SURGERY
LEC. 21
Dr. Yasser Naif Qassim
Lec. 1
BURNS
Tues. 7 / 4 / 2015
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2014 – 2015
BURNS Dr. Yasser Naif Qassim
7-4-2015
2
BURNS
3
rd
year Dr. Yasser Naif Qassim
Plastic surgery
………………………………………………………………………………………
………………………………….
Burn is a coagulation necrosis of the skin and underlying tissues to a variable
depths.It could be due to thermal , electrical or chemical causes.
Thermal injuries are caused by:
1-hot liquids (scalds)
→ superficial to superficial dermal burns.
2-flame
→ deep dermal or full thickness.often associated with inhalational injury and other
concomitant trauma.
3-contact with hot object
→ deep dermal or full thickness burns.Common in an unconscious or
epileptic patients.
Electrical injuries are caused by conversion of electricity into thermal energy:
Domestic electricity
→ Low voltages tend to cause small, deep contact burns at the exit and entry
sites.Its alternating nature can interfere with the cardiac cycle
→ dysrrhythmias.
High tension injuries occur when the (voltage is 1000 V or greater). There is extensive tissue
damage in addition to cardiac dysrrhythmias.
“Flash” injuries can occur when there has been an arc of current from a high tension voltage
source.The heat from this arc
→ superficial burns.
Chemical injuries are caused by acids or alkalis.
These burns tend to be deep and
alkalis tend to penetrate deeper and cause worse burns than acids.
The body response to a burn :
Burn injuries result in both local and systemic responses.
Local response:
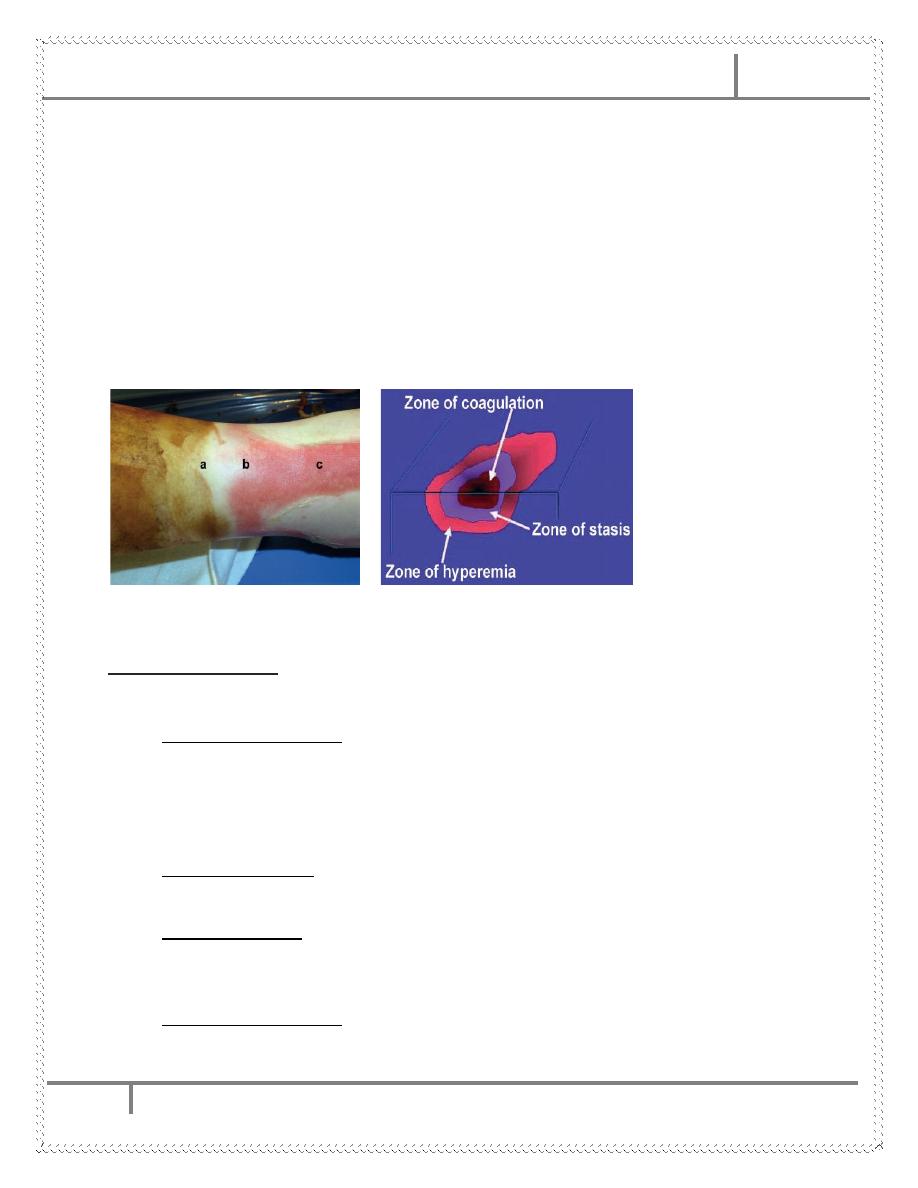
The three zones of a burn were described by Jackson in 1947.
BURNS Dr. Yasser Naif Qassim
7-4-2015
3
a.Zone of coagulation—This occurs at the point of maximum damage. In this zone there is
irreversible tissue loss due to coagulation of the constituent proteins.
b.Zone of stasis—Surrounds the zone of coagulation and is characterised by decreased tissue
perfusion. The tissue in this zone is potentially salvageable. The main aim of burns
resuscitation is to increase tissue perfusion here and prevent any irreversible damage.
Additional insults—such as prolonged hypotension, infection, or oedema—can convert this zone
into an area of complete tissue loss.
c.Zone of hyperaemia—In this outermost zone tissue perfusion is increased. The tissue here will
invariably recover unless there is severe sepsis or prolonged hypoperfusion.
These three zones of a burn are three dimensional, and loss of tissue in the zone of stasis will
lead to the wound deepening as well as widening.
Jackson burn zones
Systemic response:
The release of cytokines and other inflammatory mediators at the site of injury has
a systemic effect once the burn reaches 25 – 30 % of total body surface area.
Cardiovascular changes—Capillary permeability is increased→ loss of intravascular
proteins and fluids into the interstitial compartment→edema.
Peripheral and splanchnic vasoconstriction occurs. Myocardial contractility is decreased
,possibly due to release of tumour necrosis factor . These changes, coupled with fluid loss
from the burn wound, result in systemic hypotension and end organ hypoperfusion.
Respiratory changes—Inflammatory mediators cause bronchoconstriction , and in severe
burns adult respiratory distress syndrome can occur.
Metabolic changes—The basal metabolic rate increases up to three times its original rate.
This, coupled with splanchnic hypoperfusion, necessitates early and aggressive enteral
feeding to decrease catabolism and maintain gut integrity.
Immunological changes—Non-specific down regulation of the immune response occurs,
affecting both cell mediated and humoral pathways.
BURNS Dr. Yasser Naif Qassim
7-4-2015
4
Hematologic—There is immediate red blood cell destruction in direct proportion to the
extent of the burn, particularly third-degree burns. Endothelial injury may lead to release
of thromboplastins and to collagen exposure; the latter then initiates platelet adhesion,
aggregation, and contact activation of factor XII. Severe full-thickness burns induce
consumption of coagulation factors at the burn site, which contributes to the (DIC).
Gastrointestinal—Ileus is universal in patients with burns of more than 25% total body
surface area (TBSA). Gastric and duodenal mucosal damage, secondary to focal
ischemia, can be observed as early as 3–5 hr postburn. If the mucosa is unprotected, the
early erosions may progress to frank ulceration.
Endocrine—In the early postburn period, a catabolic endocrine pattern develops that is
characterized by elevated glucagon, cortisol, and catecholamine levels with depressed
insulin and triiodothyronine levels→ negative nitrogen balance. Their magnitude
correlates with the size of the burn area.
Assessment of burn area(surface area and depth):
It is important that all of the burn area is exposed and assessed.During assessment,
the environment should be kept warm .
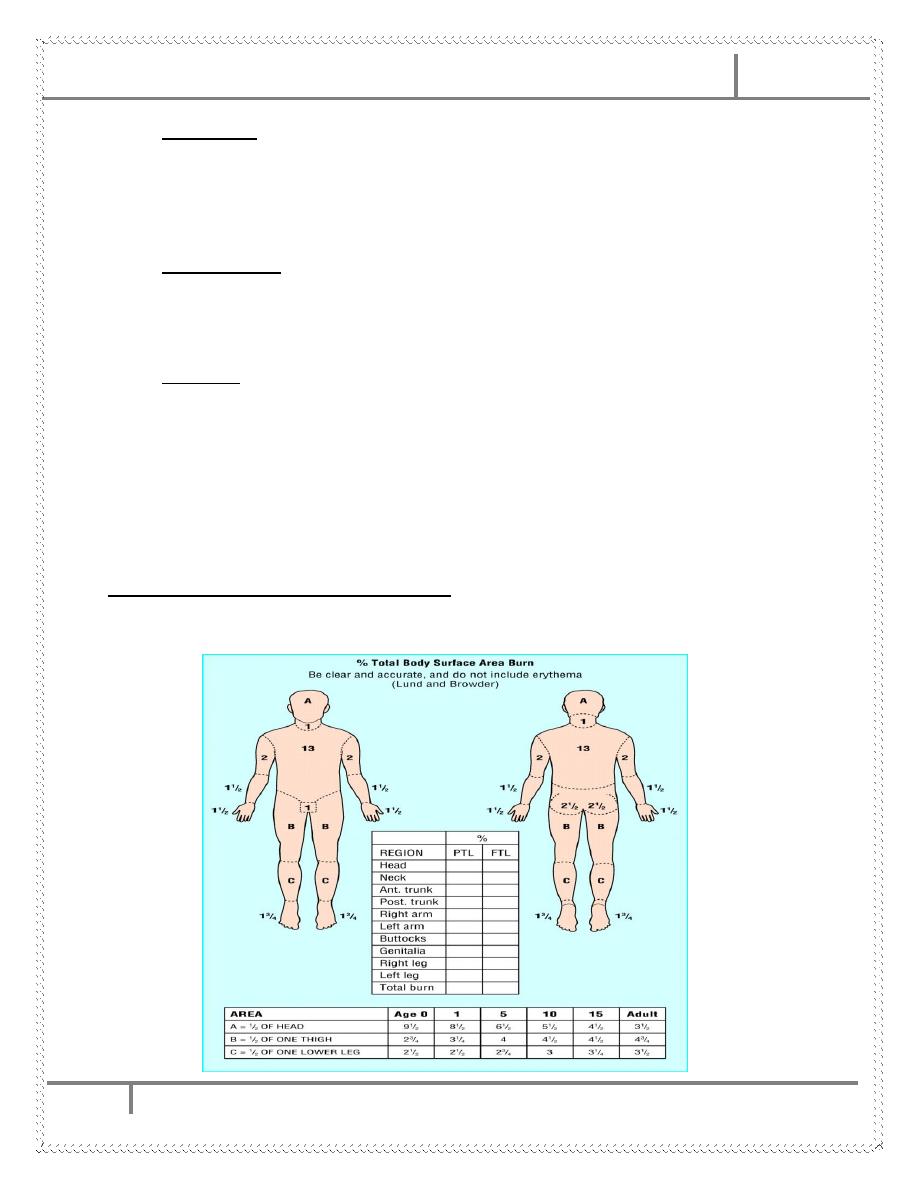
1-Assessment of burn surface area by:
a. Lund and Browder chart , the most accurate method .
BURNS Dr. Yasser Naif Qassim
7-4-2015
5
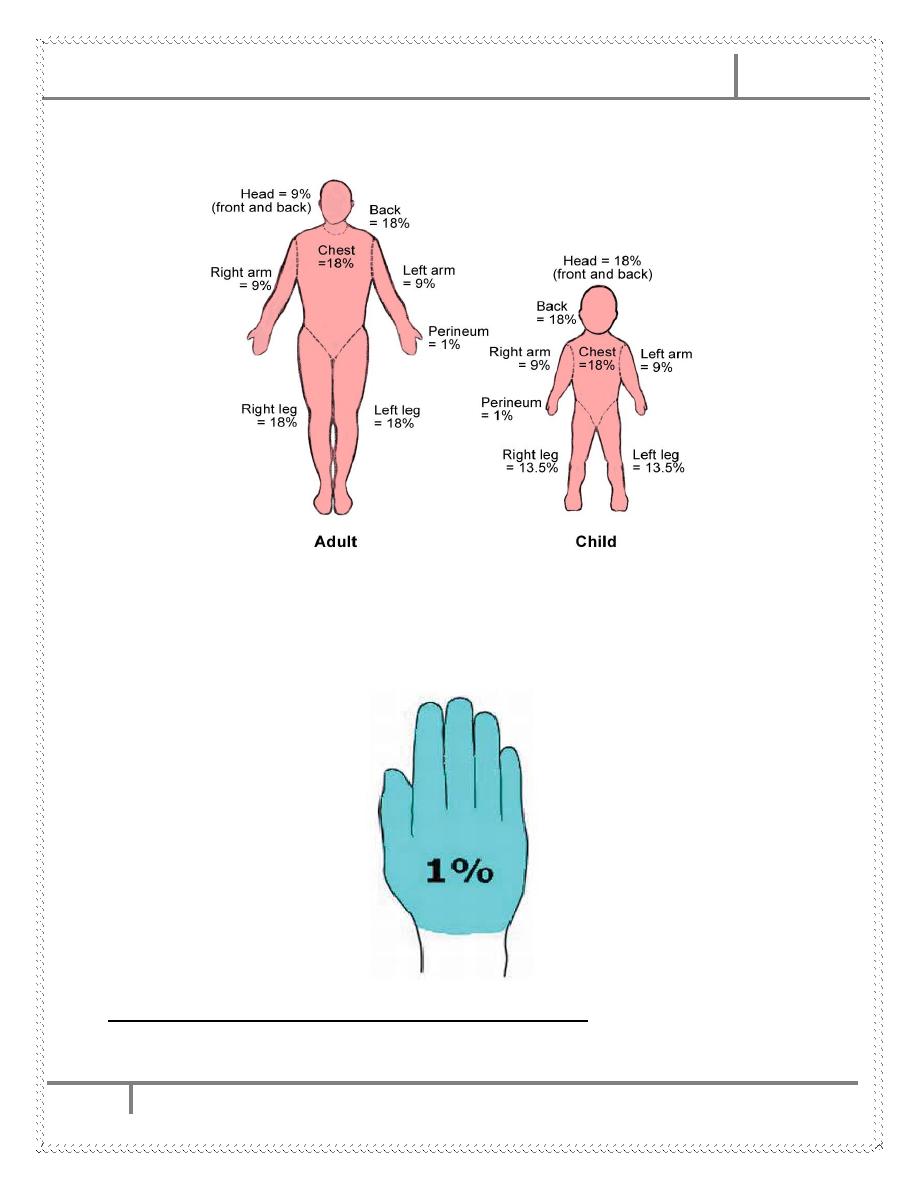
b.Wallace rule of nines.
b. Rule of palm—The surface area of a patient’s palm (including fingers) is roughly 0.8 -
1% of total body surface area.
2-Assessment of burn depth by clinical examination : as shown in the table
below.
BURNS Dr. Yasser Naif Qassim
7-4-2015
6
Bu
rn
degr
ee
(D
epth)
Skin
lay
er
inv
o
lv
ed
Cli
n
ical
app
earan
ce
P
ain
Sen
satio
n
Cap
illar
y
Refill
1
st
d
eg
ree
(S
u
p
erfi
cia
l)
Ep
id
ermis
o
n
ly
Erythe
m
at
o
u
s
P
ai
n
fu
l
+
v
e
bris
k
retu
rn
2
nd
d
eg
re
e
(p
ar
ti
al
th
ic
kn
es
s)
Su
p
erficia
l 2
nd
d
egree
(S
u
p
e
rfi
cial
p
ar
tial
)
Epi
d
erm
is
+
P
ap
illar
y D
er
m
is
P
in
k
to
r
ed,M
o
ist,
Bli
ste
rs.
Very
P
ain
fu
l
+v
e
Sl
o
w
return
D
ee
p
2
nd
d
egree
(D
e
e
p
p
ar
tial
)
Epi
d
erm
is
+pap
illar
y D
er
m
is
+
P
ar
t
o
f R
et
icu
lar
D
er
m
is.
M
o
tt
led
pin
k ,c
h
err
y re
d
&
white,
D
ry
,Bli
ste
rs
(larg
er
).
D
u
ll
-ve
3
rd
d
eg
re
e
(Fu
ll th
ic
kn
es
s)
Fu
ll t
h
ickness
Skin
(Epid
erm
is
+D
er
m
is)
Mi
x
ed
whi
te,
d
ark
an
d k
ha
k
i
c
ol
ou
rs
.T
he
s
k
in i
s
dr
y
,
lea
the
ry
or
wax
y
.T
hrom
bo
s
ed
v
es
s
el
s
m
ay
be
s
ee
n u
nd
er t
he
es
c
ha
r.
In
sensate
-ve
4
th
d
eg
re
e
Fu
ll t
h
ickness s
kin
+
Su
b
cutan
eo
u
s
ti
ssues
(Fat,
M
u
scle,
Te
n
d
o
n
, Bo
n
e
…
.et
c).
As 3
rd
d
egree
b
u
t w
ith
the
in
vo
lv
em
ent
and
e
xp
o
sur
e
o
f
sub
cutan
eo
u
s
structur
es.
In
sensate
-ve
BURNS Dr. Yasser Naif Qassim
7-4-2015
7
Criteria for referral to a burn unit (indications for admission to hospital):
1. Second and third degree burns greater than 10% TBSA in patients younger than 10 years and
older than 50 years.
2.Second and third degree burns greater than 20% in other age groups.
3.Third degree burns greater than 5%.
4.Burns to face, hands, feet, genitalia, perineum and major joints.
5.Electrical burns (including lightning injury).
6.Chemical burns.
7.Inhalation injury.
8.Patients with pre-existing medical conditions e.g. DM.
9.Circumferential deep burns to extremity or chest.
10.Burns with concomitant trauma e.g. chest or severe head injuries.
Apart from these indications, the patient is managed as an out-patient as the
followings:
1-Open large blisters(the small one can be left) and wash with normal saline or sterilized water
and soap.
2-Pain killers.
3-Topical antimicrobial agents:
• Silver sulfadiazine (1% Silvadene , Flamazine).
• Mafenide acetate (Sulfamylon).
• Silver nitrate (0.5%).
4- With or without systemic antibiotics.
5-Dressing→ Ideally, a burn dressing should be absorbent, non-adherent, and should act as a
barrier to prevent colonization of the wound by pathogenic bacteria.
BURNS Dr. Yasser Naif Qassim
7-4-2015
8
Management of in-patients :
1-ABC rule of trauma.
2-100% O2.
3-Two or more IV lines,if not possible →Venous cutdown.
4-Urine catheter to assess urine output.
5-Fluid
resuscitation:
There is no ideal resuscitation regimen,all the fluid formulas are only guidelines.
The main aim of resuscitation is to maintain tissue perfusion to the zone of stasis and so prevent
the burn deepening.
Burns covering more than 15% of total body surface area in adults and more than 10% in
children warrant formal resuscitation.
The most commonly used resuscitation formula is the Parkland formula(crystalloid formula):
Total fluid requirement in ml per 24 hours =
4 ml×(total burn surface area (%))×(body weight (kg))
50% of the calculated amount is given in first 8 hours.The other 50% is given in next 16
hours.
High tension electrical injuries and inhalational injuries require more than this amount.
Children require maintenance fluid in addition to this at an hourly rate of
4 ml/kg for first 10 kg of body weight plus
2 ml/kg for second 10 kg of body weight plus
1 ml/kg for > 20 kg of body weight.
The starting point for resuscitation is the time of injury,NOT the time of admission and the
burn area of the first degree should NOT be included . The preferred crystalloid fluid is
Ringer lactate.
At the end of 24 hours, colloid infusion is begun at a rate of 0.5 ml×(total burn surface area
(%))×(body weight (kg)), and maintenance crystalloid (usually dextrose-saline) is continued at a
rate of 1.5 ml×(burn area)×(body weight).
Parkland formula is merely a guideline to the probable amount of the fluid required. This should
be continuously adjusted according to urine output (0.5-1.0 ml/kg/hour in adults and 1.0-1.5
ml/kg/hour in children) and other physiological parameters(CVP,pulse rate, blood pressure).
Investigations at intervals of four to six hours are mandatory for monitoring a patient’s
resuscitation status mainly packed cell volume(PCV).
BURNS Dr. Yasser Naif Qassim
7-4-2015
9
6-
Management of pain:
Morphine IV, (not in neonates), 0.1 mg/kg/dose ,4-6 hourly( do not
use it more frequently than
every 2 hours).
Pethidine IV, 1-1.5 mg/kg/dose , 4-6 hourly.
7-Tetanus prophylaxis .
8-When the burn surface area is 25% or more of deep burn,the patient is liable to
develop paralytic ileus and stress gastro-dudenal erosions or ulcers
→ put an NG
tube and prescribe antacids.
9-
There is no role for prophylactic antibiotic therapy.Give antibiotics when there
are features of infections.
10-Frequent checking of pcv,s.electrolytes,and renal function tests.
11-
Escharotomy and fasciotomy may be needed for circumferential deep
constricting burns.Both are useful to treat distal ischemia in the extremities.
Escharotomy may also be needed in deep circumferential burns involving the
chest to prevent respiratory embarrassment.
12- Nutrition support: Give high calorie and high protein diet In addition to
Vitamins A and C, Iron and Zinc suppliments.
13-Local wound care:by wound debridment and excision of all the devitalized
tissues,daily wash with water and soap(hydrotherapy),application of local
antimicrobial agents e.g. silver sulfadiazine,mafenide acetate …etc.The partial
thickness (2
nd
degree) burns heal within 2-3 weeks.Full thickness(3
rd
degree) burns
do not heal , but granulate
→ skin grafts.In 4
th
degree burns
→multiple wound
excisions and even amputations with skin grafts or flaps.Dont forget splinting the
wounds overlying the joint crease to prevent contractures.
14-Psychlogical support.
15-Rehabilitation and physiotherapy.
BURNS Dr. Yasser Naif Qassim
7-4-2015
10
Burn complications:
1-Shock:
a.neurogenic due to severe pain.
b.hypovolemic due to
↑capillary permeability→interstitial odema and
intravascular hupovolemia
→organ hypoperfusion and multiple organ failure
may be the end result.
c.septic shock in severe uncontrolled infections.
2-Wound infection and septicaemia.
3-UTI and pneumonia.
4-GIT problems
→paralytic ileus and stress ulcers.
5-Anaemia .
6-DVT.
7-Scarring and contractures.
8-Psychological trauma.
#END
Done by
Ali Kareem

FLUID RESUSCITATION Dr. Yasser Naif Qassim
14-4-2015
11
Fluid Resuscitation
Parkland formula(crystalloid formula) :
• Total fluid requirement in ml / 24 hours = 4 ml× total burn surface area
(%) × body weight (kg))
• 50% → first 8 hr.
The other 50% is given in next 16 hr.
High tension electrical injuries and inhalational injuries require more
than this amount.
Children require maintenance fluid in addition
The starting point for resuscitation is the time of injury ,NOT the time of
admission and the burn area of the first degree should NOT be included.
The preferred crystalloid fluid is Ringer lactate.
At the end of 24 hours, colloid infusion is begun at a rate of 0.5 ml×(total
burn surface area (%))×(body weight (kg)), and maintenance crystalloid
(usually dextrose-saline) is continued at a rate of 1.5 ml×(burn
area)×(body weight).
Maintenance fluid :
Up to 10 kg 4 cc/kg/hr or 100 cc/kg/24 hrs
From 11- 20 kg 2 cc/kg/hr or 50 cc/kg/24 hrs
≥ 21 kg 1 cc/kg/hr or 20 cc/kg/24 hrs
At the 3
rd
post-burn day→Oral feeding or the maintinence IV fluids.
Parkland formula is merely a guideline to the probable amount of the fluid
required. This should be adjusted according to urine output (0.5-1.0
ml/kg/hour in adults and 1.0-1.5 ml/kg/hour in children).