Dr. Tarik Al-Obaidi
Lec. 2
STOMA
Mon. 2 / 11 / 2015
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2015 – 2016
STOMA Dr. Tariq Al-Obaidi
2-11-2015
2
STOMA
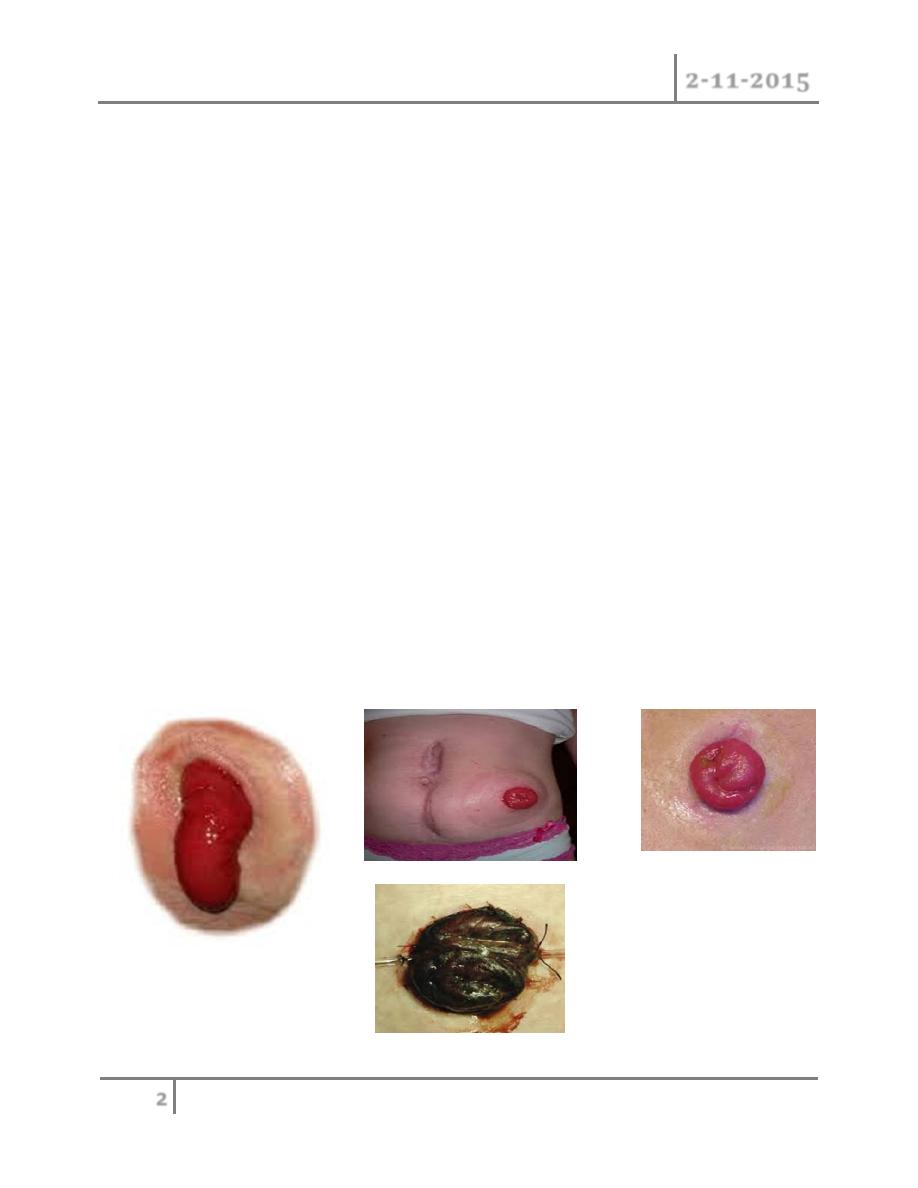
Complications of colostomy
1. Psychological trauma especially in the women and in the young age group
due to bad smell and sounds of air which is uncontrolled so need a medical
advise about the kinds of foods to prevent smell and sounds
2. Prolapsed
3. Retraction
4. Necrosis of distal end
5. Stenosis of the orifice
6. Colostomy hernia
7. Bleeding from the margin
8. Colostomy diarrhea, this is infective enteritis respond to treatment
Colostomy with complication can be reformed by operation.

STOMA Dr. Tariq Al-Obaidi
2-11-2015
3
Caecostomy
In disparately ill patient with advanced large bowel obstruction, a
caecostomy may be useful. In late cases of obstruction the cecum may
become so distended ans ischemic that rupture of cecal wall may be
distended.
This can occur spontaneously, giving rise to fecal peritonitis, or at
operation, when an incision in the abdominal wall reduces its supportive
role and allows the cecum to expand.
Direct suture to cecum is possible, resection of cecum by right
hemicoloectomy in bad injury or performing of caecostomy, which is a
temporary measure until the condition of the patient is improved then a
definitive procedure then performed.
Ileostomy
Artificial opening in the ileum and can be temporary or more common
permanent. The ileum should be brought through the lateral edge of rectus
abndominis muscle.

STOMA Dr. Tariq Al-Obaidi
2-11-2015
4
Care of ileostomy :
During 1
st
few postoperative days the fluid electrolyte balance must be
adjusted with great care. The fluid of ileostomy is irritant and contain
pancreatic juice which cause severe skin inflammation.
Indication
In case of total colectomy as in ulcerative colitis, rest of inflammatory
process in ulcerative colitis and diverticulitis in fulminant phase as
temporary ileostomy, in traumatic injury to the bowel.
Closure of colostomy
In temporary colostomy closure should be done in 2 moths of previous
operation provided that there is no distal obstruction and distal anastomosis
is healed.
The patient should be admitted to the hospital 5 days before closure with
encouraging fluid diet and use laxatives drug and antibiotics in form 3
rd
generation cephalosporin and metronidazole and this called chemical
preparation and the use of frequent enemas to clean the distal bowel called
mechanical preparation.
Mannitol solution can be used with caution in fear of dehydration. Ba-
enema should be done before operation to ensure there is no distal
obstruction.

STOMA Dr. Tariq Al-Obaidi
2-11-2015
5
In summary
May be colostomy or ileostomy
May be temporary or permanent
Temporary or defunctioning stomas as loop stoma
An ileostomy is spouted , a colostomy is flushed
Ileostomy effluent is usually liquid where colostomy is usually solid
An ileostomy patients more likely to develop electrolyte problems
An ileostomy is usually sited in right iliac fossa while a temporary colostomy
may be transverse colostomy sited in right upper quadrant
End colostomy is usually sited in left iliac fossa
All patients should be counselled by a stomas care nurses before operation
Complications include skin irritation, prolapse, retraction, necrosis,
parastomal hernia, bleeding and fistulation.
#END
Done by
Ali Kareem