1
forth stage
Surgery
Lec-3
.
د
ﺳﻣﯾر اﻟﺻﻔﺎر
26/10/2015
Abdominal wall hernia
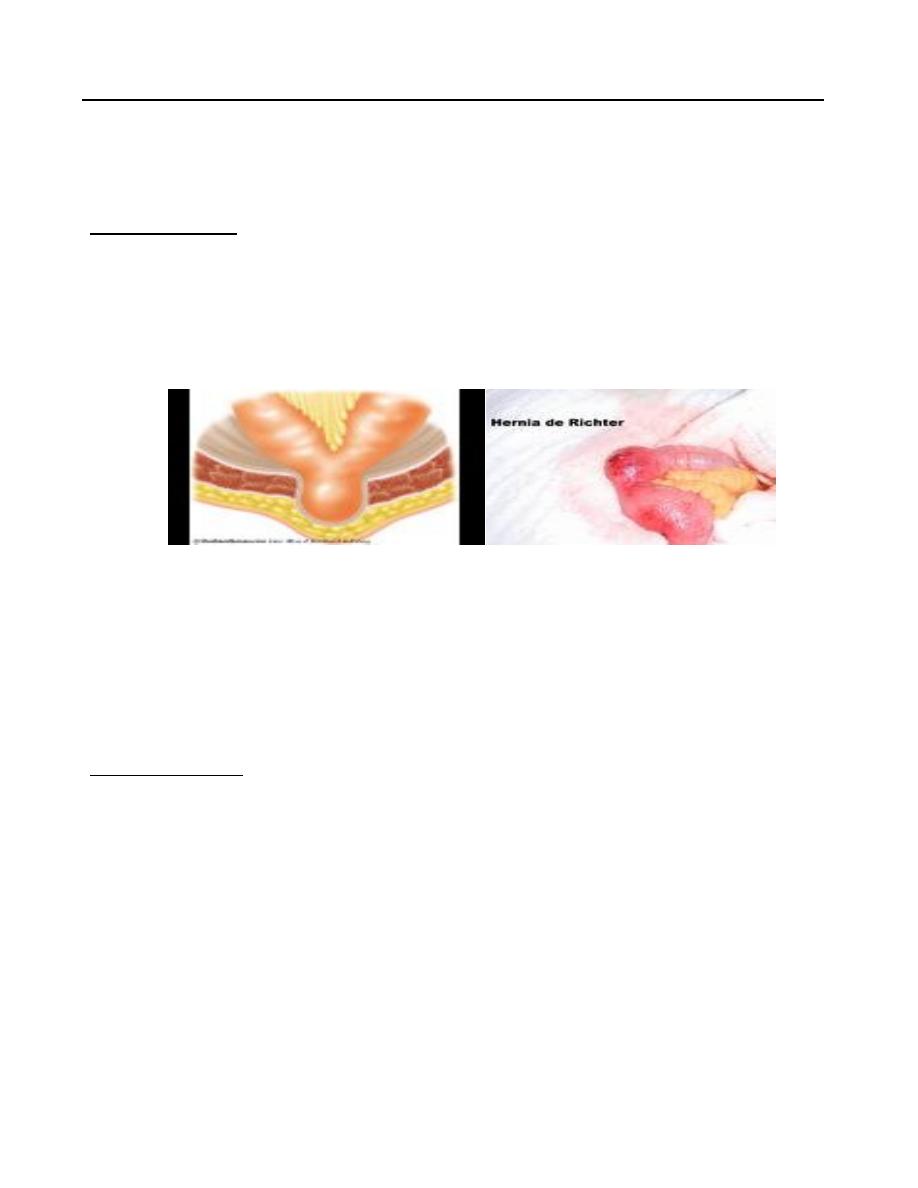
Richter’s hernia
Frequent complication of femoral hernia
Only part of circumference of bowel enclosed in the hernia sac which may become
gangrenous
Clinically; abdominal symptoms of IO but with no constipation.
Diagnosis:
High index of suspicion
Urgent surgical interference
Almost always the diagnosis made at surgery
Umbilical hernia
In neonates
Exomphalos
1/6000 of births
Failure of all or part of midgut to return to the coelom
In infants and children
Defect in the umbilical cicatrix
Equal sex incidence
Black infants 8 times more
2
Clinical features
Symptomless
More prominent during crying
Obstruction or strangulation is rare below 3 years of age
Most of cases resolve by itself within 2 years
Diagnosis
Swelling with umbilical cicatric at fundus of swelling
Reducible
ECI +ve -----Crying
Treatment
Conservative below the age of 2 years – reassurance of parents
After 2 years needs surgical repair
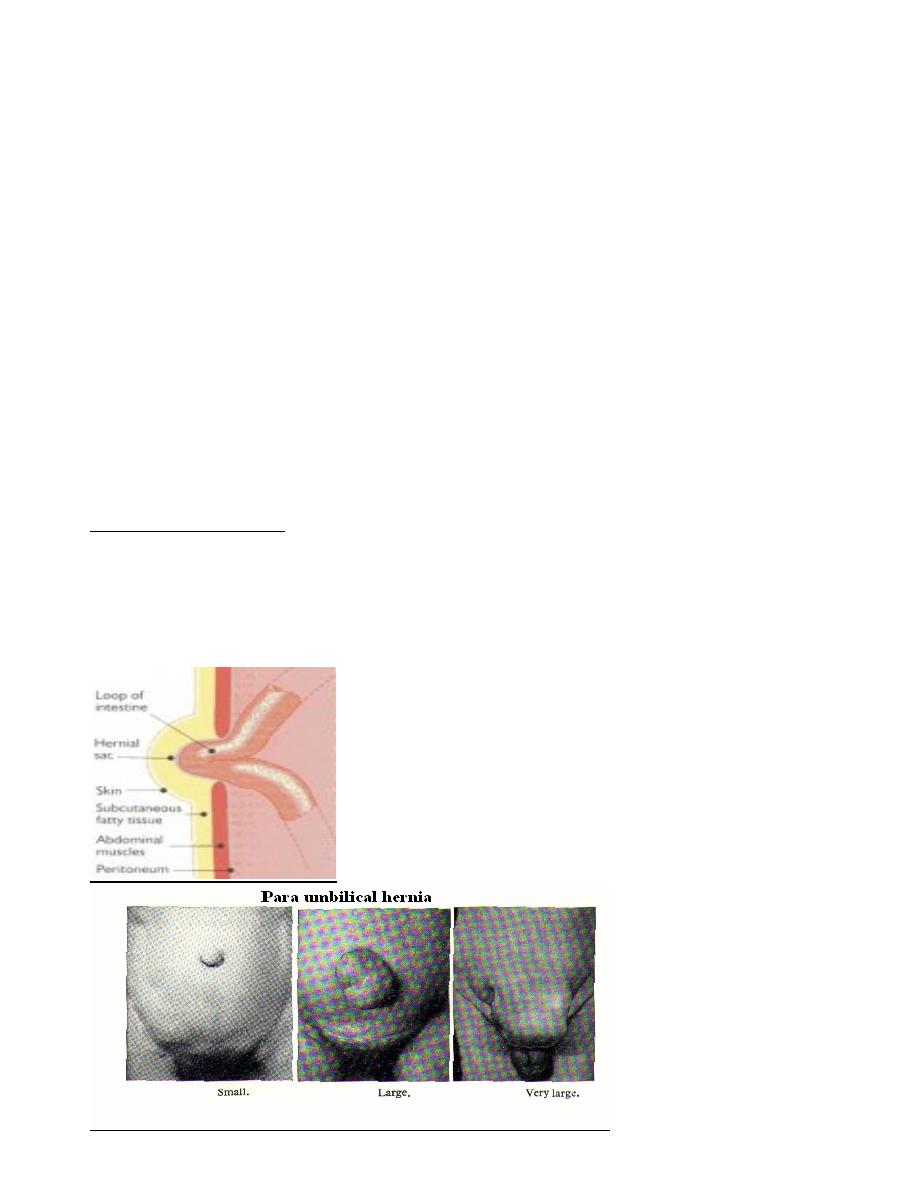
Paraumbilical Hernia
Adults
Women> men
Risk factors :Obesity ,Pregnancy
Repair primarily or with mesh

3
Pathogenesis
Weak point in the linea alba just above or just below the umbilical cicatrix
Round or oval in shape
May sag downwards
May become a large size
The neck of sac is often remarkably small in size
Contents; mostly small intestine or omentum or both(Sometimes part of transverse
colon)
Clinical features
Classical patient:
Adult Female (F:M ; 5:1)
Aged between 35 and 50 years
Overweight
multipara
Symptoms
Abdominal swelling
Dragging pain
Intestinal colics—obstruction
Epigastric pain (stomachache)
Complications
1. Irreducibility with possibility of IO
2. Ulceration of skin over fundus of sac
3. Intertrigo
Diagnosis -------> clinical :
Swelling just above or below the umbilicus
Prominent on standing
Disappear on lying
Expensile cough impulse
4
Treatment
Operation is advised in nearly all patients.
Indications:
1. Liable for complication
2. Cosmetic
The operation is "Herniotomy and Repair" ,Either Myo’s repair or Mesh repair.
Mesh repair is indicated for
1. Large defect > 4 cm
2. Recurrent hernia
Postoperative complications
Local and specific
1. Collection(Hematoma,Seroma )
2. Infection (Wound infection,Pus collection)
3. Recurrence
Epigastric Hernia(Fatty hernia of linea alba)
Incidence 1-5%
Men> women
Between xiphoid and umbilicus
20% multiple
Repair primarily
Pathogenesis
Extraperitoneal fat protrusion through decussating fibers at linea alba
At sites of blood vessels
Clinical features
Symptomless:
Accidental finding
The size of a Pea
Felt not seen
Painful ---local pain and tenderness
Referred pain----DU like symptoms
Treatment: operation
5
Spieghelian Hernia
Rare
Hernia through subumbilical portion of semi-lunar line
Difficult to diagnose
–
Clinical suspicion (location)
–
CT scan
Repair primarily or with mesh
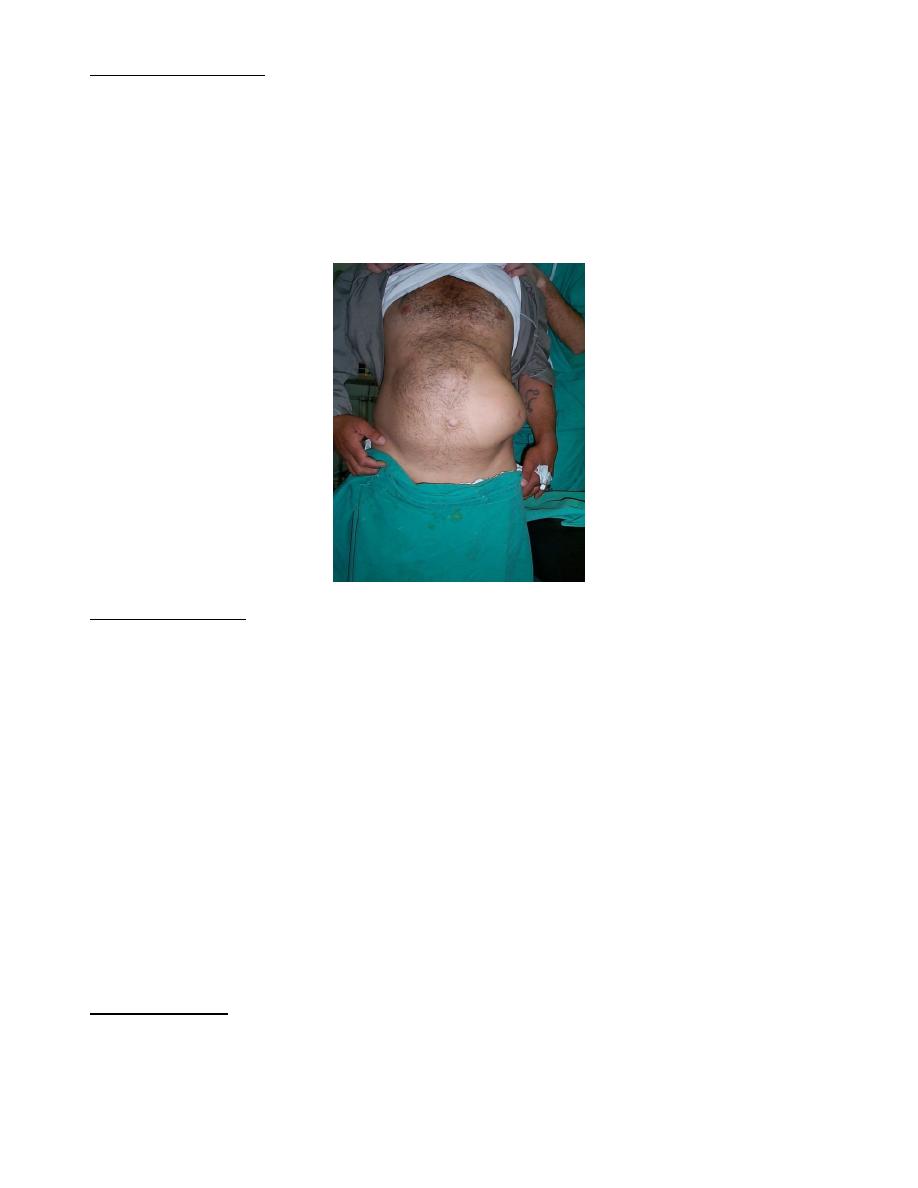
Incisional Hernia
This occurs after 2-10% of all abdominal surgeries, although some people are more at
risk.
After surgical repair, these hernias have a high rate of returning (20-45%).
Risk factors
–
Technical
–
Wound infection
–
Smoking
–
Hypoxia/ ischemia
–
Tension
–
Obesity
–
Malnutrition
Laparoscopic vs. open repair
Lumbar Hernia
Congenital, spontaneous or traumatic
Grynfeltt’s triangle:
–
12th rib, internal oblique and sacrospinalis muscle
–
Covered by latissimus dorsi
6
Petit’s triangle:
–
Latissimus dorsi, external oblique and iliac crest
–
Covered by superficial fascia
Pelvic Hernia
1) Obturator hernia
–
Most commonly in women
–
Howship-Romberg sign
2) Sciatic hernia
3) Perineal hernia
Parastomal Hernia
Variant of incisional hernia
Paracolostomy > paraileostomy
Low rate if through rectus muscle
Traditionally relocate stoma, repair defect
Concern for mesh erosion
Laparoscopic repair
Abdominal Wall Hernia
1) Richter’s hernia
2) Littre’s hernia
3) Hernia in W
4) Pantallon
Umbilical Hernia
Common in infants
Close spontaneously if <1.5 cm
Repair if > 2 cm or if persists at age 3-4 years
Repair primarily or with mesh