Dr. Nadia Aziz
F.A.B.C.M , Lecturer
community medicine department

1-Define what is meningitis
2-Types of meningitis
3-Identification of meningococcal meningitis,
the diagnosis, its occurrence & ways of
controlling this disease.
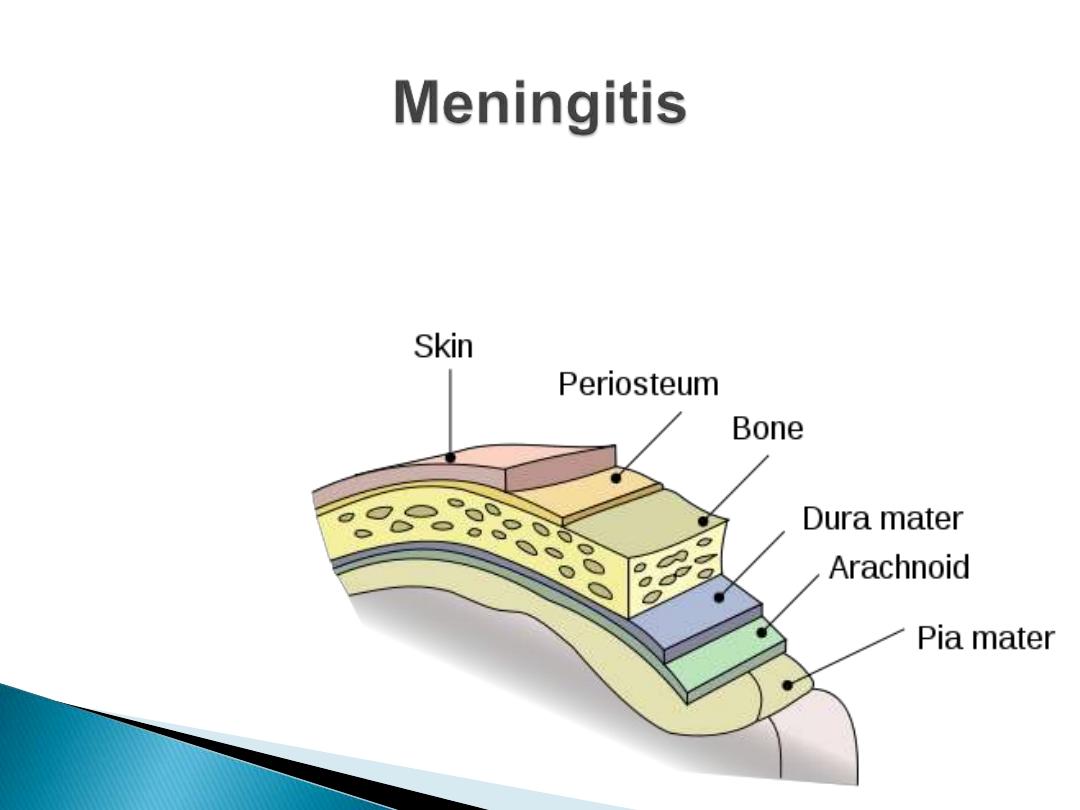
Is an inflammatory process of liptomeninges
and the CSF

1- Acute pyogenic (
bacterial
) meningitis
2-Acute aseptic (
viral
) meningitis
3-Acute
focal
suppurative infection (brain
abscess, subdural and extradural empyema)
4-
Chronic bacterial infection
(tuberculosis)
1-
Neisseria meningitidis
2-
Streptococcus pneumoniae
and
3-
Haemophilus influenzae type b
(Hib)
Constitute more than
75%
of all cases of
bacterial meningitis in most studies, and
90%
of bacterial meningitis occur in children
.
An acute bacterial disease, characterized by:
Sudden onset of
fever
intense
headache
nausea
and
vomiting
stiff neck
and photophobia
A
petechial rash
with pink macules may be
observed.

With antibiotics, intensive care units and
improved supportive measures have
decreased but it remains high at
8%
–15%.
long-term sequelae :
10
–20%
of survivors will suffer
mental
retardation
,
hearing loss
and
loss of limb use
.
1-
Meningitis
(the
most common
presentation)
2-
Bacteremia
and
3-
Sepsis
Meningococcaemia
is the
most severe
form of
infection with petechial rash, hypotension,
disseminated intravascular coagulation and
multiorgan failure.
Other forms of meningococcal disease such as
pneumonia, purulent arthritis, and
pericarditis are less common.
1-
CSF
or
blood culture
: Isolation of meningococci
from a sterile site CSF or blood (
gold standard
).
The sensitivity of culture, especially in patients
who have received antibiotics, is low.
2-
Latex agglutination test
: Identification of
group-specific meningococcal
polysaccharides
in
CSF by latex agglutination in culture-negative
cases
3-
Polymerase chain reaction
: detecting
meningococcal DNA in CSF or plasma and
not
requiring live organisms
is of help but false-
negative results are common.
4-
Gram-stained smears
from petechiae: may
show Neisseria.
Neisseria meningitidis, the meningococcus, is a
Gram-negative
,
aerobic diplococcus
. Neisseria
are divided into serogroups according to their
capsular polysaccharide. Group A, B, and C
organisms account for at least 90% of cases,
although the proportion of groups Y and W135
and X is increasing in several regions.
In Europe and North America the incidence of
meningococcal disease is higher during
winter
and
spring
In Sub-Saharan Africa (African meningitis belt)
the disease classically peaks during the
dry
season

Infants
have the highest risk of
meningococcal disease.
Rates of disease decrease after infancy and
then increase in
adolescence and young
adulthood.
In addition to
age
, other risk factors include
underlying immune deficiencies
, such as
asplenia, properdin deficiency.
Crowding
,
low socioeconomic status
, active or
passive
exposure to tobacco smoke
and
concurrent
upper respiratory tract infections
In
some countries
males
are at higher risk than
females
Reservoir: Humans.
Mode of transmission
Direct contact
, including respiratory droplets
from nose and throat of infected people
Up to
5%
–10%
of people may be
asymptomatic
carriers
with nasopharyngeal colonization by N.
meningitidis.
2 to 10 days, commonly
3
–4
days.
Until live meningococci are no longer present
in discharges from nose and mouth.
Meningococci usually
disappear from the
nasopharynx within 24 hours
after institution
of antimicrobial treatment to which the
organisms are sensitive.
Susceptibility to the clinical disease is low and
decreases with age; this induces a high ratio of
carriers to cases.
Persons
deficient in certain complement
components are especially prone to recurrent
disease;
splenectomized persons
are susceptible
to bacteraemic illness.

A. Preventive measures
1)
Educate
the public on the need to reduce
direct contact and exposure to droplet infection.
2)
Reduce overcrowding
in living quarters and
workplaces, barracks, schools and ships.
3)
Vaccines
containing groups A, C, Y and W-135
meningococcal polysaccharides are been
available
Two polysaccharide vaccines:
1-
Quadrivalent
ACYW-135 vaccine
2-
Bivalent
AC Polysaccharide meningococcal
vaccines against serogroups A and C are safe
and effective in adults and children over 2, but
do not elicit long-term protection.
Vaccines are effective for:
1-
outbreak control
2- prevention among
high-risk groups
, such as
travellers
to countries where disease is epidemic,
Hajj pilgrims, military groups, and individuals
with
underlying immune dysfunctions
.
Because these vaccines are often
poorly
immunogenic
in young children and have
limited
duration of efficacy
, they are not
generally used in routine childhood
immunization programs.
1) Isolation:
Respiratory
isolation for 24 hours after
start of treatment.
2) Protection of contacts: Close
surveillance
of
household, daycare, and other intimate contacts
for early signs of illness, to
initiate appropriate
therapy without delay
prophylactic
administration of chemotherapeutic
agent to intimate contacts
Younger children in
day care centers
, even if
not close friends, should
all
be given
prophylaxis after an index case is identified
1-
Rifampicin
Twice daily for 2 days
: adults 600 mg per dose;
children over 1month old, 10 mg/kg
2-
Ceftriaxone
For adults, 250 mg IM, given in a
single dose
, 125
mg IM for children under 15.
3-
Ciprofloxacin
500 mg PO, a
single dose
to adults.
Penicillin
given parenterally in adequate doses
is the
drug of choice
Ampicillin
and
chloramphenicol
are also
effective.
Ceftriaxone
Ciprofloxacin
Penicillin-
resistant
strains have been reported in
many countries,
strains resistant to chloramphenicol also have
been reported.
Treatment should start as soon as the
presumptive clinical diagnosis is made
, even
before menin-gococci have been identified.
In children, until the specific agent has been
identified, the drug chosen must be effective
against Haemophilus influenzae type b
(Hib)
as well as
Streptococcus pneumoniae
.
1) When an outbreak occurs, major emphasis
must be placed on:
Careful surveillance
,
early diagnosis
and
immediate treatment
of suspected cases.
Thresholds
(alert and epidemic)
When thresholds are passed,
immunization
campaigns must be implemented.
1) setting up an epidemic management
committee
,
enhancing surveillance, undertaking
field
epidemiology
and
bacteriological investigations, ensuring supplies
of drugs and laboratory material
mass vaccination
2)
Reduce overcrowding
and ventilate living and
sleeping quarters
3) Intimate contacts should all be considered for
prophylaxis
4) The use of
vaccine in all age groups
affected
is strongly recommended if an
outbreak occurs in a large institutional
or community setting

Thank you
&
Good luck