
CASE-CONTROL STUDIES
Ass.Prof. Dr Faris Al-Lami
MB,ChB MSc PhD FFPH
Dept. of Community Medicine/ College
of Medicine/ Baghdad University

CASE-CONTROL STUDIES
•It is a type of observational analytic
studies.
•Study subjects are selected on the basis
of whether they do
(cases)
or do not have
(controls)
the outcome under study.
•The groups then compared for the
proportion of having a history of exposure
or characteristic of interest.
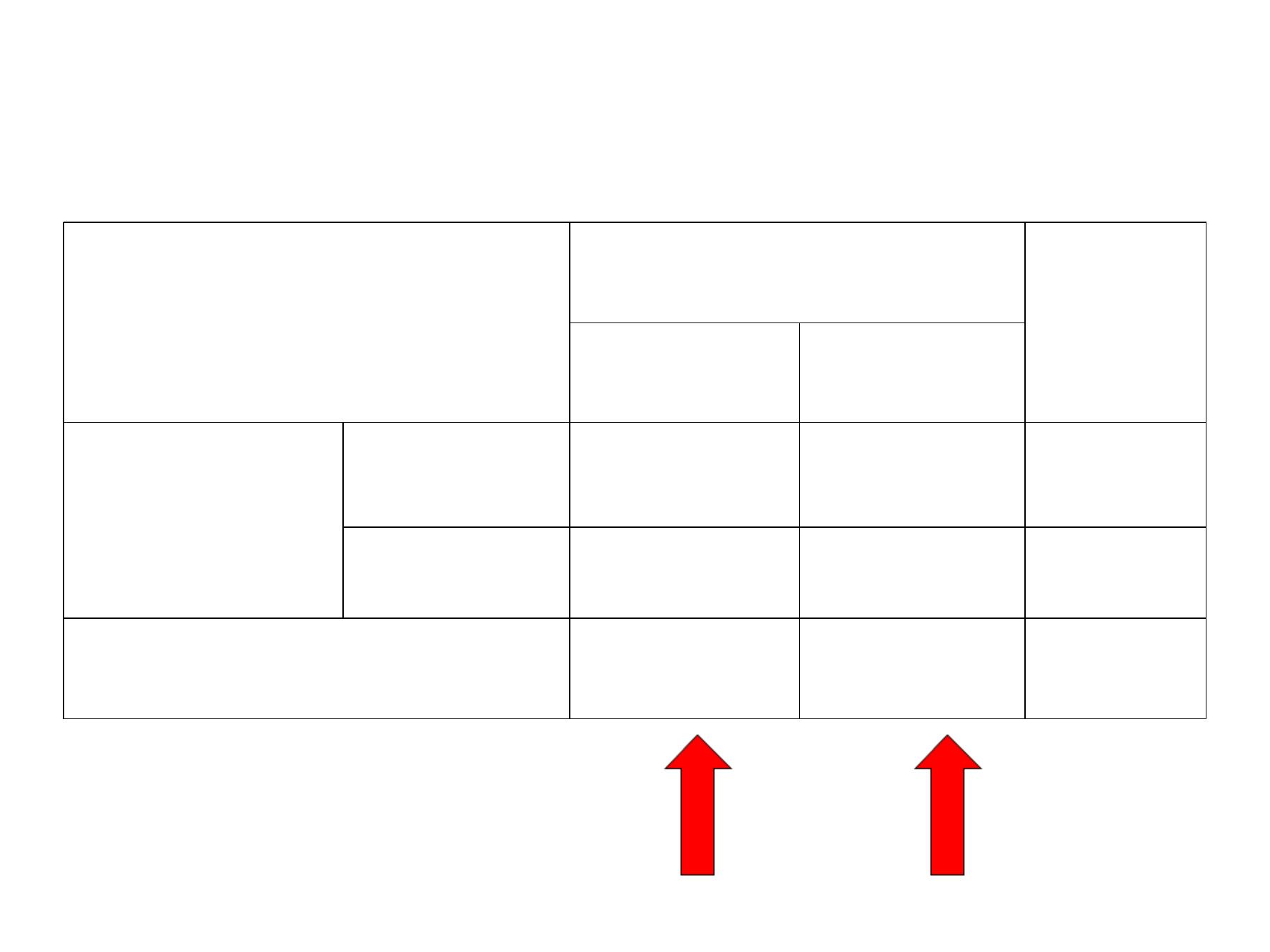
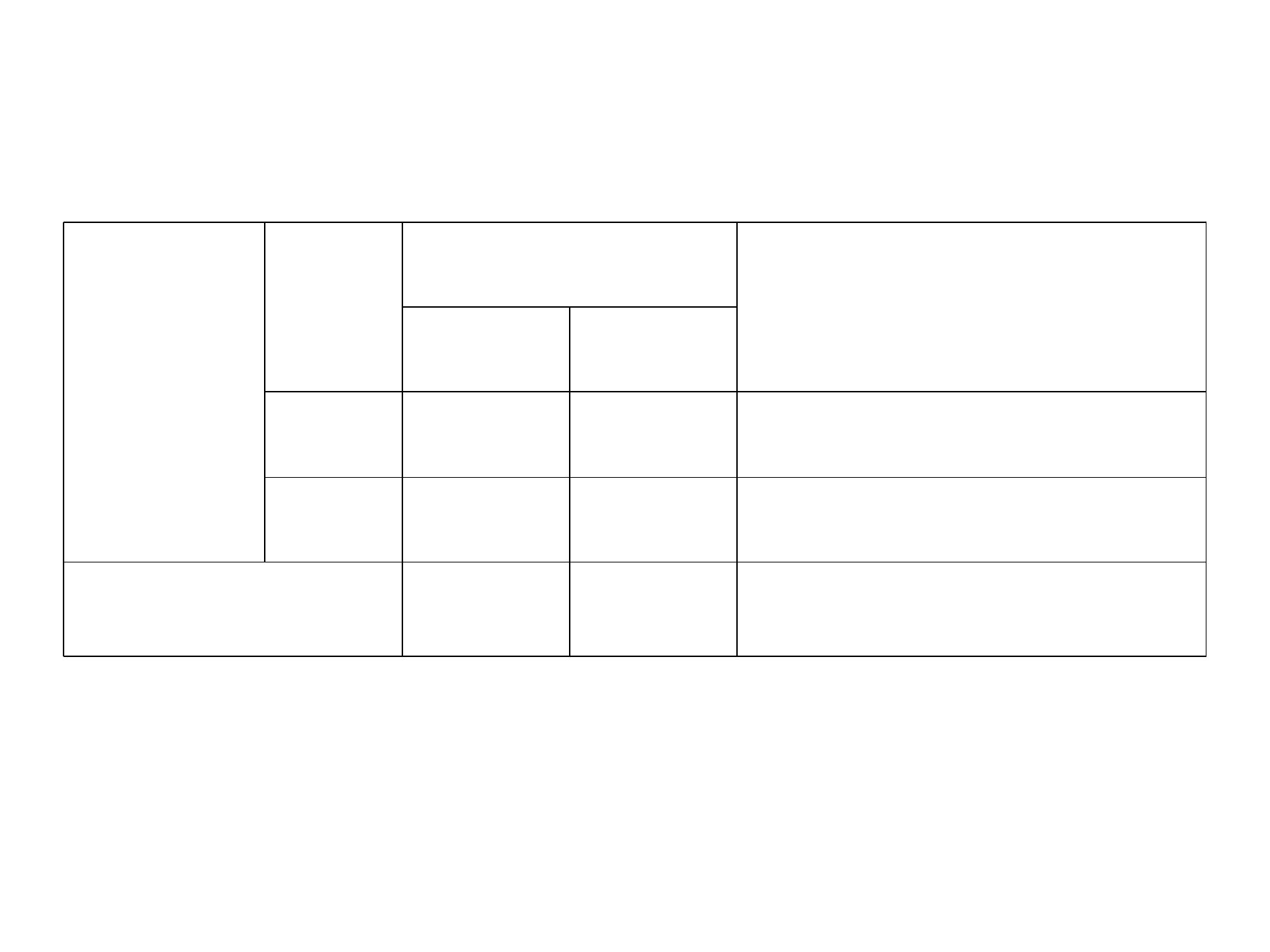
CASE-CONTROL STUDIES
Disease
Total
Present
Absent
Exposure
Present
a
b
a+b
Absent
c
d
c+d
Total
a +c
b+d
N
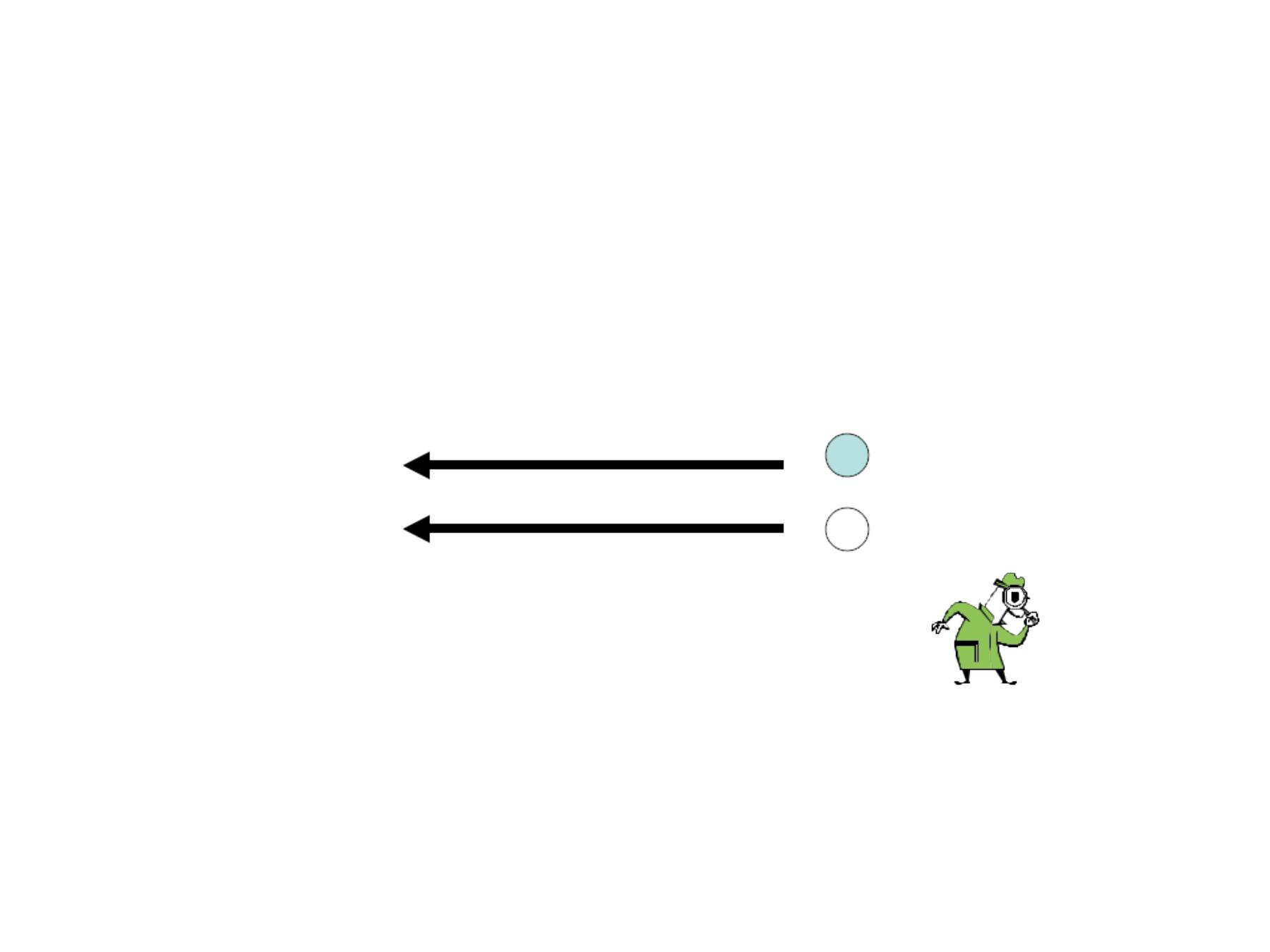
Case-Control Studies –
Timing
Exposure
?
?
Exposed
Unexposed
Disease
Yes (case)
No (control)
Investigator
Exposure
• Cat ownership in
childhood disorder,
• Body-mass index
• Physical disability
• Hiatus hernia
• Hair dyes
• History of shingles
• Pig farming
• Ghee (clarified butter)
• Pickled vegetable
consumption
• Turf running surface
Outcome
• Schizophrenia, schizoaffective
or bipolar disorder
• Pancreatic cancer
• Earthquake mortality
• Reflux oesophagitis
• Connective tissue disorders
• Systemic lupus erythematosus
• Nipah virus infection
• Neonatal tetanus
applied to umbilical cord stump
• Oesophageal cancer
• Musculoskeletal injury in
thoroughbred racehorses
Examples of topics investigated with
case-control studies

Strengths:
1. Suitable for diseases of long latency period
2. Quick and inexpensive (as compared to other
analytic studies)
3. Suitable for rare diseases
4. Can examine multiple etiologic factors for a
single outcome.
5. Requires fewer subjects at entry
6. Few ethical problems

Limitations:
Since the exposure and outcome are
already occurred at the time the
participants enter the study, this will lead
to:
Ø
Differential selection of either the cases
or the controls into the study on the basis
of their exposure status
(selection bias)
Ø
Differential reporting or recording of
exposure information between study
groups on their disease status
(informational bias)
.

Limitations-
ØUsually cannot measure disease risk
ØRelies on recall or records for information
on past exposures (potential recall bias)
ØMay be difficult to determine that ‘
cause’
preceded ‘
effect’
(Temporal relationship)
ØUnsuitable for rare exposures

Case-Control Studies –Steps
1. Identify cases of disease of concern
2. Identify appropriate non-diseased
comparison group (“
controls”
)
3. Document exposures among cases
and controls
4. Calculate odds ratios
5. Perform statistical tests or calculate
confidence intervals

Definition of Cases
The definition of the cases should depend
on:
1. Homogenous disease entity
2. Strict diagnostic criteria
Depending on certainty of diagnosis, and
amount of criteria one can classify the
diagnosis into definite, probable, and
possible

Sources of Selection of the cases:
1. Hospital-based case control studies
The cases will be identified from the
hospitals, or other health care facilities.
These are common, relatively easy, and
inexpensive.

Sources of Selection of the cases:
2. Population based case-control studies.
It involves locating and obtaining data
from all affected individuals or a random
sample from a defined population.

Population based case-control
studies: advantages
•Avoid bias in selecting factors that lead
affected individuals to utilize certain
hospital
•Describe the picture of the disease in the
population
•Compute rates of the disease in exposed
and unexposed individuals.

Selection of Controls
It is the most difficult aspect in CCS.
It depends on:
Ø Characteristics and sources of cases,
Ø Need to obtain comparable and
reliable information from cases and
controls,
Ø Practical and economic consideration.

Selection of Controls
The controls should be comparable to the
source of the population of cases and that
any exclusions or restrictions made in the
selection of cases should be applied
equally to the controls and vice versa.

Where to Find Controls
•Hospital- or clinic-based
•Population-based
•Special group as Neighbors, Friends

Types of controls:
1. Hospital control:
consist of patients at
the same hospital with conditions other
than the disease under study.

1. Hospital control:
Advantages
:
• Easily identified insufficient number, with minimal
cost, and effort.
• May come from the same catchments area
• More willing to know about previous exposures
than healthy people (less recall bias).
• They are exposed to the same factors that make
them select this particular hospital (less selection
Bias)
• More willing to cooperate than healthy people,
(less non-response).

1. Hospital control:
Disadvantage
Ø
They are by definition ill and not healthy.
Ø
Hospitalized controls differ from general
population
Ø
Control disease may be linked to exposure
The patient in the control should not have a
disease that is related to the same risk factors of
the disease under study (CA-lung, MI, Smoking)

2. General population control
Used when the cases are chosen from the
general population, and if the hospital
control is not desirable or feasible.

2. General population control
Difficulties:
ØMore costly and time consuming
ØPopulation lists are not always available
ØDifficult to contact healthy people with
busy work

2. General population control
Difficulties:
ØThe quality of information may differ from
cases and control (more recall bias)
ØLess motivated to participate (more non-
response)
ØThose who accept to participate may
systematically differ from those who
refused (volunteer Bias).
3. Special Group Control
• Friends, relatives, neighbours of the cases .
• They have the advantage of the general
population control, in that they are healthy, but
they are more willing to cooperate, and offer a
degree of control on certain confounding factors
as ethnic background, socioeconomic status, or
environment

No. of Controls
•When the number of cases and controls is
large and the cost of obtaining them is
similar we choose one control for every
case (1:1 ratio), but if the number of cases
is small then the number of controls can
be increased and this will increase the
power of the study , but this should not
exceed 4:1.

Ascertainment of the disease, and
exposure status
• Outcome status can be made from death
certificates, case sheets, discharging cards.
• Exposure status can be obtained by interview, a
questionnaire, or medical records.
• It is important that the data collector should not
aware of: who the case is, and who the control is
and about the hypothesis under study to
minimize the possibility of observational bias.

Step 4 — Measure of
Association
•Odds Ratio (OR)
•Odds ratio
- Good estimator of risk or rate ratio,
especially for rare disease
- Odds of exposure among cases divided
by odds of exposure among controls
Case-Control –2-by-2 Table
Case
Exposed
a
Unexposed
c
V
1
Control
b
d
V
2
Odds Ratio = (a/c) / (b/d) = ad / bc

Measure of Association between
Exposure and Outcome
The association between outcome, and
exposure in CCS is estimated by Odds
Ratio (OR)
ad
Odds Ratio =--------------
bc
Example
Cigarette
Smoking
Lung Cancer
Total
Cases
Control
Yes
70
30
100
No
30
70
100
Total
100
100
200

Exercise
ad
70 x 70
Odds Ratio= ------------=-----------------= 5.4
bc
30 x 30
= OR
(1± z/√x2)
95% CI =5.4 1± 1.96/ √32
= 3.1- 9.6

Role of Bias in case control studies:
1. Selection Bias
: occur when the inclusion of
cases or controls into the study depends on
the exposure of interest.

Role of Bias in case control studies:
2.
Observational Bias
: error in obtaining,
reporting, or recording of information by
the investigator.
It is affected by knowledge of the disease
status or the hypothesis by the interviewer
will increase this bias.
Role of Bias in case control studies:
3.
Recall Bias
: related to difference in the
ways the cases and the controls will recall
their exposure history.
Cases are more likely to remember
exposures than healthy controls.

Role of Bias in case control studies:
4.
Misclassification
: refers to errors in the
categorization of either the exposure or
disease status.