Sunday 29 / 3 / 2015
©Ali Kareem 2014-2015
Name
:
______________________________
Class
:
_______________________________
مكتب اشور لالستنساخ
DRUGS USED IN GIT
Lecture 8
Total lectures NO. 49
Dr. Samer Matloub
1
Dr. Samir Matloub
Acid peptic diseases include: gastroesophageal reflux disease (GERD),
peptic ulcers (DU & GU) and stress related mucosal injury.
Acid and pepsin versus mucosal resistance:
peptic ulcers are produced when the balance between (acid and pepsin) and
the mucosal resistance is disturbed (i.e. the balance between the aggressive
factors and the defensive mechanisms is disturbed). This is usually either by
↑aggressiveness or ↓mucosal resistance.
Usually the ↓in the mucosal resistance is the predisposing factor.
Both genetic and environmental factors play an important role in the
causation of ulcers… environmental factors include:
1. Helicobacter pylori infection (over 90% of peptic ulcers are caused by
infection with this organism) 2. NSAID 3.Smoking
Factors protecting the mucosa:
1. Ability to secrete mucus and bicarbonate ion (HCO
3
).
2. Impermeability to H
+
by the tight junctions between the mucosal cells and
their lipo-protein layers.
3. Blood flow (microvasculature) of mucosa.
4. Capacity of quick replacement of the damaged epithelial cells
PGs play a critical role in the protection of mucosa.
2
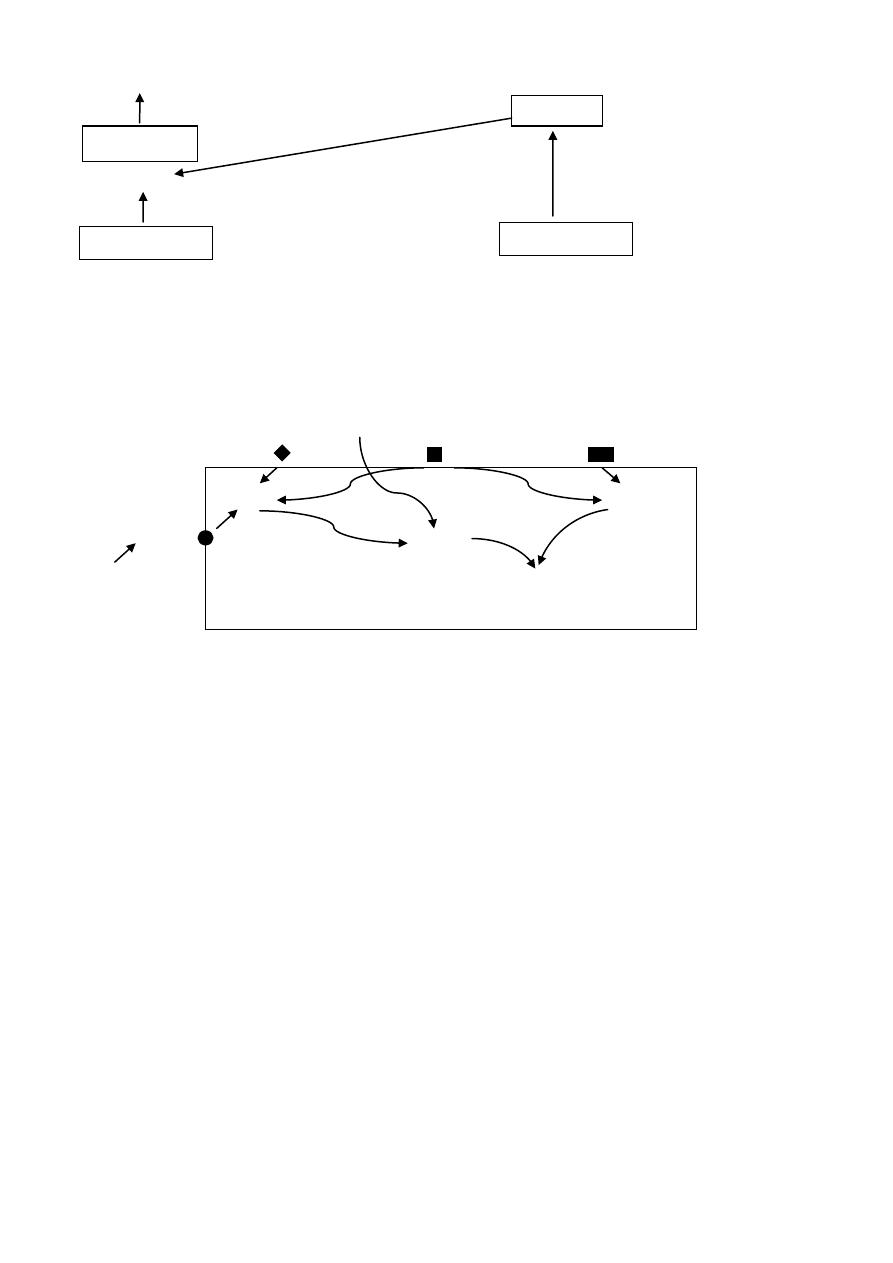
P cells G cells
+
+
ECL
_
_
D cells D cells
(Oxyntic mucosa) (Pyloric mucosa)
Endocrine and paracrine cells that stimulate or inhibit HCl secretion
From parietal cells directly or indirectly
Ach Hist. PGE
M
3
H
2
PGE
Model for
regulation of
CCK-B the parietal
cell secretion
Blood gastrin
H
+
K
+
Histamine is the most potent stimulant for gastric acid secretion.
Histamine by stimulating H
2
receptors results in activation of adenylate cyclase
thus increasing cAMP which leads to activation of protein kinase which in turn
will stimulate the proton pump leading to secretion of acid . ACh and gastrin on
the other hand increase Ca
+
and IP
3
, which will ↑gastric acid secretion. PG
s
are
inhibitory; they inhibit adenylate cyclase to inhibit acid secretion.
Proton pump is the final stage, so if we block it, all acid secretion whatever
is the stimulus will be blocked.
Gastrin
Histamine
Somatostatin
Somatostatin
+
IP
3
cAMP
Ca
+
kinase
Proton pump H-K ATPase
3
To approach a patient with peptic ulcer: drugs can alter the balance
towards healing and prevention of recurrence of ulcer in the following ways:
1. Reduction of acid secretion by:
a. Histamine H
2
receptor antagonists e.g.: cimetidine, ranitidine,
nizatidine, and famotidine.
b. Proton pump inhibitors e.g.: omeprazole, lansoprazole, pantoprazole,
rabeprazole, and esomprazole.
c. Antimuscarinic drugs: e.g.: pirenzepine, and telenzepine.
2. Neutralization of secreted acid by antacids e.g.: magnesium trisilicate,
aluminum hydroxide.
3. Enhancement of mucosal resistance by:
a. Protecting the base of peptic ulcer e.g.: bismuth chelate, sucralfate.
b. Cytoprotection (misoprostol) a PGE
1
analog.
c. Eradication
helicobacter
pylori
infection
by
antimicrobials
(amoxicillin, metronidazole, clarithromycin and tetracycline), we use
two Abcs preferably (clarithromycin and amoxicillin) + an
antisecretory agent (e.g. PPI) and
/
or bismuth.
1. Reduction of Acid Secretion:
A. Histamine H
2
-Receptor Antagonists:
They differ in structure:
Cimetidine contains imidazol ring.
Ranitidine contains phenol ring.
Famotidine and nizatidine contain thiazol ring.
All are equally effective in producing healing; however these drugs may differ in
their pharmacokinetics, potency and range of S/E.
Mechanism of Action:
H
2
receptors are present on the parietal cells. H
2
receptors blockers inhibit
gastric acid secretion by competitively blocking of H
2
receptors in the parietal
cells; therefore, they inhibit the direct action of histamine on gastric acid
secretion and inhibit the potentiating action of histamine on acid secretion
stimulated by gastrin and Ach .
H
2
-receptors blockers ↓basal acid secretion and nocturnal acid secretion more
than 90% and food stimulated acid secretion by ≈70%.
Both concentration and volume of H
+
will ↓and the concentration of pepsin is
also ↓ by the effect of H
2
-receptor blockers.
4
Pharmacokinetics:
All of them are well absorbed after oral dose.
Antacids ↓their absorption in about 10-20%.
Peak serum concentration is reached within 1-2hrs. after oral dose.
All cross BBB and placenta.
They are excreted in milk.
Bioavailability of cimetidine, ranitidine, and famotidine is decreased by 30-
50% by 1
st
pass elimination while nizatidine has no 1
st
pass metabolism,
bioavailability of nizatidine is 90-100% (they are excreted by liver and
kidney).
Efficacy is the same for all, but potency differs (different doses are used).
Ranitidine binds 4-10 times less avidly than cimetidine to P
450
.
Negligible interactions occur with nizatidine and famotidine.
Side Effects:
They are few in short term use. Minor side effects include headache,
dizziness, constipation, diarrhea, tiredness, and muscular pain.
Bradycardia and cardiac conduction defects may occur after I.V. injection
of cimetidine (due to blockade of H2 receptors in the heart).
Cimetidine has weak anti-androgenic effect and it ↑ prolactin secretion
leading to gynecomastia and sexual dysfunction in males other H
2
antagonists have no anti-androgenic effects.
In elderly, H
2
receptor antagonists may cause CNS disturbances including
lethargy, confusion, and hallucination.
Nizatidine may cause pruritis and rhinitis.
H2 antagonists may rarely cause blood dyscrasias and reversible
abnormalities in the liver chemistry
Main Uses of H
2
-receptor Antagonists:
1. GERD.
2. Peptic ulcer disease.
3. Non-ulcer dyspepsia.
4. Prevention of bleeding from stress related gastritis complicating burns,
hepatic failure, renal failure or trauma.
5. Healing of NSAID ulcers if the NSAID is discontinued.
6. Given before emergency surgery or labor to decrease risk of aspiration
pneumonia.
7. Combined with H1 blockers in the treatment of chronic urticaria
5
Cimetidine:
Is a well known inhibitor of hepatic digesting oxidizing enzyme system
P
450
, so it leads to↑ plasma level of many drugs like: warfarin, cyclosporine, Ca
+
channel blockers, Propranolol, theophylline, diazepam, sulfonyl ureas, TCA, and
antiarrhythmic like quinidine, mexiletine, Phenytoin, and lignocaine.It also
inhibits the excretion of procainamide by the renal tubules.
Treatment Course:
This course continues for 4-6 weeks and for gastric ulcer 6-8 weeks.
B. Muscarinic Antagonists:
These agents reduce basal secretion by about 50% but stimulated secretion is less
affected because of the unselectivity and the many inconvenient side effects like
dry mouth, blurred vision, constipation, tachycardia..etc.they are no more used.
The newer selective antagonists acting on (M
1
receptors) like pirenzepine,
telenzepine made them more useful.
These selective drugs have higher affinity for M
1
receptors and less affinity
to M
2
and M
3
receptors.
M
1
receptors are found in the intramural neurons and probably on the
enterochromaffin like cells which are responsible for secretion of histamine.
M
1
receptors antagonists are used in the treatment and prevention of
recurrence of peptic ulcer, but they are less effective than H
2
-receptors blockers.
Side Effects:
Are the same of atropine and selectivity is lost with increasing the dose.
Usual dose is 100-150 mg/d for pirenzepine (t
1/2
=11hrs), absorption from the
stomach is poor and it is excreted unchanged in urine and bile.
6
C. Proton Pump Inhibitors PPI:
Are omeprazole, lansoprazole, pantoprazole, rabeprazole, and esomprazole(it
is the S- isomer of omeprazole) , of which omeprazole is the prototype.
They act at the final stage or step of acid secretion, they inhibit the action
of H
+
-K
+
ATPase enzyme (i.e. the proton pump) found on apical membrane of
parietal cells in the stomach and no other place in the body, it catalyzes the
exchange of H
+
and K
+
in the process of acid secretion, so PPI antagonize all
stimulants of acid secretions.
These agents are substituted benzimidazole containing sulfinyl group, they
are lipophilic weak bases. At neutral PH, PPIs are chemically stable and are
devoid of inhibitory activity (prodrugs).
After intestinal absorption, they reach the parietal cells from the blood and
when they are in the canaliculi of parietal cells they become active where PH is
about 1. In the canaliculi they are protonated to form a cationic sulfinamide
which forms covalent bonds with the sulfhydryl group at critical sites of the
enzyme, they form a complex called (cystinyl sulfinamide complex) and this step
will irreversibly block the pump.
Omeprazole produces a profound and long lasting enzyme inhibition of
both basic and stimulated acid secretion, this is probably irreversible.
Single dose of 20mg of omeprazole decreases acidity by about 90% over
24hrs.
PPIs have minor direct anti-helicobacter properties.
Pharmacokinetics of PPIs:
Omeprazole must be given in enteric-coated formulations(capsules or
tablets), for it is degraded at low PH, t
1/2
=1.5hr, peak plasma level is reached
within 2-3hrs and the metabolite is inactive and excreted in the urine. It's
metabolized by cytochrome P
450
oxidase. Omeprazole is also available as a non-
enteric coated powder that contain NaHco3 that becomes immediate release
suspension when mixed with water,it is given by mouth or through entral tube
resulting in rapid absorption and rapid onset of acid inhibition.
Lansoprazole is also available as tablet formulation that disintegrates in
the mouth or maybe mixed with water and administrated via oral syringe or oral
tube.
Esomprazole, lansoprazole, pantoprazole are also available as I.V
formulation.
Rabeprazole due to its high PKa also have faster onset of acid inhibition.

7
Up to 3 – 4 days of daily medication are required before the full acid
inhibiting potential is reached. Similarly after stopping the drug 3-4 days are also
needed to regain full acid secretion.
The bioavailability of these agents is decreased by 50% by food hence these
drugs should be administrated 1hr before meals.
PPIs are inhibitors of P
450
oxidase too, but less than cimetidine
(pantoprazole, rabeprazole have no significant interactions)
.
The dose of PPIs should be reduced in patients with severe hepatic
disorders while compromised renal function patients are not affected by PPIs.
Uses of PPIs:
1. Duodenal and benign gastric ulcer.
2. Reflux esophagitis better than H
2
-blockers.
3. They are drugs of choice for hypersecretory conditions such as gastrinomas
and the Zollinger-Ellison syndrome.
4. They are drugs of choice for ulcers produced by NSAID, they can produce
healing inspite of continuation of the NSAIDs. It is also used to prevent
NSAID ulcers and their complication.
5. Prevention of rebleeding from peptic ulcer.
6. Prevention of stress related mucosal bleeding.
7. Non-ulcer dyspepsia.
Side Effects:
they are extremely safe
Nausea, vomiting, headache, diarrhea, constipation, abdominal pain and
rash occur but usually are uncommon. PPIs may impair the absorption of vit.
B12, calcium, zinc, and iron.
Omeprazole inhibits metabolism of warfarin, Phenytoin and diazepam but
much less than cimetidine.
Potential problems due to suppression of acid secretion by PPIs:
1. Suppression of acid secretion →↑gastrin release →leads to hyperplasia of
enterochromaffin cells →carcinoid tumors may develop (this has not been
documented in human).also hypergastrinemia leads to increased colonic
mucosal proliferation potentially promoting carcinogenesis (also not
documented in humans)
8
2. Decreased gastric acidity (prolonged hypochlorhydria) →bacterial
overgrowth in the stomach → these bacteria convert the ingested nitrates
into carcinogenic nitrites and N-nitroso amines. This has been
demonstrated in animals but not in human so they are safe to be used.
3. Patients infected with H. pylori, long term acid suppression → atrophic
gastritis and intestinal metaplasia which ↑the risk of adenocarcinoma (again
there is no evidence that this has occurred in human).
4. Enteric infection: ↑the risk of salmonella and shigella enteric infection
and increased risk of cl.difficile infection ,there is also increased tendency
of respiratory infections (increased risk of CAP and nosocomial infections).
2. Neutralization of the Acidity by Antacids:
Antacids are basic substances that ↓the acidity by neutralization of HCl
(antacids react with HCL to form salt and water) . the most commonly used
bases include: trisilicate, hydroxide,carbonate and bicarbonate ions.
They protect gastric mucosa from pepsin which is inactive above PH of 5.
The therapeutic efficacy and the S/E depend also on the metal with which
the base is combined( Al, Mg, Na).
The therapeutic efficacy also depends on the rate of dissolution, water
solubility, rate of reaction with the acid and rate of gastric emptying.
Aluminum hydroxide also ↓H. pylori colonization and stimulate
endogenous PGE production (some cytoprotective properties).
Continuous elevation of PH is limited by the rate of gastric emptying.
Ca
+
-containing antacids are not used anymore because it neutralizes the
acidity, but then causes hypersecretion of acid.
Bismuth containing antacids are also no more used.
Uses of Antacids:
1. Mainly used to in non-ulcer and to relieve ulcer symptoms especially in the
1
st
few days in the course of treatment with H
2
-receptor blocker.
2. Large amount of antacids are shown to accelerate healing of peptic ulcer,
but patient compliance is poor.
9
Individual Antacids:
(no single one is satisfactory and mixtures are often used)
A. Magnesium Oxide and Hydroxide:
React quickly but cause diarrhea, Mg trisilicate reacts slowly to form MgCl
2
which reacts with intestinal secretion to form the carbonate, the chloride being
released and reabsorbed. Systemic acid-base balance is thus not significantly
altered.
B. Aluminum Hydroxide:
Reacts with HCl to form AlCl
3
which reacts with intestinal secretion to form
insoluble salts especially phosphate. The chloride being released and reabsorbed,
thus acid-base balance is not affected. It may cause constipation,
hypophosphatemia, and it creates a risk of encephalopathy in patients with
chronic renal failure.
Usually Magnesium antacids are combined with aluminum hydroxide to
neutralize the effect on the bowel.
C. NaHCO
3
:
Reacts quickly with acids to produce Co2 and NaCl, Co2 causes bletching.
NaHCO3 is absorbed causing alkalosis. Na
+
absorption may exacerbate edema in
patients with heart failure or renal disease.
D. Ca
+
and Bismuth-Containing Antacids:
They should be avoided. Those containing Ca
+
may cause: rebound acid
hypersecretion, hypercalcemia, and alkalosis. Bismuth may be absorbed and
cause encephalopathy and arthropathy.
E. Alginic Acid (Gaviscon):
Combined with antacid to encourage the adherence of the mixture to the mucosa,
e.g.: for reflux esophagitis.
F. Dimethicone:
Added to antacids to reduce flatulence (anti-foaming agent), it is a silicone
polymer that ↓the surface tension.
Antacids may interfere with absorption of certain drugs as iron supplement,
digoxin, tetracycline, and antifungal agents, so the patient either stop using
these drugs or take it at least 2 hrs. after the antacids.
11
3. Enhancement of Mucosal Resistance:
A. Eradication of H. pylori by Antimicrobials:
70-90% of patients with peptic ulcer have antral gastritis.Experimental infection
of healthy volunteers with H. pylori produces gastritis. Its eradication protects
against relapse of peptic ulcer. It ↑the placebo healing rates and of anti-secretory
drugs. Eradication of H.pylori results in long term remission of the ulcer.
Regimens of Eradication:
1. Antimicrobial therapy (1-2 weeks) compromising 2 ABCs (antibiotics):
metronidazole with amoxicillin or clarithromycin or both (clarithromycin
and amoxicillin) + suppression of acid secretion (omeprazole). (this is the
most efficacious)
Note: the preferred 2 ABCs combination is clarithromycin and amoxicillin.
2. Bismuth based therapies: these are more complicated and less well
tolerated.
B. Protection of the Base of Peptic Ulcer:
(site protection)
I. Colloidal Bismuth:
Tripotassium dicitratobismuthate (de-nol), bismuth subsalicylate,
and bismuth dinitrate is also available.
Mechanism of Action:
1. Selectively chelates with protein material in the ulcer base
forming a coating that protects it from adverse influence of acid,
pepsin and bile.
2. It may also stimulate PGs, mucus, and HCO
3
secretion.
3. Bismuth has anti H. pylori action.
Conventional Bismuth triple therapy originally consisted of:
Bismuth + metronidazole and tetracycline.
11
Uses of Colloidal Bismuth:
1. For benign gastric and duodenal ulcer.
2. It is also used for acute diarrhea and prevention of traveler’s
diarrhea due to PG inhibition by salicylate also due to inhibition
of chloride secretion.Bismuth also binds enterotoxins accounting
for its benefit in treating and preventing traveler’s diarrhoea.
Adverse Effects:
Darkening of the tongue, teeth and stool for liquid formulation.
Systemically may cause encephalopathy and arthropathy.
II. Sucralfate:
It's a salt of sucrose complexed to sulphated Al(OH)
3
(basic Al. salt
of sucrose octasulphate or octaphosphate).
Mechanism of Action:
In acidic environment of stomach the Al. moiety is released and the
compound
(-ve
charged
sucrose
octasulphate)
binds
electrostatically to the (+ve charged protein molecule) that
transudate form damaged mucosa. The result is a viscous paste that
adheres to the ulcer base. It also inactivates pepsin and bile acids.
and also enhances mucosal repair (angiogenesis and granulation
tissue formation) by binding epithelial growth factor and fibroblast
growth factor. Also it enhances endogenous production of PGs and
thus enhances the mucosal defense and prevents recurrence.
Uses of Sucralfate:
For Benign gastric ulcer and chronic duodenal ulcer, it also
prevents bleeding from stress-related gastritis.
Efficacy is less than that of H
2
-receptor blockers
Maintenance treatment is effective for preventing relapse.
Side Effects: only constipation.
12
Drug Interactions:
As it acts in acidic medium only, it should not be given with
antacids.Sucralafate like antacids may bind to other medications
impairing their absorption.
C. Cytoprotection:
PGs and their Analogues:
Mechanism of Action:
1. It stimulates secretion of mucus and HCO
3
.
2. It maintains mucosal blood flow.
3. It prevents luminal H
+
back diffusion to mucosa.
4. It enhances the rate of cell replication in the mucosa to hasten
the repair of damaged epithelium.
The mentioned effects are considered as (cytoprotective effects).
PGE
2
and I
2
are potent inhibitors of gastric acid secretion.PGE
2
and
PGE
1
and F
2
α enhance the protective mechanisms in the stomach
and intestine.
Misoprostol:
Is a synthetic analogue of PGE
1
, that enhances mucosal resistance
(cytoprotection). Also Misoprostol has acid inhibitory action at
higher doses.Misoprostol inhibits acid secretion by reducing
histamine stimulated cAMP production.
Uses:
1. Used for the treatment of chronic gastric and duodenal ulcer due
to its inhibition of acid secretion (independent of cytoprotective
action).
2. Also it is used for prevention of NSAIDs-induced ulcer
(considered the drug of choice for this purpose, PPIs may be as
effective and better tolerated).
Side Effects:
Include diarrhea and abdominal pain.
Contraindications:
It is contraindicated in pregnant women because it may cause
abortion.

13
How can you treat a patient with peptic ulcer?
we can treat him by using one of the following:
1. The best treatment is by using proton pump triple therapy which consists
of:
a. PPI as omeprazole = one drug (antisecretory).
b. Two of the following = 2 ABCs: amoxicillin, metronidazole,
calrithromycin. The preferred: calrith. + amox.
2. We can use H
2
-receptor antagonist triple therapy but the first is better.
3. Also there is quadriple therapy used when PPI triple therapy is not
successful and it consists of: 2 antibiotics + 2 adjunctive: bismuth + PPI
Antibiotics are used for 1-2weeks with the PPIs and then you continue with
the PPI treatment for 4-6 weeks.
Done by
Ali Kareem