
Vitamins

Vitamins
organic substances with key roles in certain
metabolic pathways; they are required in small
amounts in food because they are not
synthesized in the body .
body stores
is varied
vit.B
12
and vit.A need years to deplete their
stores.
Folate (vit.B
9
) and thiamine (vit.B
1
) need
weeks to deplete their stores.

Vitamins
Vitamins are
fat-soluble
(vitamins A, D, E and K)
water-soluble
(vitamins of the B
complex group and vitamin C).

Thiamin (vitamin B1)
Function
thiamin pyrophosphate (TPP), is an essential
cofactor in carbohydrate metabolism.
1. Involved in the oxidative decarboxylation of
acetyl CoA in mitochondria.
2 .In the Krebs cycle, is the key enzyme for the
decarboxylation of α-ketoacid.
3. Has role in peripheral nerve conduction (unknown
mech.)

Thiamin (vitamin B1)
Source
many foodstuffs
cereals, legumes
pork, as well as beef meat.
Coffee and tea (have anti-thiamine factors),
and raw fish (has thiaminase), all decrease
the vitamin .
milled and polished rice have little vit.B
1
.

Thiamin (vitamin B1)
Deficiency
1. Cells cannot metabolize glucose aerobically
this likely to affect the nervous system .
2 .There is accumulation of pyruvic and lactic
acids, which produce vasodilatation and
increased cardiac output.

Thiamin (vitamin B1)
Causes
1. poor dietary intake, in severe prolonged
hyper -emesis gravidarum
3 . where the only food consumed is polished
rice
2 . In chronic alcohol-dependent patients
4. Chronic illness as cancer

Thiamin (vitamin B1)
Clinical feature
Body stores are small and signs of deficiency
quickly develop with inadequate intake.
• Non specific at early stage : anorexia, fatigue,
irritability
• Two clinical forms
Dry beriberi
Wet beriberi

Thiamin (vitamin B1)
• Dry beriberi
1. peripheral neuropathy:
Sensory and motor
pain and parasthesia
2.Cerebral involvement :
Wernicke-encephalopathy
mental impairment
cerebellar ataxia
ophthalmoplegia
horizontal nystagmus
Thiamin (vitamin B1)
Korsakoff syndrome
:
loss of new memory
confabulation
• Wet beriberi
high output failure (3 months)
peripheral neuropathy

Thiamin (vitamin B1)
Diagnosis
measurement of the circulating thiamin
concentration
enzymatic assay of transketolase activity.

Thiamin (vitamin B1)
Treatment
• 100 mg/d of thiamine given parenterally for 7
days, followed by 10 mg/d orally until
complete recovery.
• Cardiovascular and ophthalmoplegic
manifestations improve within 24 h .Others
gradually clear
• Wernicke-Korsakoff syndrome may be
permanent or persist for several months.
• VitB1 must be replaced in alcoholic patient
after feeding

Riboflavin (B2 )
• Riboflavin is a flavoprotein that is a cofactor for
many oxidative reactions in the cell for energy
production.
Source
widely distributed all plant and animal sources
(main source) cereals, milk, dairy products
(good source) legume, Meat , fish , egg

Riboflavin (B2 )
Deficiency causes
almost is dietary with other VitB
Clinical manifestations
1. Mucocutaneous lesion
angular stomatitis or
cheilosis
red inflamed tongue
2. Seborrhoeic dermatitis
(face around the nose)
scrotum or vulva.

Riboflavin (B2 )
3.Conjunctivitis with vascularization of the
cornea .
4. Anemia
5. Personality changes
Diagnosis
serum or urinary level
Treatment
Riboflavin 10 mg daily, usually given as the
vitamin B complex.

Niacin (B3)
two chemical forms, nicotinic acid, nicotinamide
Function
Many oxidative steps in the production of
energy and in DNA repair
source
many foodstuffs: plants, meat and fish.
can be synthesized in humans from Eggs,
and milk contain tryptophan.

Niacin (B3)
Causes of deficiency
1. Dietary deficiency (corn based diet)
2. In malabsorption (rare)
3. In Hartnup's disease. (Tryptophan renal, or GIT
absorption defect)

Niacin (B3)
4. In alcohol-
dependent patients (who don’t eat)
5. In the carcinoid syndrome (tryptophan is
needed for serotonin).
6.Isoniazid therapy ( lead to a deficiency of
vitamin B6, which is needed for the synthesis
of nicotinamide from tryptophan).

Niacin (B3)
Clinical features
Pellagra :
dermatitis
,
diarrhoea
and
dementia
1. early non specific symptoms anorexia,
weakness, irritability
2. bright red glossitis and angular stomatitis
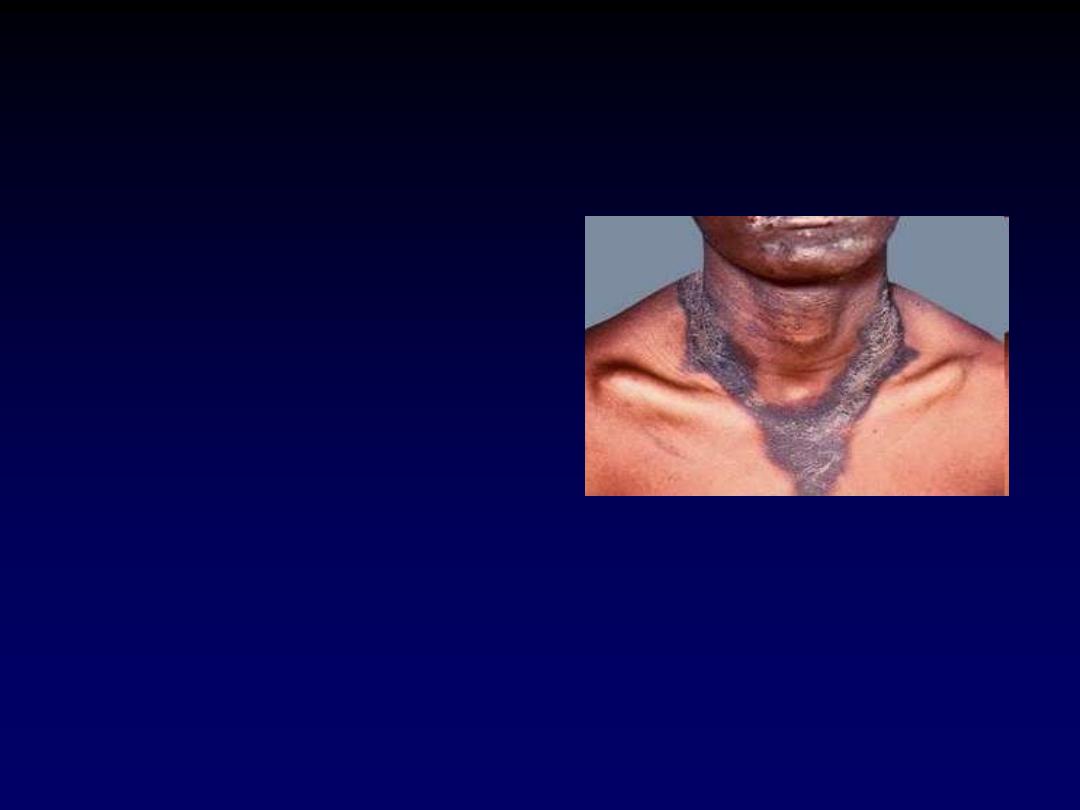
Niacin (B3)
3. Dermatitis
Scaling pigmented skin rash
exposed to sunlight
(casal s necklace)
4. Diarrhea
proctitis
esophagitis
(non infective)
5. Dementia
milder cases cause depression.
severe cases cause hallucinations and
acute psychosis

Niacin (B3)
Diagnosis
assesing the urinary excretion of the 2 pyridone
and 2 methyl nicotinamide.
Treatment
Nicotinamide 300 mg daily by mouth with a
maintenance dose of 50 mg daily
NB
. VitB3 used in RX of hyperlipidemia

Vitamin B6
• Vitamin B6 exists as pyridoxine, pyridoxal and
pyridoxamine.
Function
• cofactor of many enzymes involved in the
metabolism of many amino acids.
• neurotransmitters synthesis
• heme synthesis.
• Vitamine metabolism as niacin

Vitamin B6
Source
is found widely in plant and animal foodstuffs.
Cause of deficiency
1.
Dietary deficiency
( isolated extremely
rare)
2.
Some drugs
isoniazid
hydralazine
methyldopa
penicillamine
interact with pyridoxal phosphate, producing
the deficiency.

Vitamin
B6
Clinical features
1. mucosal changes
2. The peripheral neuropathy
personality changes
depression, confusion
3. Microcytic hypochromic anaemia
Treatment
100 mg daily should not be exceeded.
NB
. VitB6 used as antiemetic especially in the
pregnancy

Vitamin B12
function
• cofactor for activation of the folate
(demethylation of methyl THF polyglutamate
to THF, with methylation of homocysteine to
methionine).
• Coenzyme for many synthetic reactions
Source
• animal sources meat, fish, eggs and milk, but
not in plants.
• The storage may take 2 years or more after
absorptive failure before
deficiency develops.
(total stored amount in the adult is about 2-5
mg).

Vitamin B12
Deficiency
1.
Low dietary intake
, Vegans
2.
Impaired absorption
• Stomach : Pernicious anaemia
Gastrectomy
Congenital deficiency of
intrinsic factor
• Pancreatic insufficiency
• Small bowel: ilea disease or resection
Bacterial overgrowth
Diphyllobothrium latum (fish
tapeworm).
3.
Abnormal utilization
Congenital
transcobalamin II
deficiency

Vitamin B12
Clinical features
1. megaloblastic anemia
2. glossitis and angular stomatitis.
3. The neurological changes
•
polyneuropathy
• subacute combined degeneration of the
spinal cord
• psychiatric problems
• Dementia
• optic atrophy
•

Vitamin B12
polyneuropathy
symmetrical paraesthesiae in the fingers and
toes
subacute combined degeneration
( posterior, lateral columns of the spinal cord)
• loss of vibration sense and proprioception
• sensory ataxia
• progressive weakness
• Paraplegia may result.

Vitamin B12
psychiatric problems
• depression
• hallucinations
Dementia
optic atrophy

Vitamin B12
Investigations
1. Hematological findings
features of a megaloblastic anemia
2. Bone marrow
features of megaloblastic erythropoiesis
)
3. Serum bilirubin
may be raised
result of ineffective erythropoiesis.
4. Serum vitamin B12
below the normal (160 ng/L)

Vitamin B12
Treatment
Hydroxocobalamin 1000 μg can be given
intramuscularly.
improvement of the polyneuropathy may
occur over 6-12 months,
long-standing spinal cord damage is
irreversible.

Folates
in food as in reduced dihydrofolate or
tetrahydrofolate (THF)
function
• coenzymes in the transfer of single carbon
units in amino acid metabolism and DNA
synthesis.
Source
• Dietary intake Folate is found in green
vegetables
• Cooking causes a loss of 60-90% of the
folate
.
Folates
Causes of folate deficiency
1.
Nutritional
major cause
Poor intake
• Old age
• Poor social conditions
• anorexia
Gastrointestinal disease
• partial gastrectomy
• small bowel disease as coeliac disease,
Crohn’s disease
Antifolate drugs
• Anticonvulsants:
– Phenytoin, barbiturates
• Methotrexate, , trimethoprim, sulphasalazine
Folate
2.
Excess utilization
Physiological
• Pregnancy
• Lactation
Pathological
• Haematological disease with excess red cell
production, e.g. haemolysis
• Malignant disease with increased cell turnover
• Inflammatory disease
• Haemodialysis or peritoneal dialysis (loss with
the fluid)

Folate
Clinical features
• asymptomatic
• symptoms of anaemia or of the underlying
cause.
• Glossitis can occur.
• CNS manifestations does not occur .
Investigations
The haematological findings are those of a
megaloblastic anaemia
.
low levels of serum folate (4-18
μg/L).

Folate
Treatment of folate deficiency
• 5 mg of folic acid daily for about 4 months to
replace body stores.
• Rx (i.e. treatment) of underlying cause, e.g.
coeliac disease
.
• Prophylactic folic acid is recommended for all
women planning a pregnancy. (neuronal tube
defect)
• Prophylactic folic acid is also given in chronic
haematological disorders (when there’s rapid
cell turnover)

Vitamin C
(Ascorbic acid)
function
• It is involved in the
hydroxylation
of proline to
hydroxyproline, which is necessary for the
formation of
collagen
.
Source
• Vitamin C is present in all fresh fruit and
vegetables.

Vitamin C
(Ascorbic acid)
Deficiency
1. is seen mainly in the
elderly
and single
people who do not eat vegetables.
2. Increase need in the trauma, burn infection
3. drugs as steroid, indomethacin, aspirin,
tetracycline
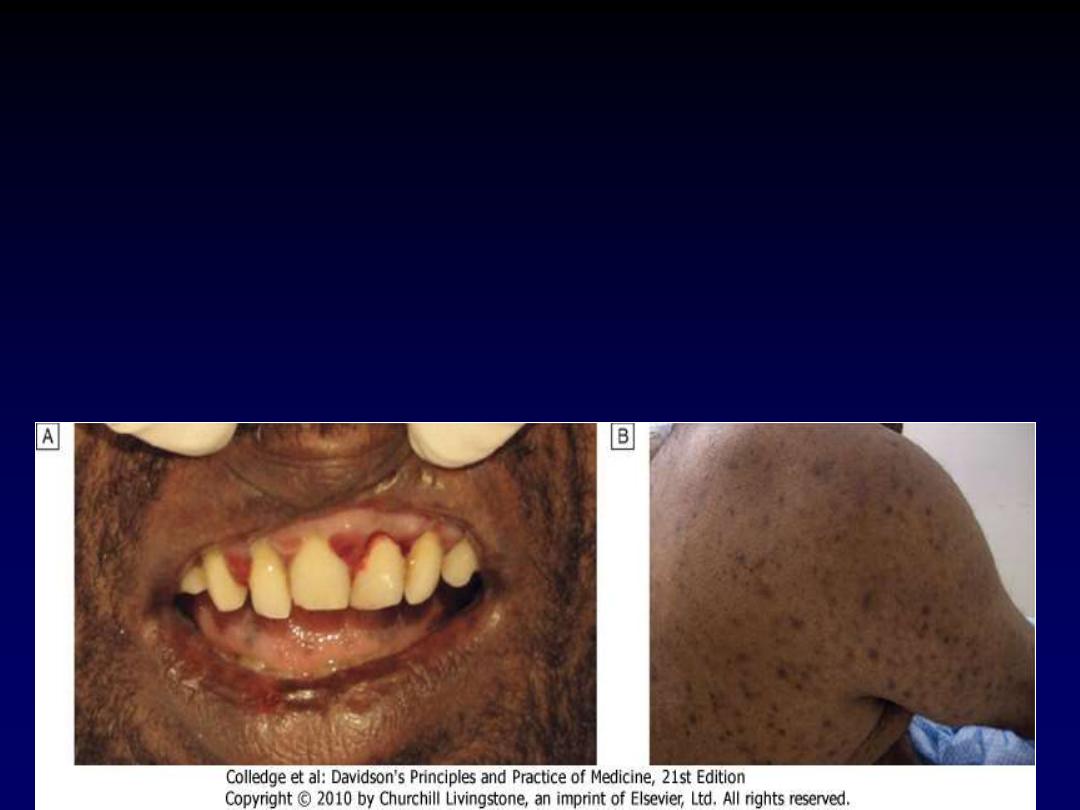
Vitamin C
Ascorbic acid
Clinical features :
scurvy
• Perifollicular hemorrhages
• Swollen, spongy gums with bleeding and
superadded infection
• Spontaneous hemorrhage (GIT, joint,
peritoneum)
• Failure of wound healing

Vitamin C
Ascorbic acid
Diagnosis
• Plasma ascorbic acid is very low (less than
11
μmol/L) .
Treatment
200 mg of ascorbic acid daily and
encouraged to eat fresh fruit and vegetables.
NB
.
Vit.C in large amount used in upper
respiratory tract infection

Thanks