1
Lecture: 3
Parasitology
.د
هيفاء
New world cutaneous Leishmaniasis
It is called American cutaneous leishmaniasis, which is caused by:
1- L. mexicana complex
2- L. braziliensis complex
The vector is sand fly genus Lutzomyia
1- Lesions caused by L. mexicana complex
L. mexicana lesions are usually single, self-limiting cutaneous papules,
nodules or ulcers on face and ears (about 60%), they are painless and
usually heals within few months.
Ulcerative lesions on the ears (Chiclero’s ulcer) may cause destruction
of the ear cartilage.
Reservoir hosts are rodents and dogs.
Sometimes lead to diffuse cutaneous leishmaniasis.
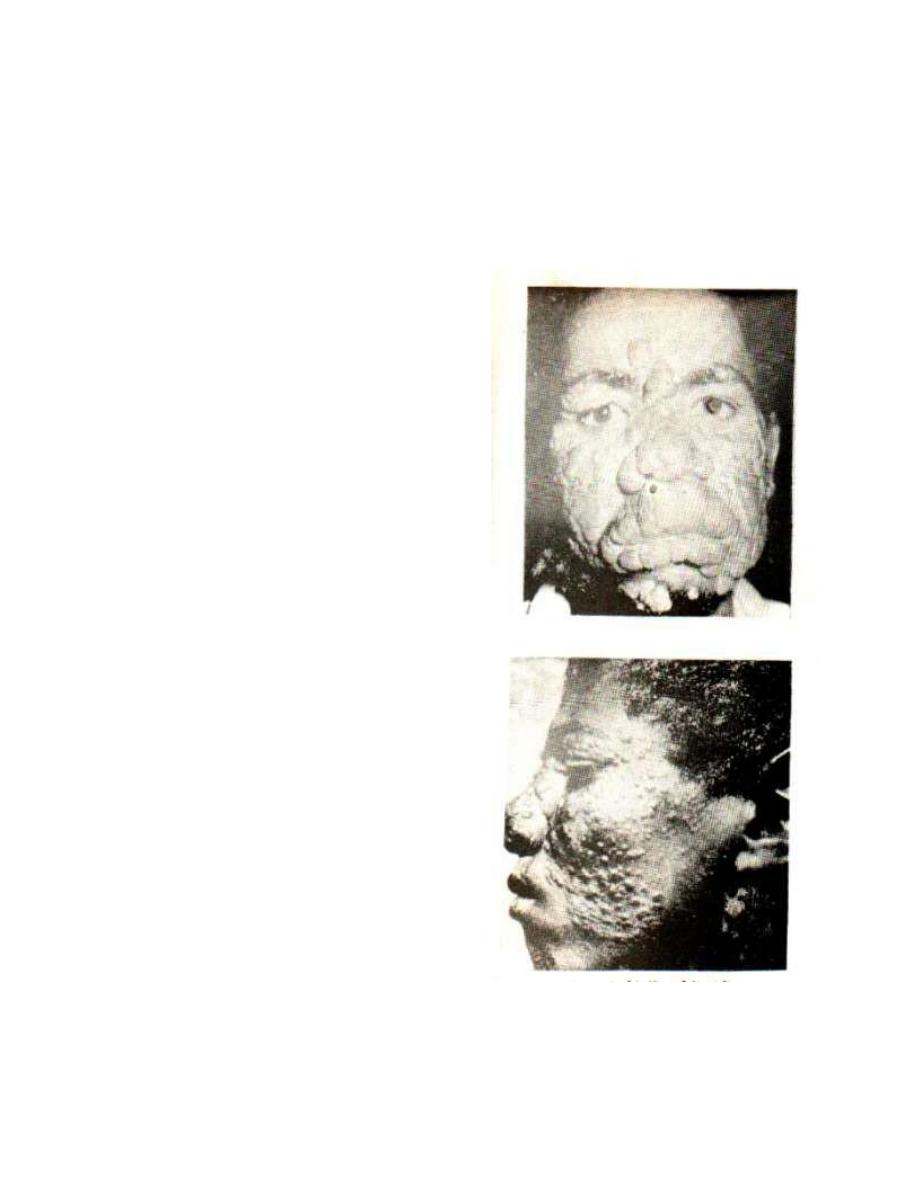
2- Lesions caused by L. braziliensis complex
(MucocutaneousLeishmaniasis (Espundia))
Produced by species belongs to Leishmania braziliensis complex. It is
distributed in South Africa.The cutaneous lesions develop exactly as
does the oriental sore, but they are more frequently multiple and may
become large. Secondary infection plays a prominent role in the
persistence of these ulcers, sometimes ulceration of the adjacent areas
extend to involve mucosal surfaces, but more frequently the lesions
seem to develop by metastasis.
Nasal mucosa and that of the hard and soft palate is affected.
The nasal septum is destroyed but does not involve the bone, ulceration
may result in loss of all the soft parts of the nose, the lips, and the soft
2
palate and may lead to severe facial disfiguration.Death usually occurs
from secondary infection.
Various rodents and dogs are infected; sand flies belonging to the genus
Lutzomyia are vectors.
Visceral Leishmaniasis (Kala-azar) (Dum-Dum fever,
black fever)
It involves different age groups in various geographical areas. VL is
divided into four clinical and epidemiological (ecological) forms:-
1- Mediterranean (Infantile) type
Sporadic cases.
Distributed in the Mediterranean basin, Middle East, former
southern USSR and northern China (this type is found in middle
and south of Iraq).
Affects chiefly infants and young children (especially under 5
years).
Reservoir hosts are domestics and wild dogs (fox and Jackal), so
it is a zoonotic disease.
Caused by L. Infantum.
2- Indian (classical) type
Epidemic disease.
Distributed in Indian subcontinent.
Man is the reservoir host, lack of an animal reservoir host (not
a zoonotic disease).
Seen in young adults and adolescents.
Frequent presence of amastigote in peripheral blood
(circulating macrophages).
Caused by L. donovani.
3- African type (Sudanese) type
Seen in adults men.
3
Rodents and dogs are the reservoir hosts (zoonotic disease).
Distributed in Sudan and East Africa.
Presence of the parasites in peripheral blood is less common.
Caused by L. donovani (as Indian type).
4- South America type
Distributed in central and south America.
Affects mainly children.
Reservoir host are foxes, domestic dogs and cats (zoonotic
disease).
Caused by L. chagasi.
Mode of transmission
1- Vector born transmission (by insect bite): represents the most
common mode of transmission, while the others are rare.
2- Blood transfusion.
3- Needle sharing.
4- Congenital transmission (not transplacental transmission) but
during the exchange of the mother’s blood at the time of passage of
the fetus through birth canal → transmission occurs.
5- Sexual transmission.
6- Laboratory acquired transmission: from needle stick injuries,
handling contaminated specimens and some to oral exposure.
7- Person to person transmission: via contact with infected fluid
(nasal and oral secretions, tonsillopharyngeal mucous and urine) of
patient with VL.
Clinical presentation
Incubation period vary from 2 weeks to 18 months.
Visceral leishmaniasis characterized by pentad of irregular faver,
hepatosplenomegaly,
pancytopenia
(leucopenia,
anemia
and
thrombocytopenia), hypergammaglobulinemia and weight loss.

4
However after infection most cases remain asymptomatic or associated
with symptoms that resolved spontaneously, but the disease (VL) may
be fetal (95%) if left untreated.
Other clinical manifestations may include paleness, ecchymosis,
epistaxis and gingival bleeding, oedema, ascitis, skin hyper-
pigmentation, jaundice, abdominal distension and lymphadenopathy.
Pathogenesis
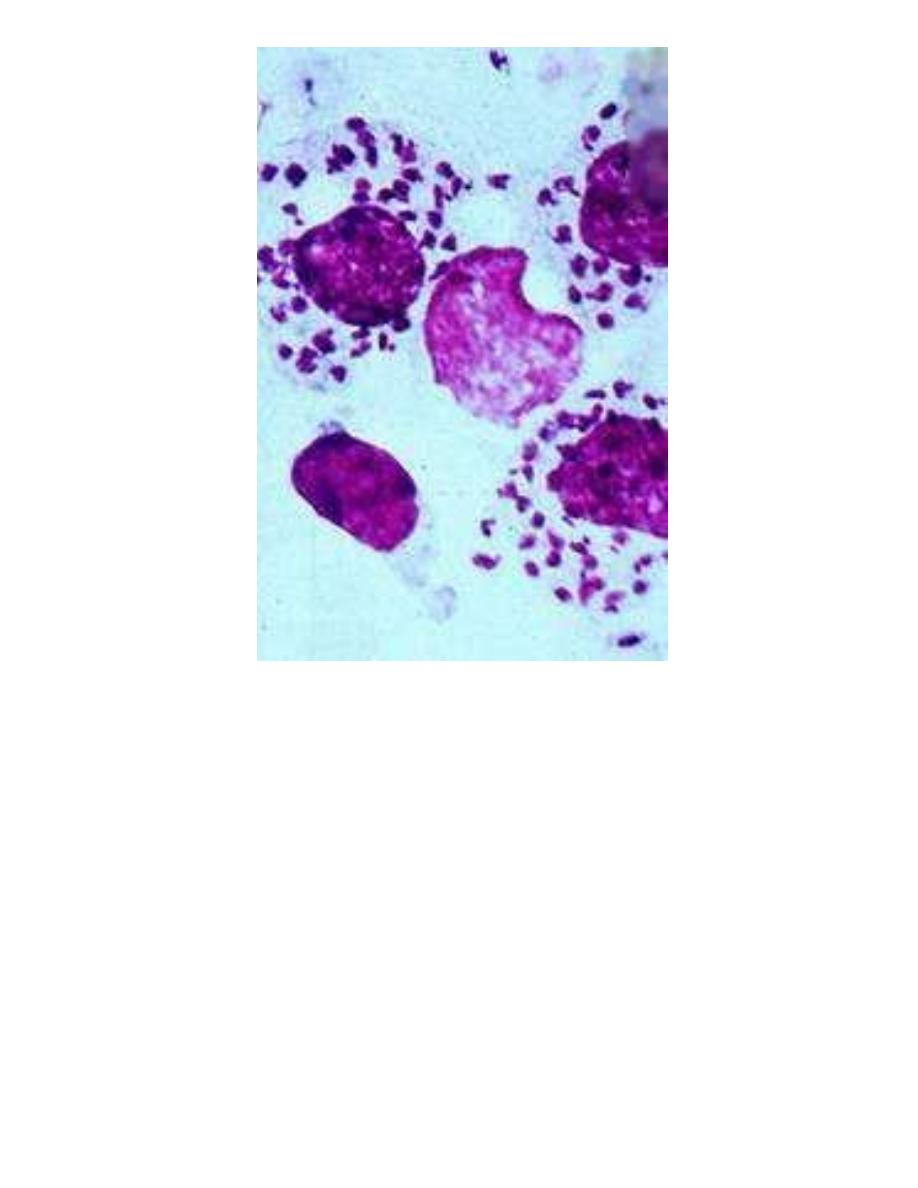
The parasite (amastigotes of various species of L. donovani
complex) infect RE cells throughout the body.
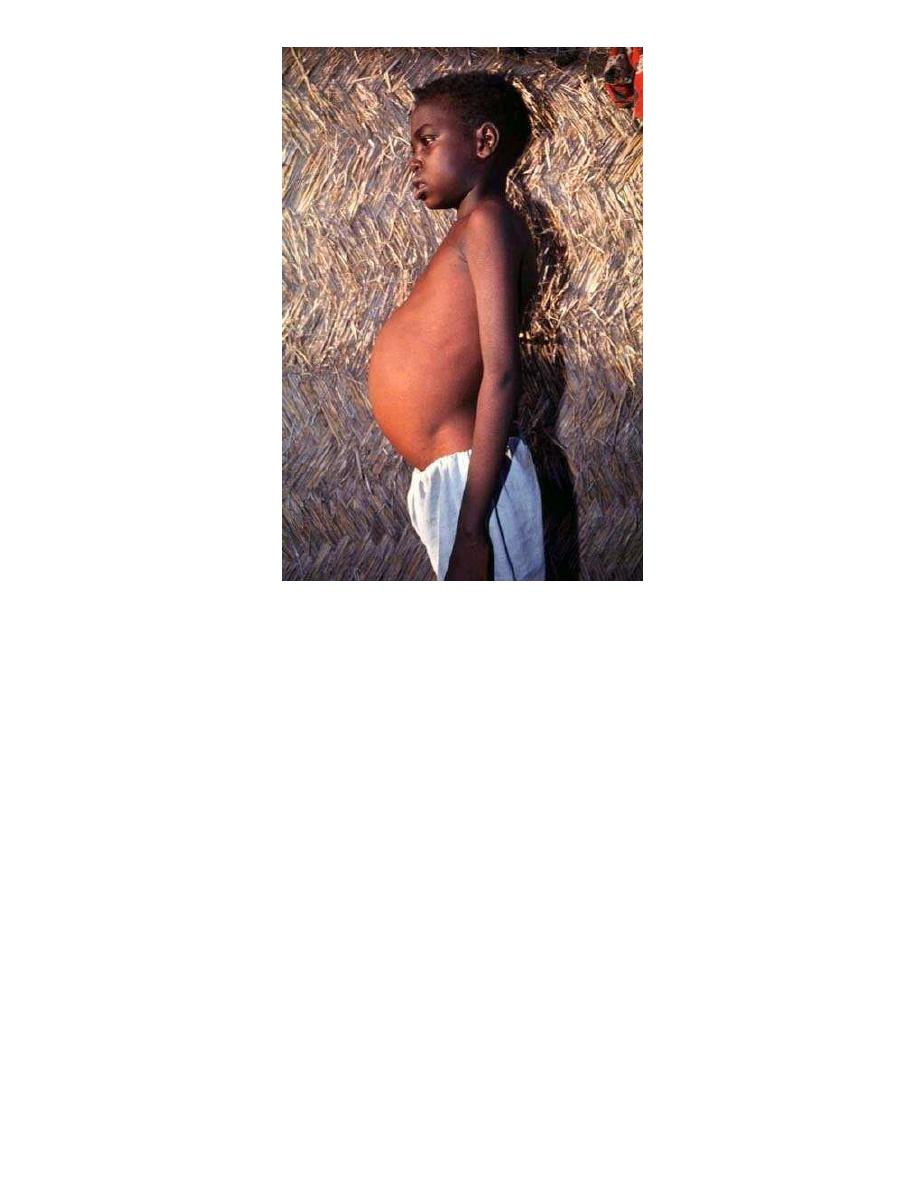
Proliferation of the RE cells, particularly of the spleen and liver
leads to massive hepatosplenomegaly (hypertrophy of these
organs).
The bone marrow may be involved, resulting in anemia and
leucopenia.
Hypoalbuminemia → oedema.
Gamma globulins may constitute 60% to 70% of the serum
proteins → reverse albumin/globulin ratio.
Splenomegaly with stasis of blood in the sinusoids may results in
increased destruction of both red and white blood cellsresulting in
anemia and leucopenia.
Recovery from leishmanial infection is generally believed to
involve interaction between T lymphocytes and macrophages.
Melanocyte stimulation → hyperpigmentation → so it is called
Kala-Azar which means black fever.
Thrombocytopenia →lead to severe mucosal bleeding, epistaxis
and ecchymosis.
Death occurs usually due to secondary infection as dysentery,
pneumonia and tuberculosis, due to disturbed immunity.
5
Post Kala-azar dermalleishmaniasis (PKDL) (Dermal
Leishmaniod)
It is a dermatotropic form of leishmaniasis, it is found in areas where L.
donovani is the causative agent of VL (Indian and African types) and
develops after 2-10 years from cure of VL.
Three clinical type of PKDL are encountered:
1- Depigmented macules.
2- Erythmatous pathches.
3- Nodular lesions.
Mucocutaneous Leishmaniasis
(Espundia)
6
L.D. bodies in tissue section
7
Patient with kala-azar, hepatospenomegaly