IMMUNOLOGY
ا.م.د.هيفاء الحديثي
Immunodeficiency
OBJECTIVES:
1- Define immunodeficiency and list the type of it.
2- Determine each type of congenital deficiency.
3- List the causes of secondary immunodeficiency.
4- Discuss causes, phases and immune status in Acquired immune
deficiency syndrome.
____________________________________________________
When the immune system fails to protect the host from disease-causing
agents or from malignant cells, the result is ID.
ID disorders
Primary (congenital)
secondary acquired
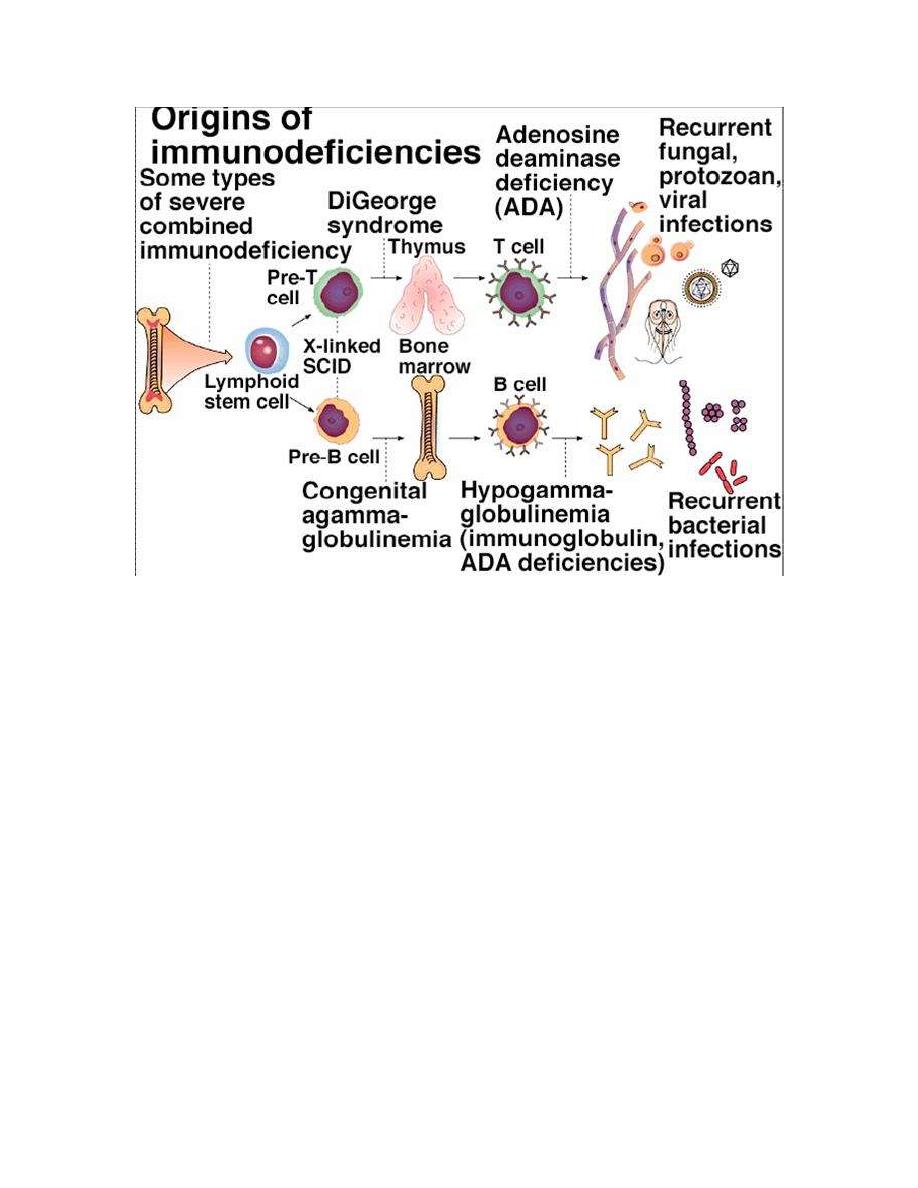
Primary ID:
4 major
immune
components
B-cell
deficiencies
T-cell
deficiencies
Phagocytic cell
defect
Complement
deficiencies
B-cell ID disorders
1. X-linked hypogammaglobulinemia (Bruton’s) low serum level of all
classes of Ig (the level of Abs are absent or greatly reduced) due to
failure in maturation of pre-B cells into B-Cells, also lymphoid organs
are incompletely developed. The actual genetic background for this
disease involves some types of mutation in the gene for an essential
enzyme (Tyrosine Kinase) required by B cells to servive and mature.
Clinically, recurrent pyogenic infections occur in infants at about
6months of age, when maternal Ab is no longer protective. Treatment
with pooled gamma globulin reduces the number of infections.
The transient hypogammaglobulinemia in infancy mainly resolve
by its own by (16-30) months of age.
2. Selective immunoglobulin deficiencies:
Decrease in the level of one Ig or more but with normal or increase
level of other Igs. IgA class deficiency most prevalent (1/600) with
normal quantities of B cells but unable to synthesize IgA. IgA
deficiency result in sinus and lung infections.
Patients with selective Igm deficiency or IgG subclasses deficiency
are liable for recurrent sinopulmonary infections caused by pyogenic
bacteria..
T-cell ID disorders
1. Thymic aplasia (digeorge’s syndrome) results when embryonic
third & 4
th
pharyngeal pouches fail to develop, or associated with
deletion in chromosome 22. Both thymus and the parathyroids fail
to develop properly result is sever viral, fungal or protozoal
infections. The most common presenting symptom is tetany due to
hypocalcemia. Ab production is either normal or decreased.
Thymus transplant may be of some benefit.
2. Chronic mucocutaneous candidiasis, these children who present
with skin and mucous membrane candidal infection have a T-cell
deficiency specifically for Candida albicans. Usually treated with
antifungal drugs.
Combined B-cell and T-cell deficiencies
1. Hyper-IgM syndrome: In this syndrome, sever, recurrent infections
begin early in life. T-helper cells have a defect in the surface protein
that interacts with CD40 on B-cell surface, this result in inability of B-
cell to switch from production of IgM to other classes of Igs.
2. Sever combined Immunodeficiency disease (SCID) this either due to
stem cell defect results in absence of T and B cells or the number of
cells is normal but they do not function properly, some due to gene
mutation or absence of certain enzymes as:
- Adenosine deaminase and nucleosides phosphorylase deficiency.
Lymphocytes develop but a metabolic product build up cells
abnormally and selectively destroy them.
- X-linked deficiency in IL receptors for T&B cells.
- Wiskott-Aldrich Syndrom.
- Ataxia-Telangiectasia.
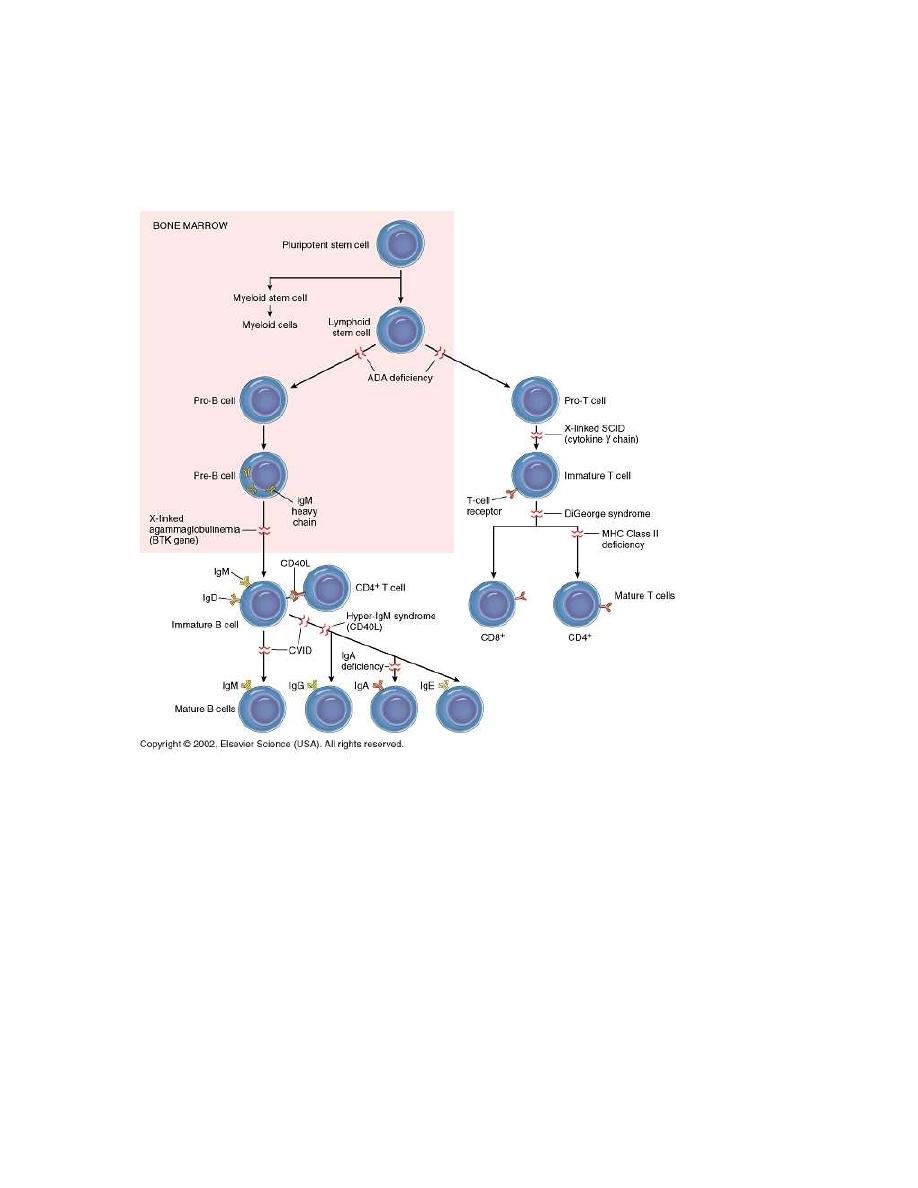
- Also deficient expressional MHC molecules may result in combined
deficiencies as lack of gene that code for HLA, MHC I & MHC II
(Bare-lymphocyte syndrome)
Complement deficiency
Deficiencies in components or functions, grouped as (early component, late
component or alternative cascade deficiencies). These may result in:
1. Hereditary angioedema. Absence of C1-inhibitor
C1 act on C4-
C4a
vasoactive (C3a & C5a)
capillary permeability and
edema in several organs.
2. Recurrent infections

Patient with C3 deficiency are particularly susceptible sepsis with
pyogenic bacteria such as S. aurous.
Those with reduced C6, C7 or C8 are prone to bacteremia with
Neisseria meningitides or Neisseria gonorrhoeae.
3. Autoimmune diseases: Patient with C2 & C4 deficiencies have
autoimmune diseases. C3 deficiency are associated with SLE.
4. Paroxysmal Nocturnal Hemoglubinurea:
Episodes of brownish urine (hemoglobin urea) complement-mediated
hemolysis caused by deficiency of decay-accelerating factor (DAF).
Phagocytic cell defects
1. Quantitative defects
a. Neutropenia
increased destruction decreased production
- Autoimmune phenomena following By bone marrow suppression.
certain drugs Leukemia
- Hypersplenism from Inherited stem cells defect.
exaggerated destructive function.
b. Asplenia
- Congenital
- Surgical
- Malignancy
- Sickle cell anemia
2. Qualitative defects
Defect may involve any of the phagocytic activities (chemotaxis,
ingestion or intracellular killing) as in:
- Chronic granulomatous disease
- G6PD deficiency .
- Job’s syndrome ( characterized by increase IgE, sever atopic
dermatitis& repeated pyogenic infections).
- Lazy leukocyte syndrome
- Chediak-Higashi syndrome ( abnormality in lysosomal granules)

Secondary immune deficiencies
1. Malnutrition-Zinc deficiency
-Vitamine deficiency
2. Systemic disorders-renal insufficiency
-Extensive burns
3. Drug induced-alcohol
-Opiates
-Immune suppressive treatment during
transplantation or cancer
Postsurgery- Transient depression of immune function due to surgery
itself or general anesthesia
4. Splenectomy
5. Thymetomy
6. Malignancy -NHL
-B cell malignancy
7. Infectious diseases
a. Bacterial infection (TB)
IL10 & IL4
↓ Th1
b. Parasitic infection (trypanosome Cruzi) ↓ CMI
c. Measles & other viral infections
Transient suppression of
delayed hypersensitivity.
d. Acquired immune deficiency syndrome (AIDS)
Caused by human immunodeficiency virus (HIV) which interact
with a large number of different cells in the body and escaping the
host immune response against it. Transmit through sexual
intercourse and contact with infected blood, and infected mothers
can pass HIV to their infants.

Phases (clinical stages) of HIV infection
- Acute retroviral infection lasting from infection until onset of
detectable virus-specific Ab. lasts 3-8 weeks (IMN like symptoms)
- Asymptomatic phase: last for mouths to >15 years but viral replication
continues and the immune response is active and virus escape.
- Clinical progression to AIDS, the host immune response. Include
early & late symptoms and followed by advanced infection (full-
blown syndrome)
HIV and immune system
- Primary cellular target is CD4
+
, the initial interaction between HIV &
CD4
+
involves specific region (gp120) and CD4
+
, and this interact
with a protein found on the surface of some immune cells as co-
receptor accepting HIV (CCR5).
The expression of CD4 and CCR5 is highest in memory T-cells, so
their rapid loss leads to increasing ID.
Reduced CD4 T cells may also result in an incomplete activation of
CD8 T cells, resulting in a decreased ability to destroy virally
infection cells. Also down regulation of HLA class I
inactivation of
CD8 T cells [During asymptomatic phase, cell mediated immunity is
prominent and CD8
+
& CD28
+
cells release a soluble factor that
inhibit the replication of HIV]
- High mutation rates of HIV also allow virus to escape immune
responses.
- A stronger humeral response against HIV can be detected
(neutralizing Ab against gp120 & gp41) but the virus does not expose
the immune dominant region of gp120 invivo, preventing the
effectivity of gp120 Ab.
Diagnosis of HIV infection
- Screening of anti-HIV Ab by ELISA
- Confirmatory test by western blot to detect structural protein (P24)
and envelope glycol-proteins *gp41 & pg120).
- By PCR

Treatment of AIDS
Ant-retroviral drugs inhibit the growth and replication of HIV at various
stages of its life cycle. Now highly active anti-retroviral therapies develop
include combination of more than one inhibitor. (HAART).
Attacking HIV with antiretroviral drugs
SUMMARY:
1-
When the immune system fails to protect the host from disease-causing
agents or from malignant cells, the result is ID.
2-
Primary ID:
4 major
immune
components
B-cell
deficiencies
T-cell
deficiencies
Phagocytic cell
defect
Complement
deficiencies
3-
Secondary immune deficiencies include:
Malnutrition, Systemic disorders, Drug induced, Postsurgery, Splenectomy,
Thymetomy, Malignancy and Infectious diseases
4- Acquired immune deficiency syndrome (AIDS)
Caused by human
immunodeficiency virus (HIV) which interact with a large number of
different cells in the body and escaping the host immune response against it.
Brought to you by :
Ali Kareem