1
Endometriosis
Learning Objectives:
By the end of this lecture, you need to:
1- Define endometriosis.
2- Demonstrate the most common site of its occurrence.
3- Enumerate the various presenting features of this gyn. problem.
4- Related this disease with female infertility.
5- Know how to investigate women who suspect to have this disease.
6- Discuss the method of treatment of each type of this health problem.
Introduction:
A- Definitions.
■
Endometriosis is the presence of endometrial glands and stroma (glandular and stromal elements of the
endometrium, both must be present for the dx) outside the lining of the uterine cavity.
■ Endometriosis is primarily a pelvic disease with implants in the ovaries, the fallopian tubes,
uterosacral ligaments, recto-sigmoid, bladder, and appendix. Less commonly, endometriosis can be
found outside the pelvis, suggesting a metastatic spread.
■ It is one of the comments benign gynecological conditions. Generally benign disease usually affects
women in their reproductive years. However, there have been several case reports of adenocarcinoma
developing within foci of endometriosis.
B- EPIDMIOLOGY:
1- Incidence:
●
10-15% of women presented with gynecological symptoms have the condition.
This estimate of prevalence is usually made on identifying the lesions at Laparoscopy undertaken
for pain or subfertility investigations.
●
Sometime seen in asymptomatic women at the time of laparoscopic sterilization.
● Can be seen in 30-40% of patients with infertility.
● Usually regresses following menopause and not usually found prior to menarche.
● No differences among ethnic groups.
● Genetic predisposition 6-7% increased risk with history of first degree relative.
● lesion can be very small 2-3 mm, or can be extensive, in some cases completely obliterating the
normal anatomy of the pelvis.
2- Risk Factors for Endometriosis:
●
Increasing age (up to menopause), but mostly seen between 20-40.
● Shorter menstrual cycle length (less than 27 days).
● Longer duration of menstrual flow (greater than 7 days).
● Heavy menstrual flow.
● Delayed childbirth.
● Low or no parity, the relation with fertility??? Pregnancy is protective.
● First-degree relative (mother, sister, daughter) with endometriosis, 7×Higher
● Social and economic factors
C- Pathogenesis:
●
Cells exhibit a pattern of hormone responsiveness, has cyclical changes.
2
●
Unlike the normal endometrium, they don’t have an order blood supply, but there is an in-grwoth
of new capillaries. Cyclical bleeding can occur within, and from, the endometriotic deposits and
this contribute to a local inflammatory reaction. With healing and subsequent fibrosis overlying
peritoneal damage will lead to adhesions between associated organs.
● Ovarian implant lead to formation of chocolate cyst or endometrioma, where Localized bleeding
cannot be discharged from the body, continuous absorption of some of fluid content lead to tarry
chocolate material.
● Rupture of the cyst lead to scattering of their contents and dissemination of endometrial cells. This
lead to peritoneal reaction to the material with adhesion and fixation.
● Various forms include: Lesions, nodules, polyps and cysts ranging in size from microscopic to
>10cm.
● Common sites: ovaries, fallopian tubes, ligaments supporting the uterus and other surfaces of the
uterus, anterior and posterior cul-de-sac, uterosacral ligaments, posterior uterus and posterior
broad ligaments.
● Less common sites: GI tract, urinary tract, external genitals and rarely disseminates to distant
organs as CNS, extremities, skin, eye, nasal mucosa, episiotomy scars. Can occur in almost every
organ.
Etiology:
The precise etiology remains unknown, several theories explain the process but no single one can
explain the location of endometriotic deposits in all the sites reported.
Theories of pathogenesis:
● Transplant of endometrial tissue via retrograde menstruation: (Sampsons theory)
Retrograde flow of menstrual debris which contains viable endometrial glands and tissue through the
fallopian tubes causes the endometrial cells to spread into the pelvis, form implants there.
■Clinical evidence: Endometriosis is commonly found in dependent portions of the pelvis, most
frequently on the ovaries, cul-de-sac, and uterosacral ligaments. In addition, patients with outflow
obstruction (e.g., mullerian anomalies) have a significantly increased risk of endometriosis.
● Coelemic metaplasia : transformation of embryonic tissue ( Ivanoff &meyer theory ). There is a
common origin of the cells lining the Mullerian duct, the peritoneal cells and the cells of the ovaries.
These cells may undergo de-differentiation back to their primitive origin and then transformed into
endometrial cell.
The transformation of coelomic epithelium into endometrial cells results from some yet-unspecified
stimuli may be hormonal stimuli of ovarian origin by as yet unidentified chemical substances liberated
from uterine endometrium, or those produce from inflammatory irritation. This theory explains
endometriosis reported in: Prepubertal girls, women who have never menstruated and men.
● Lymphatic or vascular transport:
Endometriosis at sites distant from the pelvis may be caused by vascular or lymphatic transport of
endometrial fragments. This could explain the presence of endometriosis at distant sites such as the
brain, joints, skin and lungs.
● Genetic and immunological factors:
The relative risk of endometriosis is 70% in siblings, compared with 1% in control groups. An altered
immunologic response may be involved in the pathogenesis of endometriosis with racial difference as
the incidence is more in oriental than Afro- Caribbean origin. Immune mechanisms supported by that
not all women with seeding of menstrual debris into the pelvis develop endometriosis.
Environmental factors:
■
It has been suggested that the prevalence of the disease has been increased in the recent year which
may be link to environmental pollution.
A possible link between endometriosis and exposure to dioxin,
3
an environmental toxin, found in humans through pesticides in diet, or airborne dioxin released by
certain types of waste incineration. It has been found that endometriosis increased in rhesus monkeys,
the higher the dose of dioxin, the more severe the monkey’s endometriosis.
However apparent increase of the disease may be reflect the greater use of diagnostic laparoscopy to
investigate pain symptoms. There appear to be no relation between the extent of the disease process
seen at laparoscopy and the patient’s age or symptoms.
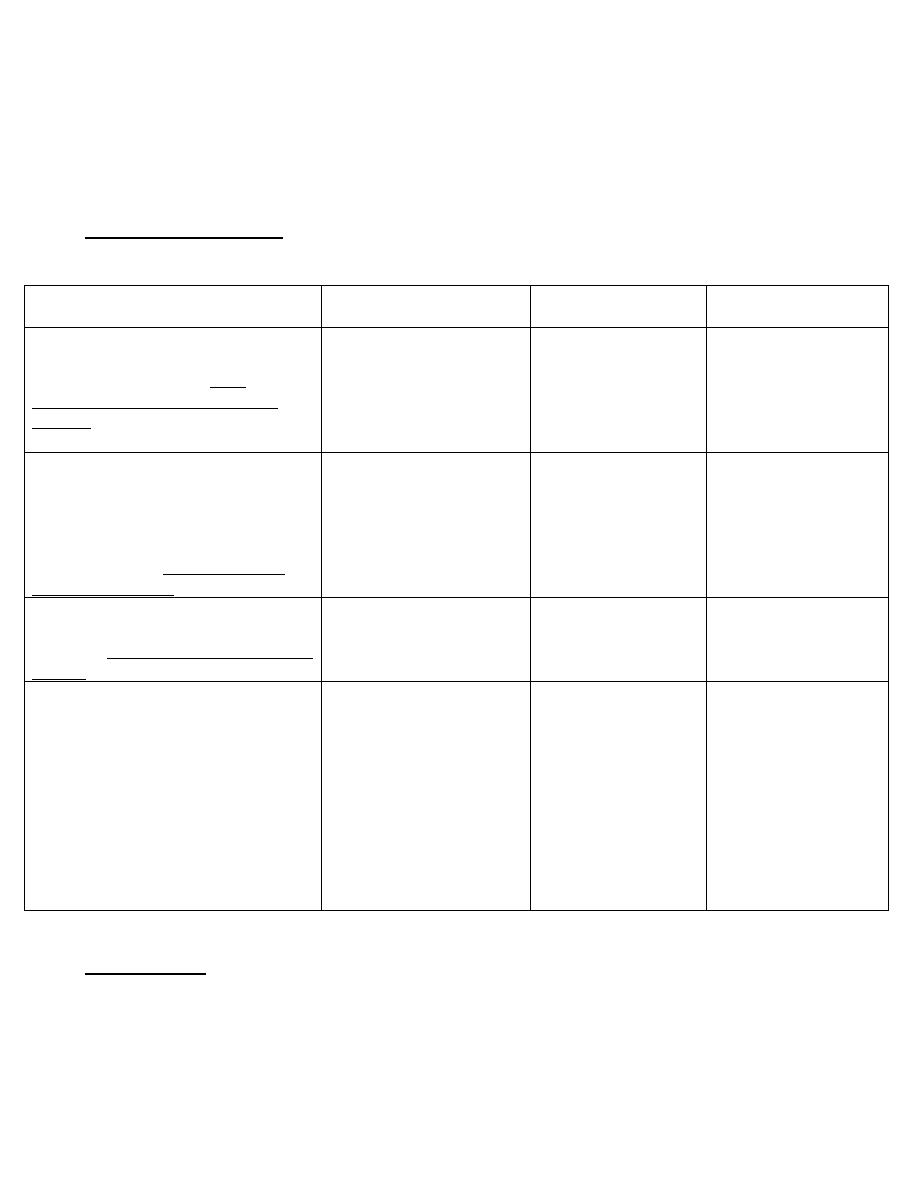
Histological subtypes:
Endometrial deposits-correlation between histological, morphological and functional activity:
Histological subtype
Components
Hormonal response
Laparoscopic
appearance
Free
(polypoidal cauliflower-like structure).
Grow along the surface .Very
sensitive to hormones suppressive
therapy.
Surface epithelium glands
and stroma
Proliferative,
secretory& menstrual
changes. Highly
responsive to
alteration in
Oestrogen secretion.
Haemorrhagic vesicle/
bleb
Enclosed
At this stage, the implant has been
covered with a surface layer of
peritoneum so located within the
tissue. React in a similar way as basal
endometrium and partly respond to
hormonal treatment
glands and stroma
Proliferative,variable
secretory changes ,
no menstruation
Papule & later nodule
Healed
Have features of cystically dilated
glands.
Insensitive
to
hormonal
therapy
Glands only
No response
White
nodule
or
flattened fibrotic scar
Ovarian endometriosis
Presented as superficial form with
haemorrhagic leasion or as enclosed
haemorrhagic cyst
Endometrioma: means endometriotic
or (Chocolate cyst) of the ovary.
Formed by lesion from outer surface
of the ovary and with growth, there is
inversion of ovarian cortex and with
increase inflammatory reaction it
become occluded
Wide variation in the
presence of endometriotic
tissue, the cyst wall can be
lined by free endometrial
tissue. In long standing
endometrioma, the cyst
wall
becomes
covered
only by thickened fibrotic
reactive tissue, no specific
features of glandular or
stromal tissue.
Superficial
haemorrhagic lesion,
red
vesicles,
blue
black
(powder-burn)
lesion with adhesion
formation
or
endometrioma
الجدول اعاله لالطالع: ةظحلام
Presentation:
A. Symptoms: they are variable, depending on the site. But sometime there is a lack of correlation
between apparent extent of the disease and the intensity of the symptoms.
1- Pain: three common types of pain in endometriosis:

4
a. Dysmenorrhea. Spasmodic dysmenorrhea (menstrual pain secondary to an anatomic
pelvic abnormality) is the most common symptom of endometriosis. The painful menses
usually develop after years of relatively pain-free menses.
b. Chronic pelvic pain. Pelvic pain for more than 6 months (diffuse or localized in the
pelvis) is considered chronic. However, many women with endometriosis are asymptomatic,
and the degree of endometriosis often does not correlate with the existing amount of pain, it
also may associate with low backache &lower abdominal pain.
c. Dyspareunia. (Deep dyapareunia) Painful intercourse may be caused by:
i- Endometrial implants of the uterosacral ligaments.
ii- Endometriomas of the ovaries.
iii- Fixed retroversion of the uterus secondary to endometriosis and adhesions.
● Pathogenesis of pain in endometriosis.
a. Lesions of the peritoneum can cause scarring and retraction of the peritoneum. They may
also transmit pain through somatic afferent pain fibers.
b. Pain may result from elevated prostaglandins and histamines in endometriotic tissues and
peritoneal fluids. Use of prostaglandin synthetase inhibitors may help many women with
endometriosis.
2- Infertility and endometriosis:
● Endometriosis has been demonstrated by laparoscopy in as many as 30 to 40% of women who are
infertility. No sufficient evidence supports the fact that minimal endometriosis is associated with
infertility and that treating minimal endometriosis laparoscopically enhances fertility. Exactly how
minimal endometriosis causes infertility is still under investigations. How endomtetriosis could
impaired fertility due to:
i. Ovarian function: Oocyte maturation defect, endocrinopathies, luteinized unruptured follicle
syndrome (which the ovum is trapped in the follicle and not released with the luteinizing hormone
(LH) surge), altered prolactin released & anovulation.
ii. Fallopian tubes: Impaired fimbrial oocyte pick-up, altered tubal motility & tubal blockage.
iii. Coital function: Deep dyspareunia – reduce coital frequency.
I iv. Sperm function: Antibodies causing inactivation & Macrophage phagocytosis.
v. Early pregnancy failure: Prostaglandin induced, Immune reaction & luteal phase deficiency.
3- Associated Symptoms.
a. Urinary. Urinary symptoms are common in patients with endometriosis; as many as one third of
patients with endometriosis have urinary tract involvement including, bladder, lower ureter,
upper ureter, and kidney. Symptoms range from intermittent dysuria, frequency, and urgency
to complete ureteral obstruction. Gross or microscope hematuria is present in many patients
and frequently follows the menstrual cycle.
b. Gastrointestinal. 7-35% of all women with endometriosis have bowel involvement. Symptoms
may vary from dyschezia (pain on defecation) and hematochezia (bloody bowel movements)
to other symptoms of partial or complete bowel obstruction, may need radiographic
evaluation of the bowel with barium contrast to exclude other causes.
B- Signs: Perform good bimanual exam:
Uterosacral ligament tenderness and nodularity is very specific to endometriosis
Pain/nodularity in cul-de-sac
Obliteration of the cul-de-sac occurs with fixed uterine retroversion implying severe
disease.
Adnexal tenderness and palpable enlargement of endometriomas (chocolate cysts).

5
Diagnosis:
History and physical examination may be suggestive of endometriosis, but the only way to diagnose the
condition is by visualization at surgery (usually laparoscopy) and by biopsy of implants. Clinical
diagnosis is usually made following the laparoscopic observation of haemorrhagic or fibrotic lesions in
the peritoneal or the serosal surface of various pelvic organs.
A- History. The patient might have one or more of the characteristic symptoms. A history of
endometriosis in the patient's mother or sister is also important.
B- Pelvic examination. The pelvic examination in minimal endometriosis is usually normal.
i- Nodularity and tenderness of the uterosacral ligaments are characteristic findings
on rectovaginal examination.
ii- Endometriomas (ovarian cysts filled with old blood from endometriosis, forming "chocolate
cysts") are palpated as adnexal masses often fixed to the lateral pelvic walls or to the posterior
cul-de-sac.
iii- The uterus is often in a fixed retroverted position.
C- Laparoscopy and the classification of endometriosis:
Laparoscopy : is the golden standard mean of diagnosis and could be of help as therapeutic tool also.
1. Appearance:
- The classic endometriotic implant: is characterized as brown or black pigmentation (powder-burn
lesion) and fibrosis.
- "Atypical" or "subtle" lesions: Lesions ranging from clear vesicular, white opacified, glandular,
polypoid, or red hemorrhagic vesicles have been increasingly apparent on laparoscopy and confirmed by
biopsy to be endometriosis. Recent studies also suggest that these early implants may be the most
metabolically active.
- Tissue damage: Endometriosis may cause deep tissue damage, resulting in local scarring and
reduplication of peritoneum and leading to surface peritoneal defects.
2- Staging of endometriosis:
The extent of formation of classic lesions, ovarian involvement, and adhesive disease is classified
First stage:
Minimal disease --small amount of brownish, reddish, blue-black, white, or clear implants.
Second stage:
Mild disease -- deeper and more numerous than stage one.
·
Third stage:
·
Moderate disease -- many deep implants, small endometriomas on ovaries and some filmy adhesions.
·
Fourth stage:
Severe disease -- many deep implants and dense adhesions, large endometriomas on ovaries, rectum
may adhere to the back of the uterus.
of
D- Pelvic ultrasound: to detect endometrioma of the ovary.
E- CA 125: is a glycoprotein expressed on the cell surface of some coelomic epithelium (including
endometrial tissue), elevated levels found in women with endometriosis, shouldn’t be used for
screening but may correlate with patient’s response to treatment and its elevated in other benign
conditions - early pregnancy, acute pelvic inflammatory disease, uterine fibroids, and menstruation.
This test is useful as marker for response to treatment or recurrence but not as a diagnostic test because
it lacks specificity
f- Other Imaging technique: include CT scan and MR
Differential diagnosis:
6
Chronic salpingo-oophoritis
Corpus luteum cyst or neoplastic cyst
Ut. Leiomomas
Malig dis. of the ovary, or metastases on pelvic peritoneum
Ca of the cervix or vagina
Bowel malig
Any case of acute abdomen
All cases of intestinal obstruction
All tumour of umbilicus
Hernia and any swelling in the inguinal canal
All causes of haematuria.
Treatment:
a. General considerations. Age of the patient, extent of disease, duration of the infertility, and
severity of symptoms are important considerations. The patient's reproductive plans should also be
taken into account. Pregnancy tends to alleviate the symptoms of endometriosis.
b. Expectant treatment.
1- Expectant therapy may be appropriate in young women who have pelvic pain with apparent
endometriosis on laparoscopy and no immediate interest in pregnancy. Goals are relief of the
dysmenorrhea and prevention of further growth of endometriosis. So it's of help in cases of:
- Small multiple lesions with few symptom
- Newly married women
- Endometriosis with pregnancy
c. Medical therapy: Ectopic endometrium responds to cyclic hormone secretion in a fashion similar
to normal endometrium. Hormonal suppression of menses constitutes the basis of medical therapy.
1- Nonsteroidal anti-inflammatory drugs (NSAIDs). The prostaglandin synthetase inhibitors are
effective in controlling endometriosis-related dysmenorrhea. Women with endometriosis show
increased concentrations of prostaglandins in the peritoneal fluid. When (oral contraceptive pills)
OCPs and NSAIDs are administered simultaneously, they have a synergistic effect.
NSAIDs,
Inhibit prostaglandins produced by endometrial implants, Begin 1 to 2 days before the onset of
menses and continue for the duration of menstrual cycle.
2- Oral contraceptive pills (OCPs). Continuously administered OCPs for up to 6 months are
appropriate for mild disease because they reduce the amount of endometrial buildup and shedding,
thereby preventing further growth of endometriosis, it produces a pseudopregnancy state with
amenorrhea and causing decidualization and resorption of the ectopic endometrium. This treatment
is appropriate only in mild endometriosis that does not produce much distortion of the pelvic
anatomy by adhesions or endometriomas.
3- Progestins. Suppress ovarian function and cause atrophy of endometrial implants,
Depo-Provera –IM every 3 months, and dydrogesterone given on continues base to produce pseudo-
decidualization of the endometrium and comparable changes in endometriotic lesion.
Visanne: it is a 2 mg dienogest, is a new drug for treatment of endometriosis for a period of around
15 months.
Side effects of progestins– Breakthrough bleeding, depression, nausea, bloating & breast tenderness.
.
4- Danazol. synthetic isoxazol derivative of 17 alpha-ethinyl testosterone consistently improved
symptoms of endometriosis. It has been now replaced by the GnRH agonists because of its side
effects, it eliminates midcycle surge of LH and FSH, decreasing estrogen and progesterone; creates
high androgen – low estrogen state Side effects –are androgenic type; weight gain, greasy skin and
7
acne. Prolong use will affect lipid profile or liver function. Its use now had been restricted because
of possible association with ovarian cancer.
5- Gestrinone: Synthetic trienic, 19 norsteroid with androgenic and antigonadotrophic effect,
causing progressive endomometrial atrophy.
6- Gonadotropin-releasing hormone (GnRH) agonists. These agents are the most
commonly used method for medical treatment of endometriosis:
a- Mode of action. GnRH is a decapeptide that controls the release of the anterior pituitary
hormones (FSH & LH). Normally, the release of GnRH is pulsatile. Chemical alterations of the
amino acids at positions 6 and 10 produce synthetic derivatives of GnRH (GnRH agonists) that
resist cleavage by endopeptidases but retain a high affinity for the pituitary GnRH receptor. If the
gonadotrope is exposed to GnRH for a prolonged time, downregulation and desensitization occur,
and gonadotropin secretion is suppressed.
b- Administration. GnRH agonists may be administered intranasally, subcutaneously, or
intramuscularly daily or as a depot injunction every month or every 3 months.
c- Adverse effects. Menopausal-type symptoms (e.g., hot flashes, decreased libido, vaginal dryness,
and headaches) occur because of the hypoestrogenic state. Prolonged use (more than 6 months) may
result in significant bone loss, leading to osteoporosis. Using "add-back therapy" (estrogen and
progestin) may minimize bone loss.
d- Prognosis. Amenorrhea and atrophic endometrial changes occur in most patients. Regression of
endometriotic lesions occurs in 80% of cases, and symptomatic relief results in more than 50% of
cases after 6 months of therapy. However, recurrence rates are 25 to 30% per year after therapy is
discontinued.
d- Surgical therapy. Use when medical therapy does not dissolve adhesions or eliminate
endometriomas. The success of surgery in relieving infertility is directly related to the severity of the
endometriosis.
● Conservative surgery involves the excision, fulguration, or laser vaporization of endometriotic
tissue. The excision of ovarian endometriomas; and the resection of severely involved viscera.
● Radical surgery involves a total hysterectomy and bilateral salpingo-oophorectomy.
This approach is used in patients who do not desire future fertility or those whose endometriosis is
so severe.
● Estrogen replacement therapy is important in patients who undergo radical surgery to prevent
osteoporosis and premature aging of the cardiovascular system.
●Pre-sacral neurectomy has been used to treat severe dysmenorrhea.
V- Recurrences
- May recur with medical therapy or surgical therapy
- GnRH agonists or Danazol-Minimal disease – 37%, severe disease – 74%
- Surgery – 40% after 5 years
- 56% of all patients after 7 years
- Possibility of adenocarcinoma in endometriosis??
Adenomyosis
:
When the endometrial tissue present in the myometrium, response to
ovarian hormones is limited, because the adenomyoma is composed of basal type of endometrium
which is normally insensitive to an endocrine stimulus.
To differentiated from fibromyoma, adenomyoma has no capsule and cause diffuse enlargement of the
uterus; while the myoma is localized nodule.

8
■ Mechanism of origin:
- down growth from the basal layer of the endometrium
- venous and lymphatic spread can also explain
■Presentation:
- usually multiparous and diagnose in their late thirties or early forties
- menorrhagia 75%
- progressive enlargement of the uterus, diurnal frequency, heaviness in the pelvis
- dysmenorrhea 30%. Increasingly sever spasmodic dysmenorroea
■ O/ E:
- enlarge tender uterus, mobile, rarely the uterus more than 12-14 wks.
■ Investigations:
- US: may be helpful which show alteration in the echogenicity within the myometrium from the
localized haemorrhage filled the distended endometrial glands.
- Hysteroscopy: may help in the diagnosis
- MRI: now have a role and regarded as the investigation of choice.
■Treatment:
- Occasionally hormonal treatment as Gestrinone, Danazol and GnRHa could be of help as any
treatment which could induce amenorrhoea would be of help, but symptoms are returned rapidly once
treatment stop.
- If symptomatic, surgery which is the only method making the diagnosis certain, hysterectomy is the
method of choice (because we can’t remove the mass alone).
……………………………………………………………………………………….