
1
Third stage
Medicine
Lec-2
د
.
وائل
1/1/2014
Obesity
Obesity is widely regarded as a pandemic, with potentially disastrous consequences for
human health.
There is increasing public awareness of the health implications of obesity. Many patients
will seek medical help for their obesity, others will present with one of the complications
of obesity, and increasing numbers are being identified during health screening
examinations
Complications of obesity:
1. 'Metabolic syndrome‘:Type 2 diabetes, Hypertension, dyslipidaemia and central
obesity which lead to increase risk of Coronary heart disease,stroke, and
complication of diabetes.
2. Liver fat accumulation:Non-alcoholic steatohepatitis(NASH),cirrhosis.
3. Restricted ventilation:Exertional dyspnoea, Sleep apnoea, Respiratory failure
(Pickwickian syndrome).
4. Mechanical effects of weight:Urinary incontinence,Osteoarthritis,Varicose veins.
5. Increased peripheral steroid interconversion in adipose tissue:Hormone-dependent
cancers (breast, uterus),Polycystic ovary syndrome (infertility, hirsutism)
6. Others:Psychological morbidity (low self-esteem, depression), Socioeconomic
disadvantage (lower income, less likely to be promoted), Gallstones, Colorectal
cancer, Skin infections (groin and submammary candidiasis; hidradenitis).
For some complications of obesity, the distribution rather than the absolute amount of
excess adipose tissue appears to be important. Increased intra-abdominal fat causes
'central' ('abdominal', 'visceral', 'android' or 'apple-shaped') obesity, which contrasts with
subcutaneous fat accumulation causing 'generalised' ('gynoid' or 'pear-shaped') obesity; the
former is more common in men and is more closely associated with type 2 diabetes, the
metabolic syndrome and cardiovascular disease.
Aetiology:
Accumulation of fat results from a discrepancy between energy consumption and energy
expenditure which is too large to be defended by the hypothalamic regulation of BMR. A
continuous small daily positive energy balance of only 0.2-0.8 MJ (50-200 kcal; < 10% of
intake) would lead to weight gain of 2-20 kg over a period of 4-10 years. Given the
cumulative effects of subtle energy excess, body fat content shows 'tracking' with age such
that obese children usually become obese adults. Weight tends to increase throughout
adult life, as BMR and physical activity decrease .
2
Reversible causes of obesity and weight gain:
1. Endocrine factors:
Hypothyroidism
Cushing's syndrome
Insulinoma
Hypothalamic tumours or injury
2. Drug treatments:
Tricyclic antidepressants
Sulphonylureas
Oestrogen-containing contraceptive pill
Corticosteroids
Sodium valproate
β-blockers
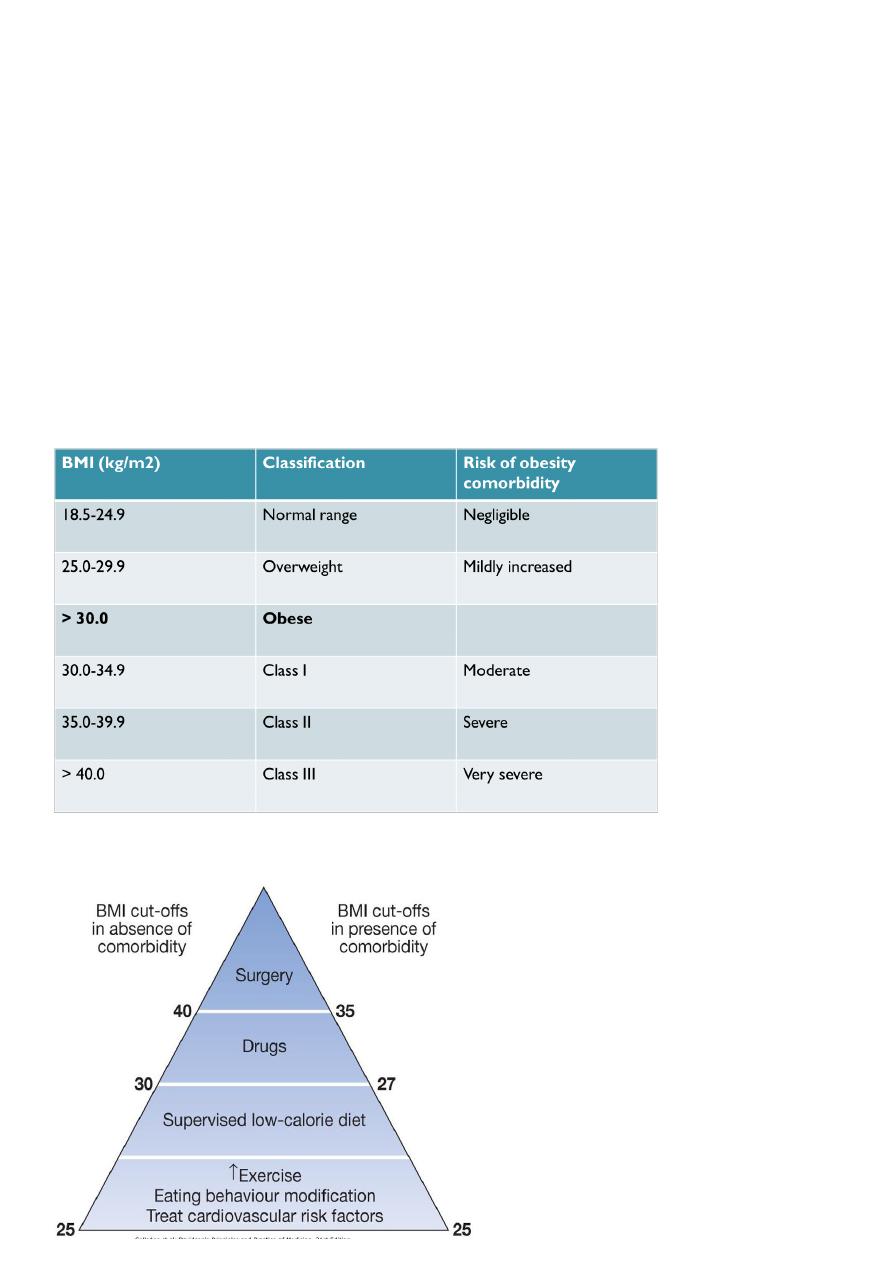
Quantifying obesity with body mass index (weight/height2):
Management:
3
1) Lifestyle advice :Regular eating patterns and maximising physical activity are advised.
2) Weight loss diets :
3) Drugs:Currently recommended:
A. Orlistat:a Pancreatic lipase inhibitor
B. Sibutramine,a Serotonergic in CNS.
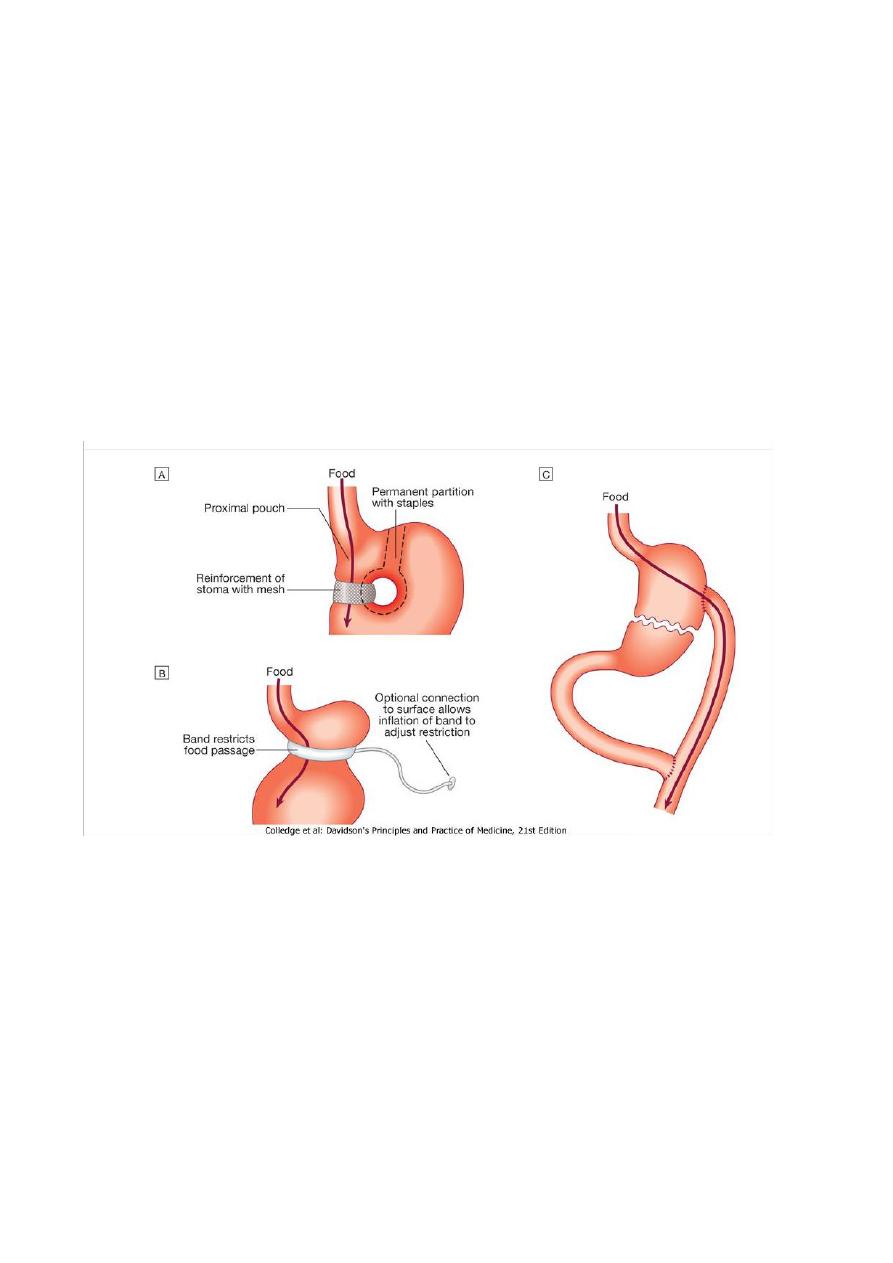
4) Surgery:'Bariatric' surgery to reduce the size of the stomach is by far the most effective
long-term treatment for obesity and is the only anti-obesity intervention that has been
associated with reduced mortality. Bariatric surgery should be contemplated in
motivated patients who have very high risks of complications of obesity , in whom
extensive dietary and drug therapy has been inadequately effective.
5) Treatment of additional risk factors : Obesity must not be treated in isolation and
other risk factors must be addressed, including smoking, excess alcohol consumption,
diabetes mellitus, hyperlipidaemia and hypertension.