1
GRAM-POSITIVE BACTERIA
Genus Staphylococcus
Objectives: Upon completion of this lecture, the student will:
Outline the medically important staphylococci species.
Describing the morphology & physiology for
staphylococci.
Determine the virulence factors for staphylococci.
Analyze the diseases & pathogenicity for staphylococci.
Demonstrate the epidemiology/transmission for
staphylococci.
Outline the laboratory diagnosis for staphylococci.
State the drug of choice and prophylaxis where regularly
used.
Lec.1
Dr.Sarmad Zeiny
2013-2014
BCM
2
GRAM-POSITIVE BACTERIA
Genus Staphylococcus
The 3 medical important species:
- Staphylococcus aureus.
- Staphylococcus epidermidis.
- Staphylococcus saprophyticus.
Important Properties of genus staphylococcus:
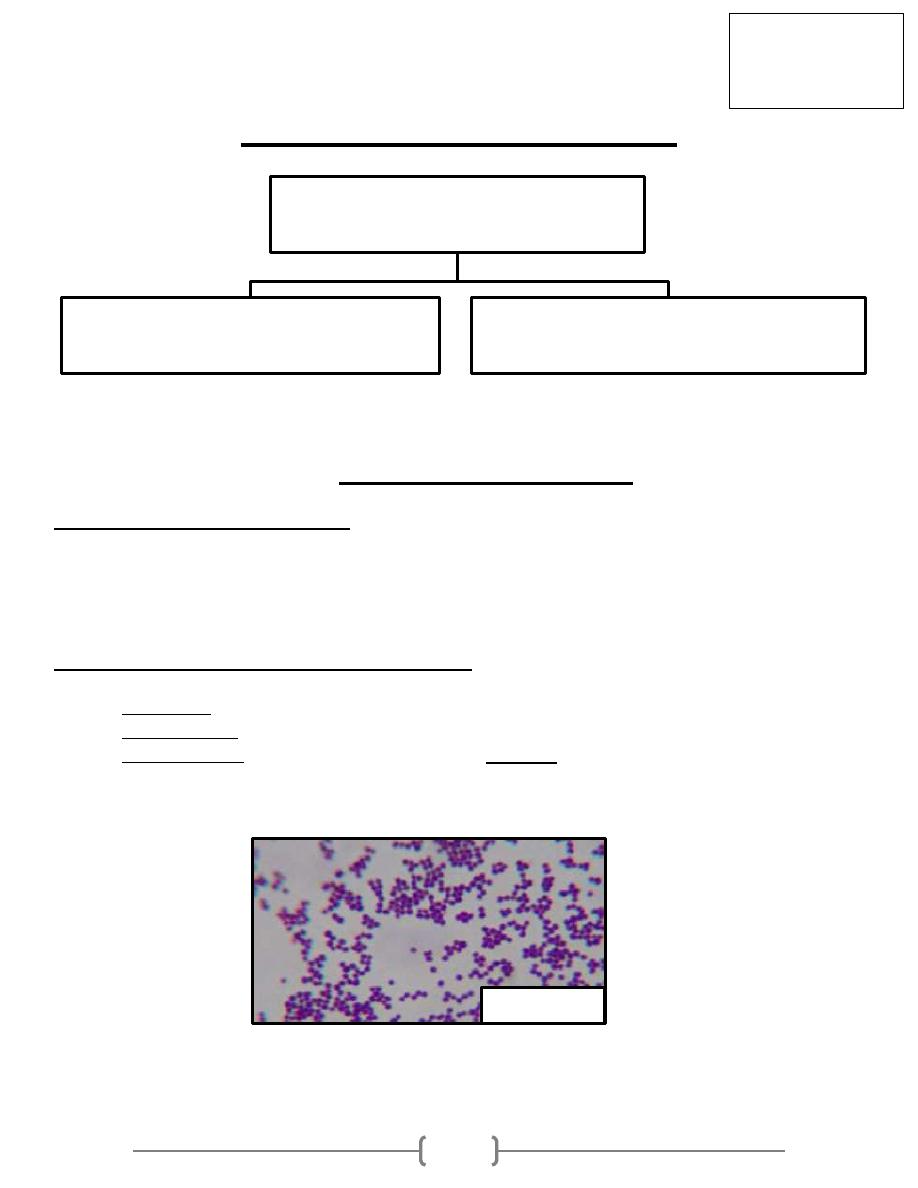
- The Shape: Staphylococci are spherical gram-positive cocci
- Arrangement: arranged in irregular grapelike clusters (Figure 1).
- Biochemically: All staphylococci produce catalase enzyme, whereas no streptococci
do (catalase degrades H
2
O
2
into O
2
and H
2
O), Catalase is an important virulence
factor because H
2
O
2
is microbicidal and its degradation limits the ability of neutrophils
to kill.
- S.aureus is by far the most pathogenic species. S.aureus is distinguished from the others
primarily by coagulase production, for that reason, S.aureus called coagulase positive
Fig.1
Lec.1
Dr.Sarmad Zeiny
2013-2014
BCM
Gram positive cocci
Streptococci (catalase –ve)
Staphylococci (catalase +ve)
3
staphylococcus. Coagulase is an enzyme that causes plasma to clot by activating
prothrombin to form thrombin. Thrombin then catalyzes the activation of fibrinogen to
form the fibrin clot.
- S.epidermidis and S.saprophyticus are often referred to as coagulase-negative
staphylococci.
- All Staphylococci tolerate high salt concentration (up to 9.5% Nacl).
- S.aureus produces a pigment called staphyloxanthin, which imparts a golden color to
its colonies. This pigment enhances the pathogenicity of the organism by inactivating
the microbicidal effect of superoxides and other reactive oxygen species within
neutrophils.
- S aureus usually ferments mannitol and hemolyzes red blood cells, whereas the
others do not.
- S.saprophyticus resistant to novobiocin (type of antibiotic) while others are sensitive.
- Staphylococci and streptococci are non-motile and do not form spores.
Staphylococcus aureus (Staphylococcus pyogenes):
Distinguishing Features:
• Small, yellow colonies on blood agar.
• β – hemolytic on blood agar (complete destruction of RBC).
• Coagulase positive (all other Staphylococcus species are negative).
• Ferments mannitol on mannitol salt agar.
Fig. 2: Staphylococci lie in grape-like clusters as seen on Gram
stain. Visualize this cluster of hospital staff posing for a group
photo. Staphylococcus aureus is catalase-positive, thus
explaining the cats in the group photo. Staphylococcus aureus
(aureus means "gold") can be differentiated from the other beta-
hemolytic cocci by their elaboration of a golden pigment when
cultured on sheep blood agar. Notice that our hospital Staff
(Staph) all proudly wear gold medals around their necks. Note
how all the Gold-Medalists (Staphylococcus aureus) hang out
together to show each other their gold medals. You can think of
them as coagulating together.
Reservoir:
• Normal flora
- Nasal mucosa (25% of population are carriers)
- Skin
Fig.2
4
Transmission:
•
Hands
• Sneezing
• Surgical wounds
• Contaminated food
- Custard pastries
- Potato salad
- Canned meats
Virulent factors and pathogenesis:
S.aureus has a microcapsule surrounding its huge peptidoglycan cell wall, which in turn
surrounds a cell membrane containing penicillin binding protein (also called transpeptidase).
Numerous powerful defensive and offensive protein weapons stick out of the microcapsule or
can be excreted from the cytoplasm to wreak havoc on our bodies:
a) Proteins That Disable Our Immune Defenses:
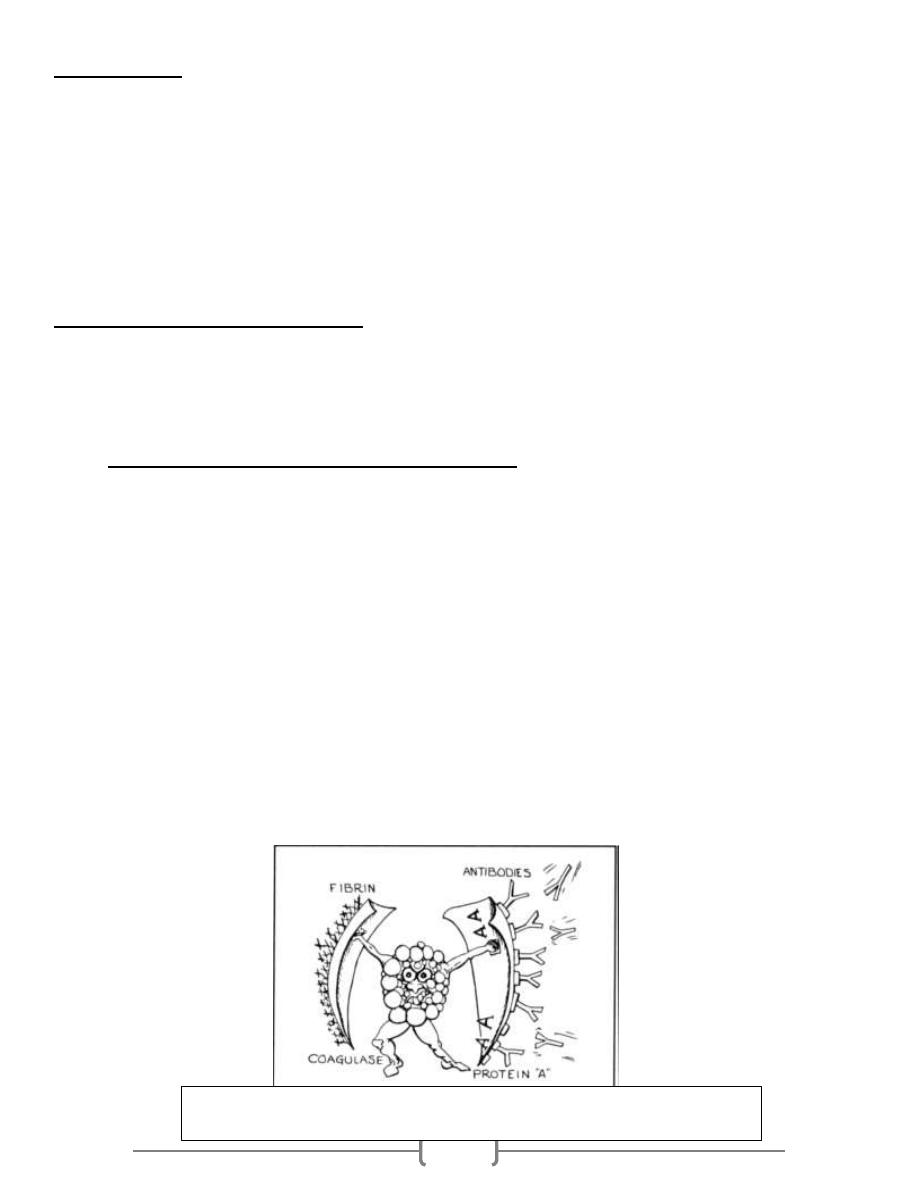
1) Protein A: This protein has sites that bind the Fc portion of IgG. This may protect the
organism from opsonization and phagocytosis. See fig.3
2) Coagulase: This enzyme can lead to fibrin formation around the bacteria, protecting it from
phagocytosis. See fig.3
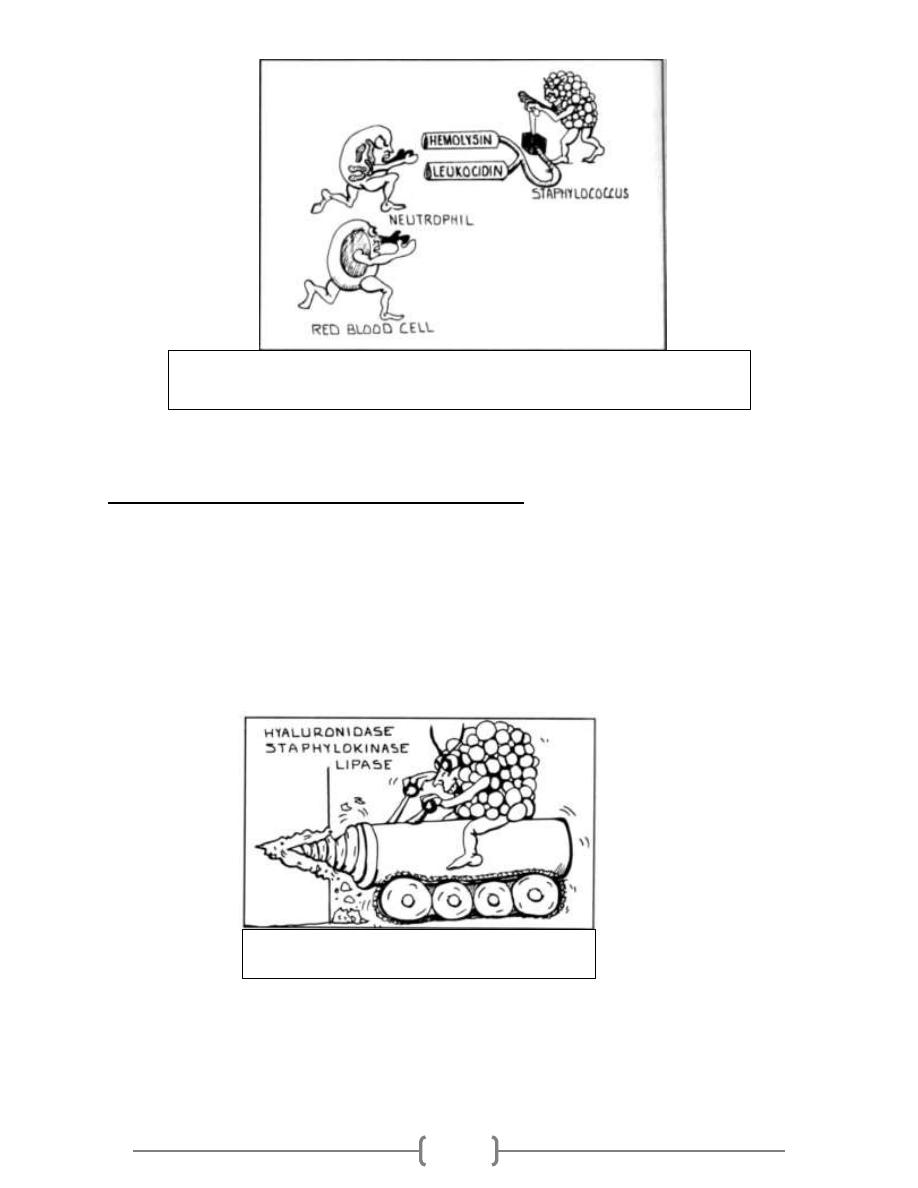
3) Hemolysins (4 types): Alpha, beta, gamma, and delta. They destroy red blood cells,
neutrophils, macrophages, and platelets. See fig.4
4) Leukocidins: They destroy leukocytes (white blood cells). See fig.4
5) Penicillinase: This is a secreted form of beta-lactamase. It disrupts the beta-lactam portion
of the penicillin molecule, thereby inactivating the antibiotic.
6) Novel penicillin binding protein: This protein, also called transpeptidase, is necessary for
cell wall peptidoglycan formation and is inhibited by penicillin. Some strains of Staphylococcus
aureus have new penicillin binding proteins that are resistant to (penicillinase - resistant
penicillins and cephalosporins antibiotics).
Fig. 3: Staphylococcus aureus wielding protein A and coagulase shields,
defending itself from attacking antibodies and phagocytosis.
5
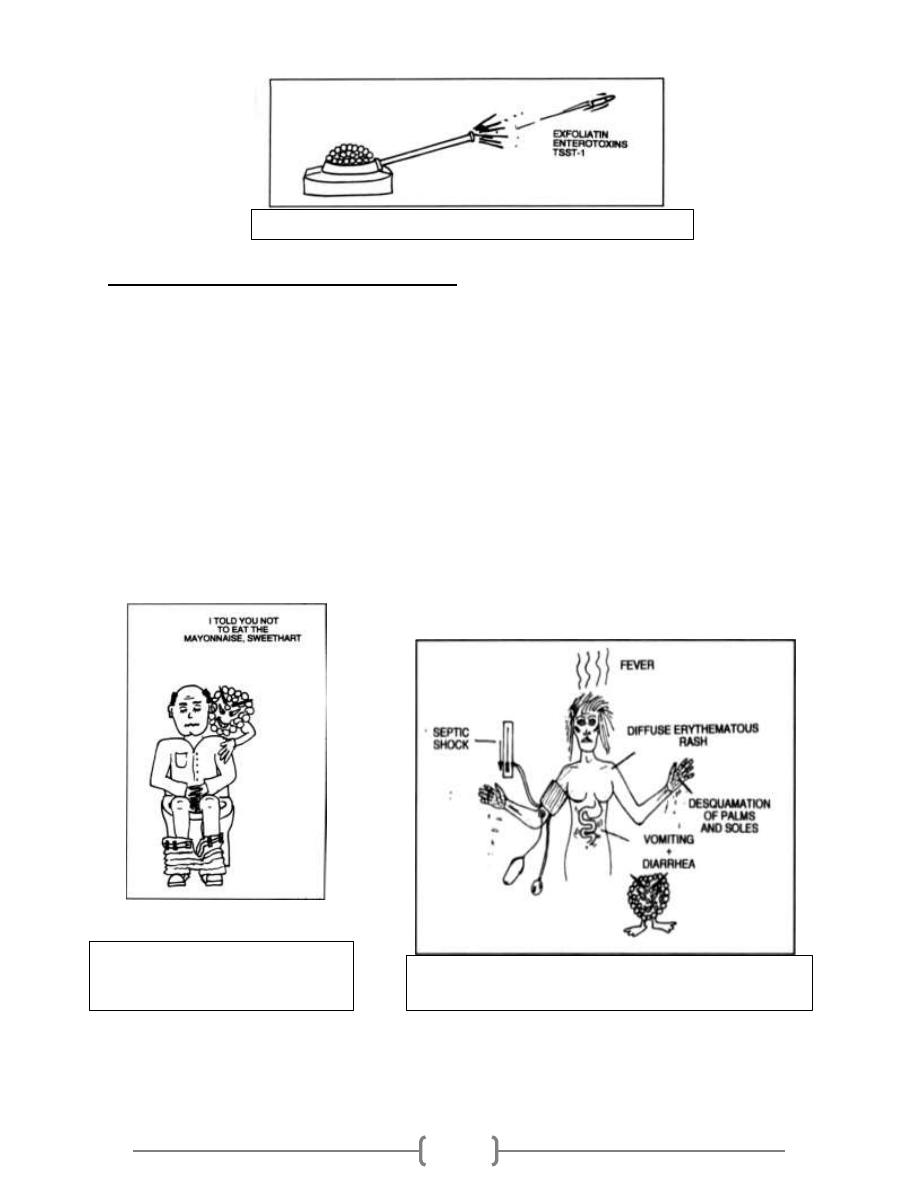
b) Proteins (enzymes) to Tunnel Through Tissue:
1) Hyaluronidase ("Spreading Factor"): This protein breaks down proteoglycans in
connective tissue.
2) Staphylokinase: This protein lyses formed fibrin clots (like streptokinase).
3) Lipase: This enzyme degrades fats and oils, which often accumulate on the surface of
our body. This degradation facilitates Staphylococcus aureus colonization of sebaceous
glands.
4) Protease: destroys tissue proteins. See fig.5
Fig.4: Luckless red blood cell following a neutrophil, running to destruction at the
hands of Staphylococcus aureus and its hemolysis and leukocidin dynamite.
Fig.5: Staphylococcus aureus produces proteins that
allow the bacteria to tunnel through tissue.
6
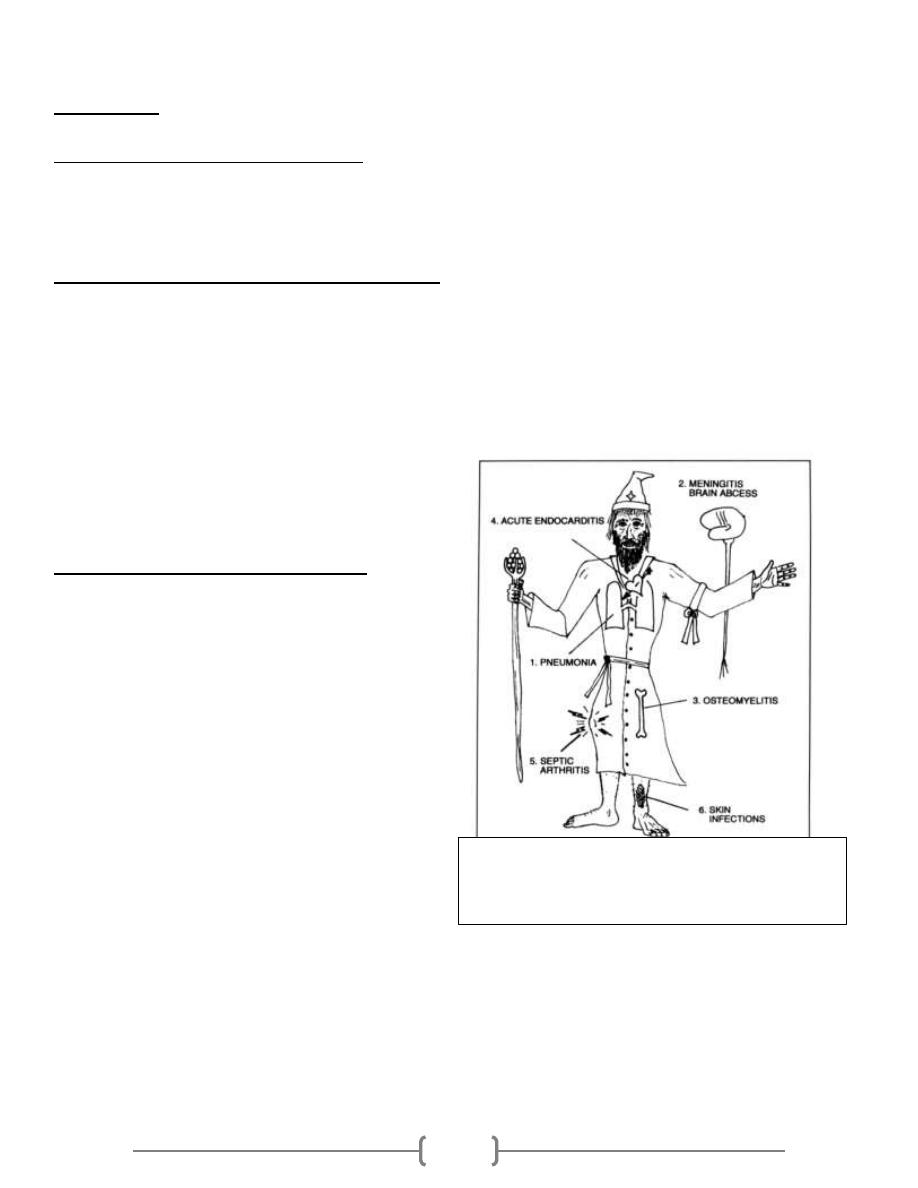
c) Exotoxin Assault Weaponry: (see fig.6)
1) Exfoliatin: A diffusible exotoxin that causes the skin to slough off leads to a disease
called: (SSS “scalded skin syndrome”).
2) Enterotoxins (heat stable): Exotoxins which cause food poisoning 2-6h after eating
preformed toxin, resulting in vomiting and diarrhea. (See fig.7)
3) Toxic Shock Syndrome toxin (TSST-1): This exotoxin is analogous to the pyrogenic
toxin produced by Lancefield group A beta-hemolytic streptococci, but is far more
deadly. This exotoxin causes toxic shock syndrome and is found in 20% of S. aureus
isolates. These pyrogenic toxins are called superantigens which bind to the MHC class II
molecules on antigen presenting cells (such as macrophages). The toxin-MHC II complex
causes a massive T cell response and outpouring of cytokines, resulting in the toxic
shock syndrome described below. (See Fig.8).
Fig.6: Staphylococcus aureus produces exotoxin assault weaponry.
Fig. 8:
Toxic shock syndrome caused by Staphylococcus
aureus releasing TSST-1.
Fig.7: Staphylococcus aureus
gastroenteritis. "I told you not to eat
the mayonnaise, sweetheart!"
7
Diseases:
Disease caused by exotoxin release:
1) Gastroenteritis (food poisoning).
2) Toxic shock syndrome.
3) Scalded skin syndrome (SSS).
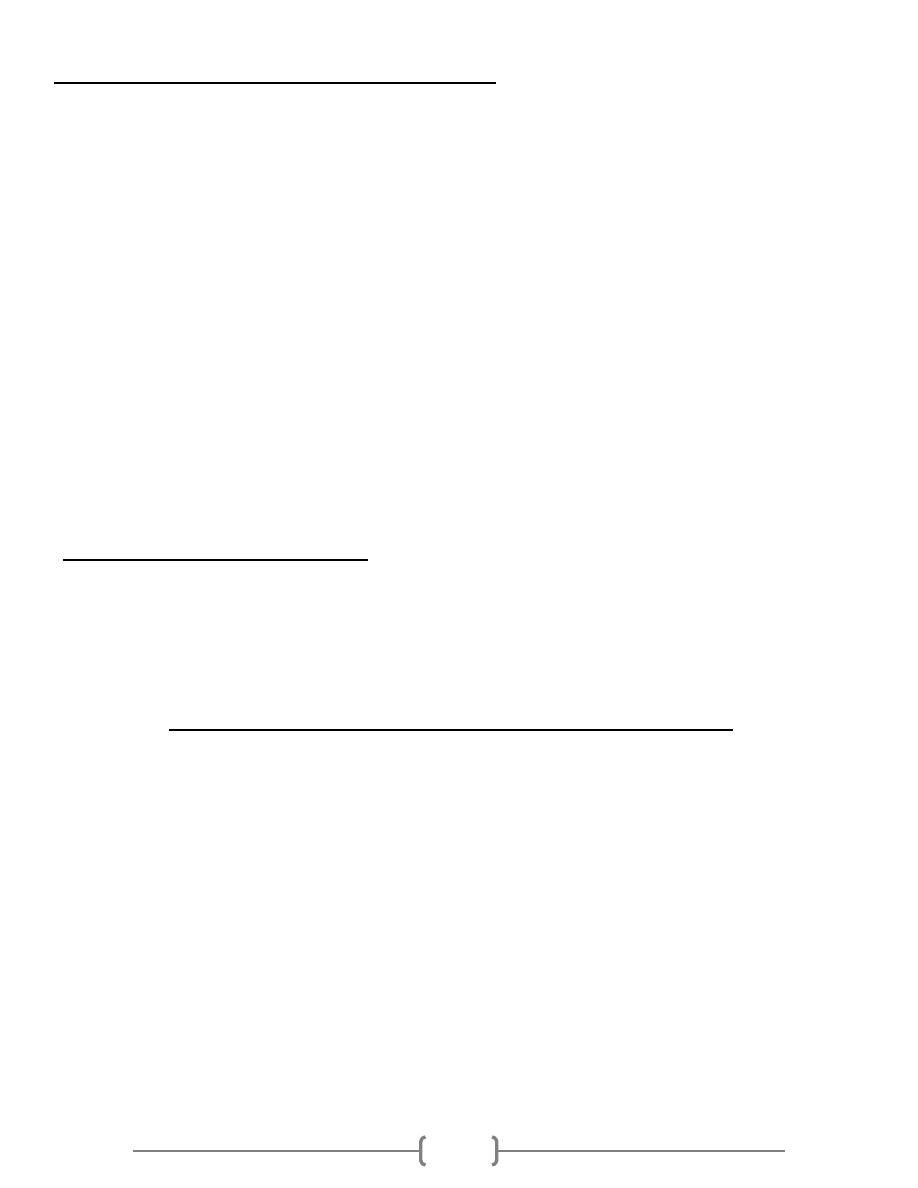
Disease resulting from direct organ invasion: see fig.9
1) Pneumonia
2) Meningitis
3) Osteomyelitis (most common cause).
4) Acute bacterial endocarditis (rapid and destructive, emergency case)
5) Septic arthritis (most common cause in pediatric age and adult above 50, emergency case)
6) Skin infections (Folliculitis, Pustule, Boil (furuncle): e.g. Stye, Carbuncle, Impetigo,
cellulites).
7) Bacteremia/sepsis
8) Urinary tract infection.
Predisposing Factors for Infection:
• Surgery/wounds
• Foreign body (tampons, surgical packing,
sutures)
• Severe neutropenia (<500/ µl)
• Intravenous drug abuse.
• Chronic granulomatous disease
• Cystic fibrosis
Fig.9: Diseases caused by direct organ invasion by
Staphylococcus aureus. Visualize the Staph-wielding
wizard. (Note the cluster of staphylococci at the head
of his staff.)
8
Staphylococcus aureus and antibiotics:
More than 90% of S.aureus strains contain plasmids that encode β-lactamase
(penicillinase), the enzyme that degrades many, but not all, penicillins. Rx. With
β-lactamase–resistant penicillins, e.g., nafcillin or cloxacillin.
Some strains of S.aureus are resistant to the β -lactamase–resistant penicillins, such as
methicillin and nafcillin, by feature of changes in the penicillin-binding protein (PBP) in
their cell membrane. Genes on the bacterial chromosome encode these altered PBPs.
These strains are commonly known as methicillin-resistant S.aureus (MRSA) or
nafcillin-resistant S.aureus (NRSA). MRSA currently accounts for more than 50% of
S.aureus strains isolated from hospital patients in the United States Rx. With
vancomycin.
Strains of S.aureus with intermediate resistance to vancomycin (VISA) and with full
resistance to vancomycin (VRSA) have also been detected. The gene that encodes
vancomycin resistance in S.aureus is located on a plasmid. MRSA, NRSA, VRSA &
VISA can be treated with either Linezolid, quinupristin/dalfopristin or daptomycin.
Mupirocin is very effective as a topical antibiotic in skin infections caused by S.aureus. It
has also been used to reduce nasal carriage of the organism in hospital personnel and in
patients with recurrent staphylococcal infections.
S.aureus can resist antibiotics by:
1) β –lactamase production, encoded by plasmid.
2) Change in molecular structure of PBP, encoded by bacterial chromosome.
3) Resistant to Vancomycin, transmitted from other bacteria, encoded by plasmid.
Staphylococcus epidermidis (Staphylococcus albus
):
Normal bacterial flora of the human skin.
It is coagulase-negative.
Infections are almost always hospital-acquired: compromised hospital patients with
Foley urine catheters or intravenous lines can become infected when this organism
migrates from the skin along the tubing.
Diseases: Infections of prosthetic devices in the body, such as prosthetic joints,
prosthetic heart valves, CSF
shunts, and peritoneal dialysis catheters. In fact,
Staphylococcus epidermidis is the most frequent organism isolated from infected
indwelling prosthetic devices.
The organisms have a polysaccharide capsule (slime layer) that allows adherence to
these prosthetic materials.
(It allows other bacteria to bind to the already existing biofilm, creating a
multilayer biofilm. Such biofilms decrease the metabolic activity of bacteria within them. This decreased
metabolism, in combination with impaired diffusion of antibiotics, makes it difficult for antibiotics to effectively
clear this type of infection)
9
S.epidermidis is highly antibiotic resistant. Most strains produce β-lactamase and many
are methicillin-/nafcillin-resistant due to altered penicillin-binding proteins. The drug of
choice is vancomycin.
Staphylococcus saprophyticus
Normal flora of the female genital tract and perineum. It has been isolated from other
sources too including meat and cheese products, vegetables, the environment, and
human and animal gastrointestinal tracts.
This organism is a leading cause (second only to E.coli) of urinary tract infections
(UTI) in sexually active young women
"Honeymoon cystitis".
It is most commonly acquired by females in the community (NOT in the hospital).
This organism is coagulase-negative, novobiocin resistant.
Urinary tract infections can be treated with a quinolone, such as norfloxacin, or with
trimethoprim-sulfamethoxazole. See table1.
Laboratory features for genus Staphylococcus:
Slide: (microscopic characteristics) :A Gram’s stained film will shows spherical G+ve
cocci arranged in grape like irregular
Culture: (macroscopic characteristics):
- Aerobic or facultatively anaerobic,
- Grow in ordinary media as (nutrient agar or blood agar).
- Tolerate high salt conc. (9%NaCl).
- The colonies are round, smooth, raised & glistening,
- Producing pigments: S. epidermidis & S.saprophyticus white, S. aureus appear
golden-yellow colonies.
- Only S.aureus produces β-hemolysis, a zone of β-hemolysis will appear as clear zone
around the colony on blood agar.
- Only S.aureus can ferment mannitol.
The selective & differential medium used is called (Mannitol salt agar), this medium
contain: Mannitol +7.5% NaCL + Phenol red (indicator), the pink color of the indicator
turn to yellow because of mannitol fermentation & acid production (only by S.aureus), &
the salt inhibit most other normal flora.
10
Steps of laboratory Diagnosis:
1) Specimens: according to type of infection, such as pus, blood, urine…etc.
2) Gram Stain: Gram’s positive cocci, Grape-like arrangement (clusters).
3) Culture: on both
- Blood agar: see large, round, smooth, raised & glistening white or golden color, β-
hemolysis if S.aureus.
- Mannitol Salt Agar: S.aurues: yellowish discoloration of media, other Staphylococci:
no discoloration (remains pink media)
4) Biochemical tests:
a) Coagulase test: is recognized as the most important test for testing the virulence of
S. aureus which is the only coagulase +ve staphylococci. So this test used to detect the
ability of S. aureus to clot blood plasma (fibrinogen fibrin). There are two main
methods: Slide method and tube method.
a) Catalase test: This is done to differentiate Staphylococci from Streptococci. A drop
of 3% H
2
O
2
solution placed on a slide, and a small amount of bacterial growth is in the
solution placed on the slide, the formation of bubbles indicates a positive test of oxygen
release.
5) Serological test: Latex agglutination test to detect S.aureus.
6) Antibiotic Sensitivity test.
7) For epidemiological purposes, S.aureus can be subdivided into subgroups based on
the susceptibility of the clinical isolate to lysis by a variety of bacteriophages. A person
carrying S.aureus of the same phage group as that which caused the outbreak may be the
source of the infections.
Prevention: (very important):
There is no vaccine against staphylococci.
Cleanliness, frequent hand washing, and aseptic management of lesions help to control
spread of S.aureus.
Persistent colonization of the nose by S.aureus can be reduced by intranasal mupirocin
or by oral antibiotics, such as ciprofloxacin or trimethoprim-sulfamethoxazole, but is
difficult to eliminate completely.
Shedders may have to be removed from high-risk areas, e.g., operating rooms and
newborn nurseries.
Cefazolin is often used preoperatively to prevent staphylococcal surgical-wound
infections.
11
It is extremely important to know how to differentiate staphylococci from streptococci because
most staphylococci are penicillin G resistant.
Both staphylococci and streptococci are gram-positive cocci, but they are distinguished by
two main criteria:
1. Microscopically, staphylococci appear in grapelike clusters, whereas streptococci are in
chains.
2. Biochemically, staphylococci produce catalase (i.e., they degrade hydrogen peroxide),
whereas streptococci do not.
Summary:
• S.aureus is the most pathogenic species because of their virulent factors.
• S.aureus colonizes nasal mucosa (25% of population are carriers).
• Staphylococci easily diagnosed in the lab. By using Gram’s staining, culture and biochemical tests.
• S.aureus and S.epidermidis are highly antibiotic resistance and causing nasty hospital acquired
infections.
• Staphylococci infection can be prevented by regular hygiene precautions and by antibiotics, no
vaccine.
References:
-
Review of Medical Microbiology and Immunology11th edition 2010.
-
Clinical Microbiology Made Ridiculously Simple, 6
th
ed, 2014.
-
Baily & Scott diagnostic microbiology, 12
th
ed.
#END
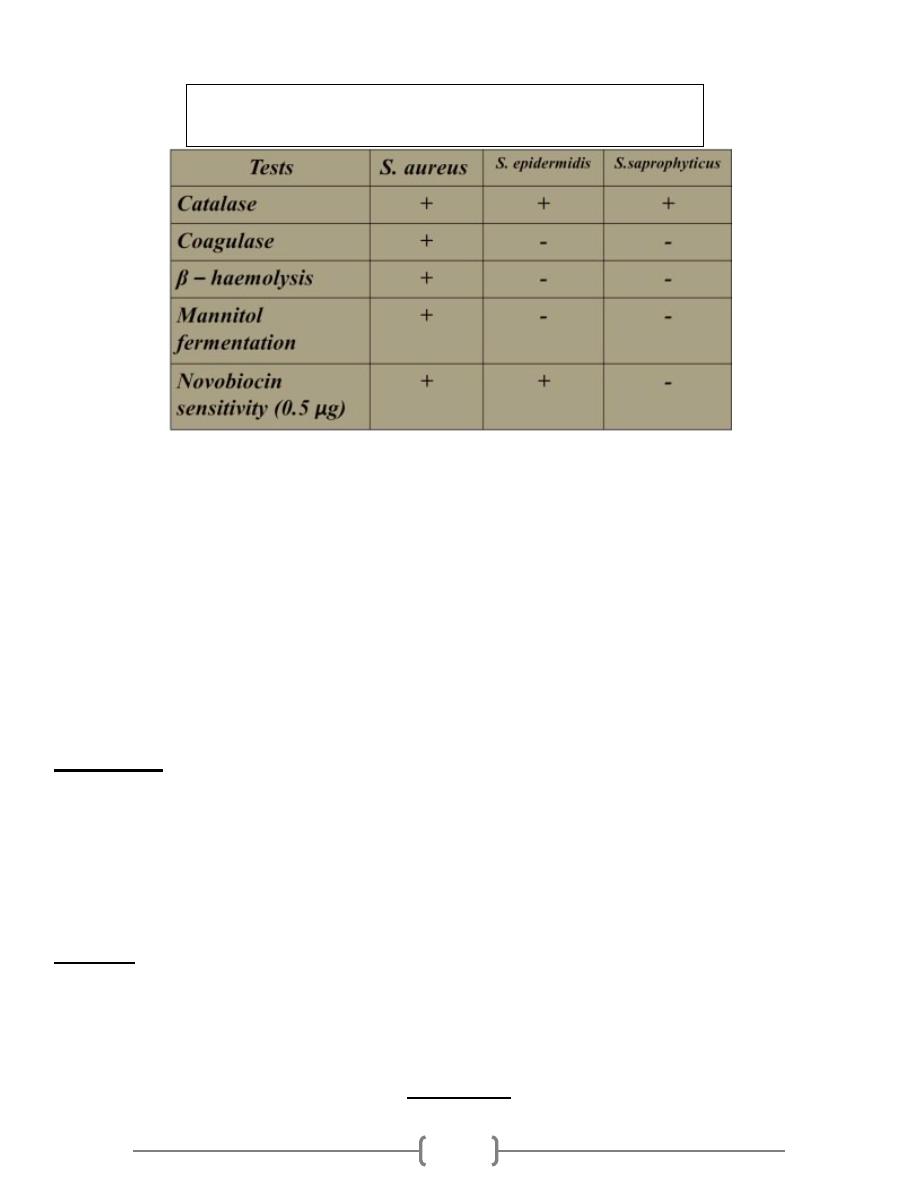
Table 1: summarized the points of differences between 3 medically
important Staphylococci species