SCOLIOSIS
Lec-4Sadeq Al-Mukhtar - Consultant orthopaedic surgeon
Definition:
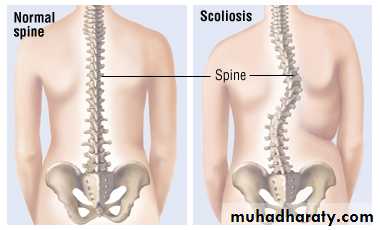
It is lateral curvature of the spine to one side but actually a tri-planer deformity:-Lateral.
Antero-posterior.
Rotational.
In the thoracic region, the rotation throws the ribs into prominence producing Rib hump deformity whereas in the lumbar region the same degree of curvature may not be noticeable.
Scoliosis-TYPES:
Mobile Scoliosis:The vertebrae are not rotated.
The curve is transient.
Never develops into fixed scoliosis.
Secondary and compensatory to problems outside the spine and once the problem is corrected the deformity will improve.
Fixed scoliosis
Features:-
It is always accompanied by rotation of the vertebrae; the bodies rotate towards the convexity of the curve, the neural arches and spinous processes toward the concavity.
Non-correctable deformity.
Secondary compansatory curve develo to keep the alignment of the spine straight.
Worsening decreases after skeletal maturity (17-18 years in males and (16-17 years in girls).
It is the commonest type.
There are usually three curves; the middle one is primary and fixed from the start, while the other two may later become fixed.
Fixed “Structural” Scoliosis Types
Idiopathic Scoliosis:Infantile.
Juvenile.
Adolescent.
Congenital Scoliosis:
Paralytic-Neuromuscular Scoliosis.
Others-5% Like-Syringomyelia (High thoracic scoliosis: There is loss of pain and temperature sense. Spastic weakness, trophic changes and often claw hands).
Friedreichs ataxia:
Familial scoliosis. Age is between 5-15 years, ataxia ,tremor, and slurred speech.Dystrophies: e.g; Osteogenesis imperfecta and Marfans syndrome.
Adolescent Idiopathic scoliosis:
It is the commonest form.Occurs at puberty 10-25 years.
Slightly more common in girls.
Usually convex to the right.
Deformity increases on flexion of the spine.
Shoulder is elevated on the convex side.
Factors in assessing progression
Sex: Progression is more common in girls.Age: Progression is more when there is potential for skeletal growth i.e presence of apophysis of iliac crest indicates more likelihood of worsening of scoliosis “Rissers sign” .The curve stops increasing when the spine stop growing-a reliable guide to spinal maturity is the complete appearance of iliac apophysis on x- ray
Site: Thoracic curves are progress more than lumbar.
Double curves are more likely to progress than single curve.
Progression is more likely with curves more than 30 degrees.
Slender spines are more likely to progress.
Knowledge of these risk rates can lead to more rational patient management.
Low risk patients need to be seen less frequently and far fewer radiographs need to be taken.Increased awareness of the problem of spine deformity has resulted in an increased concern for the potential risk of repeated radiograph exposure (Breast, thyroid, and bone marrow are the most radiosensitive tissues).
Clinical Features
Notice the above features.
On examination the site, flexibility and cosmetic effect of the curve are noted.
Neurological examination.
Presence of café au lait patches.
Diagnosis
Assessment of Scoliosis accurately by X-ray, full length film of the spine and measurement of Cobbs angle (It is the angle formed by crossing of upper and lower lines of the curve “convexity” out of which the spines start to regain the normal alignment).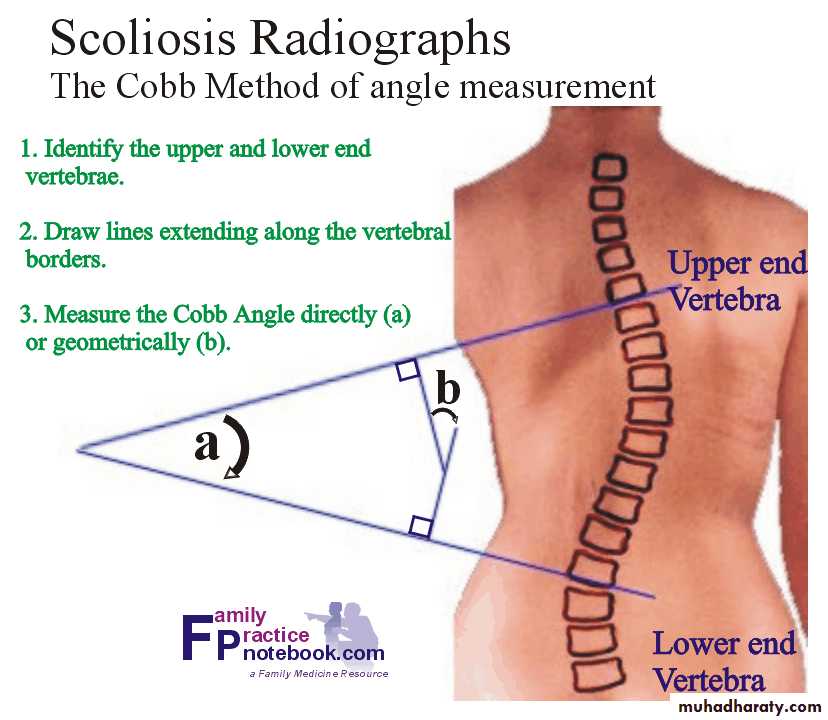
Treatment
Conservative:Milwaukee brace: Anterior and posterior struts that support a neck ring and sub-occipital pads.
Boston brace: It is an under arm device constructed from a pelvic module fitted with pads to correct lumbar and thoraco-lumbar curves. It is worn under the clothes so it is more acceptable but not suitable for high curves.
Conservative-Indications:
Curves less than 25 degrees .upper limit of bracing is 40-45 degrees.To keep those more than 25 degrees until the age of 10 years when fusion is more likely successful.
Balanced curves: Pendol test (one line of pendol is hanging from the occipit to the anal cleft).
To prevent recurrence.
Notes:
Bracing does not correct scoliosis, but used to prevent progression until skeletal maturity.
Part-time bracing (16 hours per day) had results almost equal to those in similar group of patients who used their brace full-time.
Boston brace is effective more than Milwaukee in patients with curves with apices at Th.8 level or lower.
Electrical stimulation : Effect similar to brace.
Surgery
Indications:If the curve more than 45 degrees.
Sites which are difficult to brace e.g: High thoracic, double thoracic curves.
Fixed curve.
Loss of spinal balance: By pendol test.
Rapid deterioration.
Cosmetic appearance.
Surgery is to correct, stabilized, and fuse. There are many types of techniques; the most common type is Harrington rods for stabilization.
Congenital Scoliosis:
Causes:Failure of formation e.g: Hemi-vertebrae.
Failure of segmentation e.g:Bar.
Mixed type: Single or multiple.
Neuromuscular Scoliosis:
Occur in :
Cerebral palsy.
Poliomyelitis.
Spina bifida.
Muscular dystrophy.
Treatment: Early bracing is necessary and surgery is important to prevent severe deformity with reduction of respiratory function.
KYPHOSIS
Definition:Excessive dorsal curvature more than 45 degrees.
Types:
Mobile Kyphosis.Fixed Kyphosis.
Mobile Kyphosis
Postural: Common in adolescents ,women after child birth, and obese.Treatment: Postural training, exercise, and weight-lowering programs.
Muscle weakness: e.g: Polio,muscle dystrophy.
Compensatory: As in hip deformities e,g:DDH,Fixed flexion deformities which causes excessive lumbar lordosis and thoracic kyphosis.
Fixed kyphosis
Congenital Kyphosis (children).
Scheuermanns disease (adolescents).
Ankylosing Spondylitis (adult).
Osteoporosis (senile),Paget’s disease, and pathological fractures of spine (elderly).
T.B (all ages).
Scheuermann’s disease
Osteochondritis of the growth plates, so irregularly ossified. That defect threw undue strain on the anterior portion of the vertebral bodies, which lead to kyphosis, and the disc material penetrate into the vertebral bodies.It is common in females
Uniform kyphosis. Smooth thoracic kyphosis and compensatory lumbar lordosis.
Movement are normal and SLR-test is limited to 60 degrees by tight hamstrings.
X-ray: The bodies of adjacent vertebrae usually D 6-10, are wedged. They may contain Schmorls nodes. The epiphyseal plates appear fragmented especially anteriorly.Treatment:
Severe degrees (rare) are treated by surgery by correction and fusion.Mild and moderate, by conservative methods
Exercise.
Brace; Milwaukee.
Sleep in plaster shell at night.
Analgesia.
Angular Kyphosis-”Kyphos”
Fixed, Forward angulation, that occurs in:
T.B.
Fractured spine.
Calves disease:- A rare condition which is a sequel to eosinophilic granuloma with one vertebral body become flattened but disc space is normal.