Baghdad College of Medicine / 4
th
grade
Student’s Name :
Dr. Montadhar Al-Madani
Lec. 4
Renal Mass
Thurs. 28 / 4 /2016
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2015 – 2016

Renal Mass Dr. Montadhar Almadani
28-4-2016
2
©Ali Kareem 2015-2016
Evaluation of renal masses
Causes
Benign causes:
- Ureteropelvic junction
obstruction (most common
cause).
- Obstructed mega ureter.
- Sever grade of reflux.
- Polycystic kidney disease
(adult, infantile).
- Simple renal cyst.
- Calyseal diverticulum.
- Abscess.
- Angiomyolipoma.
- Oncocytoma.
- Others.
Malignant causes:
- Renal cell carcinoma (adult).
- Wilm's tumor (children).
- Liposarcoma.
- Sarcoma.
- Lymphoma.
- Transitional cell carcinoma.
- Metastatic tumors.
Presentation
During antenatal ultrasound.
Accidental finding during imaging
study doing for another cause.
Abdominal mass.
Hematuria (macroscopic or
microscopic).
Flank pain, bone pain.
Anemia, cough.
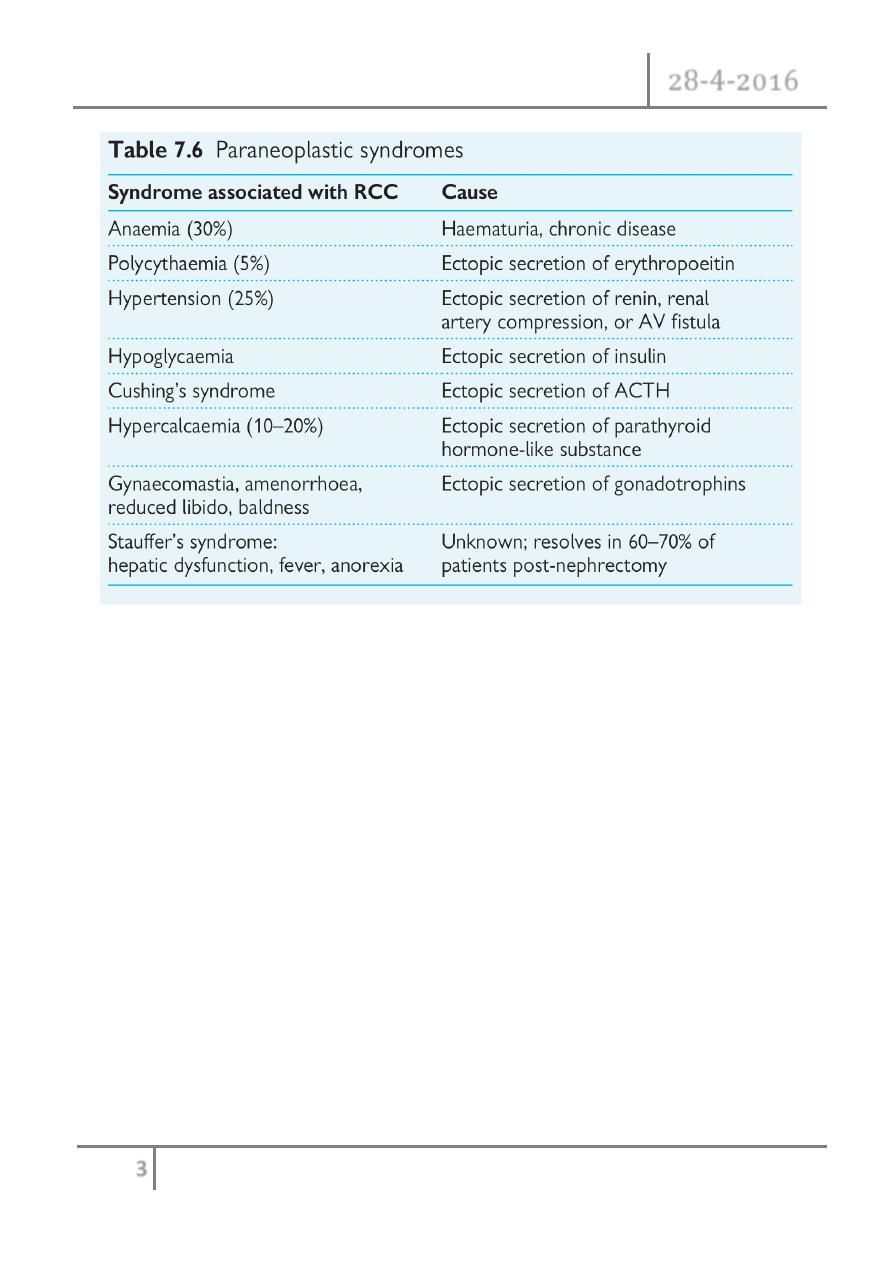
Paraneoplastic syndrome.
Fever, wt loss and sweating,
symptoms of metastasis
Polycythemia.
Shock.
Lower limb odema, varicose veins.
Others.
Renal Mass Dr. Montadhar Almadani
28-4-2016
3
©Ali Kareem 2015-2016
Work up
Biochemical:
Urine analysis to evaluate infections and hematuria.
Renal function tests to evaluate renal impairment.
Complete blood picture and ESR.
Electrolyte assessment.
AFB and PCR.
Urine cytology.
Imaging study:

Renal Mass Dr. Montadhar Almadani
28-4-2016
4
©Ali Kareem 2015-2016
CXR.
Abdominal ultrasound.
Abdominal CT scan and MRI.
Chest CT scan and MRI.
Isotope study.
Brain CT scan and MRI.
Doppler ultrasound.
IVP.
Other tests:
FNA, biopsy.
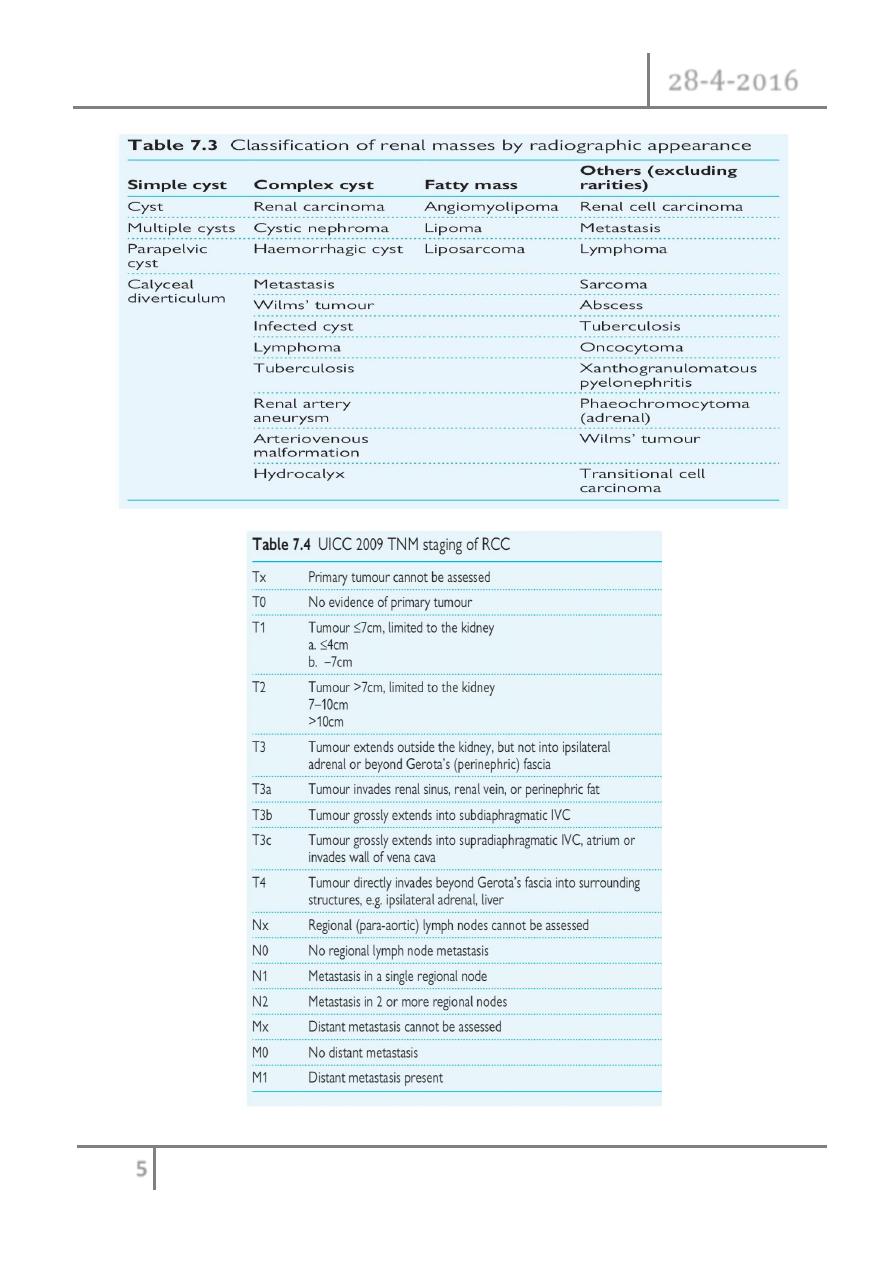
Radiological classification of renal cysts
Uncomplicated simple (smooth-walled, round or oval, without internal echoes,
and complete transmission with a strong acoustic shadow posteriorly), benign;
no follow-up if asymptomatic.
Minimally complicated; septa, calcification, hyperdense (contain blood);
benign, but require radiological follow-up.
Complicated; irregular margin, thickened septa, thick irregular calcification;
indeterminate, surgical exploration indicated unless there is history of trauma
or infection.
Large, irregular cyst margins with solid components internally; cystic renal
carcinoma until proven otherwise; surgery required.
Renal Mass Dr. Montadhar Almadani
28-4-2016
5
©Ali Kareem 2015-2016
Renal Mass Dr. Montadhar Almadani
28-4-2016
6
©Ali Kareem 2015-2016

Renal Mass Dr. Montadhar Almadani
28-4-2016
7
©Ali Kareem 2015-2016
Staging of wilm's tumor
Stage I Wilms’ tumour (43% of patients)—at least one of the following criteria
must be met:
- Tumour is limited to the kidney and is completely excised.
- The surface of the renal capsule is intact.
- The tumour is not ruptured or biopsied (open or needle) prior to removal.
- No involvement of extrarenal or renal sinus lymph–vascular spaces.
- No residual tumour apparent beyond the margins of excision.
- Metastasis of tumour to lymph nodes not identified.
Stage II Wilms’ tumour (23% of patients)—at least one of the following criteria
must be met:
- Tumour extends beyond the kidney, but is completely excised.
- No residual tumour apparent at or beyond the margins of excision.
- Any of the following conditions may also exist.
- Tumour involvement of the blood vessels of the renal sinus and/or outside
the renal parenchyma.
- The tumour has been biopsied prior to removal or there is local spillage of
tumor during surgery, confined to the flank.
- Extensive tumour involvement of renal sinus soft tissue.
Stage III Wilms’ tumour (23% of patients) at least one of the following criteria
must be met:
- Unresectable primary tumour.
- Lymph node metastasis.
- Tumour is present at surgical margins.
- Tumour spillage involving peritoneal surfaces, either before or during
surgery, or transected tumour thrombus.
Renal Mass Dr. Montadhar Almadani
28-4-2016
8
©Ali Kareem 2015-2016
Stage IV Wilms’ tumour (10% of patients) is defined as the presence of
haematogenous metastases (lung, liver, bone, or brain) or lymph node
metastases outside the abdominopelvic region.
Stage V Wilms’ tumour (5% of patients) is defined as bilateral renal
involvement at the time of initial diagnosis.
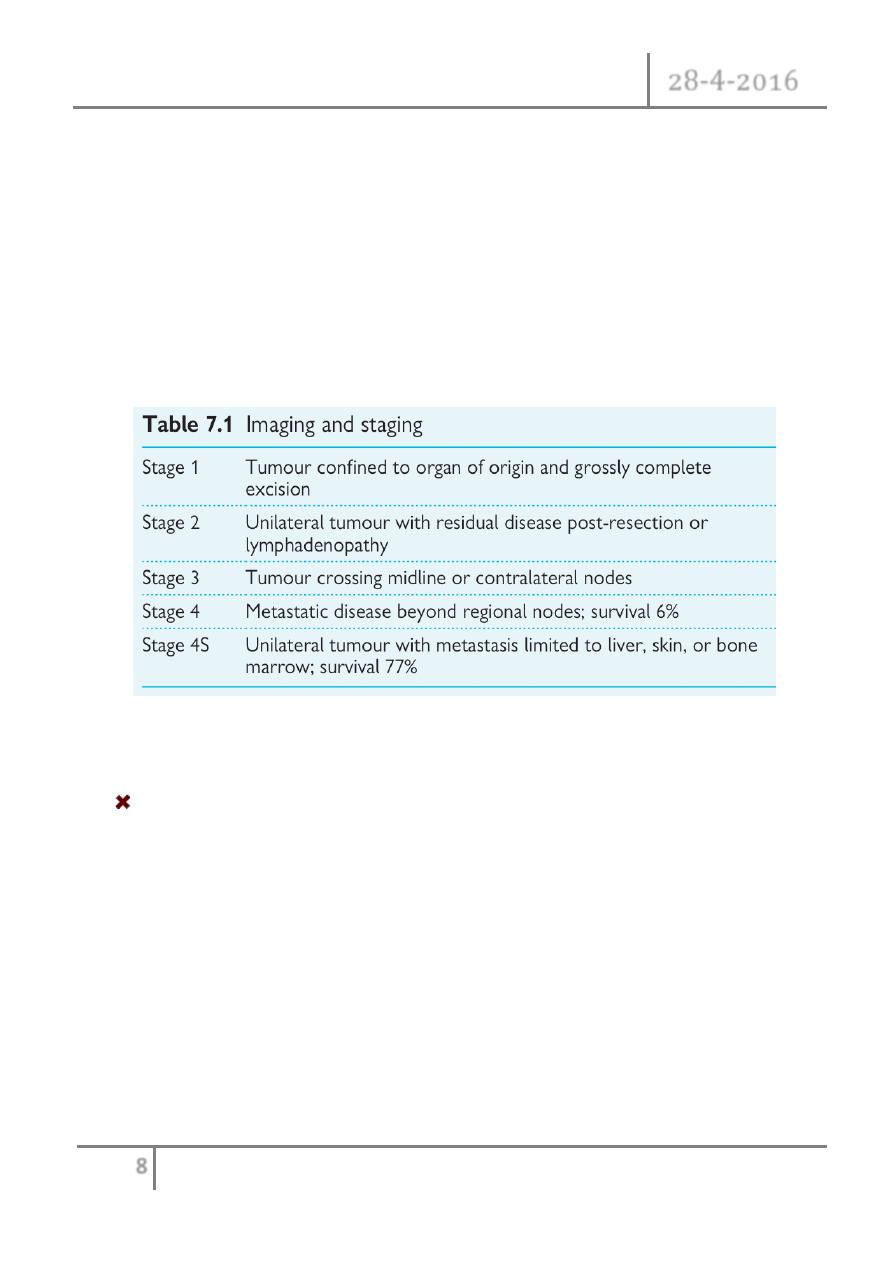
Neuroblastoma staging
Management
The management depends on the following factors:
- Behavior of mass (benign or malignant).
- Unilateral or bilateral.
- Total renal function.
- Size of mass (e.g. Angiomyolipoma).
- Age of patient.
- Localize or metastatic (if malignant).
- Mass effect like obstruction of renal pelvis.
- Options of treatment.

Renal Mass Dr. Montadhar Almadani
28-4-2016
9
©Ali Kareem 2015-2016
In simple word the treatment range from no treatment to radical nephroctomy
with chemoradiotherapy
- No treatment (e.g simple cyst).
- Cyst aspiration with sclerotic agents inside the cyst.
- Cystic removal (open, laparoscopic).
- Partial nephrectomy (open or laparo.).
- Radical nephrectomy (open, laparo.).
- Simple nephrectomy.
- Chemoradiotherapyn.
END OF THIS LECTURE
…