Sunday 19 / 10 / 2014
@Ali Kareem 2014-2015
Name
:
______________________________
Class
:
_______________________________
مكتب اشور لالستنساخ
CHOLINERGIC SYSTEM
Lecture 3
Total lectures NO. 5
Dr. Samer Matloub
16
Lec:3
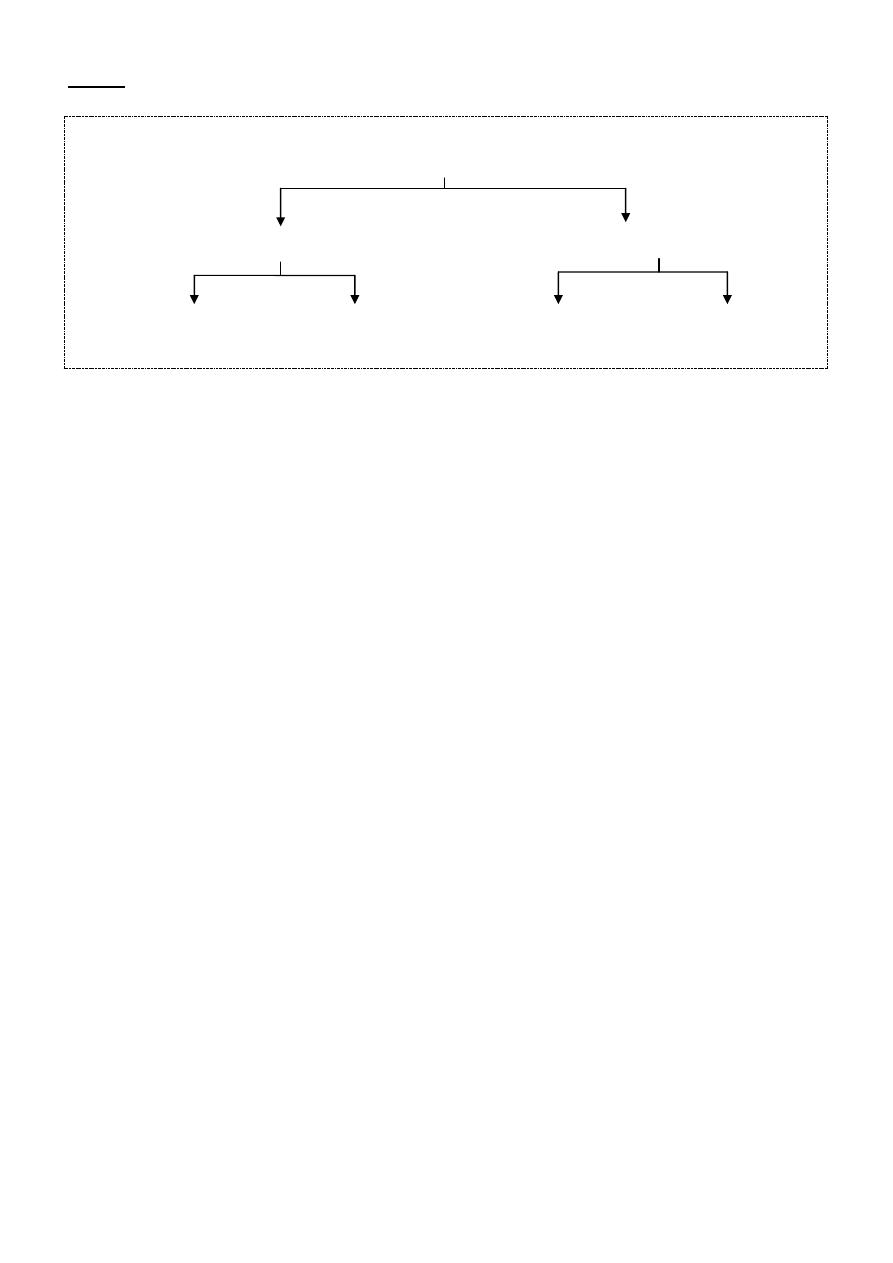
Cholinergic Antagonists
"cholinoceptor blockers"
Anti Muscarinics
Anti Nicotinics
M1 selective
Nonselective Ganglion blockers N-M blockers
Muscarinic Antagonists:
These agents (e.g. Atropine & Scopolamine) act as competitive
"surmountable" pharmacological antagonists.
They block muscarinic receptors causing inhibition of all muscarinic
functions and their blocking effects are overcome by increasing the
concentration of Ach or by other muscarinic agonists.
These drugs also block the few exceptional sympathetic neurons that are
cholinergic "e.g. sweat gland" .
These drugs have little or no effect on the autonomic ganglia or the N-M
junction.
Most of these drugs are nonselective for muscarinic receptors except for
pirenzepine and telenzepine which are M1 selective (used in treatment
of peptic ulcers).
The action of muscarinic blockers (e.g. atropine) is mostly predictable
effects derived from cholinoceptor blockade.
17
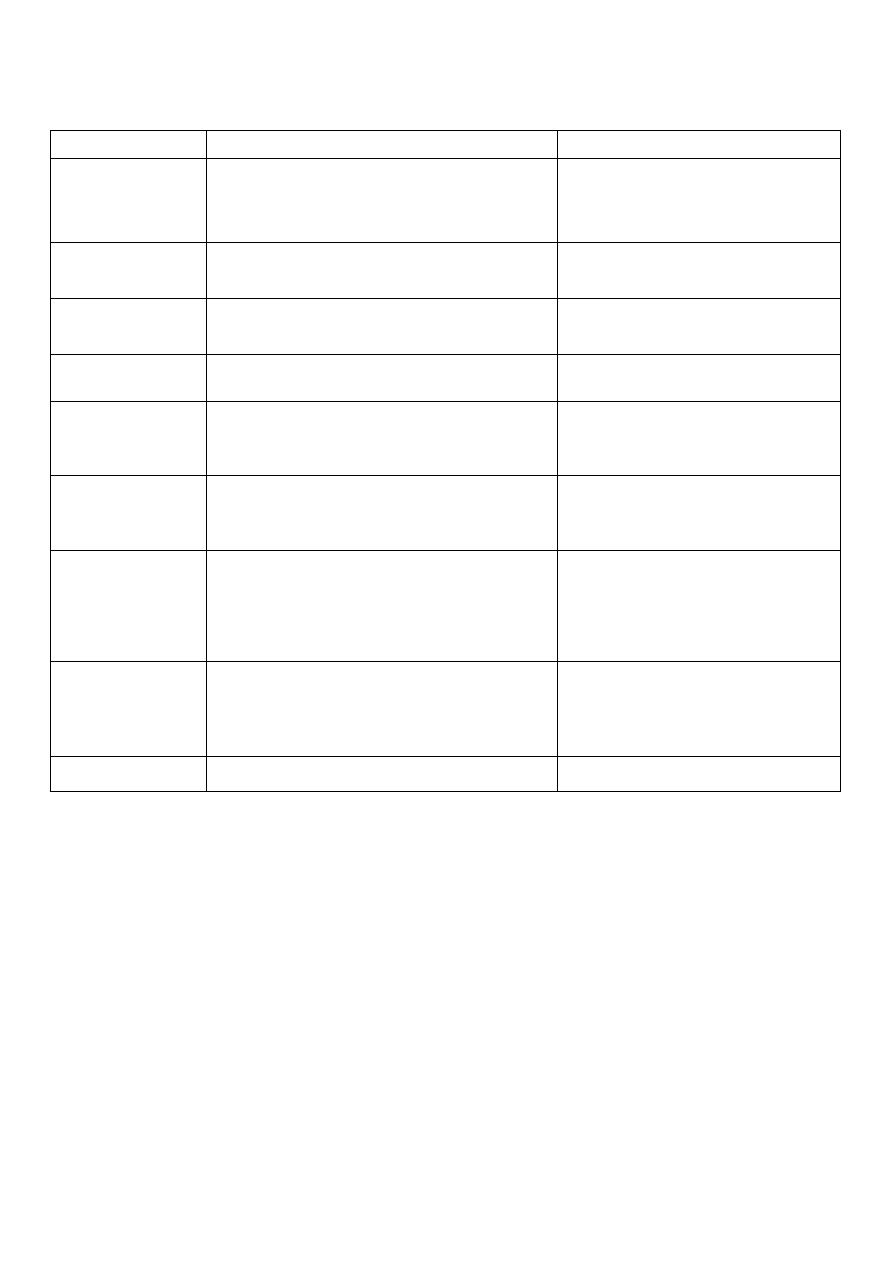
Effects of muscarinic blocking drugs:
Organs
Effect
Mechanism
CNS
Sedation, anti motion sickness
action, anti parkinsonian action,
amnesia, delirium.
Block of MRs, unknown
subtype.
Eye
Mydriasis, cycloplegia (paralysis
of accommodation)
Block of M3 Rs
Bronchi
Bronchodilatation esp. if
constricted.
Block of M3 Rs
GIT
Relaxation, slowed peristalsis.
Block of M1,M3 Rs
Genito-
urinary tract
Relaxation of the bladder wall,
Urinary retention.
Block of M3 Rs
Heart
Initial bradycardia, esp. at low
doses then tachycardia.
Tachycardia from block of
M2 R in the heart.
Blood vessels
Block of muscarinic
vasodilatation , not manifested
unless a muscarinic agonist is
present.
Block of M3 Rs on
endothelium of B.Vs
Glands
Marked reduction of salivation,
lacrimation,sweating, less
reduction of gastric secretion.
Block of M1, M3
receptors.
Skeletal m.
none
Notes:
CNS effects are less predictable. CVS effects at therapeutic doses include an
initial slowing of the heart rate caused by a central mechanism (medullary
stimulation of the cardiac inhibitory centre) or more likely by presynaptic
vagal effects (blocking the presynaptic M1R on vagal post ganglionic fibers
that normally limit Ach release in the SA node).this slowing is followed by
tachycardia and decrease AV conduction time as it would be predicted from
peripheral vagal blockade (blocking of M2 receptors in the heart).

18
The effect on the blood vessels include blockade of the endothelial
muscarinic receptors that mediate vasodilatation and also vasodilatation
produced by sympathetic cholinergic nerve stimulation to the skeletal muscle
vascular bed. However there is a little effect on blood pressure of normal
persons. At toxic doses atropine may cause cutaneous vasodilatation in the
upper part of the body, the mechanism is unknown.
Clinical uses of muscarinic antagonists:
Note:
topical activity (the ability to enter the eye after conjuctival
administration) and similar ability to cross lipid barrier (e.g. BBB) is
important in determining the usefulness of several antimuscarinics often used
in ophthalmology and in Parkinsonism. In contrast the antimuscarinic drugs
used for their antisecretory or antispasmodic actions in the gut or in the
bronchi are often selected for minimum CNS activity (these drugs may
incorporate quaternary amine group to limit penetration to the CNS).
1-CNS:
- Motion sickness: scopolamine is the standard therapy in motion
sickness.
-
Parkinsonism: Benztropine, biperidine, trihexphenidyl (these drugs
are mainly effective to control tremors).
Benztropine is sometimes used to treat acute dystonias caused by
antipsychptic drugs.
2- Eye:
are used to dilate the pupil (mydriasis) and to paralyze
accommodation (cycloplegia).
Drugs used to this purpose include (in descending order of duration of
action).
Atropine < 72 hours, homatropine (24 hrs.), cyclopentolate (2-12 hrs.),
tropicamide (0.5-4 hrs.).

19
3-Bronchi:
Parentral atropine has been used to reduce airway secretion
during surgery. Ipratropium a quaternary agent is used by inhalation to
reduce bronchoconstriction in asthma and COPD (chronic obstructive
pulmonary disease). This drug has very few antimuscarinic effects outside the
lung because it is rapidly metabolized and poorly absorbed. it is less effective
than B
2
agonists in this regard.
4- CVS:
Parentral atropine and similar antimuscarinics are used to H.R
in cases of bradychardia due to depression of the SA node or the AV node
function (e.g. after myocardial infarction (MI) and in persons with
hyperactive carotid sinus reflexes).
5- Gut:
Atropine, methscopolamine and propantheline were used in the
past in acid peptic disease to reduce acid secretion (volume, amount of acid
and pepsin and mucin are all reduced but large doses are required).
These drugs are less effective than the H2 antagonist (e.g. cimitidine)
and produce frequent side effects.
Pirenzepine and telenzepine are M
1
, selective antagonist, may be more
useful in peptic ulcer (M
1
receptors are present on the ECL cells and not
on parietal cells which possess M
3
R.)
Muscarinic antagonist e.g. glycopyrolate, dicyclomine, hyoscin butyl
bromide and methscopolamine can be used to reduce cramping
(antispasmodic) and hepermotility in transient diarrheas but
diphenoxylate (an opioid) is more effective.
6- Urinary system:
Oxybutynin, glycopyrolate, dicyclomine are used
in the treatment of spasm and urgency induced by mild inflammation e.g.
(cystitis), surgery and neurological conditions but can precipitate urinary
retention in elderly men with benign prostatic hyperplasia (Bph).
Tolterodine (is an M
3
selective antimuscarinic) is used in adult with
urinary incontinence.

21
7- Other uses
: As an antidote for cholinergic agonists atropine is used in
the treatment of organophosphorus poisoning and some types of mushroom
poisoning.Atropine because of its ability to enter CNS is used to block the
effect of excess Ach resulting from inhibition of ChE by drugs such as
physostigmine.
Atropine:
Is the protypical non selective muscarinic blocker , It is an alkaloid found
in atropa belladonna. It is a tertiary amine (lipid soluble and crosses to the
CNS). It is eliminated partly by metabolism and by renal excretion t ½ is 2
hrs., Duration of action is 4-8 hrs except in the eye where the effect lasts for
72 hrs. or longer. the antidote in atropine poisoning is physostigmine.
Scopolamine (hyoscine):
Is another belladonna alkaloid similar to atropine but has a longer duration
of action and greater action on the CNS. It produces sedation. Its use is limited
for the prevention and treatment of motion sickness.
Adverse effects and toxicity:
Most of the adverse effects are predictable antimuscarinic effects, although
there are some unpredictable actions.
Predictable include: Dry mouth, blurred vision, tachycardia, constipation,
hyperthermia due to blockage of thermo-regulatory sweating also called
atropine fever (this occurs esp. in infants which may be dangerous.)
Atropine toxicity is described as feeling as dry as a bone because
sweating, salivation and lacrimation are reduced or stopped. In the elderly
atropine may cause acute angle-closure glaucoma and urinary retention esp.
in patients with Bph (benign prostatic hyperplasia)
Unpredictable include:
1- CNS toxicity which includes: sedation, amnesia and delirium or
hallucination (described as mad as a hatter) convulsions may also occur.

21
2- CVS which include: intra ventricular conduction block and cutaneous
vasodilatation of the vessels of head, neck, arms and trunk (atropine flush)
which is described as red as beet, which may be diagnostic.
Contra indications:
These drugs should be cautiously used in infants (hyperthermia) these
drugs are relatively CI in patients with glaucoma and in men with Bph.