Dr. Tarek Al-Obaidi
Lec. 1
DISEASES OF THE
APPENDIX
Tues. 10 / 3 / 2015
DONE BY :
Qasim M. Al-Hussainy
مكتب اشور لالستنساخ
2014 – 2015

1
|
P a g e
Diseases of the Appendix
Anatomy: the vermiform appendix is present only in humans, certain anthropoid apes
and wombat. It is blind muscular tube with mucosal, submucosal , muscular and serosal
layers. Morphologically , it is underdeveloped distal end of the large cecum found in
many lower animals.
At birth, the appendix is short and broad at its junction with the cecum, but
differential growth of the cecum produces the typical tubular structure by about the
age of two years.
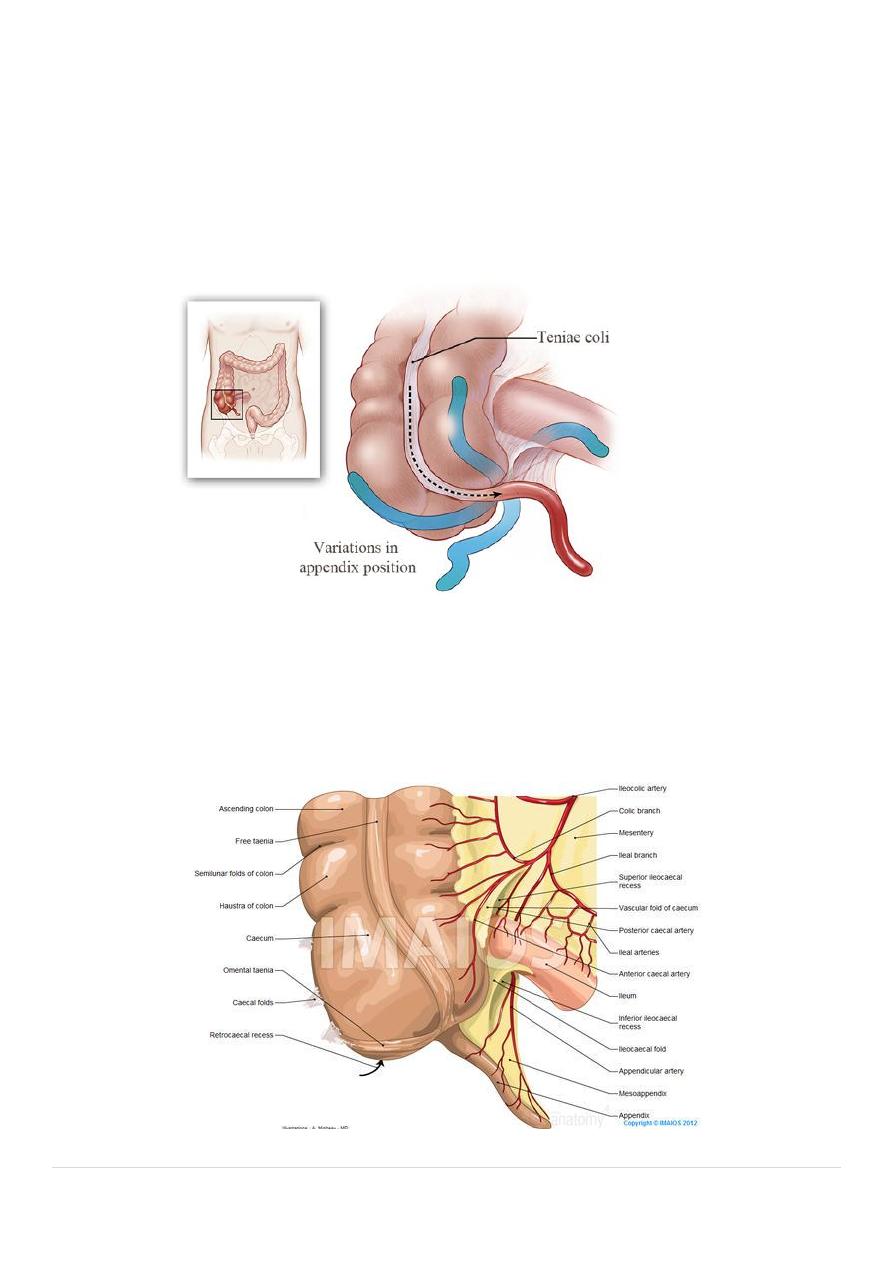
During childhood , continued growth of the cecum commonly rotates the appendix
into a retrocecal but intraperitonial position, in approximately one quarter of cases
rotation of the appendix does not occur resulting in pelvic, subcecal, or paracecal
position. Occasionally the or tip of the appendix becomes extraperitoneal lying
behind the cecum or ascending colon . rarely the cecum does not migrate during
development to its normal position in the right lower quadrant of the abdomen.
2
|
P a g e
In these circumstances the appendix can be found near the gall bladder (subhepatic)
or in the case of intestinal rotation , in the left iliac fossa, causing diagnostic difficulty
if appendicitis develops. the position of the base of the appendix is constant, being
found at the confluence of the three taeniae coli of the cecum, which fuse to form
the outer longitudinal muscle coat of the appendix. at operation, use can be made of
this to find an elusive appendix, as gentle traction on the taeniae coli, particularly the
anterior taenia, will lead the operator to the base of the appendix.
The mesentery of the appendix or mesoappendix arise from the lower surface of the
mesentery or the terminal ileum and is itself subject to great variation. Sometimes as
much as the distal one third ofb the appendix is bereft of mesoappendix. Especially in
the childhood, the mesoappendix is so transparent that the contained blood vessels
can be seen . in many adults, it becomes laden with fat, which obscures these vessels.
3
|
P a g e
•
The appendicular artery , a branch of the lower division of the ileocolic artery , passes
behind the terminal ileum to enter the mesoappendix a short distance from the base
of the appendix. It then comes to lie in the free border of the mesoappendix. An
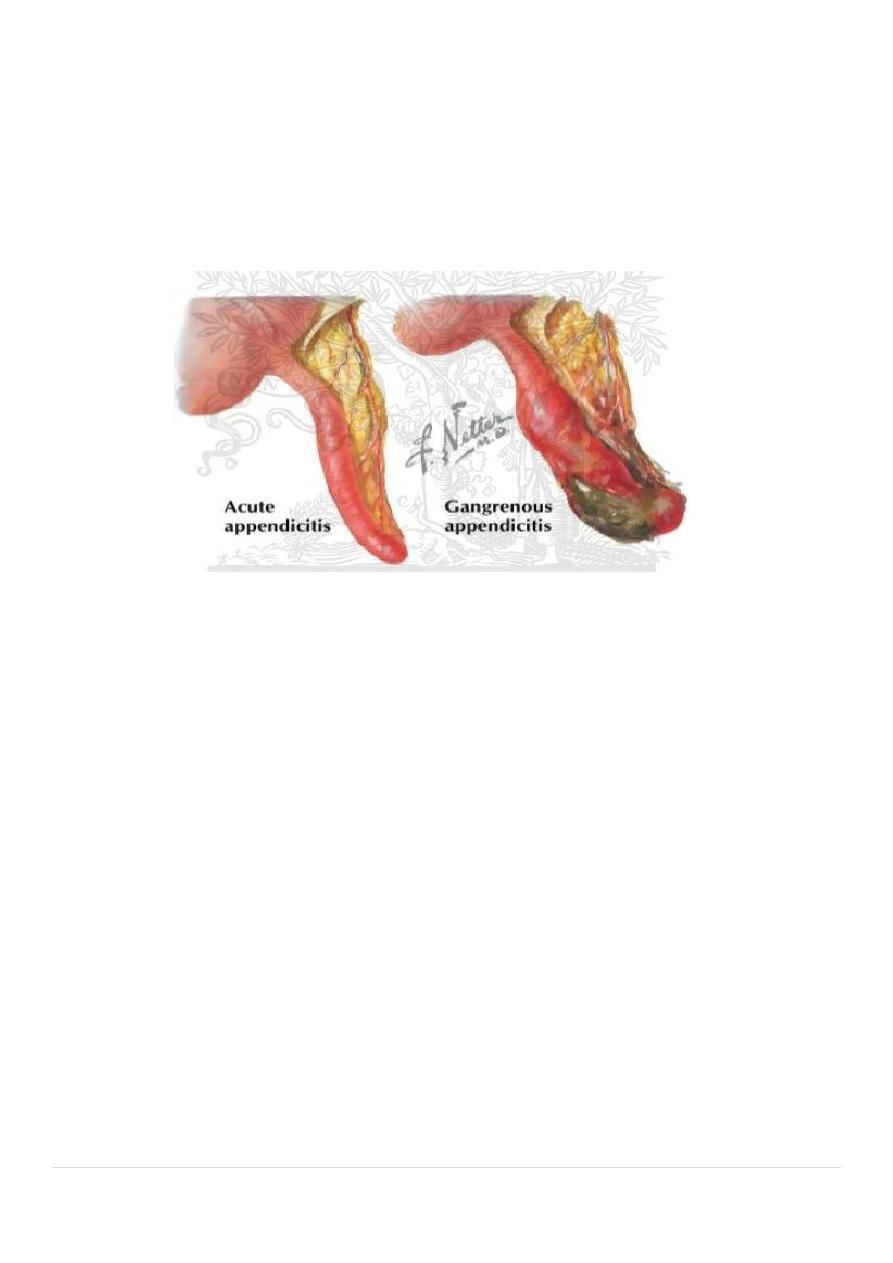
accessory appendicular artery may be present but in most people the appendicular
artery is an end artery, thrombosis of which results in necrosis of the appendix as in
gangrenous appendicitis. Four, six of more lymphatic channels traverse the
mesoappendix to empty into the ileocecal lymph nodes.
Microscopic Anatomy: the length of appendix vary between average 7.5 cm and 10 cm. the
lumen is irregular folded of mucus membrane lined by columnar cell intestinal mucosa of
colonic type. Crypts are present but are not numerous. In the base of the crypts lies
argentaffin cells (kulchitsky cells), which may give rise to carcinoid tumor. The submucosa
contains numerous lymphatic aggregation or follicle but of no change in immune system
following appendectomy, and it explain the frequency of acute appendicitis in young adults.
Acute appendicitis: it is the most common surgical emergency in the world, and its
incidence is increased in the first half of this century specially in Europe , America and
Australia with up to 16% of the population undergoing appendectomy. It is relatively rare in
infants and becomes increasingly common in childhood and early adult life reaching peak
incidence in the teens and early 20s.
After middle age the risk of developing the disease is quite small. The incidence is equal in
male and female before puberty. In teenagers and young adults the ratio male to female is
increase to 3:2 at age of 25, thereafter the incidence in male declines.
4
|
P a g e
Etiology: no specific cause for acute appendicitis but there are a lot of factors are
responsible, as low fiber diet and high refined carbohydrates may share in etiology.
The incidence is decreased in western countries due to good hygiene and change in
the pattern of gastrointestinal infection in childhood related to increase in use of
antibiotics may be responsible.
Appendicitis is usually associated with bacterial proliferation with in the appendix ,
no single organism is responsible , mixed growth of aerobic and anaerobic organisms
is usual.
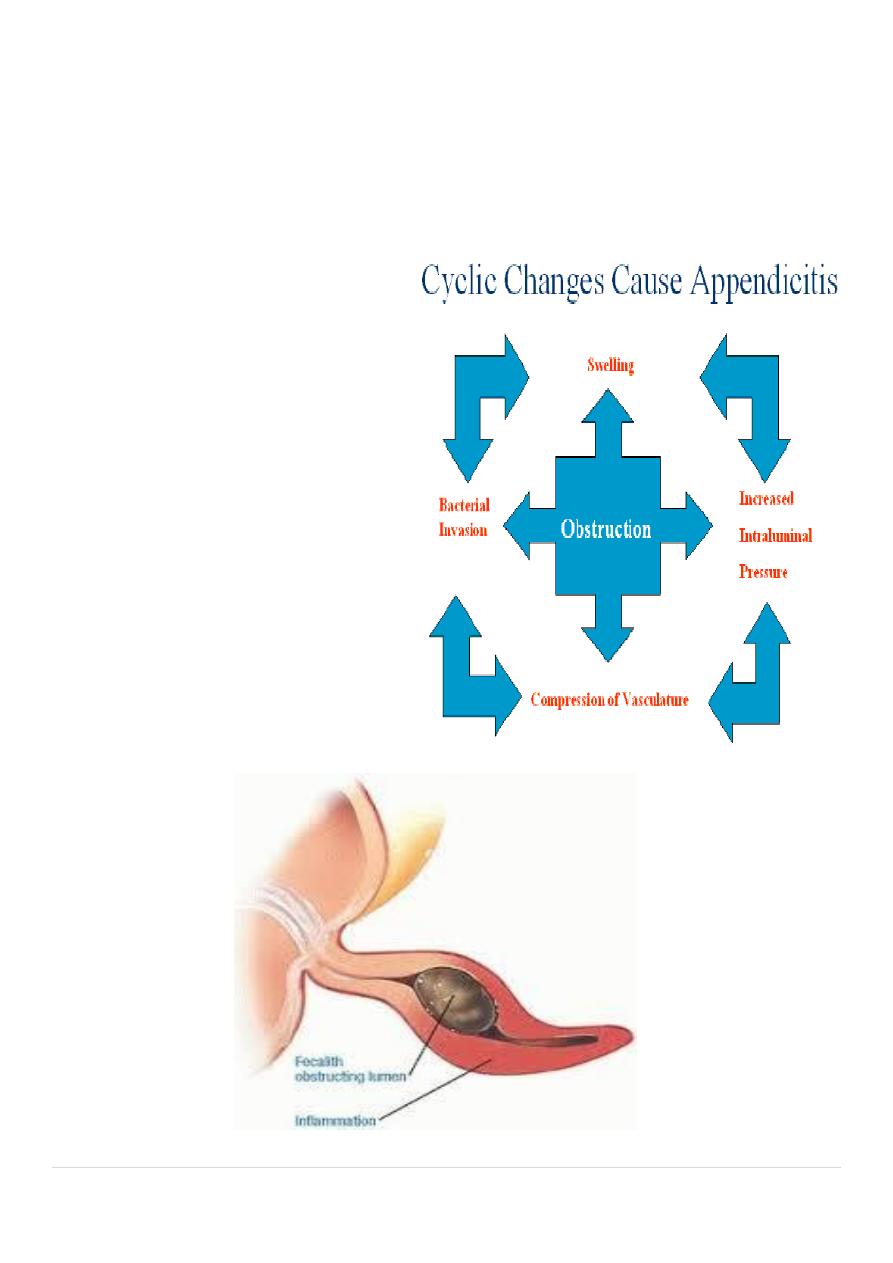
The initiating point for proliferation of
bacteria is controversial. Obstruction of
the appendix lumen has been widely
held to be important, and some form of
luminal obstruction either by fecolith or
stricture is found in majority of cases. A
fecolith is composed of inspissated fecal
material , calcium phosphate, bacteria
and epithelial debris, rarely foreign body
is incorporated into the mass. A
presence of a fecolith is a relative
indication for prophylactic
appendectomy.
5
|
P a g e
A fibrotic stricture of the appendix is usually indicate previous appendicitis that
resolved without surgical intervention. Obstruction of appendicular orifice by tumors
particularly carcinoma of cecum is an occasional cause of appendicitis in middle age
or elderly patients. Intestinal parasites particularly Oxyuris vermicularis pin worm can
proliferate in the appendix and occlude the lumen
Pathology: obstruction of the lumen seems to be essential for development of
appendicecal gangrene and perforation . yet, in many cases of early appendicitis, the
appendix lumen is patent despite the presence of mucosal inflammation and lymphoid
hyperplasia. Viral infection can occurs in children with seasonal variation more cases
between May and August in north Europe than other times of the year.
Lymphoid hyperplasia narrows the lumen of the appendix leading to luminal
obstruction , once obstruction occurs continued mucus secretion and inflammatory
exudate increase intraluminal pressure obstructing lymphatic drainage . edema and
mucosal ulceration develop with bacteria translocation to submucosa. Resolution at
this point may occur either spontaneously or in response to antibiotics therapy.
If the condition progresses further distension of the appendix may cause venous
obstruction and ischemia of the appendicular wall. With ischemia, bacterial invasion
occurs through the muscularis properia and submucosa producing acute appendicitis,
with free contamination to peritoneal cavity..
Alternatively, the greater omentum and loops of small bowels becomes adherent to
the inflamed appendix , walling off the spread of peritoneal contamination and
resulting in a phlegmonous mass or paracecal abscess. Rarely appendicecal
inflammation resolves , leaving a distended mucus-filled organ termed a mucocele of
the appendix
Peritonitis is a bad complication of acute appendicitis and to be as result of free

6
|
P a g e
migration of bacteria through an ischemic appendicular wall or from frank
perforation or gangrenous appendix or from delayed perforation of appendicular
abscess.
Factors that may play a role in perforation and peritonitis are extremes of age,
immunosuppression, diabetes and fecolith obstruction of the appendix lumen, a free-
lying pelvic appendix and previous abdominal surgery that limits the ability of the
greater omentum to wall off the spread of peritoneal contamination. At this case a
rapid deteriorating clinical course is accompanied by signs of diffuse peritonitis and
systemic sepsis syndrome called septic shock.