Dr. Ahmed Khalaf
Lec. 1
SKIN TUMOUR
Tues. 21 / 4 / 2015
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2014 – 2015
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
2
SKIN TUMOUR
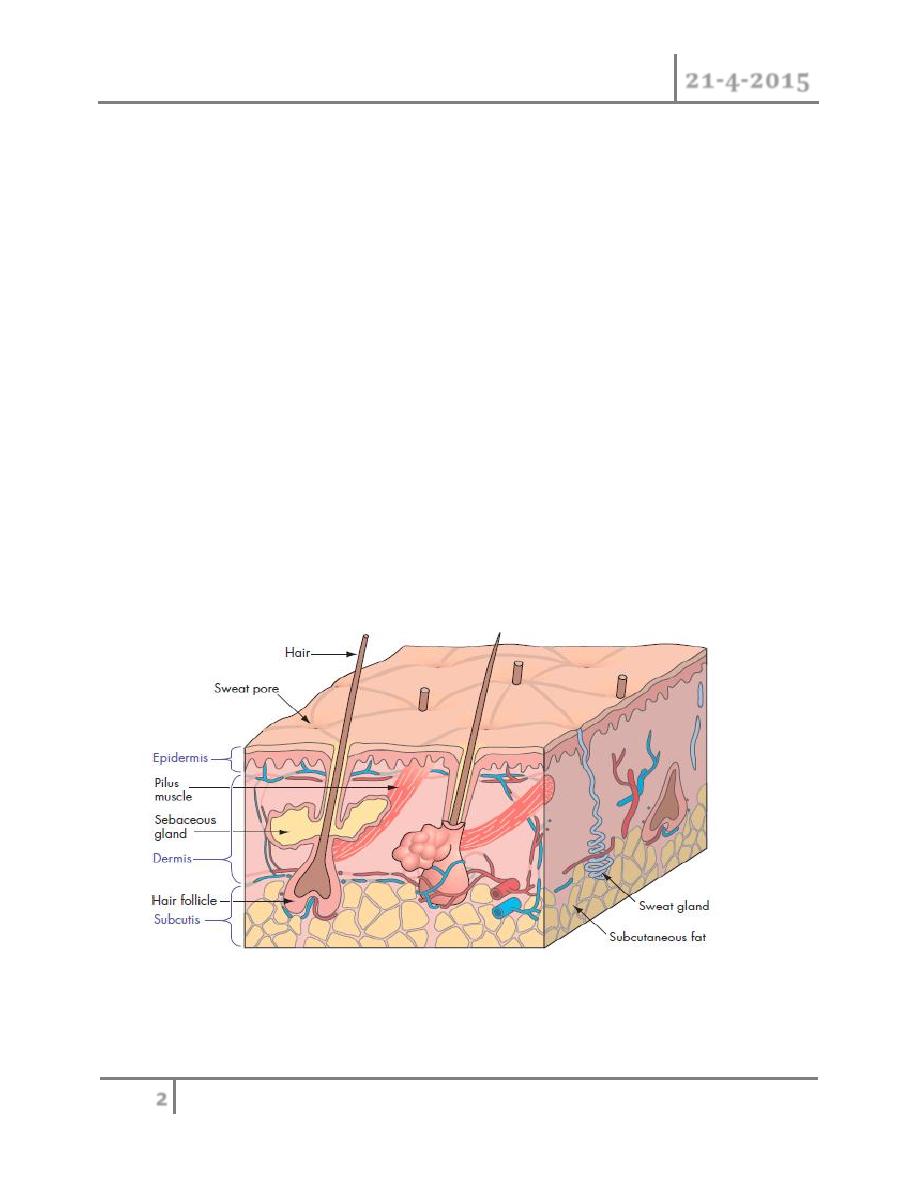
ANATOMY OF SKIN :
Epidermis
The epidermis is composed of keratinised, stratified, squamous epithelium
and can be subdivided further into five layers: the stratum basale (deepest),
the stratum spinosum, the stratum granulosum the stratum lucidum and the
stratum corneum (superificial). It accounts for 5% of the total skin.
Dermis
The dermis constitutes 95% of the skin and is structurally divided into two
layers. The superficial papillary layer is composed of delicate collagen and
elastin fibres in ground substance, into which a capillary and lymphatic
network ramifies . The deeper reticular layer is composed of coarse
branching collagen, layered parallel to the skin surface
Skin adnexa
Adnexal structures such as hair follicles and sebaceous and sweat glands
span both the epidermal and dermal layers and contain some keratinocytes

SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
3
in their ducts. In injuries in which epidermis is lost, re-epithelialisation
occurs from these structures as well as from the wound margins.
FUNCTION OF THE SKIN :
Barrier to the environment: trauma, radiation, pathogens
Temperature and water homeostasis.
Excretion (e.g. urea, sodium chloride, potassium, water).
Endocrine and metabolic functions.
Sensory organ for pain, pressure and movement.
Swelling of the skin and subcutaneous tissues it could be arise from :
- Epidermis - Blood vessels
- Dermis - Sebaceous gland
- Subcutaneous fat - Hair follicle
- Nerves - Sweat gland
Could be benign or malignant .
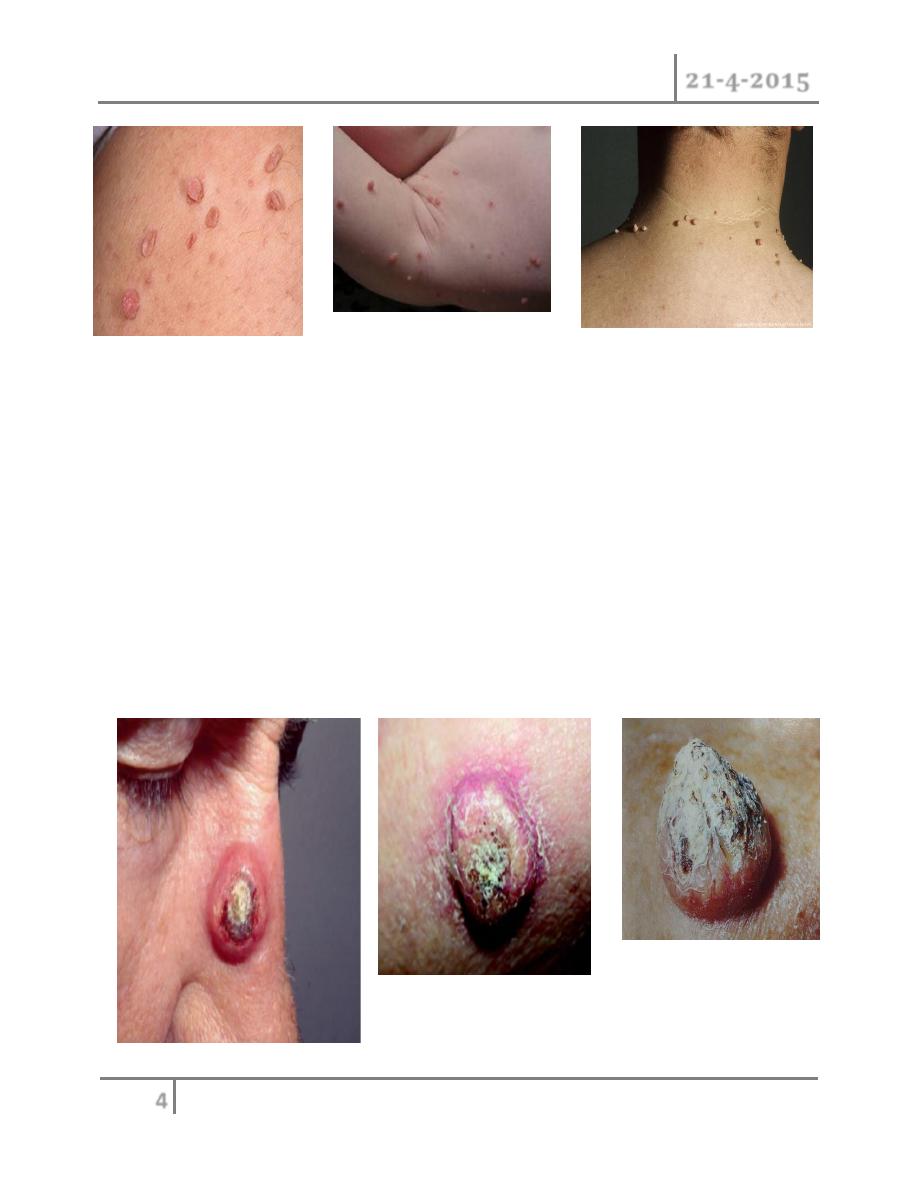
Fibroepithelial polyp (skin tag):
It of unknown aetiology. Theories include viral infection, hormonal
imbalance, localized paucity of elastic tissue, or from skin rubbing up
against skin, since they are so often found in skin creases and folds .
Associated with obesity and non-insuline dependent diabetes.
Is a simple overgrowth of all layers of the skin with central fibrovascular
core. It occurs anywhere on the skin, commonly in axilla or on neck, it
small soft pedunculated skin neoplasm , they have colour of the normal skin.
It can become red and swollen and ulcerated if it is injured. Very common ;
46% of population have one.
Treatment : reassurance; excision if symptomatic such as when it irritated
by clothing.
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
4
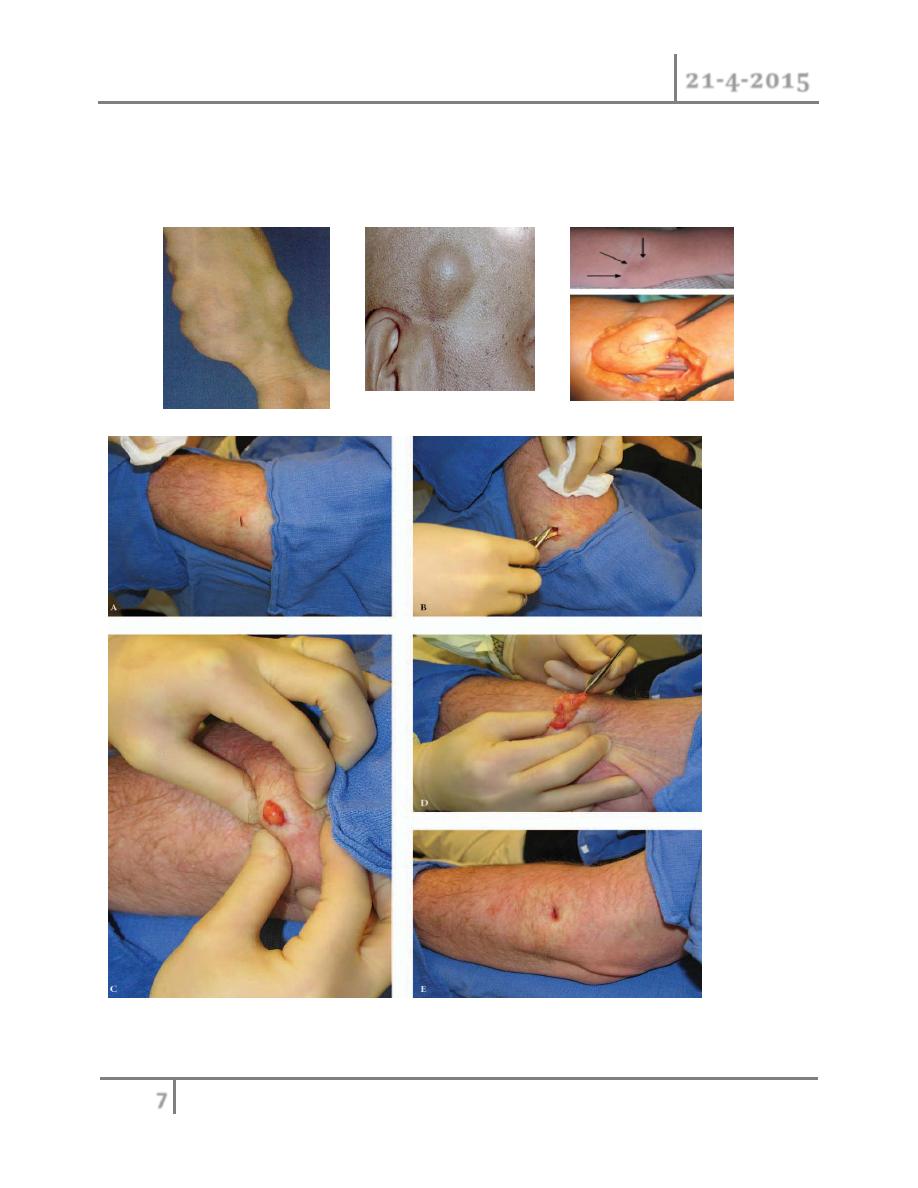
Keratocanthoma :
Is rapidly growing nodule (over weeks to months) with central ulceration or
keratin plug that found mainly in sun exposed skin, usually Present as round
swelling on the face or hands 1-2cm in diameter..
It is self limiting overgrowth and subsequent spontaneous.
Keratocanthoma can be difficult to be distinguish histologically from
squamous cell carcinoma.
Treatment : although keratocanthoma may regress spontaneously, the
tumor should be excised for histopathologic confirmation. Also excision of
lesion can limit the scar that may occur after spontaneous regression.
Keratocanthoma can recur.
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
5
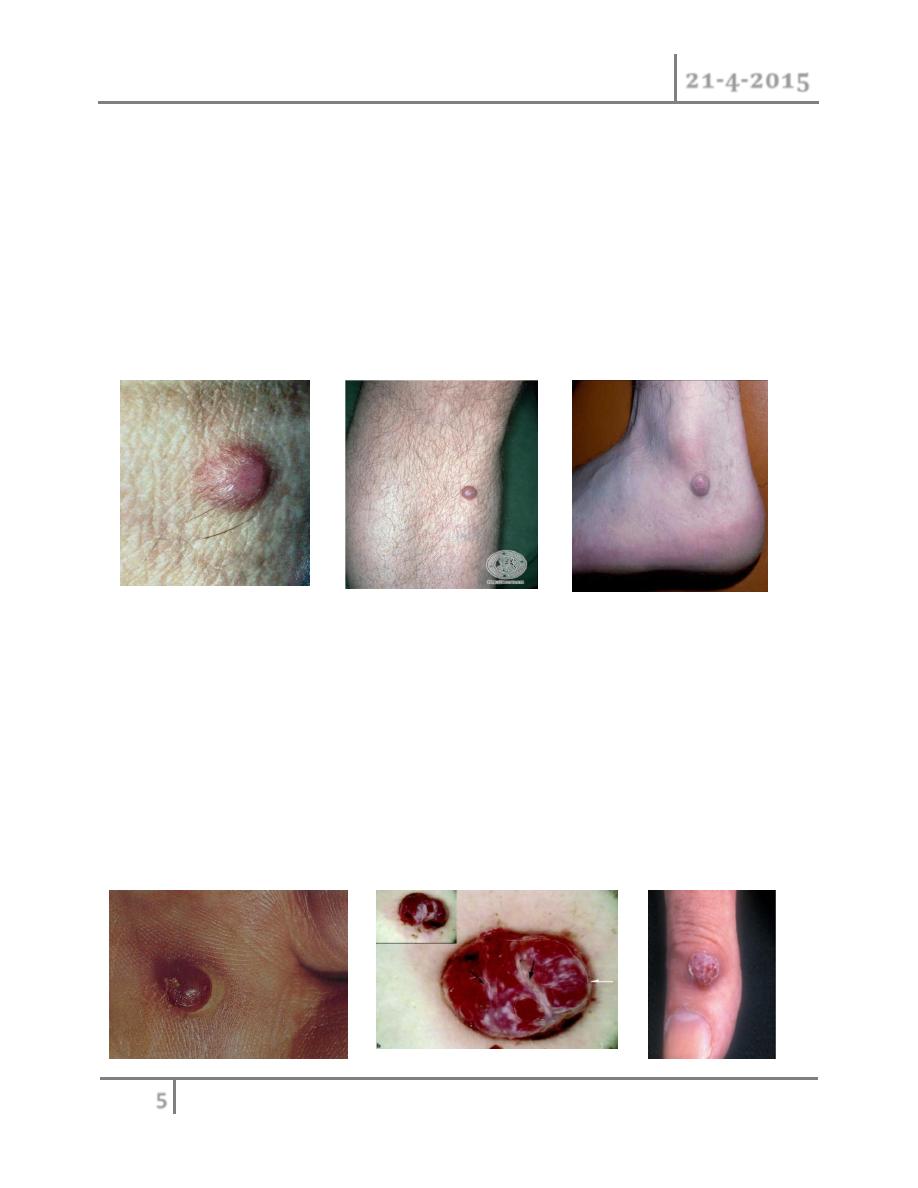
Dermatofibroma:
Is a firm skin-coloured or reddish brown sessile papule or nodule that arise
spontaneously or after an insect bite, it believed to be arise as reaction to
previous injury such insect biet. Can be found anywhere on extremiities and
trunk , but they are most likely to occur on anterior surface of lower legs. It
benign , asymptomatic lesion occur frequently in woman, sometime it may
cause little discomfort or itching.
Treatment: curettage or excision
Pyogenic granuloma:
Small capillary loops develop in healing wound to knit it together. when the
capillary loops grow too vigorously; they form protruding mass of tissues
called pyogenic granuloma.
It appears as soft, compressible ,red nodule that covered by fragile
epidermis, commonly occur on face or extremities, sometime patient give
history of previous trauma. it tends to bleed easily.
Treatment : cautery, curettage, or excision.

SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
6
Neurofibromatosis :
Neurofibroma are flesh-coloured papules or nodule with soft consistency
,the size varies considerably.
The tumours are benign and contained mixture of neural (ectodermal) and
fibrous (mesoermal) tissues.
Neurofibroma may occur as solitary lesions or as Multiple
neurofibromatosis (Von-Reckling-Housen disease) which is an autosomal
dominant condition in which multiple neurofibromata at birth that increase
in number, with café-au-lait which is patches of light-brown discolorization
of the skin
Lipoma :
Lipomas its the most common tumor in man. Lipoma it a dermal or
subcutaneous collection of benign adipose tissue. Most lesion are solitary ,
discrete nodule that remain asymptomatic and occur commonly in trunk and
extremities. Often the lesions may have a fibrous capsule that can
surrounded the collection of adipose cells.
Dercum syndrome : is a rare condition characterized by multiple, painful
lipomas. These lipomas mainly occur on the trunk, the upper arms and
upper legs.
Treatment : usually removed for cosmetic reasons or on occasion pain, as a
result of a neural or vascular component (angiolipoma) or when they
compress an adjacent nerve.
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
7
Large lipomas (>10cm) as well as deep-seated one Should arouse the
suspicion of malignant change. The most frequent malignant counterpart is
the liposarcoma.
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
8
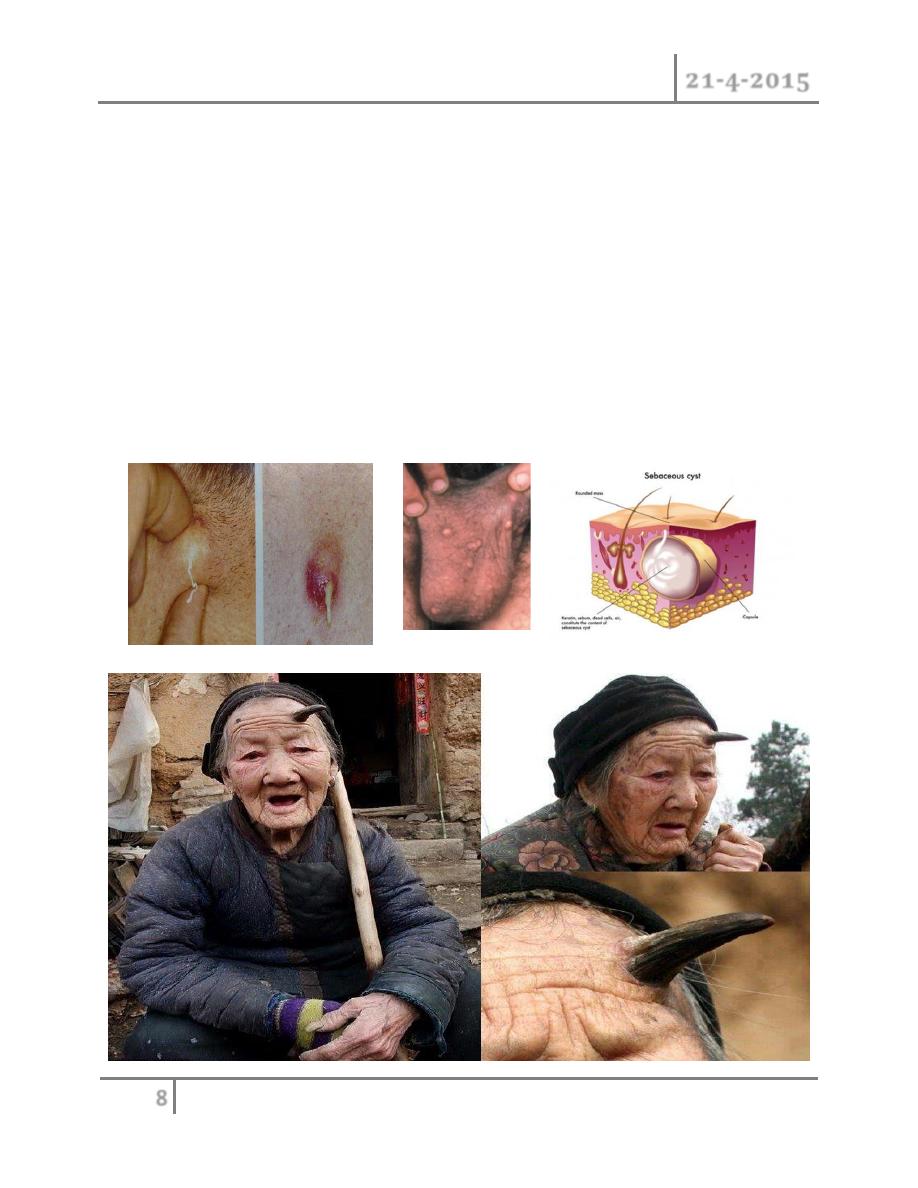
Sebaceous cyst (epidermal cyst) :
Are the most common form of cysts, they can occur at any age and any body
location except in the palm and soles. Most commonly , they occur in areas
of increase pilosebaceous activity on the head and upper trunk. The lesion
occur when The duct of sebaceous gland become blocked, it distended with
its own secretion and ultimately become sebaceous cyst. It is firm swelling,
adherent to skin and has punctum. It may get infection and ulceration.
Complications : infection, ulceration, calcification, keratin horn and
malignant change which is very rare
Treatment : if infected treated by drainage the abscess and later on surgical
excision
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
9
Haemangioma and vascular malformation :
Anomalies affecting blood vessels and lymphatic.
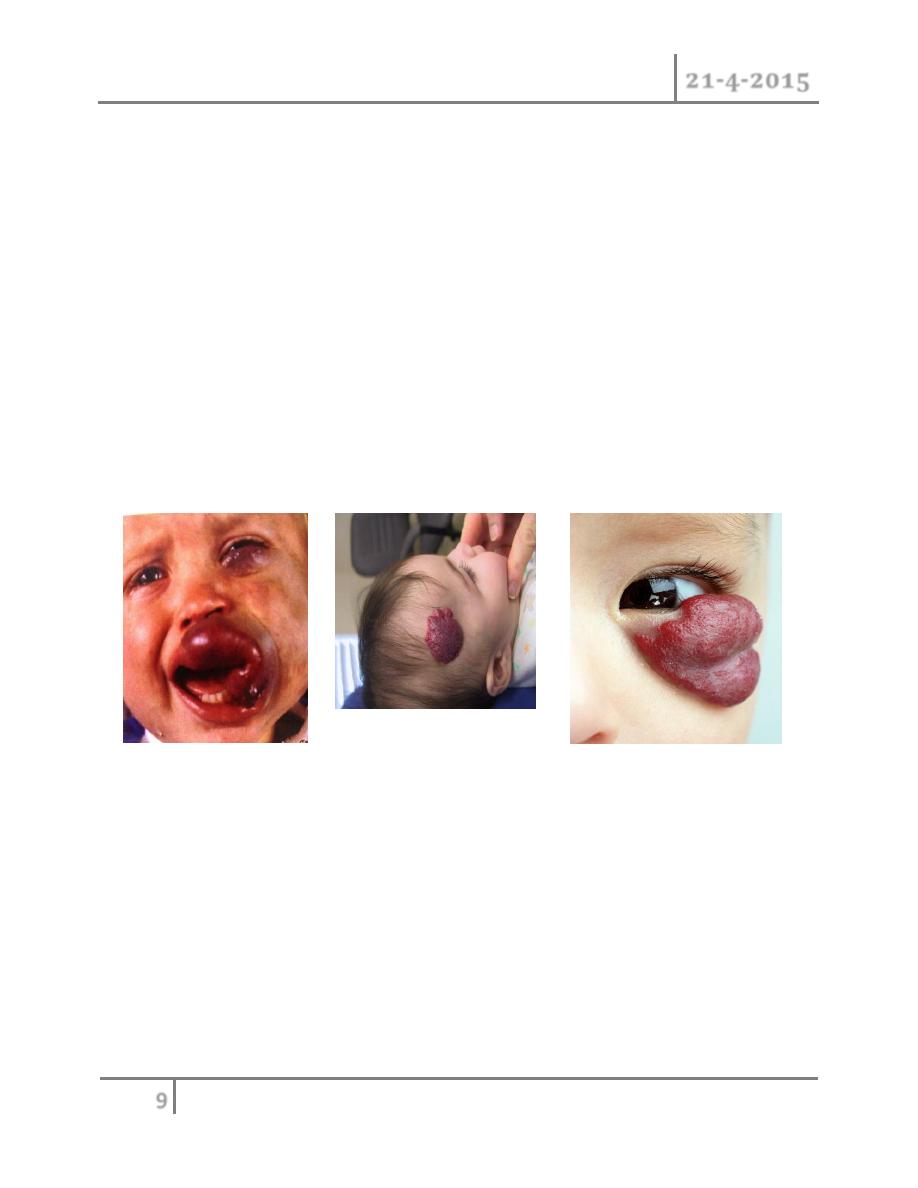
Haemangioma :
Benign proliferative neoplasm of endothelial cells of unknown aetiology,
present in first few weeks at birth and rapidly increase in size during first
year of life and regress in size with age. about 70% regress by age of 7
years old. Hemangiomas are the most common tumor seen in the pediatric
age group. These lesions have a predilection for the head and neck region,
the female sex (3-5:1, F:M ratio) and premature infants.
Twenty percent of these lesions may be multiple.
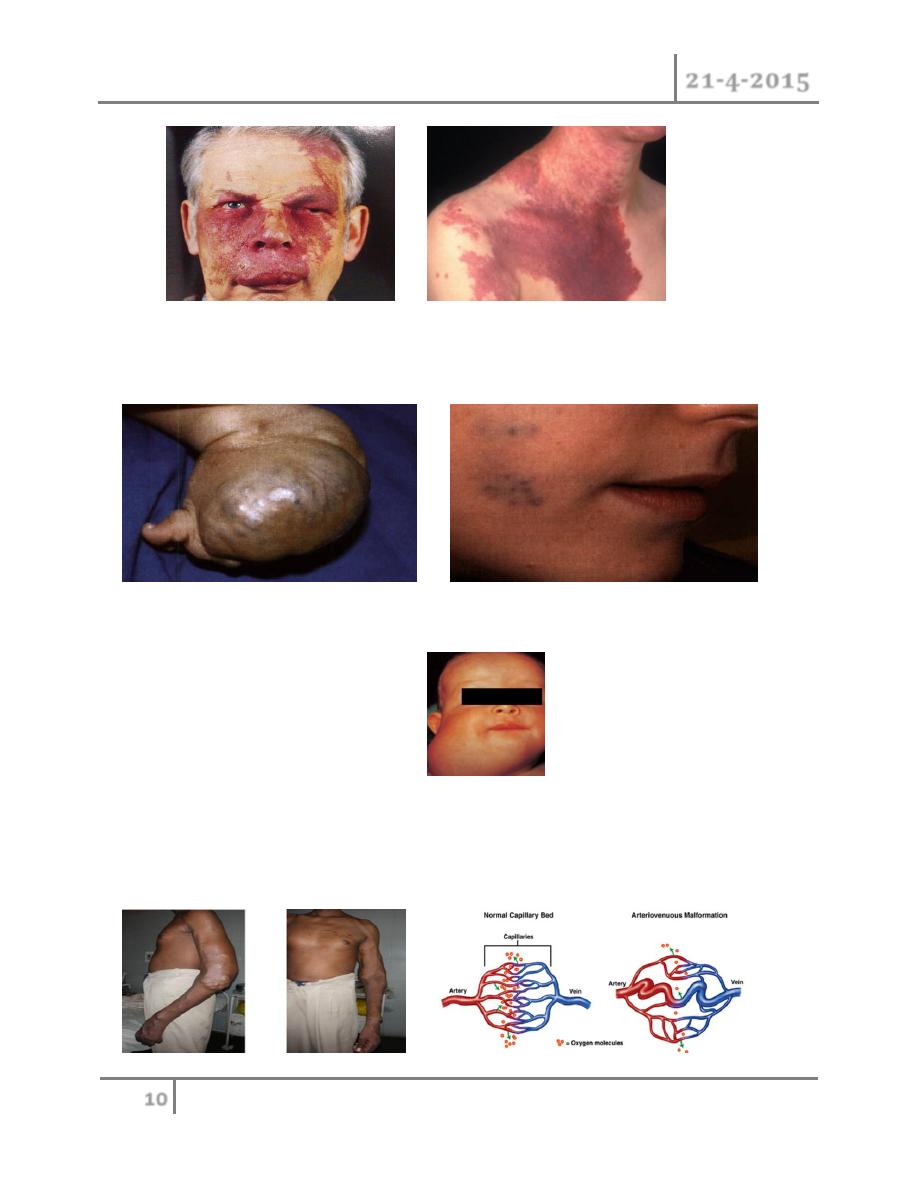
Vascular malformation :
Errors of development comprising dysplastic dilated vessels lined by
quiescent epithelium. usully present at birth and progresses proportionate
with growth and show no spontaneous regression. the lesionsa are
classified according to the type of vessels involved and as slow-flow
(capillary, lymphatic, venous, or mixed) or fast-flow (arteriovenous) lesions
Capillary malformation (port-wine stain): lesion may be present on anybody part.
In face distribution typically fallow the trigeminal nerve distribution. CM in this
location may be associated with Sturge-Webers syndrome where patient have
epilepsy , glucoma, mental retardation.
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
10
Cavernous malformation: bluish discolorization of skin. Compressible spongy
with slow refill, lead to engorgement by dependant position.
Lymphatic malformation: classified to micro and macrocystic.head, neck and
axilla affected in majority of cases.
Arterio-venous malformation: abnormal connection between arteries and vein
without intervening capillary bed, presented with thrill, increase body
temperature, pulsation and bruit. it may developed growth disturbances or
skeletal distortion.
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
11
Complications :
1- Obstruction: e.g. airway, visual axises.
2- Distortion: e.g. lip, nasal tip, eyelid.
3- Destruction: by erosion skin and cartilage.
4- Ulceration.
5- Bleeding.
6- Altered physiology: when present in large number can cause heart
failure,hepatomegaly and anemia.
7- Loacalized hypertrophy.
8- Associated syndrome e.g. sturge-weber syndrome in which port wine stain
in trigeminal distribution with convulsion and visual impairment.
Treatment : fallow up, oral steroid, intralesional steroid, laser therapy, alpha
interferon, sclerotherapy, surgery.
Premalignant skin conditions :
Disease that can turn to malignant tumours.
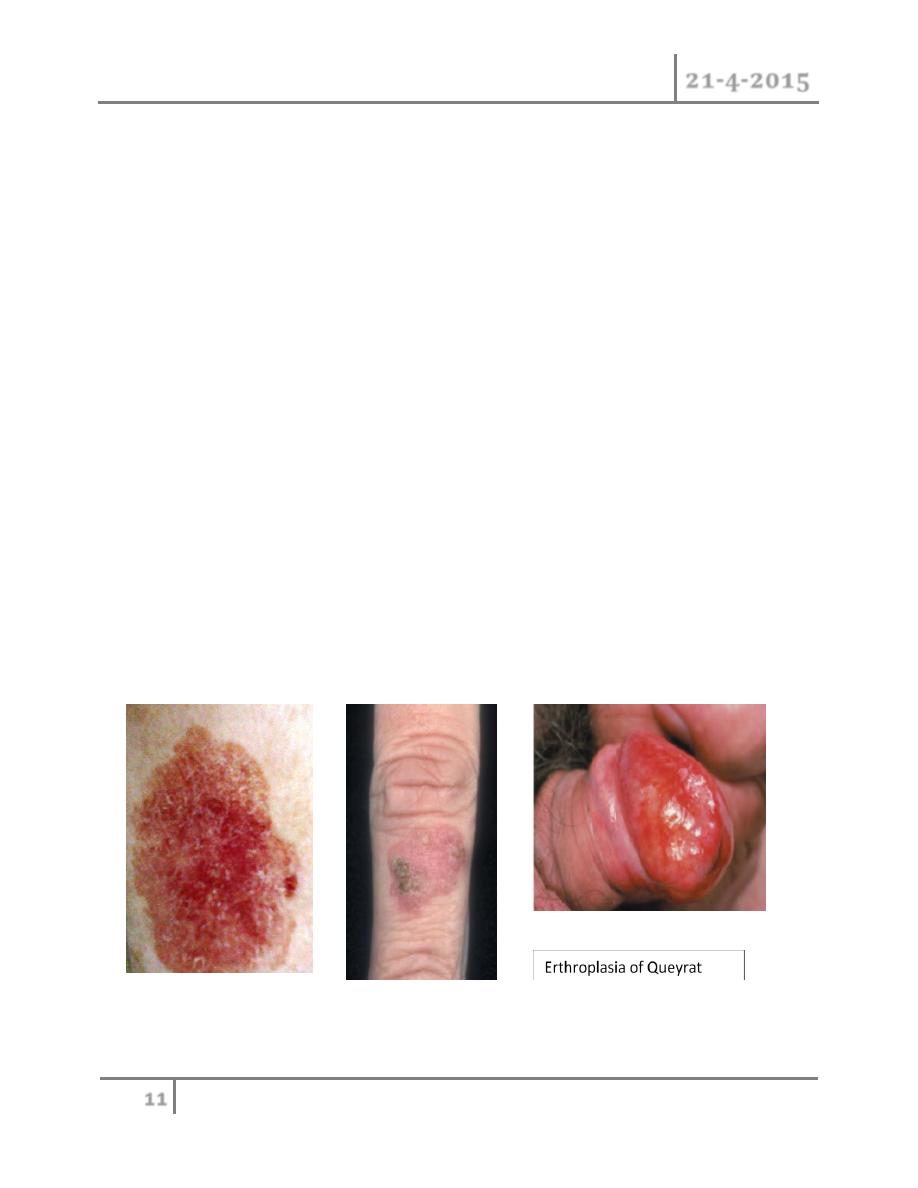
1- Bowen disease
- It consider squamous cell carcinoma in situ present as slowly grow well
define pink scaly plaque.
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
12
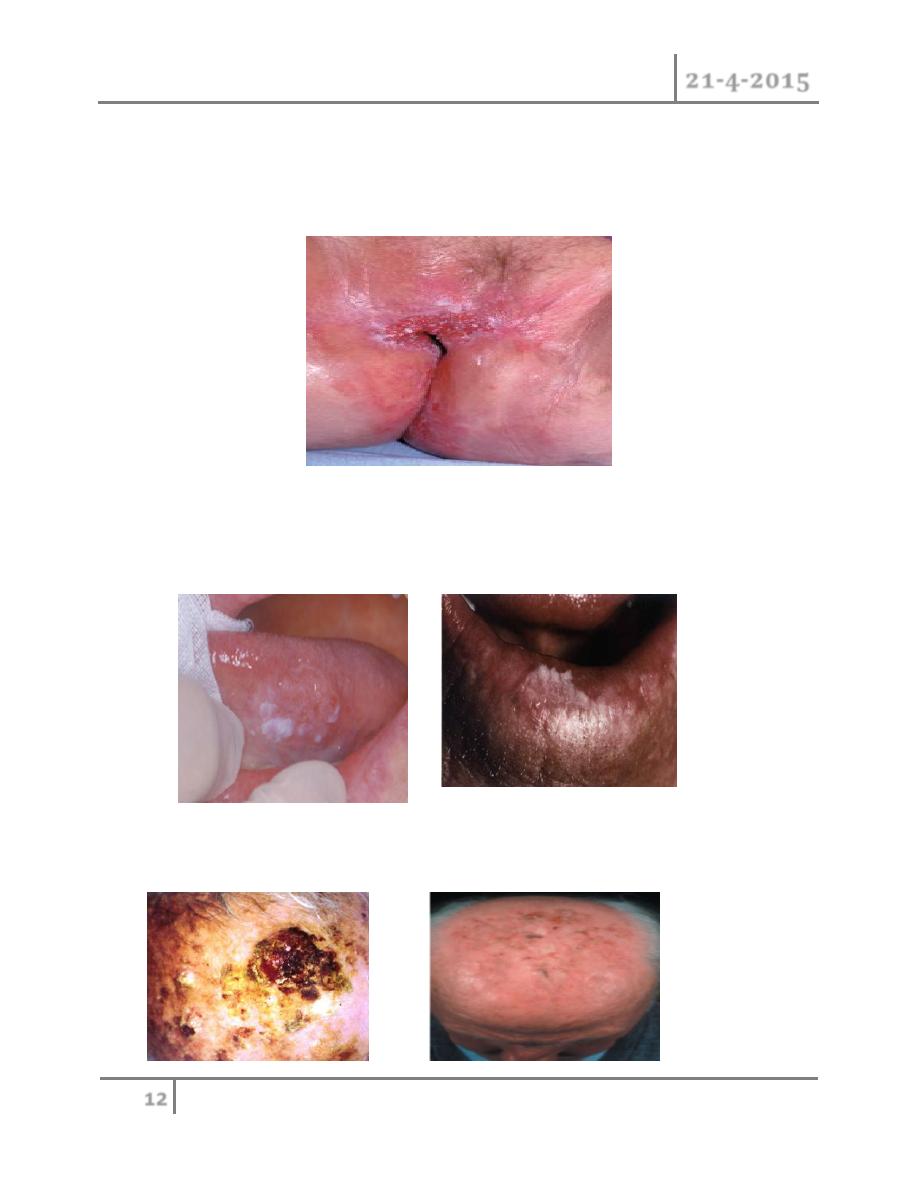
2- Extramammry Paget disease :
- This is form of intra-epidermal adenocarcinoma usually occur in genital
area or any area rich of apocrine glands e.g. axilla. early skin change
are subtle and mimic eczematous or intertrigo .
3- Leukoplakia :
- Thickened whit patches of mucosa, occur anywhere in mouth. other site
larynx ,the anus and the vulva.the affected area may show cracks or
fissures.
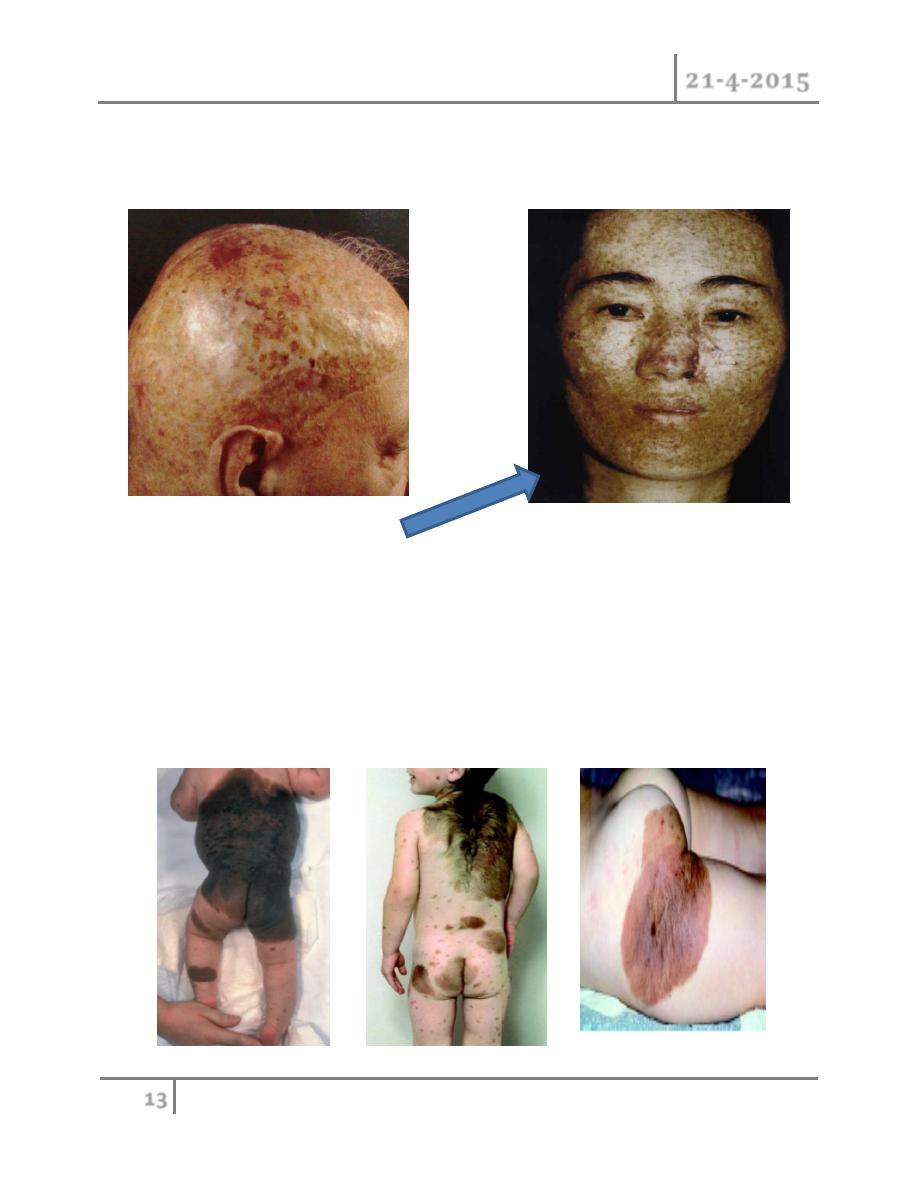
4- Solar keratosis :
- Small hard brown scaly tumour on sun-exposed area of the elderly.
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
13
5- Radiodermatitis :
- The skin thin out and appear darker because of hyperpigmentation with
poor wound healing.
6- Xeroderma pigmentosum :
- Autosomal recessive, caused by abnormality of (patch) gene of
chromosome 9q,result in aberrant nucleotide repair during DNA
maintenance. manifested by erythema,pigmentation and photophobia.
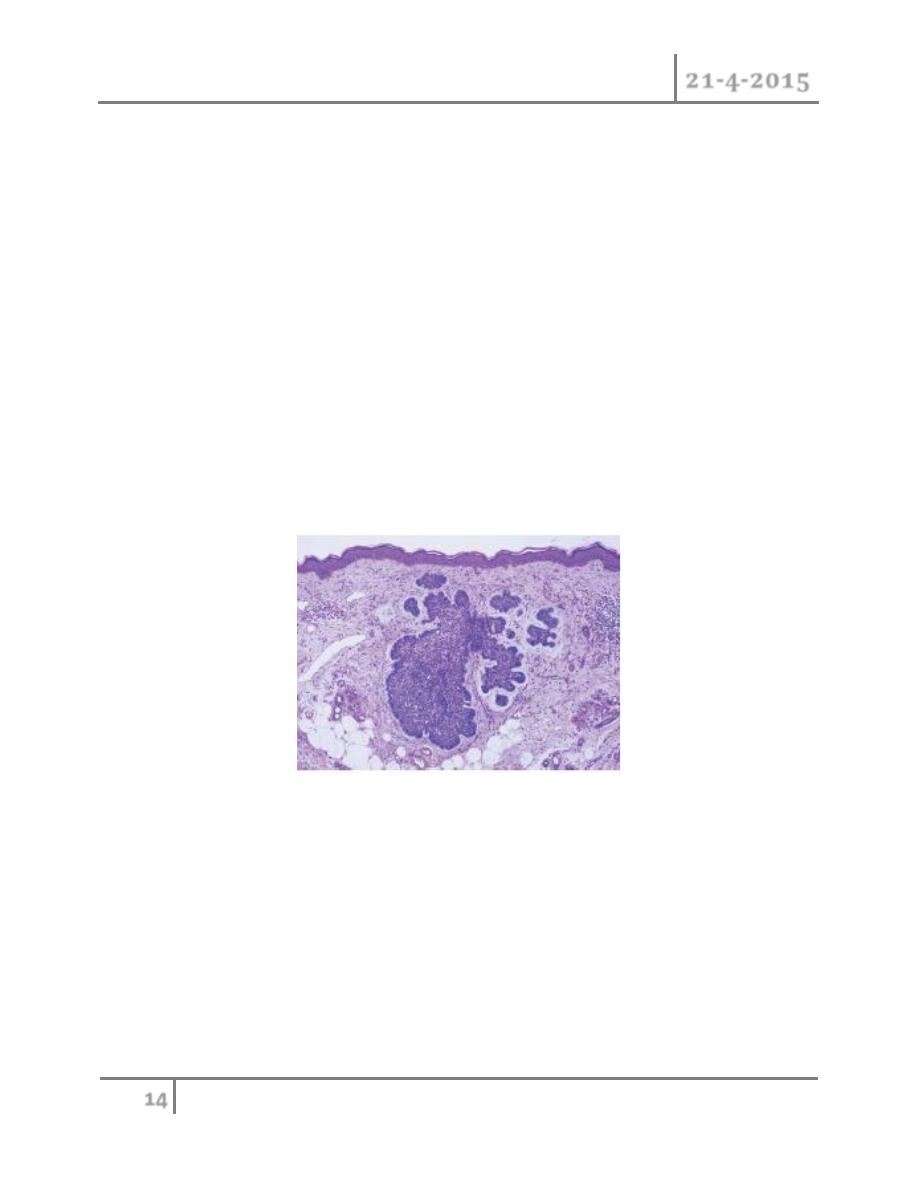
7- Giant hairy naevus :
- It has similar histology to compound Naevi,but the naevus cells are
distributed variably from the epidermis throughout all layers and into the
subdermal fat and muscle.
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
14
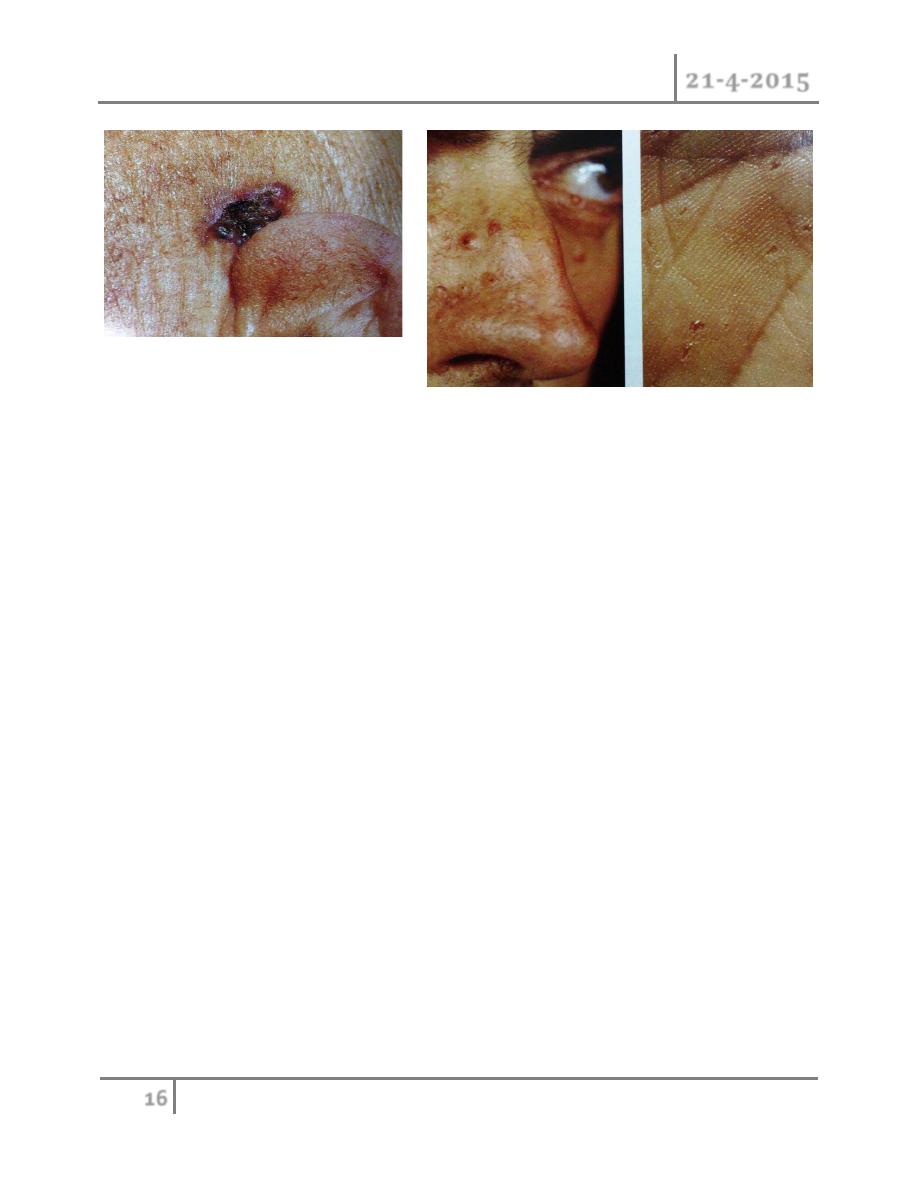
Basal cell carcinoma :
It is the most common malignancy of whites. It arise from
A-basal layer epithelial cells.
B-external root sheath of hair follicle.
It is slowly growing tumor, it doesn’t metastasize but can infiltrate the adjacent
tisssues.commonly found in face above line drawn from angle of mouth to lobe of
ear. It could occur anywhere, but particularly in the skin of scalp, face, arm and
hands i.e sun exposed area.
Microscopic appearance :
Characteristic finding is of ovoid cells in nest with a single outer (palisading)
layer.
Risk factors :
1- Sun exposure.
2- Adancing age.
3- Faint complexion.
4- Long term exposure to psoralene and UVA therapy (for psoriasis).
5- Arsenic exposure.
6- Immunedefeciency.
7- Radiation
8- Viral infection e.g. HPv 16,HIV.

SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
15
Type of basal cell carcinoma :
1- Nodular ulcerative type.
2- Superfscail spreading.
3- Sclerosing type.
4- Pigmented type.
5- Basal cell naevoid syndrome (Gorlin syndrome).
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
16
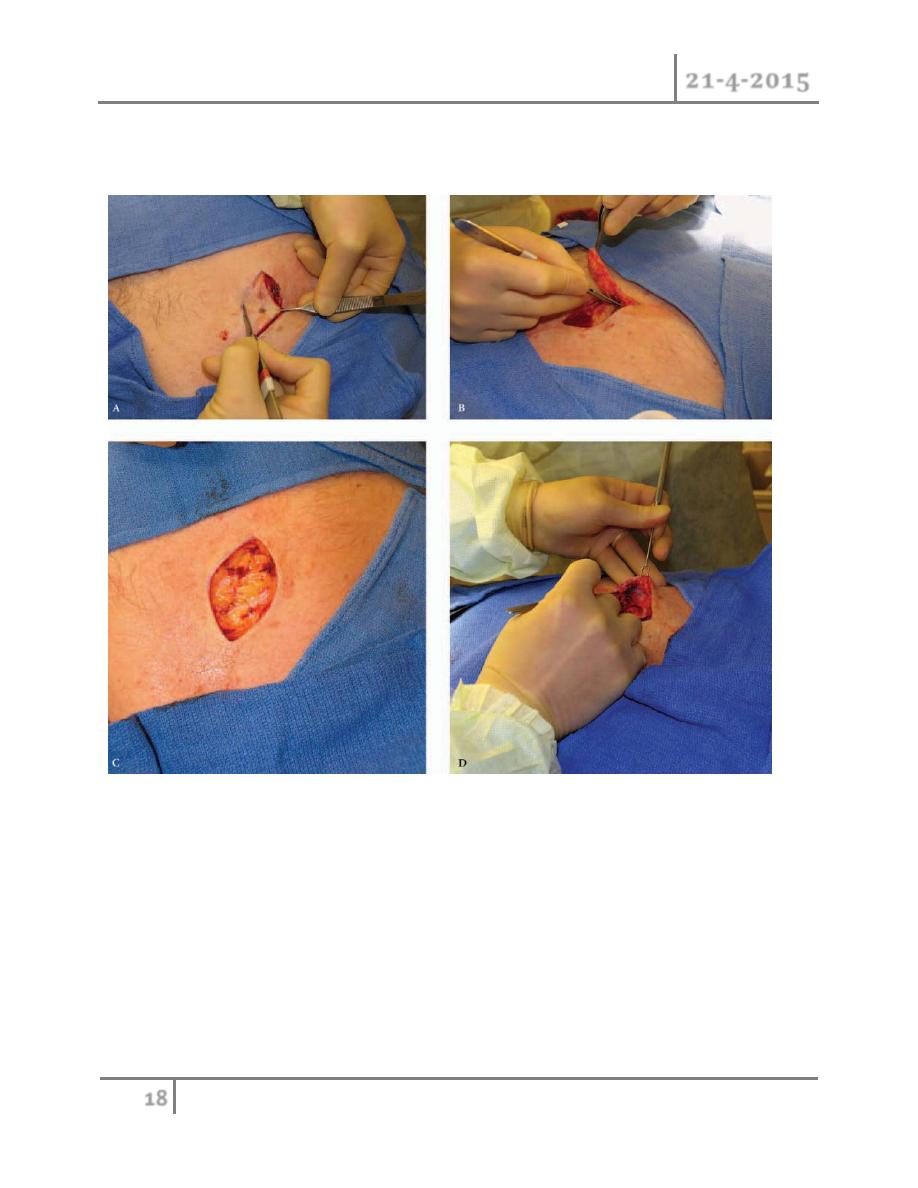
Treatment of basal cell carcinoma :
Curettage and desiccation.
Surgical excision with safty margin (0.5 cm).
Cryotherapy.
Radiation therapy.
Mohs fresh frozen section.
Dermobrasion and chemical peel.
Interferon alpha.
Co2 LASER.
Local chemotherapy e.g 5-fluorouracil
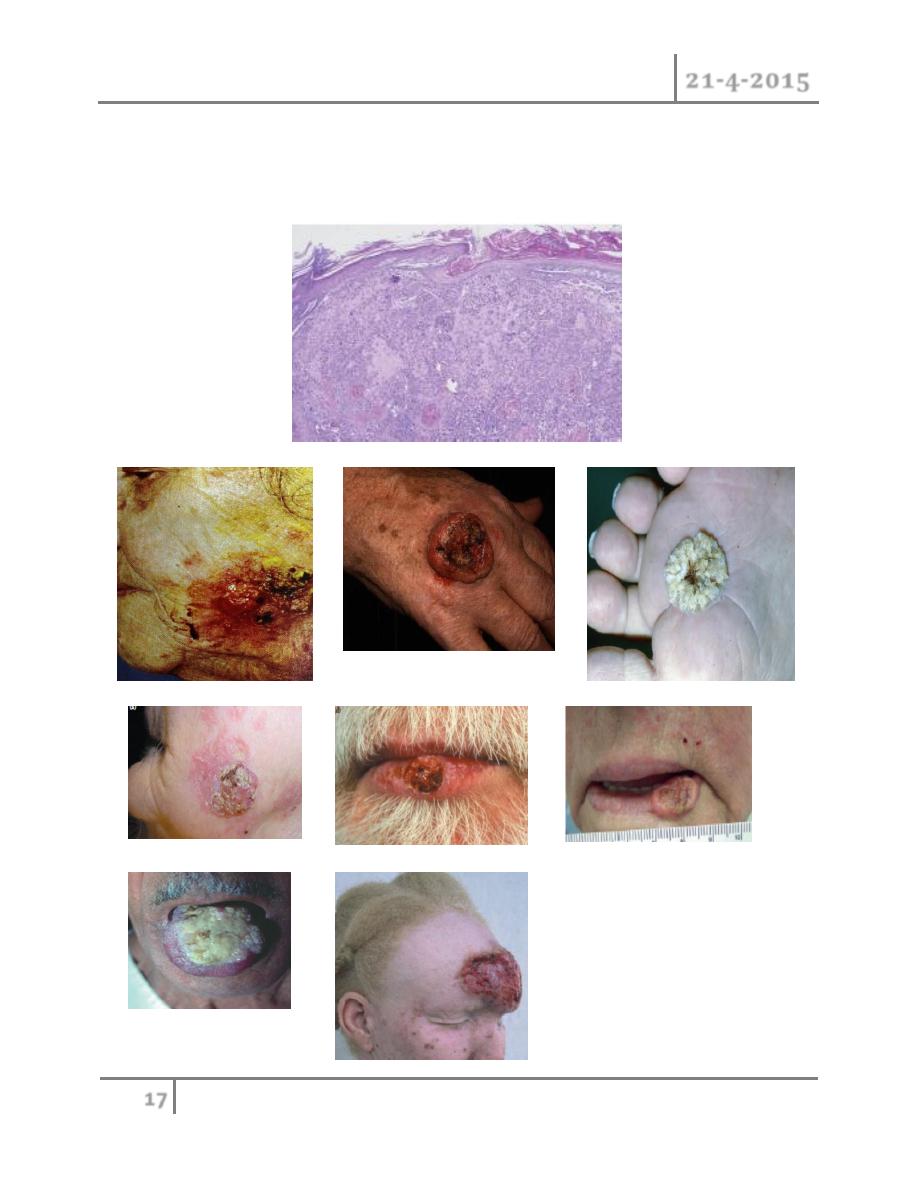
Sequamous cell carcinoma :
It originates from the keratinising cells of epidermis or its appendages. it
also arise from stratum basale of epidermis but, unlike BCC,it expresses
cytokeratins I and 10.
Types of sequmaous cell carcinoma:
A-verrucous SCC: slow growing,exophytic,and less likely to metastasize.
B-ulcerative SCC:grow rapidly and is locally invasive.
Microscopic appearances :
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
17
Charactrestic irregular masses of squamous epithelium are noted to proliferate
and invade the dermis from the germinal layer.this tumor is stains positive for
cytokeratin 1 and 10.
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
18
Treatment : as for basal cell carcinoma but with exception is safe margin are
more than that of basal cell carcinoma (1-2 cm).
Malignant melanoma :
It is neoplasm of melanocyte which is neural crest derived cells that have
differentiated toward melaoncytes.it occur in skin but can occur anywhere in body
where the melanocyet are exist, such as bowel mucosa, retina…etc.
Pathology :
Two phase described :
• Radial growth phase with proliferation of neoplastic melanocyteds within
epidermis.

SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
19
• Vertical growth phase where the neoplastic melanocytes extend into the
papillary and reticular dermis.
Microscopic appearances :
Atypical melanocyte invades from the dermis-epidermis junction down into the
dermis.
Spread :
as well as growth and ulceration, malignant melanoma seed by lymphatic
permeation also by blood stream to any organ in body. free melanin in blood may
produced generalized skin pigmentation and melanuria in late stage.
Epidemiology :
cutaneous melanoma is caused largely by exposure to UVR.it account for less than
5% of skin malignancy but it responsible for over 75% of death related to skin
malignancy. it account for 3% of all malignancy. commonest cancer in young
adults(20-39 years). Auckland ,newzeland report the highest incidence
Clinical features :
appeared as change in pre-existing naevus or as new lesion.
Assess lesion for ABCDE :
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
20
Asymmetry
Border irregularity
Colour change
Diameter more than 6mm
Extra features (itch,bleeding…. ).
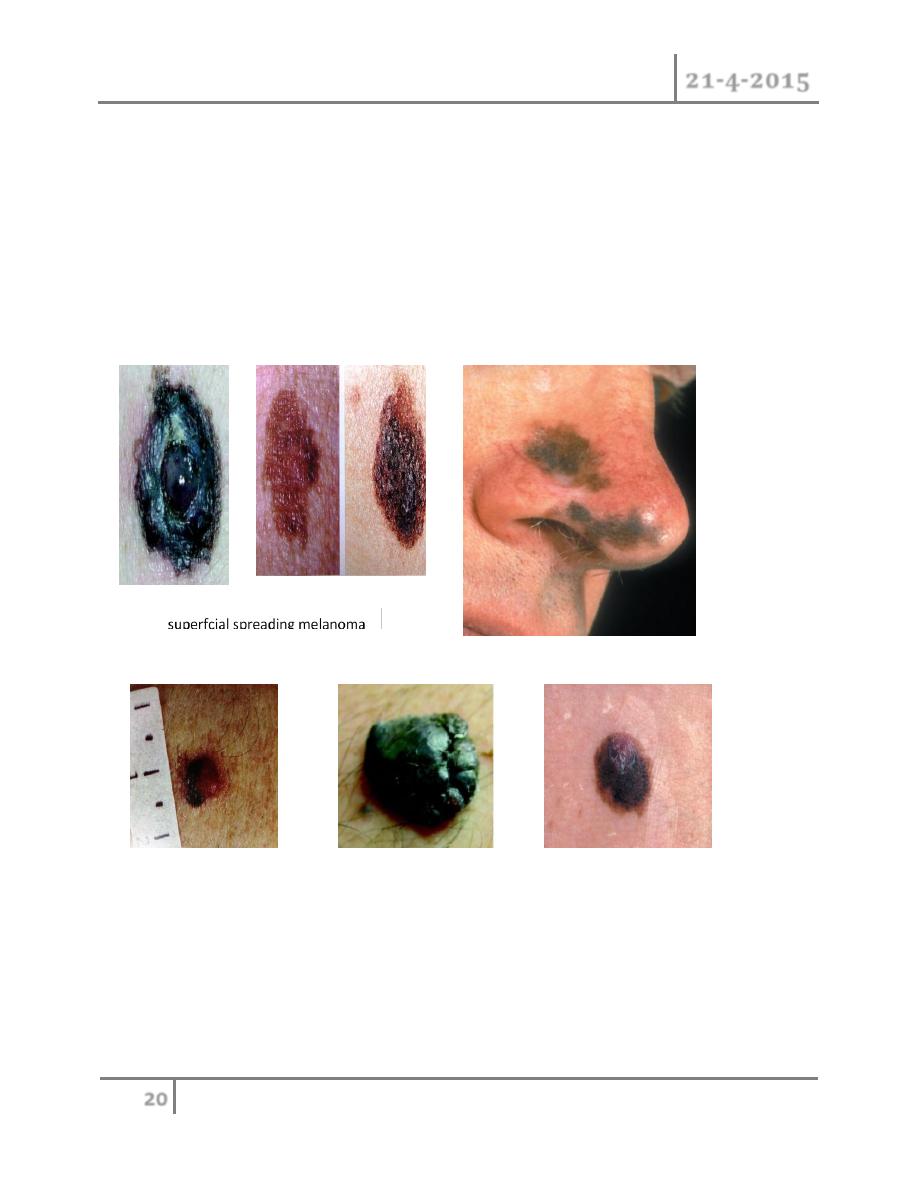
Types of melanoma :
Nodular melanoma
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
21
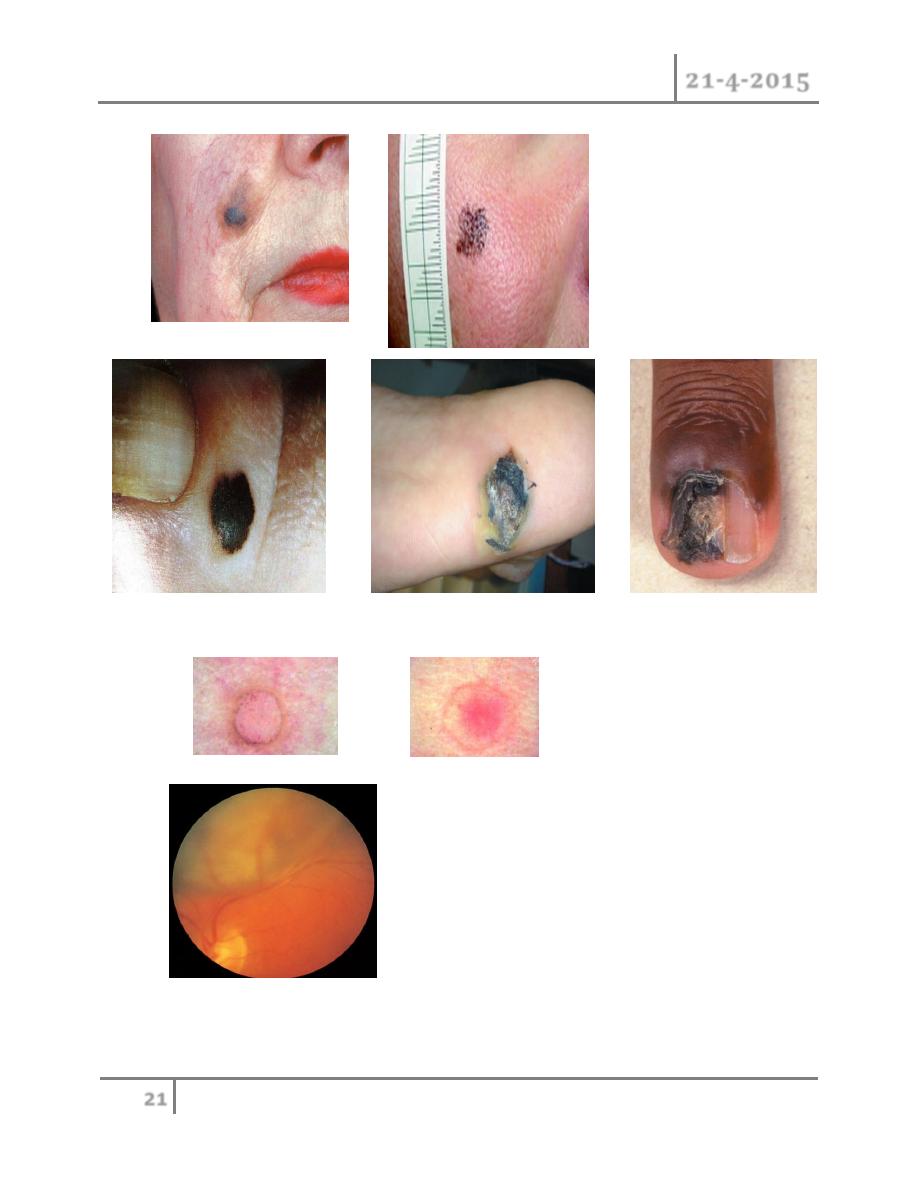
Lentigo maligna melanoma
Acral lentiginous melanoma
amelonotic melanoma
Choroid melanoma
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
22
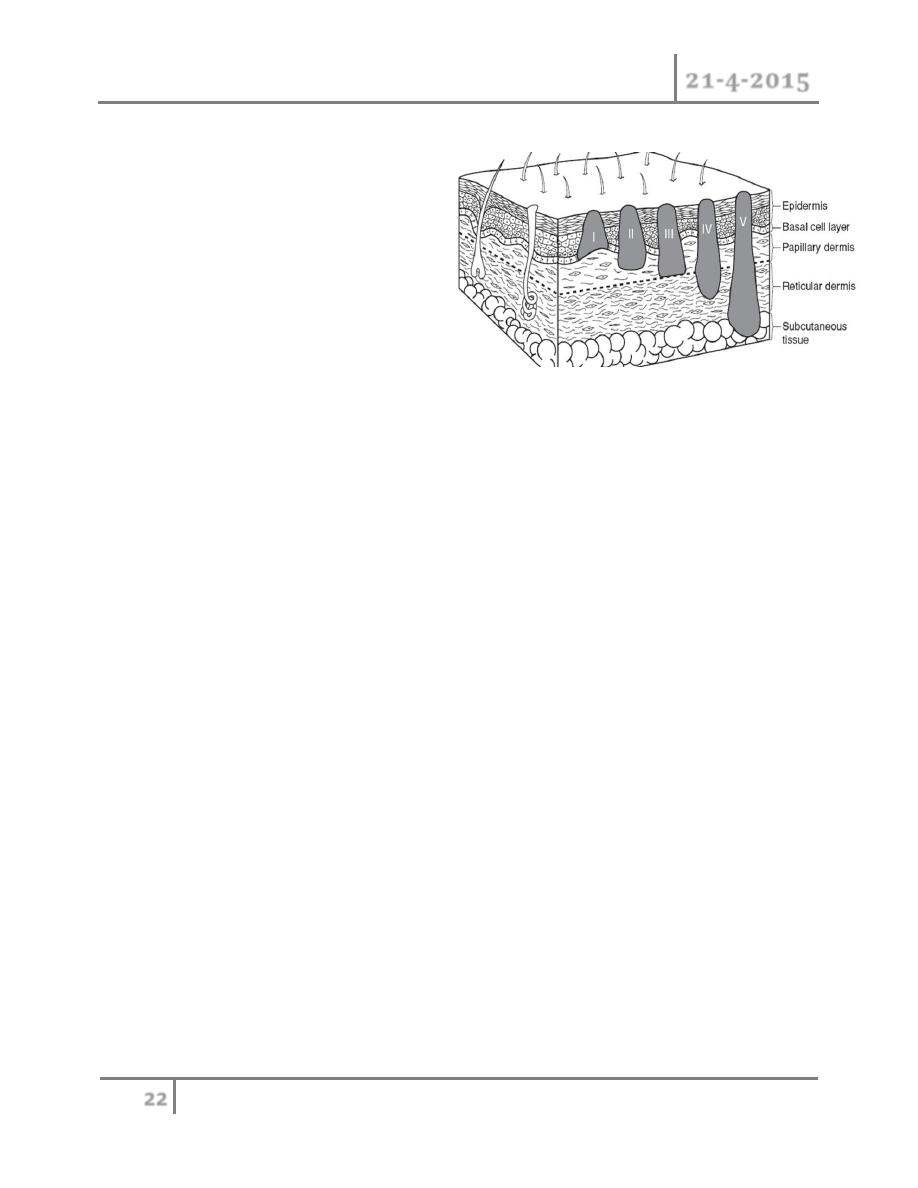
Melanoma thickness grading :
Clark level :
1- In situ
2- Papillary dermis
3- Papillary reticular dermis
4- Reticular dermis
5- Sucutaneous
Breslow depth (mm) :
1- <1.00
2- 1.01-2.00
3- 2.01-4.00
4- >4.00
5- More depth in mm means more aggressive tumours
Treatment of malignant melanoma :
Surgical excision of primary tumour is the mainstay of treatment.
In situ 0.5 cm safety margin
< 1 mm 1 cm
1 to 4 mm 2 cm
> 4 mm 2-3 cm
With lymph node dissection (in case of lymph nodes metastasis).
For advanced melanoma number of therapeutic modalities which included:
systemic chemotherapy, immunotherapy, isolated limb perfusion, and
radiotherapy.

SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
23
Prognosis :
1- Breslow depth.
2- Type of lesion: superficial type better prognosis.
3- The anatomical site: tumor on the trunk and scalp have poor prognosis.
4- Lymph node metastasis.
5- Sex: good prognosis in female than male
Prevention :
1- Avoid sun exposure by using physical and chemical barrier
2- Prophylactic removal of suspicious naevus
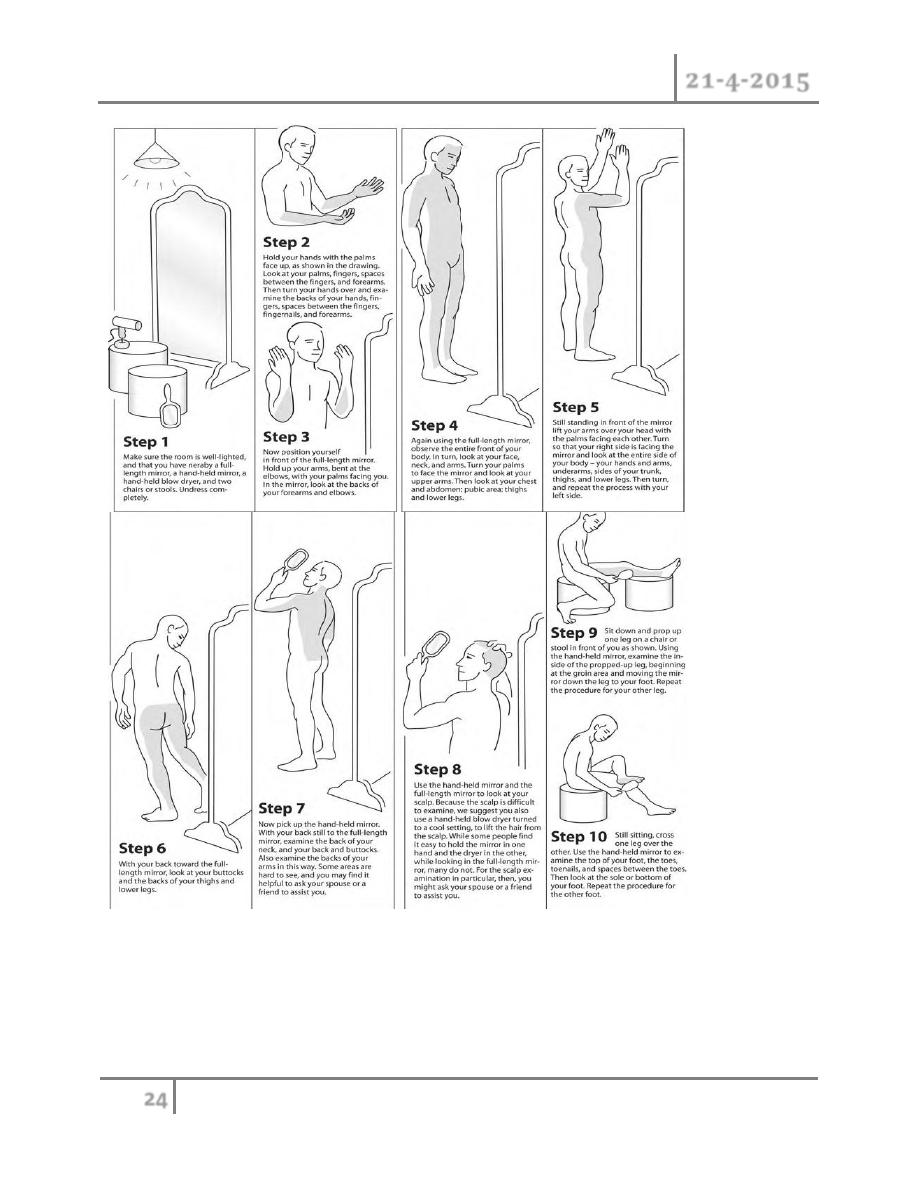
3- Periodic self examination in front of mirror
#END
Done by
Ali Kareem
SKIN TUMOUR Dr. Ahmed Khalaf
21-4-2015
24