Sunday 8 / 3 / 2015
©Ali Kareem 2014-2015
Name
:
______________________________
Class
:
_______________________________
مكتب اشور لالستنساخ
ANTI-MICROBIAL DRUGS
Lecture 10
Total lectures NO. 42
Dr. Haidar Al-Shakarchi
Pharmacology
Anti-Microbial Drugs 4
1
Dr. Haidar Al-Shakarchi
Lec. 10
Protein synthesis inhibitors:
A number of antibiotics exert their antimicrobial effects by targeting the bacterial
ribosome, which has components that differ structurally from those of the
mammalian cytoplasmic ribosome. The mammalian mitochondrial ribosome,
however, more closely resembles the bacterial ribosome. Thus although drugs that
interact with the bacterial target usually spare the host cells, high levels of drugs
may cause toxic effects as a result of interaction with mitochondrial ribosomes.
Protein synthesis inhibitors include:
1. Tetracyclines
2. Aminoglycosides
3. Macrolides
4. Chloramphenicol
5. Clindamycin
6. Quinupristin / dalfopristin
7. Linezolid
Tetracyclines:
The tetracyclines are a group of closely related compounds that, as the name
implies, consist of four fused rings with a system of conjugated double bonds.
Mechanism of action:
Tetracyclines enter microorganisms in part by passive diffusion and in part by an
energy-dependent process of active transport.
Susceptible cells concentrate the drug intracellularly. Once inside the cell,
tetracyclines bind reversibly to the 30S subunit of the bacterial ribosome, blocking
the binding of aminoacyl-tRNA to the acceptor site on the mRNA-ribosome
complex. This prevents addition of amino acids to the growing peptide.
Classification:
Tetracyclines are classified as short action (chlortetracycline and tetracycline),
intermediate acting (demeclocycline), or long acting (doxycycline and
minocycline) based on serum ½ lives.
Pharmacology
Anti-Microbial Drugs 4
2
Dr. Haidar Al-Shakarchi
Lec. 10
Antibacterial spectram:
Tetracyclines are broad spectrum bacteriostatic antibiotics that inhibit protein
synthesis. They are active against many gram +ve and gram –ve bacteria,
including anaerobes , spirochetes, mycoplasma, chlamydiae and rickettsiae; and
against some protozoa. The antibacterial activities of most tetracyclines are similar
except that tetracycline-resistant strains may remain susceptible to doxycycline or
minocycline.
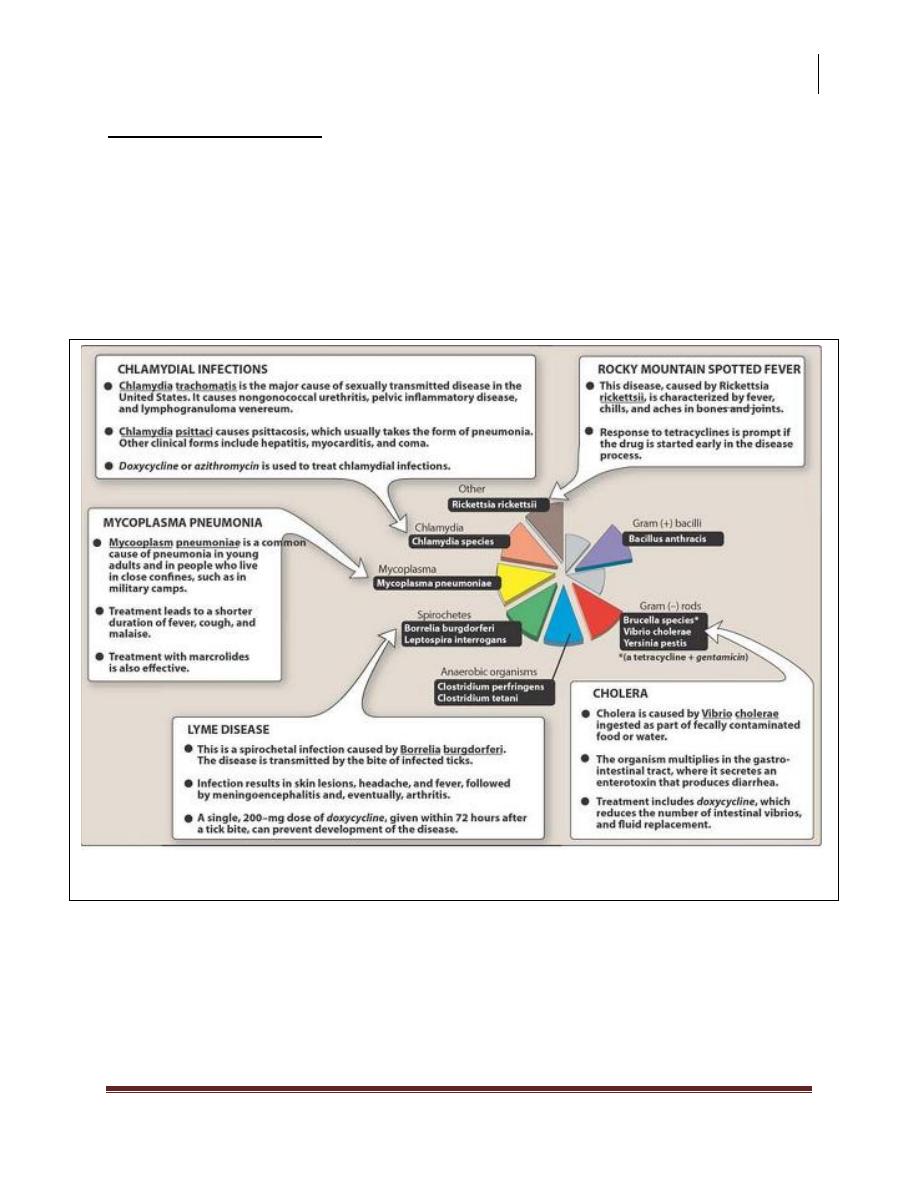
Typical therapeutic applications of tetracyclines.
Pharmacology
Anti-Microbial Drugs 4
3
Dr. Haidar Al-Shakarchi
Lec. 10
Resistance:
Three mechanisms of resistance to tetracycline have been described:
1. Inability of the organism to accumulate the drug.This is accomplished by
Mg-depended active efflux of the drug.
2. Enzymatic inactivation of the drug .
3. The production of bacterial proteins that prevent tetracyclines from binding
to the ribosome.
Pharmacokinetics:
1. Absorption: All tetracyclines are adequately but incompletely absorbed after
oral ingestion. However, taking these drugs concomitantly with dairy foods
decreases absorption due to the formation of non-absorbable chelates with
calcium ions. Non-absorbable chelates are also formed with other divalent
and trivalent cations (e.g those found in magnesium and aluminum antacids
and in iron preparations).Doxycycline and minocycline are almost totally
absorbed on oral administration.
2. Distribution:
Tetracyclines are distributed widely to tissues and body fluids. They bind to
tissues undergoing calcification e.g teeth and bones. Although all
tetracyclines enter the CSF, levels are insufficient for therapeutic efficacy,
except for minocycline. Minocycline enters the brain in the absence of
inflammation and also appear in tears and saliva. Although useful in
eradicating the meningococcal carrier stare, minocycline is ineffective for
CNS infections. All tetracyclines cross the placental barrier, and concentrate
in fetal bones and dentition.
3. Fate:
All the tetracyclines are metabolized in the liver and conjugated to form
soluble glucuronides. The parent drug and/or its metabolites are secreted into
the bile. Most tetracyclines are reabsorbed in the intestine via the
enterohepatic circulation and enter the urine by glomerular filtration. Unlike
other tetracyclines, doxycycline can be employed for treating infections in
renally compromised patients, because it is preferentially excreted via the
bile into the feces. Tetracyclines are also excreted in breast milk.
Pharmacology
Anti-Microbial Drugs 4
4
Dr. Haidar Al-Shakarchi
Lec. 10
Clinical uses:
1. A tetracycline is the drug of choice in infections with mycoplasma
pneumonia, chlamydiae and rickettsiae .
2. They are used in combination regimens to treat gastric and duodenal
ulcer disease caused by helicobacter pylori.
3. Tetracyclines rapidly stop the shedding of vibrios in cholera, but
tetracycline resistance has appeared during epidemics.
4. A tetracycline usually in combination with an aminoglycosides is
indicated for plague , tularemia and brucellosis.
5. A tetracycline is indicated in the treatment of some spirochetes as lyme
disease and leptospirosis .
6. Tetracyclines are sometimes employed in the treatment of protozoal
infections e.g those due to Entamoeba histolytica or Plasmodium
falciparum.
7. Minocycline can eradicate the meningococcal carrier state.
8. Demeclocycline inhibits the action of ADH in the renal tubule and has
been used in the treatment of inappropriate secretion of ADH
9. They may be employed in serious gram +ve and gram –ve infections.
Adverse effects:
1. Gastric discomfort: Epigastric distress commonly results from irritation of
the gastric mucosa and is often responsible for non-compliance in patients
treated with these drugs.
2. Effects on calcified tissue: Deposition in the bone and primary dentition
occurs during calcification in growing children. This causes discoloration
and hypoplasia of the teeth and a temporarily stunting of growth.
3. Fatal hepatotoxicity: This side effect has been known to occur in pregnant
women who received high doses of tetracyclines, especially if they were
experiencing pyelonephritis.

Pharmacology
Anti-Microbial Drugs 4
5
Dr. Haidar Al-Shakarchi
Lec. 10
4. Phototoxicity: Phototoxicity such as severe sunburn, occurs when a patient
receiving a tetracycline is exposed to sun or ultraviolet rays. This toxicity is
encountered most frequently with tetracycline, doxycycline, and
demeclocycline.
5. Vestibular problems: Dizziness, nausea and vomiting occur particularly with
minocycline which concentrates in the endolymph of the ear. Doxycycline
may also cause vestibular effects.
6. Pseudotumor cerebri: Intracranial hypertension characterized by headache
and blurred vision may also cause vestibular effects.
7. Superinfections: Overgrowth of candida in the vagina or resistant
staphylococci in the intestine may occur. Pseudomembranous colitis due to
overgrowth of clostridium difficile has also been reported.
8. Contraindications: Renally impaired patients should not be treated with any
of the tetracyclines except doxycycline. Accumulation of tetracycline may
aggravate preexisting azotemia by interfering with protein synthesis, thus
promoting amino acid degredation. The tetracyclines should not be
employed in pregnant or breast feeding woman or in children under 8 years
of age.
Aminoglycosides:
Aminoglycosides antibiotics had been the mainstays for treatment of serious
infections due to aerobic gram –ve bacilli. The group includes streptomycin,
neomycin, kanamycin, amikacin, gentamicin, tobramycin, netilmicin.
Neomycin and kanamycin are now largely limited to tropical or oral use. All
members of this family are believed to inhibit bacterial protein synthesis.
Mechanism of action:
Pharmacology
Anti-Microbial Drugs 4
6
Dr. Haidar Al-Shakarchi
Lec. 10
Susceptible gram –ve organisms allow aminoglycosides to diffuse through
porin channels in their outer membranes. These organisms also have an oxygen
dependent system that transports the drug across the cell membrane. The
antibiotic then binds to the 30S ribosomal subunit and distorts its structure,thus
interfering with the initiation of protein synthesis.It also allows misreading of
the mRNA, causing mutations or premature chain termination. Polysomes
become depleted.
Resistance: resistance can be caused by:
1. Decreased uptake of the drug when the oxygen dependent transport system
or porin channels are absent.
2. An altered 30S ribosomal subunit aminoglycoside-binding site that has a
decreased affinity for the drug.
3. Plasmid associated synthesis of enzymes (e.g. acetyltransferase,
nucleotidyltransferase, phosphotransferase) that modify and inactivates
aminoglycoside antibiotics. Each of these enzymes has its own
aminoglycoside specificity; therefore, cross resistance is not an invariable
rule. Amikacin is less vulnerable to these enzymes.
Antibacterial spectrum:
The aminoglycosides are effective in the empirical treatments of infections
suspected of being due to aerobic gram –ve bacilli including Pseudomonas
aeuroginosa. To achieve an additive or synergistic effect, aminoglycosides are
often combined with a β-lactom, or vancomycin, or a drug active against anaerobic
bacteria. The aminoglycosides synergize with β-lactom antibiotics, because the
latter’s action on cell wall synthesis, which enhances diffusion of the
aminoglycosides in the bacterium. All aminoglycosides are bactericidal, some
therapeutic applications of four commonly used aminoglycosides – amikacin,
gentamicin, tobramycin and streptomycin are listed below:
1. Enterococcus species: gentamicin or streptomycin plus vancomycin or a β-
lactom, such as penicillin-G

Pharmacology
Anti-Microbial Drugs 4
7
Dr. Haidar Al-Shakarchi
Lec. 10
2. Pseudomonas aeuroginosa: infections in immunocompromised patients and
in burn victims: tobramycin in combination with an anti-pseudomonal
penicillin, such as piperacillin or ticarcillin.
3. Klebsiella species: an aminoglycoside e.g. gentamicin plus an anti-
pseudomonal penicillin .
4. Yersinia pestis, Francisella tularensis, and brucella species: gentamicin or
streptomycin plus doxycycline.
Pharmacokinetics:
The highly polar structure of the aminoglycosides prevents adequate absorption
after oral administration. Therefore, all aminoglycosides (except neomycin)
must be given parenterally to achieve adequate serum levels. The severe
nephrotoxicity associated with neomycin precludes parenteral administration,
and its current use is limited to topical application for skin infections or oral
administration to prepare the bowel prior to surgery. The bactericidal effect of
aminoglycosides is concentration and time dependent; that is, the greater the
concentration of drug, the greater the rate at which the organisms die. They also
have a post antibiotic effect. Because of these properties, once-daily dosing can
be employed. The exceptions are pregnancy, neonatal infections, and bacterial
endocarditis, in which these agents are administered in divided doses every 8
hrs.
Aminoglycoside levels achieved in most tissues are low, and concentrations in
the CSF are inadequate, even when the meninges are inflamed. Except for
neomycin, the aminoglycosides may be administered intrathecally or
intraventricularly. High concentrations accumulate in the renal cortex and in the
endolymph and perilymph of the inner ear, which may account for their
nephrotoxic and ototoxic potential. All aminoglycosides cross the placental
barrier and may accumulate in fetal plasma and amniotic fluid.
All aminoglycosides are rapidly excreted into the urine, predominantly by
glomerular filtration. Accumulation occurs in patients with renal failure and
requires dose modification.
Pharmacology
Anti-Microbial Drugs 4
8
Dr. Haidar Al-Shakarchi
Lec. 10
Adverse effects:
It is important to monitor plasma levels of aminoglycosides to avoid
concentrations that cause dose related toxicities. When drugs are administrated
2-3 times daily, both peak (1/2 – 1 hrs. after infusion) and trough (before the
next dose) levels are measured. When once-daily dosing is employed, only
trough concentrations are monitored. All aminoglycosides are ototoxic and
nephrotoxic. Ototoxicity and nephrotoxicity are more likely to be encountered
when therapy is continued for more than 5 days, at higher doses, in the elderly,
and in the setting of renal insufficiency:
1. Ototoxicity: ototoxicity can manifest itself either as auditory damage (mostly
with neomycin, kanamycin, and amikacin), or as vestibular damage (mostly
with streptomycin and gentamicin). Ototoxicity is directly related to high
peak plasma levels and the duration of treatment. Patients simultaneously
receiving another ototoxic drug, such as loop diuretics or cisplatin are
particularly at risk. Deafness may be irreversible, and has been known to
affect fetuses in utero.
2. Nephrotoxicity: retention of the aminoglycosides by the proximal tubular
cells disrupts calcium mediated transport processes, and this results in
kidney damage ranging from mild, renal impairment to severe, acute tubular
necrosis, which can be irreversible. Neomycin, tobramycin, and gentamicin
are the most nephrotoxic. Concomitant use with loop diuretics, vancomycin,
or amphotericin can potentiate nephrotoxicity.
3. Neuromuscular paralysis: this side effect most often occurs after direct
intraperitoneal or intrapleural application of large doses of aminoglycosides.
The mechanism responsible is a decrease in both the release of Ach from
prejunctional nerve endings and the sensitivity of the post-synaptic site.
Patients with myasthenia gravis are particularly at risk.
4. Allergic reactions: contact dermatitis is a common reaction to topically
applied neomycin.
Pharmacology
Anti-Microbial Drugs 4
9
Dr. Haidar Al-Shakarchi
Lec. 10
Some adverse effects of amino-glycosides.
Done by
Ali Kareem