
D
R
. H
UDA
A
BO
- A
LEES
214 -2 -15
GR AM-NEGATIVE BAC IL L I
T HE ENT ER IC S:
Family Enterobacteriaceae:
Genus Escherichia & Genus K lebsiella
Obgectives:
¢
Describe the morphology & physiology for E.coli & Klebsiella species.
¢
Determine the virulence factors for E.coli & Klebsiella species.
¢
Analyze the diseases & pathogenicity for E.coli & Klebsiella.
¢
Demonstrate the epidemiology and transmission.
¢
Outline the laboratory diagnosis.
¢
State the drug of choice and prophylaxis where regularly used.
A
NTIGENIC CLASSIFICATION
¢
Depending on the cell surface structures that bind to specific antibodies
(antigenic determinants). The Enterics have three major surface antigens,
which differ slightly from one species to another.
¢
Somatic O antigen: this is the most external component of the
lipopolysaccharide (LPS) of the gram-negative bacteria cell wall. O=Outer.
¢
Capsular K (capsule) antigen this is the capsule that covers the O antigen.
¢
Flagellaer H antigen: so only the motile bacteria that possess flagella have
this antigen.

B
IOCHEMICAL
C
LASSIFICATION
:
¢
Some of the important biochemical properties of the organisms, which can
be measured in the lab, are:
¢
1. The ability to ferment lactose and convert it into gas and acid, which can
be visualized by using dye that changes in color when the PH changes
example MacConkey agar. Escherichia coli and most of the
enterobacteriaceae ferment lactose while Salmonella, Shigella and
Pseudomonas aeruginosa do not.
¢
2. The production of H2S, ability to hydrolyze urea, liquefies gelatin, and
decarboxylate specific amino acids.
P
ATHOGENESES
:
The enteric can produce 2 types of diseases:
¢
1. Diarrhea with or without systemic invasion.
¢
2. Various other infections such as urinary tract infection, pneumonia,
bacteremia and sepsis, especially in debilitated hospitalized patients.
D
IARRHEA
:
Generally diarrhea classifies to major categories:
¢
1. Inflammatory diarrhea due to tissue invasion
¢
2. Non- inflammatory diarrhea: no tissue invasion such as the diarrhea
results from bacterial toxins, viral and heavy metal poisoning.

The clinical manifestation of diarrhea caused by enteric vary depending on the
severity or depth of intestinal invasion.
¢
1) No cell invasion: Watery diarrhea without systemic symptoms (such as
fever) is the usual picture. Enterotoxigenic Escherichia coli and Vibrio
cholera are examples.
¢
2) Invasion of the intestinal epithelial cells: The cell death results in red
blood cell leakage into the stool. Examples: Enteroinvasive Escherichia coli,
Shigella, and Salmonella enteritidis.
¢
3) Invasion of the lymph nodes and bloodstream: Examples: Salmonella typhi,
Yersinia enterocolitica, andCampylobacter jejuni.
FAMILYENTEROBACTERIACEAE E
SCHERICHIA COLI
(E.
COLI
)
¢
Escherichia coli is one of the normal flora of human intestinal tract. However,
any genetic changes that resulting in transfer of virulence factors by
conjugation with plasmid exchange, bacteriophages, and direct DNA
insertion this will convert the non-virulence strain to virulent one in this
manner, it can cause disease.
Nonpathogenic Escherichia coli
+
virulence factor
=
Disease
(Normal flora)
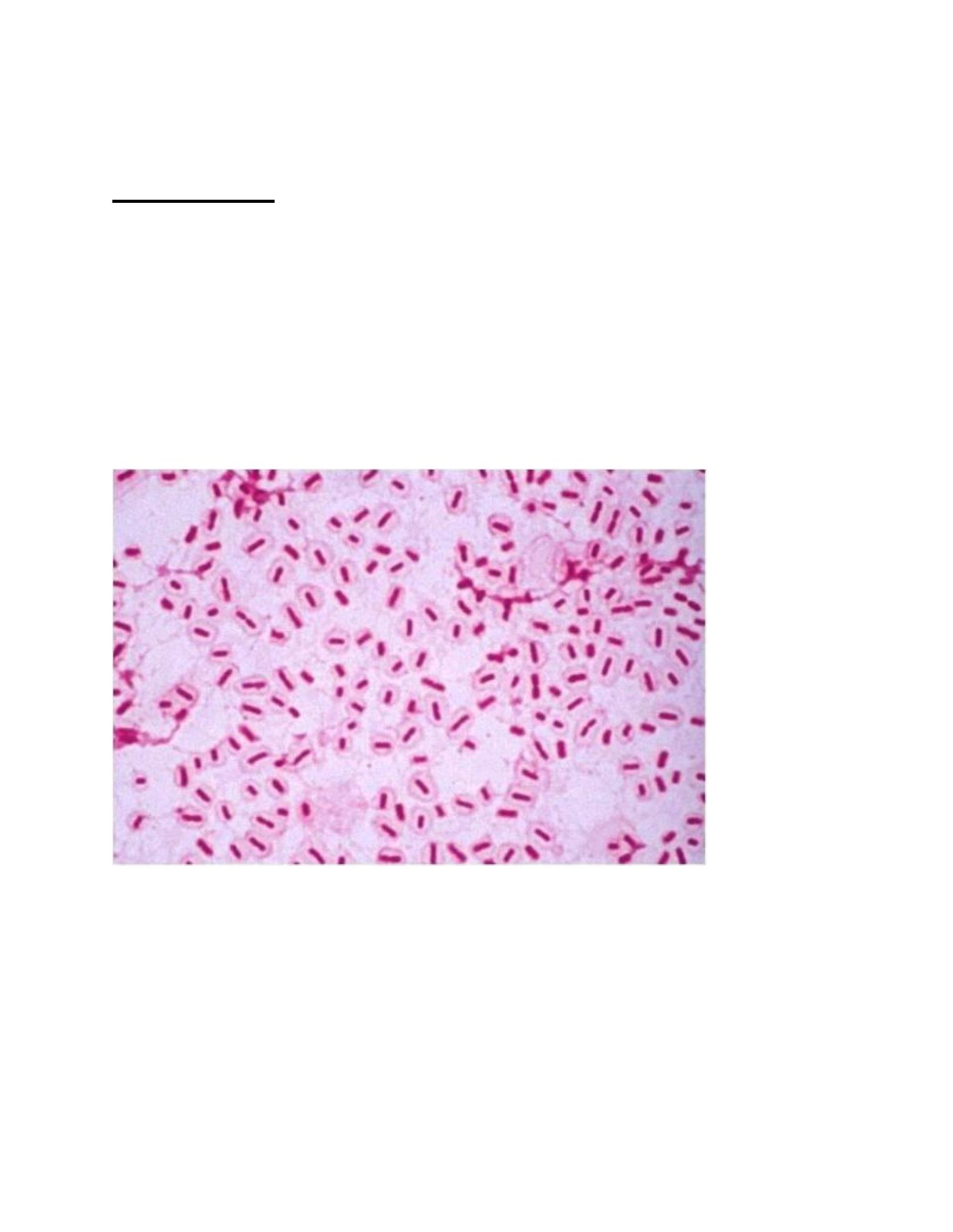
S
TRUCTURE AND PHYSIOLOGY
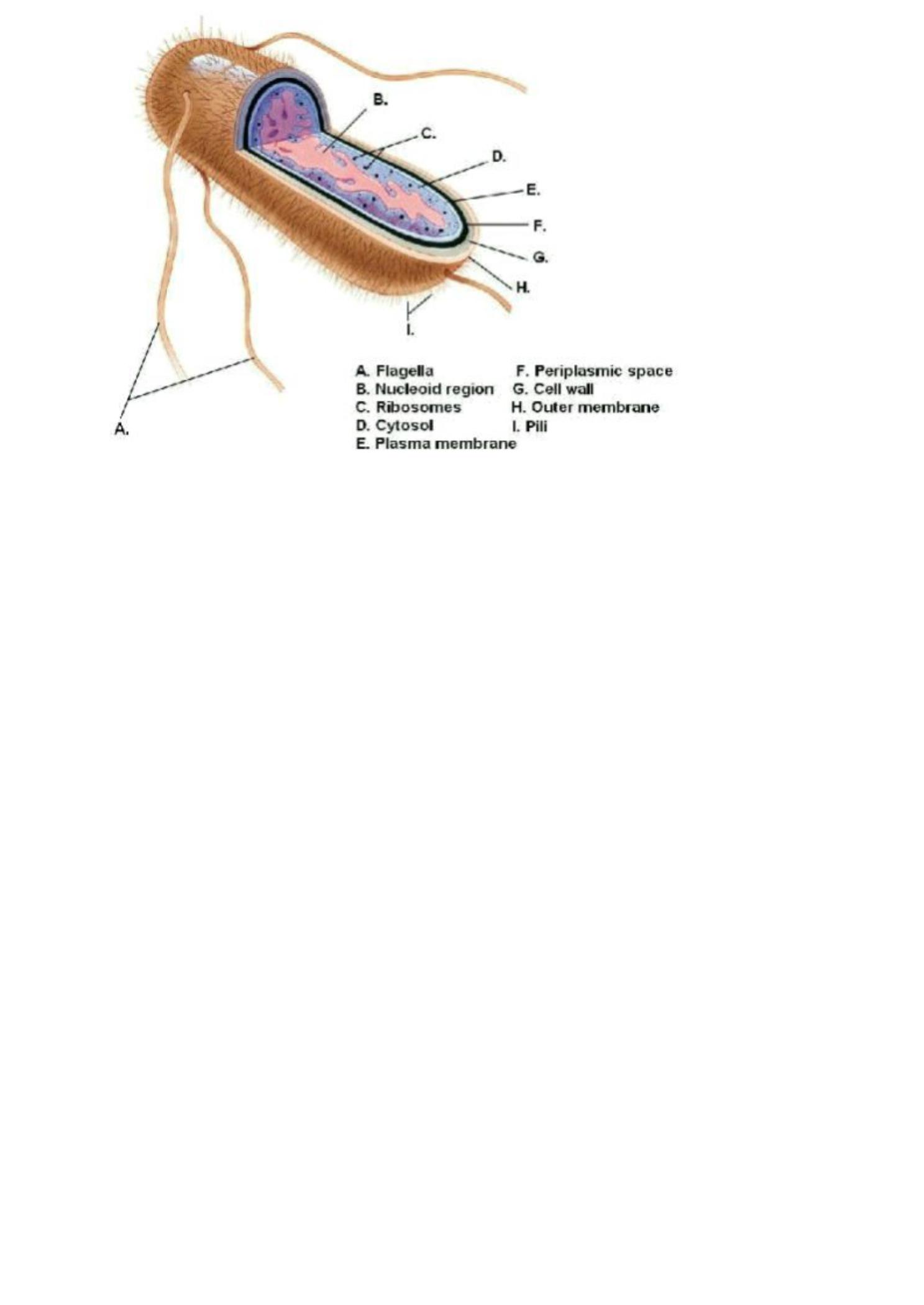
¢
E. coli is a gram negative bacilli, has fimbriae or pili that are important for
adherence to host mucosal surfaces, and different strains of the organism
may be motile or nonmotile.
¢
Most strains can ferment lactose (that is, they are L ac+ ) in contrast to the
major intestinal pathogens, Salmonella and Shigella, which cannot ferment
lactose (that is, they are L ac-).
¢
E. coli produces both acid and gas during fermentation of carbohydrates.
¢
They are all facultative anaerobes.
¢
Most strains are motile and not capsulated.
¢
They all ferment glucose.
¢
They all lack cytochrome oxidase (that is, they are oxidase negative).
¢ Typing strains is based on differences in three structural antigens: O, H,
and K .The O antigens (somatic or cell wall antigens) are found on the
polysaccharide portion of the LPS. These antigens are heat stable and may
be shared among different Enterobacteriaceae genera. O antigens are
commonly used to serologically type many of the enteric gram-negative rods.
The H antigens are associated with flagella, and, therefore, only flagellated
(motile) Enterobacteriaceae such as E. coli have H antigen. The K antigens
are located within the polysaccharide capsules. Among E. coli species, there
are many serologically distinct O, H, and K antigens, and specific serotypes

are associated with particular diseases. For example, a serotype of E. coli
possessing O157 and H7 (designated O157:H7) causes a severe form of
hemorrhagic colitis.
R
ESERVOIR
:
•Human colon (normal flora); may colonize in vagina or urethra.
•Contaminated crops where human fecal fertilizer is used.
•Enterohemorrhagic strains: bovine feces.
T
RANSMISSION
:
¢
Endogenous.
¢
Fecal-oral.
¢
Maternal fecal flora.
¢
Enterohemorrhagic strains: bovine fecal contamination (raw or under
cooked beef, milk, apple juice from fallen apples).
V
IRULENCE FACTORS
Virulence factors include the following:
¢
1)
Mucosal interaction
:
a) Mucosal adherence with pili (colonization factor). b) b)Ability to invade intestinal
epithelial cells.
¢
2)
Exotox in production
:
a) Heat-labile and stable toxin (LT and ST).
b) Shiga-like toxin (verotoxin).
¢
3)
Endotox in
: L ipid A portion of lipopolysaccharide ( LPS).
4)
Iron-binding sider ophor e
: obtains iron from human transferrin or
lactiferrin .
D
ISEASES
Diseases caused by Escherichia coli in the presence of virulence factors include
the following:
¢
1) Diarrhea.
¢
2) Urinary tract infection (MOST COMMON CAUSE OF UTI).
¢
3) Neonatal meningitis (2ND MOST COMMON CAUSE).
¢
4) Gram-negative sepsis, occurring commonly in debilitated hospitalized
patients.
E
SCHERICHIA COLI
D
IARRHEA
¢
Escherichia coli diarrhea may affect infants or adults. Infants worldwide are
especially susceptible to Escherichia coli diarrhea, since they usually do not
developed immunity yet .
¢
Since fluids lost in the stool is often not adequately replaced, death from
Escherichia coli diarrhea is usually due to
dehydration
.
¢
About 5 million children die yearly from this infection.
¢
Escherichia coli is conceded as an important cause of
Traveler’
s Diarrhea
.
¢
The severity of Escherichia coli diarrhea depends on which
vir ulence
factor s
the strain of Escherichiacoli possesses. These strains have been
named based on their virulence factors and the different diarrheal diseases
they cause.
Strains of E. coli and disease they cause
Strain of
E
.co/i
A
bbreviati
on
S
yndro
me
T
ransmission
E
nterotoxigenic
E.
c
oli
E
TEC
W
atery
d
iarrhea
(t
raveler's
d
iarrhea
)
F
ecal/oral
E
nteropathogenic
E
.
c
oli
E
PEC
W
atery diarrhea
o
f long
d
uration,
m
ostly
in infants,
often in developing
c
ountries
F
ecal/oral
{
2
n
d
m
ost
c
ommon
i
nfantile
d
iarrhea
)
E
nterohemorrhag
ic
E
.
c
oli
(
0157:H7}
M
OST
C
OMMON,
(
0104:H4}=
C
UCMBER
E.COLI
E
HEC
(
VTEC)
Bloody
d
iarrhea;
Hemorrhagic
c
olitis
a
nd
h
emolytic
uremic
s
yndrome
(
HUS),
(
AVOID
USING
A
NTIBIOTIC}
Bovine Feces,
P
itting
"
""'
E
nteroinvasive
E.
c
oli
E
IEC
B
loody
d
iarrhea
F
ecal/oral
E
nteroaggregative
E
.
coli,
(0
104:H4}
E
AEC
P
ersistent
watery diarrhea
i
n
c
hildren
a
nd
p
atients
i
nfected with
H
IV
F
ecal
/
oral
D
iffusely
a
dherent
E.coli
D
AEC
W
atery diarrhea
F
ecal
/
oral
E
XTRAINTESTINAL INFECTIONS
1)
Escherichia coli Urinary Tract Infections ( UTI):
¢
The acquisition of a pili virulence factor allows Escherichia coli to travel up
the urethra and infect the bladder (cystitis) and sometimes move further
up to infect the kidney itself (pyelonephritis). Escherichia coli is the most
common cause of urinary tract infections. Which usually occur in women
and hospitalized patients with catheters in the urethra. Symptoms include
burning on urination ( dysuria), having to pee frequently (frequency), and a
feeling of fullness over the bladder. Culture of greater than 100,000 (105)
colonies of bacteria from the urine establishes the diagnosis of a urinary
tract infection.
2) Escherichia coli Mening itis:
¢
Capsulated strain of Escherichia coli is the second most common cause of
neonatal meningitis (group B streptococcus is first). During the first month
of life, the neonate is especially susceptible
3) Escherichia coli Sepsis
¢
Escherichia coli is also the most common cause of gram-negative sepsis.
This usually occurs in debilitated hospitalized patients. Septic shock due to
the lipid A component of the L PS is usually the cause of death.
4) Escherichia coli Pneumonia
¢
Escherichia coli is a common cause of hospital-acquired pneumonia.
METHODS FOR DIFFRENTIATING PATHOGENIC E.COLI FROM
NORMAL FLORA

¢
1) Immunoassay looking for specific protein antigen (on or excreted from
the bacterium).
¢
2) Serotyping since certain serotypes are more often Pathogenic.
¢
3) DNA probe for specific gene in a culture.
4) PCR for clinical specimen.
G
ENUS
K
LEBSIELLA
Genus Features
§
Members of the genus Klebsiella are capsulated Gram-negative
rods.
§
They are non-motile but some strains express fimbriae.
§
They may survive drying for months.
§
They are facultative anaerobes.
§
Strains can be differentiated by simple biochemical tests.
§
C
APSULAR STAIN SHOWING LARGE CAPSULE AROUND
K
LEBSIELLA

A
NTIGENIC
S
TRUCTURE
¢
About 80 capsular
K
antigens are presently recognized.
¢
Types
K
1,
K
2,
K
3,
K
5 and
K
21are particularly significant inhuman
diseases.
Five different somatic O antigens occur in various combinations with
the capsular antigens
.
S
PECIES OF MEDICAL IMPORTANCE
K lebsiella pneumoniae
Distinguishing Features
:
¢
Gram-negative rods with large polysaccharide
capsule.
¢
Mucoid, lactose-fermenting colonies on MacConkey agar.
¢
Oxidase negative.
Reservoir
: human colon and upper respiratory
tract (normal flora).
Transmission
: endogenous.
P
ATHOGENESIS
(
VIRULENCE FACTORS
)
These include:
1) Complex capsule give protection against phagocytosis.
2) Endotoxin: causes fever, inflammation, and shock (septicemia).
3)L ong-chain lipopolysaccharides( L PS) protects strains from the action
of serum complement.

D
ISEASES CAUSED BY
K.
PNEUMONIAE
a) Pneumonia
¢
-Community-acquired, most often in older males; most commonly
in patients with either chronic lung disease, alcoholism, or
diabetes (but this is not the most common cause of pneumonia in
alcoholics;
(S. pneumoniae is.)
¢
-Endogenous; assumed to reach lungs by inhalation of respiratory
droplets from upper respiratory tract.
¢
-Frequent abscesses make it hard to treat with high fatality rate.
¢
-Sputum is generally thick and bloody (currant jelly) but not foul
smelling as in anaerobic aspiration pneumonia.
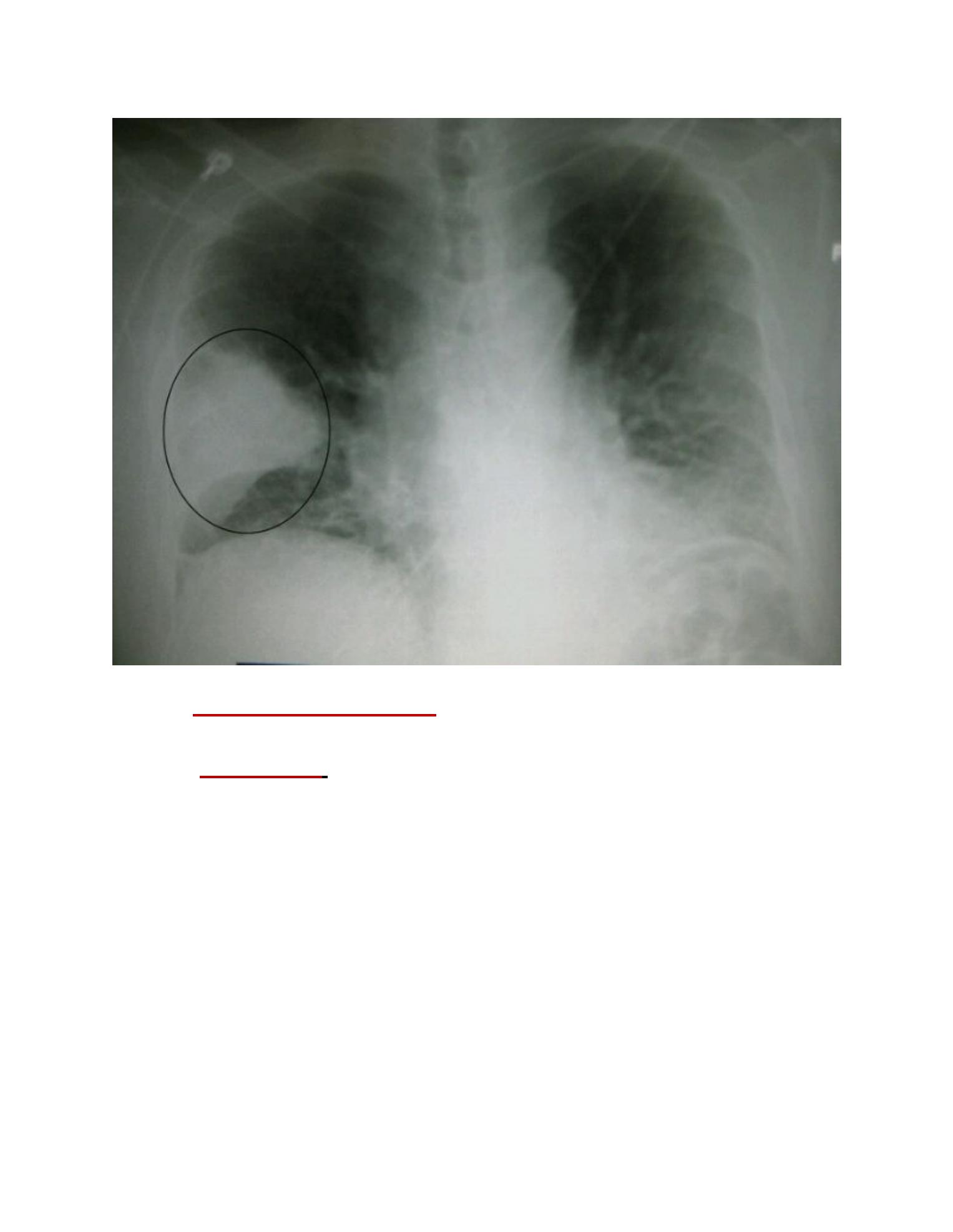
C
HEST
X-
RAYOF PATIENT WITH
K.
PNEUMONIA
¢
b) Urinary tract infections-catheter-related
(nosocomial) from
fecal contamination of catheters.
¢
C) Septicemia:
in immunocompromised patients may originate
from bowel defects or invasion of IV lines
.
L
ABORATORY DIAGNOSIS
¢
1) Specimens (site of infection e.g. urine, blood, sputum, pus...etc).
¢
2) Staining: Gram's stain and Capsular stain.
¢
3) Culture:37C 0, 24-48h.:
a) Differential media:
- MacConkey's agar (selective and differential media).

- EMB (eosin methylene blue) contains special dye.
b) Non differential medium: Blood agar.
¢
4) Biochemical tests
I. (IMViC) test.
II. The API 20E system :(API= analytic profile index).
¢
5) Motility test (at 37C0 .
¢
6) Serotyping: used for E.coli to determine the (0 Ag) and (H Ag),
There are >150 (0 Ag), >50 (H Ag).
¢
7) Antibiotic Sensitivity test: important as there is high percentage
of antibiotic resistant strains.
P
REVENTION AND TREATMENT
:
¢
Intestinal disease can best be prevented by care in selection,
preparation, and consumption of food and water.
¢
Maintenance of fluid and electrolyte balance is of primary
importance in treatment.
¢
Antibiotics may shorten duration of symptoms, but resistance is
nevertheless widespread.
¢
Extraintestinal diseases require antibiotic treatment. Antibiotic
sensitivity testing of isolates is necessary to determine the
appropriate choice of drugs
.
R
EFERENCES
:
¢
Clinical Microbiology Made Ridiculously Simple, 6th ed, 2014.
¢
Baily & Scott diagnostic microbiology,12th ed.
¢
Lippincotts lllustrated microbiology 3ed ed., 2013.
¢
Medical Microbiology, 17
th
ed 2007.

The end