Dr. Nabeel Al-Dawoodi
Lec. 2
ULCERS, SINUSES &
FISTULAE
Tues. 31 / 3 / 2015
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2014 – 2015
Ulcers, Sinuses & Fistulae Dr. Nabeel Al-Dawoodi
31-3-2015
2
Investigation
D. Mellitus – Urine sugar/ RBS/FBS
Infective - fbc, culture
TB
- CXR, AFB, ESR
Syphilis
- KT, VDRL
Discharge – smear, Gram stain, C&S
Biopsy - wedge/incisional biopsy margin of the ulcer &
normal tissue which allows
• (a) comparison with normal tissue
• (b) known organ &
• (c) +/- or infiltration
Curling’s ulcer
–
acute peptic ulcer in burn as a reaction to stress
Cushing’s ulcer
–
acute PU in head injury, early days following spinal cord injury
Marjolin’s ulcer
–
malignant change in a scar, ulcer, sinus (Chr.venous ulcer,
burn, Chr.OM sinus – slow growth – avascular, painless – scar not
have cut. nerve fibres, late lymphatic spread – obliterated lymphatics)
Ulcers, Sinuses & Fistulae Dr. Nabeel Al-Dawoodi
31-3-2015
3
Principles of Assessment
1. Combination of aetiologies in any one lesion, especially diabetic foot.
2. Pain indicates invasion of nerve endings.
3. When the diagnosis relates directly to treatment, biopsy may be necessary.
SINUS & FISTULA
SINUS ~
A tract which connects a cavity lined by granulation tissue (usually an old
abscess) with an epithelial surface. {blind tract leading from surface down to
tissue}
FISTULA ~
Pathological connection between 2 epithelial surfaces usually lined by
granulation tissue but can become epithelialized.
Ulcers, Sinuses & Fistulae Dr. Nabeel Al-Dawoodi
31-3-2015
4
History
Since birth - preauricular sinus;
due to Osteomyelitis(high fever + swelling + bone pain)
TB -lymph node enlargement or TB bone or joints
Perianal- h/o perianal/ischiorectal abscess (intermittent contraction
of anal sphincter prevent proper rest)
Ulcers, Sinuses & Fistulae Dr. Nabeel Al-Dawoodi
31-3-2015
5
[Pain + inflammatory/blockage; Fever/redness of surrounding skin
inflammatory]
Past history
TB, Crohn’s, U.colitis, actinomycosis, colloid Ca,
operation complication
Family history
TB, Crohn’s, U.colitis
INSPECTION
1.
Number
–
Single/Multiple (watering can perineum – Crohn’s
rectum/anal canal, U.Colitis – fistulae; actinomycosis (multiple
sinueses)
2.
Site
– Preauricular (failure of fusion of ear tubercles - at root of
helix or on tragus of pinna; direction – upwards and backwards)
Branchial (2nd & 5th branchial arch) at the lower 3rd of the neck in
front of sternomastoid muscle
Pilonidal – in the middle behind, finger webs
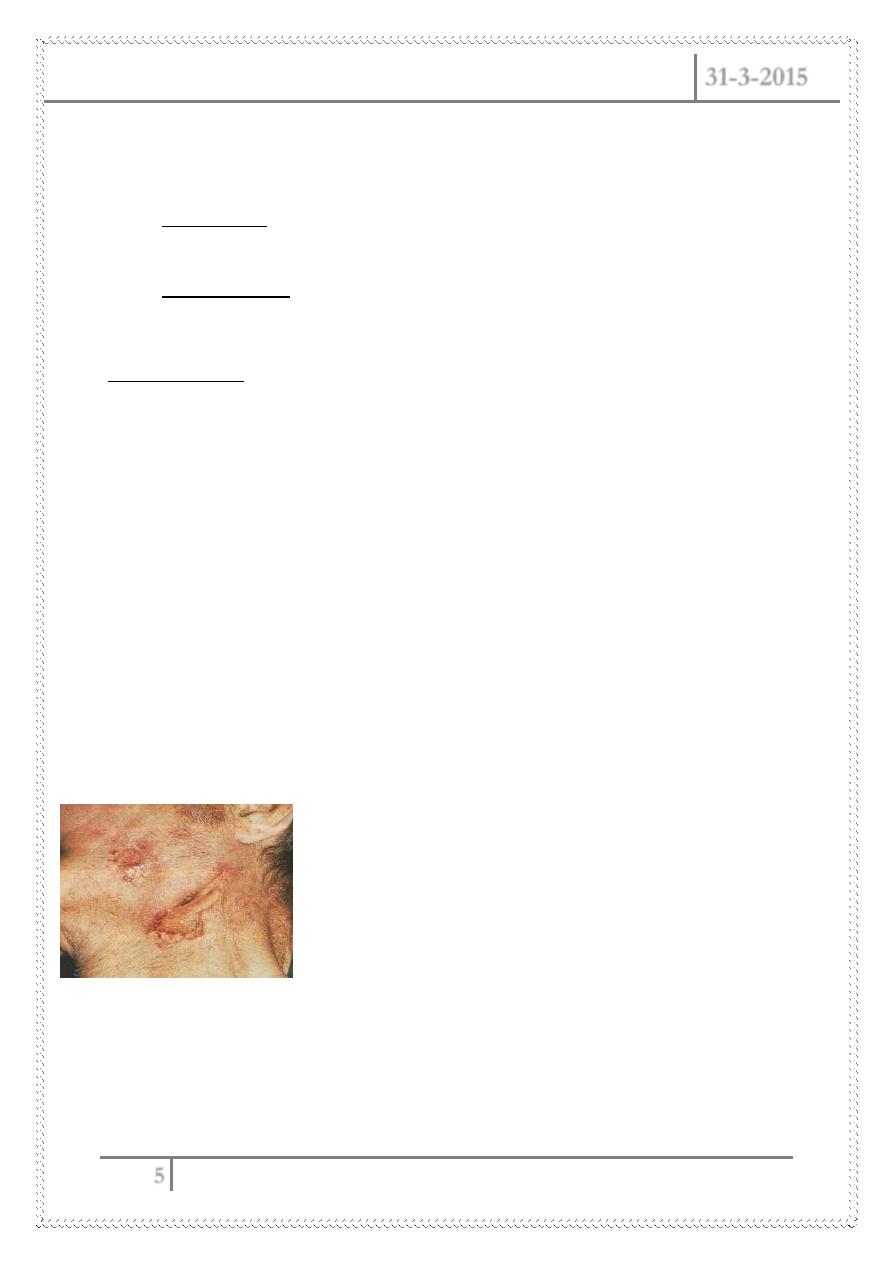
Actinomycosis – multiple indurated sinuses in upper part
o the neck
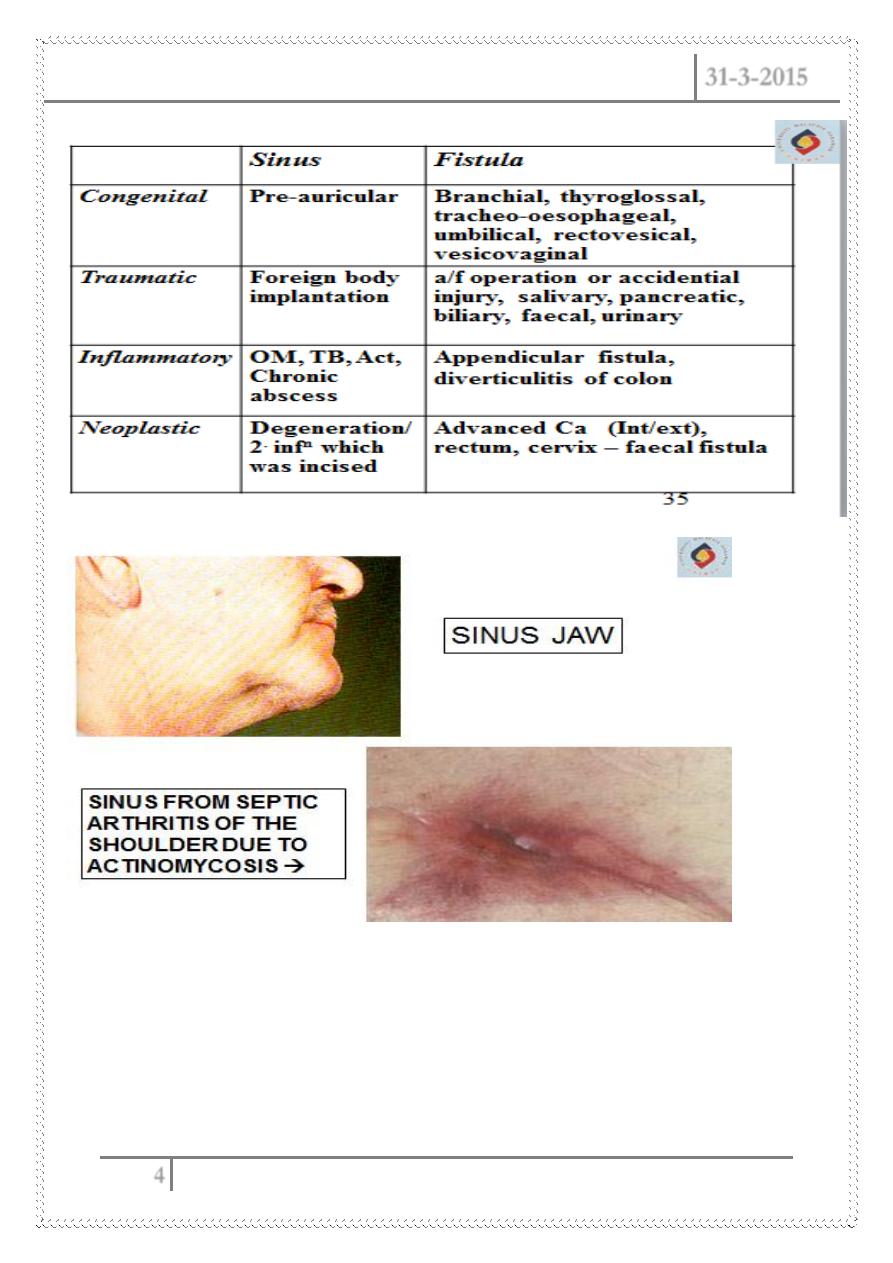
A single sinus over the lower irregular jaw – due to
osteomyelitis OM
Actinomycosis of the left side of the jaw with multiple
sinus formation.
3. Opening of sinus
Sprouting granulation tissue - + of FB (stitch, sequestrum, bullet)
Wide margin, thin blue undermined edge – TB Sinus
Ulcers, Sinuses & Fistulae Dr. Nabeel Al-Dawoodi
31-3-2015
6
4. Discharge
OM plus; TB serosanguinous; Actinomycosis sulphur granule
Urine, faeces, bile
Skin :
5. Surrounding skin
Scar indicating Chr. OM or previously healed TB.
Dermatitis with pigmentation Chron’s / Actinomycosis
PALPATION
1.
Tenderness Inflammatory source OM
2.
Wall of sinus thickening –fibrosis– chronicity
3.
Mobility Sinuses resulting from OM is fixed to bone (irregular, thickened,
tender)
4.
Lump + in neighbourhood TB adenitis
5.
Examination of draining lymph nodes
Examination with a probe (with due precaution)
direction and depth of sinus
presence of F/B (sequestrum), moveable at wound depth
fistula communicated with a hollow viscus or not
whether fresh discharge comes out on withdrawal of the probe or
Ulcers, Sinuses & Fistulae Dr. Nabeel Al-Dawoodi
31-3-2015
7
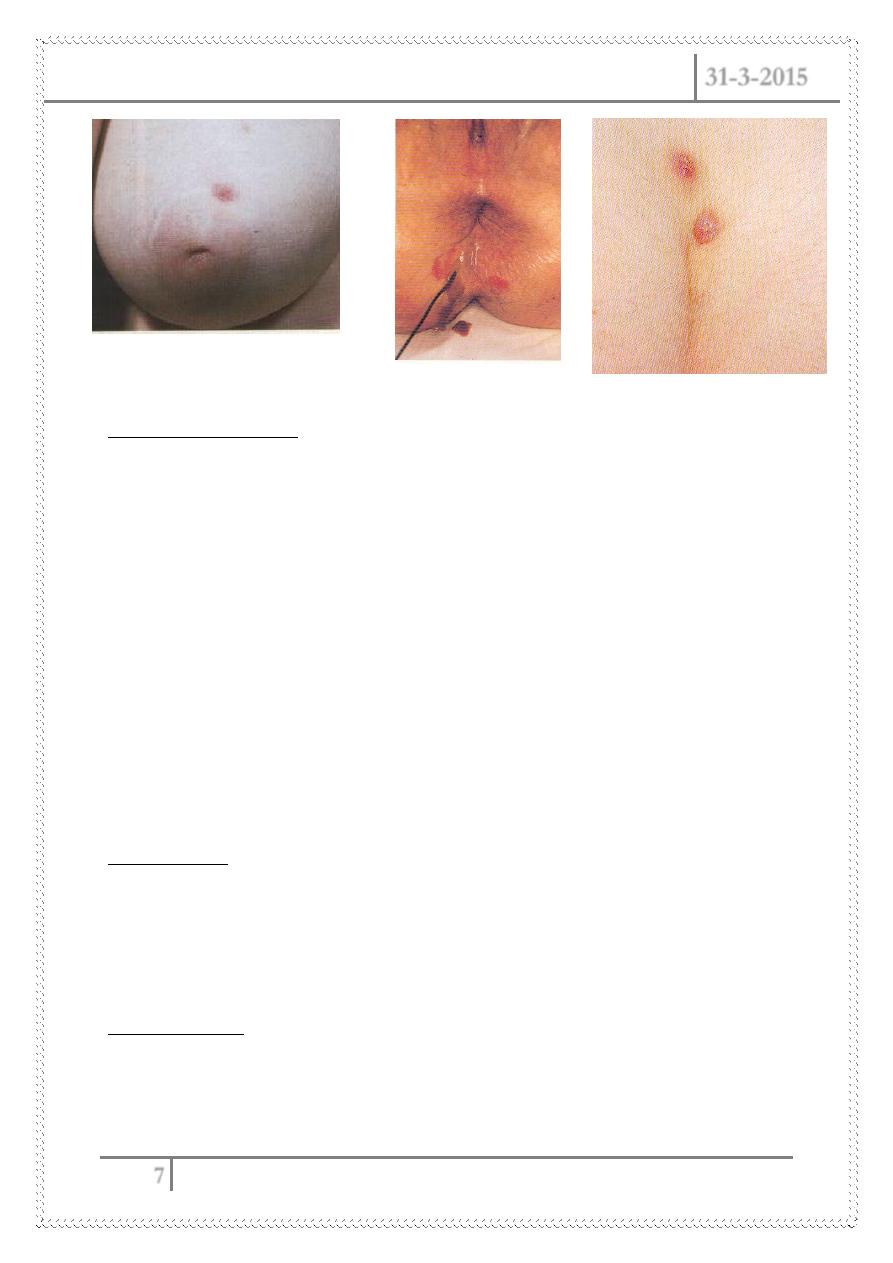
not
Mammary fistula
General Examination
Depends on site and cause – particular system
Sinus in loin - spine, ribs, kidneys
Chronic empyema - chest
Osteomyelitis- bone
Around anus- PR/proctoscopy, sigmoid scope, whole abdomen
Multiples in perineum/scrotum lower urinary tract
Groin sinus hip joint/spine (bursting of cold abscess)
Ixs:
Investigatons
Examination of discharge – marcro/physical/chemical/microscopy
X-rays - sequestrum, opaque foreign bodies/ sino/fistulogram
Failure to close
Inadequate drainage
Specific infection (actinomycosis, TB, syphilis)
Ulcers, Sinuses & Fistulae Dr. Nabeel Al-Dawoodi
31-3-2015
8
Foregin body (stitch)
Epitheliazation of cavity
Malignant change in the cavity
Dense fibrosis around the wall of the tract preventing collapse (empyema)
Absence of rest
Ulcers, Sinuses & Fistulae Dr. Nabeel Al-Dawoodi
31-3-2015
9
Done by :
Ali Kareem