Bones
Congenital diseases
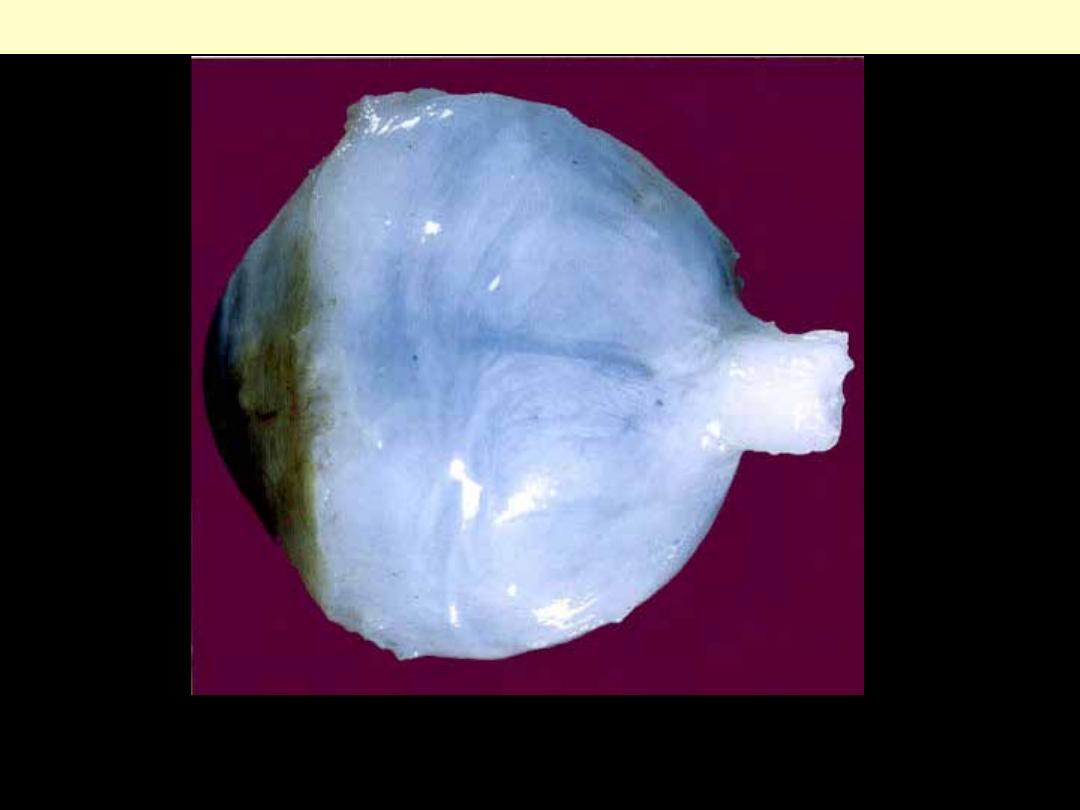
Patients with this condition have abnormally fragile bones and suffer multiple repeated fractures. They
usually have blue-coloured sclerotics, as is shown in this eye from a child who died from this condition.
Osteogenesis imperfecta
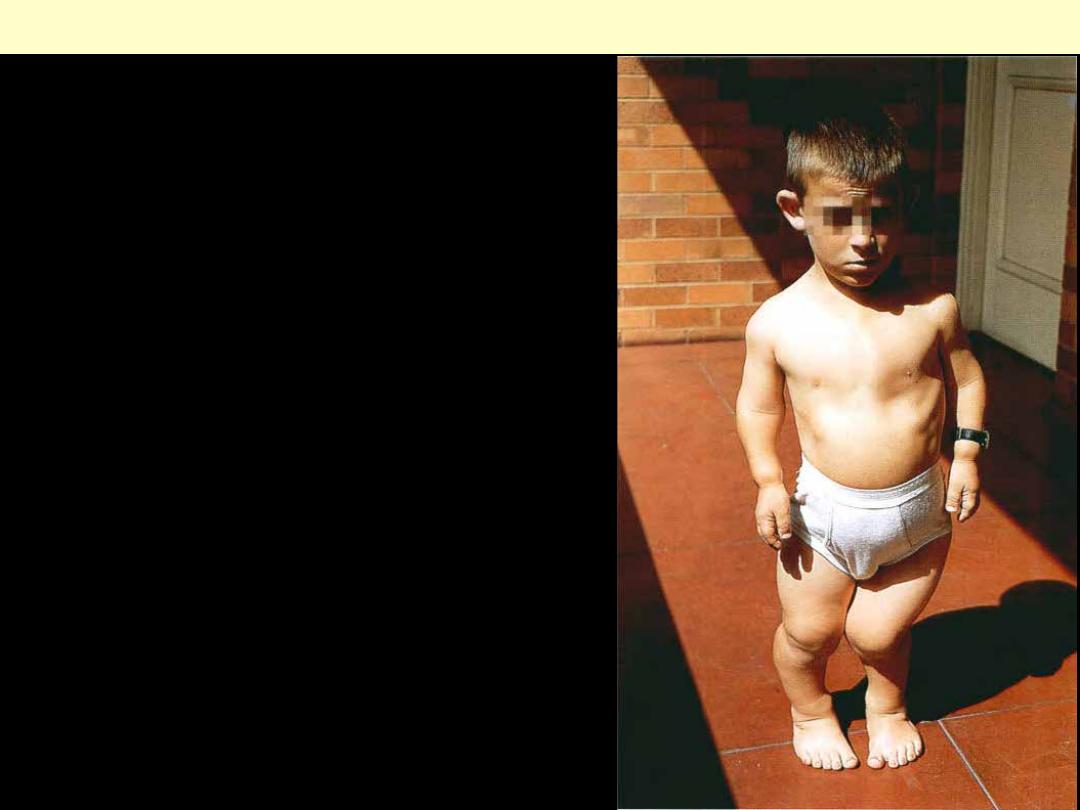
M/6. The patient demonstrates the short arms and legs of
this inherited abnormality of endochondral ossification.
Achondroplasia
Fractures
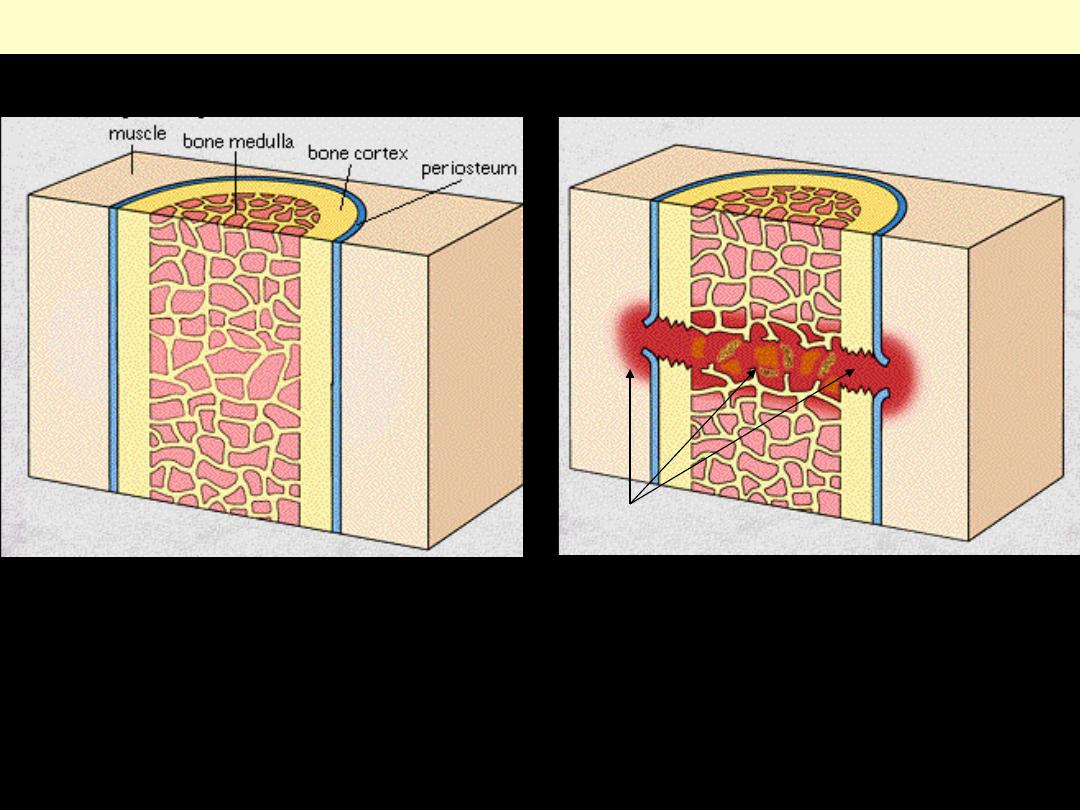
Bone fracture-hematoma formation
Normal bone
Early fracture
Hematoma
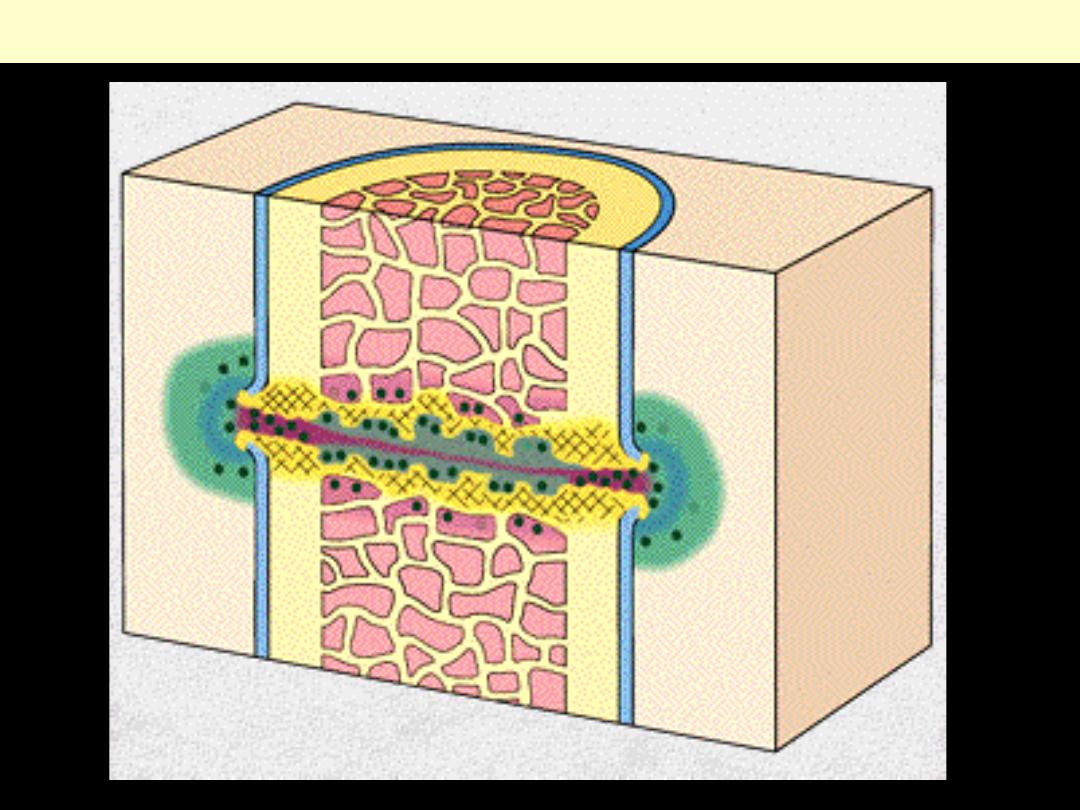
Bone fracture-osteoid (woven bone) formation
Callus in third week: replacement by compact mature lamellar bone
Lamellar bone
Fracture callus
Fractured native
bone trabeculae:
(lamellar)
Callus: woven bone
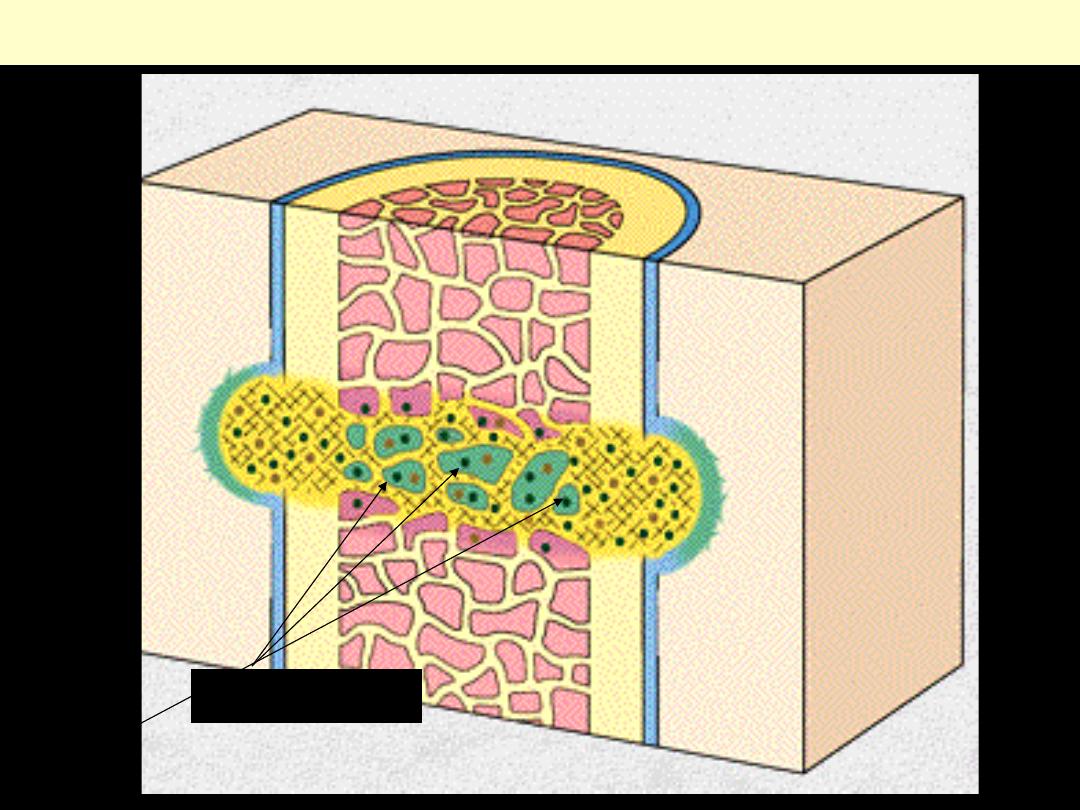
Fractured lamellar bone trabeculae
Callus: woven bone
Fracture callus
Osteoblasts rimming
trabeculae of woven
bone
osteoclast
exuberant callus formation following
fracture .
Hyperparathyroidism
Osteitis fibrosa
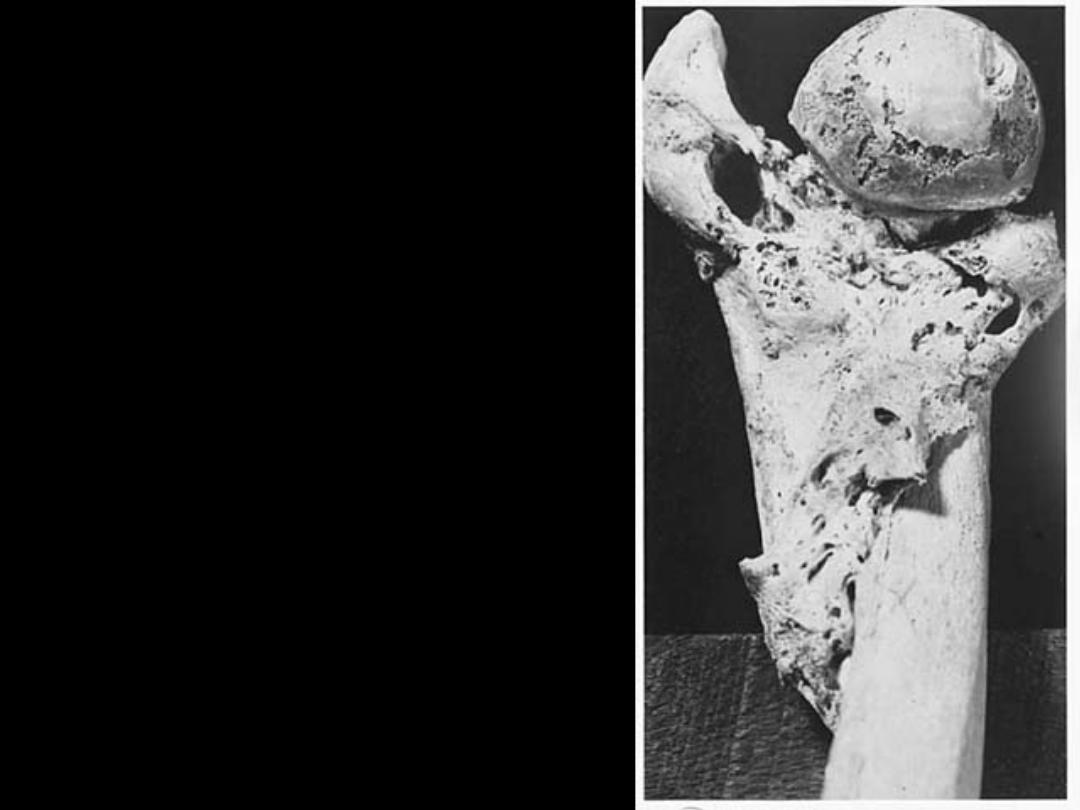
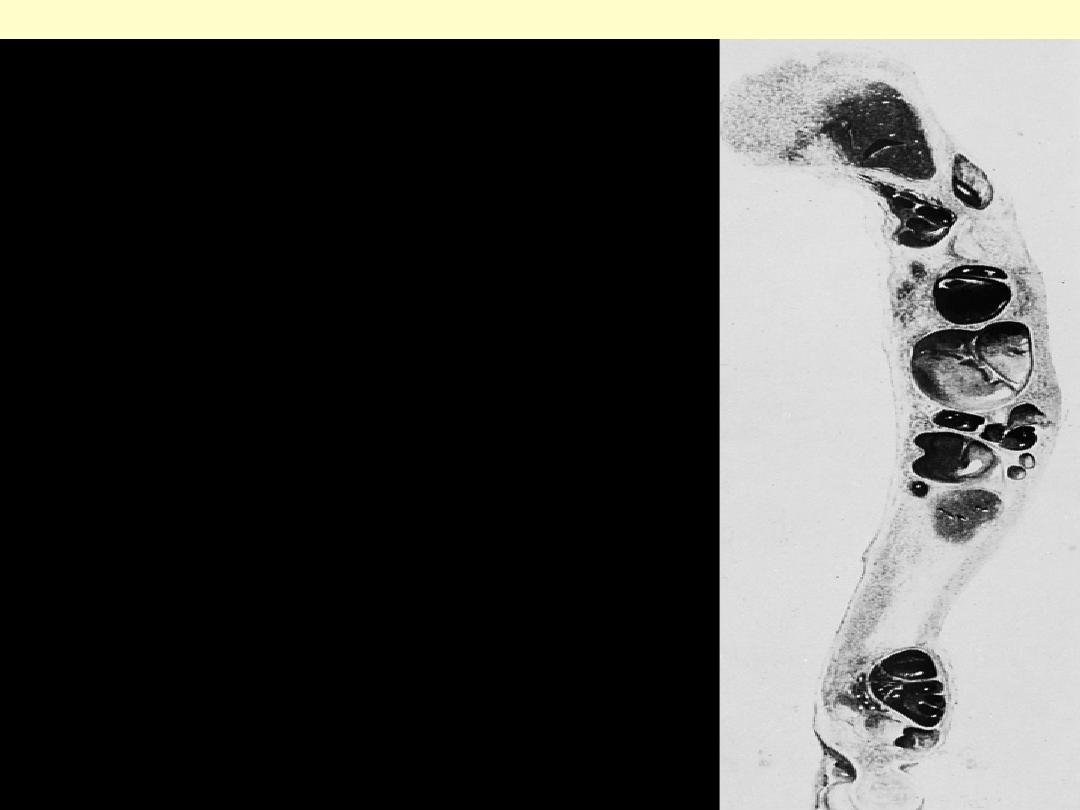
Historical example of extreme osteitis fibrosa cystica.
Note deformity of bone with numerous cysts and brown
tumors.

Osteitis fibrosa
Cystic changes and cortical alterations in bones of
hands of patient with functioning parathyroid
adenoma.
Dramatic change evident 9 months after
removal of adenoma.

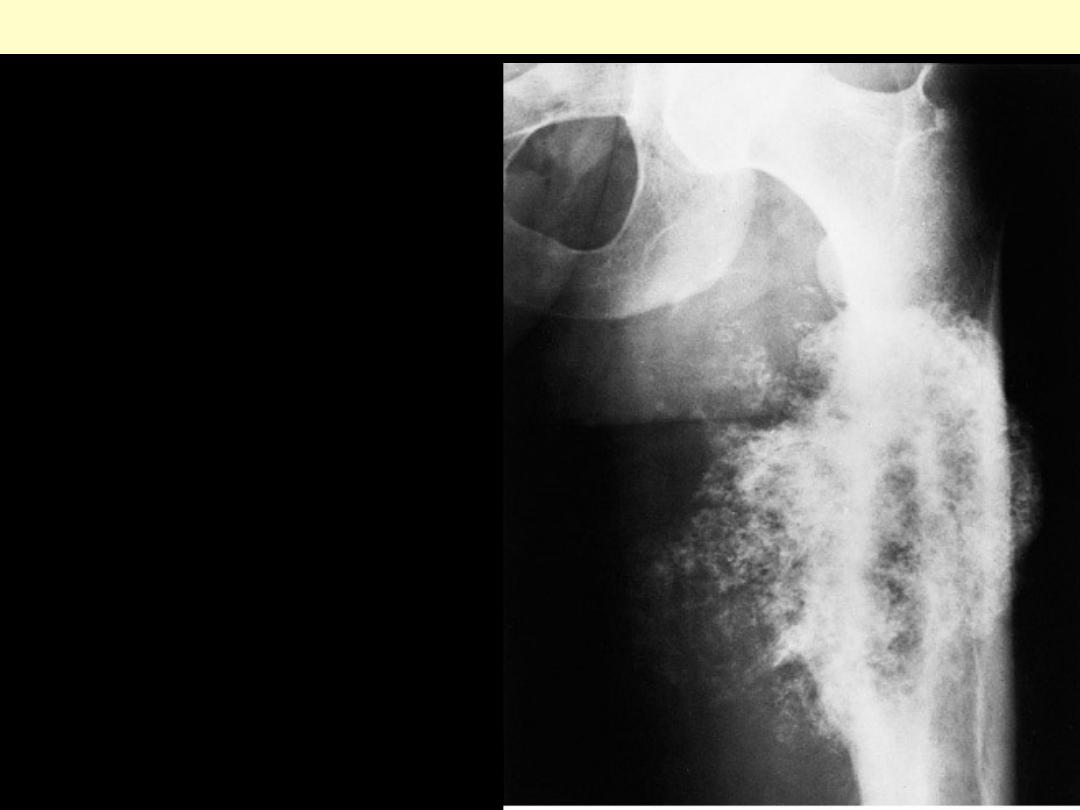
Extensive changes in bones of
pelvis and femur caused by
functioning parathyroid adenoma.
Osteitis fibrosa
Same pelvis and femur 8 years after
removal of adenoma. Note complete
reversion to normal.
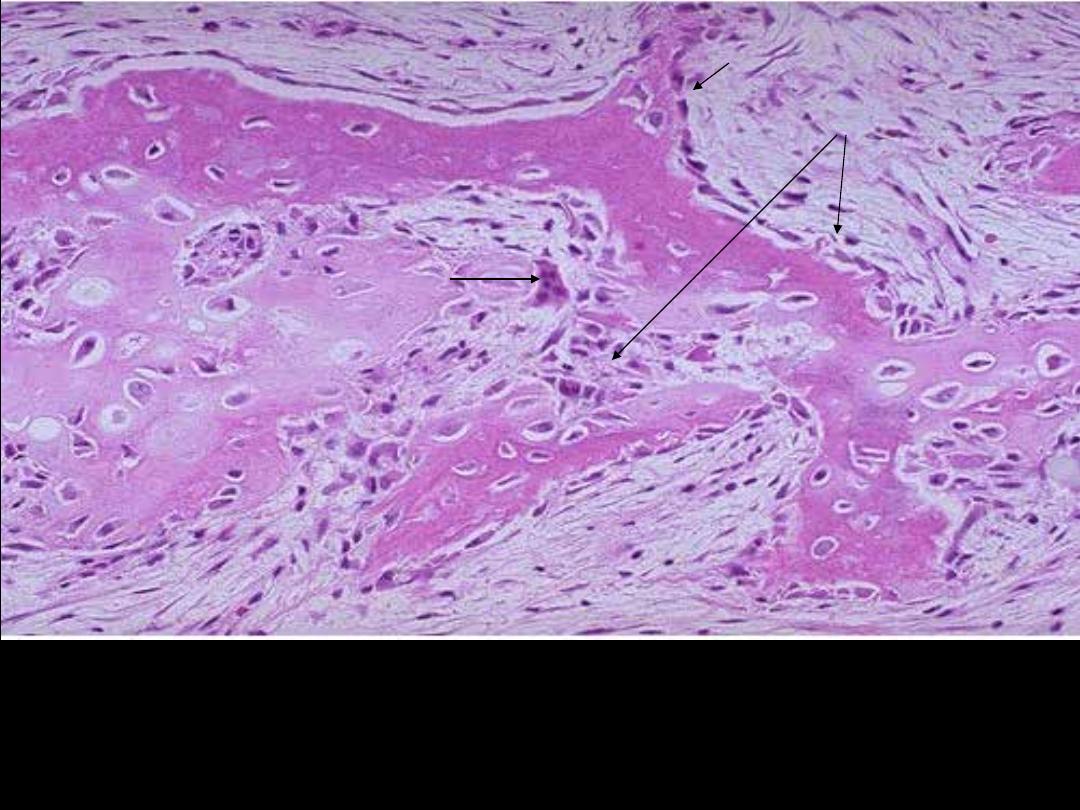
Bone changes in hyperparathyroidism. There is
marked resorption of bone trabeculae and
clustering of osteoclasts.
Osteitis fibrosa bone
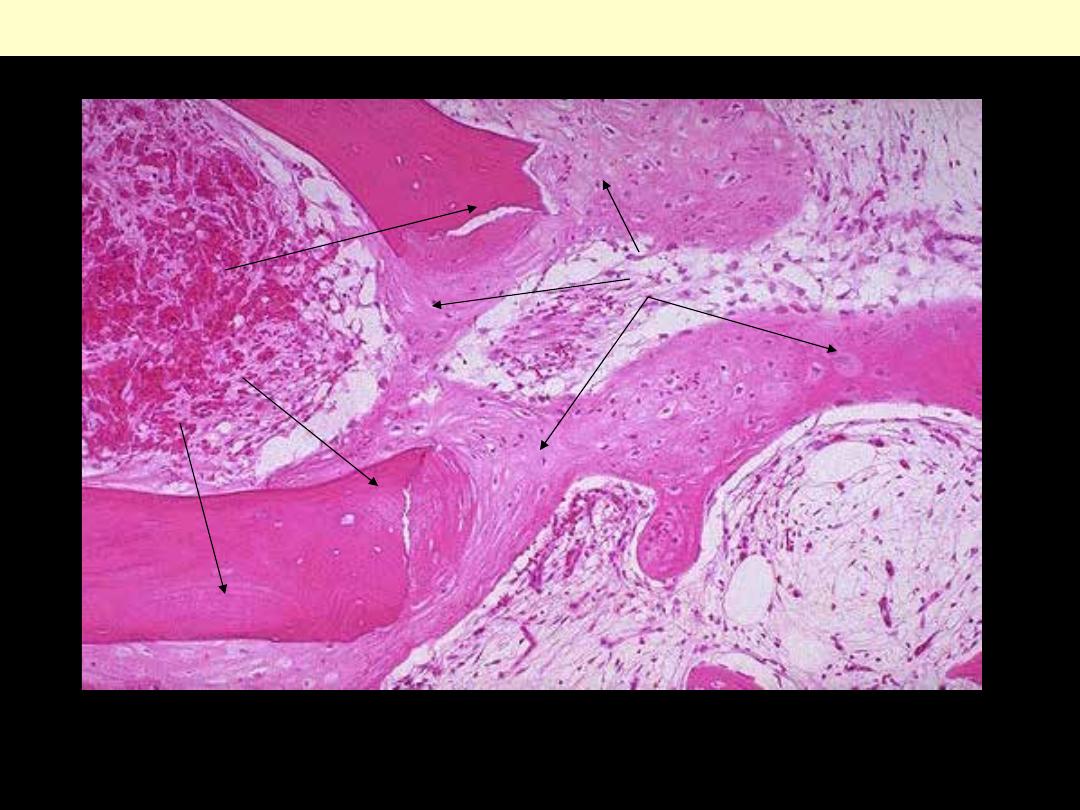
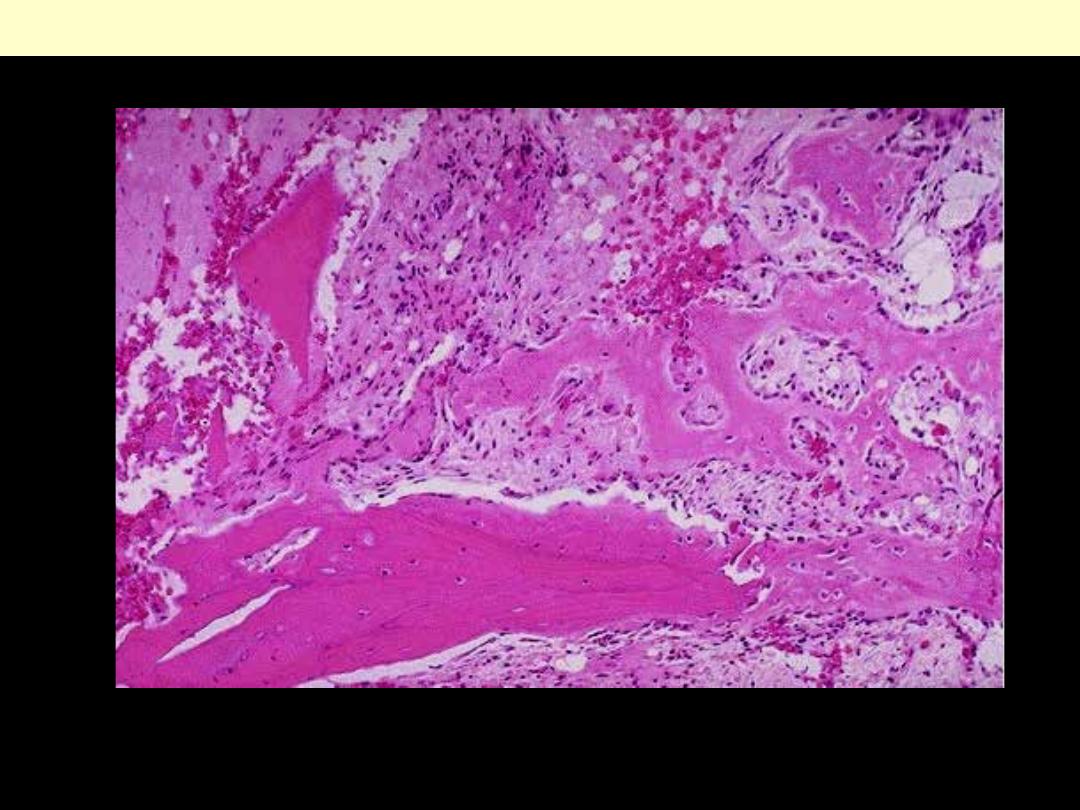
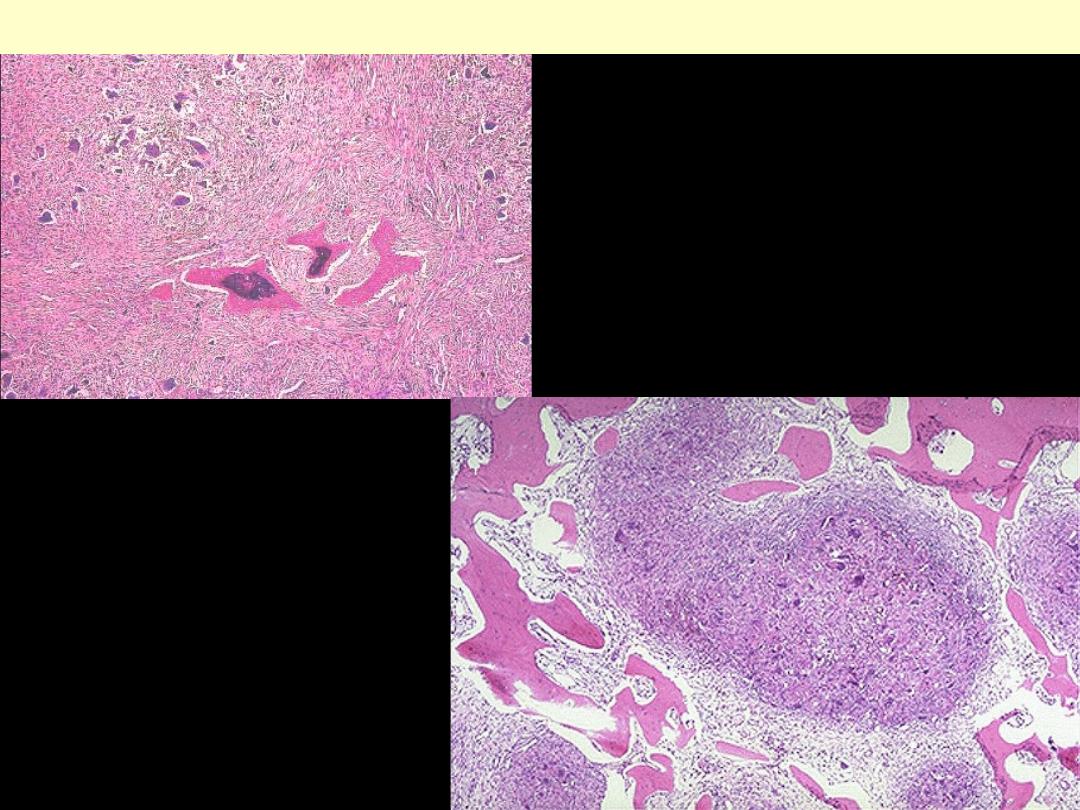
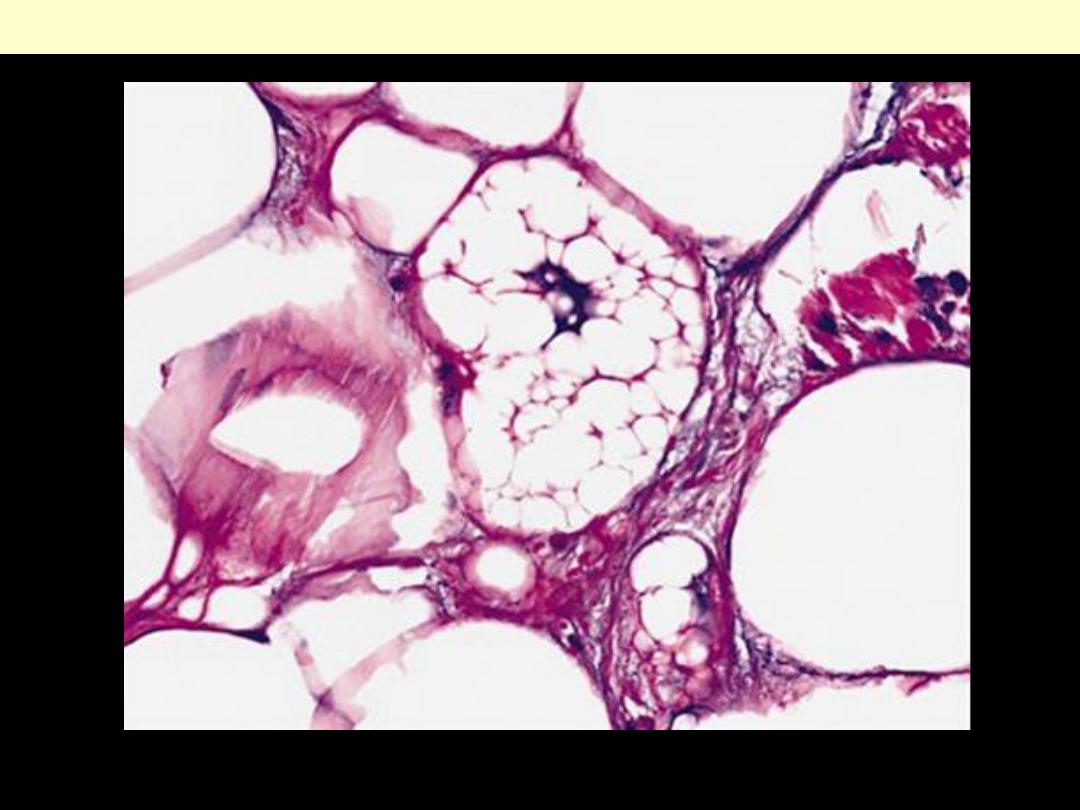
Here is a "brown tumor" of bone in a
patient with hyperpara-thyroidism. The
high parathormone levels increase
osteoclast activity and produce irregular
bone resorbtion with microfractures and
hemorrhage and macrophage
proliferation and fibrous connective
tissue proliferation.
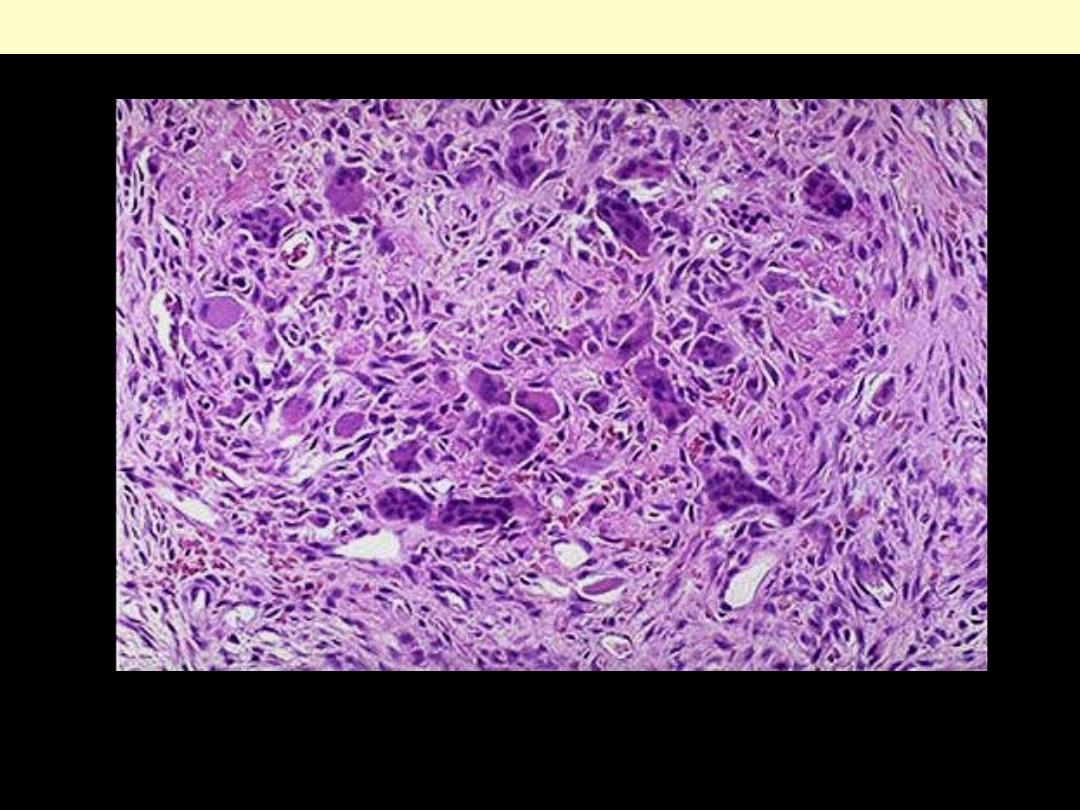
The center of the "brown tumor" contains osteoclasts, mononuclear cells and fibroblasts with focal
hemorrhages. The hemosiderin from the hemorrhage produces the grossly brown color. Such lesions
are nowadays uncommon because hyperparathyroidism is treated before such lesions develop.
Osteitis fibrosa /brown tumor/ hyperparathyroidism
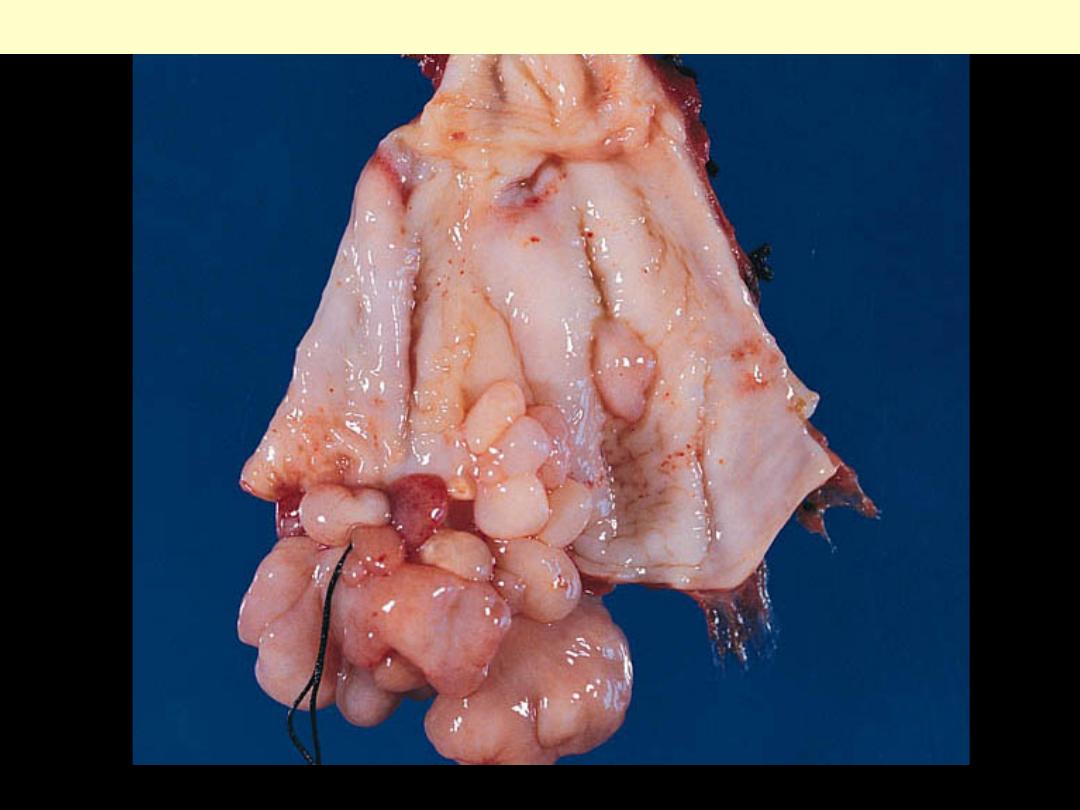
Osteomyelitits
There is a large collection of pus in the
medullary cavity of the shaft of the femur. This
patient died from acute leukaemia, and the
infection resulted from her immune deficiency
state.
Acute osteomyelitis
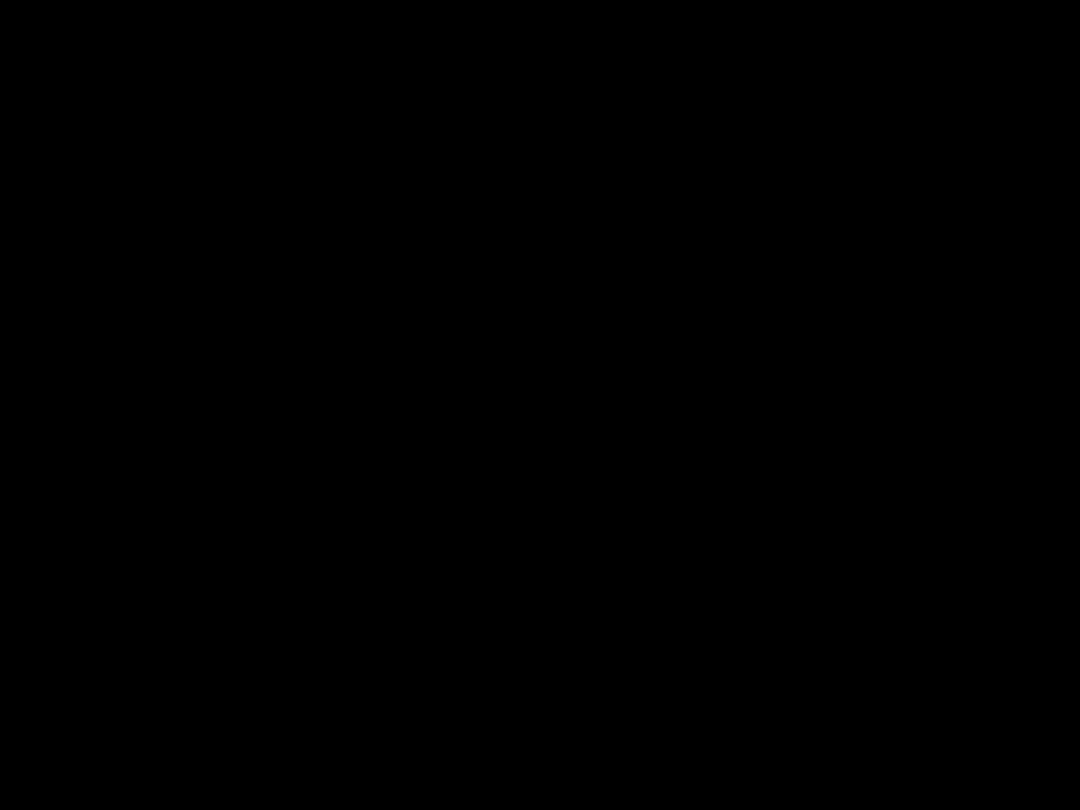
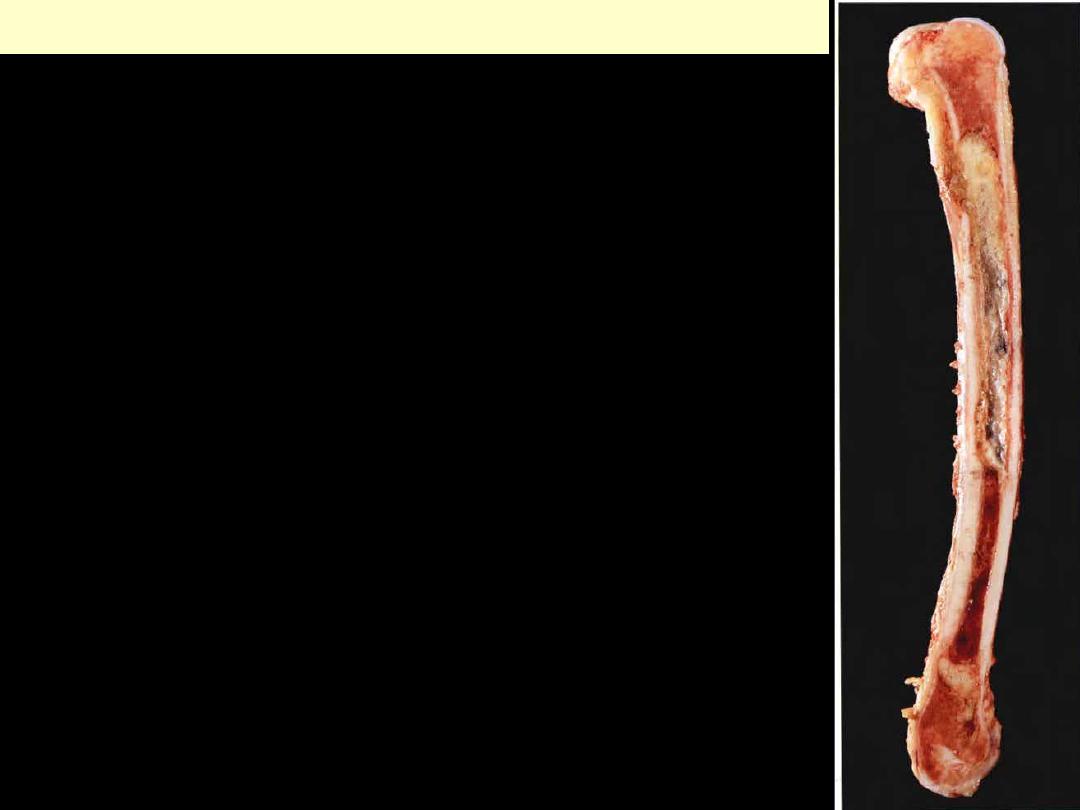
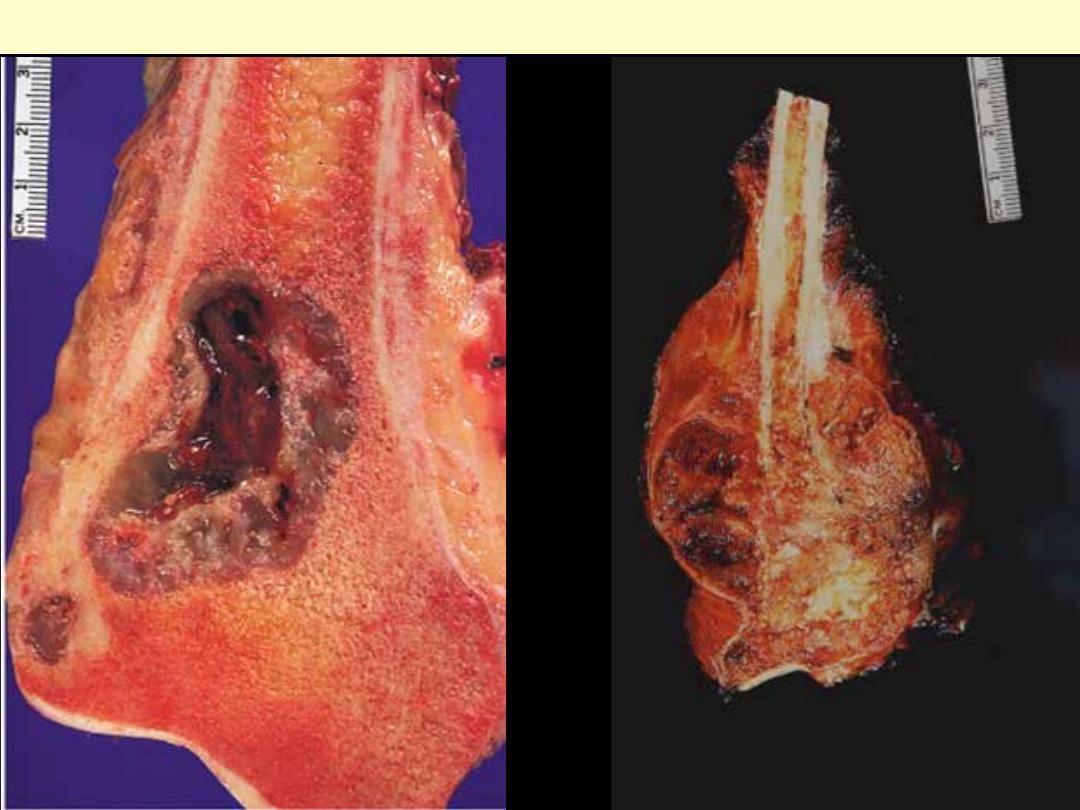
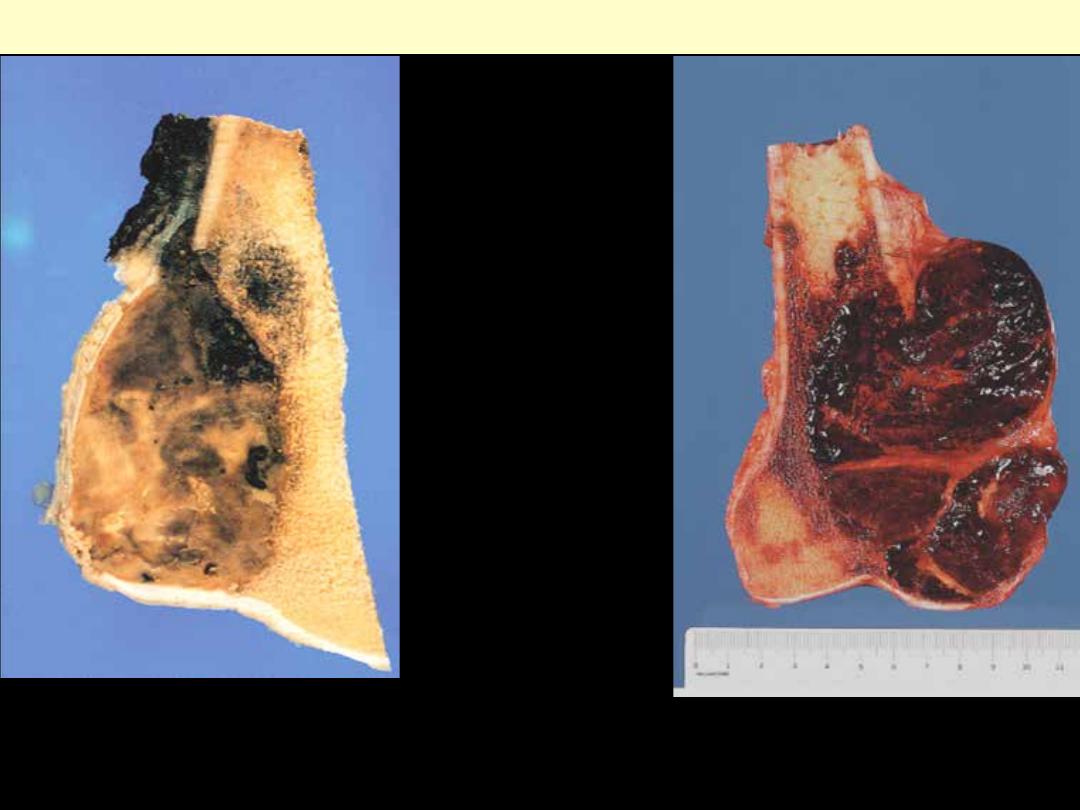
Resected femur from a person with
chronic osteomyelitis. Necrotic bone (the
sequestrum) visible in the center of a
draining sinus tract is surrounded by a
rim of new bone (the involucrum).
Chronic osteomyelitis
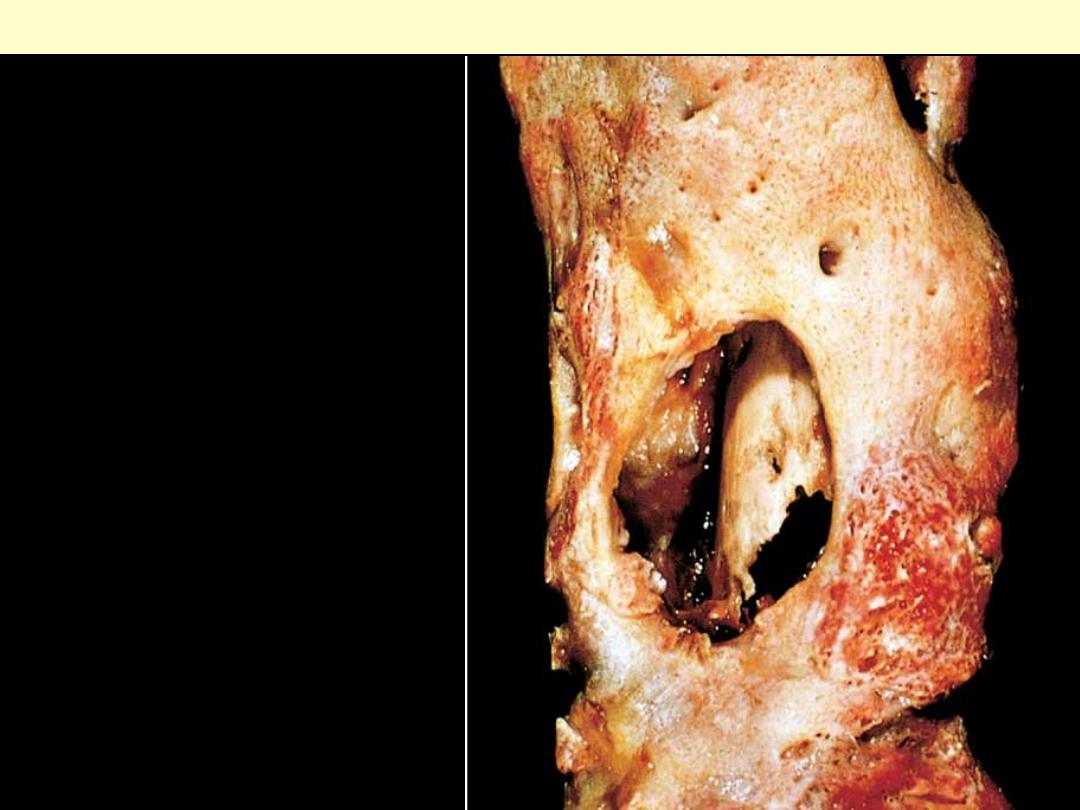
Osteomyelitis: fenestrations of bone
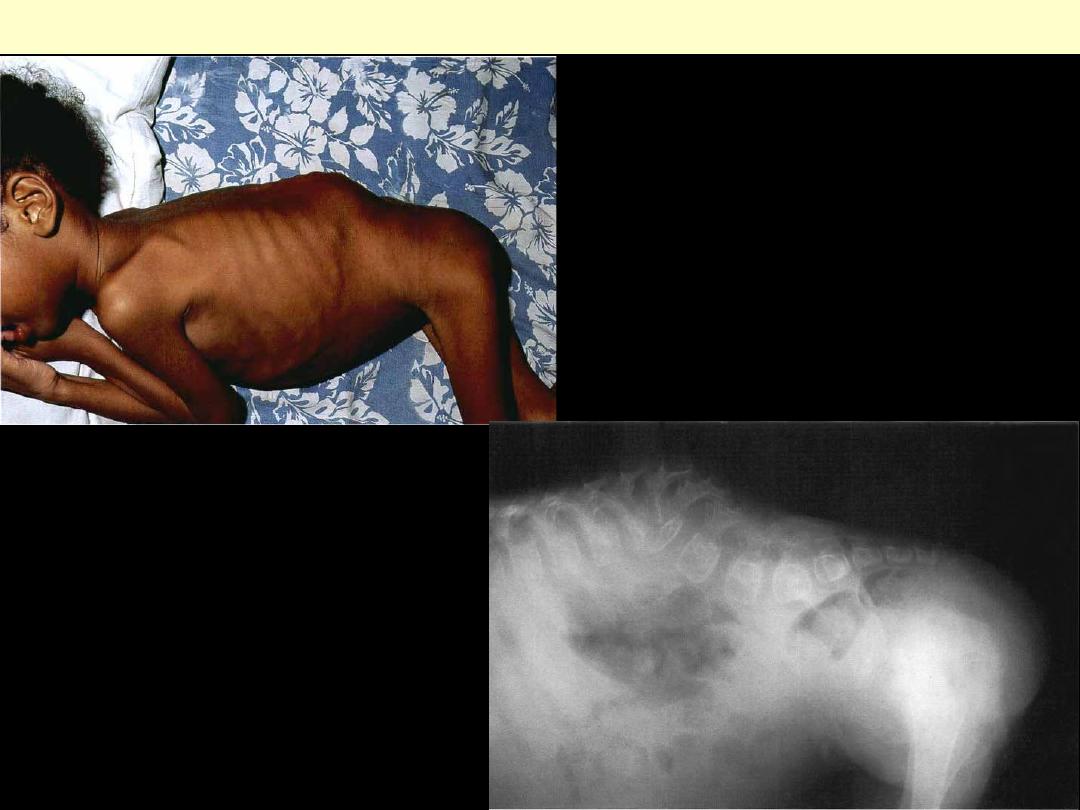
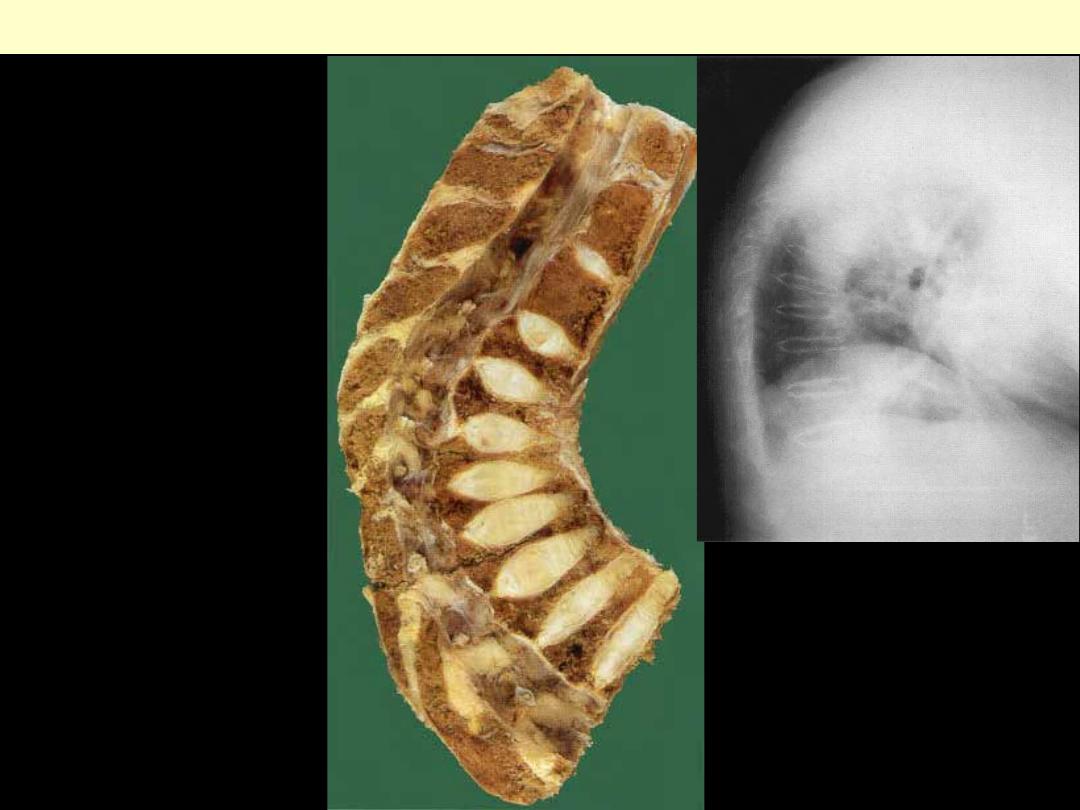
A. This child is grossly emaciated from the
disseminated infection. The deformity in the
lumbar region is characteristic of involvement
of the lumbar vertebrae by tuberculous
infection. The diseased vertebrae 'collapsed‘
B. X-ray of the child shown in A. The collapsed
lumbar vertebrae are easily seen.
Tuberculosis of the spine (Pott disease)
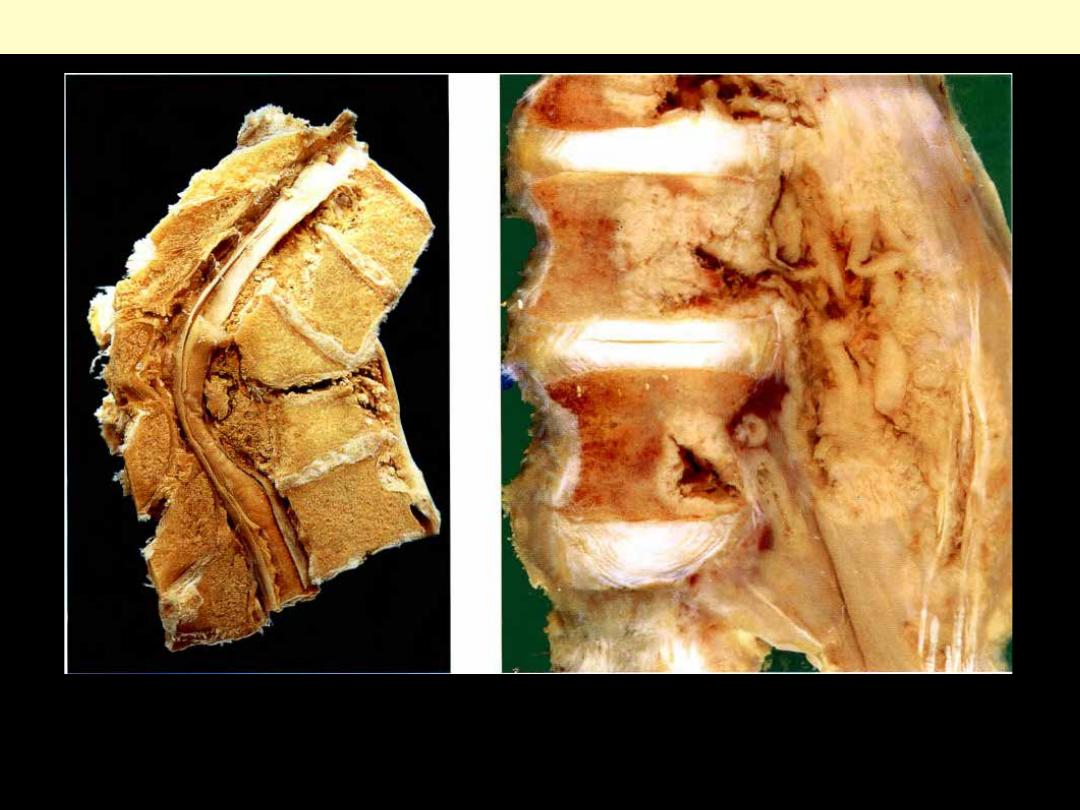
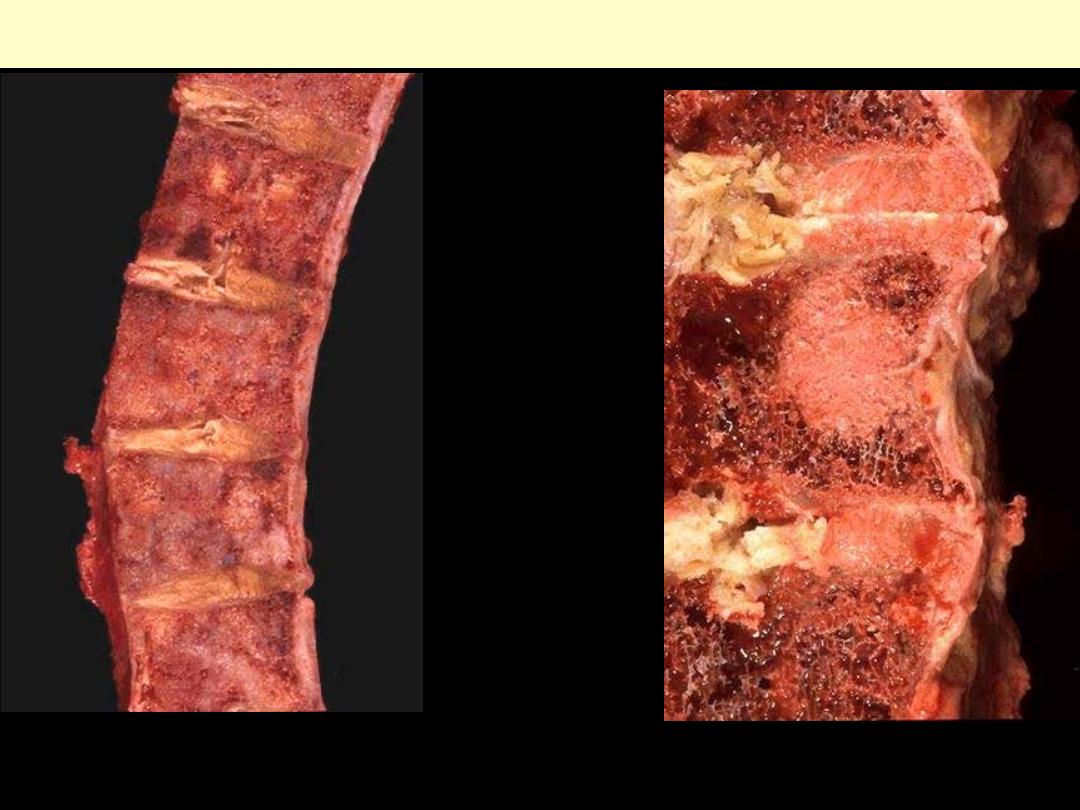
Rt. Tuberculosis in the spine of a young boy (Pott's fracture of the vertebrae).
Lt, Tuberculous psoas abscess. Two lumbar vertebrae involved by tuberculosis with extension of the
caseation into the psoas muscle. When such infection spreads along the psoas, the abscess may 'point'
in the groin.
Tuberculosis of the spine (Pott disease)
Osteonecrosis

Note the wedge-shaped area of avascular
necrosis (osteonecrosis) at the upper right
of this femoral head. Avascular necrosis
results from bone ischemia, which can be
due to many causes, including trauma and
corticosteroid administration, though
idiopathic cases are common. There is pain
with activity, progressing to pain at rest.
Eventually, the necrotic bone collapses,
distorting the overlying articular cartilage
and producing secondary osteoarthritis.
Avascular necrosis bone
Osteoporosis
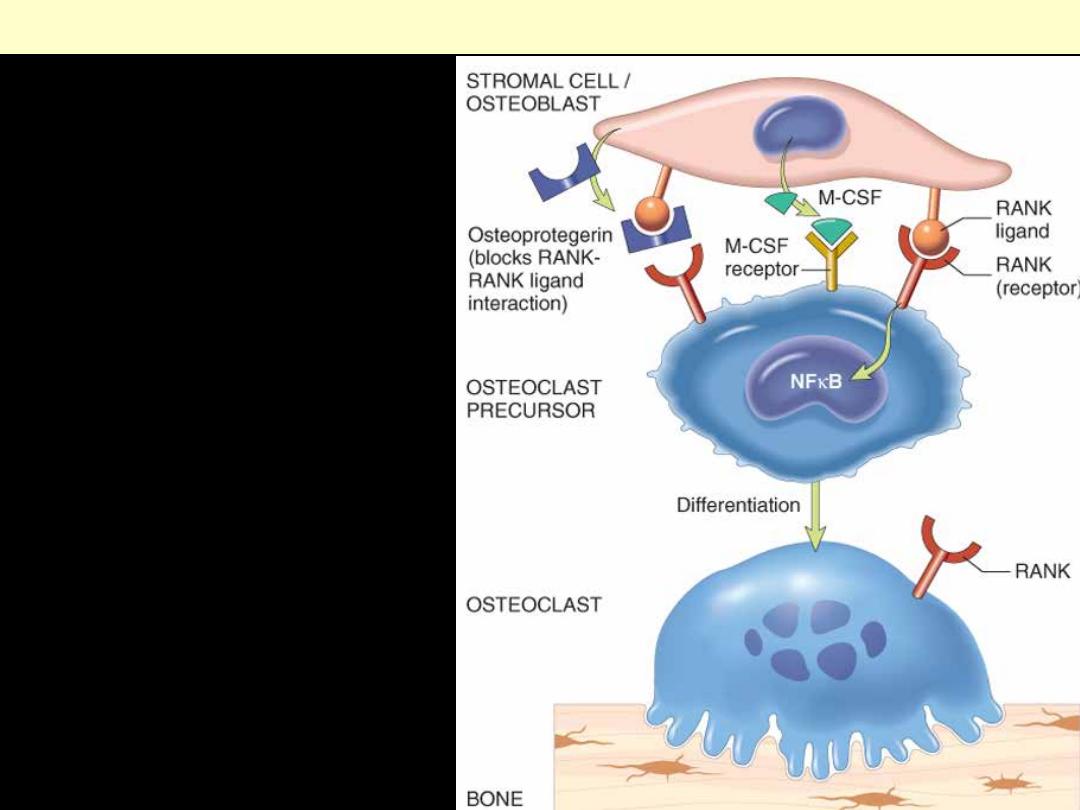
Osteoclasts are derived from the same
stem cells that produce macrophages.
RANK (receptor activator for nuclear
factor-
κB) receptors on osteoclast
precursors bind RANK ligand (RANKL)
expressed by osteoblasts and marrow
stromal cells. Along with macrophage
colony-stimulating factor (M-CSF), the
RANK-RANKL interaction drives the
differentiation of functional osteoclasts.
Stromal cells also secrete osteoprotegerin
(OPG) that acts as a decoy receptor for
RANKL, preventing it from binding the
RANK receptor on osteoclast precursors.
Consequently OPG prevents bone
resorption by inhibiting osteoclast
differentiation.
Paracrine mechanisms regulating osteoclast formation and function.
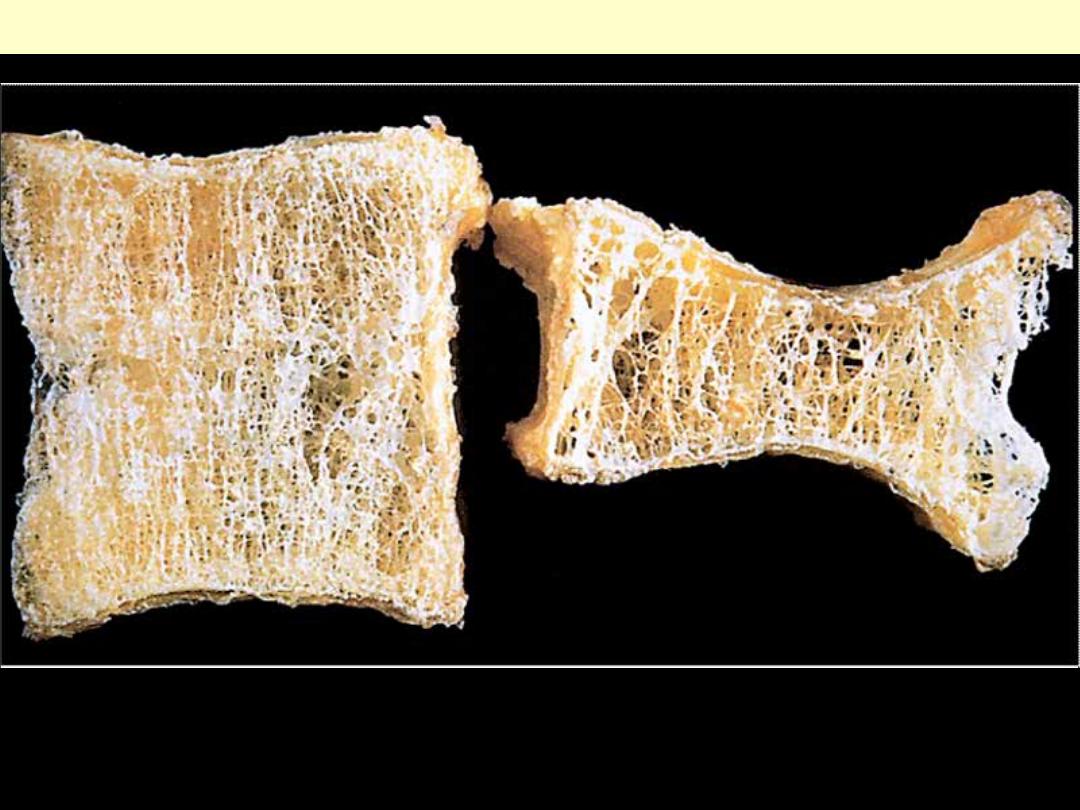
Osteoporotic vertebral body (right) shortened by compression fractures, compared with a normal
vertebral body. Note that the osteoporotic vertebra has a characteristic loss of horizontal trabeculae
and thickened vertical trabeculae.
Osteoprosis
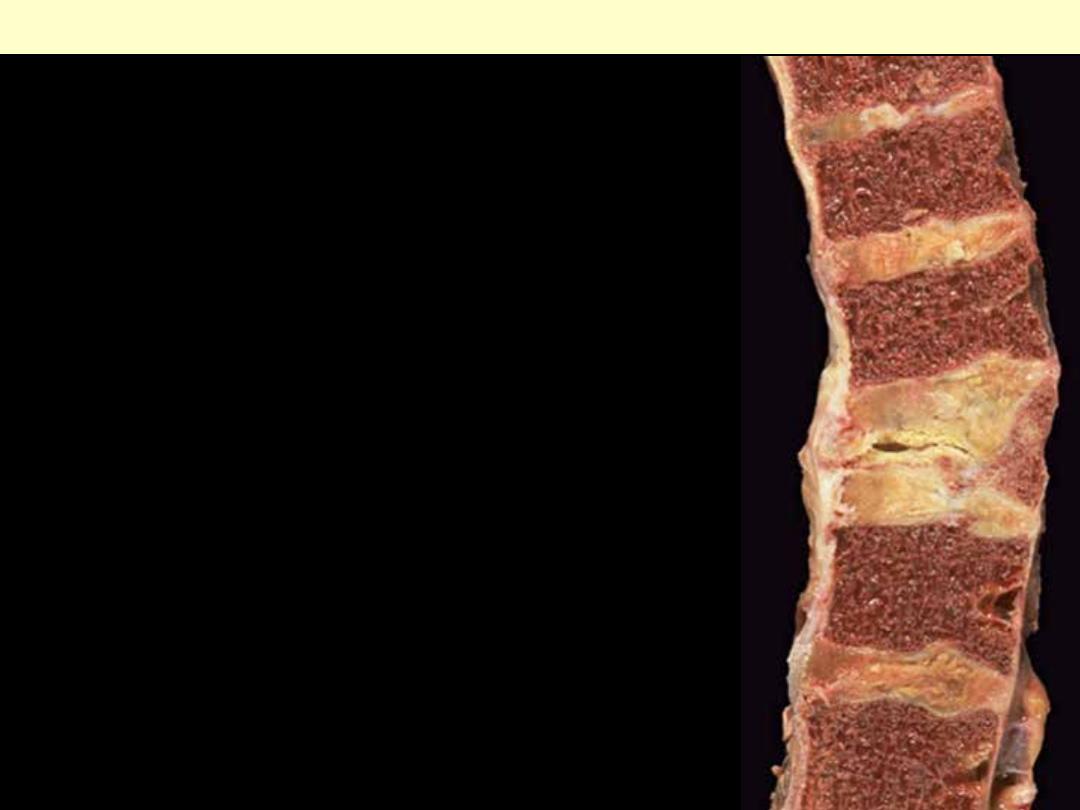
Here is a "compressed" fracture of the vertebral column.
The middle vertebral body shown here is greatly reduced in
size. Such fractures are common in persons with
osteoporosis in which there is accelerated bone loss,
particularly older women, and can occur with even minor
trauma.
Osteoprosis
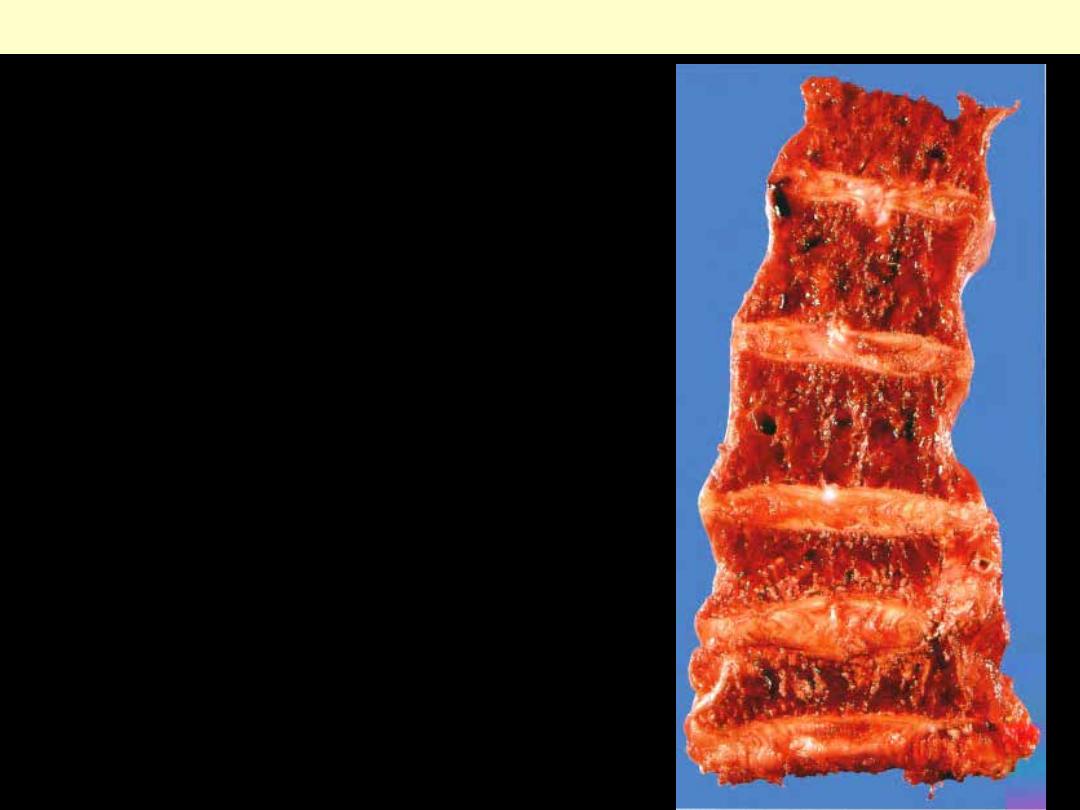
The trabecular bone in the vertebral bodies is very thin and
the two lower vertebrae show the effects of crush fracture - a
complication of this condition.
Osteoprosis
Lt. This vertical slice
through the thoracic spine
shows severe osteoporosis of
the vertebrae, with the
characteristic 'bowing' or
'curvature' of the spine
caused by collapse of the
anterior portions of the
vertebral bodies.
Osteoporosis of this severity
is more common in
postmenopausal women. It is
frequently associated with
nerve pain caused by
compression of the nerves as
they pass through the
intervertebral foramina.
Rt. X-ray of the patient
shown taken some months
before his death.
Osteoprosis
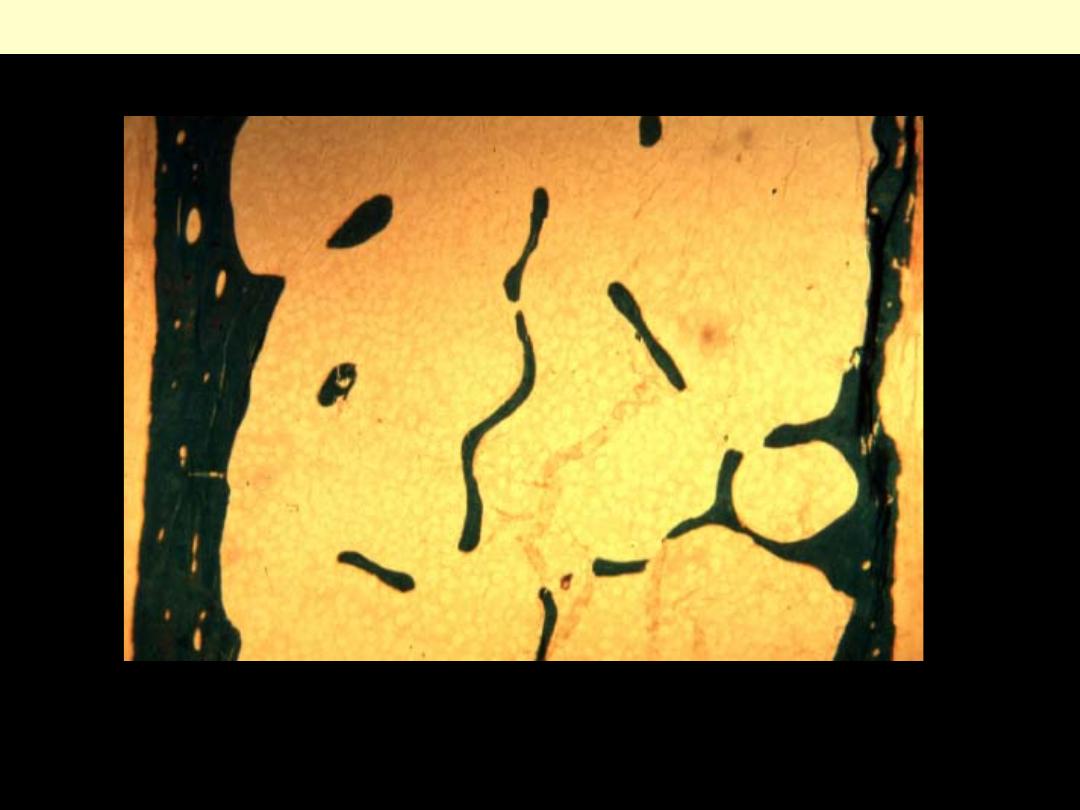
Micro: thin trabeculae disconnected from each other
Osteoporosis
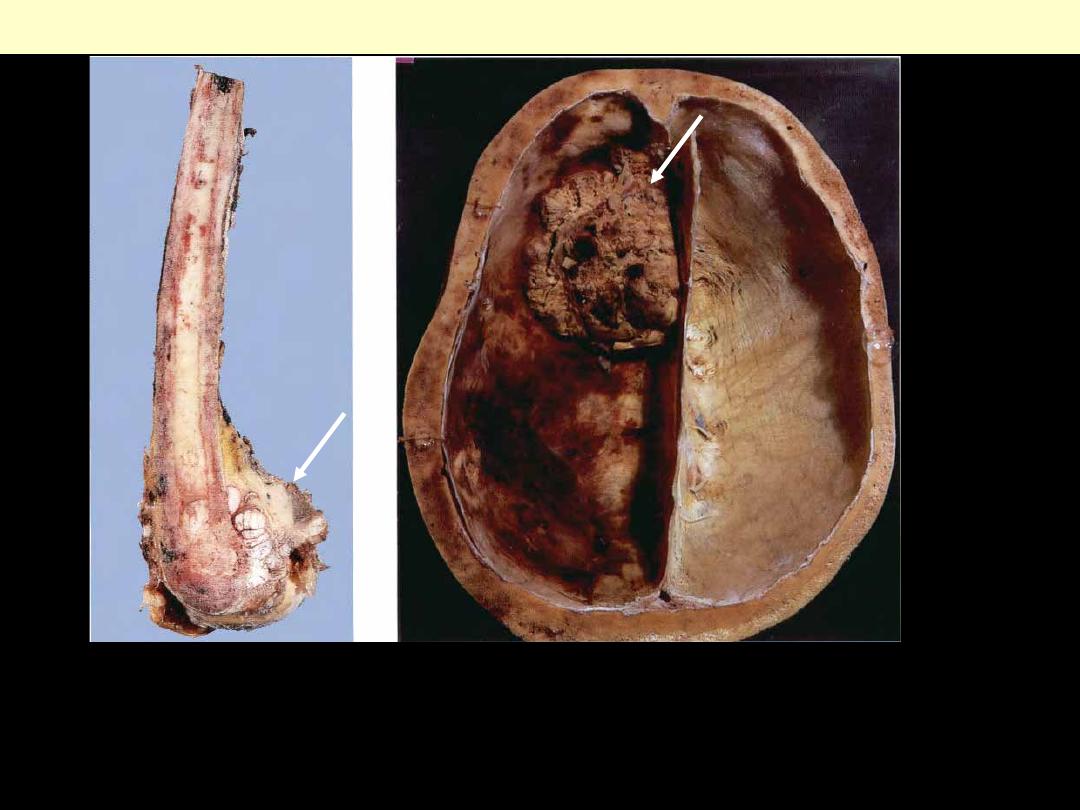
Paget’s disease

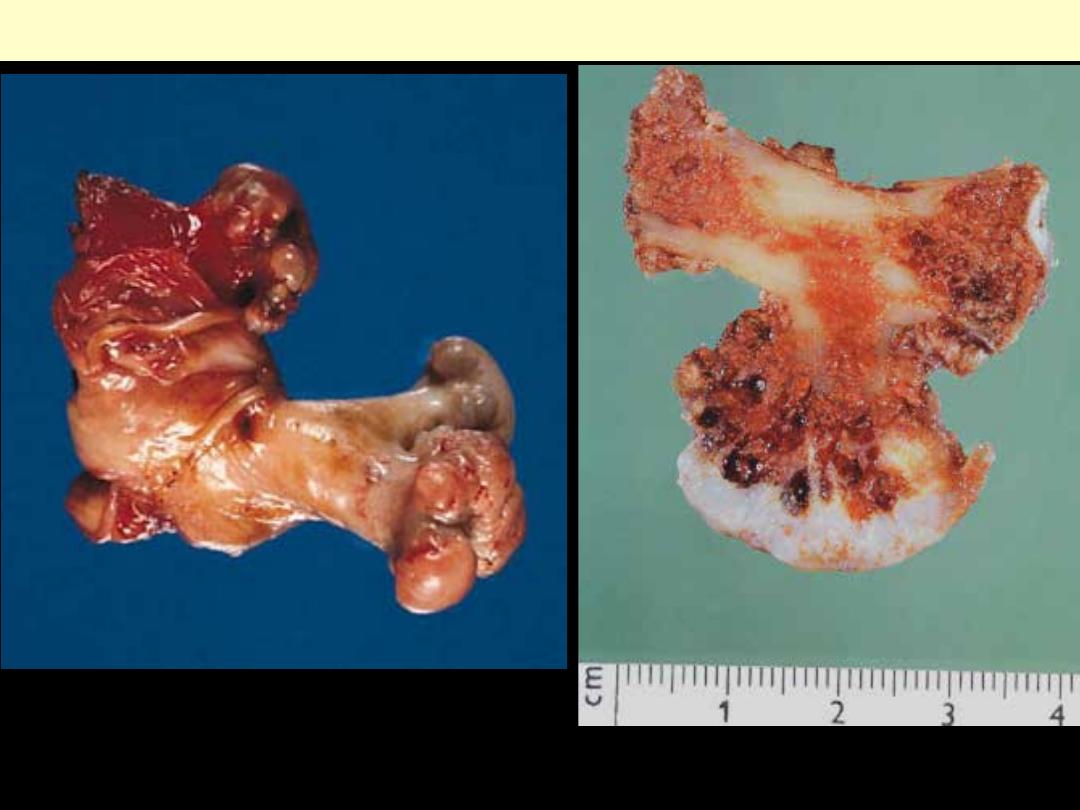
Lt., longitudinal slice of a tibia from a case of Paget disease, showing the marked thickening of the
cortical bone. The bone is thick, but softer than normal bone. As a result there is anterior bowing of the
tibia, and the bones are more liable to fracture than are normal bone.
Rt., Paget disease of the skull. Note the gross thickening of the diploe of the skull. The bone is
extremely vascular. This vascularity sometimes results in cardiac failure in patients with Paget disease.
Paget disease of bone
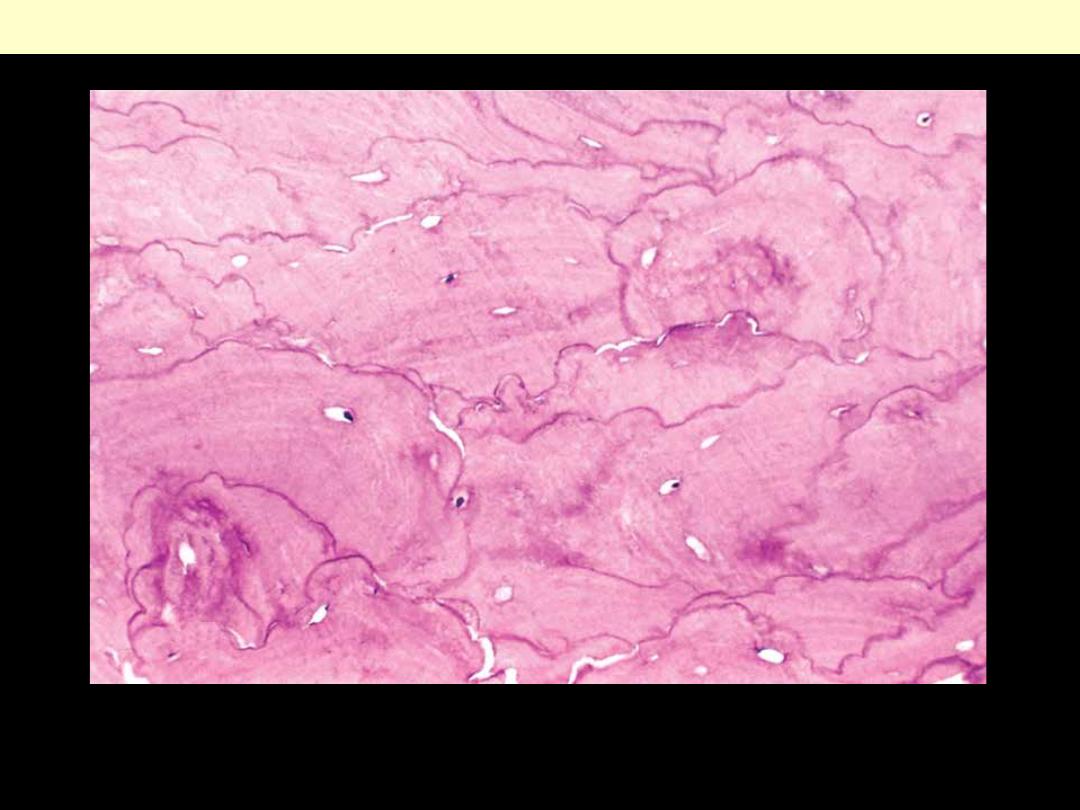
Mosaic pattern of lamellar bone pathognomonic of Paget disease.
Paget disease of bone
Rt., the sliced femur shows thickening of the cortical bone. An osteogenic sarcoma has arisen at the
distal end of the bone (arrow). Osteogenic sarcoma is a well recognized complication of Paget disease.
There are two age peaks for osteogenic sarcoma, one in adolescents and young adults, and the second in
older people with Paget disease.
Lt., Paget disease of the skull complicated by the development of an osteogenic sarcoma (arrow).
Paget disease of bone
Rickets + Osteomalacia
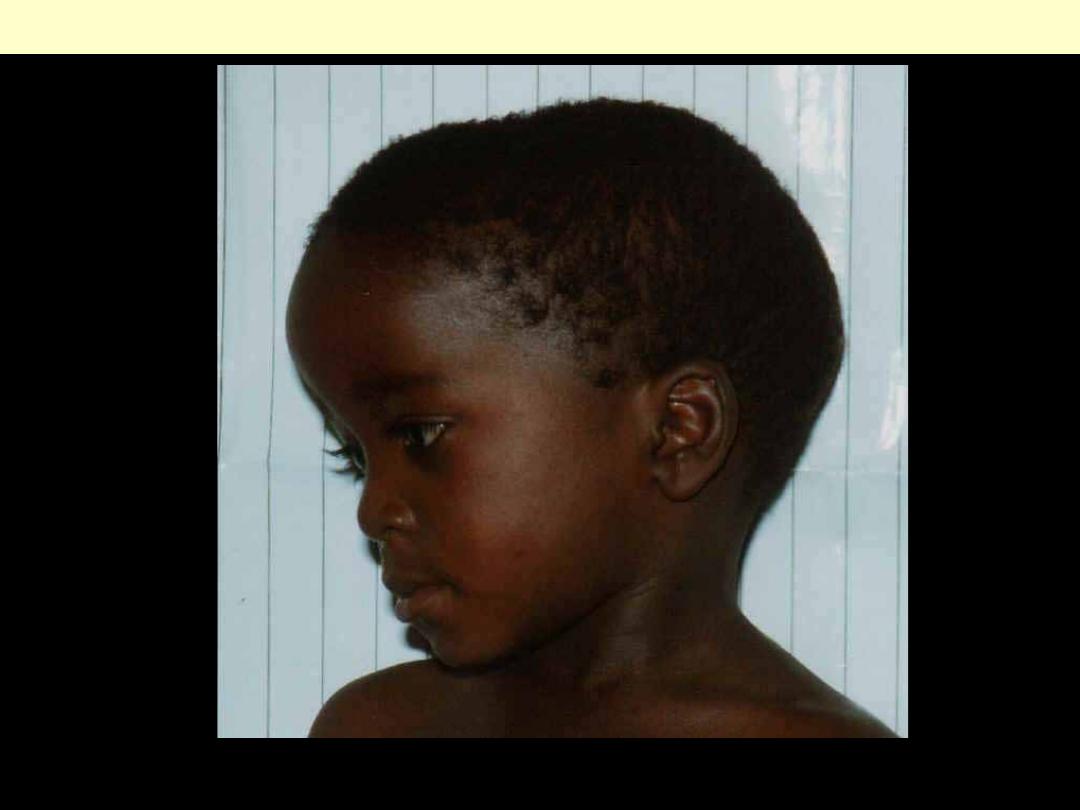
Frontal bossing
Skeletal abnormalities associated with Rickets
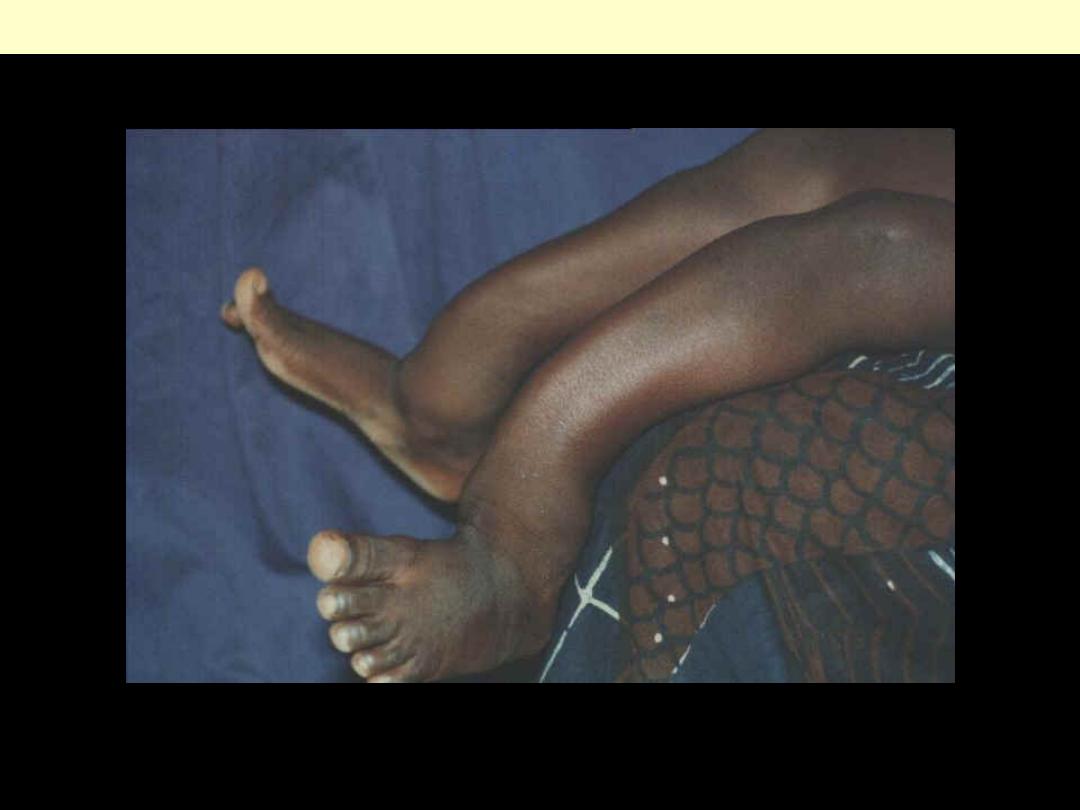
Tibial bowing
Skeletal abnormalities associated with Rickets
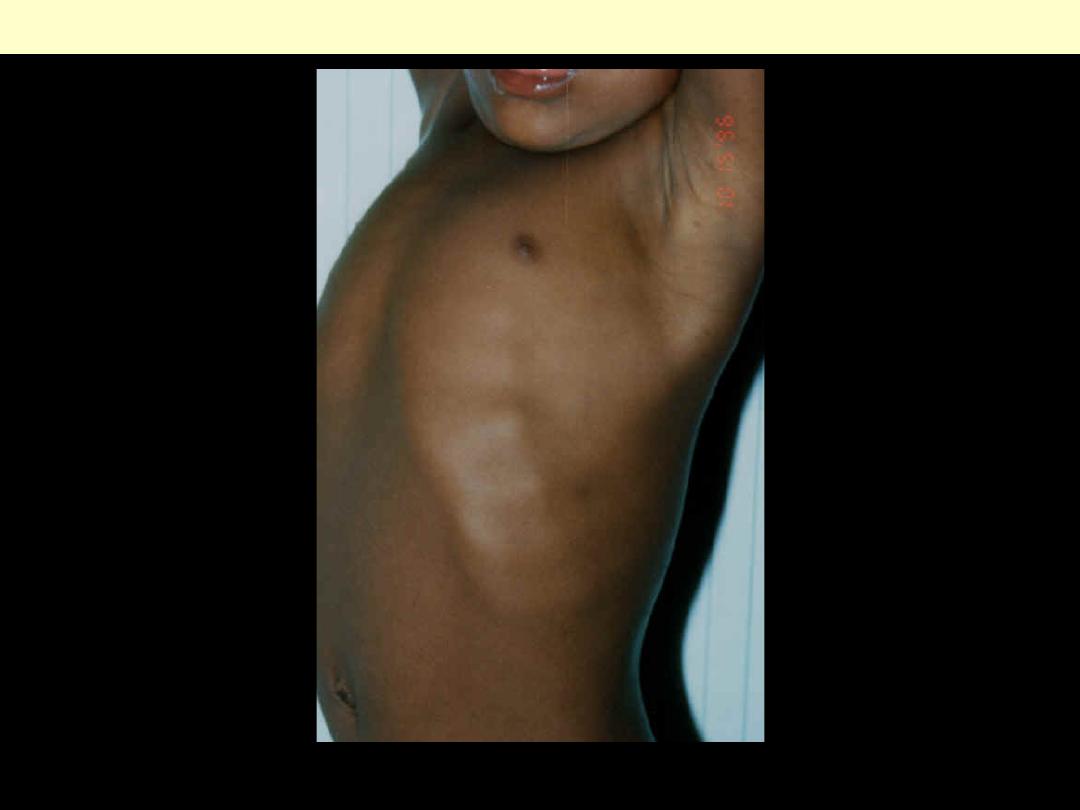
Rib beading (rachitic rosary)
Skeletal abnormalities associated with Rickets
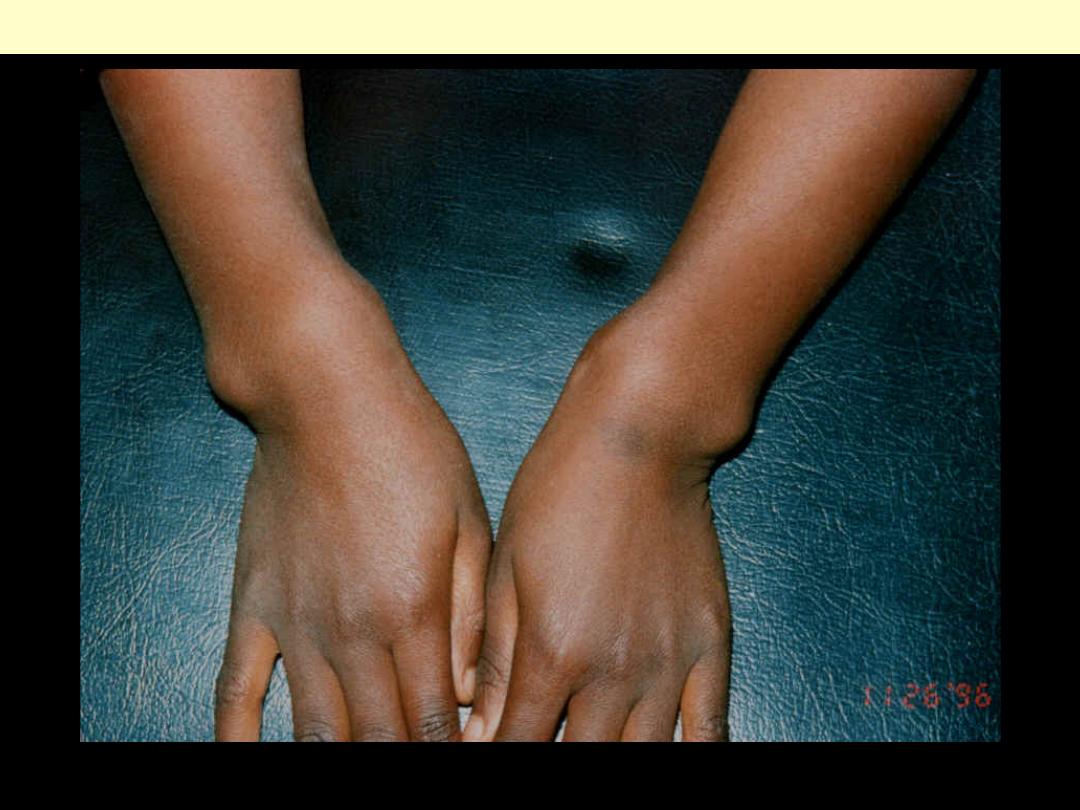
Wrist enlargement
Skeletal abnormalities associated with Rickets
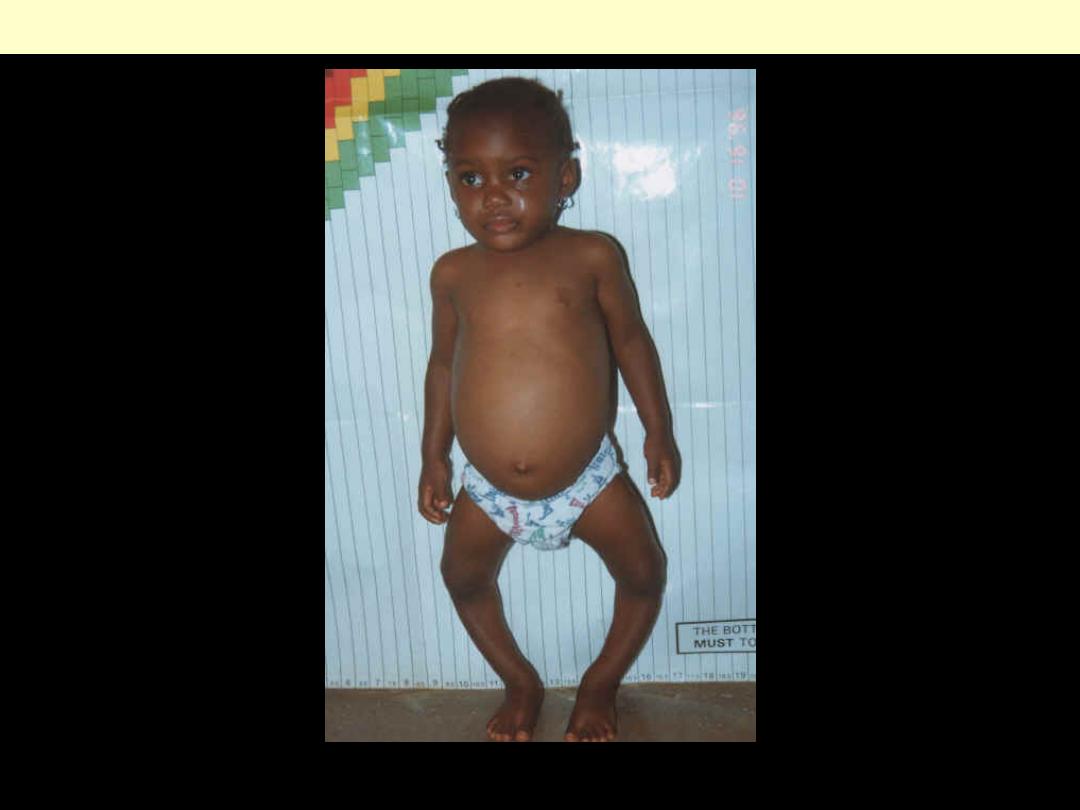
Bowleg deformity (genu varum)
Skeletal abnormalities associated with Rickets
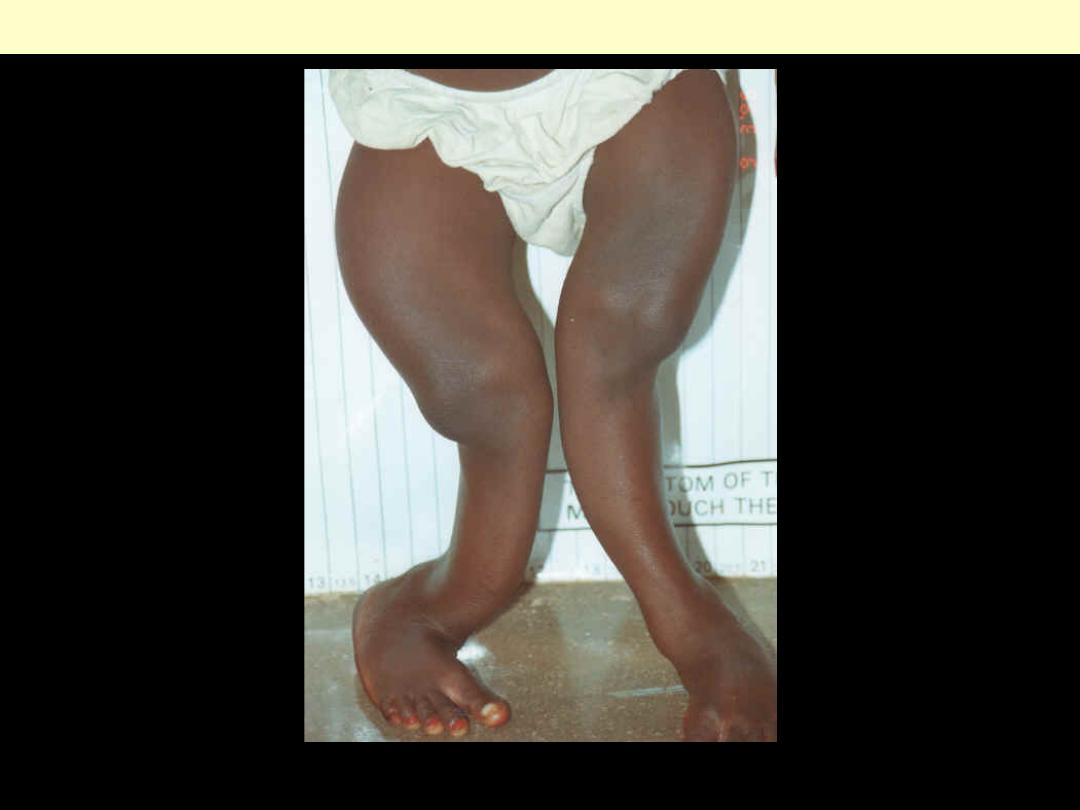
Bowing of long bones in legs
Skeletal abnormalities associated with Rickets
Note wide noncalcified matrix around bone trabeculae
Osteomalcia
Tumors - Bone
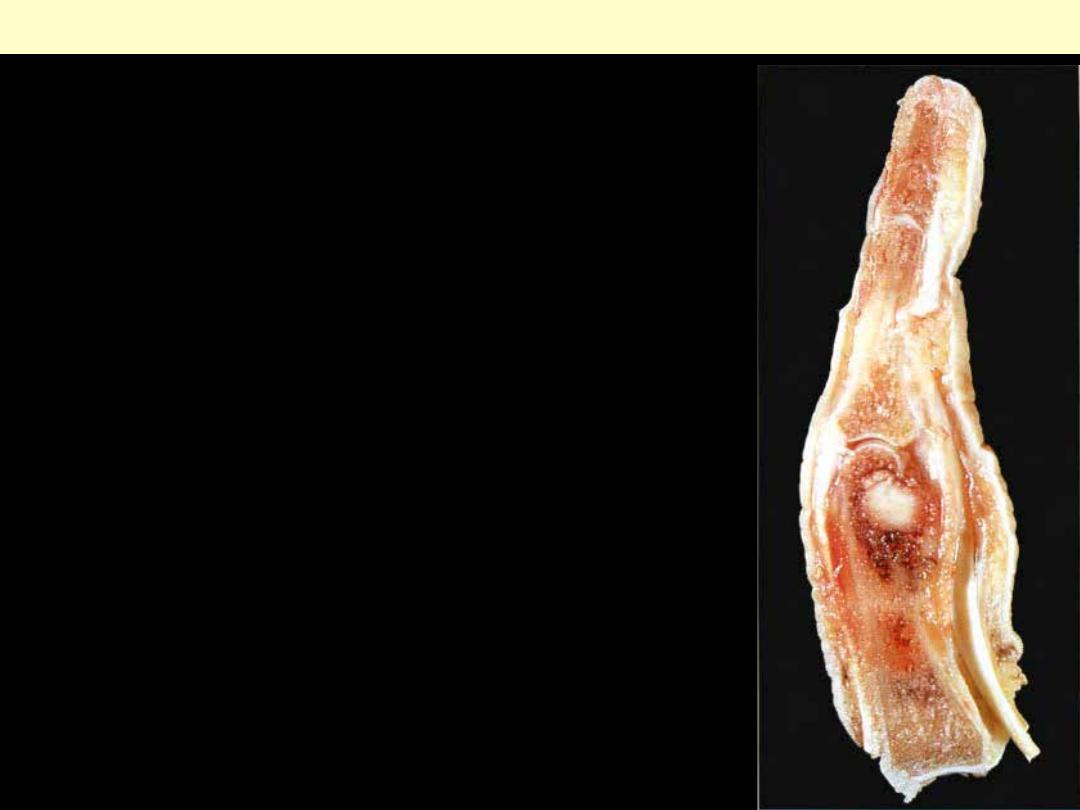
There is a benign, well circumscribed tumor within the
medullary cavity. The treatment of choice is local curettage.
Amputation such as this is overtreatment. The commonest site
for an osteoid osteoma is the upper end of the tibia.
Osteoid osteoma proximal phalanx of a finger
Osteoid osteoma
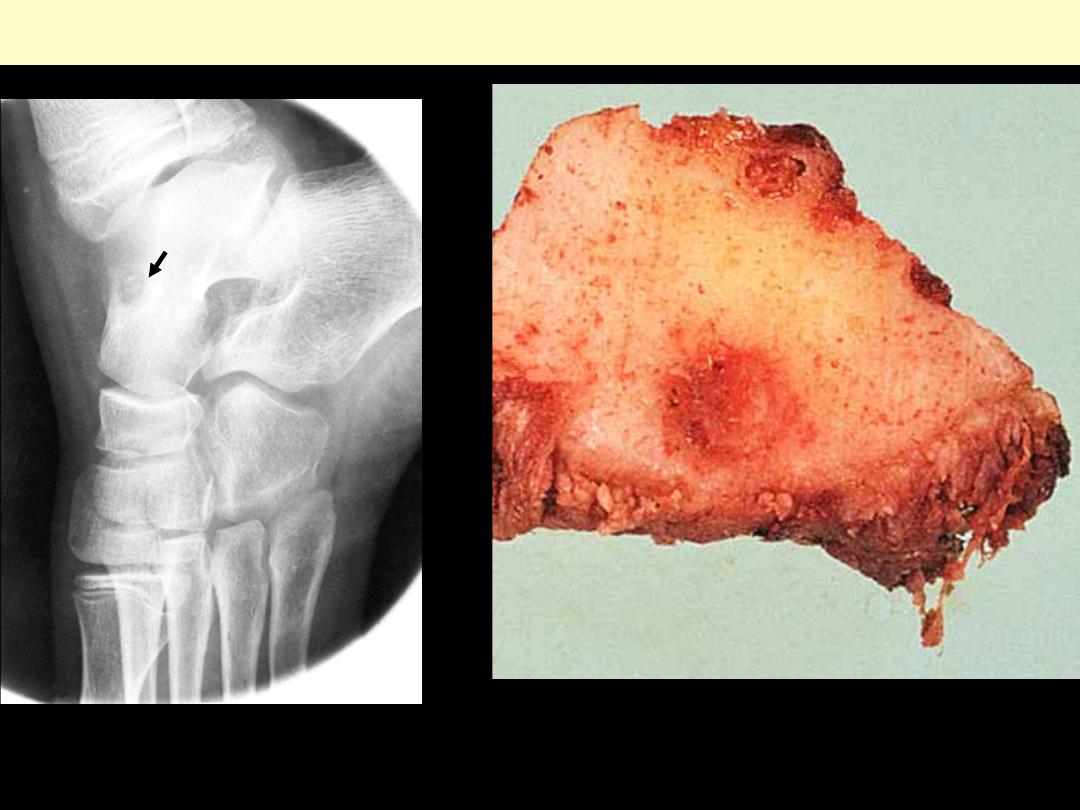
Osteoid osteoma of talus. Note the
small central osteolytic nidus
surrounded by dense bone (arrow)
The small, reddish central nidus is surrounded by a
thick layer of sclerotic bone.
Osteoid osteoma
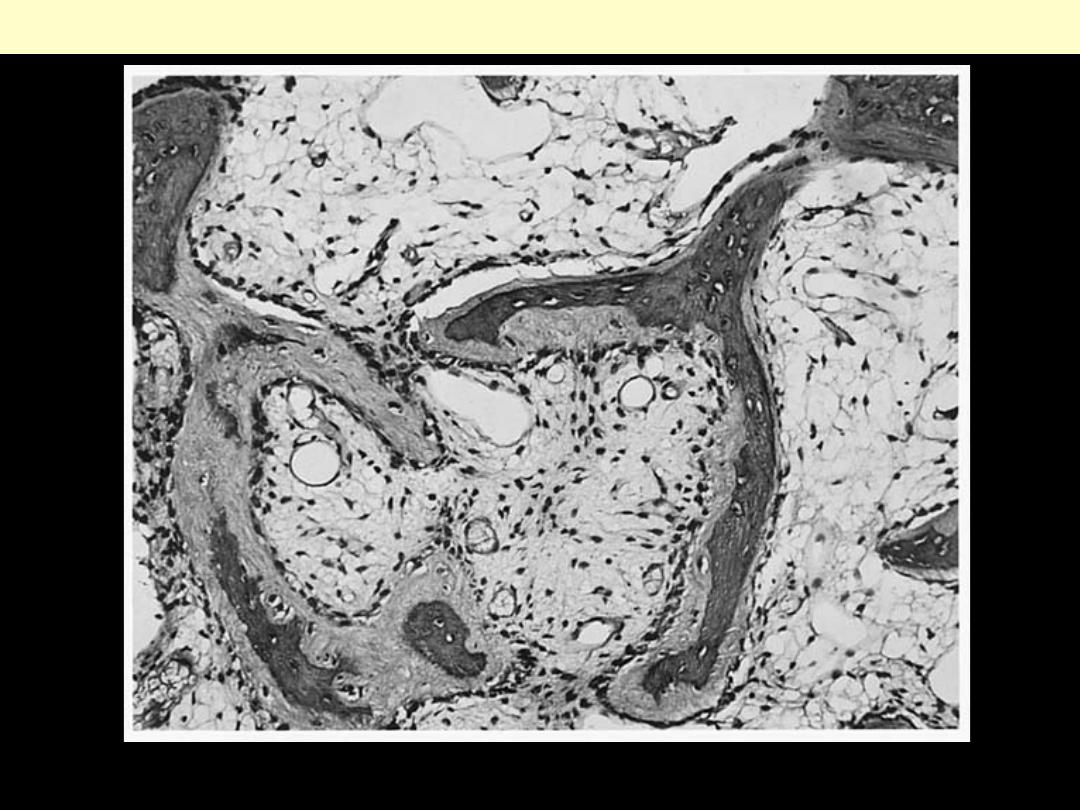
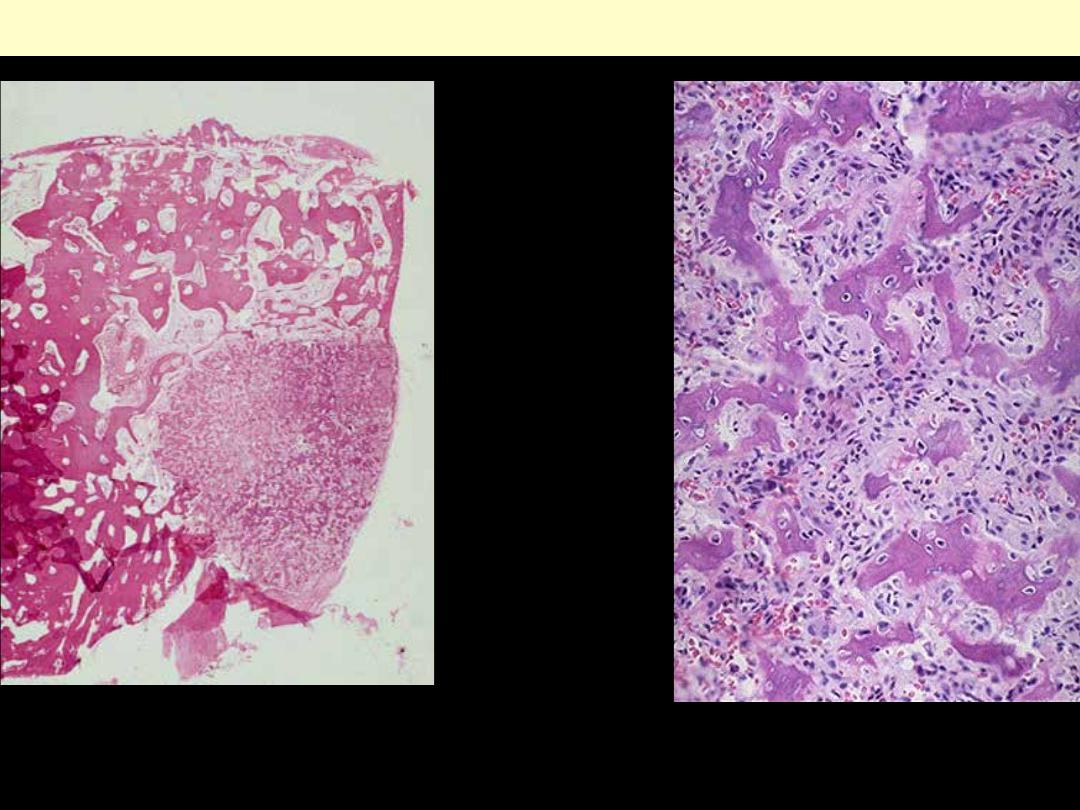
LP microscopic view showing a wedge-
shaped nidus protruding slightly above
the surface and surrounded by sclerotic
bone.
This is the central nidus of an osteoid
osteoma composed of irregular
reactive new bone.
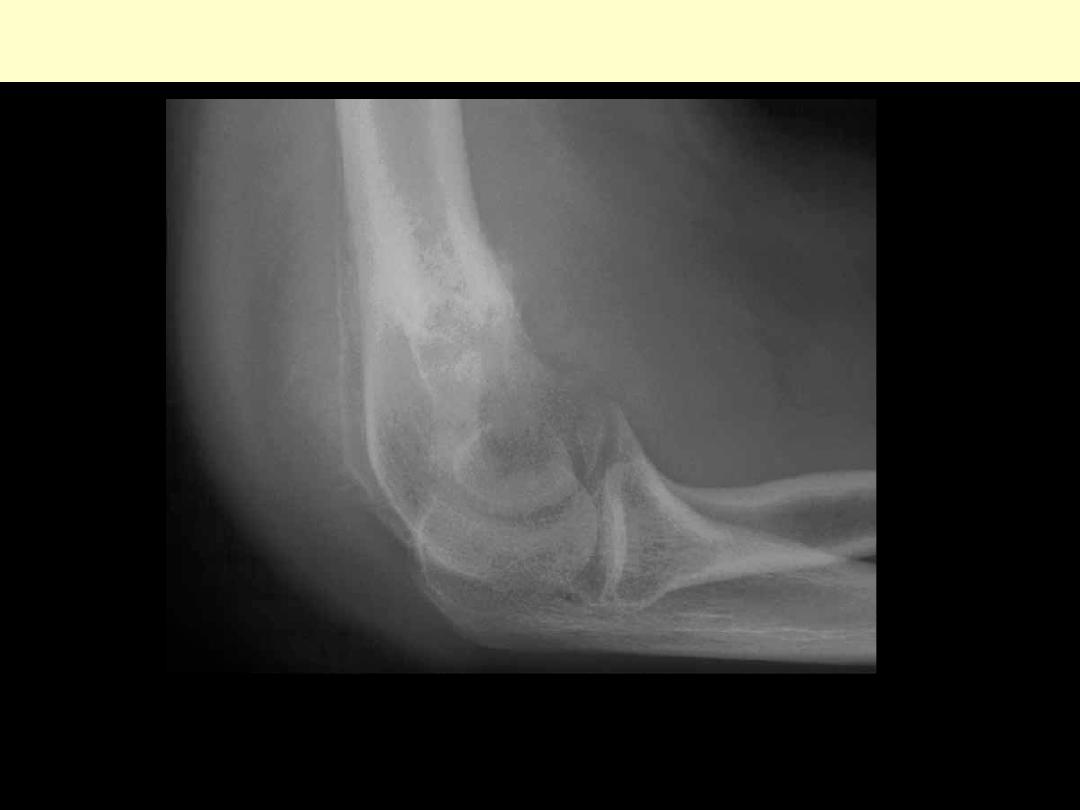
Lateral radiograph of elbow with osteoblastoma of distal humerus. Predominantly lytic expansile
lesion with associated surrounding reactive sclerosis.
Osteoblastoma

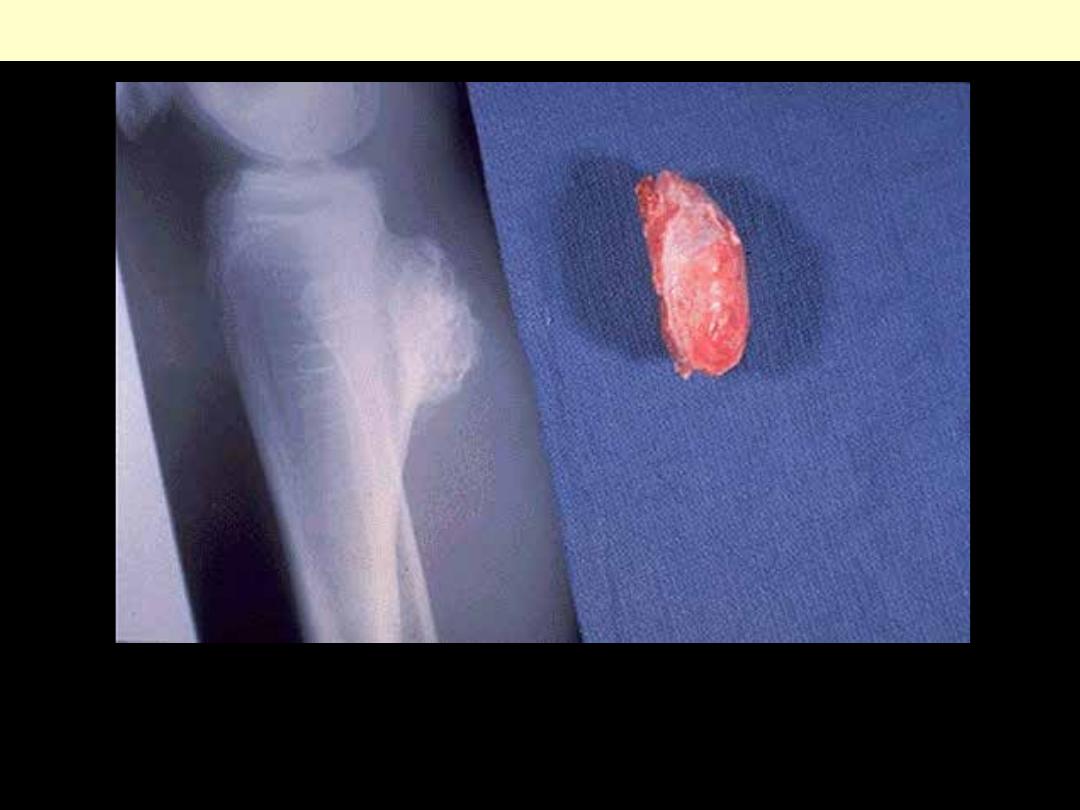
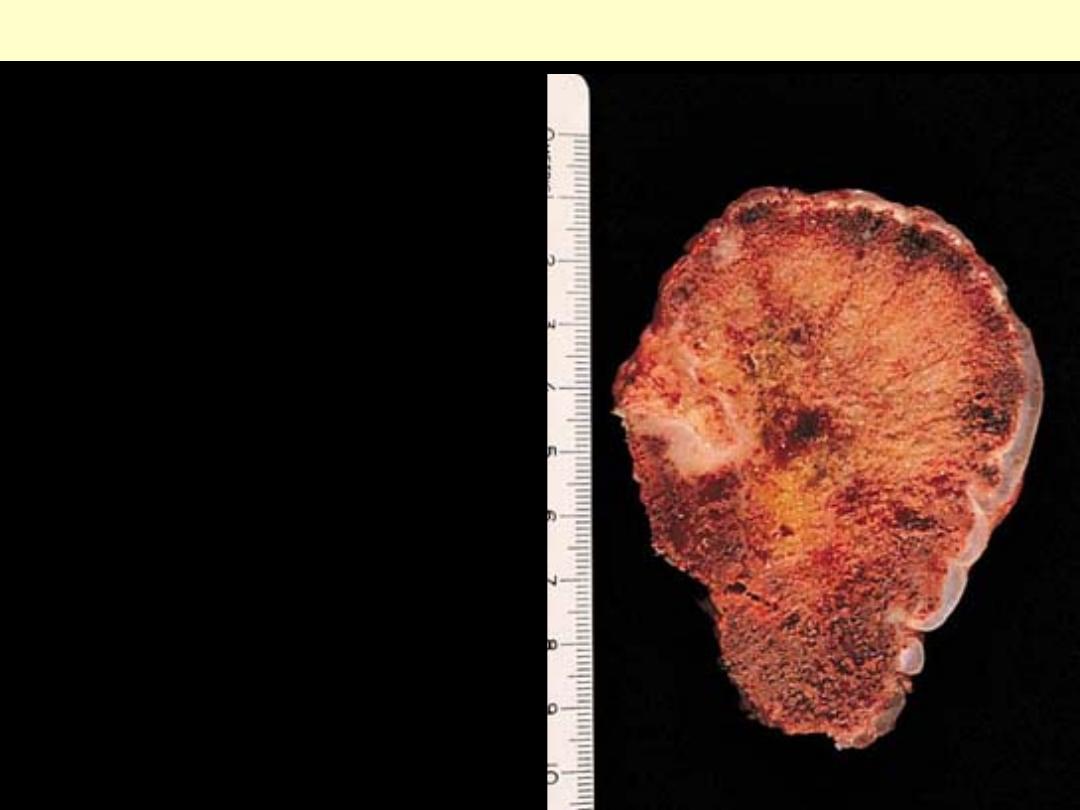
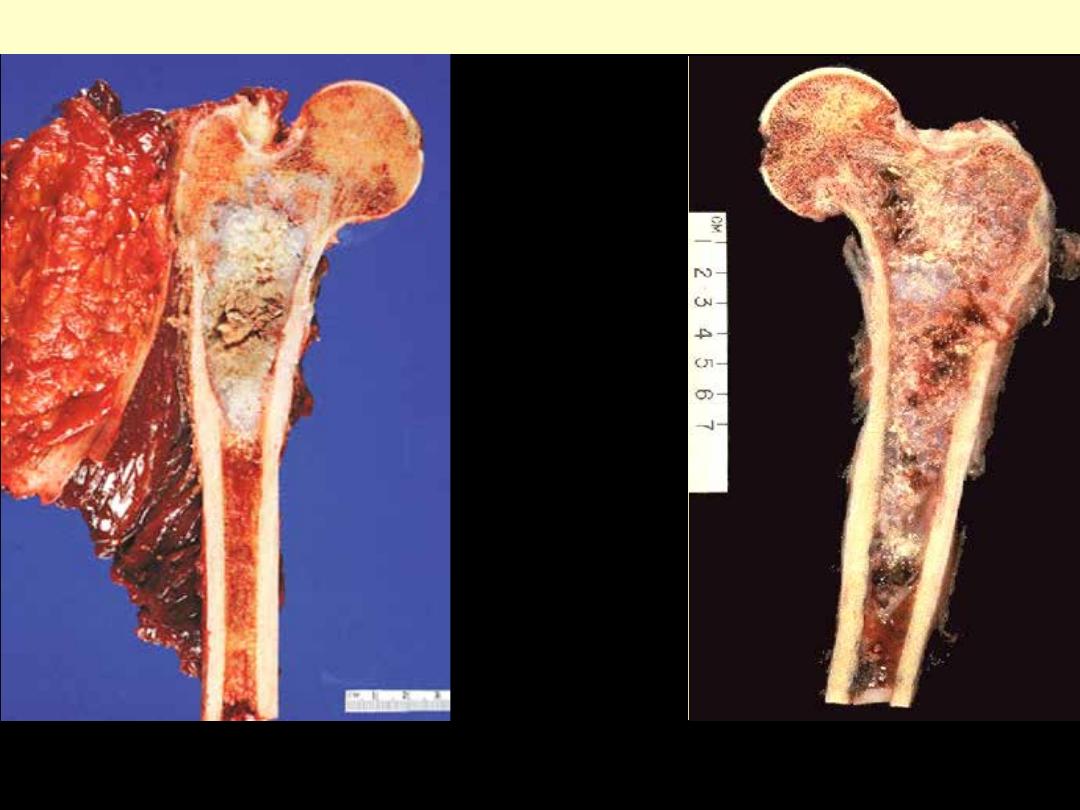
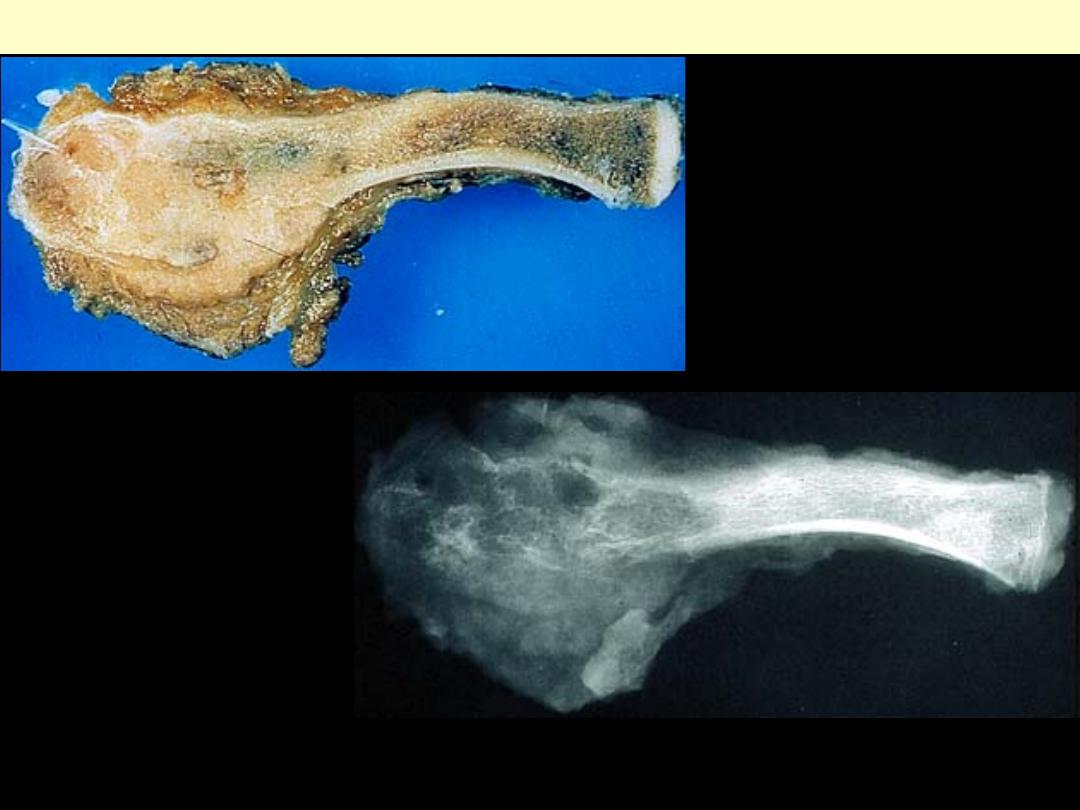
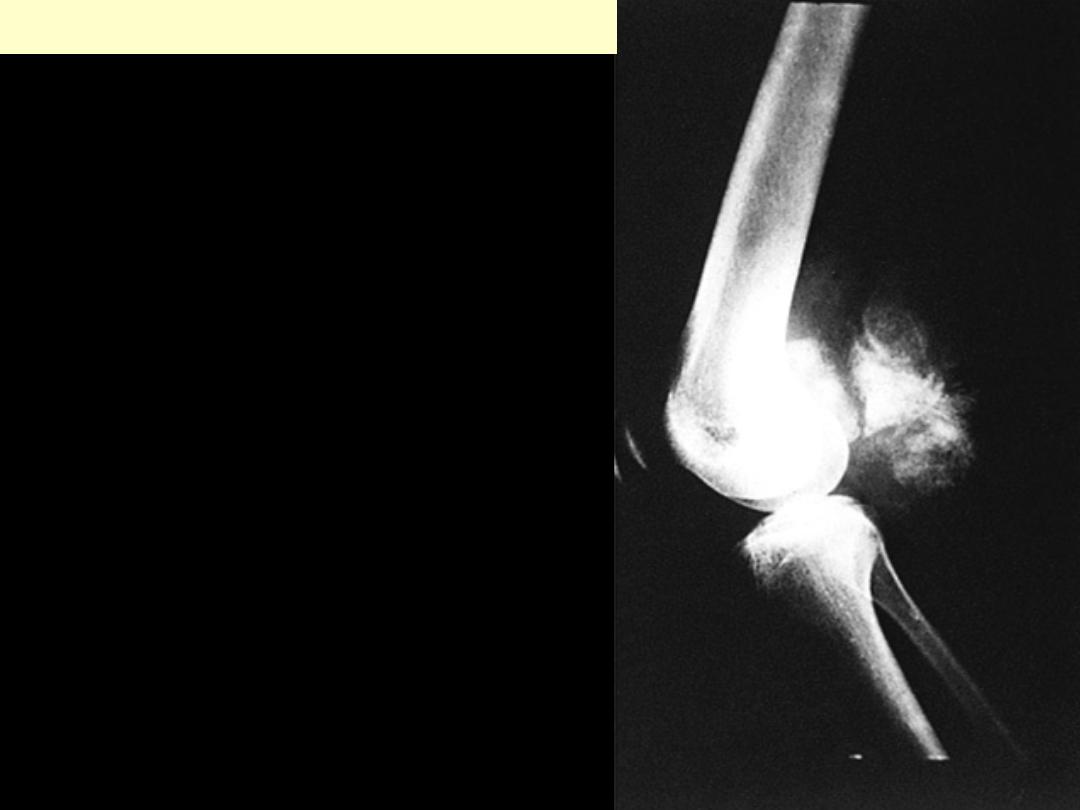
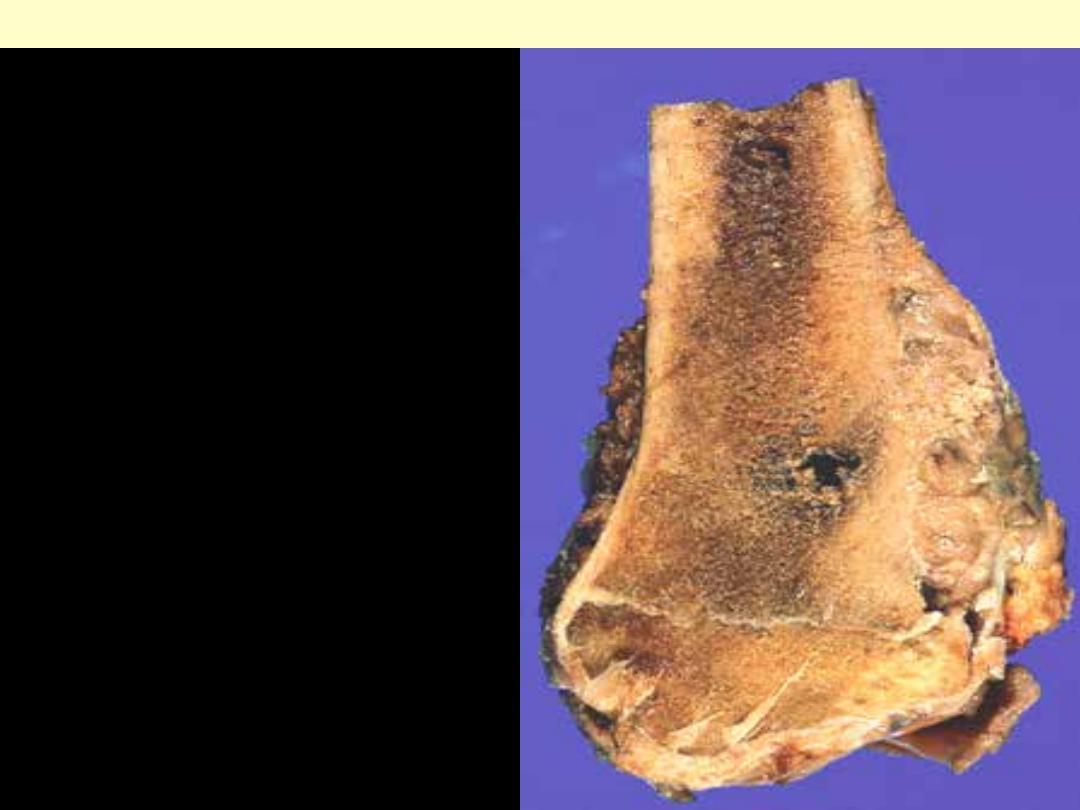
The creamy tumor has involved the lower end of the
femur and has broken through the cortical bone and
caused elevation of the periosteum.
Osteosarcoma

Osteosarcoma femur
The tumor is located at the classic
metaphyseal site and is largely
restricted to bone
The tumor is located at the classic
metaphyseal site and is accompanied by
massive soft tissue extension.
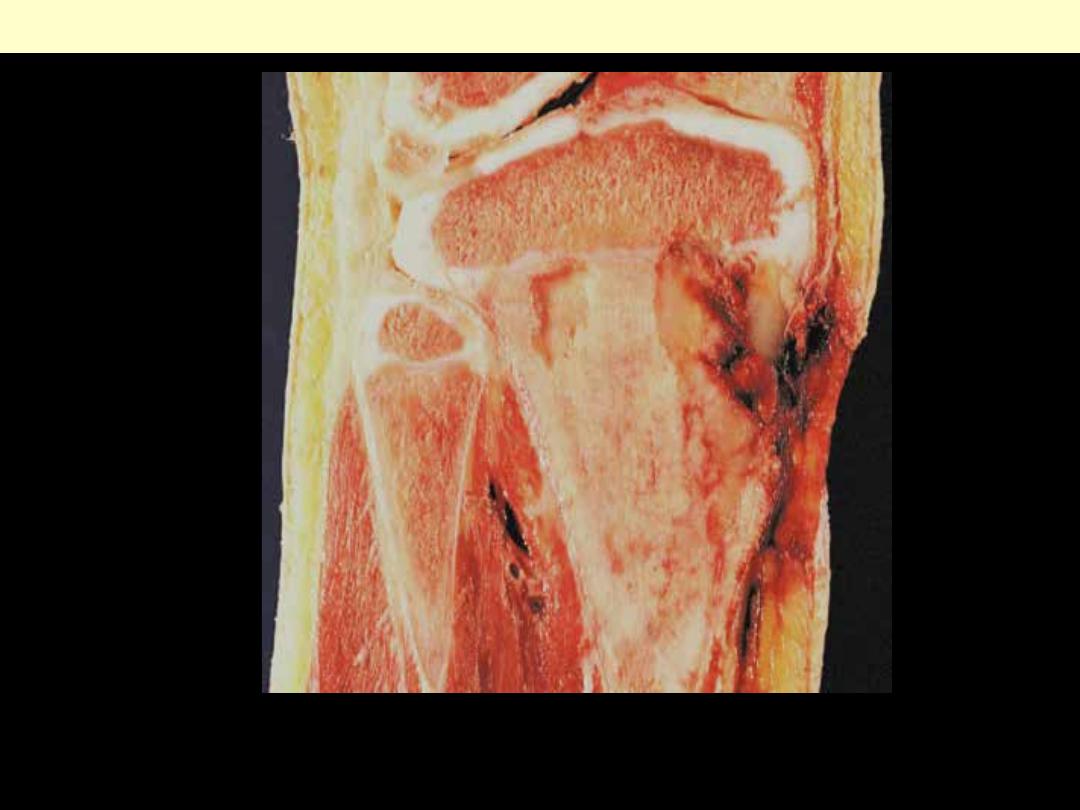
The tumor is being temporarily restrained by the
cartilage of the epiphyseal line. The hemorrhagic
area represents the biopsy site.
Osteosarcoma upper tibial metaphysis
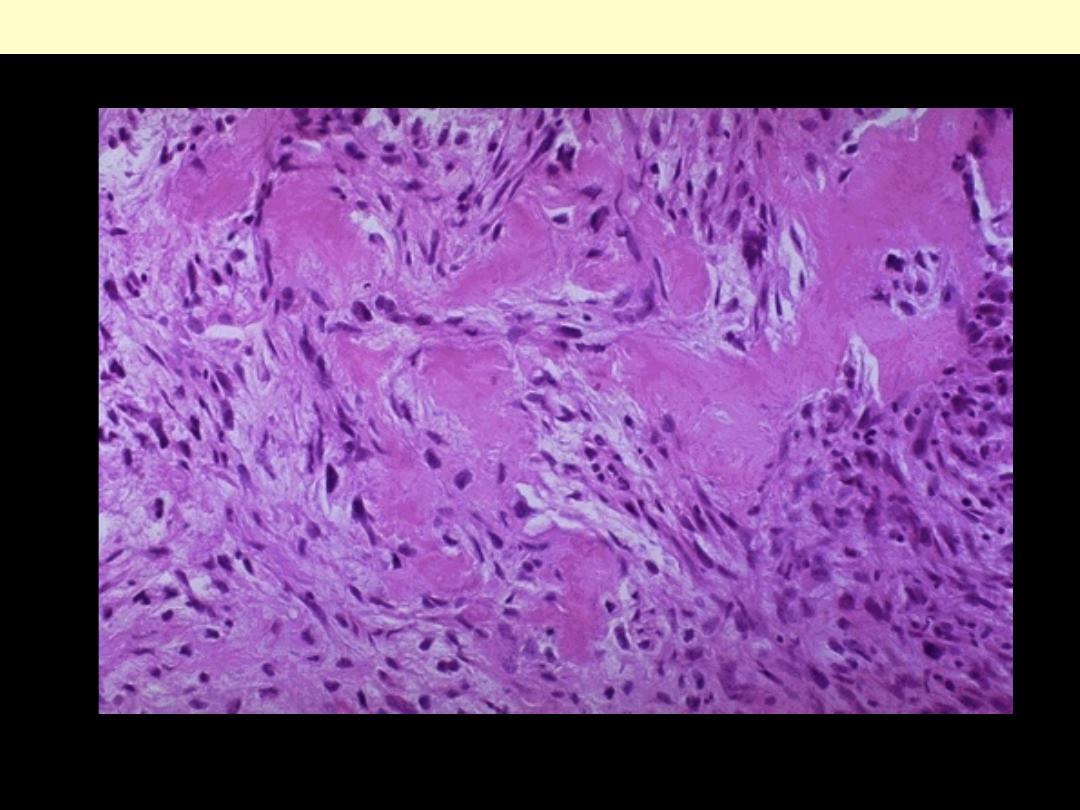
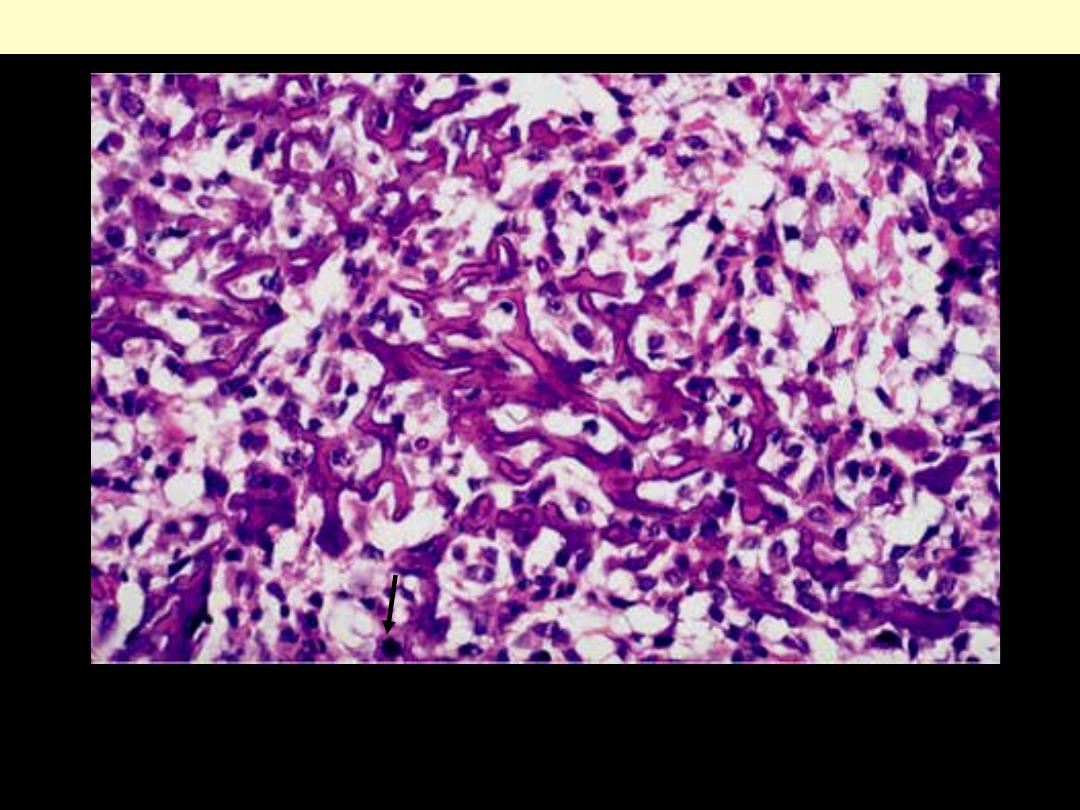
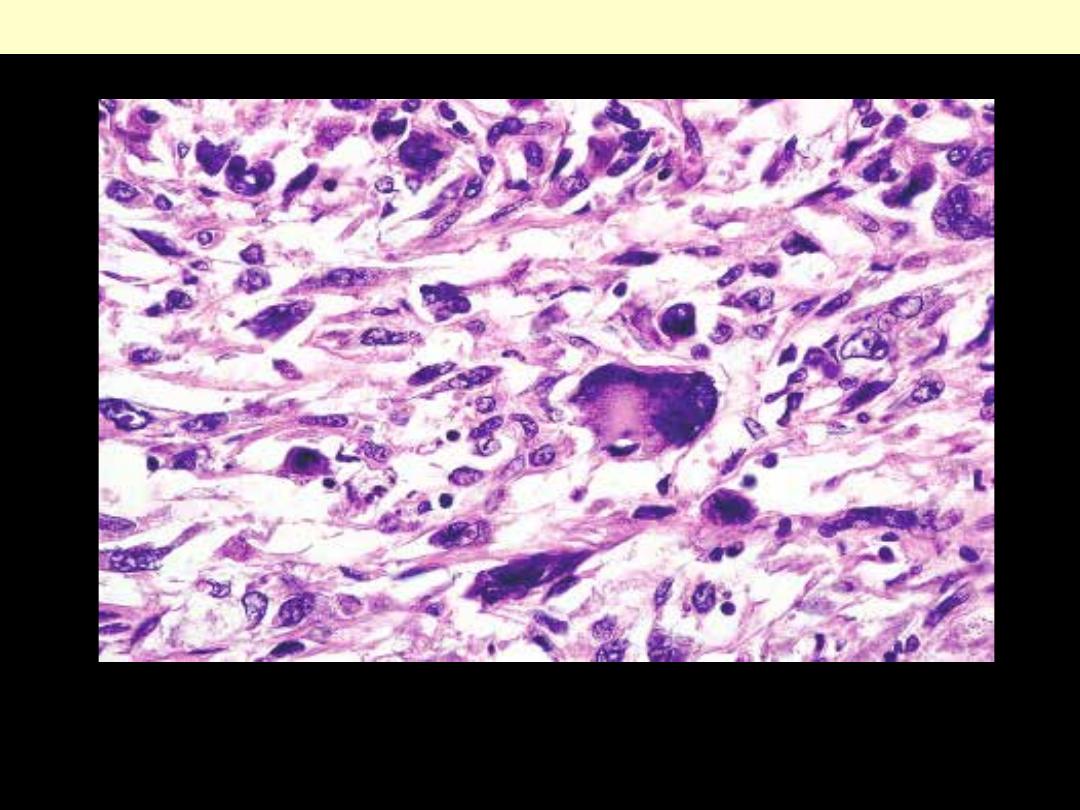
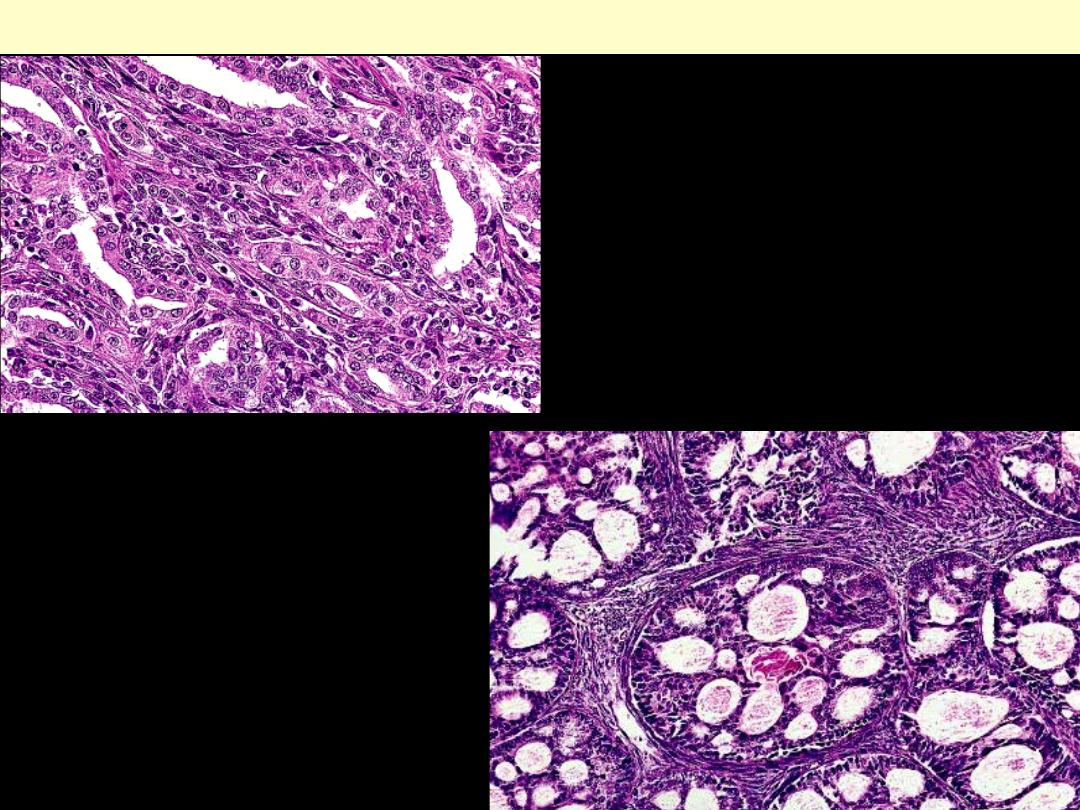
The neoplastic spindle cells of osteosarcoma are seen to be making pink osteoid here. Osteoid
production by a sarcoma is diagnostic of osteosarcoma.
Osteosarcoma
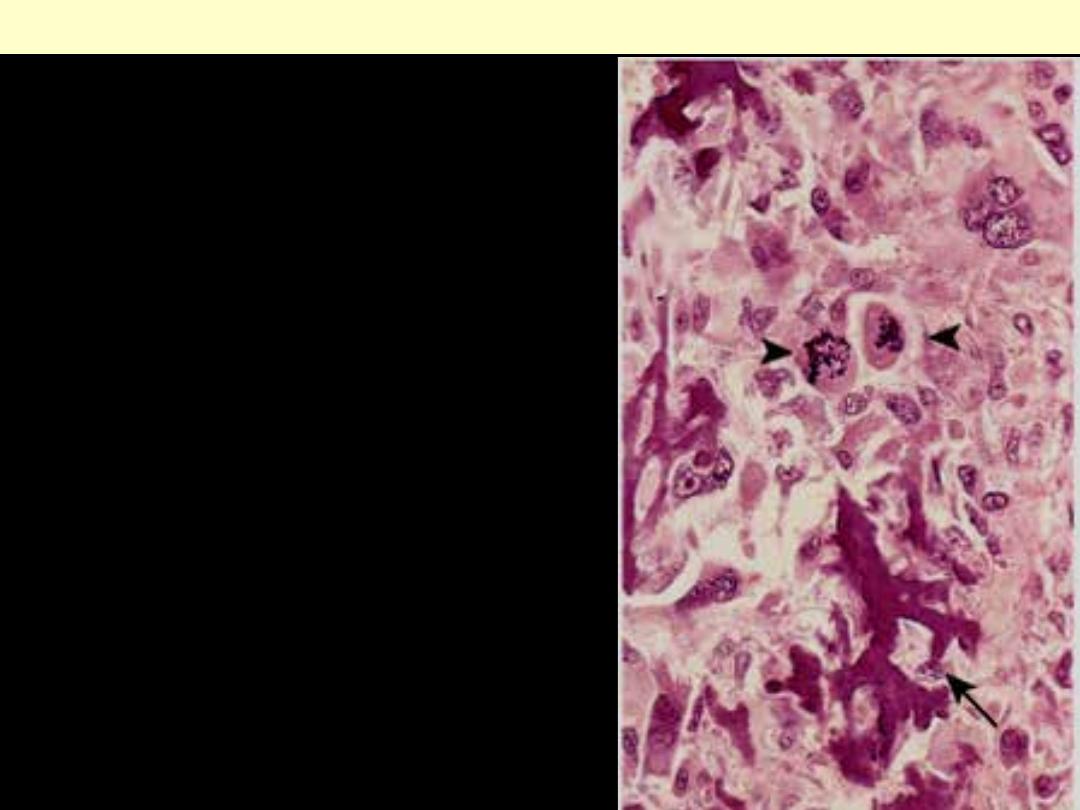
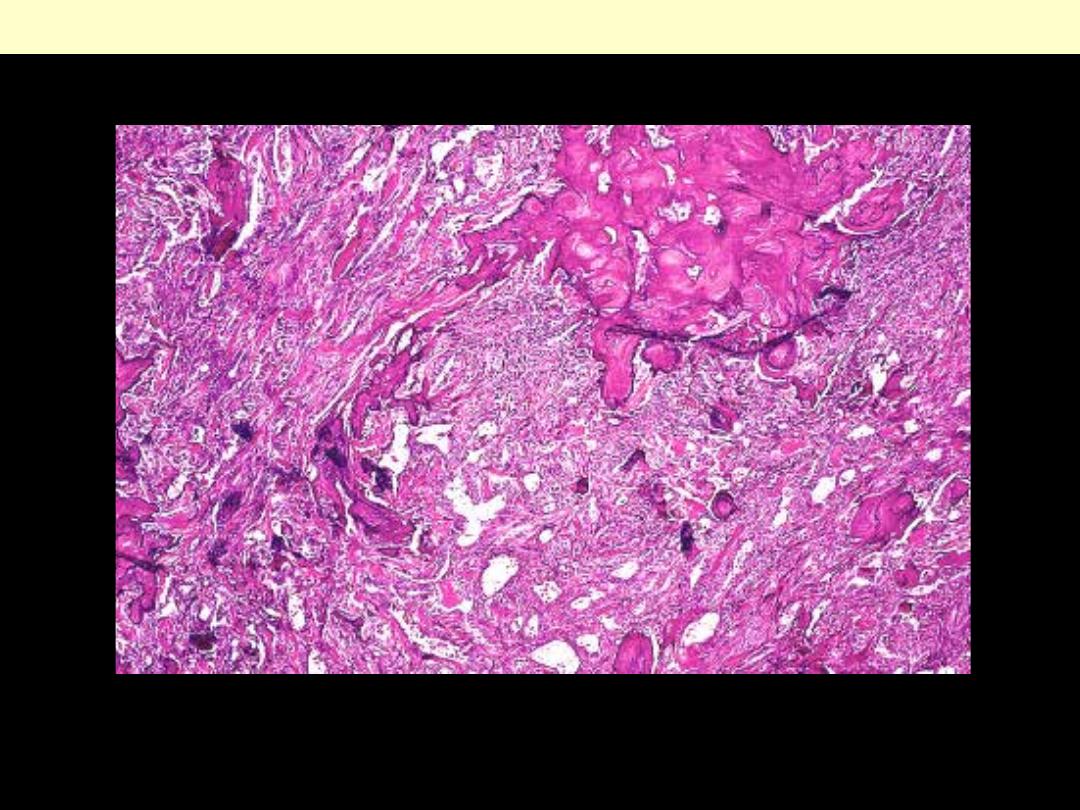
There are characteristic basophilic thin trabeculae of neoplastic bone (lace-like) with an appearance
that is reminiscent of fungal hyphae. Note the malignant background cells with mitotic activity (arrow).
Osteosarcoma
Coarse, lacelike pattern of neoplastic bone (arrow)
produced by anaplastic tumor cells. Note the wildly
aberrant mitotic figures (arrowheads).
osteosarcoma
This is an osteochondroma of bone. This lesion appears as a bony projection (exostosis).
Most are solitary, incidental lesions that may be excised if they cause local pain. There is a
rare condition of multiple osteochondromatosis marked by bone deformity and by a greater
propensity for development of chondrosarcoma.
Osteochondroma bone
Large osteochondroma of femur with a
bilobed appearance.
Osteochondroma bone
Cut surface of osteochondroma of rib. Note
the thick cartilaginous cup
Gross and whole-mount appearance
of osteochondroma. Mature bone is covered
by a well-differentiated cartilaginous cap .
Osteochondroma bone

whole-mount appearance of osteochondroma.
Mature bone is covered by a well-
differentiated cartilaginous cap
Osteochondroma bone
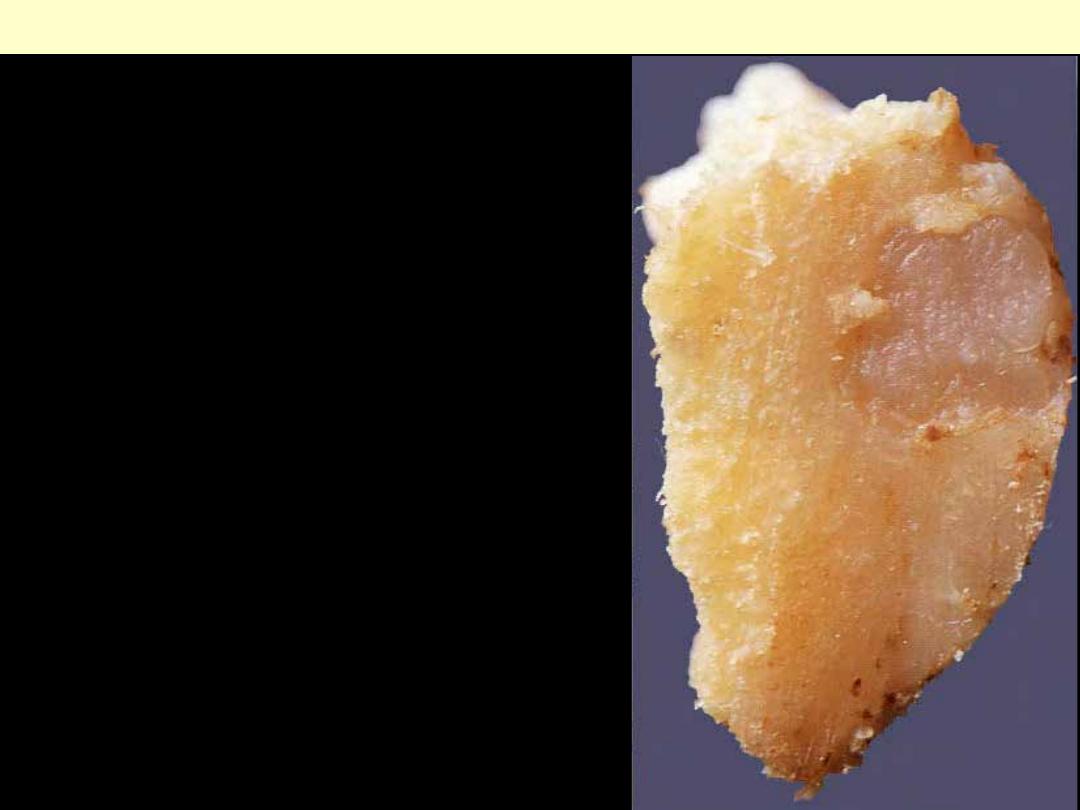
This small cartilage tumour was resected from the tibia.
Note the gray-blue, translucent appearance.
Chondroma
Chondroma: Olleir’s disease
Gross appearance of head of humerus affected by
multiple chondromas in a patient with Ollier's
disease.

The tumor produces a semispherical expansion
of the involved bone.
Juxtacortical chondroma
Enchondroma of phalanx. The tumor has a
typical lobulated appearance.
Chondroma
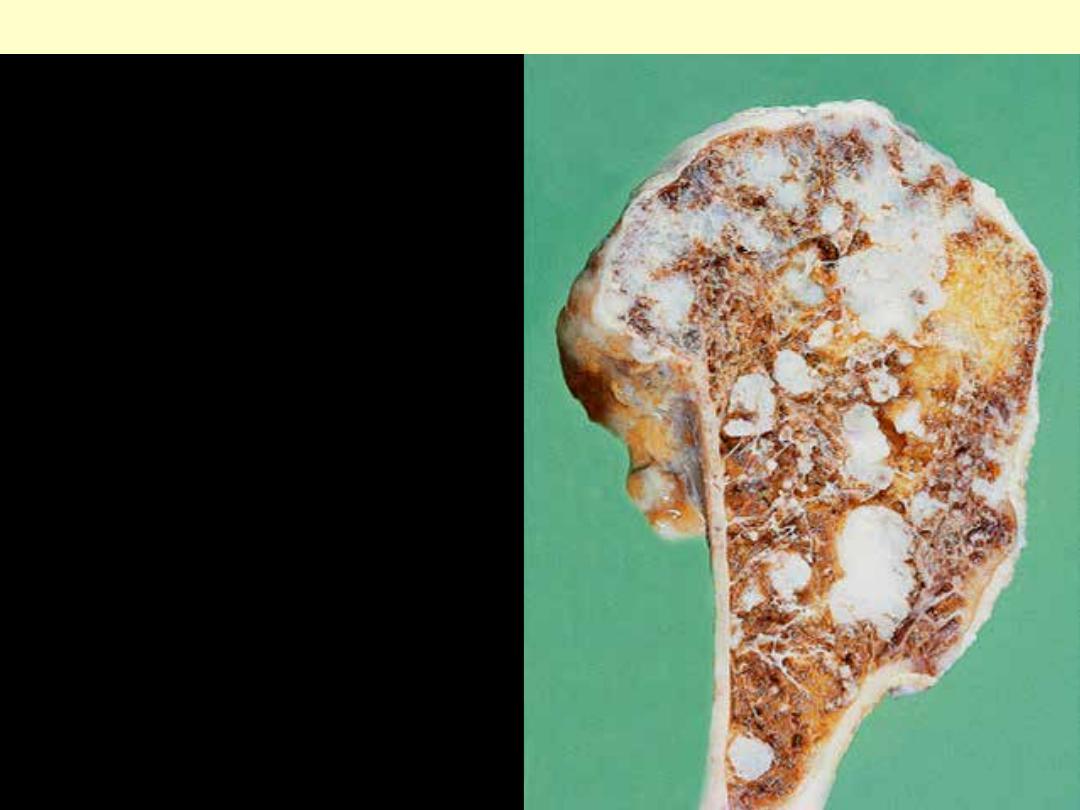
Typical chondrosarcoma of femur
showing splotchy calcification and
extensive cortical destruction.
Chondrosarcoma
Gross appearances of central chondrosarcoma: A to D, all of these tumors were located in the femur,
the single most common site of occurrence. Islands of cartilage (gray-blue glistening masses) expand
the medullary cavity and grow through the cortex to form a sessile paracortical mass in D (see next). In
Central chondrosarcoma
A
B
Central chondrosarcoma femur
C
D
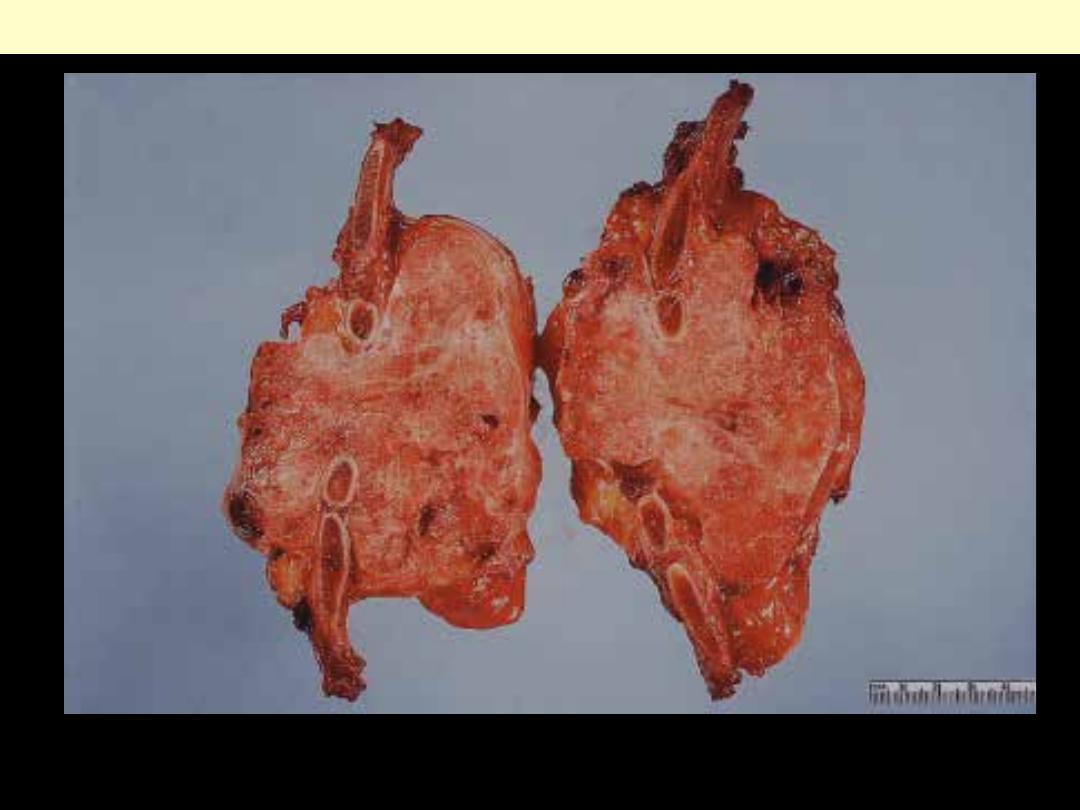
Gross appearances of central chondrosarcoma: of rib, resulting in massive expansion of the bone.
Central chondrosarcoma rib

Large expansile chondrosarcoma of sternum.
Chondrosarcoma sternum
Anaplastic chondrocytes within a chondroid matrix.
Chondrosarcoma

Metaphyseal fibrous defect/nonossifying fibroma
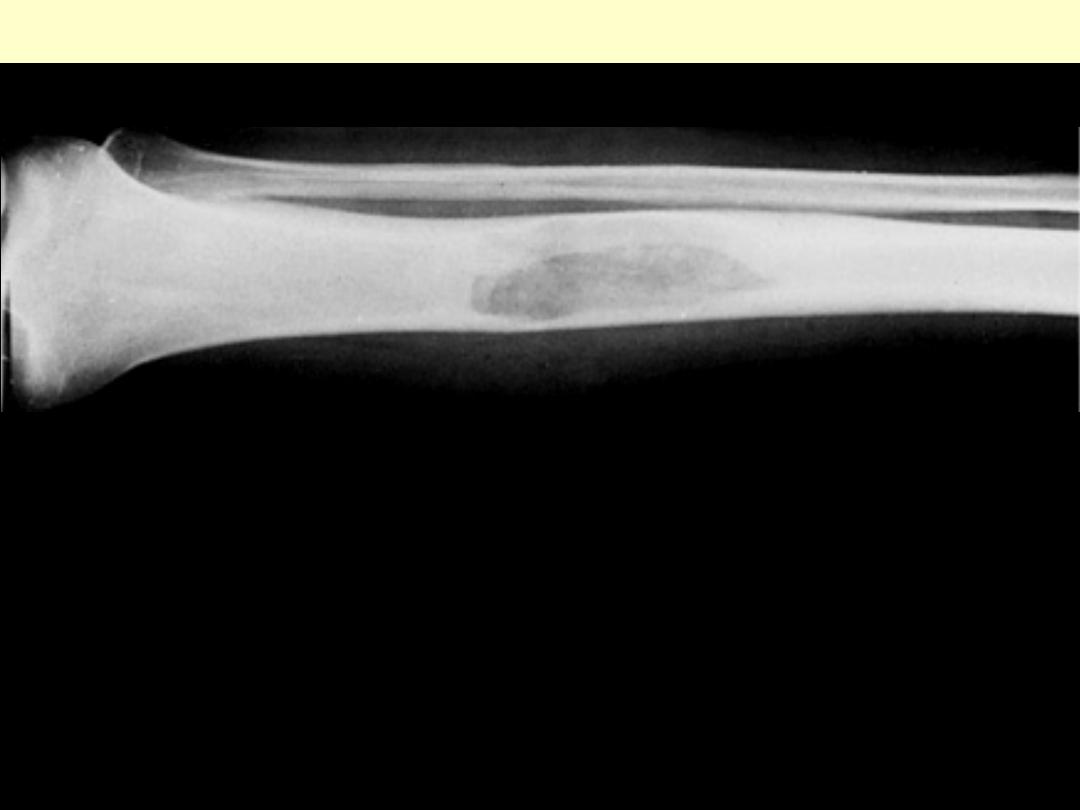
Metaphyseal fibrous defect of lower end of tibia. Note its sharp
delineation and sclerotic margins.

Large non-ossifying fibroma expanding lower tibial
metaphysis.
Characteristic storiform pattern of spindle cells interspersed with scattered osteoclast-type giant cells.
Fibrous cortical defect or nonossifying fibroma.
Metaphyseal fibrous defect. The predominant element
is a spindle cell of fibroblastic appearance. There are
also irregularly scattered osteoclasts.
Metaphyseal fibrous defect/nonossifying fibroma
Microscopic appearances of
metaphyseal fibrous defect
involving the upper metaphysis
of the tibia.
Fibrous dysplasia
Lesion of tibia forming a sharply delimited lesion.

Lesion of the rib. It forms a fusiform, expanded mass that is grayish white.
Fibrous dysplasia
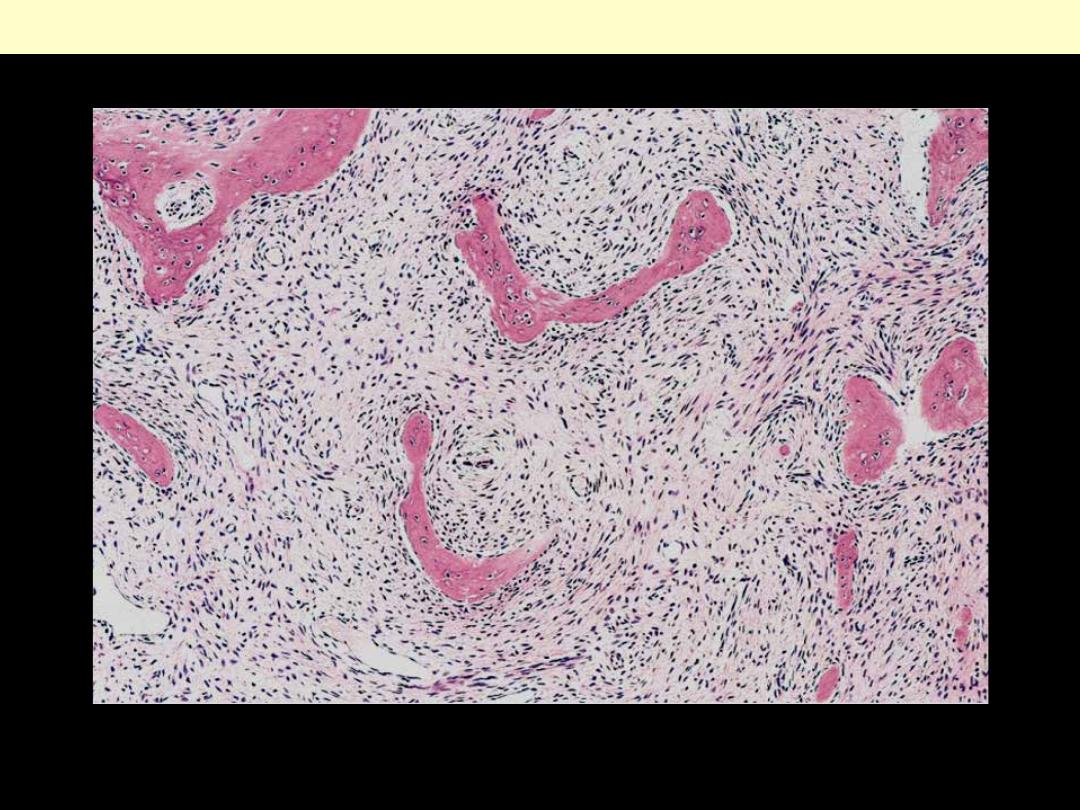
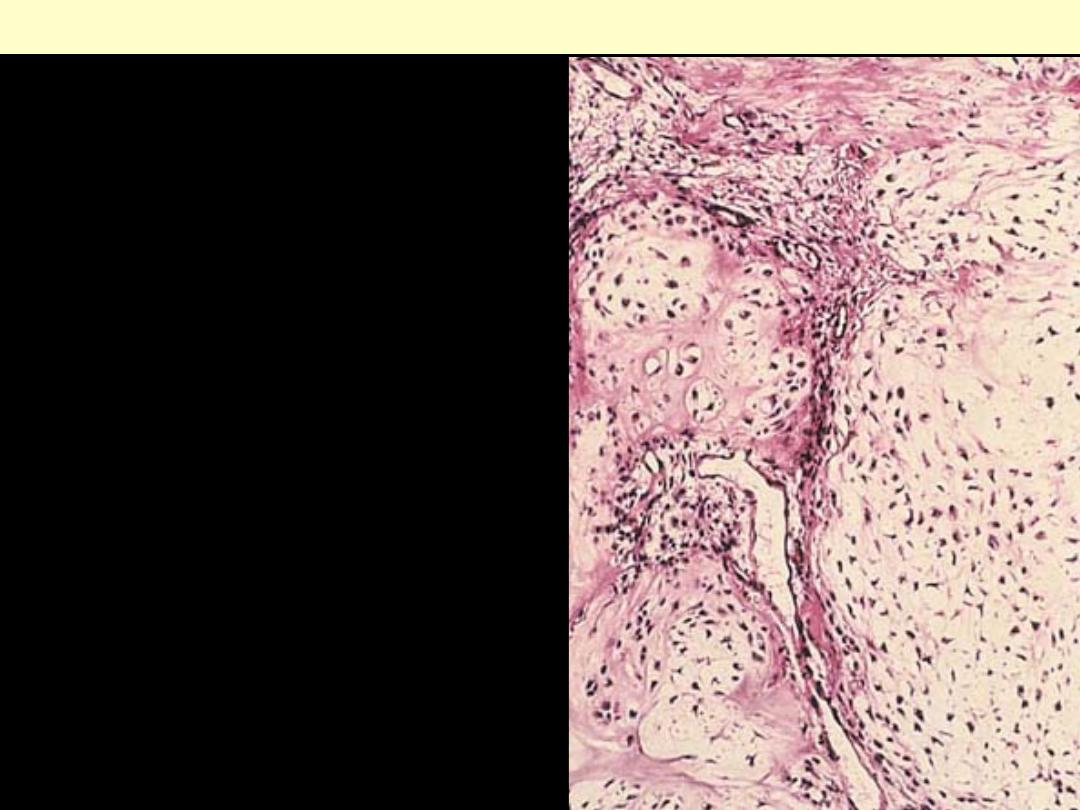
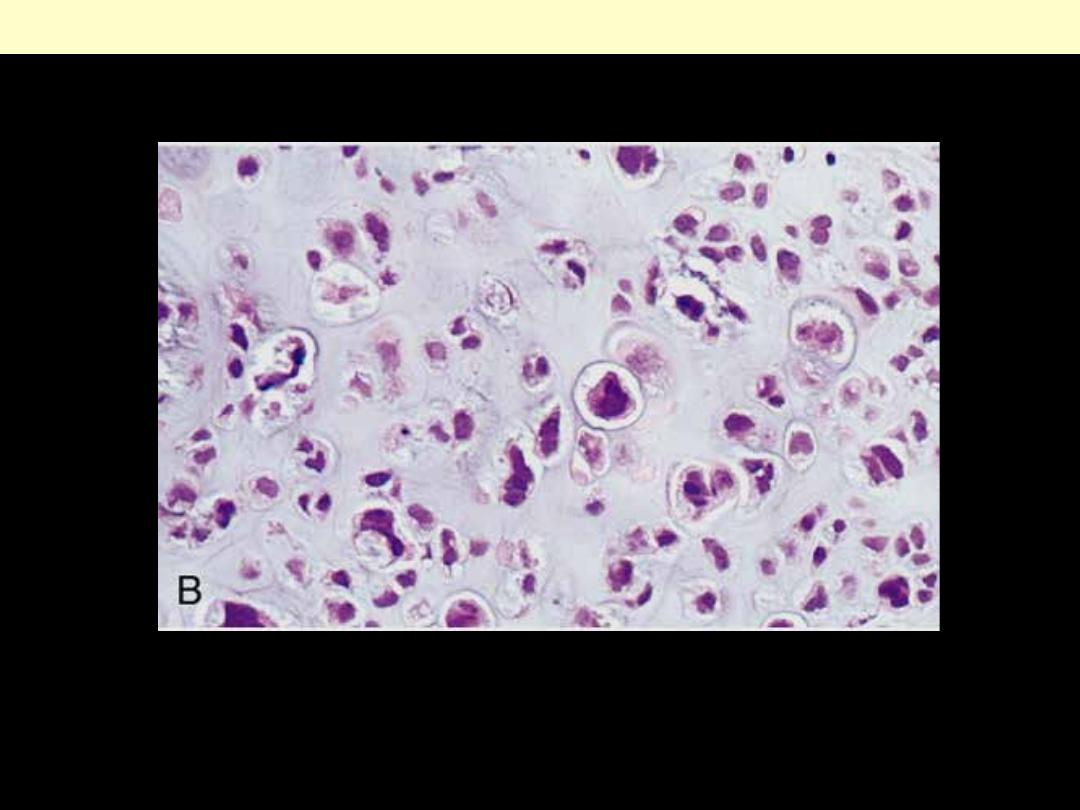
Curved trabeculae of woven bone arising in a fibrous tissue. Note the absence of osteoblasts rimming
the bones.
Fibrous dysplasia
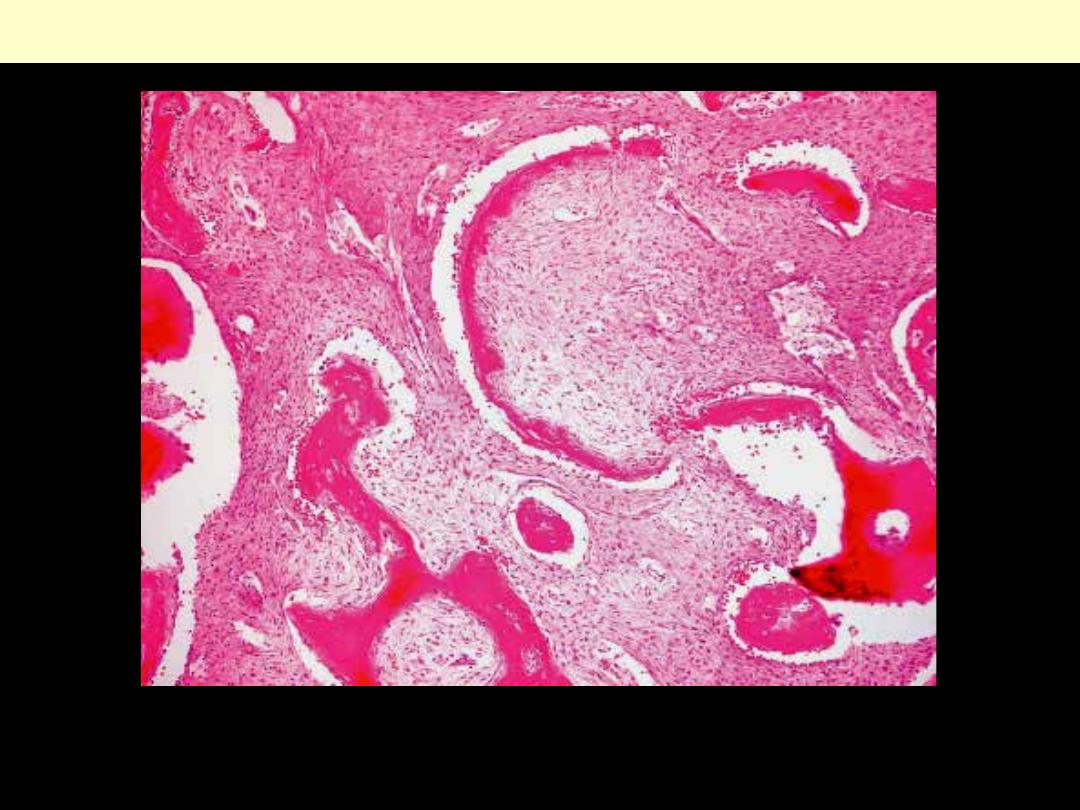
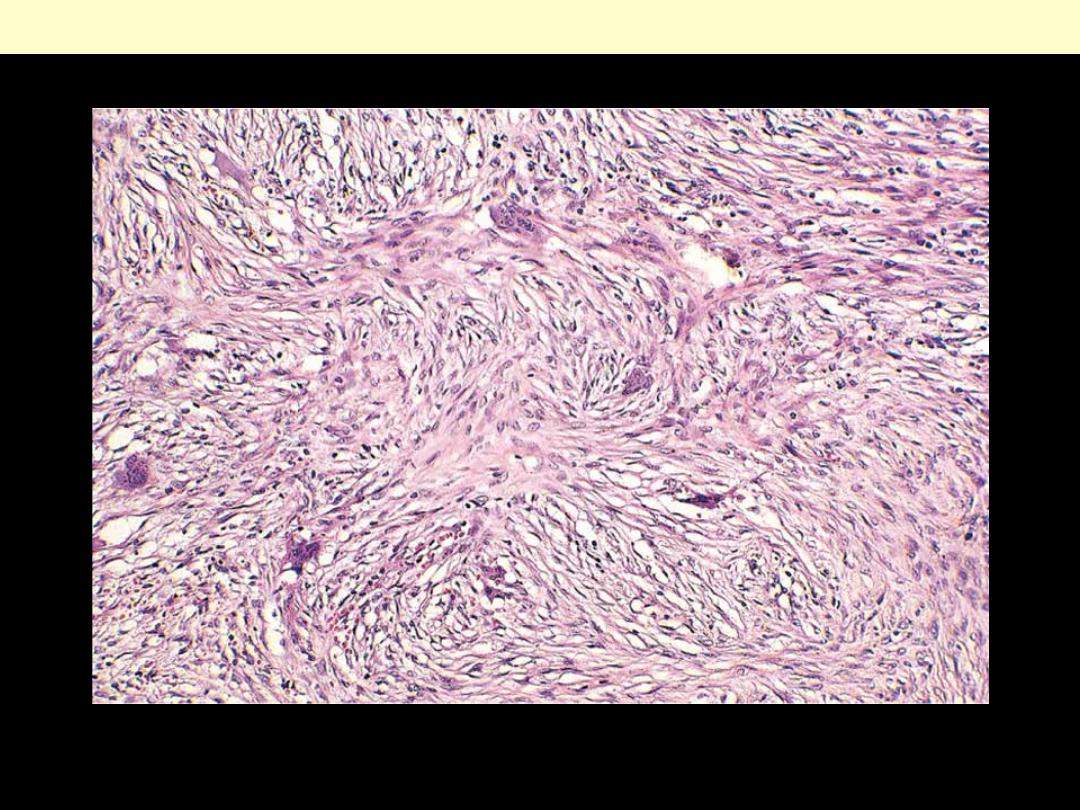
Typical low-power appearance of fibrous dysplasia.
Fibrous dysplasia
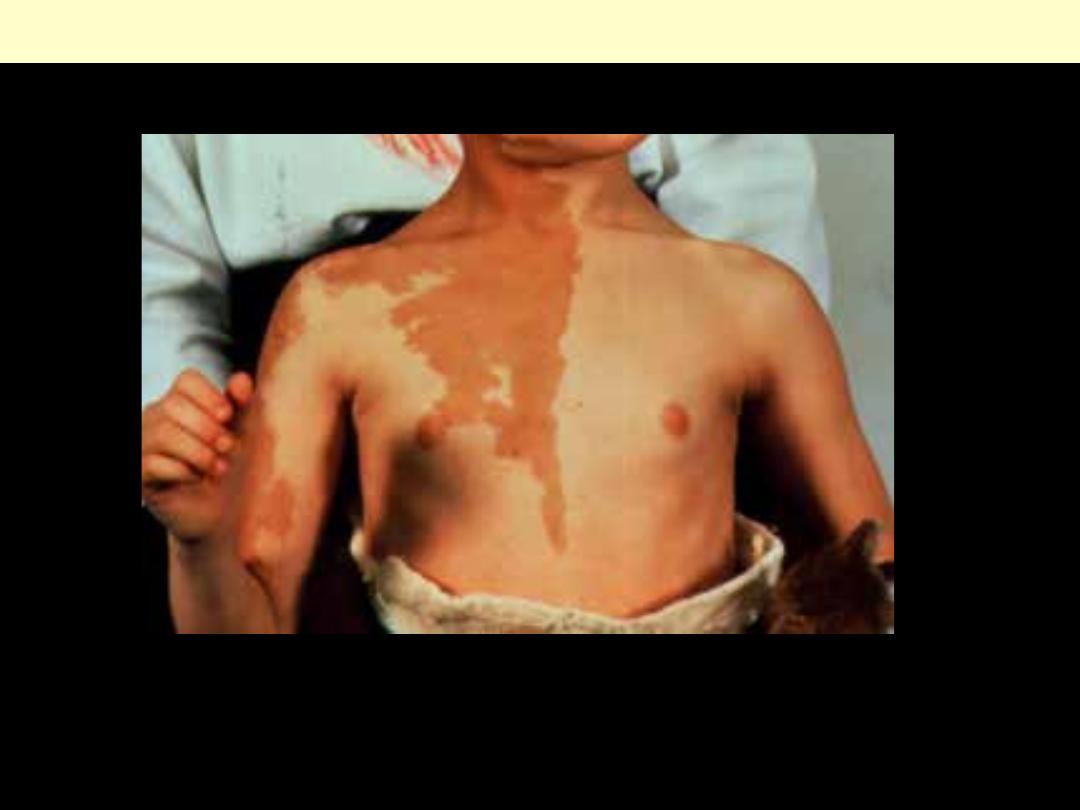
4-year-old girl with large, dark lesions with serpiginous borders in chest, neck, back (cafe-au-lait skin
pigmentation). Cast due to fractures
Fibrous dysplasia: Albright syndrome

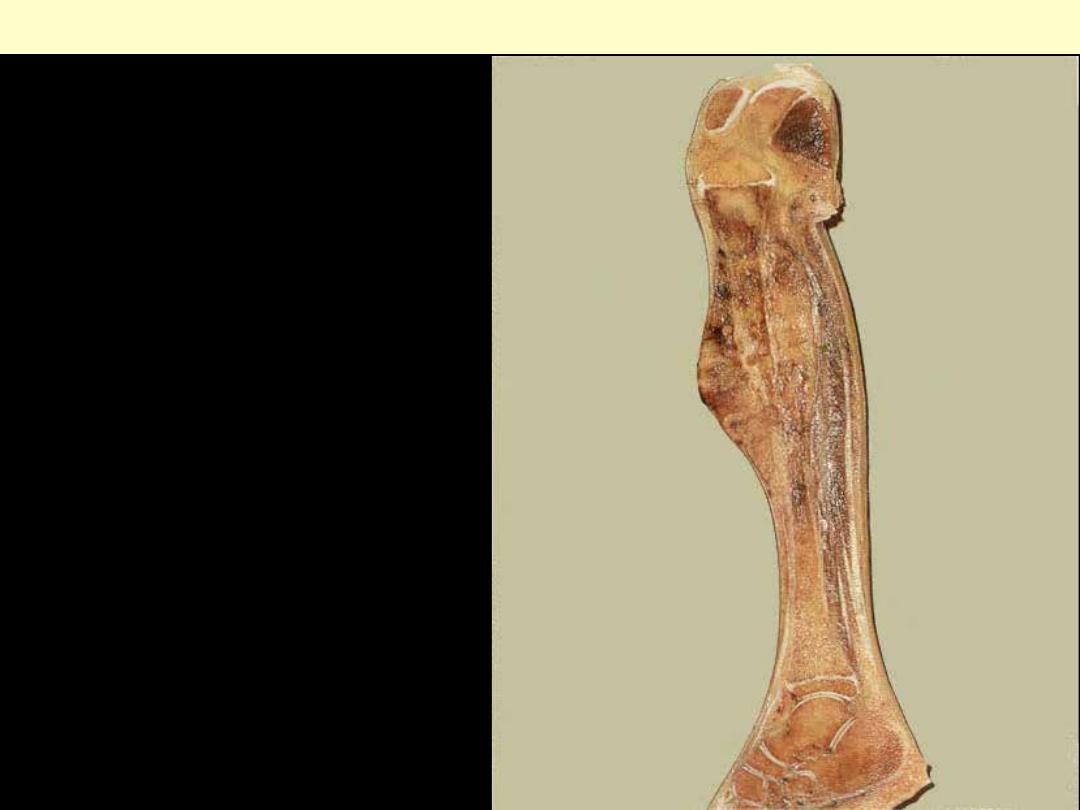
This primary bone tumor mainly occurs in the diaphysis of long bones of children and young adults.
There is a slight male predominance. This diaphyseal tumor mass is breaking through the cortex with
foci of necrosis & hemorrhage. More normal fatty marrow is seen at the right.
Ewing sarcoma
A large tumor in the upper third of the tibia
has eroded the cortical bone and extended
beneath the periosteum.
Ewing sarcoma
Ewing sarcoma
A tumor involving the distal clavicle; it is a medullary tumor that has destroyed the cortex & extend
into the surrounding soft tissue. The radiograph shows a highly permeative & destructive process with
the formation of a large soft tissue mass.
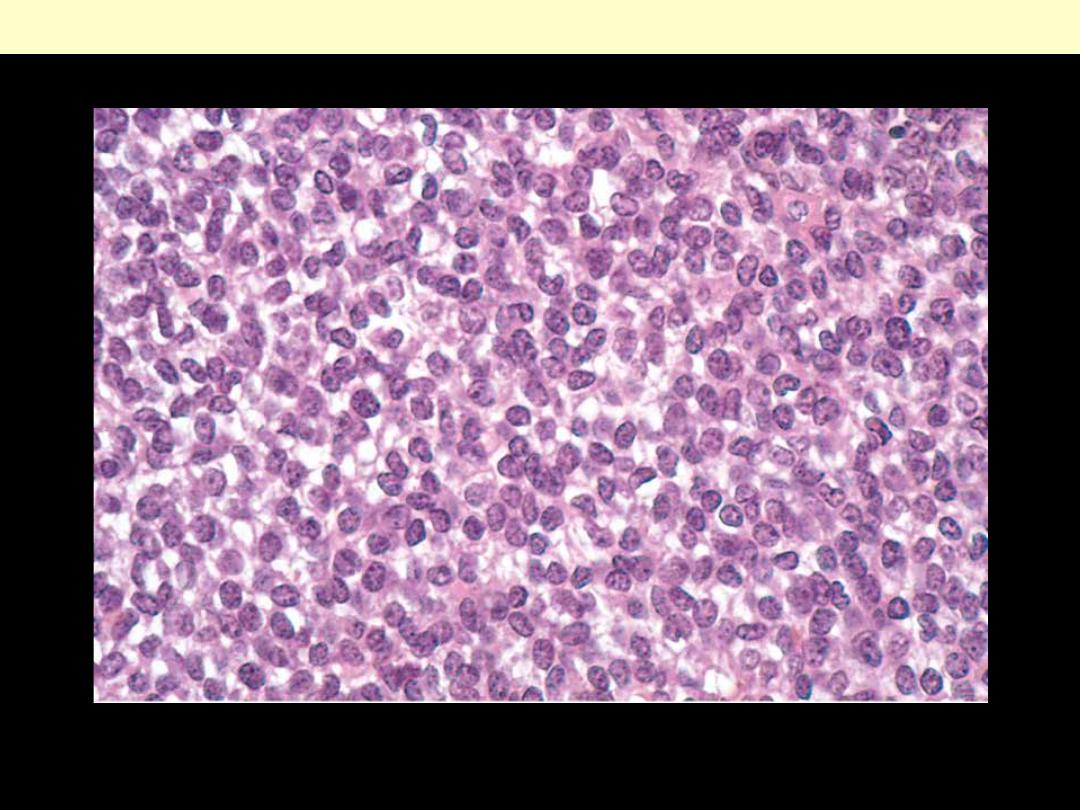
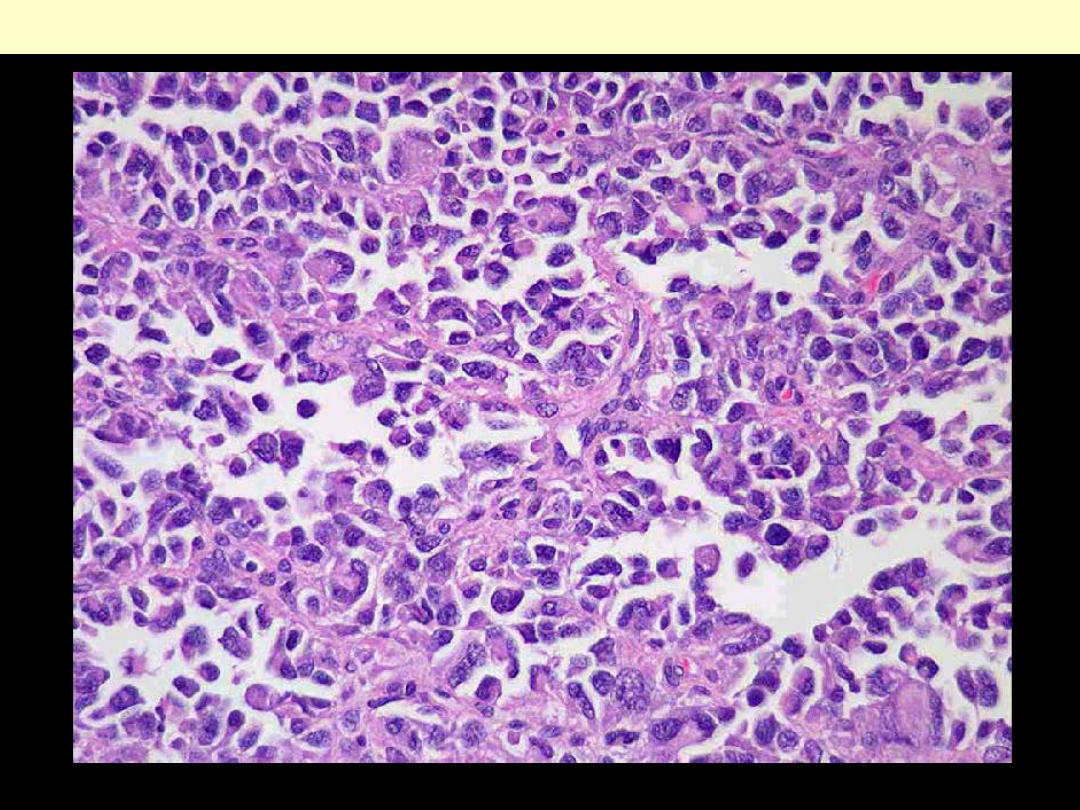
Sheets of small round cells with scant, cleared cytoplasm (PAS positive).
Ewing sarcoma
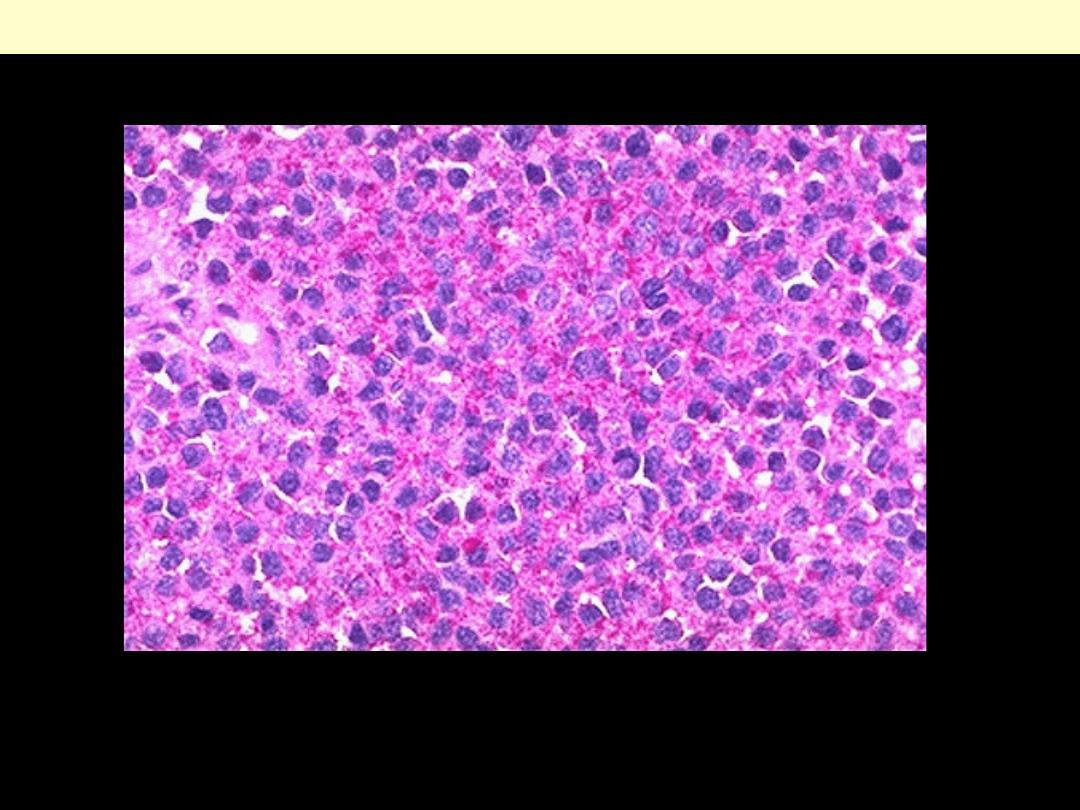
Ewing's sarcoma contains abundant glycogen, as seen by the reddish granular cytoplasmic staining by
PAS stain here.
Ewing sarcoma
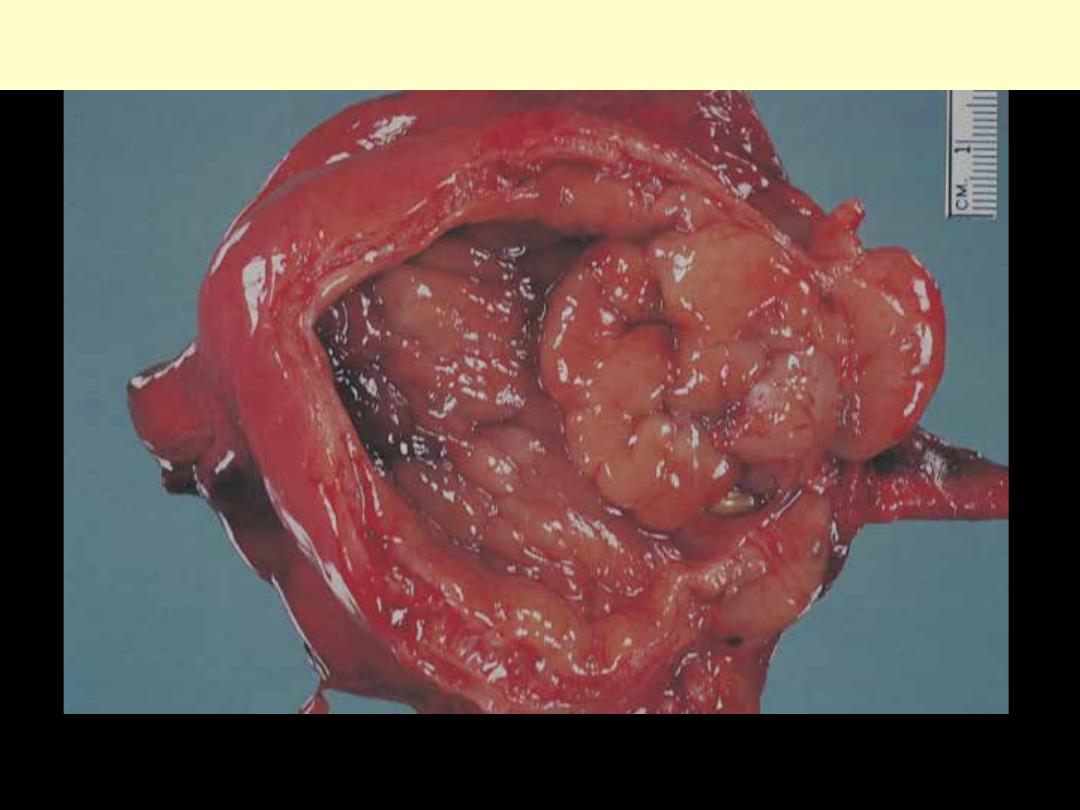
Giant cell tumor bone
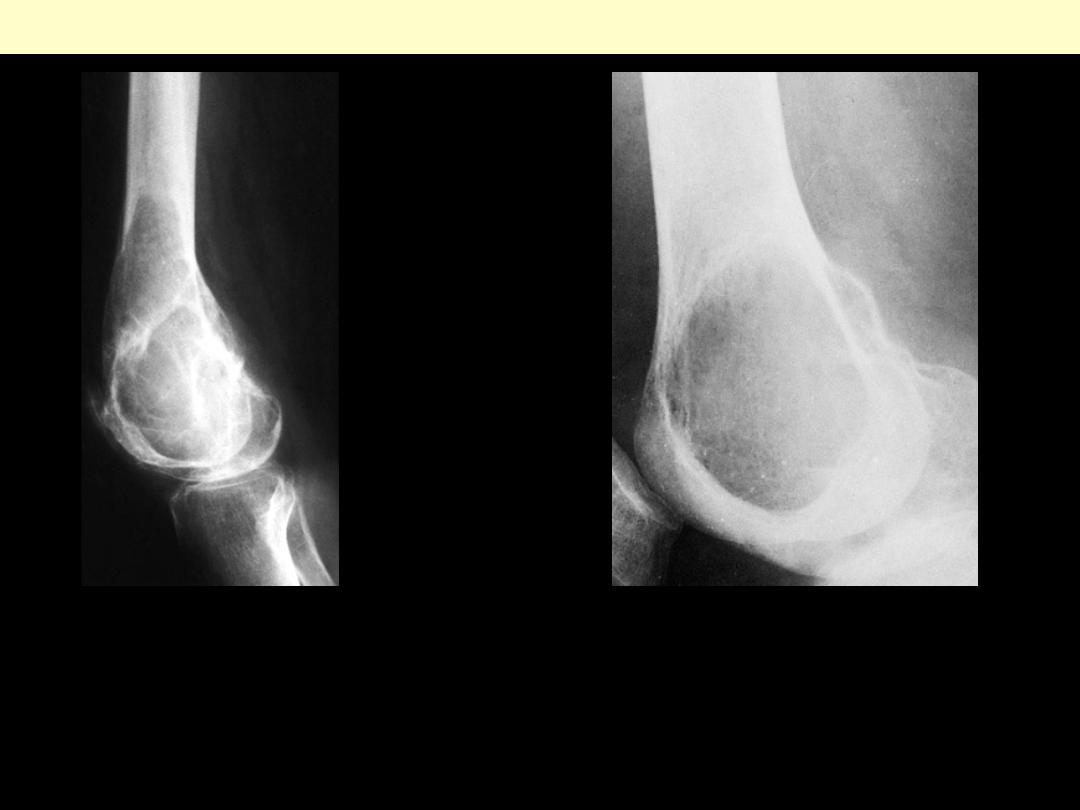
Typical radiograph of giant cell tumor of distal end of femur involving epiphysis and metaphyseal
area. The lesion was resected surgically.
Giant cell tumor of lower end of femur
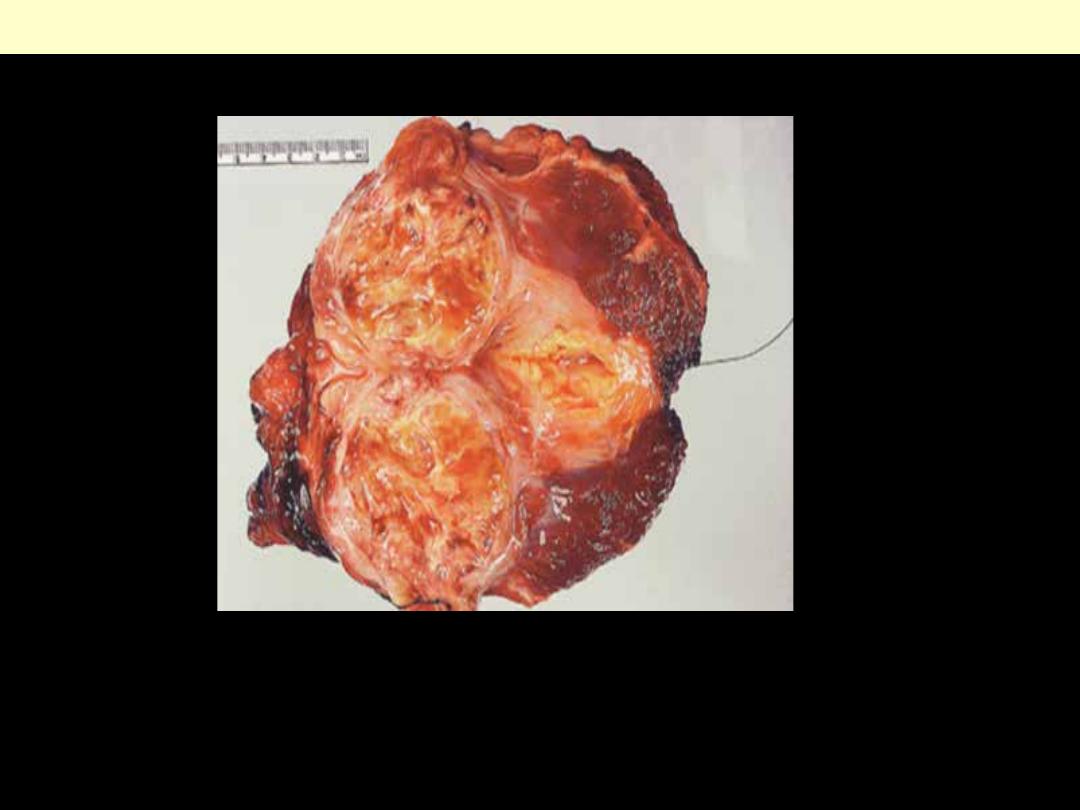
Gross appearance of giant cell tumor of lower
end of femur. The lesion is characteristically
peripheral, expansile, well circumscribed, and
hemorrhagic.
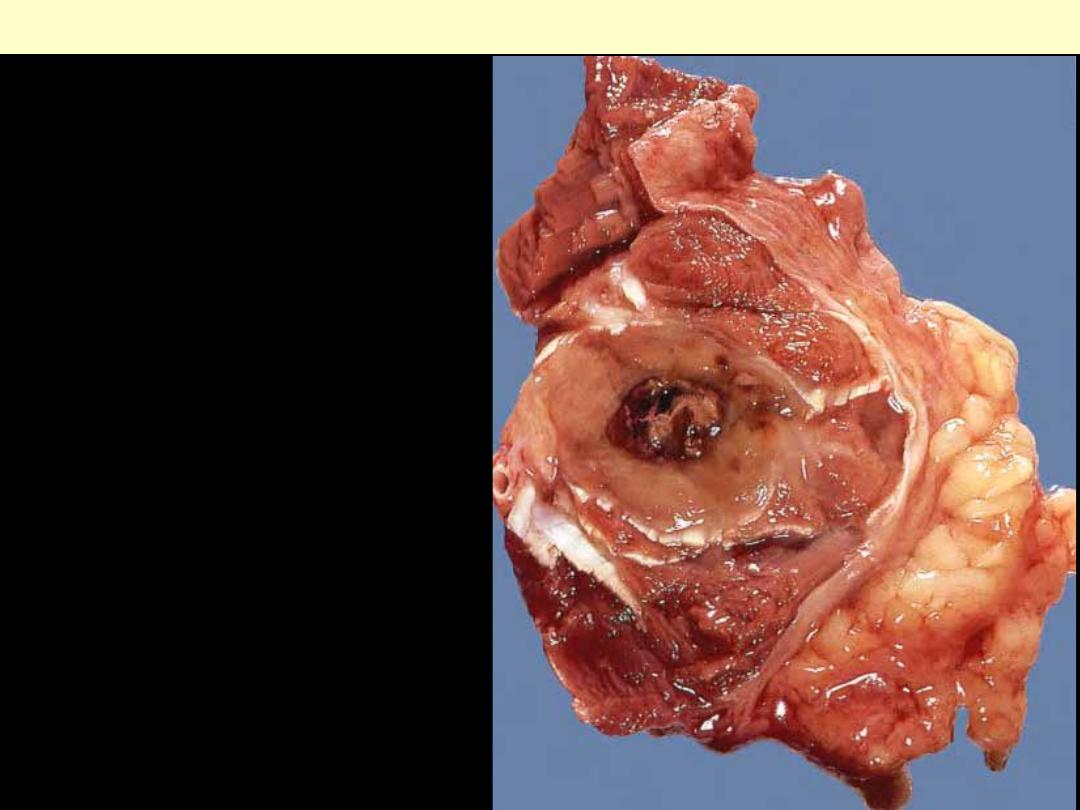
The lesion, which has a very hemorrhagic
quality, has destroyed the cortex and
extended into the adjacent soft tissues.
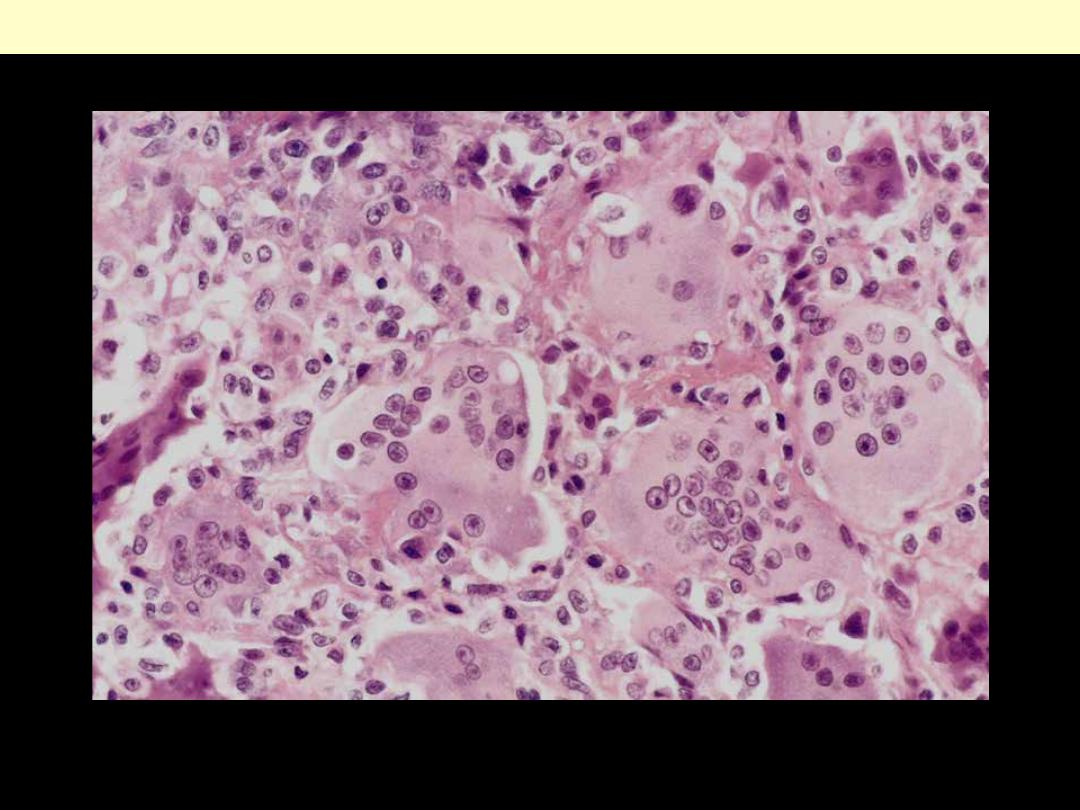
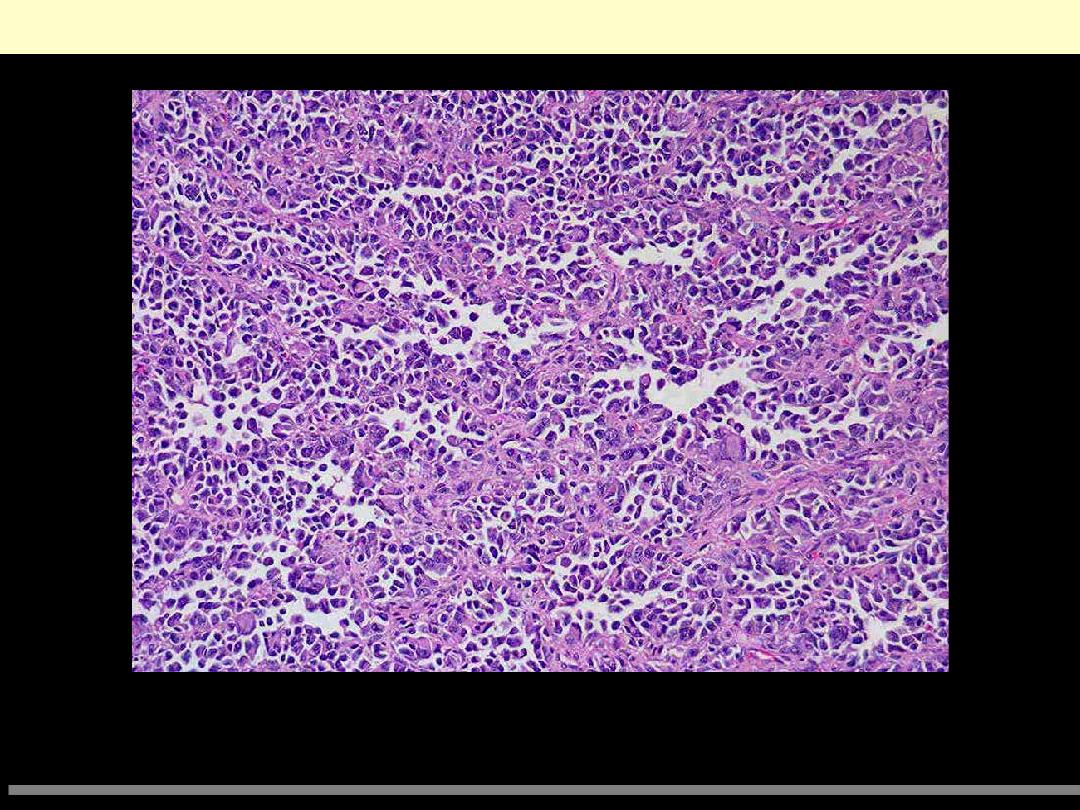
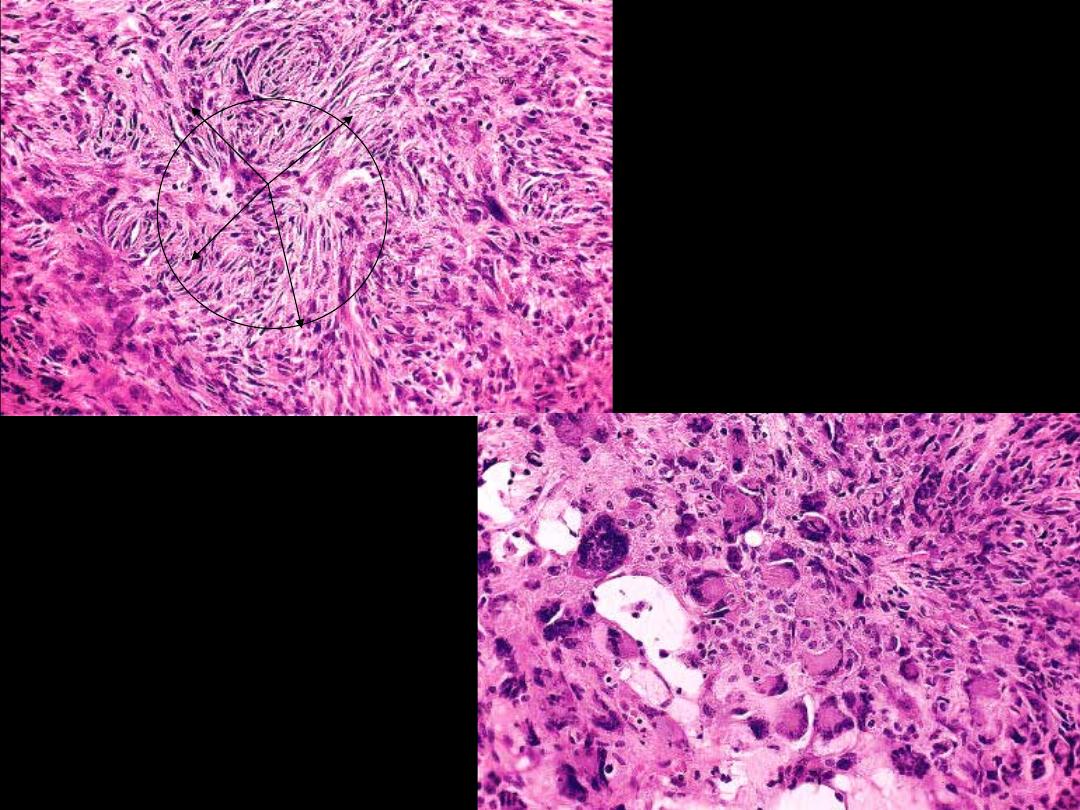
Benign giant-cell tumor showing abundant multinucleated giant cells and a background of
mononuclear cells.
Giant cell tumor of bone (osteoclastoma)
This section of vertebral bone from autopsy demostrates multiple foci of pale irregular metastases. The
most common neoplasm in bone is a metastasis. A closer view of bone metastases. Virtually all bone
metastases are from carcinomas.
Metastatic carcinoma vertebrae G
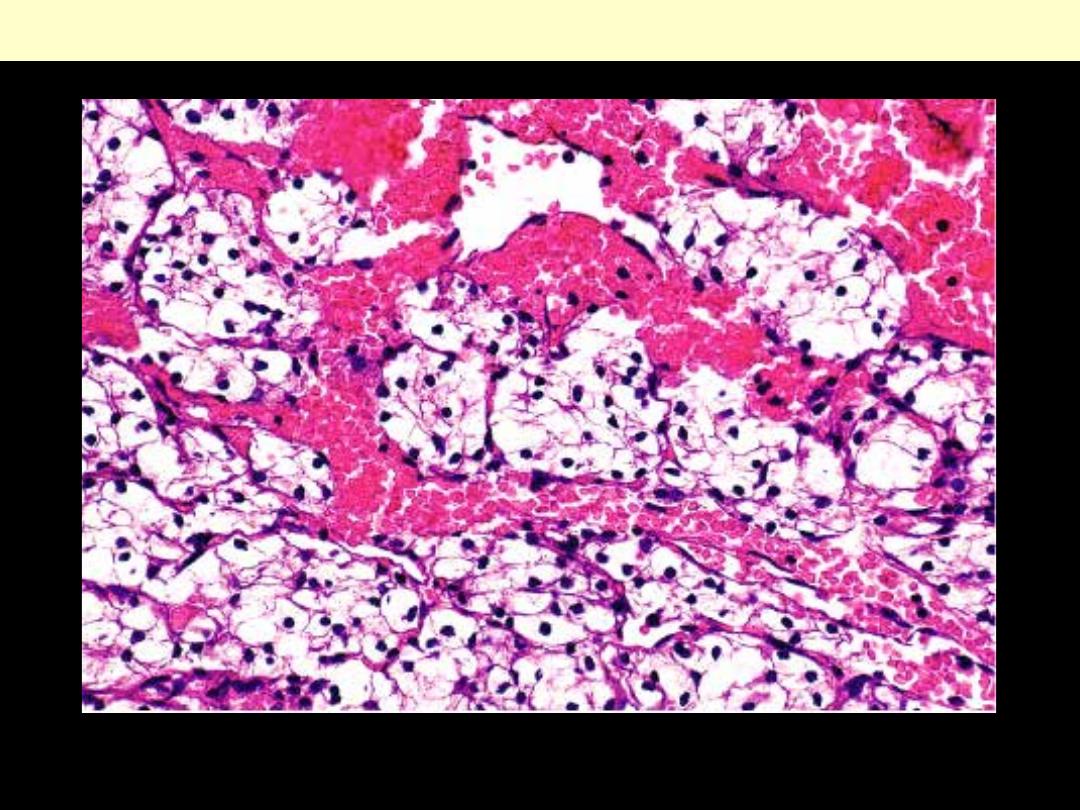
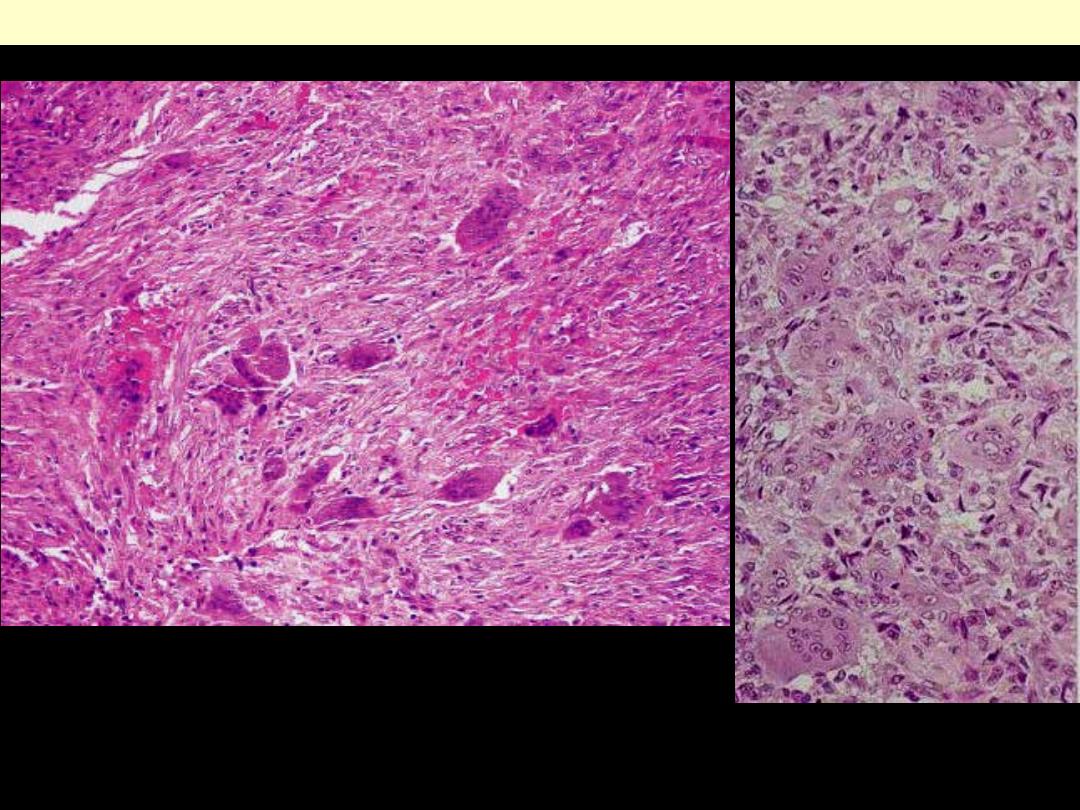
Microscopic appearance. The optically clear appearance of the cytoplasm, rich vascularity & extensive
hemorrhage are characteristic features.
Metastatic renal cell carcinoma bone
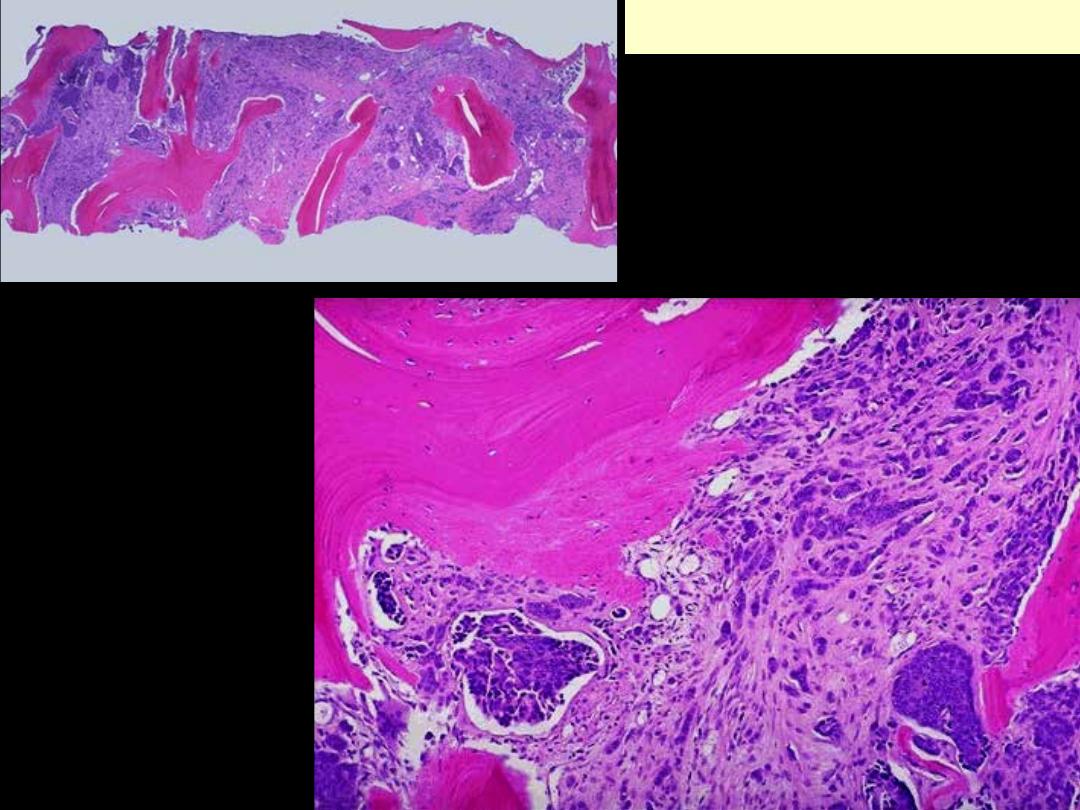
Here is a microscopic view of
metastases to bone. Such areas appear
as "hot spots" on radiographic scans. If
the bone is markedly weakened by the
metastasis, then a "pathologic" fracture
is possible.
At high magnification,
metastatic infiltrating
ductal carcinoma of breast
is seen within bone and
filling the marrow cavity.
There is reactive new bone
with pale pink osteoid
being laid down next to a
bony spicule at the upper
left.
Metastatic breast ca to bone
Muscles
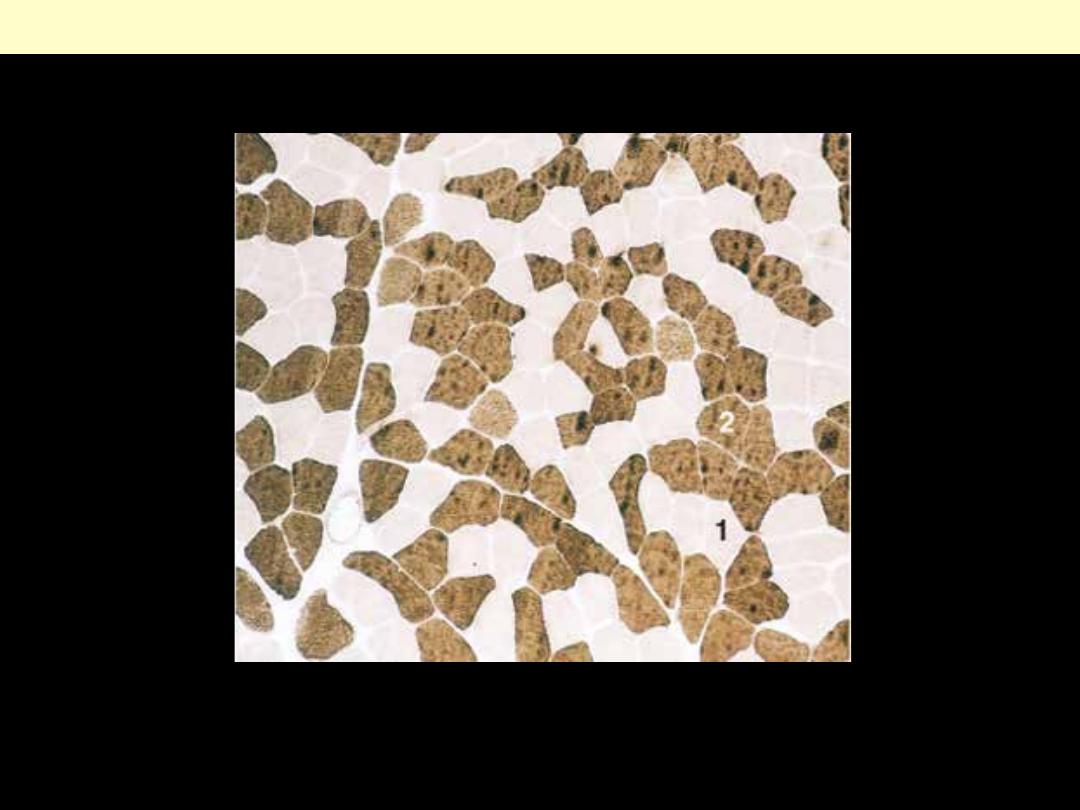
A, ATPase histochemical staining of normal muscle showing checkerboard distribution of intermingled
type 1 (light) and type 2 (dark) fibers.
Special staining technique to separate muscle fibers
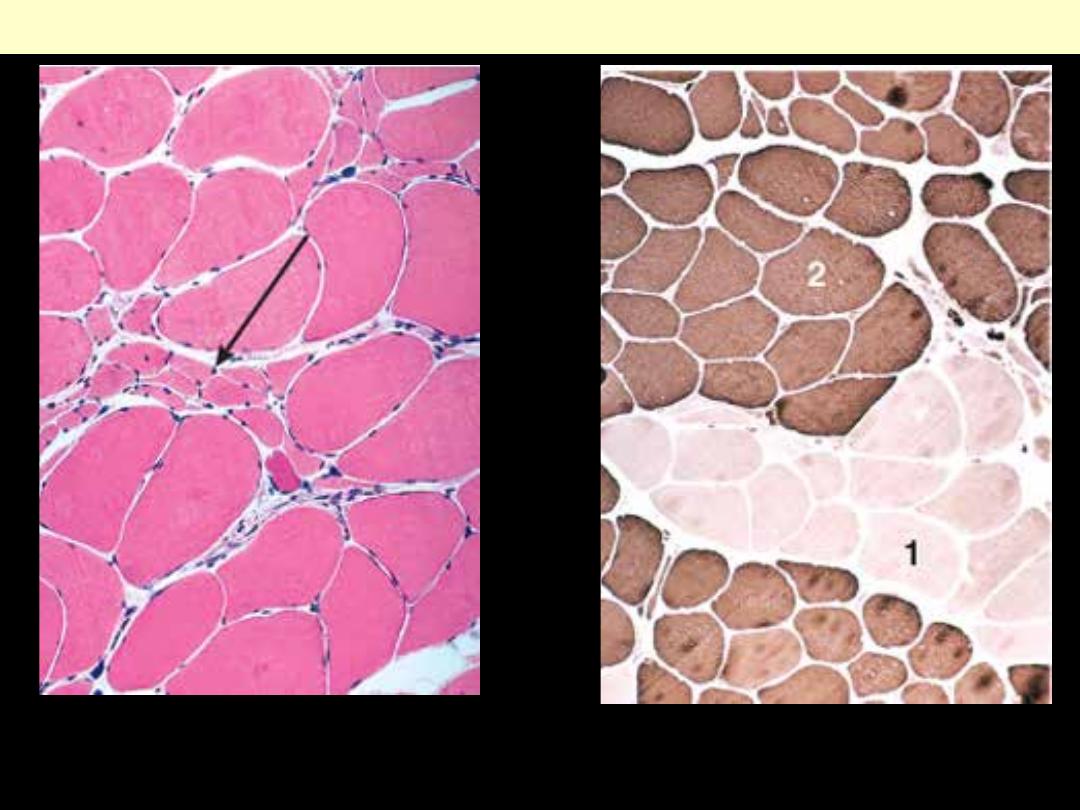
Lt. A cluster of atrophic fibers (group atrophy) in the center (arrow).
Rt. Fibers of either histochemical type (I & II) are grouped together after reinnervation of muscle. (cf.
fig.. 12-31)
Neurogenic muscle atrophy
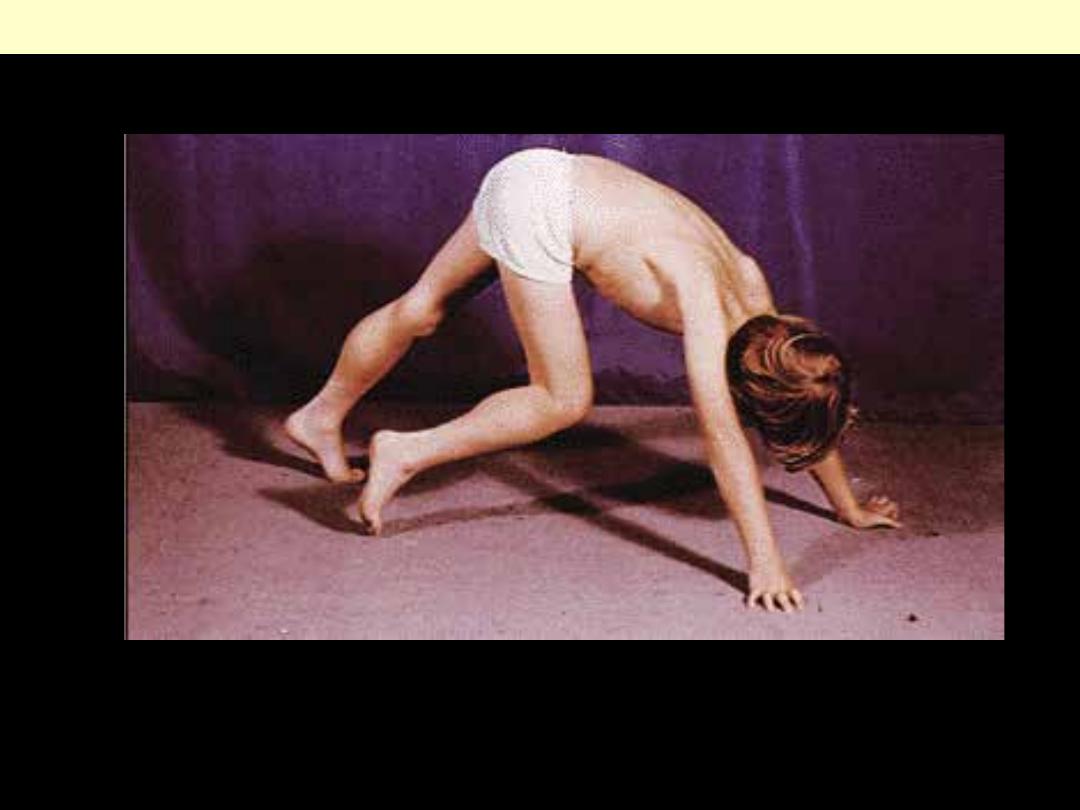
A boy with Duchenne muscular dystrophy (DMD) demonstrating pseudohypertrophy of his calves
Duchenne muscular dystrophy (DMD)
Muscle atrophy
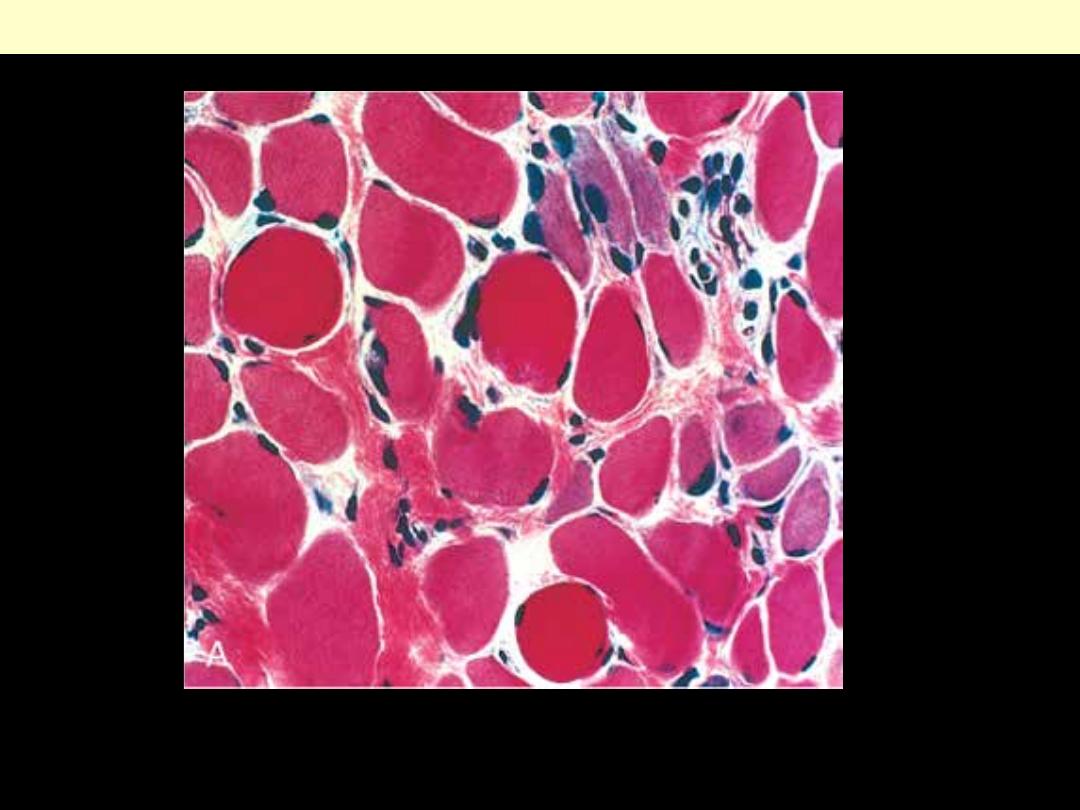
There is variation in muscle fiber size, increased endomysial connective tissue, and regenerating fibers
(blue hue).
Duchenne muscular dystrophy (DMD)
Tumors - Muscles
The grape-like configuration of this lesion is characteristic.
Sarcoma botrryoides (embryonal rhabdomyosarcoma) of vagina
Embryonal Rhabdomyosarcoma (sarcoma botryoides) Urinary
bladder
A huge glistening tumor mass is seen filling the lumen of the organ.
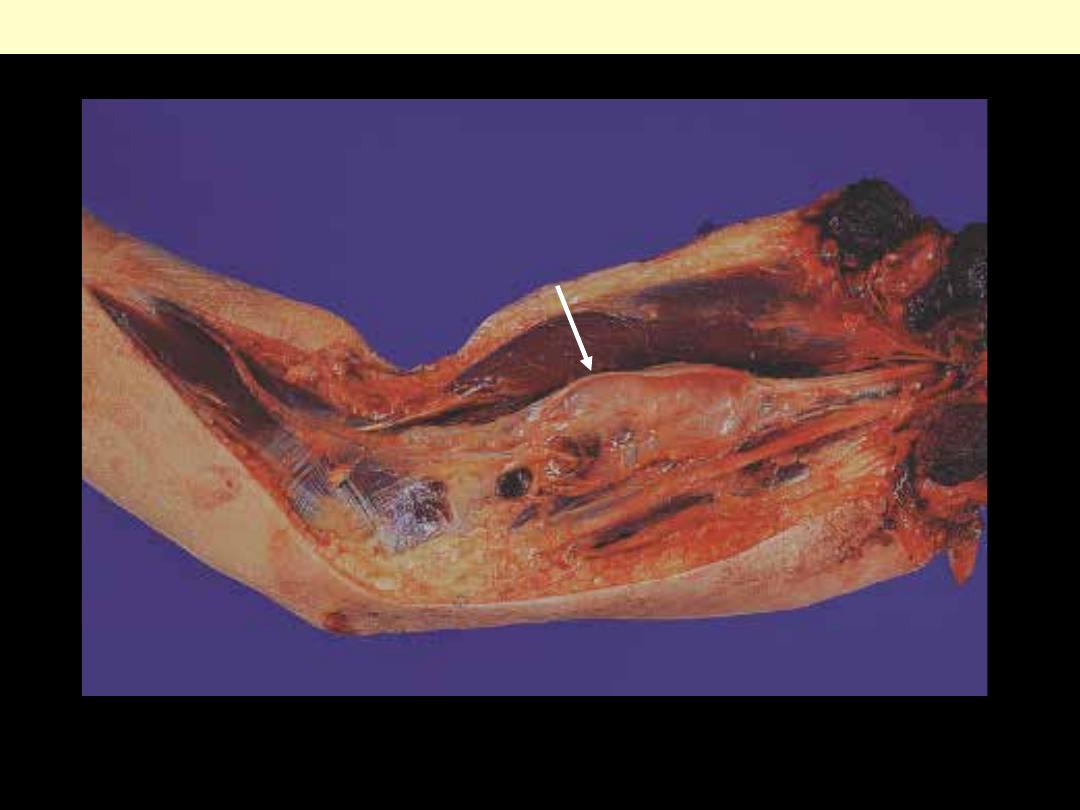
This tumor was removed from the forearm
with a good margin of muscle around it. The
tumor is brown, with a central area of
haemorrhage. Wide local resection,
wherever possible, is currently accepted as
the treatment of choice for malignant soft
tissue tumors.
Rhabdomyosarcoma

Gross appearance of alveolar rhabdomyosarcoma. The tumor is embedded within skeletal muscle.
Alveolar rhabdomyosarcoma
Nests of small round cells with scant cytoplasm grouped in nests that are separated by thick fibrous
trabeculae. Cells in centers of nests are poorly cohesive & fall away from sides to produce a pattern
reminiscent of lung alveoli. See higher power next
Alveolar rhabdomyosarcoma
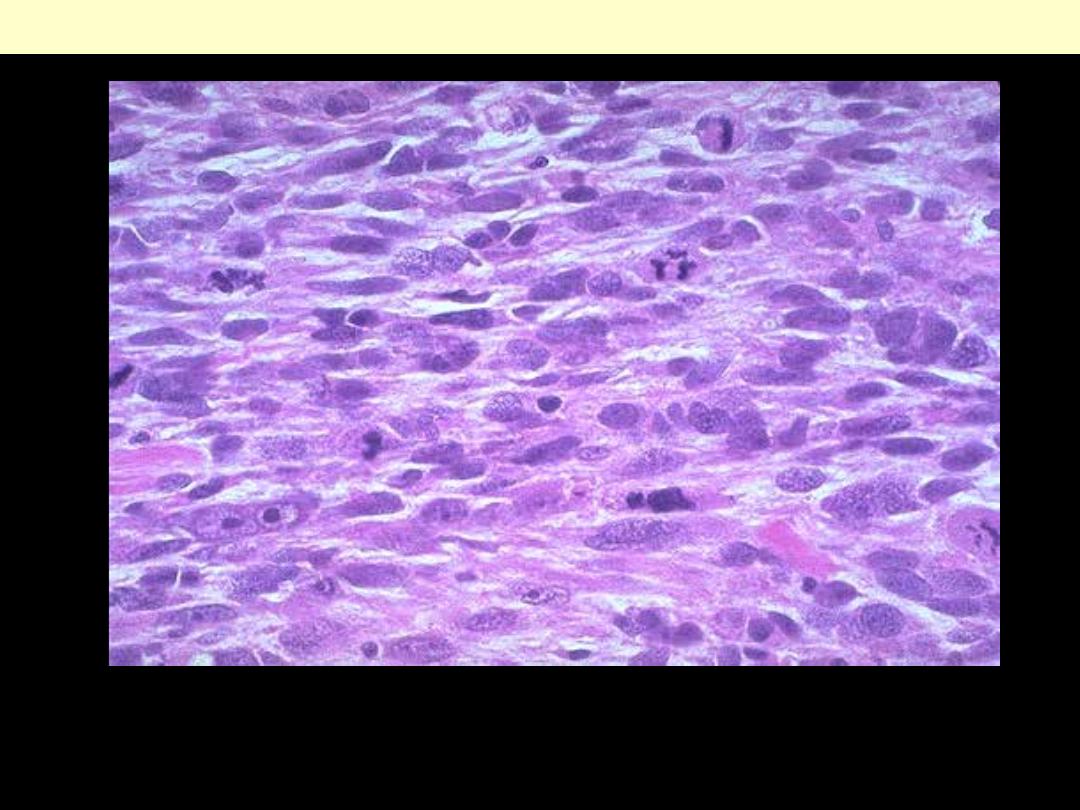
Note the eosinophilic cytoplasm & the presence of rhabdomyoblasts (malignant giant cells).
Pleomorphic rhabdomyosarcoma with tumor giant cells and tapering cytoplasmic processes
(rhabdomyoblasts).
Pleomorphic-type rhabdomyosarcoma
Soft tissue
Fat tumors
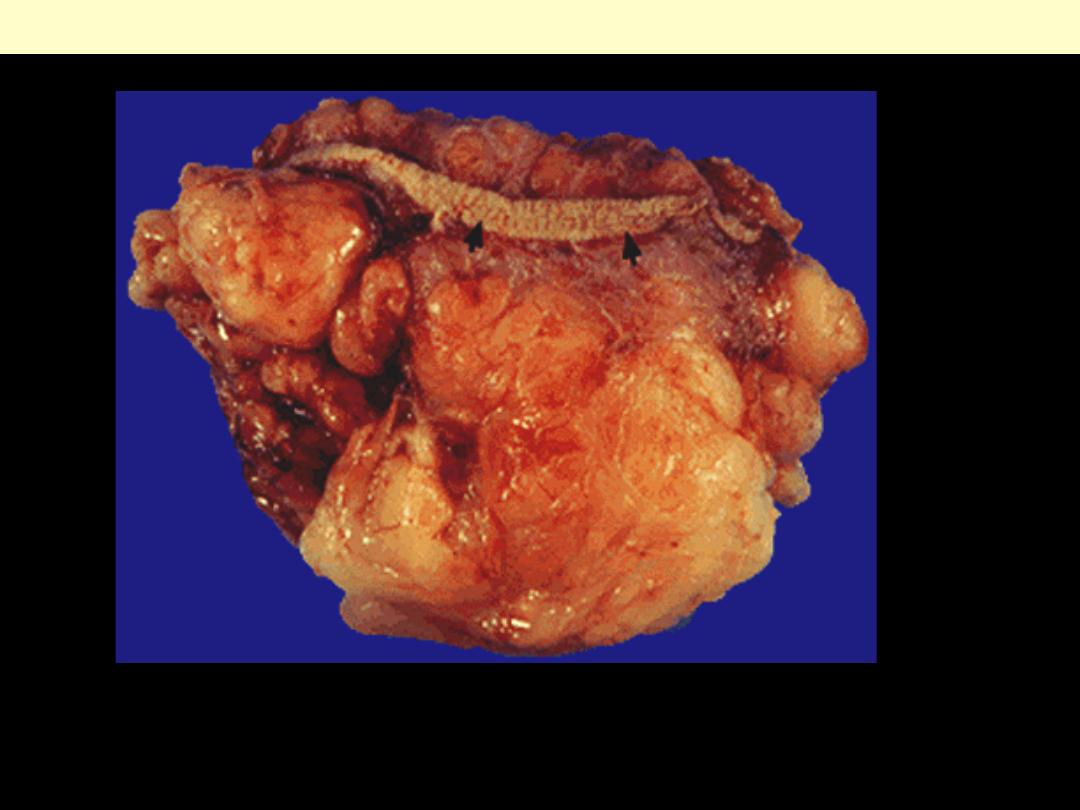
External surface of (benign) lipoma. The bright yellow color is typical of fat. Note the lobulated
appearance, which is also typical of this lesion. This particular tumor arose in the subcutaneous fat
(note the small strip of skin denoted by the black arrows).
Subcutaneous lipoma
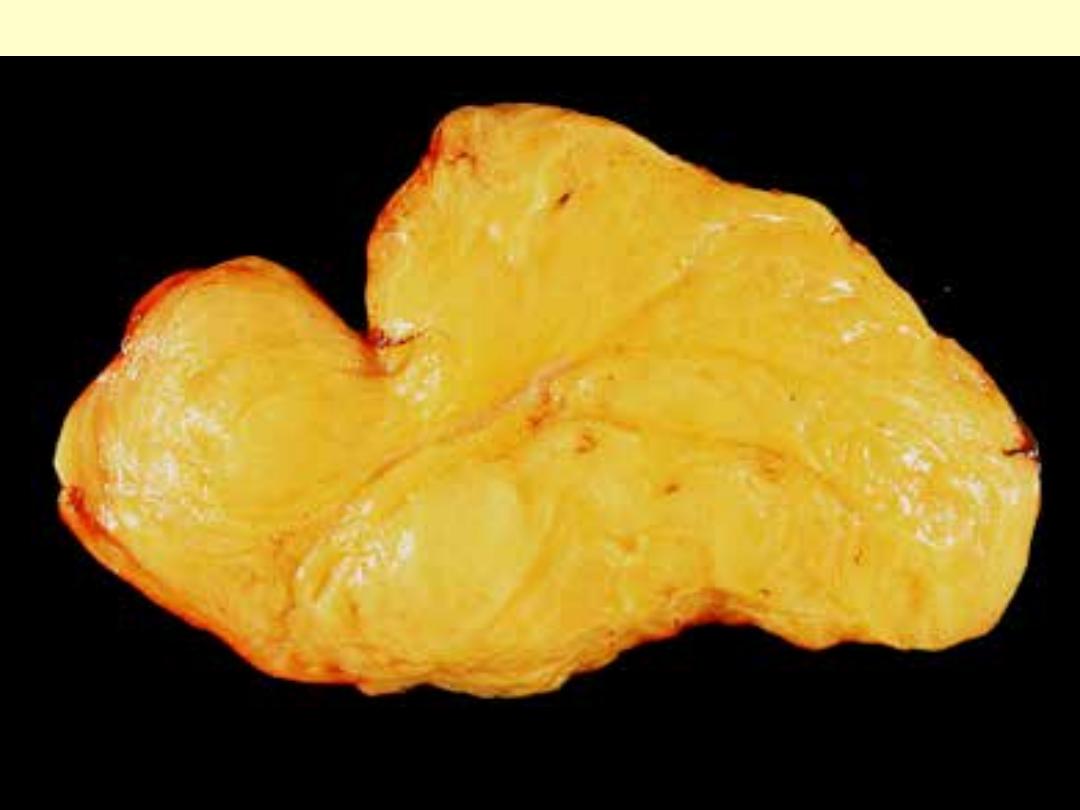
Conventional Lipoma
Except for the circumscription, the appearance is indistinguishable from that of normal fat. lipomas
consist of bright yellow fat separated by fine fibrous trabeculae
.
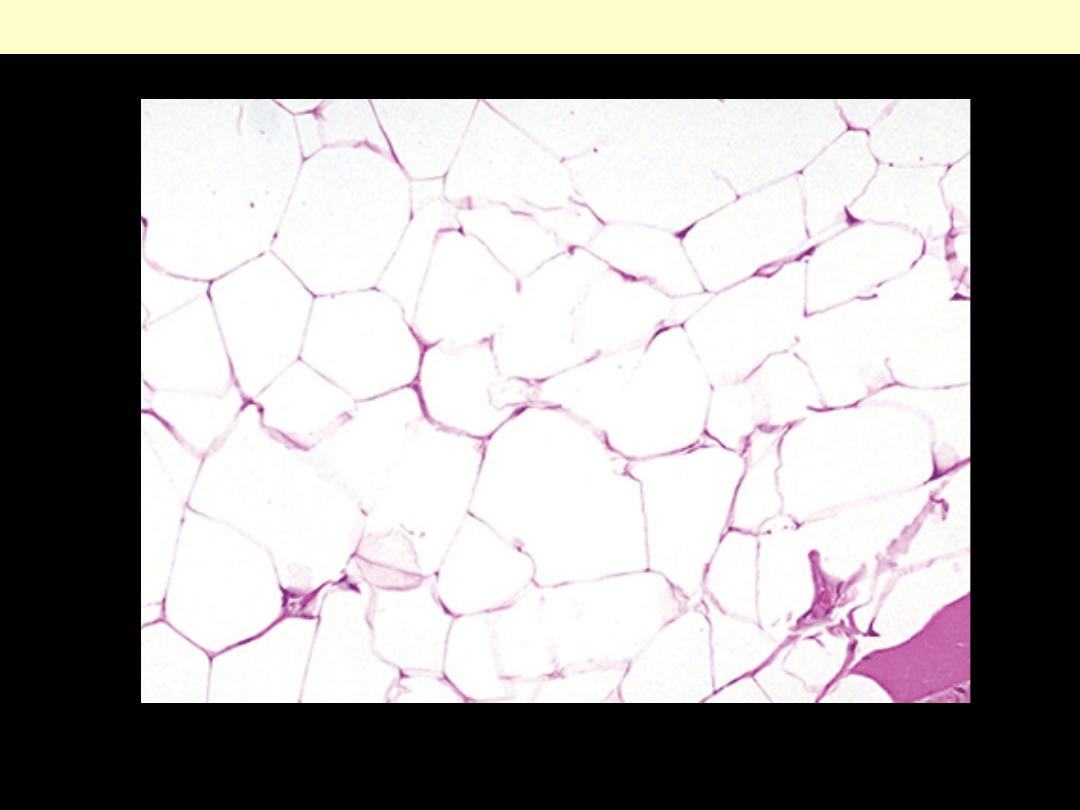
The entire lesion is composed of typical large adipocytes
Subcutaneous lipoma

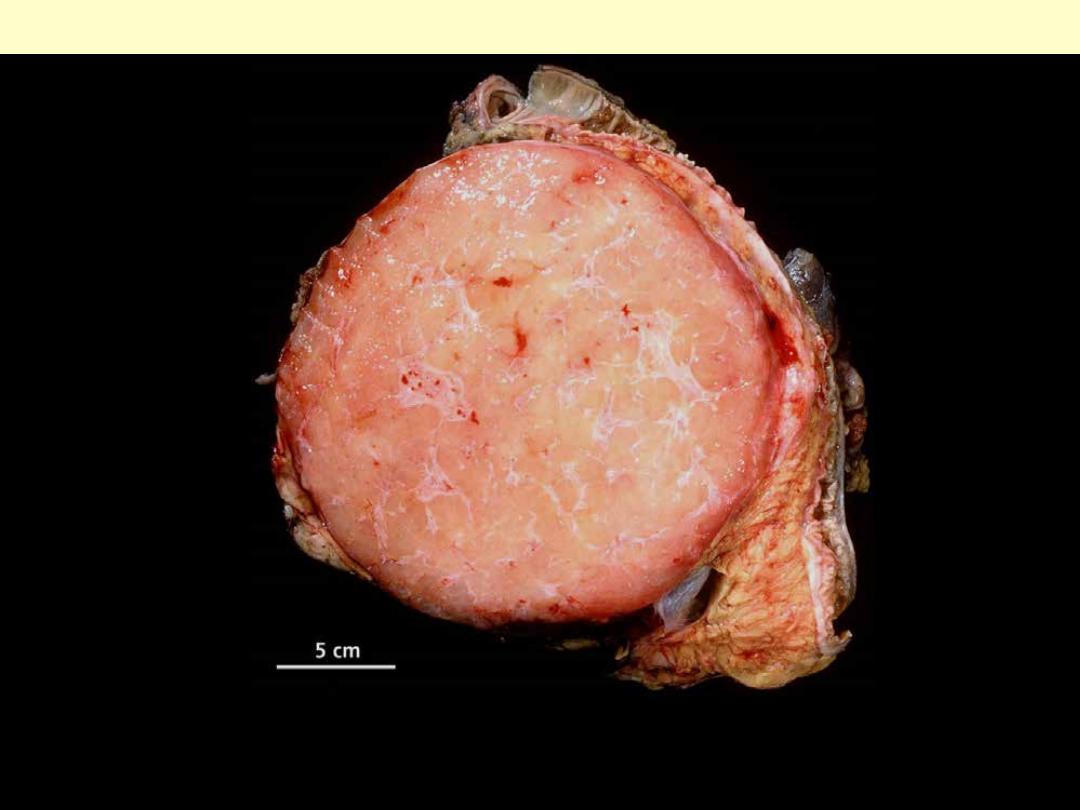
Photograph of sectioned gross specimen reveals the solid but gelatinous myxoid liposarcoma.
Myxoid liposarcoma thigh
Well demarcated lipoma-like tumor in the mesocolon. Liposarcomas are generally large tumors
Liposarcoma of mesocolon
Lipoblast: relatively specific for liposarc
These are relatively specific for liposarcoma; the cell contains multiple cytoplasmic lipid vacuoles that
scallop the nucleus.
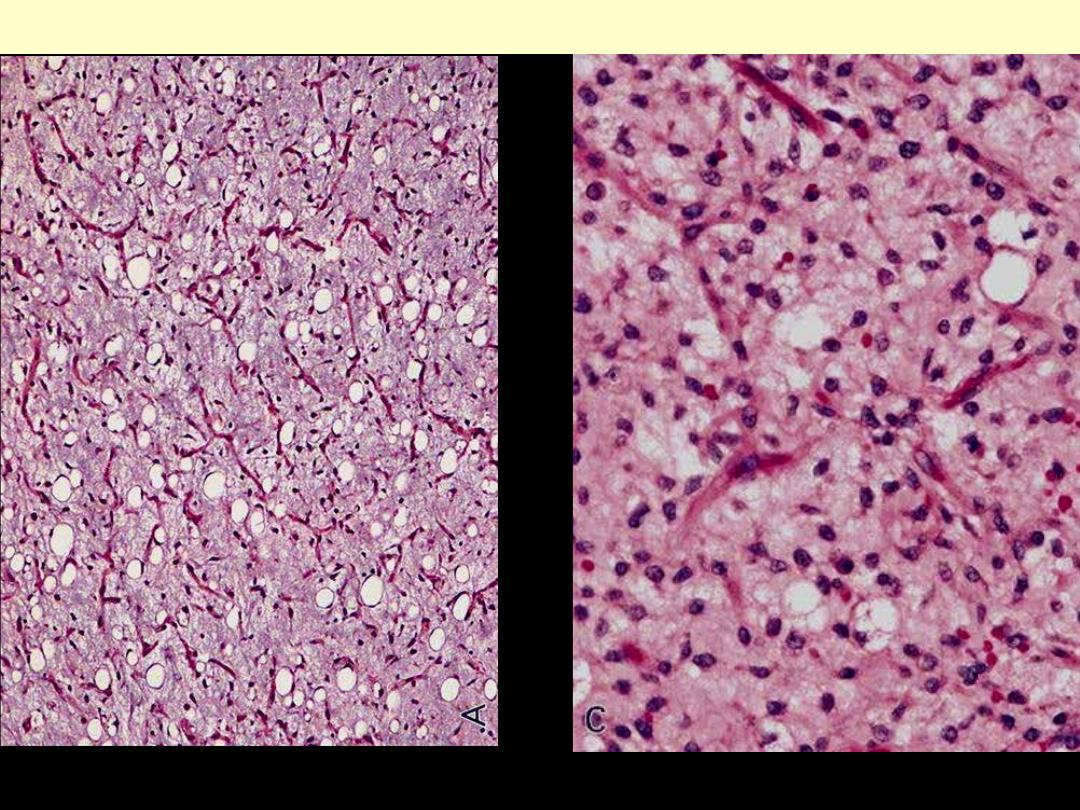
Adult-appearing fat cells and more primitive cells, with lipid vacuoles (lipoblasts) are scattered in
abundant myxoid matrix with compressed & branched capillaries
Myxoid liposarcoma thigh
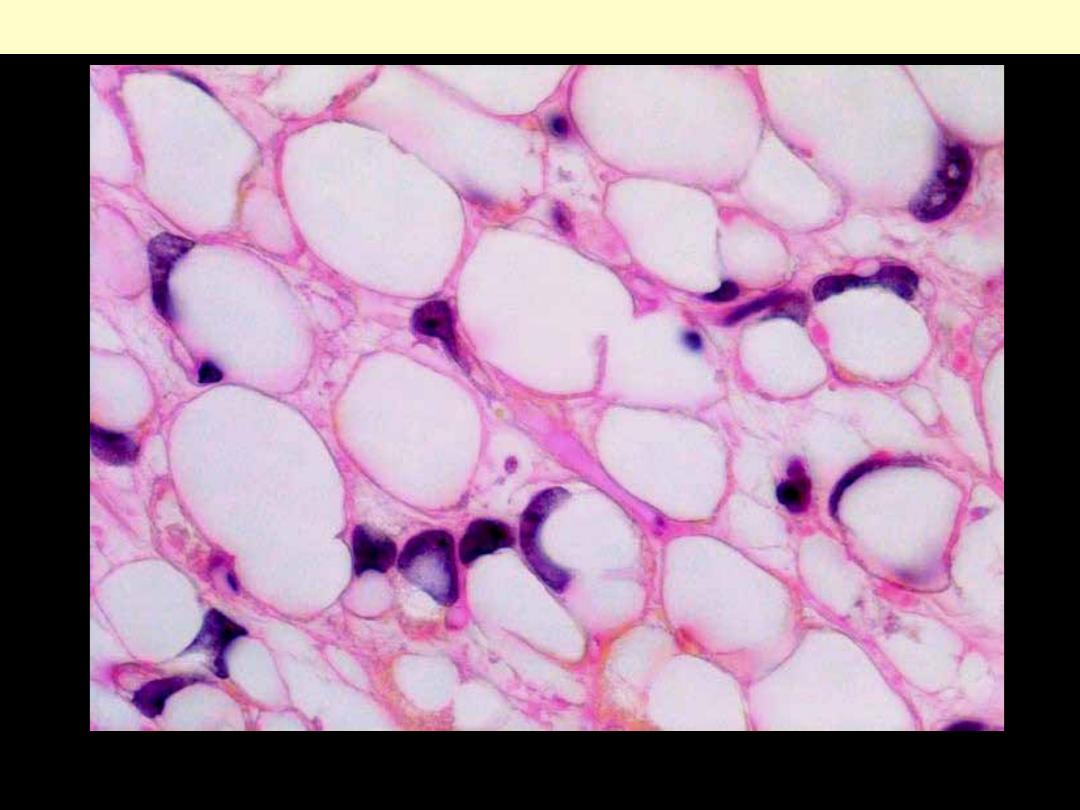
The cell nuclei of Lipoblasts show, in contrast to mature fat cells much larger nuclei with Atypia. They
are typical, but not specific for the liposarcoma.
Myxoid liposarcoma signet ring lipoblasts
Pleomorphic liposarcoma
The very poorly differentiated tumors can resemble various other high-grade malignancies.
Fibrohistiocytic tumors
Soft tissue MFH: most cases occur in deep soft tissues of extremities in adults (reported in children).
Often quite large at time of excision
Malignant fibrous histiocytoma
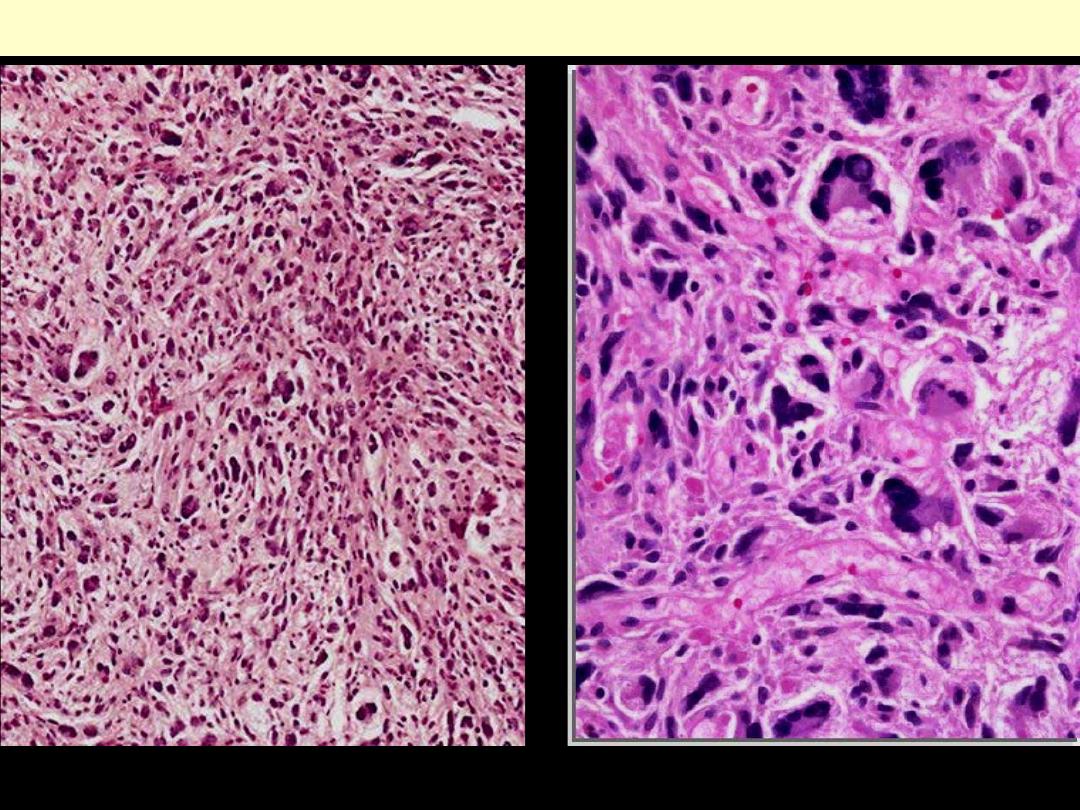
MFH of storiform/pleomorphic type.
The two most important microscopic
features of MFH are
1. Presence of highly pleomorphic
tumor cells
2. Storiform pattern of growth i.e.
bundles of spindle cells radiating
from a central focus in a cart wheel-
like fashion (arrows)
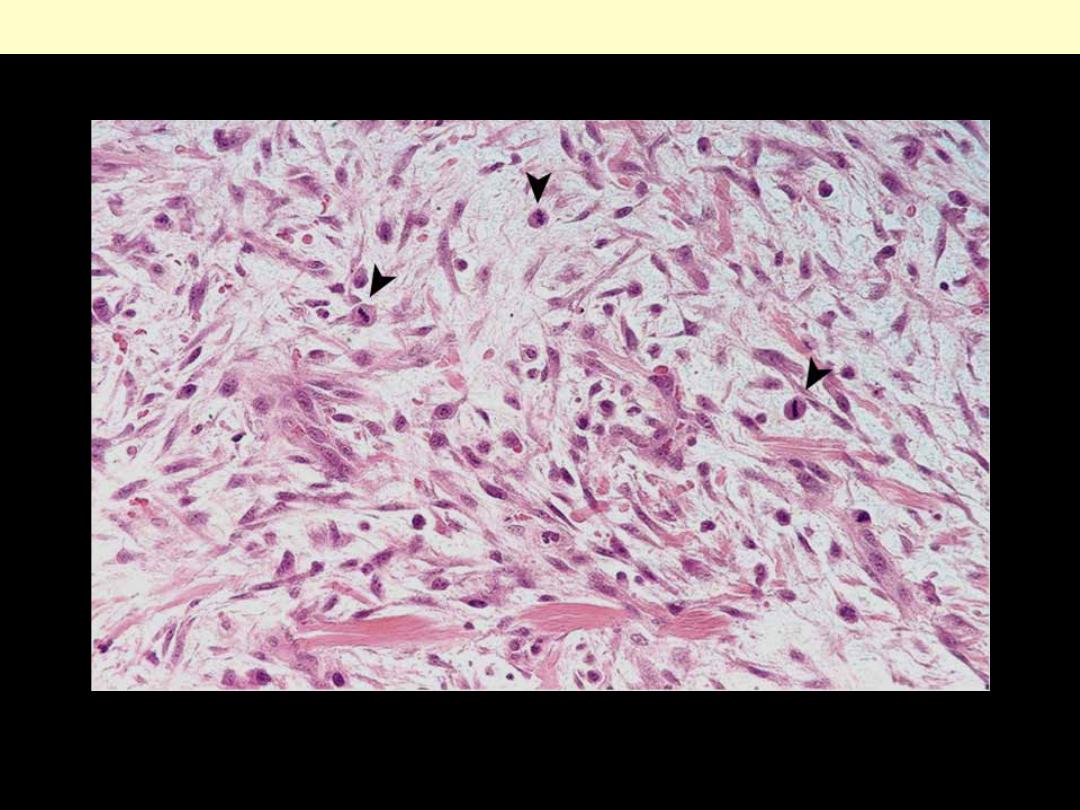
There is marked pleomorphism, with
numerous multinucleated giant cells.
Fibrous tumors + Tumor-
like lesions
A highly cellular lesion composed of plump, randomly oriented spindle cells surrounded by myxoid
stroma. Note the prominent mitotic activity (arrowheads).
Nodular fasciitis
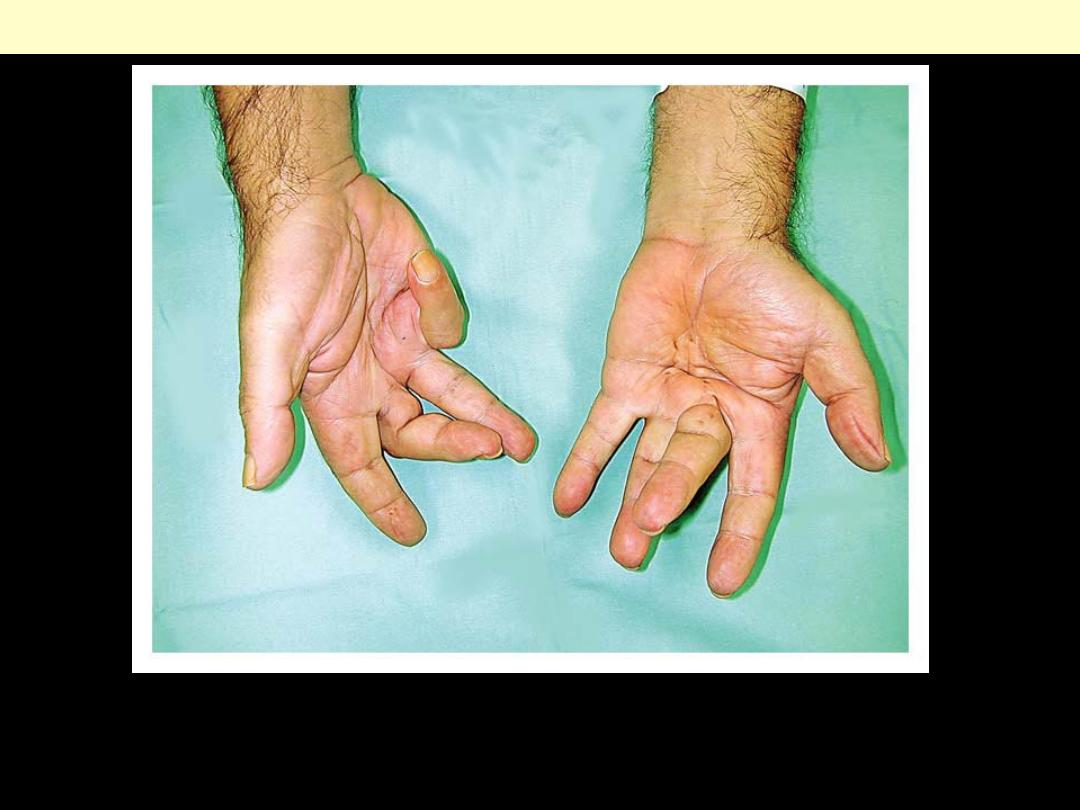
There is severe contracture of at the proximal interphalangeal joint of the right small finger and
thickened palmar fascia with multiple cords ending in firm nodules. Common risk factors for
Dupuytren's contracture include a family history of the disorder, diabetes, alcohol consumption, and
the use of vibratory machinery.
Dupuytren's contracture
Well-circumscribed fibrosarcoma growing within skeletal muscle.
Fibrosarcoma
Malignant spindle cells arranged in a herringbone pattern.
Fibrosarcoma
Smooth muscle tumors
.
The fusiform shape of the tumor is due to the fact that the tumor is following the course of the large
blood vessels from which it arose.
Leiomyosarcoma of soft tissues of arm
As with sarcomas in general, leiomyosarcomas have spindle cells but with cigar-shaped nuclei. Several
mitoses are seen here, just in this one high power field.
Leiomyosarcoma
Synovial sarcoma
Radiographic appearance of tumor located in
popliteal space.
Calcifying synovial sarcoma knee

Clinical appearance of tumor, which
presented as large ulcerated mass in ankle.
Calcifying synovial sarcoma
ankle
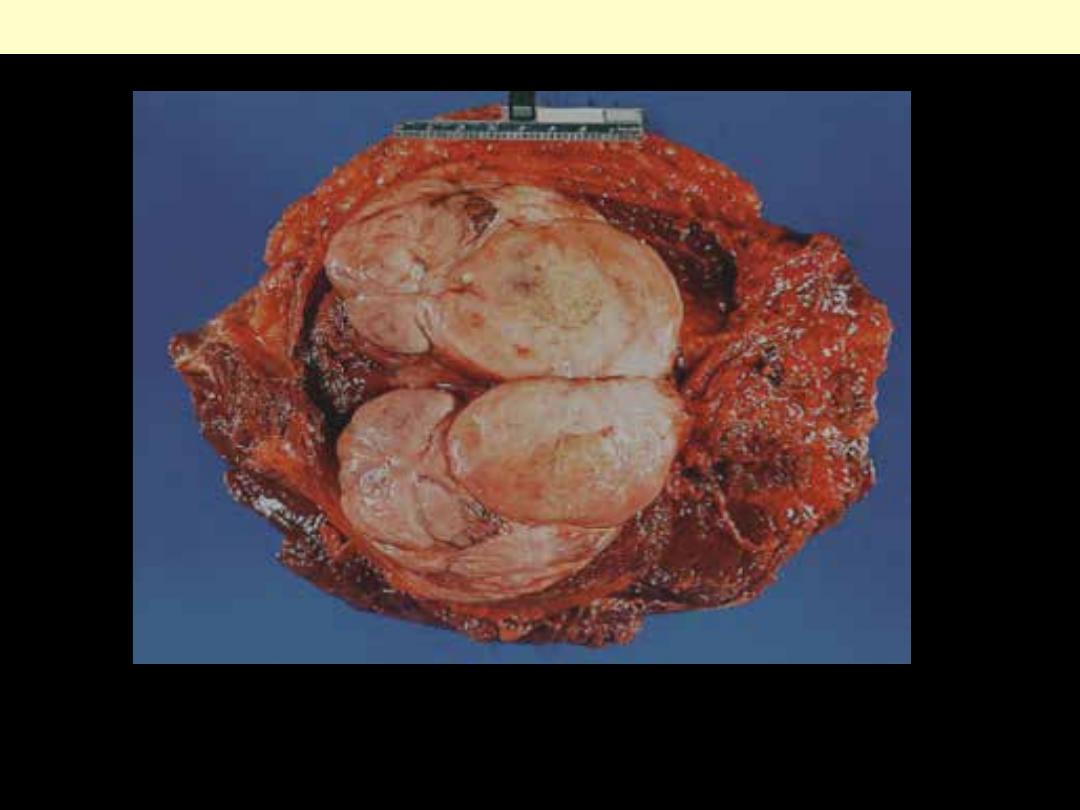
Synovial sarcoma femur
Gross appearance of deep-seated synovial
sarcoma involving periosteum of femur in
an adolescent boy.
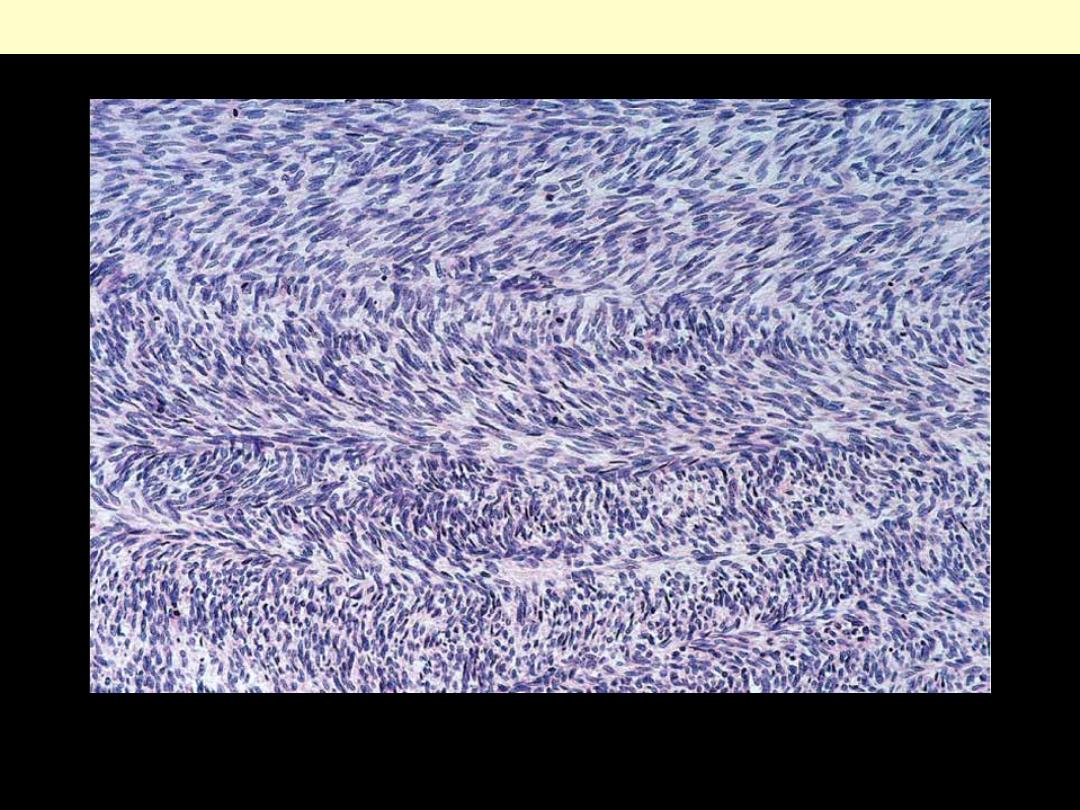
Typical biphasic appearance of synovial sarcoma
Synovial sarcoma with an adenocarcinoma-
like appearance of epithelial component
Calcifying synovial sarcoma