Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 1 of 14
Common Gynaecological Operation
Myomectomy
A myomectomy is an operation to remove fibroids while preserving the
uterus.
o
For women who have fibroid symptoms and want to have children in the
future, myomectomy is the best treatment option.
o
Myomectomy is very effective, but fibroids can re-grow )recurrence). The
younger the patient is and the more fibroids she has at the time of
myomectomy, the more likely is the recurrence in the future.
Indications:
1. Abnormal uterine bleeding, causing anemia
2. Severe pelvic pain
3. Large or multiple (Palpable per Abdomen)
4. Pressure Symptoms (Urinary tract symptoms)
5. Postmenopausal or rapid growth
6. Obscuring evaluation of adnexa
7. Indications in Infertility:
a. Deformity of Endometrial Cavity
b.Distortion of Fallopian Tubes
c. Fibroid associated with Unexplained Infertility
Approach:
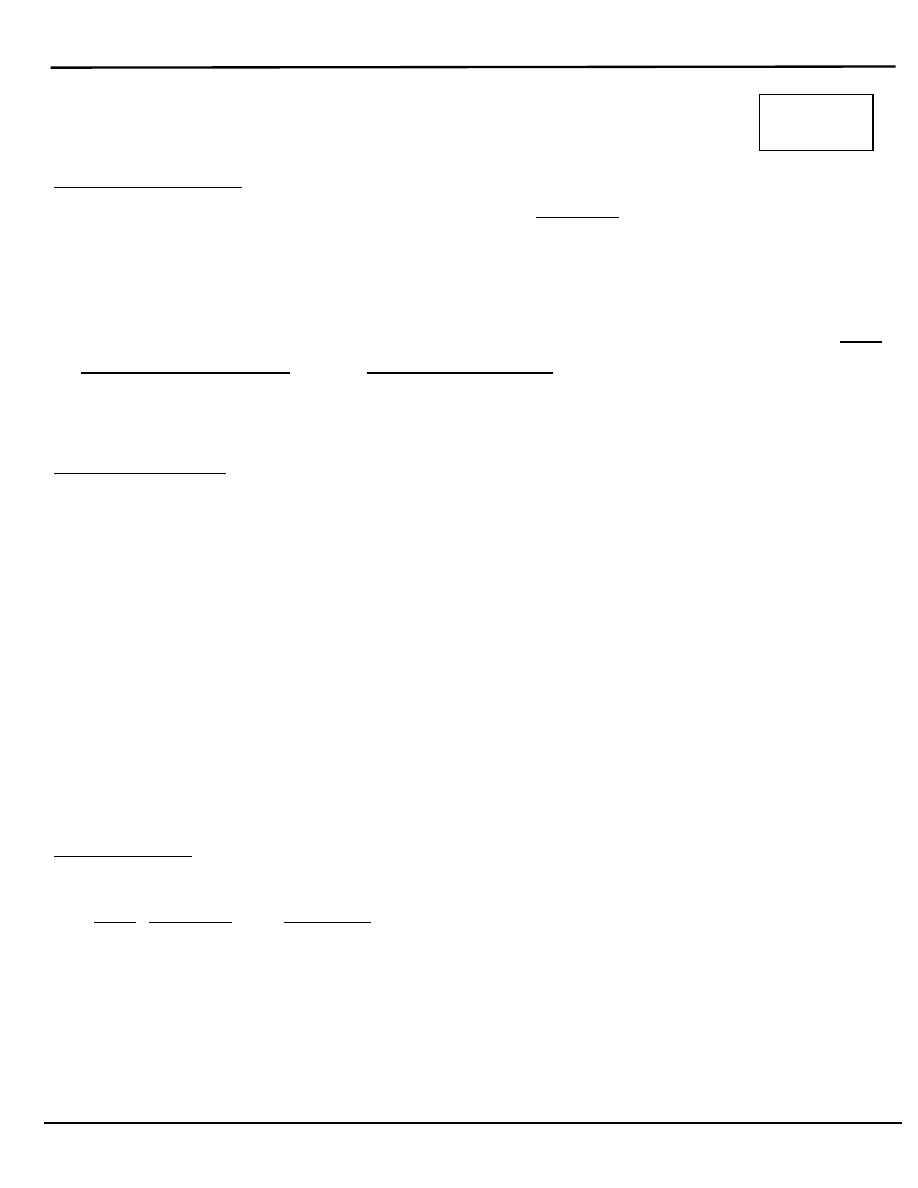
A myomectomy can be performed in several different ways depending on
the size, number and location of the fibroids:
1. Abdominally (open)
2. Laparoscopic
3. Hysteroscopic Primarily for submucosal fibroids
4. Vaginal Primarily for pedunculated submucous fibroids
16/4/2014
( :العدد
7
)
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 2 of 14
Abdominal Myomectomy
:
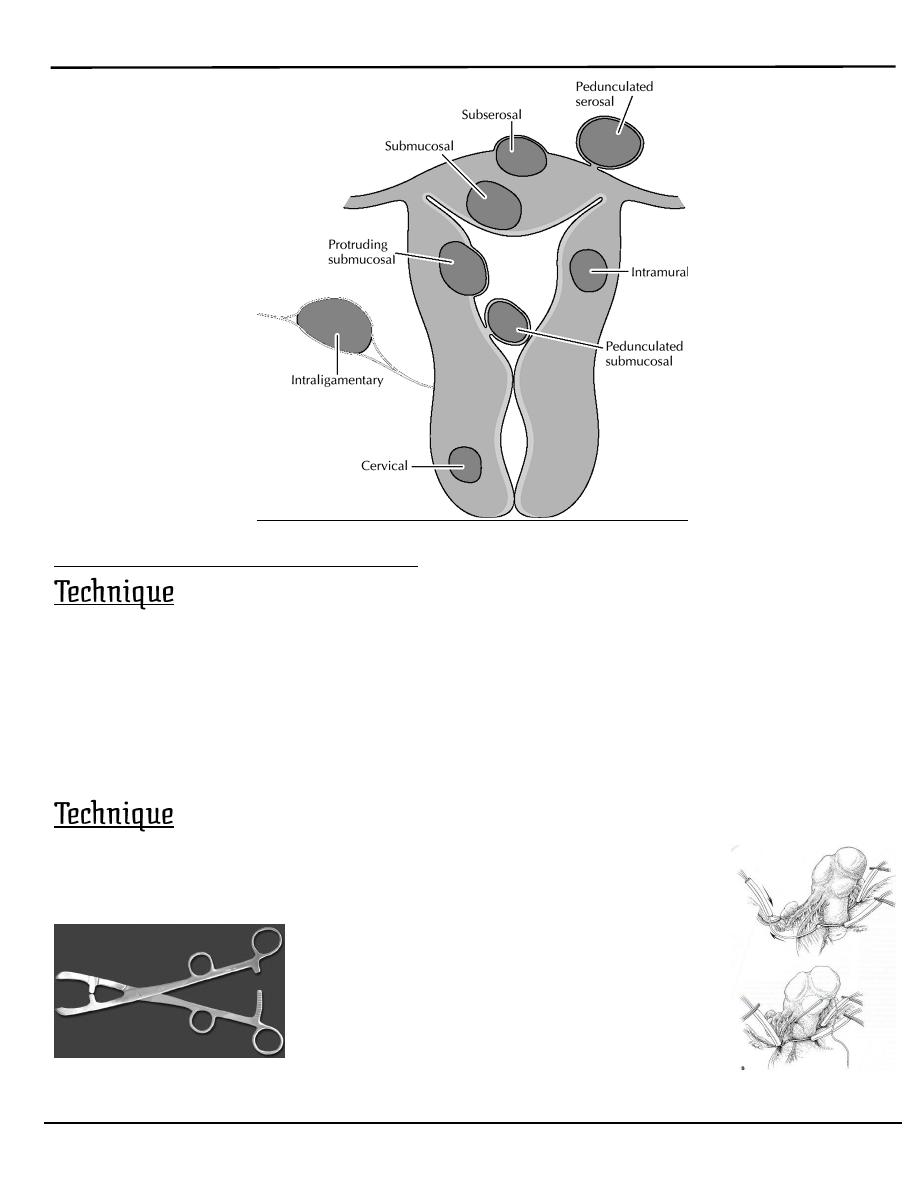
1. Localization of myoma.
2. Non- crushing clamp or Torniquet.
3. Anterior midline incision.
4. enucleation.
5. Repairing the defect.
o
Place non crushing clamp across the ovarian and uterine
arteries to minimise blood loss or use a tourniquet.
Bonney-1920’s – Uterine Artery Clamp
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 3 of 14
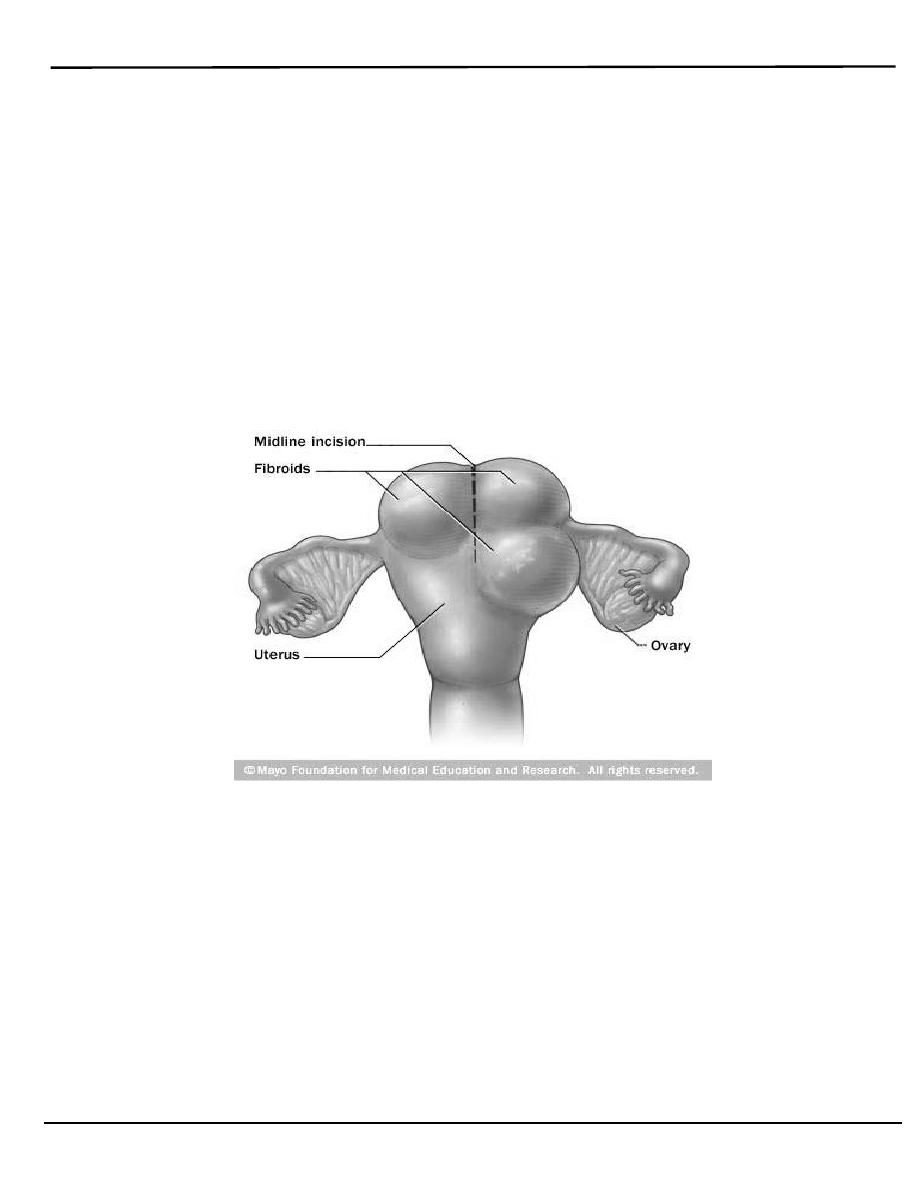
o
Attempt to remove all fibroids through a single midline incision if possible
(Avoids vascular structures laterally. An anterior incision is preferred to
minimize the risk of later adhesion of bowel & retroversion. ).
o
Tissue surrounding the fibroid is compressed tightly forming a
pseudocapsule
No vascular bundle enters the myoma
Identification of and dissection along this plane will minimize blood
loss
Cleavage planes may be altered in those who have been pretreated
with GnRH analogue.
o
Palpate the uterus for any remaining fibroids.
Remove all myomas with single anterior midline incision is the choice
o
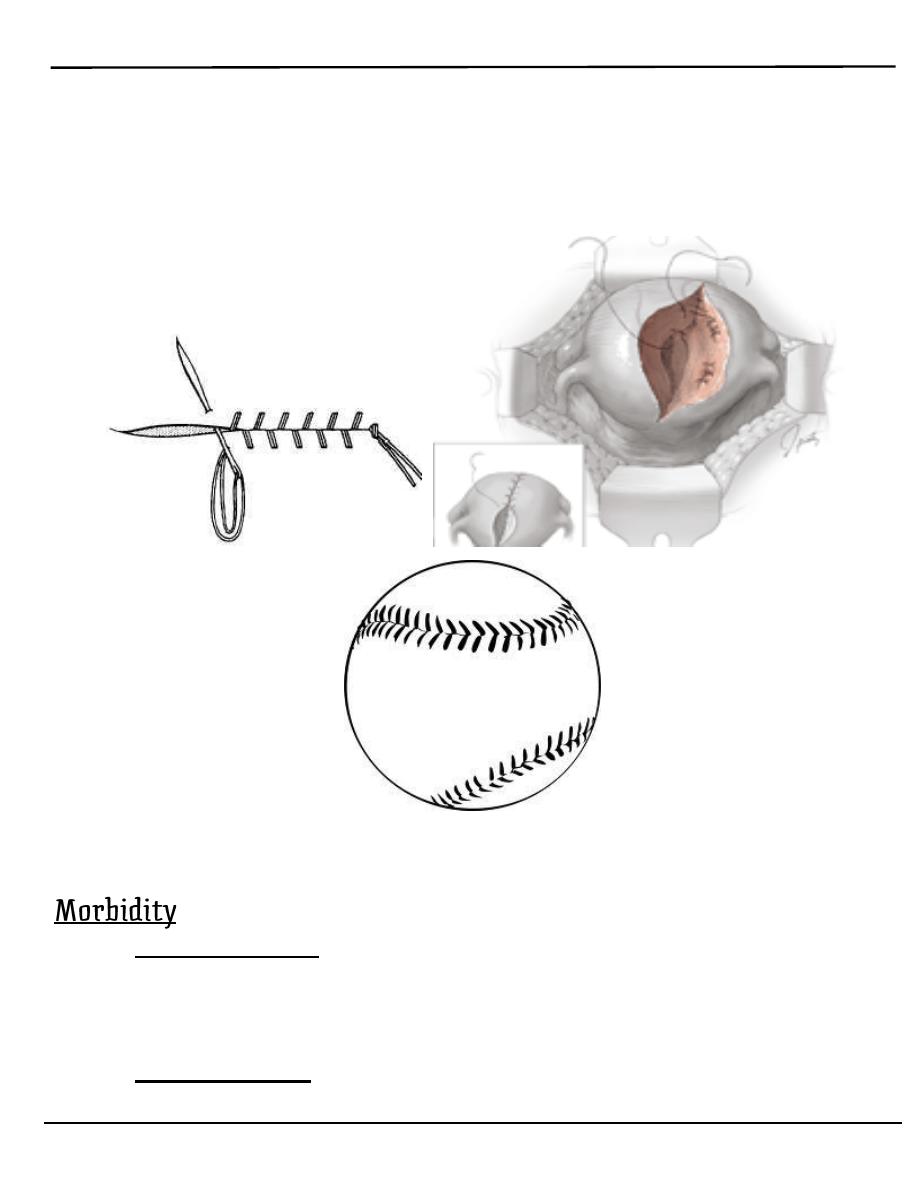
Repairing defect
Multi layered approach
Deep sutures to close dead space
Second imbricating layer
Close serosa with a “baseball stitch”
May require removal of excess myometrial tissue to allow
adequate closure
o
Apply a sheet of adhesive barrier over the incision line to avoid adhesion
formation.
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 4 of 14
o
Repairing the defect by multilayered Approach.
Deep space suturing
Second imbricating layer
Serosa with baseball suturing
Baseball like suturing
A. Intra operative:
1. Haemorrhage
2. Visceral Damage
3. Need for Hysterectomy
B. Post-operative:
Myoma Fever – 33%
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 5 of 14
C. Sequelae:
1. Recurrence / Retreatment – 4-27%
2. Adhesions
3. Uterine Rupture in Labour (Rare)
Biggest complication is blood loss
1. Reputation as “bloody” operation
2. Fibroid recurrence is possible risk
3. Adhesion formation
4. “Hysterectomy usually is a simpler procedure than multiple
myomectomy, as well as the procedure to which most gynecologists
are more accustomed”
(Te Linde: Operative Gynecology, Seventh Edition)
1. Ureteral injury (0.1 - 0.5%).
2. Changes in libido (25-33%) and orgasm.
3. Depression.
4. Decreased time to ovarian failure.
Laparoscopic Myomectomy
Limitations of laparoscopic myomectomy:
1. Special Equipment & Special skill required
2. Difficult in:
3. Broad Ligament / Cervical/ deeply embedded
4. Size >8cm
5. Number >3 fibroids
6. Separate incisions needed
7. Closure of dead space & haemostasis difficult
8. Weaker scar
9. Increased Operating Time & Blood Loss
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 6 of 14
10. Inherent Complications of Laparoscopic surgery
Hysterectomy
o
A hysterectomy is an operation to remove a woman's uterus.
o
A woman may have a hysterectomy for different reasons, including:
1. Uterine fibroids that cause pain, bleeding, or other problems
2. Uterine prolapse,
3. Cancer of the uterus, cervix, or ovaries
4. Severe and intractable endometriosis and/or adenomyosis after
pharmaceutical or other surgical options have been exhausted.
5. Abnormal vaginal bleeding that persists despite treatment
6. Chronic pelvic pain, after pharmaceutical or other surgical options have
been exhausted.
7. Postpartum to remove either a severe case of placenta praevia or
placenta percreta, as well as a last resort in case of excessive obstetrical
haemorrhage
Hysterectomy, in the literal sense of the word, means merely removal of
the uterus. However other organs such as ovaries, fallopian tubes and the
cervix are very frequently removed as part of the surgery.
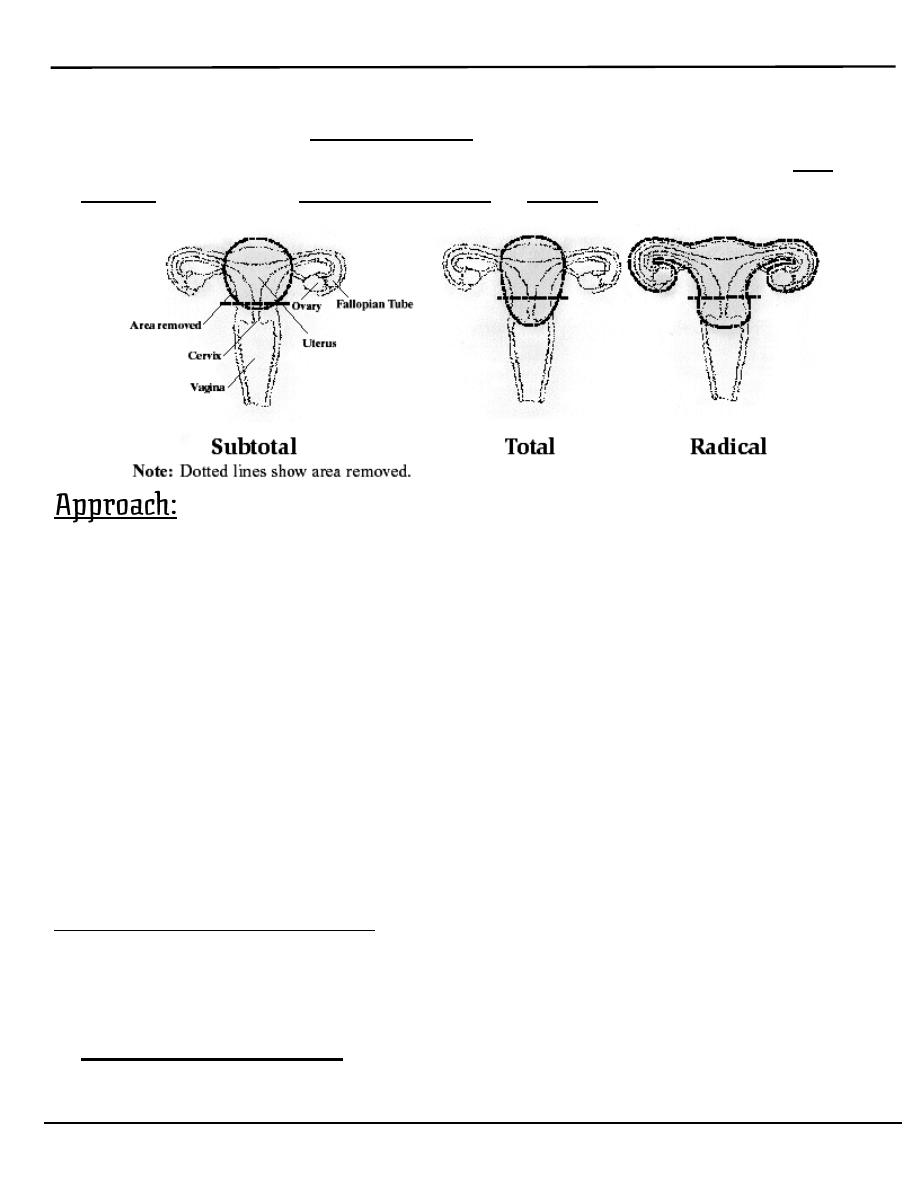
1. Radical hysterectomy or Wertheim’s hysterectomy: complete removal
of the uterus, cervix, upper vagina, and parametrium. Indicated for cancer.
Lymph nodes, ovaries and fallopian tubes are also usually removed in this
situation.
2. Total hysterectomy: Complete removal of the uterus and cervix.
3. Subtotal hysterectomy: removal of the uterus, leaving the cervix in situ.
Despite speculation that there might be different sexual outcomes
depending on
whether hysterectomy was subtotal, or total abdominal, this difference has
not been supported by recent studies
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 7 of 14
It is obvious that supracervical hysterectomy does not eliminate the
possibility of having cervical cancer since the cervix itself is left intact.
Those who have undergone this procedure must still have regular Pap
smears to check for cervical dysplasia or cancer
There are several approaches that can be used for hysterectomy:
1. Abdominal hysterectomy
2. Vaginal hysterectomy
3. Laparoscopic-assisted vaginal hysterectomy: Using laparoscopic
surgical tools, a surgeon removes the uterus through an incision in the
vagina.
4. Robot-assisted laparoscopic hysterectomy: This procedure is similar
to a laparoscopic hysterectomy, but the surgeon controls a sophisticated
robotic system of surgical tools from outside the body. Advanced
technology allows the surgeon to use natural wrist movements and view
the hysterectomy on a three-dimensional screen.
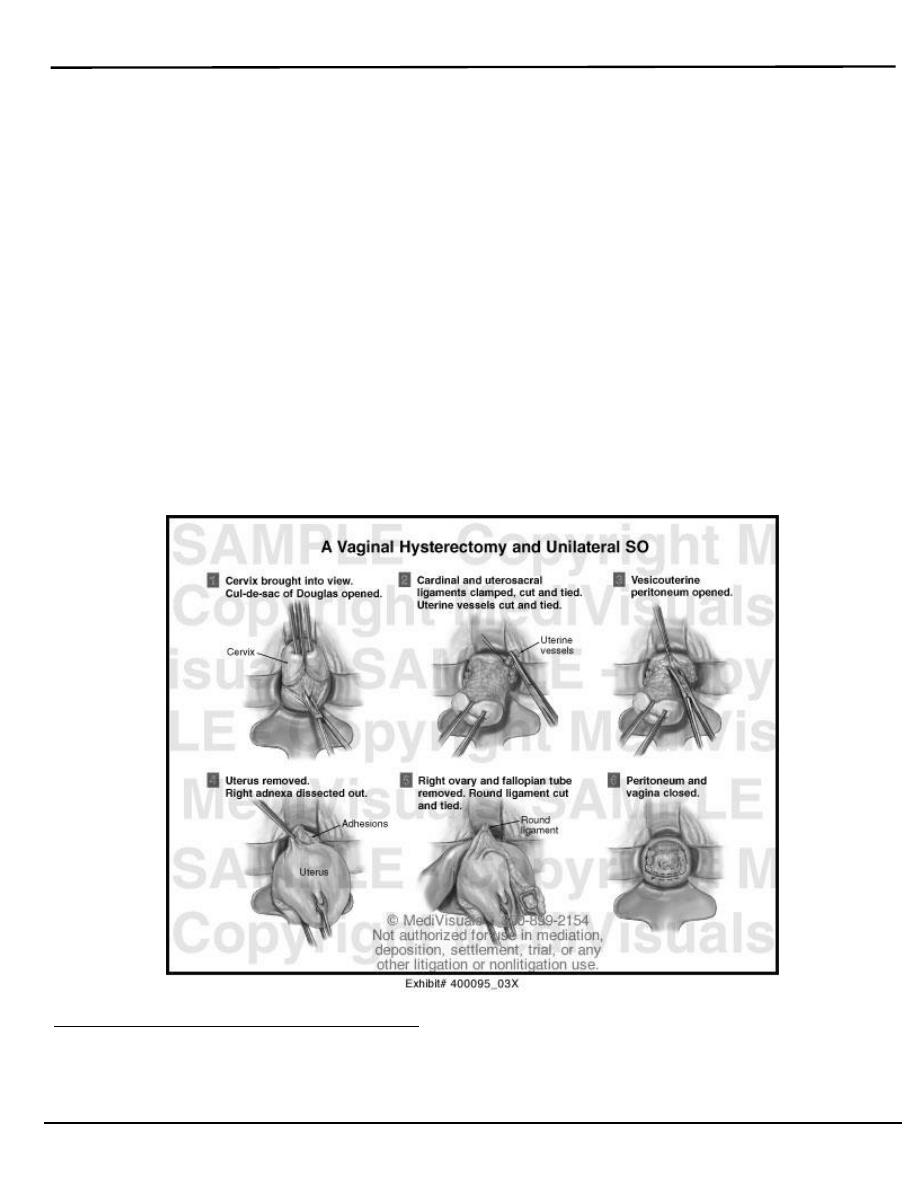
Vaginal hysterectomy:
o
The main indication is second or third degree uterine prolapse.
o
There is trend nowadays to prefer vaginal to abdominal hysterectomy
because the morbidity &postoperative discomfort are less.
o
The contraindications:
1. Presence of genital tract malignancy
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 8 of 14
2. A uterus larger than 14 weeks in size
3. Narrow subpubic arch
4. Previous abdominal procedures where
5. bowel may be adherent to uterus or tubes
6. Uncertain ovarian pathology
o
The epithelium around the cervix is circumscribed ,the bladder freed
&dissected upwards &the uterovesical peritoneal pouch is entered .
o
The cervix is lifted forwards &peritoneum of the rectouterine pouch of
Douglas identified & opened, the uterosacral ligaments are ligated.
o
Next the uterine artery &cardinal ligaments are identified & ligated.
o
Finally the ovarian pedicles are similarly identified & ligated.
o
The uterus is removed & associated anterior or posterior vaginal wall
prolapse are repaired &the vault closed.
Abdominal hysterectomy:
The same pedicles as in vaginal hysterectomy are clamped but in reverse
order i.e. ovarian followed by uterine, followed by cardinal ligaments.
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 9 of 14
1. Patient is supine under GA.
2. Skin incision:
a. Transverse lower abdominal incision.
b. Vertical incision.
o
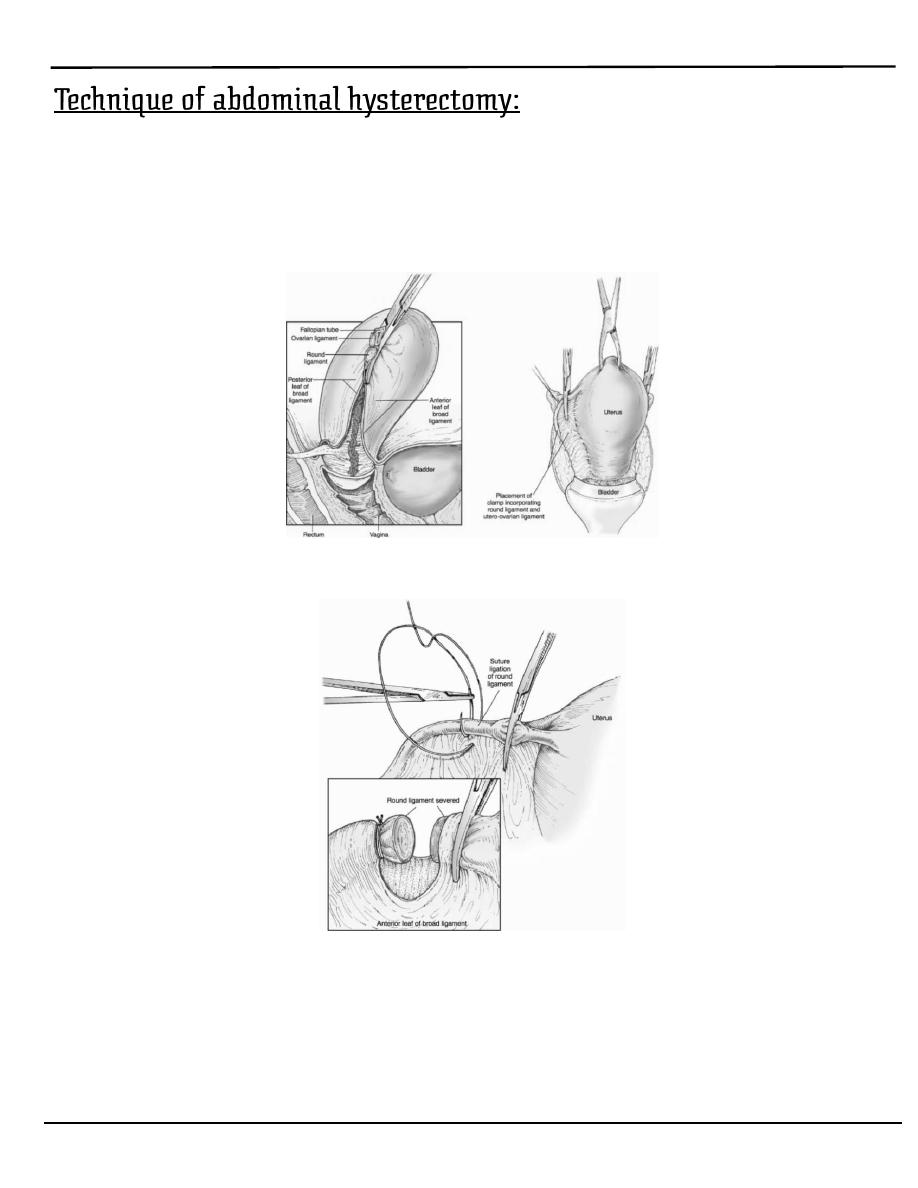
The uterus is elevated & clamps placed across the broad ligament.
the round ligament is clamped, incised and ligated .
o
The round ligament is transected and the broad ligament is incised
and opened.
the peritoneum lateral to the infundibulopelvic ligament is
incised exposing the ureter and the vesicouterine pouch is
opened reflecting the bladder away from the uterus ,the ovarian
ligament is clamped ,incised and ligated.

Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 10 of 14
o
The incision in the anterior broad ligament is extended along the
vesicouterine fold.
o
Ligation of the utero–ovarian ligament
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 11 of 14
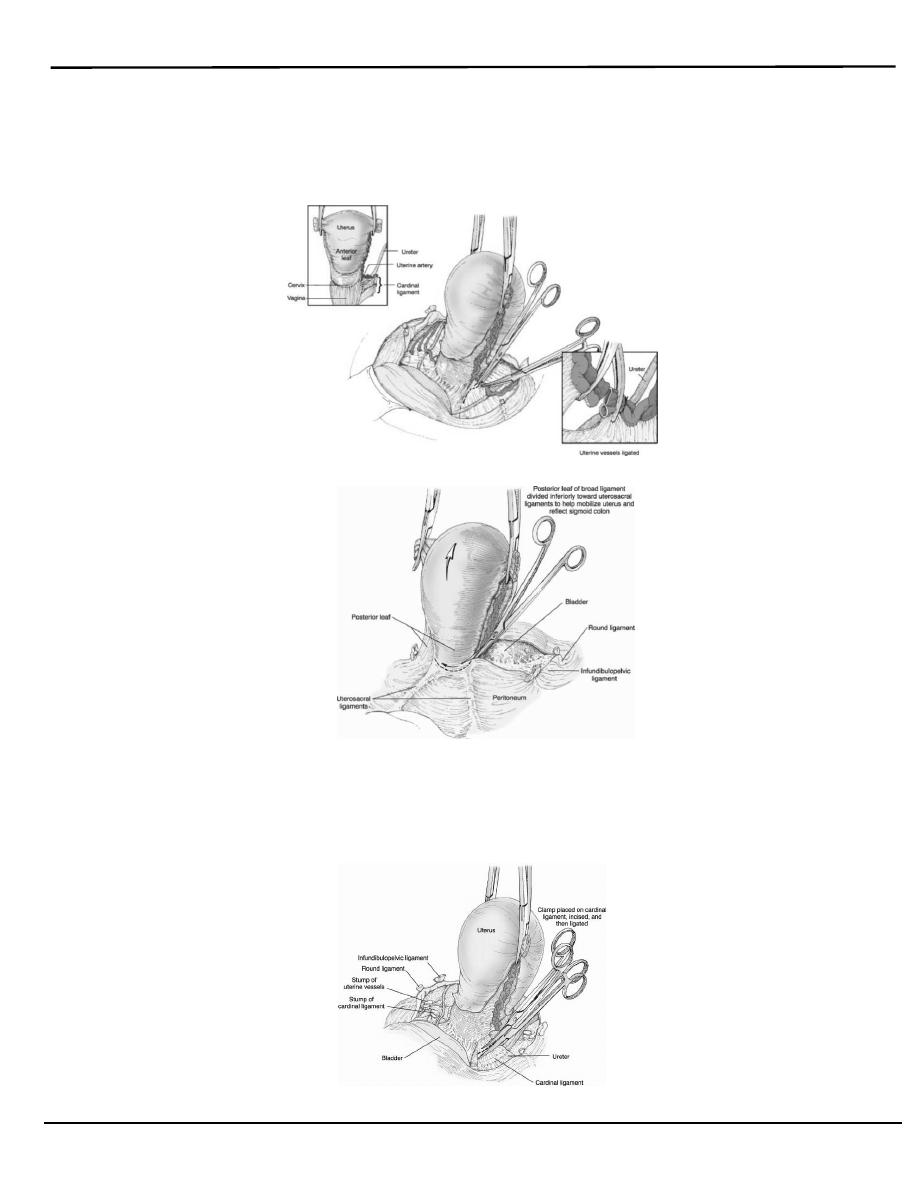
o
Dissection of the vesicouterine plane to mobilize the bladder.
medioposterior leaf of the broad ligament is incised
exposing the uterine artery.
-The uterine artery is clamped and ligated at the level of the internal os.
o
Ligation of the uterine blood vessels.
o
Incision of the rectouterine peritoneum and mobilization of the
rectum from the posterior cervix.
The cardinal ligament is clamped ,incised and ligated medial
to the uterine artery and also the uterosacral ligament .
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 12 of 14
o
Ligation of the cardinal ligament.
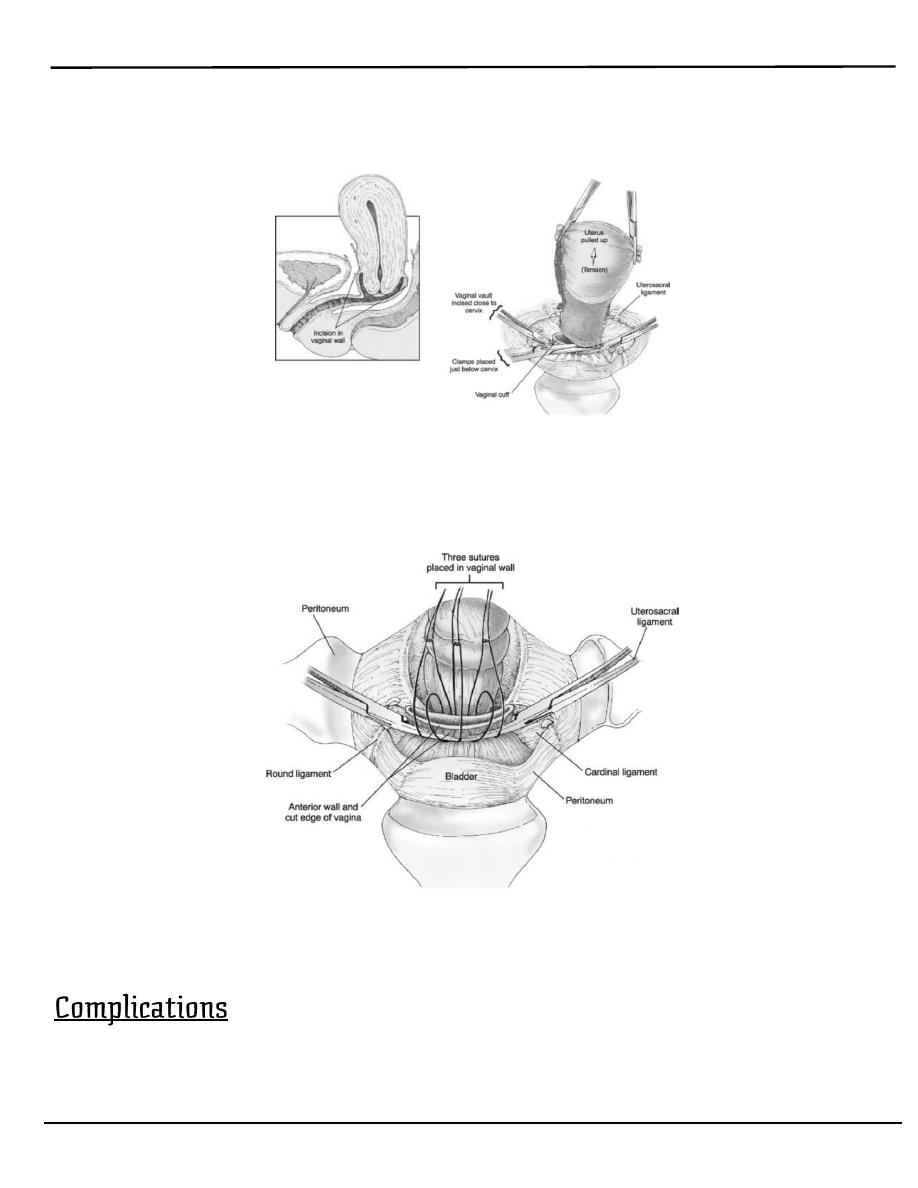
The uterus with the cervix is removed by cutting across the
vagina just below the cervix.
o
Removal of the uterus by transection of the vagina.
the vaginal cuff is normally closed with absorbable sutures incorporating the
uterosacral and the cardinal ligament to prevent development of vaginal vault
prolapse .
o
Vaginal cuff closure incorporating the uterosacral and cardinal
ligaments.
1. Anaesthesia complications
2. Primary haemorrhage due to slip ligature
3. Secondary haemorrhage due to infection
Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 13 of 14
4. Damage to ureter, bladder, or bowel
5. Infection with pelvic abscess
6. Late; adhesion with intestinal obstruction.
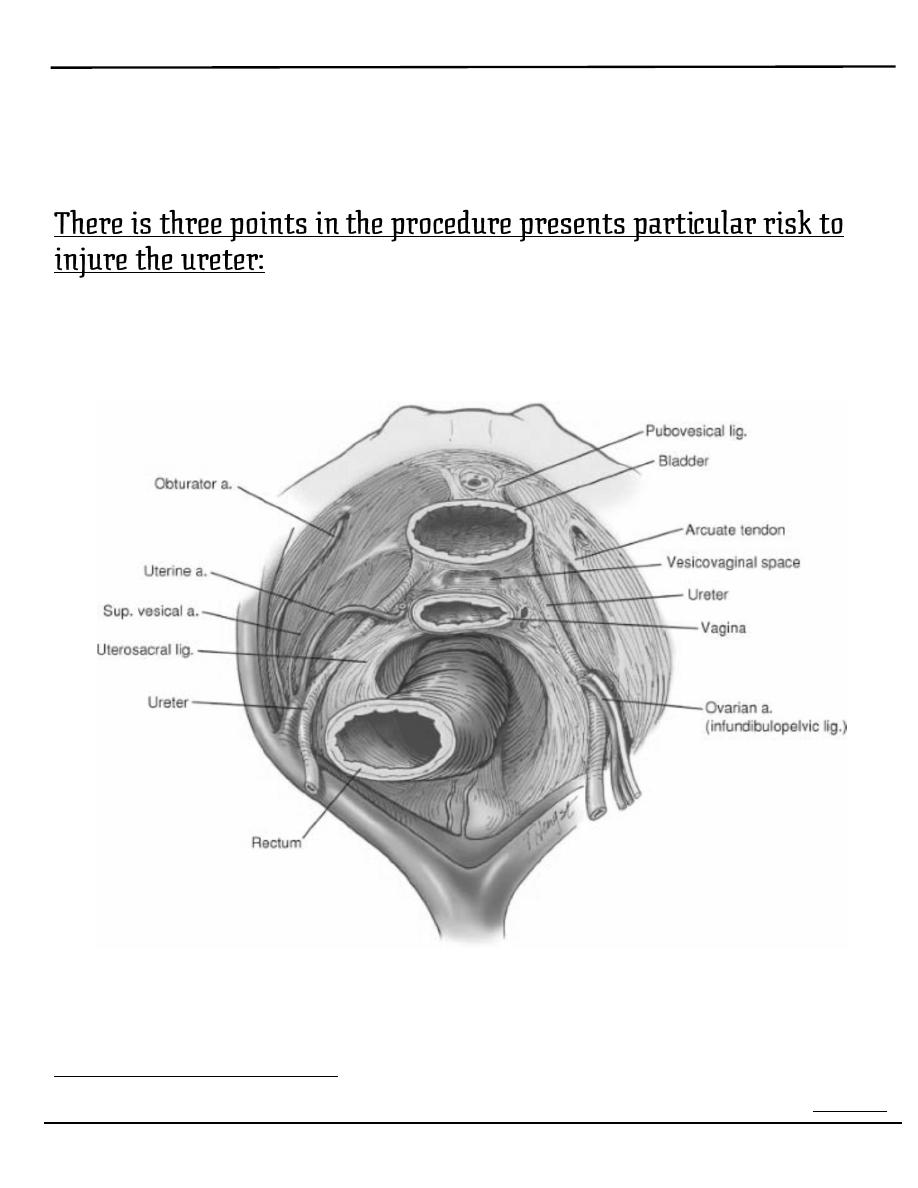
1. As the infundibulopelvic ligament are clamped incised and clamped.
2. As the uterine vessels are ligated.
3. As the cardinal ligament is ligated if the bladder is not reflected
inferiorly enough.
The course of the ureter and its relationship to the sites of greatest
vulnerability.
Ovarian Cystectomy
o
Enucleation of a cyst from the overy is frequently carried out for benign

Lecture 2
النسائية
د
.
براء لقمان
Common Gynaecological Operation
Page 14 of 14
cyst in women below 40 years of age.
o
The incision into the ovarian capsule must be made very carefully to
prevent rupture of the cyst.
o
Once the cyst is enucleated,the ovary is carefully recostructed with
meticulous hemostasis to avoid ovarian hematoma.