
THE BURDEN OF CANCER IN
BASRAH
THE STATE OF THE AR T
-First Report-
Omran S. Habib
Jawad K Al-Ali
Mohammed K. Al-Wiswasi
Narjis AH Ajeel
A report compiled in collaboration with the following institutions :
Cancer Research Unit (CRU), College of Medicine. University of Basrah
Cancer Registration Section ( CRS), College of Medicine, University of Basrah
The Oncology Centre (OC), Al-Sadr Teaching Hospital, Basrah
Cancer Control Centre (CCC), General Directorate of Health, Basrah
Oncology Ward, Basrah Maternity and Child Hospital, Basrah
Basrah October 2006

٢
THE BURDEN OF CANCER IN
BASRAH
THE STATE OF THE AR T
Edited By
Omran S. Habib
(Ph.D.), Professor of Epidemiology and Health Care,
and Director of Cancer Research Unit, Department of Community Medicine
College of Medicine, University of Basrah
Jawad K Al-Ali
(MRCP), Consultant Physician and Oncologist, Al-Sadr
Teaching Hospital, Basrah.
Mohammed K. Al-Wiswasi
(Ph.D., FRC.Path), Assistant Professor,
Department of Pathology and Forensic Medicine, College of Medicine,
University of Basrah
Narjis AH Ajeel
(Ph.D.), Professor of Community Medicine and Head,
Department of Community Medicine, College of Medicine, University of Basrah
Copyright©2006 Habib et al. No part of this document is abstracted,
reproduced or translated in part or in whole without prior permission of
the editors and clear reference to the report as a source document.
Contributors to the data base and contents of this report

٣
A. Chief contributors and editors
1. Omran S. Habib
(Ph.D.), Professor of Epidemiology and Health Care, Department of
Community Medicine, College of Medicine, University of Basrah.
2. Jawad K Al-Ali
(MRCP), Consultant Physician and Oncologist, Al-Sadr Teaching
Hospital, Basrah.
B. Other contributors
1. Mohammed K. Al-Wiswasi (Ph.D., FRC.Path), Assistant professor and Head,
Department of Pathology and Forensic Medicine, College of Medicine, University of Basrah
2. Narjis AH Ajeel (Ph.D.), Professor of Community Medicine and Head, Department of
Community Medicine, College of Medicine, University of Basrah
3. Jasim MA AL-Diab, (FIBMS Path.), Assistant Professor, Department of Pathology and
Forensic Medicine, College of Medicine, University of Basrah
4. Kareem AS Al-Imara (DCM). Specialist in Community Medicine, General Directorate of
Health Service, Basrah
5. Janan G Hasan (ACPP), Assistant professor and Paediatrics Oncologist, College of
Medicine, University of Basrah
6. Khajak Vartanian (MSc) Physicist, Directorate of Environment, Basrah
7. Asaad AA Khalaf (FIBMS), Internist and Medical Oncologist, Al -Sadr Teaching Hospital
Basrah.
8. Osama G. Al-Asady (FICMS), Internist and Medical Oncologist, Al -Sadr Teaching
Hospital, Basrah
9. Taha Y Mohammed (BSc). Directorate of Environment, Basrah
10. Janan B. Tooma (D.S.) General Surgeon, Breast Cancer Early Detection Centre, Al -Sadr
Teaching Hospital, Basrah
11. Anmar A Mohsin (FACMS)) Internist and Medical Oncologist, Al -Sadr Teaching
Hospital, Basrah
12. Jawad K Hassan (Ph.D.), Department of Pharmacology , College of Medicine, University
of Basrah
13. Hussain H. Jasim (MSc.) Histopathology). Basrah General Hospital
14. Zeki AJ Al-Faddagh ( ABMS ) Professor of Surgery, Department of Surgery, College of
Medicine, University of Basrah
15. Abbas ZM Al-Mayah , Medical Assistant and Registration Officer, The Oncology Centre,
Al-Sadr Teaching Hospital, Basrah
16. Sajjad S. Essa (M.B.Ch. B.). Postgraduate student, Iraqi Board of Medical
Specializations.
C. Technical and statistical Contribution
1. Asaad Q Al-Yassen (MSc). Assistant lecturer, Department of Community Medicine,
College of Medicine, Basrah
2. Tariq OS Habib (BSc Computer Science). Programmer. Cancer Research Unit, College of
Medicine, University of Basrah
PREFACE

٤
Planning as a process of identification of problems and priorities, setting
objectives, exploring and selecting strategies and implementing the most rele vant
programmes, is a scientific and systematic process. At each and every stage of
the process, sound and reliable data are needed. This is certainly the case for
effective handling of any significant public health problem. Therefore, the
handling of the problem of cancer in Basrah must start with the creation of an
effective mechanism to collect, analyze and present reliable indicators on
incidence, distribution ,
determinants and fatality of cancer.
Sporadic,
disintegrated and ad hoc works are beneficial by themselves but can not
guarantee continuity and comprehensiveness of long standin g programmes to
deal with such potentially growing health problem. Multidisplinary,
multisectorial approach with sustainable mechanisms is the only rational and
fruitful way to succeed in this context. The success of all proposed activities is
also dependent on the successful "cultivation" of the spirit of team work and
the recognition by all partners of the value of multidisciplinary approach to
problem solving. Without these prerequisites, nothing significant is expected to
be achieved and most efforts will remain turmoiling in a vicious circle.
This report is the first scientific document of a team work research initiated in
Basrah to deal with cancer. The project was endorsed by the Iraqi Ministry of
Health (Appendix 1). The team members hope that the contents and the spirits of
the work will encourage further steps towards the ultimate aim of creating an
effective and reliable cancer registry in Basrah or Southern Iraq . The figures
contained in the report refer to two separate research activities. In t he first all new
cancer cases diagnosed in Basrah during 2005 were included. The results
covering new cases are amenable to rectification in the future if more cases
related to 2005 are identified. We do believe however, that the figures given in
this report represent the best epidemiological profile of risk of cancer in Basrah
in 2005. The second research is on cancer related mortality in Basrah during three
years 1989, 1997 and 2005.
Results related to incidence and mortality are presented as frequencies , relative
frequencies, specific incidence rates, specific mortality rates and time trends. An
attempt was also made to calculate survival rates. The bulk of the results is
included in Section 4) Additional results are given in Appendix 2. No rigorous
interpretation of the results is attempted. Instead we
present available facts as
they are at the present stage of the project. Making sound conclusions about the
changing pattern of cancer in Basrah and any determinants requires further
efforts and more valid data. However, this does not undermine the efforts made
to prepare this report or to believe that the data on which the report is based are
not valid. It is rather a warning to any one who may make some faulty judgment
about cancer in Basrah. The authors still believe that there are some gaps in the
data base of cancer and these gaps, though might be small, they are necessary to
complete the epidemiological picture.
ACKNOWLEDGEMENTS

٥
The editors express their gratefulness to every member of the research t eam, who
worked in calm but in fruitful manner, to the members of the consulta tion team,
to all colleagues who support and/or contribute morally to the work.
Professor Thamer A. Hamdan, Dean of College of Medicine deserves special
thanks for his scientifi c and administrative support to the project and his strong
stance in favour of creating schools of thought . He and his colleagues in the
orthopedic department deserve high degree of respect
Special appreciation is also made of the active contribution from Dr. Yousif
Gague of the faciomaxilary department in Basrah general hospital and to Dr
Muayad Al-Rubaie, Director of Al-Sadr Teaching hospital who took a positive
stance from the project.
Dr Wasan Al-Elwe, pathologist, Al-Sadr Teaching hospital is a faithf ul
enthusiastic person without her hard work, good part of the data could not be
easily compiled.
We are very grateful to our friends from Japan . Dr. Katsumi F and from Germany
Professor Wolfgang Hoffmann - University of Griefswald , Professor Eberhard
Grieser of Bremen University. Dr. A. Clausen of IPPNW -Germany and Dr.
Claudia Terschuren – Griefswald University who provided tangible scientific,
technical and moral support to the project.
The authors are grateful to the members of the Cancer Research Unit, College of
Medicine for their support to the work and cooperation with the research team.
Cancer patients and their families are the people for whom the spirit of this work
is dedicated. We wish every one safe life and healthy living until the final norma l
destiny.
Finally, the editors are grateful to Dr. Asaad Q Al -Yassen for his assistance in
editorial aspects of the report and to Tariq OS Habib for his hard work in
handling, checking, statistical assistance and typing of the manuscripts.
The Editors
Basrah, October 2006

٦
1. BACKGROUND OF THE LOCAL
SITUATION
Cancer is a growing problem world - wide
(1)
. Despite the great advances in
science and technology, the aetiology of many types of cancer is still obscure and
the role of specific risk factors in the causation of certain cancers is unresolved
with substantial variation across the world
(2,3)
. The distribution of almost all
diseases including cancer is not random neither across nations nor within
individual nations, yet in many instances, the re asons behind such non -
randomness are not always clear and the exact nature of geographical variation is
hazy
(4).
Iraq as whole and the southern region including Basrah in particular has
been subjected to massive environmental damage as consequences of war s,
economic embargo and lack of resources to protect or restore safe environment.
As a result, the health status of the population was under high risk of various
diseases including cancer. A number of researchers carried out research work on
cancer incidence and mortality during the last ten years and reported some
increase in both of these two indicators
(5-7)
. However, these research works have
been under criticism by local researchers
(8)
and international Authors
(9)
for
possible bias in their results. The critics suggest that the apparent increase could
have been artificial due to better diagnosis, improved reporting and registration or
the rise reflects changes in population size and age structure. Regardless of
whether this apparent increase in risk of cancer in Basrah is real or artificial, the
reported cases do not represent the true situation. At any previous year, case
detection and registration is incomplete and fluctuating despite the initiation of
official cancer registry in Basrah for more tha n a decade. From one point of view,
many cases from inhabitants of Basrah may consult sources of care outside
Basrah and are not registered with registration centres in Basrah at all. From the
other point of view, a number of registered cases, though small , are not
inhabitants of Basrah governorate. In addition, the population denominators are
likely to have some errors partly because of population movement during the last
20 years or so. In the last three years, the situation became more complicated ,
when many of the expatriated Iraqis returned to the country. Their exact numbers
might be very difficult to determine. Such complicated situation with the added
security issues makes research a real adventure. In an attempt to improve the data
base on cancer in Basrah, to estimate the risk of cancer and to enhance better
health care for people at risk of cancer, a study plan was prepared
(10).
This plan
was then modified when a team of researchers from medical and related
specialties initiated a FOUR-LEGGED PROJECT.

٧
The four-legged project consists of
1. Measurement of environment pollution and mapping of major pollutants
with specific emphasis on pollution with radioactive matters like depleted
uranium.
2. Improvement of cancer registration and creation of population-based
cancer
data base (Population-based cancer registry.
3. Research to measure the extent of cancer in terms of incidence and
mortality
and to ascertain the relationship of cancer to possible risk
factors including
exposure to radioactive material.
4. Improvement of
care provided to cancer patients at the level of structure
(resources) process
(investigation and treatment techniques) and outcome
(better survival and
quality of life).
2. PRACTICAL ACTIVITIES DURING 2005
Apart from efforts made during the last ten years by local care providers, local
health authorities and a number of international NGOs to improve care for cancer
patients, the following practical activi ties took place
Activity One
A ten-day seminar (Health and environment in post war Iraq) was held in
Amman (Feb. 7-17, 2005) with support from DAAD , IPPNW, University of
Bremen and University of Greifswald. Nine scientists from Basrah participated in
this seminar. The seminar was a good opportunity to exchange information and
expertise about cancer and environment pollution and to set the first significant
step towards cancer registration and research in Basrah.
Activity Two
A number of scientific acti vities were carried out in Basrah (Lecture to faculty of
Basrah Medical College, Report to the University of Basrah and a one -day
seminar (19 April 2005) by the research team. The main question asked : What
can we do about cancer in Basrah? The participant s agreed on the following
points:
1. During the last 20 years, extensive environmental damage took place in Iraq
and Basrah in particular.
2. Such damage is likely to be associated with risk to health and life of people .
Cancer is one important health prob lem.
3. The extent of pollution, cancer and the relationship of the two to each other is
not well understood and defined.
4. The participants agreed that individual research activities are ineffective .
Multidisciplinary teamwork is highly recommended

٨
5. The participants agreed to take part in a " FOUR-LEGGED PROJECT" as
researchers, consultants or co -coordinators in the project.
Activity Three
A full proposal covering the short term objectives of the four -legged project was
prepared and submitted to the M inistry of Health and Ministry of Environment. A
positive response and official endorsement was issued by the Ministry of Health
on December 11, 2005. No response yet was obtained from the Ministry of
Environment. A good support for the project is being given by Basrah
Environmental Office. Two of their staff are members in the research team. The
endorsement of the Ministry of Health made the project under official legal
cover. The project is also supported by the Medical College and University of
Basrah who facilitated the participation of research team in all the activities
inside and outside Iraq.
Activity Four
Initiation of Cancer Registration Section at the Department of Pathology and
Forensic Medicine, College of Medicine, University of Basrah. This s ection is
supervised by a committee of histopathologists. It aims at registering every case
of cancer diagnosed histopathologically and/or cytologically in Basrah. It records
minimum items of information.
Activity Five
Two review papers were prepared on c ancer and environment in Basrah.
1. Khalaf AA. Cancer trends of cancer after Gulf War . Clinical Medicine in
Tomorrow 2005; 17: 3-11.
2. Habib OS.
Environment and health in Southern Iraq: Facts and future
prospects. Marina Mesopotamica 2006; 20:7-19.
The research team initiated immense activities during 2005 to improve conduct
and outcome of cancer registration in Basrah . Coordinated work among five
major partners took place despite the many constraints facing us . The five
partners are:
1. The Cancer Registry at the Directorate General of Health in Basrah
2. The Cancer Registration Section at the Department of Pathology and
Forensic Medicine, Basrah College of Medicine.
3. The Oncology Centre at Al -Sadr Teaching Hospital
4. The Oncology Ward at Basrah Maternity and Children Hospital
5. The Department of Community Medicine , Basrah College of Medicine
The collaborative work yielded substantial results on cancer identification,
registration and analysis. The Cancer Registrat ion Section published a report on
its activity during 2005. More scientific work is going on .

٩
3. PRACTICAL ACTIVITIES DURING 2006
Activity One:
A seminar (Cancer Registration and Environmental Health Risk Assessment
for the Population: Methods, Imp lementation and Analysis) was held at the
Institute of Community Medicine , University of Greifswald Feb 19-28 with the
participation of 14 Iraqi scientists of different medical biological and physical
specialties. The seminar was backed by highly speciali zed staff from Germany,
Japan And Basrah (Iraq). The seminar was funded by The German DAAD and
IPPNW. The seminar was planned for in a meeting held in Amman between two
German and two Iraq scientists on November 14m, 2005.
Activity Two
One –day seminar in Basrah (March 27, 2006) was organized by the research
team in collaboration with the College of Medicine. Fifty doctors of various
specialties were invited to participate in the seminar. Three storming questions
were raised in the seminar:
1.
Do you believe that cancer has increased in Basrah during the last 10
years or so? What is the evidence for your answer ?
2.
If cancer is really increasing in Basrah , how can you ascertain this
increase? How can you identify the causes for such increase ?
3.
If cancer is not increasing, how can you explain the rise in registered cases
for example from
488
in 1990 to
1604
in 2005 or by about 228%?
At the end of the seminar, the Dean of Basrah Medical College and other senior
doctors from the attendant s appraised the work and proposed the initiation of
"Cancer Council" in Basrah governorate. An expert meeting was held next day
and two more activities were decided :
1. Another broader seminar is to be held later ( May 28
th
, 2006). In this seminar,
local experience with cancer and difficulties are to be presented by various
medical specialists and a working paper (Cancer and cancer registration in
Basrah: Where we are now and where to go next ?) is to be presented for
discussion.
2. A conference is to be held late in 2006 or early 2007, but this depends on
security issues and financial support from local and international partners .
Activity Three
1. The coordinated work among the five partners mentioned above is continuing
at least at the level achieved during 2005

٠١
2. Three scientific research works are underway. They are under the supervision
of the Department of Community Medicine, College of Medicine, and University
of Basrah in collaboration with the research team. All are planned to be
preliminary studies The three studies are:
a. Breast cancer and life style risk factors: A case -Control study.
b. Risk factors of childhood cancer (leukaemia and lymphoma) in Basrah
c. Analysis of cancer mortality in Basrah: A record –based study
Activity Four
A one-day seminar under the slogan "The control of cancer contributes to better
health" is planned to be held on May 28
th
, 2006. The seminar aimed at providing
the opportunity for different medical specialists from Basrah to present their
experience with cancer and the difficulties they face in their work. A working
paper was put for discussion.(See Appendix 3) It was envisaged from the
proceedings and discussions that participants would approve a strategy to deal
with cancer in accordance with the four -legged project. At least three disciplines
showed material support by sending short forms on cases of cancer diagnosed by
them. These three disciplines are the orthopaedic surgeons group, the
neurosurgeons group and the faciomaxilary surgery group
4. CANCER IN BASRAH: EXTENT OF THE
PROBLEM
4.1. Sources of data and methods
The results presented in this paper are based on all cases of cancer which were
diagnosed by histopathologists or haematologists in Basrah during 2005 and
registered with the following instit utions:
a. The Oncology center in Al -Sadr Teaching hospital, which is the main centre
for registration of cases and administration of cytotoxic chemotherapy in
southern Iraq.
b. Cancer registration section at the Department of Pathology and Forensic
Medicine, College of Medicine. This section compiles the great majority of
cancer cases which are diagnosed by histopathological methods.
c. Pediatrics' Oncology Ward in Basrah maternity and child hospital, which is
responsible for the treatment of childhood m alignancies.
d. Other sources. Some specialist doctors keep their own collection of cancer
cases as part of their own routine clinical work. They were contacted and
requested to provide a list of their cases. The main contributors in this aspect are
orthpaedic surgeons, faciomaxilary surgeons and neurosurgeons .
All these sources are now cooperating with each other and with the research
team to improve cancer detection and registration in Basrah. Lists obtained from
various sources were typed first on an excel sheet. They were matched and

١١
checked for any repetition resulting from cases being reported by more than one
source. The data were then transmitted into An SPSS (Statistical Package for
Social Science) computer file for statistical analysis. Two points are stressed
here. The first is that we do not claim that the results presented in this report
represent all cases of cancer in Basrah governorate. Rather we can claim that they
represent the best achievement so far in this respect. The second is th at the
registered cases are derived, in principle, from the inhabitants of Basrah, but
some of them are inhabitants of other governorates who are diagnosed and or
treated in Basrah. Great efforts were made to identify each and every case
regarding the exact place of residence. However, misclassification can not be
totally excluded. To compare time trends of registered cancer cases we used
cases diagnosed and registered with the Cancer Registration Section at the
Department of Pathology and Forensic Medicine during the years 1990, 1997,
1999 and 2005. Until the end of 2005, the records of this section did not
distinguish cases by place of residence and consistently registered cases from
within and from outside Basrah governorate. The restriction of cases used in the
time trend analysis to this source was based on two assumptions:
1. The data for the four years are comparable with respect to criteria of diagnosis
and extent of coverage.
2. The proportion of cases from outside Basrah is small and does not vary from
year to year.
Estimation of epidemiological indicators of the extent of risk of cancer (age
specific, sex specific, area specific incidence rates and other indicators) in Basrah
governorate for the year 2005 was based on data available for 2005 from all
sources after exclusion of cases from outside the governorate. The total cases
registered with the Cancer Registration Section for the years 1990, 1997, 1999
and 2005 were 488, 544, 688 and 1327 in that order. These cases were used only
once to describe the time trend as mentioned earlier. The total number of cases
registered with all sources including the Cancer Registration section in 2005 was
1885 cases. It was possible to classify these
cases into those who were
inhabitants of Basrah governorate ( 1604 cases) and those who were inhabitants of
other governorates (281 cases). The 1604 cases were used to estimate indicators
of the extent of risk in Basrah in 2005.
Information related to population of Basrah were based on data available with
Basrah Health Authorities, the electorate lists and the Statistical Office in Basrah
(11).
The age structure was based on pooled results of 10 household surveys carried
out in different parts of Basrah governorate during the last 12 years
(12-13).
Regarding cancer deaths, data were compiled from all records of deaths in the
city centre and other administrative units. The data on deaths related to cancer
were obtained for three years ; 1989 a relatively normal year for Basrah following
the cessation of the Iraq -Iran war, 1997 the year which represented the end of the
severest economic embargo (before the oil for food memorandum) and 2005
when economic embargo is no longer existing. The process of data compilation
was labourious. It required the examination of available data on every death to

٢١
identify cases for which the cause of death was written as cancer . Two sources
for data on death are available in Basrah: death certificates and death registries
(death inventories). The two sources generally contain the sam e range of
variables on each case (Name, age at the time of death, sex, place of residence,
date of death, cause of death and place where death was certified). In this study
we used death registries and discard the use of death certificates for major
missing and deficiencies. The total number of deaths (all causes of death) for the
three years 1989, 1997 and 2005 were obtained, together with available data on
each and every case for which cancer was written as the cause of death were
compiled. .
Despite all efforts made to obtain as accurate data as possible on cases, deaths
and denominator population, we can not claim perfectionism at all. Some
margins of error do exist. Some cases are not compiled in our data base, fewer
deaths are also likely to hav e been missed and the exact number of population is
not totally ascertained. Nevertheless, we are confident that the figures reported in
this report are the best epidemiological estimations at this stage of work.
For the purpose of geographical dis tribution, the system used by the health
authorities in which Basrah governorate is divided into Health Sectors, which
with specified services and populations . The geographical areas (Administrative
areas) are: Basrah city, Northern Area (Qurna, Mdaina and Hartha), Western
Area (Zubair district inclusive of Safwan and Um -Qasr), Southern Area (Abul -
Khasib and Fao districts) and Eastern Area (Shatt AL -Arab district).
4.2. Cancer incidence in Basrah 2005
Incidence and incidence rates are useful epidemiologic al parameters to estimate
the risk of acquiring cancer for the whole population and for subsets of it. This
parameter is influenced by variation in exposure to various risk factors and
aetiological agents in the surrounding environment, host factors and th e nature
and carcinogenicity of the causes. The estimation of the incidence rate is also
affected by the completeness and accuracy of case detection and recording as
well as by the accuracy of population (denominator) estimation. The results
reported in the following sections are by no means immune against all these
potential sources of error. They represent, in the viewpoint of the authors, the
best available epidemiological estimates for the year 2005. They are inclusive of
cases diagnosed in 2005 and validated up to the end of September 2006. The
numbers are moving numbers. They are amenable to change in the future if more
cases are identified and verified as cases which belong to the year 2005.
Distribution of new cases by sex and type of cancer
Table 4.1 shows the distribution of new cancer cases reported in Basrah
governorate during 2005 classified according to sex and type of cancer. Over all,
45.7% are male cases and 54.3% are female cases. The five leading cancers are
٣١
those of breast (17.6%), urinary bladder (6.7%), Lymphomas (Hodkins and Non -
Hodkins: 6.4%). Skin (6.1%) and lung (5.5%). The five leading cancers in males
and females are different . For males these are urinary bladder (10.8%),
lymphomas (9.7%), lung (8.7%), skin (7.4%) and larynx (6.5%). For females,
breast cancer form just under one third of all cancers in women (31.7%),
followed by cancers of uterus &cervix (5.5%), skin (5.1%), ovary (4.9%) and
colon-rectum (4.2%). Among the major cancers which are relatively more among
males are cancer of the urinary bladder, lymphomas, Skin, lung, larynx,
leukemia, pharynx and soft tissue. Cancers which are relatively more common
among females are those of the breast and thyroid gland.
Annual cancer specific incidence rates
Table 4.2 summarizes the annual incidence rates of different cancers in Basrah
governorate. For all cancers together, the annual incidence rate is 74.3/100 000.
Breast cancer shows the highest annual incidence rate in Basrah in 2005
(13.1/100 000). Other important cancer are tho se of urinary bladder (5.0/100
000), Lymphomas both Hodgkin 's and Non-Hodgkin's (4.8/100 000), skin
(4.5/100 000) and lung (4.1/100 000). Less frequent are leukemia (3.2/100 000),
cancer of colon-rectum (3.2/100 000) cancer of larynx (3.1/100 000), cancer of
stomach (2.8/100 000) and soft tissue tumours (2.7/100 000). These ten leading
cancer account for about 46.5/100 000 or 62.6% of the over all risk of cancer in
Basrah in 2005.
Table 4.1: Distribution of new cancer cases in Basrah 2005 by type of cancer
and sex
Type of cancer
Males
No. %
Females
No. %
Total
No. %
Breast
Urinary bladder
Lymphomas
Skin
Lung
Leukaemia
Colon-rectum
Larynx
Stomach
Soft tissue
Other lymphoid cancer
Uterus &cervix
Bone
Ovary
Pleura
CNS
Peritoneum
Thyroid gland
6
0.8
79
10.8
71
9.7
54
7.4
64
8.7
36
4.9
31
4.2
48
6.5
31
4.2
39
5.3
28
3.8
-
0.0
24
3.3
-
0.0
18
2.5
17
2.3
11
1.5
6
0.8
276
31.7
28
3.2
32
3.7
44
5.1
24
2.8
32
3.7
37
4.2
18
2.1
29
3.3
19
2.2
21
2.4
48
5.5
22
2.5
43
4.9
15
1.7
13
1.5
18
2.1
23
2.6
282
17.6
107
6.7
103
6.4
98
6.1
88
5.5
68
4.2
68
4.2
66
4.1
60
3.7
58
3.6
49
3.1
48
3.0
46
2.9
43
2.7
33
2.1
30
1.9
29
1.8
29
1.8
٤١
Pharynx
Liver
Kidney
Prostate
Pancreas
Secondary
Parotid gland
Testis
Bone marrow
Retroperitoneal
Choriocarcinoma
Nose
Oral cavity
Gall bladder
Intestine
Abdomen
Vulva/vagina
All others
21
2.9
13
1.8
11
1.5
21
2.9
8
1.1
12
1.6
7
1.0
11
1.5
7
1.0
4
0.5
-
0.0
6
0.8
3
0.4
4
0.5
6
0.8
2
0.3
-
0.0
35
4.8
6
0.7
11
1.3
13
1.5
-
0.0
12
1.4
6
0.7
6
0.7
-
0.0
3
0.3
6
0.7
10
1.1
3
0.3
6
0.7
4
0.5
1
0.1
3
0.3
5
0.6
34
3.9
27
1.7
24
1.5
24
1.5
21
1.3
20
1.2
18
1.1
13
0.8
11
0.7
10
0.6
10
0.6
10
0.6
9
0.6
9
0.6
8
0.5
7
0.4
5
0.3
5
0.3
69
4.9
Total
733
100.0
871
100.0
1604 100.0
Out of grand total
45.7
54.3
100.0
Table 4.2: Reported cases of cancer (all types) in Basrah governorate in
2005: Incidence rates per 100 000 by type of cancer
Incidence rate
per 100 000
Percentages
No. of cases
Type of cancer
13.1
5.0
4.8
4.5
4.1
3.2
3.2
3.1
2.8
2.7
2.3
2.2
2.1
2.0
1.5
1.4
1.3
1.3
1.3
17.6
6.7
6.4
6.1
5.5
4.2
4.2
4.1
3.7
3.6
3.1
3.0
2.9
2.7
2.1
1.9
1.8
1.8
1.7
282
107
103
98
88
68
68
66
60
58
49
48
46
43
33
30
29
29
27
Breast
Urinary bladder
Lymphomas
Skin
Lung
Leukemia
Colon-rectum
Larynx
Stomach
Soft tissue
Other lymphoid cancer
Uterus &cervix
Bone
Ovary
Pleura
CNS
Peritoneum
Thyroid gland
Pharynx
٥١
1.1
1.1
1.0
0.9
0.8
0.6
0.5
0.5
0.5
0.5
0.4
0.4
0.4
0.3
0.2
0.2
3.2
1.5
1.5
1.3
1.2
1.1
0.8
0.7
0.6
0.6
0.6
0.6
0.6
0.5
0.4
0.3
0.3
4.9
24
24
21
20
18
13
11
10
10
10
9
9
8
7
5
5
69
Liver
Kidney
Prostate
Pancreas
Secondary
Parotid gland
Testis
Bone marrow
Retroperitoneal
Choriocarcinoma
Nose
Oral cavity
Gall bladder
Intestine
Abdomen
Vulva/Vagina
All others
74.3 (SIR=117.7)
100.0
1604
Total
Distribution of cancer by age and sex
A comparison of the relative frequency of cancer for age and sex for the year
2005 is shown in Table 4.3. The over all distribution for males and females is
similar. The relative frequency is lower in children and young adults and high for
older people. Up to the age of 34 years, the relative share of cases is generally
low and exhibit similar pattern for males and females. In children aged <15 years,
the percentage in males is higher (9.2%) than in females (6.1%). In the age
groups 15-54, the percentages are higher for females than for males. In ol der
people (55 years and above) the percentages are higher for males. The r elative
predominance of females in young and middle aged adults reflects the high
incidence of breast cancer among females in this time of life.
Table 4.3: Age and sex distribution of cases of cancer (all types) reported in
Basrah in 2005
Total
No
%
Females
No. %
Males
No. %
Age
42
2.6
78
4.9
78
4.9
24
2.8
29
3.3
50
5.7
18
2.5
49
6.7
28
3.8
<5
5-14
15-24
٦١
135
8.4
232
14.5
345
21.5
339
21.1
267
16.6
88
5.5
84
9.7
152
17.5
214
24.6
169
19.4
118
13.6
31
3.6
51
7.0
80
10.9
131
17.9
170
23.2
149
20.3
57
7.8
25-34
35-44
45-54
55-64
65-74
75 & above
1604
100.0
871
100.0
733
100.0
Total
F i g ure :R e la ti ve fre q ue nc y o f a ll c a nc e rs b y
a g e a nd s e x
0
1 0
2 0
3 0
1
2
3
4
5
6
7
8
9
A g e
%
To t a l %
F e m a le s %
M a le s %
This figure is based on data in Table 4.3
Age: 1=<5, 2=5-14, 3=15-24, 4=25-34, 5=35-44, 6-45-54, 7=55-64, 8=65-74, 9=75 and above
Age and sex specific Incidence rates of cancer
Table 4.4 shows the age and sex specific annual incidence rates of all cancers
reported in Basrah in 2005 for different age groups in males and females. In
children aged <5 years, the annual incidence rate is 13/100 000 for males and
17.6/100 000 for females. In older children (5-14 years), the annual incidence
rate is 17.2 and 10.5/100 000 for males and females respectively . In adults, the
annual incidence rate increases sharply with increasing age. Among males, it is
31.4 for those aged 15-44, 261.5 for those aged 45-64 and 660.2 for the elderly
aged 65 years and above. The corresponding figures for females in the same age
groups are 54.5, 361.1 and 390.7 per 100 000 in that order. Again the higher rates
among females in the age range 15-64 reflects the high risk of breast cancer in
this time of life. The over all incidence rate is 68.1/100 000 for males and
80.5/100 000 for females.
Table 4.4: Population of Basrah by sex and age, total cancer cases by sex and
age and annual incidence rates for the year 2005
٧١
Age (yrs)
Males
Population Cases IR
Females
Population Cases IR
<5
5-14
15-44
45-64
65&over
138790
18
13.0
285112
49
17.2
505670
159
31.4
115121
301
261.5
31201
206
660.2
136354
24
17.6
277037
29
10.5
524855
286
54.5
106054
383
361.1
37876
148
390.7
Total
1 075 894
733
68.1
1 082 176
871
80.5
Over all Standardized incidence rate using World Standard Population = 117.7/100 000
F ig u re : C a n c e r in c id e n c e ra te b y
s e x : B a s ra h 2 0 0 5
0
1 0 0
2 0 0
3 0 0
4 0 0
5 0 0
6 0 0
7 0 0
1
2
3
4
5
A g e
IR
/1
0
0
0
0
0
M a le s IR
F e m a le s IR
This figure is based on data in Table 4.4
Age: 1= <5, 2=5-14, 3=15-44, 4=45-64, 5=65 and above
Geographical (Spatial) distribution
Table 4.5 Shows the estimated annual incidence rates of all cancers for different
geographical areas in Basrah governorate in 2005. The highest incidence rate is
recorded in Western area (Zubair district: 80.0 per 100 000) followed by Basrah
city with a rate of 78.4 per 100 000, Eastern area (Shatt-Al-Arab district: 76.3 per
100 000), Southern area (Abul-Khasib district: 72.3 per 100 000) and the lowest
rate (65.3 per 100 000) is recorded in the Northern Area (Hartha, Qurna and
Mdainah).
Table 4.5: Annual incidence rates (per 100000) of all cancers in different
areas of Basrah in 2005
٨١
Area
Population
Registered
cases
IR/100 000
Basrah City
Northern Area
Western Area
Southern Area
Eastern Area
853484
609654
401481
195128
98323
669
398
321
141
75
78.4
65.3
80.0
72.3
76.3
Total
2158070
1604
74.3 (SIR= 117.7)
4.3. Cancer mortality in Basrah 2005
Mortality data are generally considered more accurate than incidence data
particularly in countries where official burial of the deceased requires legal
endorsement of death with specification of the cause of death. This is true in Iraq.
No dead person can be buried without official death certificate. Exceptions may
involve very few newly borne babies who may be buried without having official
birth and death certificates. Thes e cases are likely to have very li ttle effect on the
validity of mortality data related to cancer.
Type of cancer as a cause of death for 2005
Table 4.6 shows the frequency, relative frequency and the cause specific annual
mortality rates of cancer in B asrah governorate during the year 2005. Six groups
(cancers of lung, breast, urinary bladder, blood, lymphomas and CNS) account
for more than half of cancer related deaths (56.6%). Other significant
Contributors to cancer mortality are cancers of colon -rectum (4.3%), Liver
(4.2%), Stomach (3.7%), Bone (3.4%) and larynx (3.4%). All other cancers
Have lesser share in cancer relative contribution to mortality. Regarding the
annual mortality rate, the same order is seen. The cancer specific mortality rates
are generally lower than those reported in western countries and most of
developing countries. Some cancers (urinary bladder and lymphomas) show close
mortality rates to those in developing countries (See Tables 1.3 and 4.6)
Age and sex composition of cance r deaths in 2005
To compare the risk of death from cancer (All cancers together) between males
and females and for different age groups, age and sex specific death rates are
calculated and presented in Table 4.7. In general, age specific death rates are lo w
in children under 15 years of age and young adults aged 15-44 years with little
differences between male and female children . Young adult females aged 15-44
show some excess in the death rate (14.1/100 000) as compared to young adult
males of the same age range (8.9/100 000). Similar pattern is noticed in people
aged 45-64 years with a death rate of 116.9/100 000 among females compared to
103.4 /100 000 among males. Massive difference is observed between males and
٩١
females in the age group 65 years and above. The death rate among males is
439.0/100 000 compared to 285.1/100 000 among females. The excess among
women aged 15-64 may reflect the effect of breast cancer which is a leading
cause of death among women in this range of age. The decrease among female s
in the elderly age group is likely to reflect exhaustion of susceptible women and
increased risk of certain fatal cancers among elderly males.
Table 4.6: Relative frequency and annual mortality rates (All cancers) in
Basrah in 2005
Type of cancer
No. of deaths
Percentages
Death rate per
100 000
Lung & Bronchus
Breast
Urinary Bladder
Blood
Lymphomas*
CNS
Colon-rectum
Liver
Pancreas
Stomach
Bone
Larynx
Uterus
Secondary
Kidney
Prostate
Ovary
Skin
Oesophagus
Intestine
Gall bladder
Oral cavity
Nose
Pharynx
Thyroid
Abdomen
Penis
All other cancers
93
70
60
59
45
42
28
27
26
24
22
22
18
14
12
12
11
10
9
6
5
5
3
3
2
2
2
17
14.3
10.8
9.2
9.1
6.9
6.5
4.3
4.2
4.0
3.7
3.4
3.4
2.8
2.0
1.8
1.8
1.7
1.5
1.4
0.9
0.8
0.8
0.5
0.5
0.3
0.3
0.3
2.6
4.3
3.2
2.8
2.7
2.1
1.9
1.3
1.3
1.2
1.1
1.0
1.0
0.8
0.6
0.6
0.6
0.5
0.5
0.4
0.3
0.2
0.2
0.1
0.1
0.1
0.1
0.1
0.8
Total
649
100.0
30.1 (SMR=52.2)
* This may include few secondary lymphoretic s
٠٢
Table 4.7: Age and sex specific mortality rates (per 100 000): All cancers,
Basrah 2005
Age
(yrs)
Males
Population Deaths Rates
Females
Population Deaths Rates
< 1
1-4
5-14
15-44
45-64
65&over
31201
2
6.4
107589
4
3.7
285112
18
6.3
505670
45
8.9
115121
119
103.4
31201
137
439.0
30301
2
6.6
106053
5
4.7
277037
11
4.0
524855
74
14.1
106054
124
116.9
37876
108
285.1
Total
1 075 894
325
30.2
1 082 176
324
29.9
Over all standardized mortality rate using World Standard Population =
52.2
Geographical (Spatial) distribution of cancer deaths in 2005
Table 4.8 shows the population, annual number of deaths and mortality rates per
100 000 in each of the main areas in Basrah governorate . The highest mortality
rate (46.8) is recorded for the eastern area (Shatt -Al-Arab district) followed by
that for Basrah city (38.1), Western area (Zubair district) with a figure of 27.1
and Northern area with a rate of 22.1. The lowest rate for the southern area
(17.4). This spatial variation is rather difficult to explain. Differential exposure to
environmental risk factors can not be verified at this stage. Also, a margin of
error in both numerators and denominators is expected.
Table 4.8: Annual mortality rates (per 100 000) of all cancers in different
areas of Basrah in 2005
Area
Population
Annual
deaths
Death rate per 100 000
Basrah City
Northern Area
Western Area
Southern Area
Eastern Area
853484
609654
401481
195128
98323
325
135
109
34
46
38.1
22.1
27.1
17.4
46.8
١٢
Total
2158070
649
30.1 (SMR=52.2)
4.4. Time trends in incidence and mortality
Trends in incidence rates of cancer
To give crude estimates of the trend in cancer incidence rates in Basrah , we used
the data which were collected by the cancer registration section for the years
1990, 1997, 1999 and 2005 as mentioned in section 4.1 of this report. This
section collects data on solid tumours only ) Table 4.9 shows that the annual
incidence rate of solid tumours is more or less stable except a clear rise in 2005.
These results are very crude and can not be considered as representative of the
real situation in Basrah. They suggest some degree of rise in the risk of cancer
with time.
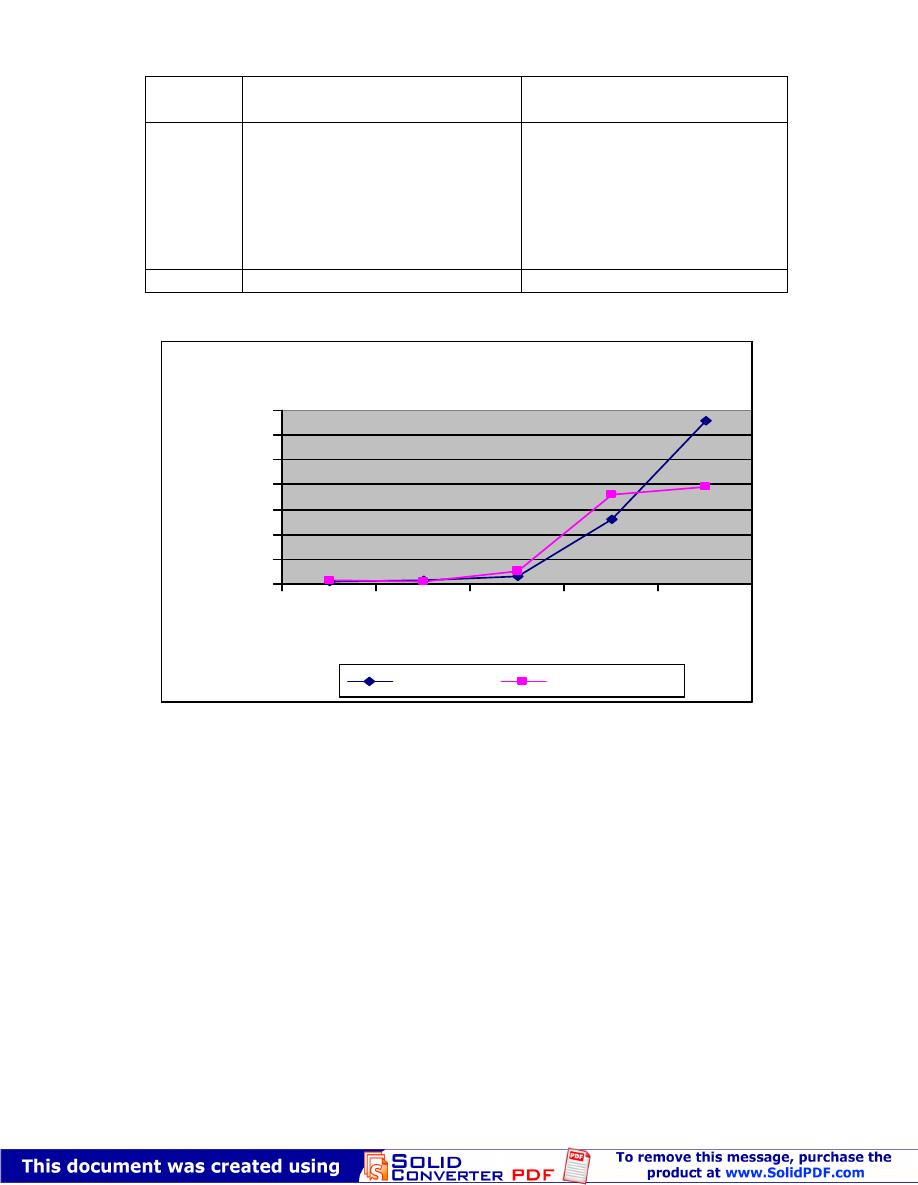
The rise in the incidence of cancer is clear , however, when a comparison is made
between cancer specific incidence rates for ten leading cancers for the years 1995
and 2005 in Table 4.10 (These two years were selected because of availability of
data on these ten cancers). It is very clear that the annual incidence rates for the
ten selected cancers are consistently higher in 2005 as compared to 1995. The
percentages of rise in the incidence rates range from 39.1% in case of leukemia to
227.1% in case of breast cancer. The change rise in the over all incidence rate
and in the incidence rates of selected cancers could reflect artificial rise due to
improved diagnosis, improved notification and recording of cases but part of this
rise is expected to reflect a real increase in the risk of cancer in Basrah .
Table 4.9: Total population, cancer cases (solid tumours) registered in the
Cancer Registration Section and estimates of annual incidence rates of all
solid cancers for selected years in Basrah governorate
Variable
1990
1997
1999
2005
Total population
1092230
1556445
1655984
2158070
Total Registered cases
488
544
688
1327
Incidence rate per 100 000
44.7
35.0
41.5
61.5
Table 4.10: Incidence rates/100 000 of selected cancers for selected years in
Basrah governorate
Years*
Cancers
1995
2005
% change
Breast
Lung and bronchus
4.0
2.1
13.1
4.1
+ 227.5
+ 95.2
٢٢
Urinary bladder
Lymphoma (HL+NHL)
Leukemia
CNS
Larynx
Stomach
Skin
Colon-rectum
2.5
2.2
2.3
0.9
1.4
1.2**
2.4**
1.7 **
5.0
4.8
3.2
1.4
3.1
2.8
4.1
3.2
+ 100.0
+ 118.2
+
39.1
+
55.6
+
121.4
+
133.3
+
70.8
+
88.2
* Figures for 1995 were obtained from Ref. 14
** For 1997
Figure: Comparison of incidence rates of ten cancers in Basrah in
1995 and2005
0
2
4
6
8
10
12
14
Breast
Lung and
bronchus
Urinary
bladder
Lymphoma
(HL+NHL)
Leukemia
CNS
Larynx
Stomach
Skin
Colon-
rectum
Cancer
IR
/
10
00
00
1995
2005
This figure is based on data in Table 4.10
Trends in mortality from cancer for the years 1989, 1997 and 2005
Mortality data are generally considered m ore accurate than morbidity data but
also suffer some limitations
.(15-16)
. In Iraq, official and medically endorsed death
certificate is always required for the burial of any deceased person regardless of
age, sex or cause of death. The death certificate i ncludes an essential field for
writing down the cause(s) of death. Accuracy of causes of death is likely to be
affected in extreme ages. Cancer as cause of death is not immune against errors
٣٢
but the error is expected to be small given the fact that cancer is an important
health problem among even lay people. Examination of time trends of cancer
specific death rates could be considered a good indicator of the burden of cancer
in population especially in places where cancer treatment does not experience
dramatic change.
Crude death rate, cancer death rate and cancer proportional death rate
For the years 1989, 1997 and 2005
Table 4.11 shows the crude death rates, cancer specific death rates and the cancer
proportional mortality ratios over the years 1989, 1997 and 2005.
The crude death rates for 1997 and 2005 are similar but much lower than that for
1989. This looks opposite to the expectation . We have no clear cut explanation .
One possible explanation for the high crude death rate in 1989 is that the rise is
artificial due to registration of newly identified dead military people from the
remnants of the Iraq-Iran War. Cancer specific death rates suggest some rise from
29.2 /100 000 in 1989 to 33.3/100 000 in 1997 and 32.3 /10 0000 in 2005. The
same is true for the cancer proportional mortality ratio which showed clear
increase with time. The latter two types of rates may suggest some degree of
increase in risk of death in Basrah with the passage of time.
Table 4.11: Time trend of crude death rate s and cancer specific death rates,
cancer proportional mortality ratios in Basrah for the years 1989, 1997 and
2005
PMR(%)
CSDR
Cancer
deaths
CRD
Total
deaths
Population
Years
١٫٣
٤٫٦
٥٫٦
٢٫٩٢
٣٫٣٣
٣٫٢٣
٧٩٢
٩٩٤
649
٥٫٩
٢٫٥
٦٫٤
٥٠٧٩
٢٥٨٧
١٢٠٠١
٣٧٠٨١٠١
1499 628
٠٧٠٨٥١٢
٩٨٩١
٧٩٩١
٥٠٠٢
CDR=Crude death rate per 1000, CSDR=Cancer specific death rate per 100 000
PMR=Proportional mortality ratio
Sex distribution of cancer deaths
for the years 1989, 1997 and 2005
Table 4.12 shows the relative composition of cancer deaths with respect to sex
for the three years 1989, 1997 and 2005. Deaths among males form 56.2%,
57.3% and 50.1% in the three years in that order . The corresponding figures for
females are 43.8%, 42.7% and 49.9%. The over all distribution exhibited a
significant statistical difference (P<0.05). The main difference in sex composition
of deaths is in some rise in female share in 2005. This rise is very likely to reflect
the rising incidence and mortality of breast cancer in females.
٤٢
Table 4.12: Comparison of cancer deaths by sex and years
Sex
1989
No. %
1997
No. %
2005
No. %
Total
No. %
Males
Females
Total
167
56.2
130
43.8
297
100.0
286
57.3
213
42.7
499
100.0
325
50.1
324
49.9
649
100.0
778
53.8
667
46.2
1445 100.0
X2 = 6.8 2df P<0.05
Mean age of cancer deaths by sex and year
Table 4.13 shows that the mean age of all cancer deaths among males is 56.98
years which significantly higher than the mean age of cancer deat hs among
females (53.35 years). P<0.05. The mean age does not exhibit significant change
with time. The figures for the three years are very close (P>0.05) despite a minor
tendency towards a decline.
Table 4.13: Mean age of patients dying from cancer by s ex and years
Variable
Number
of
deaths
Mean age +SD
P value
1.Sex
Males
Females
2. Years
1989
1997
2005
778
667
297
499
649
56.98 + 19.75
53.35 + 19.99
55.58 + 17.53
55.32 + 20.79
55.18 + 20.33
<0.05
>0.05
Spatial distribution of cancer deaths for the years 1989, 1997 and 2005
Table 4.14: compares the relative frequency of deaths in different areas of
Basrah governorate for three years (1989, 1997 and 2005). The hypothesis
beyond the choice of these three years has al ready been stated before (Section
5.1).The over all patterns in the three years are generally similar for the three
years with few exceptions. The variation can not be interpreted without further
٥٢
analysis taking into consideration a possible differential changes in the
population size in each area.
Table 4.14: Comparison of cancer deaths by areas of Basrah and years
Area
1989
No. %
1997
No. %
2005
No. %
Basrah City
Northern Area
Western Area
Southern Area
Eastern Area
159
53.5
58
19.5
53
17.8
14
4.7
13
4.4
279
55.9
94
18.8
73
14.6
37
7.4
16
3.2
325
50.1
135
20.8
109
16.8
34
5.2
46
7.1
Total
297
100.0
499
100.0
649
100.0
X2 = 15.6 8df P < 0.05
Mortality rates for the years 1989, 1997 and 2005
Table 4.15 shows the annual cancer specific mortality rates in Basrah
governorate for the years 1989, 1997 and 2005. No clear pattern can be
identified. The risk of death is not much different in different years. Most cancers
show stable or slightly fluctuating level of risk of death with time. Slight rise in
the risk of death may be noticed in cancers of CNS, blood (leukemia), Bo nes,
lymphomas and Colon-rectu
٦٢
Table 4.15: Comparison of annual mortality rates /100 000 of various
cancer deaths in Basrah for the years 1989, 1997 and 2005
2005
1997
1989
Type of cancer
4.3
2.8
2.7
3.2
2.1
2.0
1.1
1.2
1.0
1.3
1.3
0.8
0.6
0.6
0.5
0.4
0.6
0.5
2.1
5.1
3.3
3.4
1.6
2.7
2.0
2.2
1.5
1.5
1.0
1.1
1.0
1.0
1.0
0.7
0.7
0.2
0.3
1.5
5.1
3.5
2.2
3.3
1.9
1.4
1.6
1.4
0.8
1.0
0.6
0.6
1.1
0.6
0.5
0.5
0.4
0.1
2.1
Lung
Urinary Bladder
Blood
Breast
Lymphomas
CNS
Stomach
Pancreas
Bones
Liver
Colon Rectum
Uterus
Secondary
Prostate
Ovary
Oesophagus
Kidney
Skin
All Others
٣٫٢٣
33.3
29.2
Total
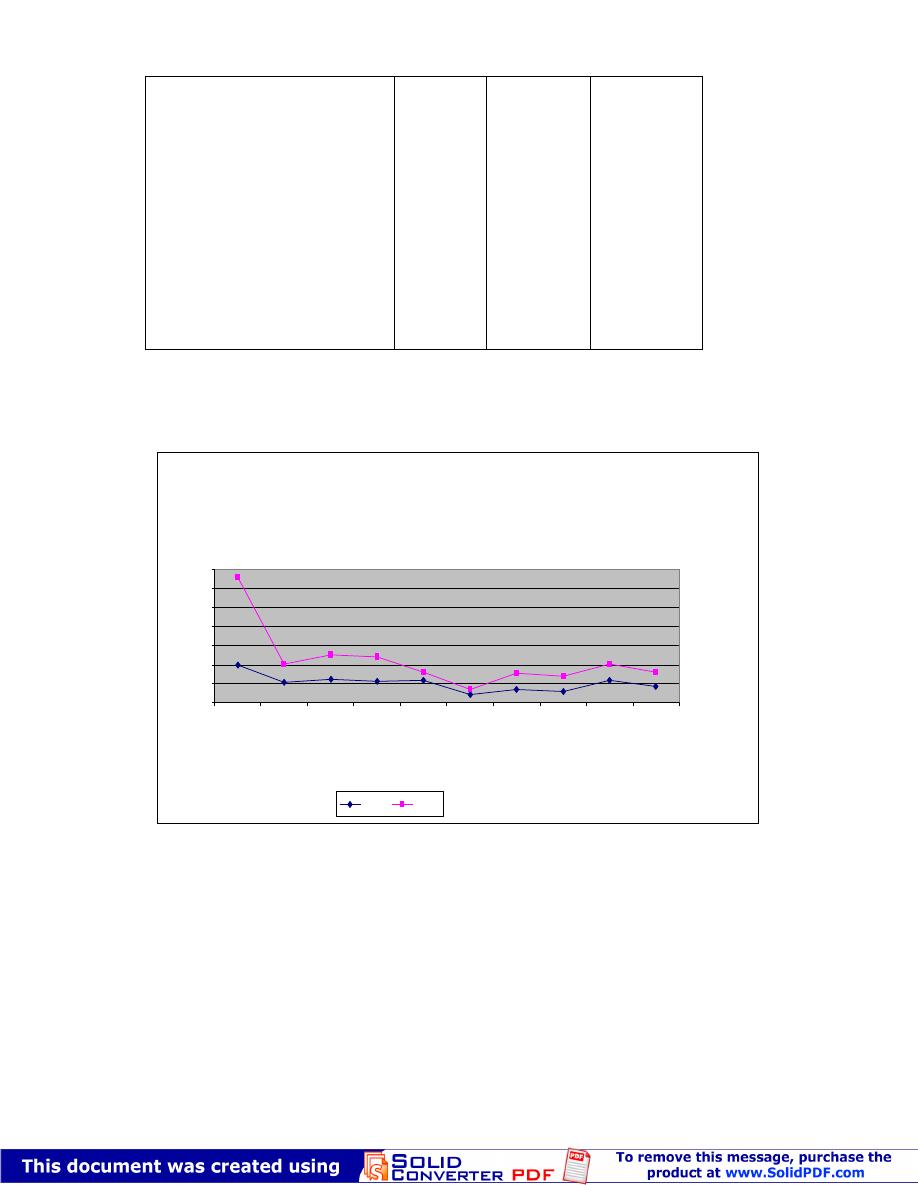
Mortality rates (per/100000) in Basrah for the years 1989, 1997 and 2005
0
1
2
3
4
5
6
Lu
ng
U
rin
ar
y
Bl
ad
de
r
Bl
oo
d
Br
ea
st
Ly
m
ph
om
as
C
N
S
St
om
ac
h
Pa
nc
re
as
Bo
ne
s
Li
ve
r
C
ol
on
R
ec
tu
m
U
te
ru
s
Se
co
nd
ar
y
Pr
os
ta
te
O
va
ry
O
es
op
ha
gu
s
Ki
dn
ey
Sk
in
Al
l O
th
er
s
Cancers
M
R
/1
0
0
0
0
0
2005
1997
1989
This figure is based on data in Table 4.15

٧٢
4.5. Survival rates for 2005 in different areas of Basrah
governorate
One of the difficult epidemiological parameters to calculate and interpret is the
survival rate given the doubts surrounding the completeness of case registration
and accuracy the registered cause of death at the death certificates. Survival rates
are affected by these possible errors as well as the availability of effective
treatment and the nature of the cancer itself . According to Parkin 2002 (7), it is
possible to estimate the five - year survival rates by the following formula:
Mortality rate
Five-year survival= (1- ------------ )
Incidence rate
We used this method to estimate the five year survival rates as shown in Tables
4.16-4.19
Survival for different types of cancer
Table 4.16 shows the estimated annual incidence rates, the annual mortality rates
and survival rates for different cancers. The range of the survival rates is from
0% in case of cancers of the lung , liver, pancreas and intestine(other than the
colon-rectum) to as high as 80% and above in case of cancers of skin , thyroid ,
pharynx, male genital organs. Apart of completeness of data, the case fatality and
hence the survival rate is affected by stage at which cancer is diagnosed, the
nature and aggressiveness of the cancer itself and the availability of effective
medical care.
Survival by age and sex
Table 4.17 shows that the survival rate is better for females (62.9%) as compared
to males (55.7%). This favourable survival in females is likely to reflect th e
effect of breast cancer which is the prime cancer among females and known to
have high survival rate.
Regarding age (Table 4.18), Survival rate is higher early in life and decreases
with advancing age . In males the survival rate for children aged <15 is 63.9% . It
is higher (71.7%) for people aged 15-45 years then declines to reach as low as
33.5 for males aged 65 years and above. Similar pattern is noticed for females
except that the trend of decreasing survival with advancing age is smoother.

٨٢
Table 4.16: Annual incidence rate, annual mortality rate and five years
survival rates for all cancers by type of cancer
Survival rate
(%)
Annual
mortality rate
Annual
incidence rate
Type of cancer
75.6
44.0
56.3
88.9
0.0
15.6
59.4
67.7
60.7
NA
NA
63.6
52.4
75.0
33.3
0.0
NA
92.3
92.3
0.0
45.5
40.0
0.0
25.0
NA
80.0
NA
NA
NA
75.0
50.0
50.0
0.0
50.0
NA
75.0
3.2
2.8
2.1
0.5
4.3
2.7
1.3
1.0
1.1
NA
NA
0.8
1.0
0.5
0.1
1.9
NA
0.1
0.1
1.3
0.6
0.6
1.2
0.6
NA
0.1
NA
NA
NA
0.1
0.2
0.2
0.3
0.1
NA
0.8
13.1
5.0
4.8
4.5
4.1
3.2
3.2
3.1
2.8
2.7
2.3
2.2
2.1
2.0
1.5
1.4
1.3
1.3
1.3
1.1
1.1
1.0
0.9
0.8
0.6
0.5
0.5
0.5
0.5
0.4
0.4
0.4
0.3
0.2
0.2
3.2
Breast
Urinary bladder
Lymphomas
Skin
Lung
Leukemia
Colon-rectum
Larynx
Stomach
Soft tissue
Other lymphoid cancer
Uterus &cervix
Bone
Ovary
Pleura
CNS
Peritoneum
Thyroid gland
Pharynx
Liver
Kidney
Prostate
Pancreas
Secondary
Parotid gland
Testis/Penis
Bone marrow
Retroperitoneal
Choriocarcinoma
Nose
Oral cavity
Gall bladder
Intestine
Abdomen
Vulva/Vagina
All others
59.6
30.0
74.3
Total
٩٢
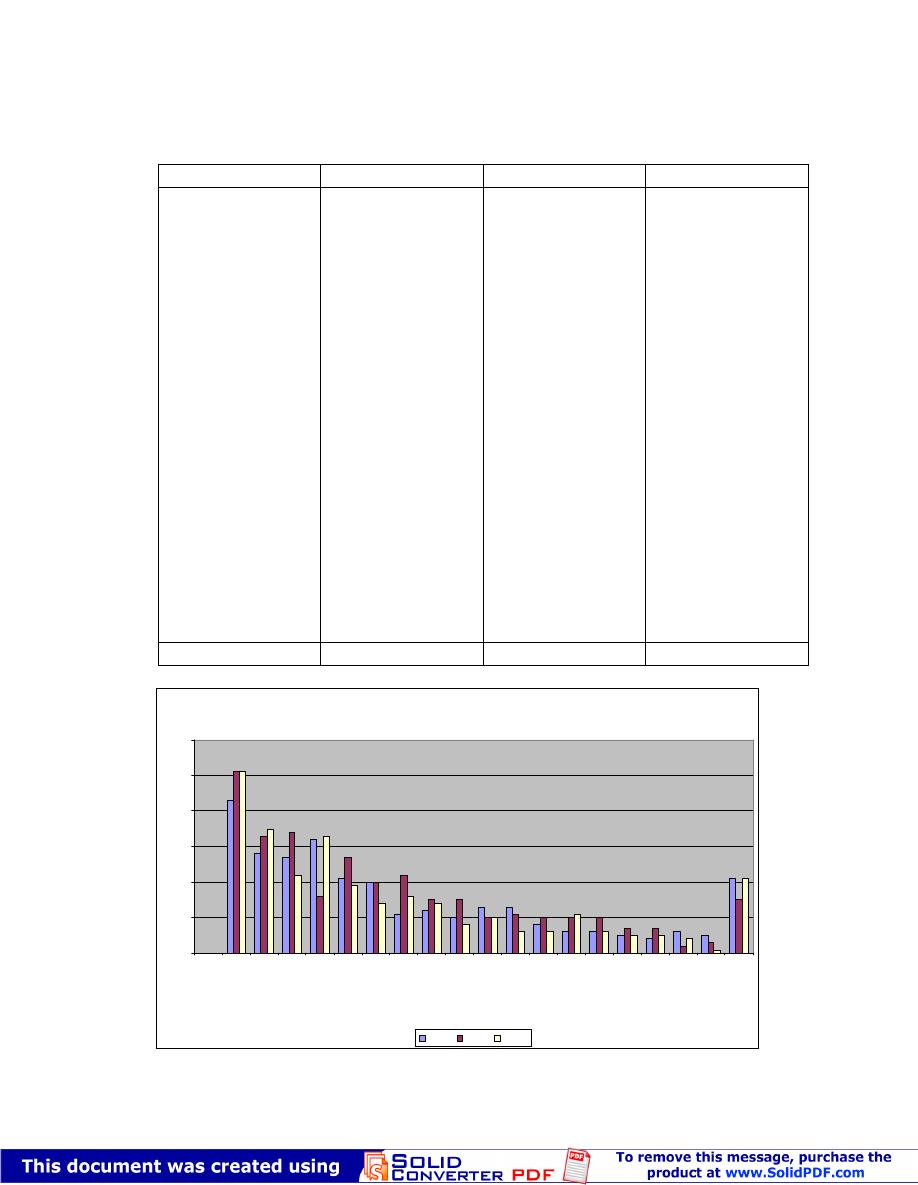
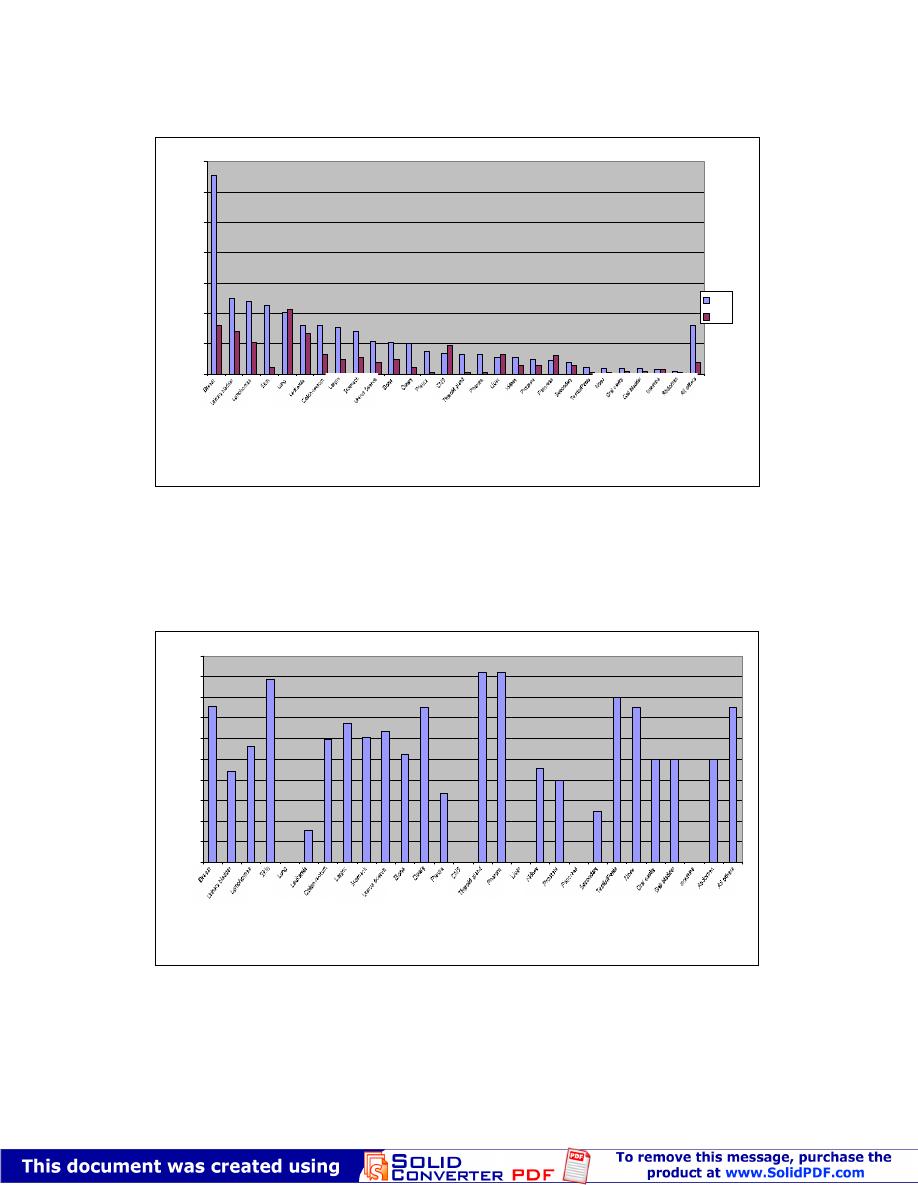
Figure :Incidence and mortality rates (per 100000) of different cancers in Basrah
2005
0
2
4
6
8
10
12
14
Cancers
R
a
te
/1
0
0
0
0
0
IR
MR
This figure is based on data in Table 4.16
Figure: Survival rate (%) for cancers in Basrah 2005
0
10
20
30
40
50
60
70
80
90
100
Cancers
S
u
rv
iv
al
r
at
e
(%
)
This figure is based on data in Table 4.16
٠٣
Table 4.17: Annual incidence rate, annual mortality rate and five years
survival rates for all cancers by sex
Sex
Annual incidence
rate/100 000
Annual mortality
rate
Five
year-survival
rate (%)
Males
Females
68.1
80.5
30.2
29.9
55.7
62.9
Total
74.3
30.0
59.6
Table 4.18: Annual incidence rate, annual mortality rate and five years
survival rates for all cancers by age and sex
Males
Females
Age
IR/100
000
MR/100
000
Survival
rate (%)
IR/100
000
MR/100
000
Survival
rate (%)
<15
15-44
45-64
65& above
15.8
31.4
261.2
660.2
5.7
8.9
103.4
439.1
63.9
71.7
60.4
33.5
12.8
54.5
357.4
390.7
4.4
26.7
236.3
285.1
65.6
51.0
33.9
27.0
Total
68.1
30.2
55.7
80.5
29.9
59.6
Survival by geographical area
With respect to geographical areas of Basrah governorate. Great variation is seen
in the five year survival rates (Table 4.19). The range is from 38.7% for the
eastern district to as high as 75.9% in the southern districts. This variation may
reflect variation in completeness of case registration, nature of cancer distribution
or differential care available for cases, accessibility to treatment may be different.
Table 4.19: Survival rates for 2005 in different areas of Basrah governorate
Area
Annual Incidence
rate
Annual
death
rate
Survival
rate(%)
Basrah city
Northern area
Western area
Southern area
Eastern area
78.4
65.3
80.0
72.3
76.3
38.1
22.1
27.1
17.4
46.8
51.4
66.2
66.1
75.9
38.7
Total
74.3
30.0
59.6

١٣
4.6. Summary conclusions
1. Cancer is a real health problem in Basrah in terms of incidence and mortality.
2. The need for and the creation of a sustainable cancer registry at the level of
Basrah governorate is crucial for the planning, management and evaluation of
epidemiological changes as well as provision of effective preventive and
therapeutic care.. Without such reliable registry, all measures to deal with cancer
are unlikely to be completely successful
3. A team approach is inevitable for the success of any work which deems fruitful
to handle the public and individual needs and consequences of cancer.
We initiated this, but the continuity depends on others in the clinical , laboratory,
administrative and statistical domains of the game.
4. Although, the data base on cancer cases is still incomplete , preliminary results
do provide clues to the rising trend in cancer incidence in Basrah. Regarding
mortality, the picture is confusing. A rise in incidence and leveling in morta lity
could reflect improvement in treatment of cancer . No doubt that the surgical
handling, the chemotherapy as well as other aspects of care are better in Basrah
during the past decade than they were two or more decades ago . Early diagnosis
is a definite contributor to the better outcome of cancer in terms of longer
survival.
5. Further analysis at individual cancer level is required but that is relevant only
after good data base is created for several years. Aggregate analysis could cancel
some time changes in incidence and/or mortality if some cancers counteract the
effect of others.
6. The sustainability of the current project towards a final destiny of
comprehensive cancer registry and effective system of cancer care requires
substantial support from local authorities, local NGOs and international
organizations.
5. FUTURE PERSEPECTIVES

٢٣
For the "FOUR-LEGGED PROJECT" to move forward, we definitely need:
1. Continuation of efforts to improve routine cancer registration. This needs a
number of practical steps:
a. Creation of administrative and scientific back up bodies. The working paper
presented at the seminar on May 28
th
, 2006, proposed a framework for the
creation of local cancer council which is entitled to supervise all cancer related
activities in Basrah. In the meanwhile, the council is part of a national network
encompassing local councils in other governorates and national cancer council. It
is envisaged that the creation of such body or bodies will enhance coordinated,
scientific and effective measures to deal with the problems of environment and
cancer.
2. The initiation of complementary population -based (household based) studies to
validate the cancer registry data base . The questionnaire (Appendix 4) may be
further developed to be used in the population-based surveys.
3. Further improvement in analytical epidemiological studies. These studies are
the basis for hypotheses testing about any proposed risk factors and
environmental exposures.
These last two areas of activities (i.e., the h ousehold based survey and the wide
scale analytical studies) requires substantial support in terms of financial,
technical and administrative . The security issue remains one of the main
obstacles to any sustainable work in this field. The success of all proposed
activities is also dependent on the successful "cultivation" of team work and the
recognition by all partners of the value of multidisciplinary approach to problem
solving. Without these prerequisites, nothing significant is expected to be
achieved.
4
.
The future of any scientific work like the one concerns cancer in Basrah
depends entirely on the will and commitment of doctors to work together towards
caring for the people, their ability to realize the value of numbers in medical
practice and research and their perception that in some time in the future they will
be audited for their performance. Without this, nothing radical will happen in the
way we are handling health care of the people.
Regardless, three envisaged hopes can be mentioned here
a. A conference on Environment and cancer is planned to be held in November
2006. This depends however on security situation and the support of local and
international interested partners.
b. A consensus is reached on Basrah population -based cancer Registry
c. A household survey is essential complementary activity to consolidate and
validate the data base on cancer in Basrah . The survey could be based on
periodical (every five years) sample household survey.

٣٣
6. REFERENCES
1. WHO. National cancer control programme s: Policies and managerial guidelines. World
Health Organization, Geneva 1995.
2. Parkin DM, Bray T, Ferlay J and Pis ani P. Global Cancer Statistics 2002. CA Cancer J.
Clin. 2005; 55: 74-108
3. Knox EG, Stewart AM, Gilman EA and K neale GW. Background radiation and childhood
cancer. Journal of Radiological Protection 1987:8: 9-18.
4. Greenberg RS, Eley JW, Daniels SR, Boring and Flanders WD. Medical Epidemiology.
Lange medical book/McGraw -Hill. Toronto, 3
rd
Edition, Toronto 2001 Chapter 1 Pp: 1-14.
5. Abood, AS. A study of time and space distrib ution of selected diseases in Basrah. PhD
thesis, University of Basrah 1999.
6. Yacoub, AAH, Ajeel NAH and Al -Wiswasy, MK. Incidence and pattern of
malignant diseases (excluding leukemia) during 1990- 1997. Medical journal of
Basrah University. 1999; 17.
7. Yacoub AAH, Al-Sadoon IO, Hassan GG and Muffid Al -Hemadi. Incidence and
pattern of malignant disease among children in Basrah with specific reference to
leukemia during the period 1990- 1998. Medical journal of Basrah University.
1999;17.
8. Hassan Jk. Cancer in Basrah: Pattern an d determinants with special emphasis on SCD
and G6PD deficiency (A new hypothesis).
Ph.D. thesis, University of Basrah 2003.
9. Fahey, D. Science or Science Fiction: Facts, myths and propaganda in the debate over
depleted uranium weapons. Internet 2003.
10. Habib OS; Al-Ali JK, Ajeel NAH and Al -Wiswasi MK. Cancer and Environment:
Problems and future. A research protocol approved by the Ministry of Health. Available at the
Department of Community Medicine, College of Medicine, University of Basrah 2005.
11. Division of Preventive Medicine in Basrah Health Authority. Personal communication.
12. Department of Community Medicine. College of Medicine, University of Basrah. Reports
of Field Practice Experience for the years 1993- 2002.
13. Al-Mulla, AYY. Pattern and determinants of fertility in Basrah. PhD thesis, University of
Basrah 2006 Pp.

٤٣
14. Ajeel NAH. Extent of cancer in Iraq. Unpublished Report, Department of Community
Medicine, College of Medicine, University of Basrah 1999.
15. Hill AB. A short textbook of medical statistics , 11
th
edition. London, EdwardArnold,1984
Pp.259-264.
16. MacMahon P, Pugh TF. Epidemiology: Principles and methods . 1
st
edition. Boston, Little
Brown and Company 1970, Pp. 75-76.