
Kyphosis:
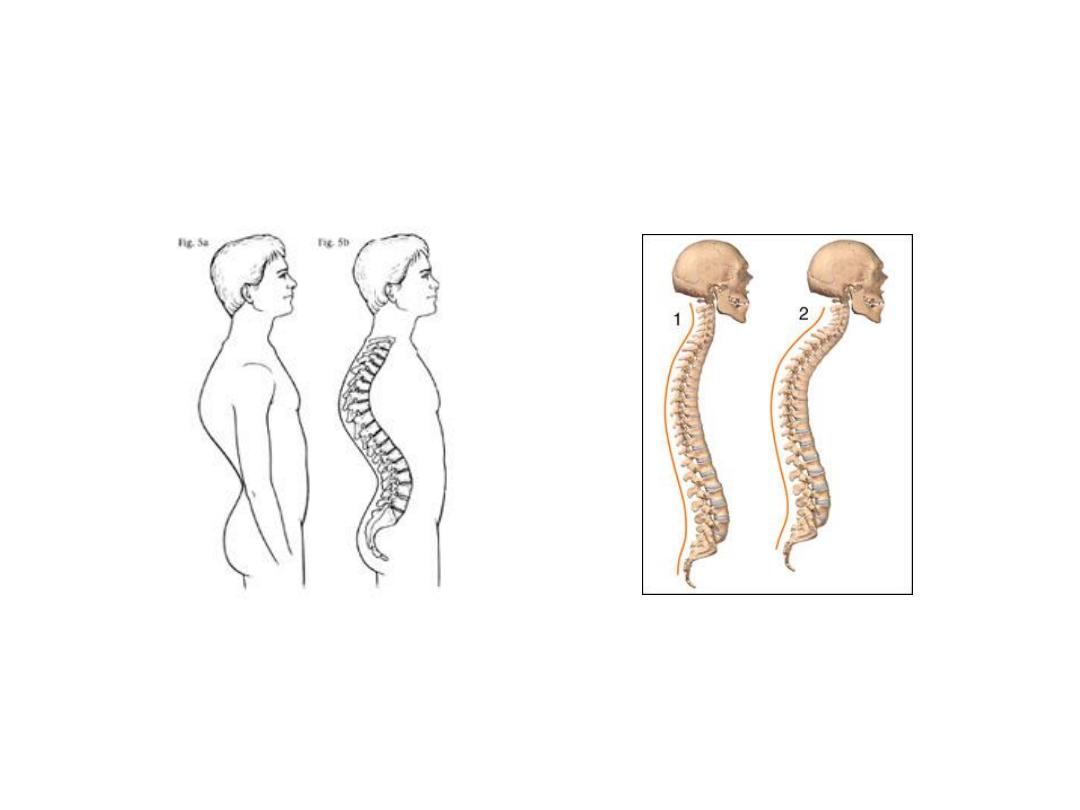
• Pathological kyphosis is the abnormal
(excessive) forward bending and posterior
curvature of the spine that mainly occurs in
the thoracic region.
• It’s the significant well recognized
deformity with rounded back, which may be
progressive.
• It can be postural or structural.

Postural as with other postural
defects as flat feet or others.
Structural as with osteoporosis
of elderly, ankelosing spondilitis
and scheuermann’s disease; or
its a primary idiopathic
kyphosis.
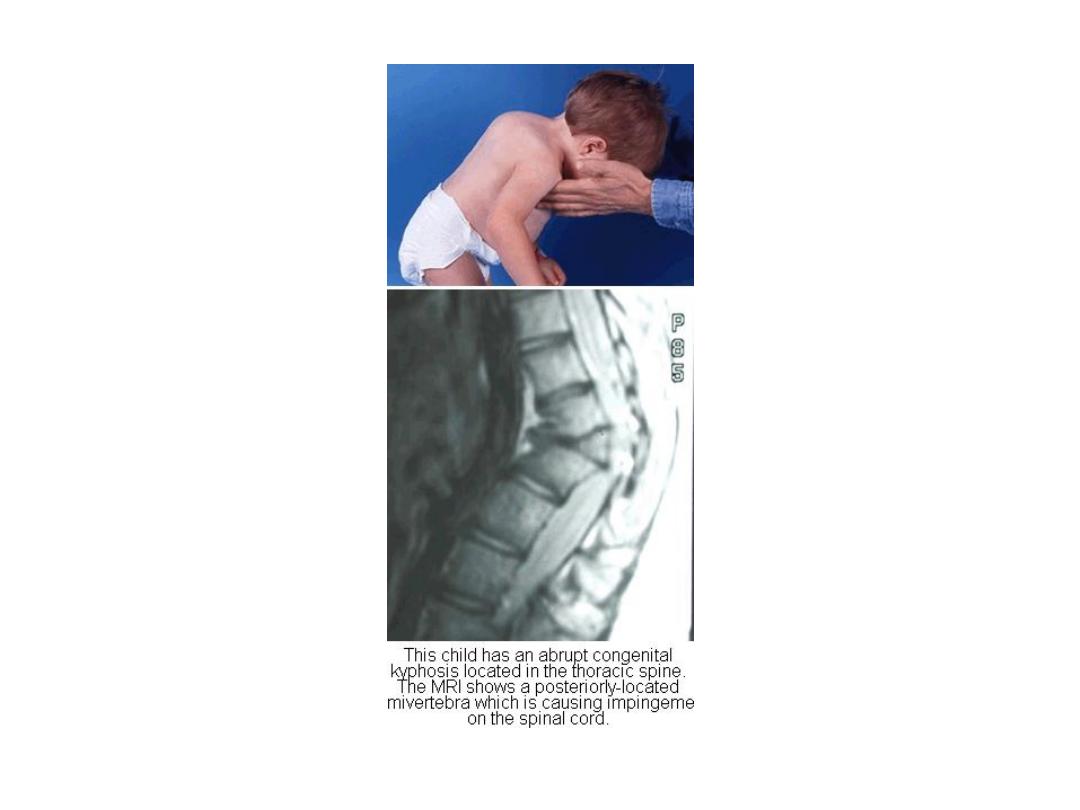
Kyphos (gibbus) is a sharp
posterior angulation due to
localized collapse or wedging of
one or two vertebrae. This may
be the result of a congenital
defect, a fracture (sometimes
pathological) or spinal
tuberculosis.

Tuberculosis of the spine (Pott’s
disease and paraplegia):
• The spine is the most common site of
skeletal tuberculosis, and the most
dangerous.

Pathology:
• Blood borne infection settles in a vertebral
body adjacent to the intervertebral disc.
Bone destruction and caseation follows,
with infection spreading to the disc space
and to the next vertebra.
• As the vertebral bodies collapses into each
other, a sharp angulations (or kyphos)
develops.


Pathology:
• Caseation and cold abscess formation may
extend to nearby vertebrae or escape into
the paravertebral soft tissues.
• There is a major risk of cord damage due to
pressure by the abscess or displaced bone.

Clinical features:
• There is usually a long history of ill-health and
backache. In some cases deformity is the dominant
feature. Occasionally the patient presents with a cold
abscess pointing in the groin, or with paraesthesia and
weakness of the legs.
• On examination the characteristic finding in the
thoracic spine is an angular kyphos (gibbus), there is
local tenderness and muscle spasm, all movements are
restricted.
• The groins and lumbar regions should be examined for
abscess formation, and the lower limbs must be
examined for neurological changes.

X-ray:
• Early on there is no more than disc space
narrowing; with bone destruction there is
collapse of adjacent vertebrae and
obliteration of the disc space.
• A paravertebral abscess may be present.
• In long-standing cases there may be
marked deformity involving a considerable
length of the spine.


Investigations:
• The Mantoux test is positive and the ESR
may be raised. If there is an abscess, pus
should be sent for bacteriological
examination and culture.

Diagnosis:
• It is often difficult to distinguish
tuberculosis from other types of infection or
(in older patients) from metastatic tumor
disease. If there is doubt, a needle biopsy
may provide the answer.

Treatment:
• Except for the more advanced cases with
progressive bone destruction, conservative
treatment is usually enough and curative.
• Antituberculus chemotherapy should be
rigidly supervised and continued for 9-12
months.
If pain and spasm are marked, a period in
hospital is of help; otherwise a well-fitted
brace is all that is needed.
The indications for
operation are:
1. Abscess formation (this must be drained).
2. Marked bone destruction and progressive
deformity (this requires spinal fusion).
3. Threatened paraplegia that does not
respond to conservative treatment.