1
Third stage
Medicine
Lec-1
د
.
خالد
نافع
1/1/2014
PRINCIPLES OF HEMATOLOGICAL DIAGNOSIS
1.HISTORY
I-Medical history
o The present illness, focus on the following:
Bleeding.
Infection or symptoms related to enlargement of L.N , LIVER or the SPLEEN.
Non-specific symptoms related to ANAEMIA:Malaise , weakness, headache &
weight loss.
o Any exposure to drugs or chemical.
o Review of systems; including the nervous system, is necessary as blood dyscrasia effect
many, if not all, organ systems .
II- Family history; information about the health of other family members as well as the
ethnic background .
2- PHYSICAL EXAMINATION
A- Thorough physical exam. Should focus on; SKIN, MOUTH ,MUCOUS MEMBRANE,& EYES.
JAUDICE
PALLOR
PETECHIAE & ECCYMOSIS.
ULCERS
B- Hepatomegaly, splenomegaly,enlarged or tender L.N ,soreness over the ribs or sternum
& variety of neurological abnormalities.
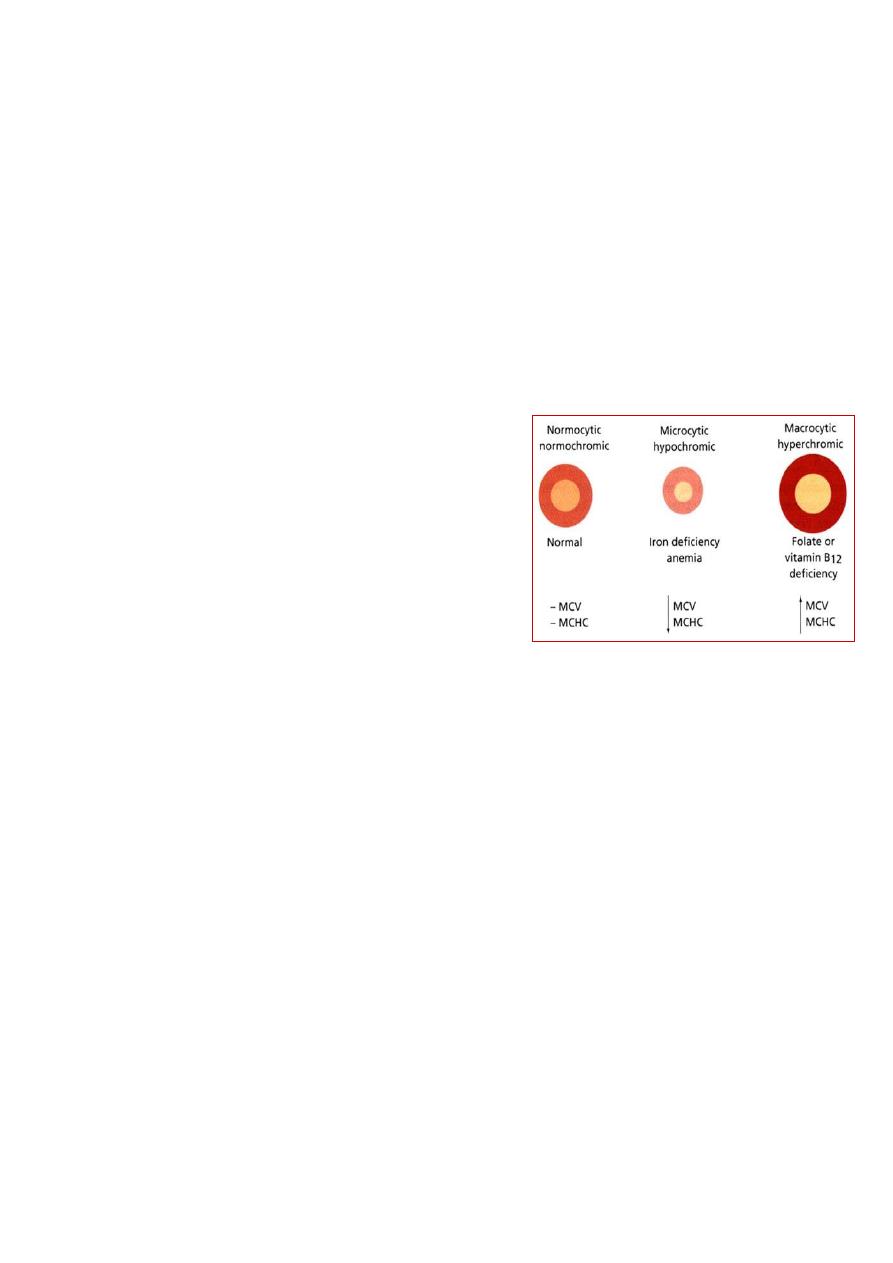
ANAEMIA
A-Symptoms & signs pertaining to anaemia.
1-Non-specific symptoms include; fatigue, weakness, shortness of breath & symptoms of
CHF
2-Signs include ; Pallor ,tachycardia , splenomegaly in minority of cases.Venous hum in
severe anaemia ( Hb < 4 gm/dl).Functional systolic murmur.
SYMPTOMS & SIGNS Specific To IRON deficiency
Pica: compulsive ingestion of non-nutrient substance (clay/ ice-pagophagia)
1- Atrophic changes in the epithelium; oral lesions;
I- Angular cheilosis; soreness & cracking in the corners of the lips.
II-Atrophy of the tongue papillae with intermittent glossitis
III-Stomatitis ; inflammation & soreness of of the tongue & mouth.
2-DYSPHAGIA.
3- Nail lesions; thinning & flattening of the nails progress to brittle & spoon-shaped nail (
koilonychia)
2
ANAEMIA
• Clinical: Weakness, Fatigue, Pallor
• Decreased Oxygen Carrying Capacity of Blood
• Result of: Decreased Number, Size, or HgB Content of RBC’s or of Defective HgB
• Secondary to:
– Nutritional / Iron Defeciency
– RBC loss or destruction (Chronic Bleeding)
– Failure of RBC formation (Leukemia)
– Hereditary HgB malformation
• Oral Features:
– Pallor
– Bald Tongue
• Possible Association with other Disease: Leukemia, Kidney Disease, etc.
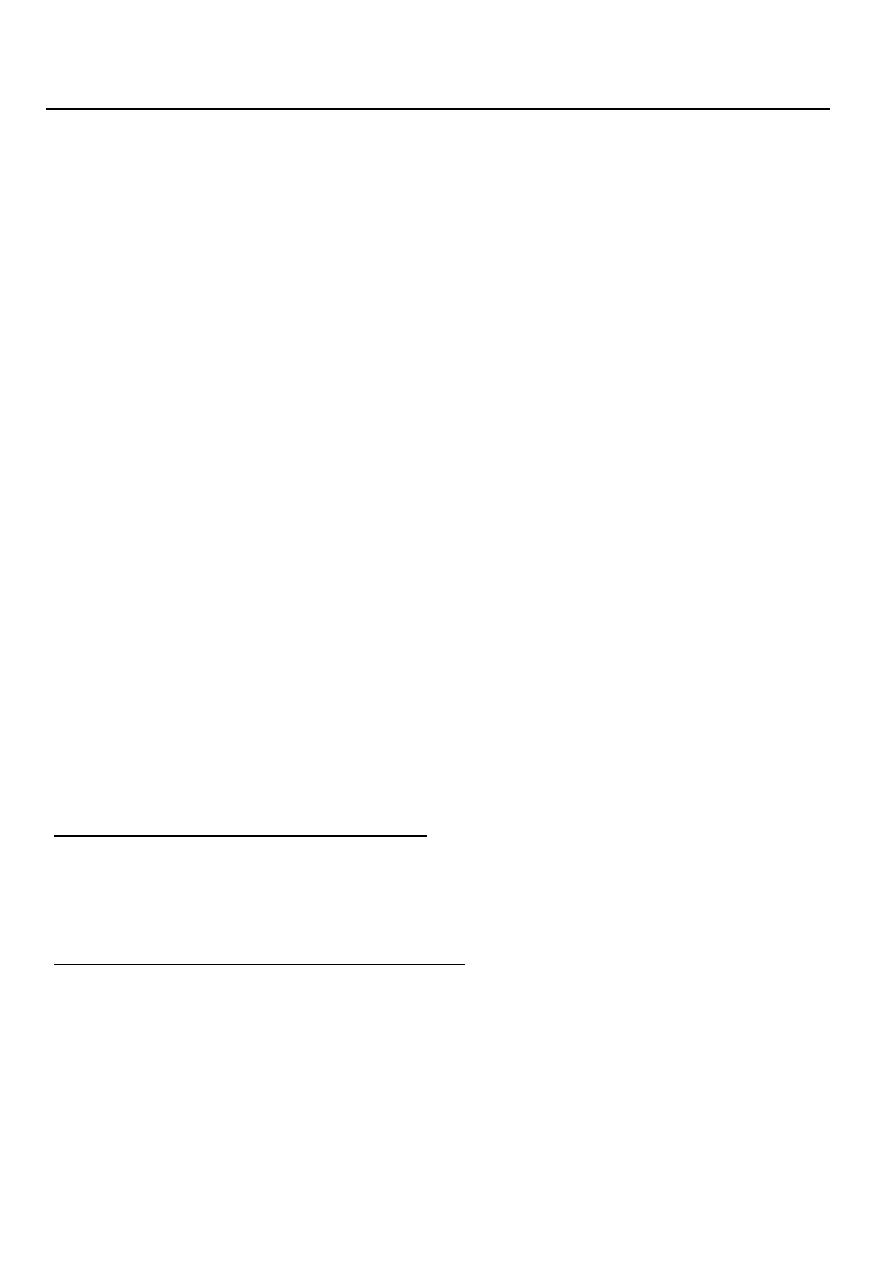
Anemia Classification
• Size of RBC’s
– Microcytic (Small)
– Macrocytic (Large)
– Normocytic (Normal Size)
• Concentration of Hgb
– Hypochromic (Less)
– Hyperchromic (More)
– Normochromic (Normal)
• Microcytic / Hypochromic
– Chronic Blood Loss, Iron Deficiency, Thalassemia
• Macrocytic (Megaloblastic) / Hyperchromic
– Vit B12 (Pernicious) or Folic Acid Deficiency
• Normocytic / Normochromic
– Hemolytic, Aplastic, Myelophthisic, Acute Blood Loss, Chronic Renal Failure
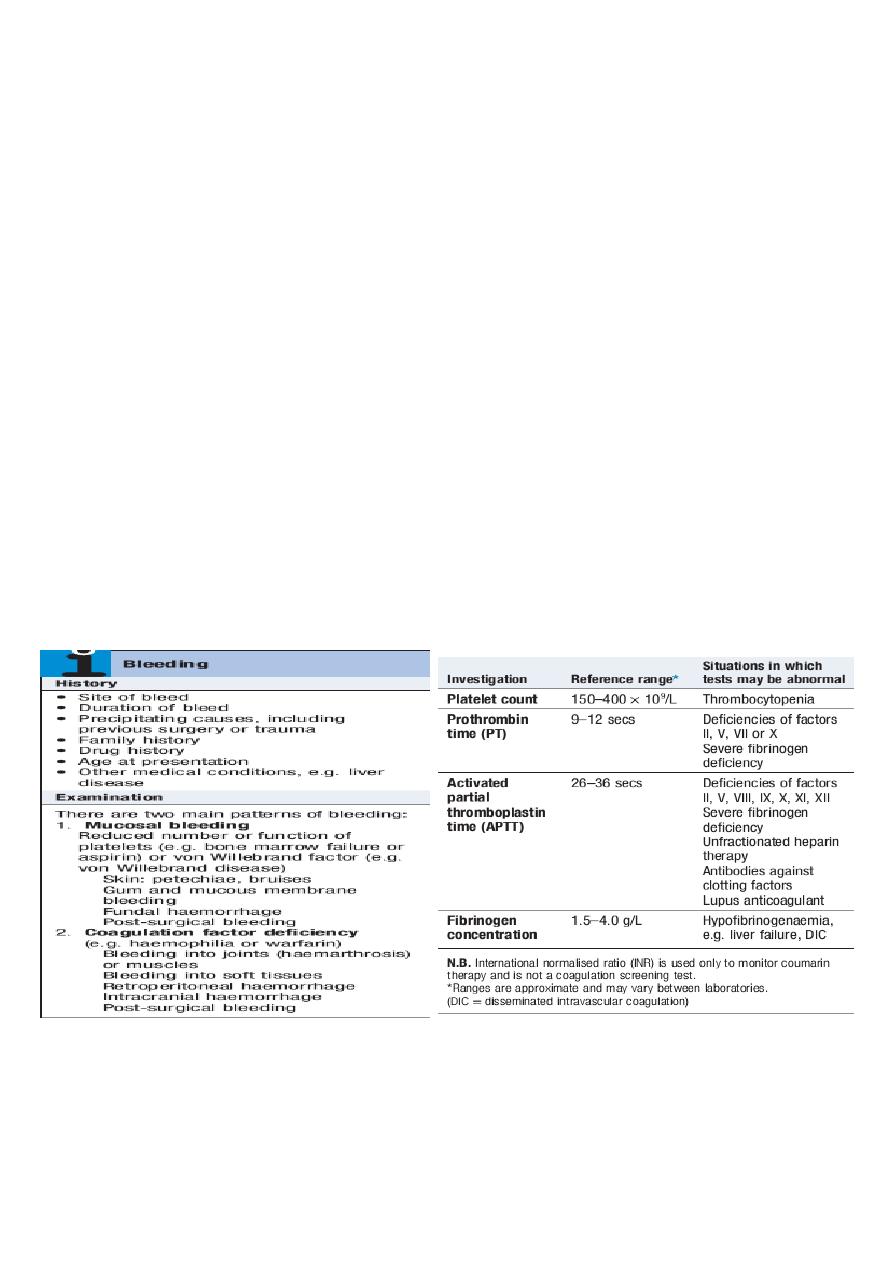
PLATELETS
NORMAL PLATELET COUNT 150-400X109/L
PLATELET disorders; Defect in count
THROMBOCYTOPENIA
Defect in function
THROMBOASTHENIA.
CLINICAL MANIFESTATIONS;
1-PETECHIAE.
2-PURPURA
3-ECCHYMOSIS(BRUSIES)
4- HAEMATOMA

3
From other lecture
Anaemia
Anaemia refers to a state in which the level of haemoglobin in the blood is below the
reference range appropriate for age and sex.
Other factors, including pregnancy and altitude, also affect haemoglobin levels and
must be taken into account when considering whether an individual is anaemic.
The clinical features of anaemia reflect diminished oxygen supply to the tissues .
A rapid onset of anaemia (e.g. due to blood loss) causes more profound symptoms
than a gradually developing anaemia.
Individuals with cardiorespiratory disease are more susceptible to symptoms of
anaemia.
Causes of anaemia
Clinical assessment
Iron deficiency anaemia is the most common type of anaemia worldwide. A thorough
gastrointestinal history is important, looking in particular for symptoms of blood loss.
Menorrhagia is a common cause of anaemia in premenopausal females, so women
should always be asked about their periods.
A dietary history should assess the intake of iron and folate, which may become
deficient in comparison to needs (e.g. in pregnancy or during periods of rapid growth).
Past medical history may reveal a disease which is known to be associated with
anaemia, such as rheumatoid arthritis (anaemia of chronic disease), or previous
surgery (e.g. resection of the stomach or small bowel, which may lead to
malabsorption of iron and/or vitamin B12).
Family history and ethnic background may raise suspicion of haemolytic anaemias,
such as the haemoglobinopathies and hereditary spherocytosis. Pernicious anaemia
may also be familial.
A drug history may reveal the ingestion of drugs which cause blood loss (e.g. aspirin
and antiinflammatory drugs), haemolysis (e.g. sulphonamides) or aplasia (e.g.
chloramphenicol).
4
Specific findings related to the aetiology of the anaemia
A patient may be found to have a right iliac fossa mass due to an underlying caecal
carcinoma.
Haemolytic anaemias can cause jaundice.
Vitamin B12 deficiency may be associated with neurological signs, including peripheral
neuropathy, dementia and signs of subacute combined degeneration of the cord.
Sicklecell anaemia may result in leg ulcers, stroke or features of pulmonary
hypertension.
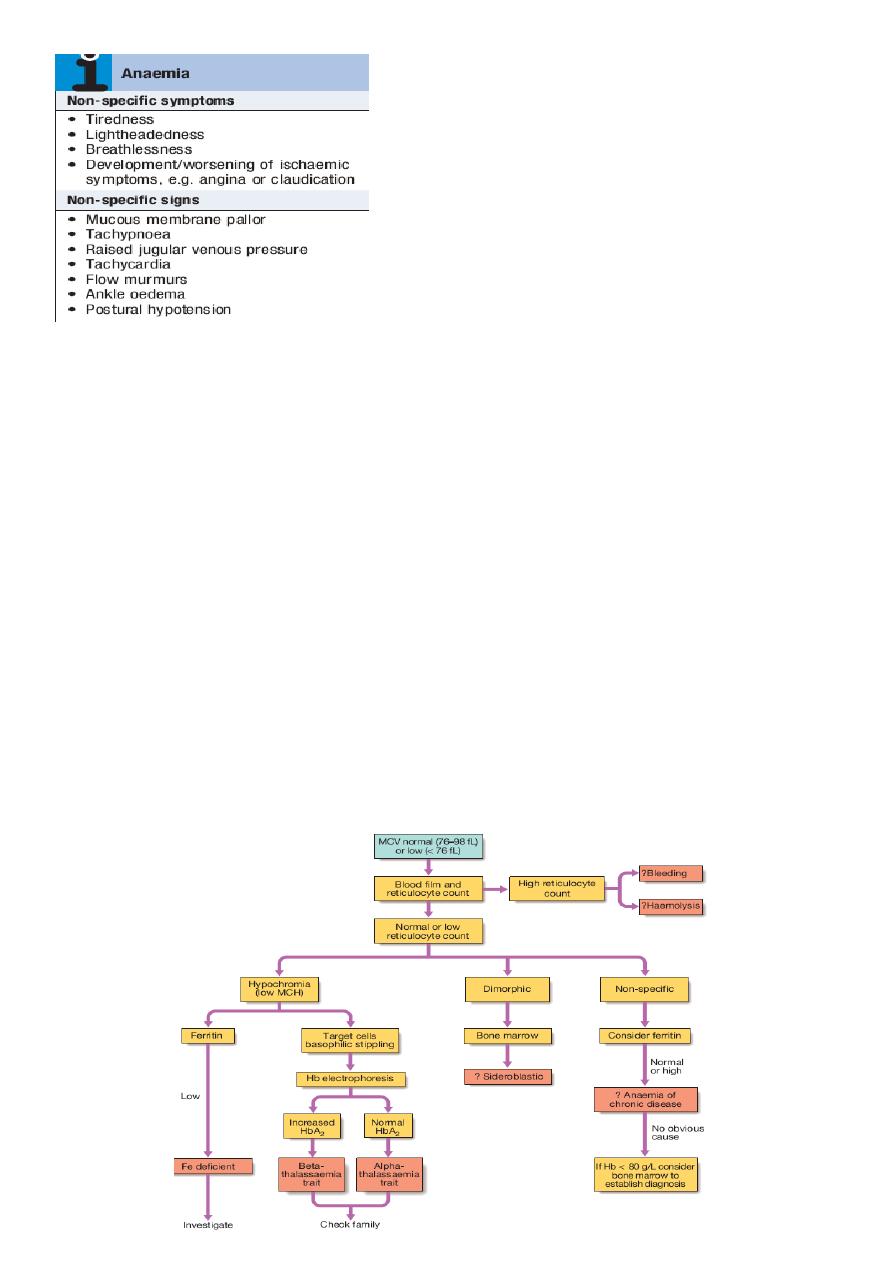
Investigations
Schemes for the investigation of anaemias are often based on the size of the red cells,
which is most accurately indicated by the MCV in the FBC. Commonly, in the presence
of anaemia:
A normal MCV (normocytic anaemia) suggest either acute blood loss or the anaemia
of chronic disease (ACD).
A low MCV (microcytic anaemia) suggests iron deficiency or thalassaemia .
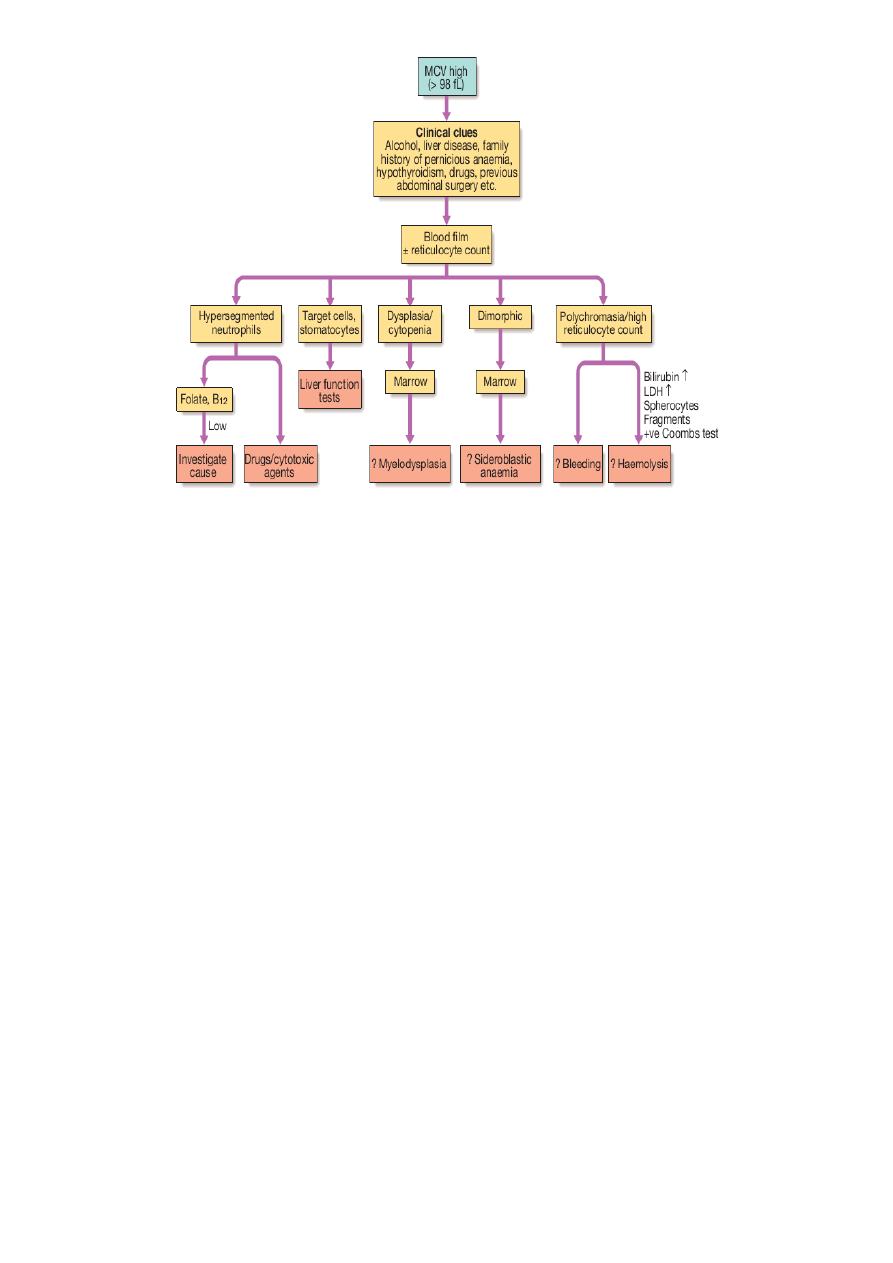
A high MCV (macrocytic anaemia) suggests
vitamin B12or folate deficiency or myelodysplasia
.
5
Bleeding
Normal bleeding is seen following surgery and trauma.
Pathological bleeding occurs when structurally abnormal vessels rupture or when a
vessel is breached in the presence of a defect in haemostasis. This may be due to a
deficiency or dysfunction of platelets, to the coagulation factors, or occasionally to
excessive fibrinolysis, which is most commonly observed following therapeutic
thrombolysis .
Clinical assessment
Site of bleeding. Bleeding into muscle and joints, along with retroperitoneal and
intracranial haemorrhage, indicates a likely defect in coagulation factors. Purpura,
prolonged bleeding from superficial cuts, epistaxis, gastrointestinal haemorrhage or
menorrhagia is more likely to be due to thrombocytopenia, a platelet function disorder
or von Willebrand disease. Recurrent bleeds at a single site suggest a local structural
abnormality.
Duration of history. It may be possible to assess whether the disorder is congenital or
acquired.
Precipitating causes. Bleeding arising spontaneously indicates a more severe defect
than bleeding that occurs only after trauma.
Surgery. Ask about operations. Dental extractions, tonsillectomy and circumcision are
stressful tests of the haemostatic system. Immediate postsurgical bleeding suggests
defective platelet plug formation and primary haemostasis; delayed haemorrhage is
more suggestive of a coagulation defect. In postsurgical patients, persistent bleeding
from a single site is more likely to indicate surgical bleeding than a bleeding disorder.
Family history. While a positive family history may be present in patients with
inherited disorders, the absence of affected relatives does not exclude a hereditary
6
bleeding diathesis; about onethird of cases of haemophilia arise in individuals without
a family history, and deficiencies of factor VII, X and XIII are recessively inherited.
Recessive disorders are more common in cultures where there is consanguineous
marriage.
Drugs. Use of antithrombotic, anticoagulant and fibrinolytic drugs must be elicited.
Drug interactions with warfarin and druginduced thrombocytopenia should be
considered. Some ‘herbal’ remedies may result in a bleeding diathesis.
Clinical examination may reveal different patterns of skin bleeding.
Petechial purpura is minor bleeding into the dermis that is flat and nonblanching
Petechiae are typically found in patients with thrombocytopenia or platelet
dysfunction.
Palpable purpura occurs in vasculitis. Ecchymosis, or bruising, is more extensive
bleeding into deeper layers of the skin.
The lesions are initially dark red or purple but become yellow as haemoglobin is
degraded.
Retroperitoneal bleeding presents with a flank haematoma.
Telangiectasia of lips and tongue points to hereditary haemorrhagic telangiectasia .
Joints should be examined for evidence of haemarthroses.
A full examination is important, as it may give clues to an underlying associated
systemic illness such as a haematological or other malignancy, liver disease, renal
failure, connective tissue disease and possible causes of splenomegaly.
7
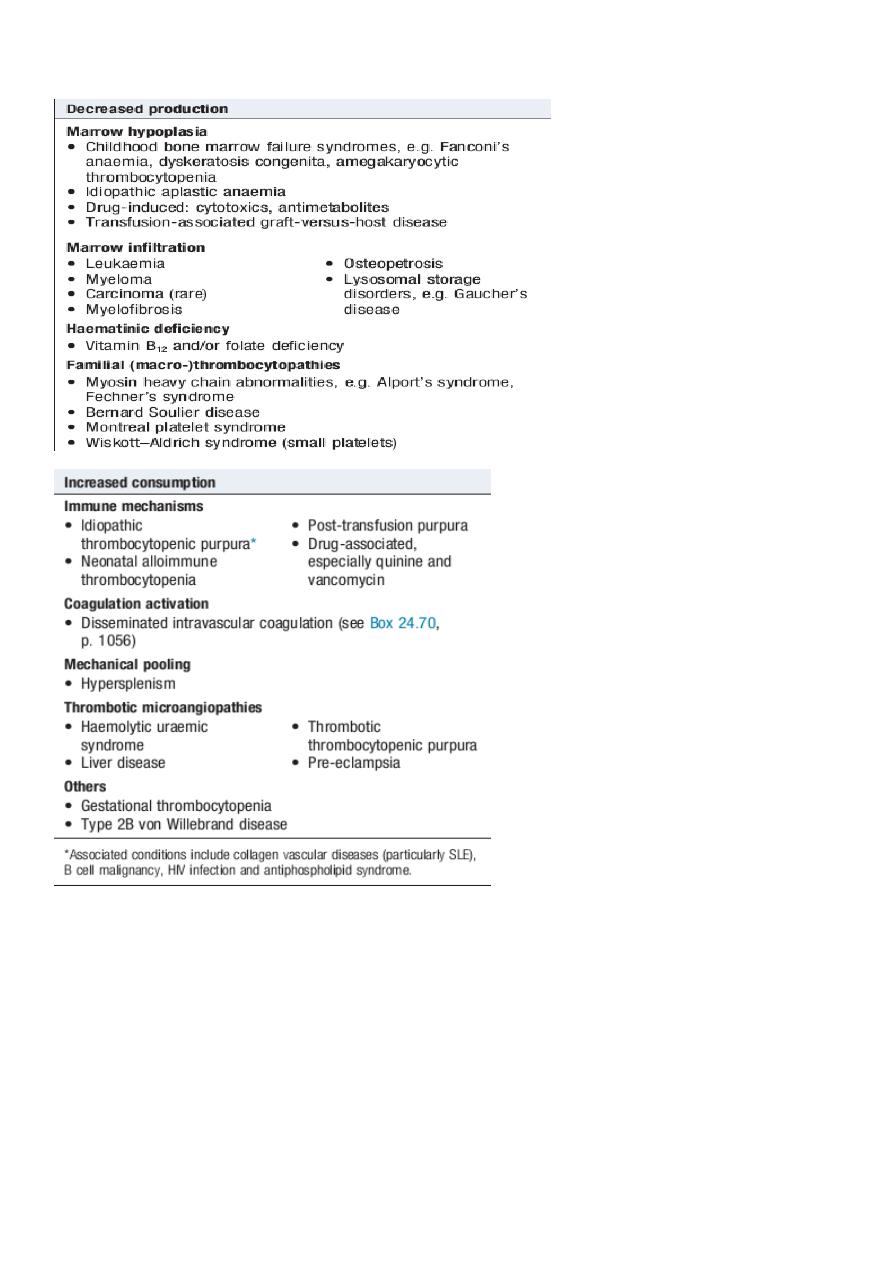
Thrombocytopenia (low platelet count)
Spontaneous bleeding does not usually occur until the platelet count falls below 20
×109/L, unless their function is also compromised.
Purpura and spontaneous bruising are characteristic but there may also be oral, nasal,
gastrointestinal or genitourinary bleeding.
Severe thrombocytopenia (<10 ×109/L) may result in retinal haemorrhage and
potentially fatal intracranial bleeding, but this is rare.
Investigations are directed at the possible causes.
A blood film is the single most useful initial investigation.
Examination of the bone marrow may reveal increased megakaryocytes in
consumptive causes of thrombocytopenia, or the underlying cause of bone marrow
failure in leukaemia, hypoplastic anaemia or myelodysplasia.