1
Fifth stage
Pediatric
Lec-7
د.ندى العلي
26/10/2015
Headache and migraine
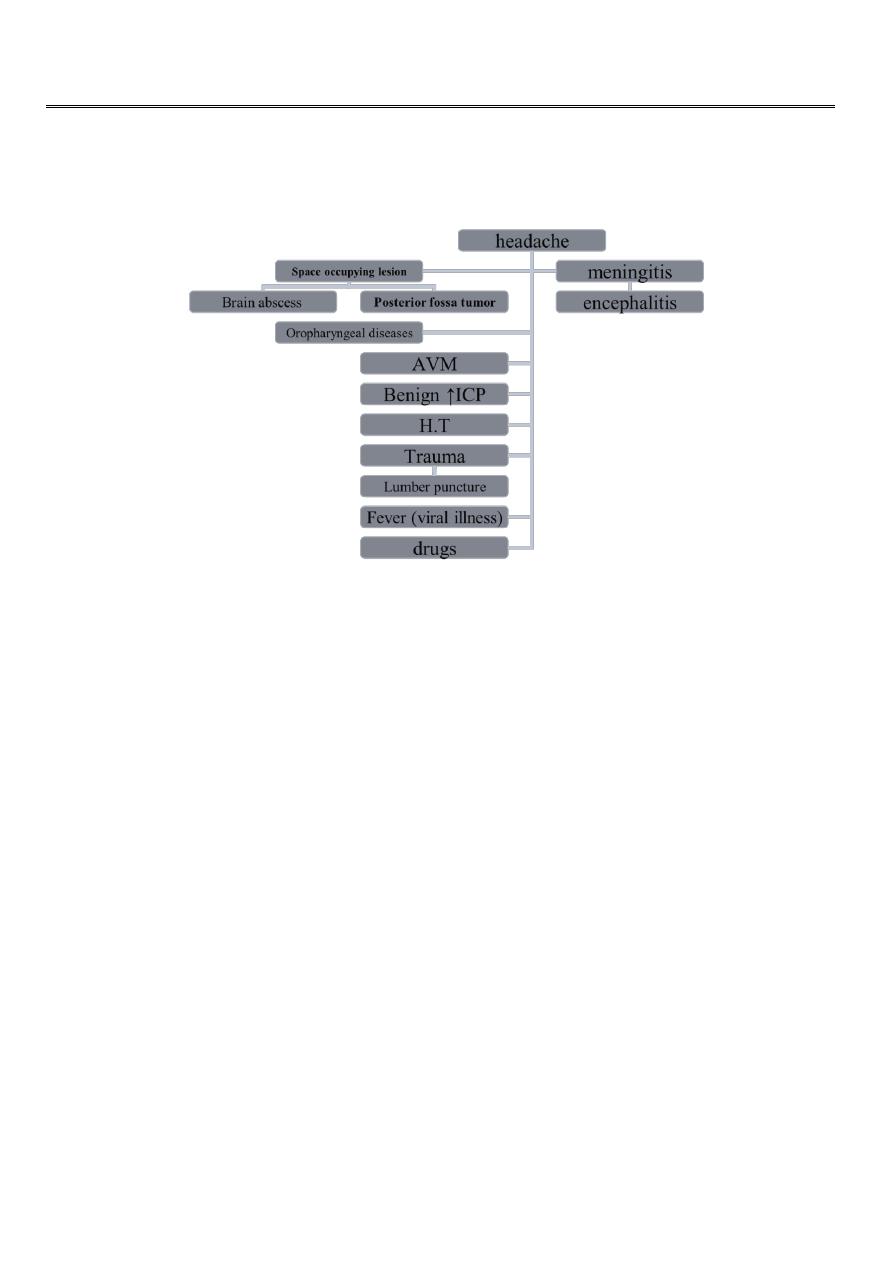
Worrisome headache
1-most sever on awakening.
2-that awaken the patient in the middle of night.
3-severly exacerbated on coughing or bending.
4-acute without previous history.
5-present daily &getting progressively more sever.
6-associated with vomiting.
Migraine headache
Common migraine (with out aura):
1-most prevalent in children
2-throbbing headache, unilateral, or bifrontal or temporal
3-persist for 1-3hr or as long as 24 hr
4-inhibition of physical activity
(aggravation of pain by motion)
5-intense nausea&vomiting.

2
6-abdominal pain&fever.
7-pallor,photophobia,phono- phobia,osmophobia.
8-family history in 90%.
Classical migraine (with aura):
1-rarely present in children
2-aura(blurrid vision,scotoma,
Flash of light,vertigo,parasthesia,
Numbness of hands and feet,
Distortions of body image
3-typical symptoms of common
Migraine.
4-family history in 90%.
Additional feature of all migraines
Precipitating factors:
1- by menstruation
2- after heavy exercise.
3- psychological stress.
4- lack of food or sleep.
5- food or drugs(cheese,chocolate, oral C.C pill
Relieve with sleep.
Migraine variants
Abdominal migraine:
(موضوع
مهم
)
is a recurrent disorder characterized by mid-abdominal pain with pain-free periods
between each attack. The pain is usually described as “dull” and may be moderate to
severe. The pain may persist from 1 to 72 hr and, although usually midline, may be
periumbilical or poorly localized by the child.
To meet the criteria of abdominal migraine, the child must complain at the time of the
abdominal pain of at least two of the following: anorexia, nausea, vomiting, or pallor. As
with cyclic vomiting, a thorough history and physical examination with appropriate
laboratory studies must be completed to rule out an underlying gastrointestinal disorder as
a cause of the abdominal pain.

3
Basilar-type migraine
:
is considered to represent a precursor of childhood migraine. Brainstem signs predominate
in these patients because of vasoconstriction of the basilar and posterior cerebral arteries.
The major symptoms include vertigo, tinnitus, diplopia, blurred vision, scotoma, ataxia, and
an occipital headache. The pupils may be dilated, and ptosis may be evident. Alterations in
consciousness followed by a generalized seizure may result.
After the attack, there is a complete resolution of the neurologic symptoms and signs. Most
affected children have a strongly positive family history of migraine. Many develop
migraine with aura as adolescents or adults. Relatively minor head trauma may precipitate
an episode of basilar migraine. The condition has been described in children of both sexes,
with girls younger than 4 yr being at particular risk.
Cyclic vomiting
1- mainly occur in infant and young children.
2- recurrent vomiting (dehydration with electrolyte disturbance).
3- fever , abdominal pain , diarrhea.
3- pallor, fright follow by deep sleep→releave symptoms.
4- family history of migraine.
5- typical migraine headache in future.
Treatment:
1- fluid replacement.
2- rectal antiemetics(ondansetron
D.Dx:(intestinal obstruction,peptic ulcer, IBD ,inborn error of metabolism ,CNS lesion).
Diagnosis of migraine
1- history&physical examination.
2- lipid profile
3- radiological study(CT and MRI)to rule out any SOL.
Treatment of migraine
Non medical:

4
1- elimination of precipitating factor.
2- reassurance.
3-psychotherapy.
Analgesia :
1- acetaminophen.
2- NSAIDS
Minor tranquilizers:
1- benzodiazepam
2- antihistamine
3- barbiturate
Antiemetics:
1- metocloppramide
2- promethazine
Combination of symptomatic medicine:
Triptans(serotonin agonist).
Prophylactic agents:
1-Tricyclic antidepressants.
2-Beta-blocker.
3-Calium channel blocker.
4-Valproic acid.
5-Cyproheptadine.
Tension headache
1-daily with work or school.
2-present all the day with worsening in afternoon
3-moderate band-like pain.
4- multiple somatic symptoms(SOB, abdominal pain, dizziness.
5
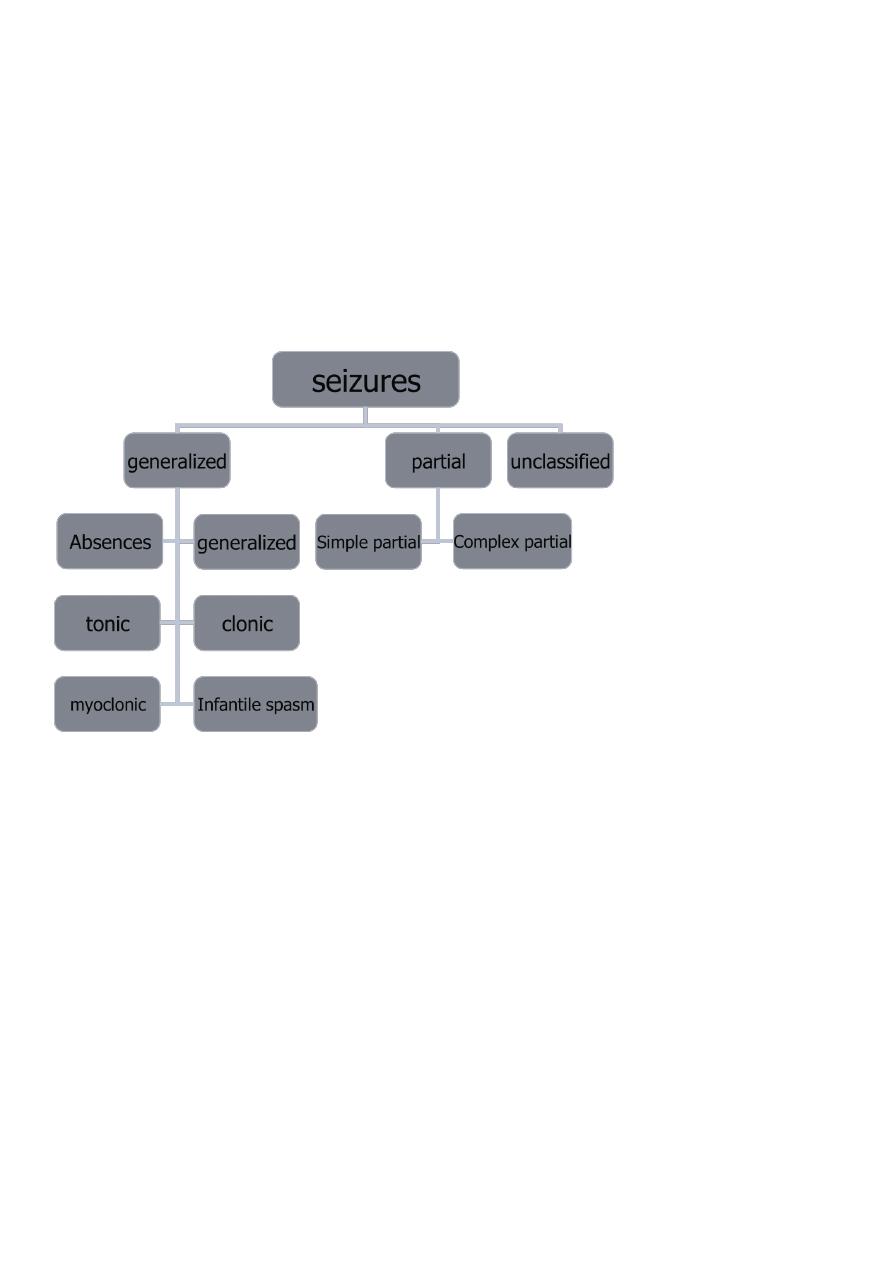
Seizures in childhood
Seizures (convulsion):
Define as a paroxysmal involuntary disturbance of brain function that manifested as a loss
of conscious, abnormal motor activity, behavioral abnormality, sensory disturbance, some
time abnormal movement without loss of consciousness.
Epilepsy:
Is defined as recurrent seizures unrelated to fever or to acute brain insult.
Absence seizures
1- 6-8%
2- age 4-6 ys
3- brief loss of environmental awareness.
4- automatism(eye fluttering,head bobbing, lip smacking)
5- neurological exam. &brain imaging are normal.
6- characteristic EEG patterns (synchronous 3-Hz spike-and-wave activity with frontal
accentuation.
7- seizure provoke by hyperventilation or flashing light stimulation.
8- last few seconds.
9- patient have dozen of seizures /day
10- treatment :Ethosuximide or Valproate+Clonazepam

6
Febrile seizures
(موضوع
مهم
)
1- Genetic predisposition to seizures in infancy that precipitate by rapid rise in body
temperature.
2- Occur in 2-4% of children .
3- age 6months-7years (50% occur between 1-2 yrs).
4- (simple febrile convulsion): generalized, last<15 minutes ,occur once in 24 hr,
(complex febrile convulsion) focal ,>15 ms, >once/24 hr.
5- prognosis excellent.
6- intellectual function normal.
7- reccurence rate: in simple type recur in 50% of those<1 yr ,28% of those>1 yr. 10%
have 3 or more recurrence, while in complex type it recur in 8%.
8- risk of epilepsy 1%.
9- factors↑ risk of epilepsy :abnormal neurological exam., family hix of epilepsy
&complex febrile convulsion.
10- Treatment:
1-I.V or rectal diazepam during seizure (0.2-0.4 mg/kg).
2- rule of phenobarbitone and Na valpoate
Generalized tonic ,clonic and tonic clonic seizures
May occur alone or with other seizure types.
Loss of posture& consciousness →tonic stiffening&upward deviation of eyes
→pooling of secretion ,pupillary dilation ,diaphoresis ,HT →clonic jerk →briefly tonic
again followed by flaccidity &urinary incontinence.
If last longer than 30 minutes it called (status epilepticus) in which 25%of them got
acute brain injury like infection or electrolyte disturbance or acute anoxia while 20%
have brain injury or congenital malformation and in 50% no causes is found.
Treatment:
A B C
Medication :diazepam(0.2-0.4 mg)I.V+phenobarbiton10-20 mg I.V
History & physical exam.
Infantile spasms (west syndrome)
(موضوع
مهم
)
Begin between the age of 4-8 mo.
Characterized by brief symmetrical contractions of the neck ,trunk and extremities.
Of 3 types: 1-flexor spasm 2- extensor spasm 3- mixed .
Mixed spasm is the most common type.
A cry may precede or follow the spasm, (that confuse with colic).

7
The clusters of seizures may persist for minutes.
Spasm occur before sleeping or
immediately after awakening.
Characteristic EEG changes called
(hypsarrhythmia).
Prognosis is poor.
Cryptogenic group(40%)good response to therapy without clear etiology.
Symptomatic type (60%)poor response to therapy with clear etiology (e.g. metabolic
like PKU ,congenital malformation of the brain , tuberous sclerosis,congnital
infection…etc.
Treatment
ACTH
steroid
Benzodiazepine
Valproic acid
Vegabatrine
Juvenile myoclonic epilepsy
A.D
Predominantly occur in the morning.
With or without generalized clonic &absence seizures.
Treatment with valproic acid but therapy must be maintained for life .
Laboratory evaluation of seizures
CBC
Blood chemistry:glucose,Ca,Na,K, Cl,HCO3,Mg, Ph .
Urea&creatinine
Blood&urine for toxicology screen.
In neonates blood for ammonia & inborn error of metabolism.
CSF analysis.
EEG & brain imaging.
Viral study specially for enterovirus.
Principles of seizure therapy
No need for long term treatment of benign febrile convulsion.
8
Therapy indicated for absence & atypical absence seizures , infantile spasm.
Single , cheap , less toxic drug is the goal that lead to better compliance.
Duration of therapy:
generalized tonic clonic ,tonic, clonic , absence &partial seizures not> than 2-4 yrs.
Myoclonic seizures , atypical absence , lennox-Gastaut treatment for life.
Risk for recurrence of seizures after discontinuation of therapy
Those children who are neurologically abnormal.
Those having seizures that were initially difficult to control.
Those having persistent epileptiform EEGs.
Acute ataxia
Abnormality of coordination resulting in impairment of direction , rate strength of
voluntary movement.
Usual symptoms are broad-based unsteady gait& tremor , that worsen by intentional
movement of limbs (dysmetria).
Defect in cerebellum and cerebellar pathways.
Etiology:
Post infectious :(chickenpox , infectious mononucleosis ,URTI)
Drug intoxication :(sedative-hypnotic associated with lethargy , carbamazepine &
phenytoin lead to only ataxia.
Tumors of posterior fossa: medulloblastoma , ependymoma.
Hydrocephalus.
Inborn error of metabolism: urea cycle defect , maple syrup urine.
Labyrinthine dysfunction.
Guillain-barré syndrome.
Corticospinal (upper) and neuromuscular (lower) loss of motor function
Upper:
This include brain stem, basal ganglia, spinal cord up to the anterior horn cell.
Loss of voluntary control but not total loss of movement.
Posture: arm flexed ,legs extended.
Tone ↑.
Reflexes ↑.

9
Babiniski:present.
Atrophy: absent.
Fasciculation: absent.
Lower:
This include AHC , motor root , peripheral motor nerve , neuromuscular junction &
muscles.
Total loss of movement.
Flaccid posture.
Tone ↓.
Reflexes ↓.
Babinski :absent.
Atrophy: possible.
Fasciculation :possible.
Diseases of UMN
Stroke in childhood:
Obstruction of the blood flow may occur in arteries or veins & may be caused by local
thrombosis or remobilization from distant site.
Cerebral embolization occur within seconds& associated with focal seizure , headache
& hemorrhagic infarction & the common sources are the heart and the carotid artery.
T I A : it precede the cerebral thrombosis that produced its full deficits in hrs.
Etiology:
Cyanotic heart diseases , Bacterial meningitis , chickenpox , vessel wall pathology , sickle
cell anemia , DIC , HUS , NS , liver disease, malignancy , polycythemia, factor V C S
deficiency, homocystinuria.
Cyanotic heart diseases:
Its important cause of stroke , 1-2% of infant with unrepaired CHD have cerebral A or V
emboli.
Predisposing factors:
Acute episode of sever cyanosis.
Febrile illness.
Dehydration.
Polycythemia.
Hyperventilation.

11
Iron deficiency anemia.
Sources of emboli:
S B E , mural thrombus , valvular diseases , atrial myxoma, cardiac catheterization , cardiac
surgery
Treatment
Complete stroke:donot benefit from medical treatment.
TIA and stroke in evolution:
Anticoagulant(heparin)
Oral warfarin.
Antiplatelate :aspirin , dipyridamole.
Thrombolysis by A or V catheters
Excise sources of emboli.