AFTER MID
SURGERY
DR. Ammar Alyassiri
Orthopaedic
Neuromuscular disorders
Dr. Ammar Alyassiri
LECTURE 10
Neuromuscular disorders
CEREBRAL PALSY
Definition:
a group of disorders that result from non-progressive brain damage during early
development and are characterized by abnormalities of movement and posture
epidemiology
The incidence is about 2 per 1000 live births,
highest rates in premature babies and those of multiple births.
Aetiology
causal factors:
◦ maternal toxaemia
◦ prematurity
◦ perinatal anoxia
◦ kernicterus
◦ postnatal brain infections or injury
◦ birth injury though often blamed, is a distinctly unusual cause.
associated problems: such as
◦ epilepsy,
◦ perceptual problems
◦ behavioral problems
◦ learning difficulties.
Consequence
The main consequence:
Neuromuscular incoordination
Dystonia
weakness
spasticity
Classification
TYPE OF MOTOR DISORDER:
◦ Spasticity:
Commonest 80%.
pyramidal system in the CNS.
hypertonia.
hyper-reflexia.
◦ Hypotonia is usually a phase, lasting several years during early childhood
before the features of spasticity become obvious.
◦ Athetosis:
continuous, involuntary, writhing movements.
extrapyramidal systems of the CNS.
◦ Dystonia may occur with athetosis. There is a more generalized increase in
muscle tone and abnormal positions induced by activity.
◦ Ataxia
appears in the form of muscular incoordination during voluntary
movements.
cerebellar damage.
◦ Mixed palsy appears as a combination of spasticity and athetosis.
TOPOGRAPHIC DISTRIBUTION
◦ Hemiplegia:
commonest.
appears as a spastic palsy on one side of the body with the upper
limb more severely affected than the lower.
can walk
respond well to treatment.
◦ Diplegia:
involves both sides of the body, with the lower limbs always most
severely affected.
◦ Total body involvement
more severe disorder affecting all four limbs, the trunk, neck and
face with varying degrees of severity.
Patients usually have a low IQ, they may have epilepsy.
unable to walk.
the response to treatment is poor.
◦ Monoplegia
occasionally appears in an upper limb
other areas are involved as well
diagnosis
Diagnosis in infancy:
◦ The full-blown clinical picture may take months or even years to develop.
◦ A history of prenatal toxaemia, haemorrhage, premature birth, difficult
labour, foetal distress or kernicterus.
◦ A neonatal ultrasound scan=I.C.H
◦ difficulty in sucking and swallowing, with dribbling at the mouth.
◦ baby feels stiff or wriggles awkwardly
◦ the motor milestones are delayed.
Diagnosis in later childhood:
◦ Most children presenting to the orthopaedic surgeon have already had the
diagnosis made
Bleck has described seven tests for childrenover 1 year
◦ The primitive neck-righting reflex,
◦ asymmetrical and symmetrical tonic neck reflexes,
◦ the Moro reflex and
◦ the extensor thrust response should all have disappeared at 1 year of age.
Children who retain more than two primitive reflexes after that age, cannot sit
unsupported by 4 years and cannot walk unaided by 8 years are unlikely ever to
walk .
child should be reviewed by a multidisplinary team (speech, hearing, visual acuity,
intelligence and motivation)
the child should be carefully observed sitting, standing, walking and lying.
NEUROMUSCULAR EXAMINATION
◦ upper motor neuron or spastic paresis.
◦ Passive movements are resisted,
◦ the reflexes are exaggerated and there is a positive Babinski response.
◦ spasticity may obscure the fact that muscle power is actually weak.
◦ Sensation is often not entirely normal and problems with stereognosis (as
well as with perception)
Management
GOAL SETTING:
For all patients with cerebral palsy the priorities are:
(1) an ability to communicate with others;
(2) an ability to cope with the activities of daily living (including personal hygiene); and
(3) independent mobility — which may mean a motorized wheelchair rather than
walking.
For the child who from an early age is recognized to be 'non-walking' realistic goals
should be:
(1) a straight spine with a level pelvis;
(2) mobile and painless hips that flex to 90 degrees (for comfortable sitting) and extend
sufficiently to allow comfortable sleeping
(3) knees that are mobile enough for sitting, sleeping and transferring; and
(4) plantigrade feet that fit into shoes and rest on the footplates of the wheelchair
comfortably
TONE MANAGEMENT:
◦ Medical treatment:
anticonvulsants for seizures
Baclofen, an agonist of (GABA), acts by inhibiting reflex activity.
Analgesic medication is needed for the reduction of pain associated
with musculoskeletal problems
Botulinum toxin it acts by blocking acetyl choline release at the
neuromuscular junction.
◦ Selective dorsal rhizotomy: Division of selected dorsal nerve roots from LI
to S2

◦ Physical therapy :
Physiotherapy attempts to reduce or prevent the problems arising
from abnormal muscle tone, imbalance between opposing muscle
groups and abnormal body balance mechanisms.
Physiotherapy is considered to be most helpful in early childhood up
to the age of 7 or 8 years
postoperative physiotherapy is essential in order to maximize the
effects of surgery
◦ Splints :
prevent muscle contracture,
maintain joint position and improve movement and hence function.
maintaining position following surgery.
Operative treatment:
◦ indications:
(1) a spastic deformity which cannot be controlled by conservative
measures;
(2)fixed deformity that interferes with function;
(3)secondary complications such as bony deformities, dislocation of
the hip and joint instability.
◦ timing of surgical intervention: delaying surgery until the age of 7 or 8 years
and then doing all the necessary operations at one or two sittings.
Operations may include
◦ release of tight muscles,
◦ lengthening of tendon,
◦ tendon transfer,
◦ osteotomy,
◦ arthrodesis or
◦ Excisional arthroplasty.
Post-operative splintage & physiotherapy is always indicated.
SPINA BIFIDA
a congenital disorder in which the two halves of the posterior vertebral arch fail
to fuse at one or more levels(neural tube detect),
occurs within the first month of foetal life,
usually affects the lumbar or lumbosacral segments of the spine.
In its most severe form, the condition is associated with major neurological
problems in the lower limbs together with incontinence.
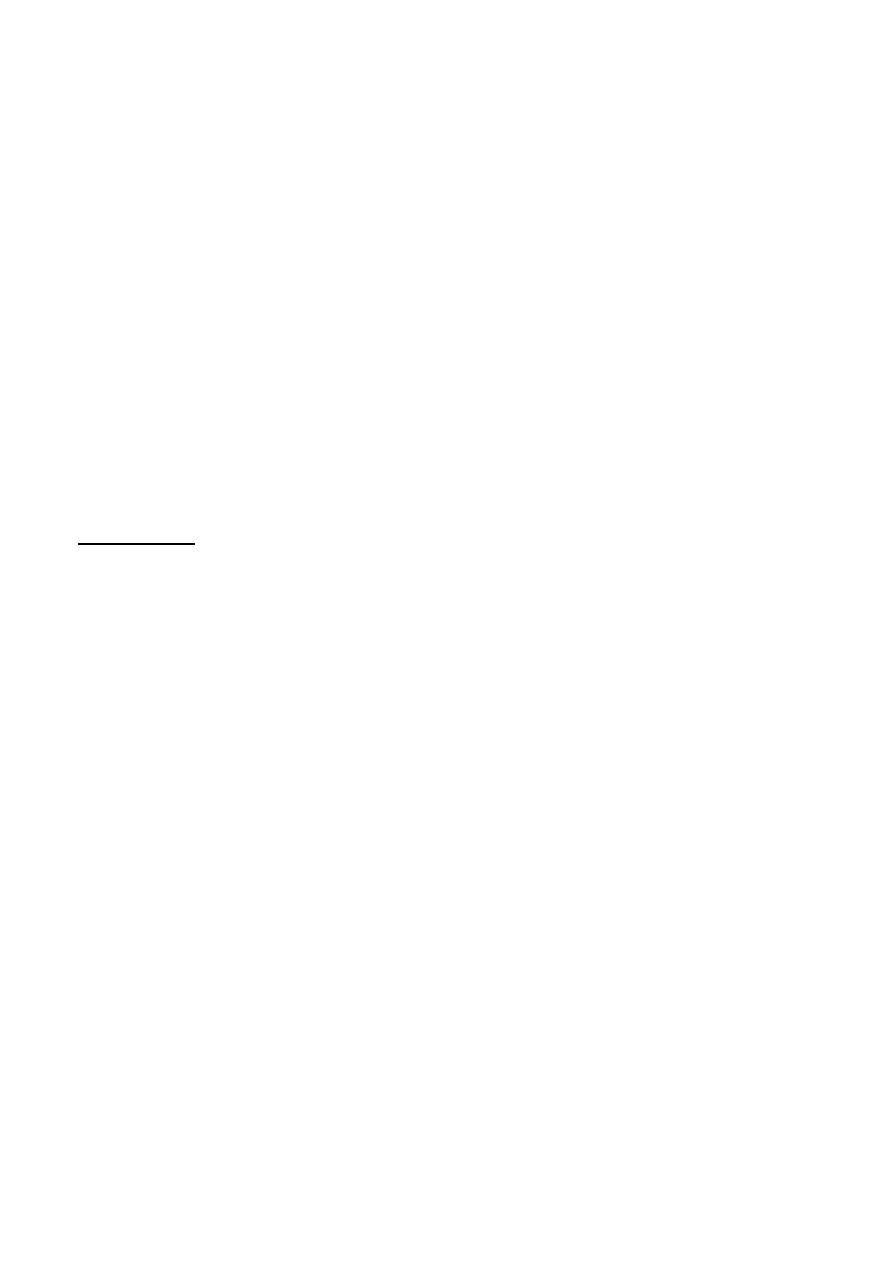
Pathology:
Spina bifida occulta I
◦ the mildest forms of dysraphism there is a midline defect between the
laminae;
◦ discovered incidentally on spine x-rays (usually affecting L5). However,
◦ if several vertebrae are affected - there are telltale defects in the overlying
skin, e.g. dimple, a pit or a tuft of hair.
◦ Occasionally there are associated intraspinal anomalies e.g. tethering of
the conus medullaris below LI, splitting of the spinal cord
(diastematomyelia) and cysts or lipomas of the cauda equina.
Spina bifida cystica
◦ more overt forms of dyspharism
◦ the vertebral laminae are missing and the contents of the vertebral canal
prolapse through the defect.
◦ The abnormality takes one of several forms:
The least disabling is a meningocele,
The most common and most serious abnormality is a
myelomeningocele,which is either 'closed' myelomeningocele or
'open' myelomeningocele
Hydrocephalus :
◦ Distal tethering of the cord may cause herniation of the cerebellum and
brain-stem through the foramen magnum, resulting in obstruction to CSF
circulation and hydrocephalus
Incidence and screening:
Isolated laminar defects are seen in over 5 per cent of lumbar spine x-rays
cystic spina bifida is rare at 2- 3 per 1000 live births.
if one child is affected the risk for future siblings is significandy higher.
Neural tube defects are associated with high levels of alpha-fetoprotein (AFP) in
the amniotic fluid and serum. This offers an effective method of antenatal
screening during the 15th to 18th week of pregnancy.
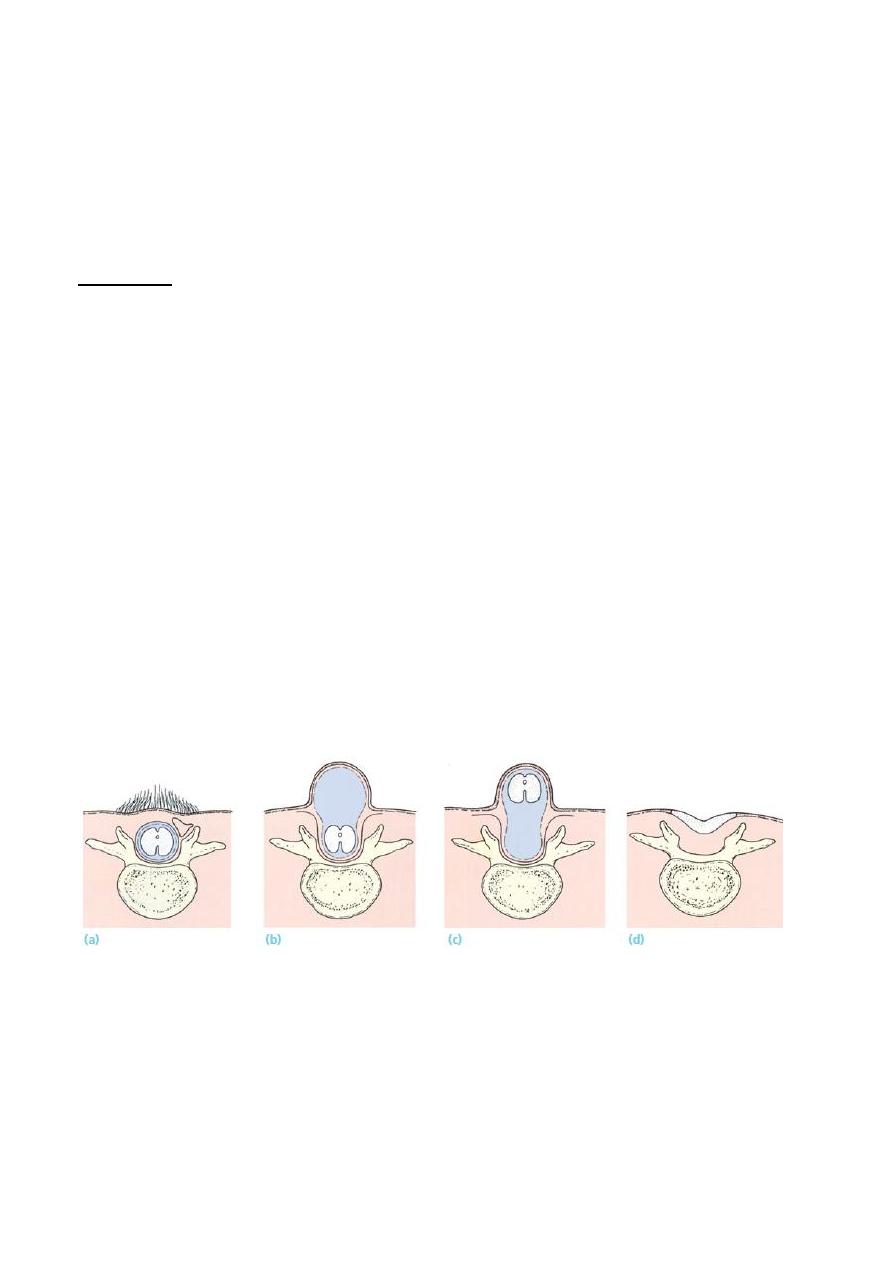
Clinical features:
EARLY DIAGNOSIS
Spina bifida occulta :
◦ encountered in normal people, and can usually be ignored.
◦ a posterior midline dimple, a tuft of hair or a pigmented naevus signifies
the potential for something more serious.
Spina bifida cystica
◦ obvious at birth in the shape of a saccular lesion overlying the lumbar spine.
Hydrocephalus may be present at birth.
Deformities of the lower limbs:
◦ equinovarus or calcaneovalgus of the feet,
◦ recurvatum of the knee and
◦ hip dislocation
probably due to a combination of factors
◦ muscle imbalance,
◦ lack of movement and abnormal limb position in utero,
◦ associated anomalies that are independent of the paralysis.
IN OLDER CHILDREN
the child (or teenager) with minor forms of spina bifida may presents with
◦ clawing of the toes,
◦ a change in gait pattern,
◦ incontinence or abnormal sensation.
This delayed presentation is often attributed to the tethered cord syndrome.

Treatment:
In recent years intrauterine surgery has been attempted.
early management timing:
Age procedure
1 day close skin defect
1week ventriculo-caval shunt
1month stretch and strap
6months-3 years orthopaedic procedure
Whenever needed urogenital operation
Surgery may include
◦ soft tissue release,
◦ tendon lengthening or transfer
◦ osteotomy.
◦ arthrodesis
Always associated with splintage & physiotherapy
Poliomyelitis
is an acute infectious viral disease, spread by the oropharyngeal route, that
passes through several distinct phases.
around 10 % of patients exhibit any symptoms at all.
involvement of the CNS occurs in less than 1 %of cases with effects on the
anterior horn cells of the spinal cord and brain-stem, leading to LMN (flaccid)
paralysis of the affected muscle groups.
Clinical features:
Poliomyelitis typically passes through several clinical phases,
◦ The acute illness :
fever and headache; in about one-third of cases the patient gives a
history of a minor illness with sore throat, mild headache and slight
pyrexia 5-7 days before.
As the symptoms increase in severity, neck stiffness appears and
meningitis may be suspected.
the muscles are painful and tender
◦ Paralysis: Soon muscle weakness appears; it reaches a peak in the course of
2-3 days and may give rise to difficulty with breathing and swallowing pain
and pyrexia subside after 7–10 days
◦ Recovery and convalescence A return of muscle power is most noticeable
within the first 6 months, but there may be continuing improvement for up
to 2 years
◦ Residual paralysis in some patients, recovery is incomplete and they are
left with some degree of asymmetric flaccid (LMN) that in time leads to
joint deformities and growth defects.

Treatment
Early treatment:
the patient is isolated and kept at complete rest, with symptomatic treatment for
pain and muscle spasm.
Active movement is avoided but gentle passive stretching helps to prevent
contractures.
Once the acute illness settles, physiotherapy is stepped up, active movements are
encouraged.
splintage may be necessary to maintain joint and limb alignment and prevent
fixed deformities.
Late treatment:
Once the severity of residual paralysis has been established, there are a number
of basic problems that need to be addressed:
◦ Isolated muscle weakness without deformity: (brace, tendon transfer)
◦ Passively corrective deformity:
splint (a calliper or lightweight brace).
tendon transfer
◦ Fixed deformity:
restore alignment operatively,
arthrodesis
Flail joint:
◦ no treatment
◦ Stabilized by splintage or by arthrodesis.
Shortening:
◦ shoe raise
◦ leg lengthening
◦ well-timed epiphyseodesis in the normal limb.
Done by : Murtedha Abbas