision, but unless the
position of the incision makes it impossible, breastfeeding should continue, or resume,
once treatment has started
If breastfeeding is not possible, expressing from the affected breast is recommended to
prevent complications such as engorgement
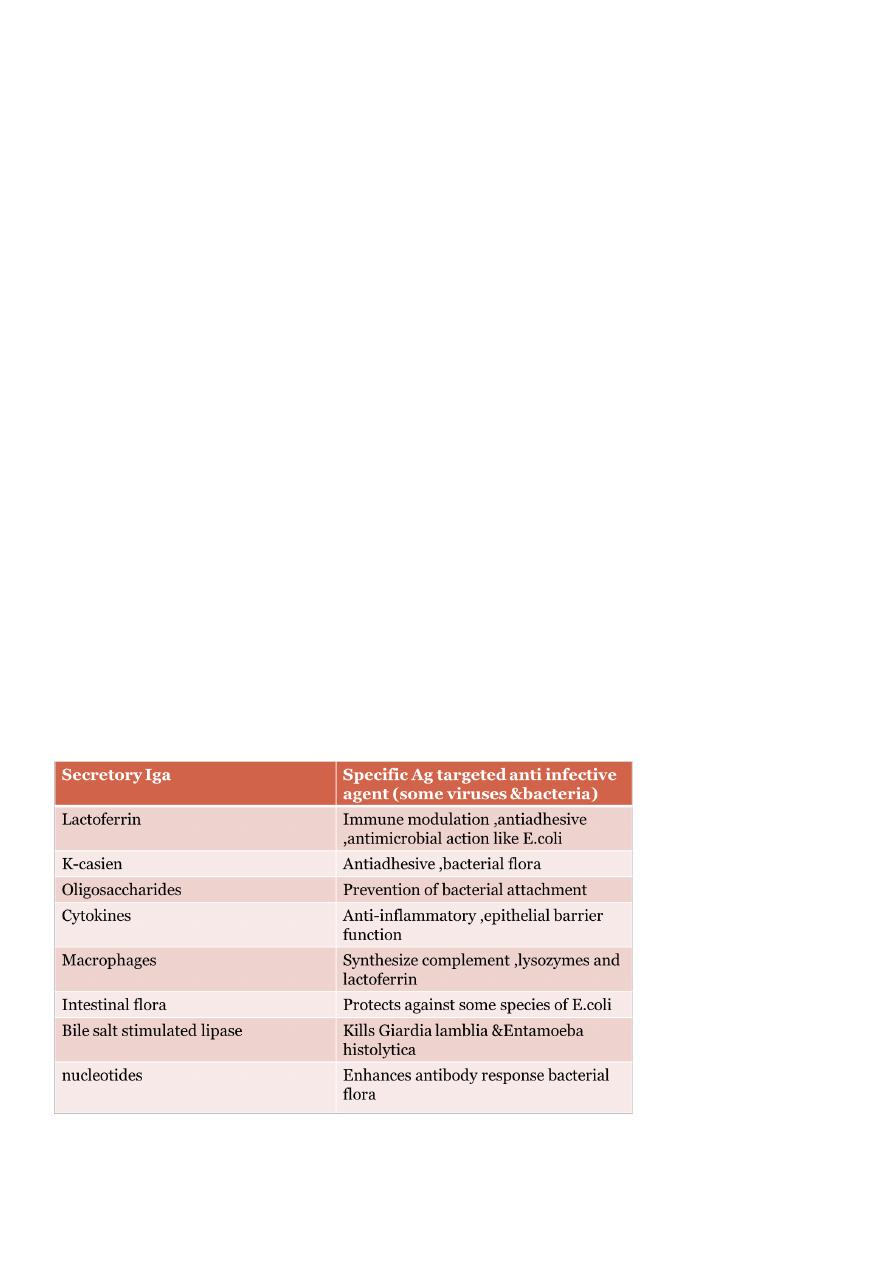
Advantages of breast feeding
1.it is always readily available fresh at proper temperature and need no time for
preparation .
2.Psychological advantages :it promote infant maternal bonding and successful breast
feeding has satisfying experience for both .
3.Human milk iron although little but well absorbed from the intestine and supplemental
iron need to be added at 6 monthes of age .
4-Sellectiv beneficial effect against infant formula