5102
-
5102
Published by : Ali Kareem
مكتب اشور لالستنساخ
Dr. Bassim Rassam
Lec. 2
LYMPHATIC SYSTEM
Tues. 25 / 11 / 2014
The Lymphatic System Dr. Bassim Rassam
25-11-2014
2
The Lymphatic System and Lymph Nodes
Functions :
1. Removes water, electrolytes, low-molecular-weight moieties (polypeptides,
cytokines, growth factors) & macromolecules (fibrinogen, albumin,
globulins, coagulation and fibrinolytic factors) from the interstitial fluid
(ISF) and returns them to the circulation.
2. Permits the circulation of lymphocytes and other immune cells.
3. Intestinal lymph (chyle) transports cholesterol, long-chain fatty acids,
triglycerides and the fat-soluble vitamins (A, D, E and K) directly to the
circulation, bypassing the liver.
Mechanisms of lymph transport :
Resting 1SF is negative (—2 to —6 mmH2O), whereas lymphatic pressures
are positive, indicating that lymph flows against a small pressure gradient. It
is believed that prograde lymphatic flow depends upon three mechanisms :
1- Transient increases in interstitial pressure secondary to muscular
contraction and external compression.
2- The sequential contraction and relaxation of lymphangions. (Valves
partition the lymphatics into segments).
3- The prevention of reflux due to valves.
Lymphangions are believed to respond to increased lymph flow in
much the same way as the heart responds to increased venous return in
that they increase their contractility and stroke volume. Contractility is
also enhanced by noradrenaline, serotonin, certain prostaglandins and
thromboxanes, and endothelin- 1.
Lymphatics may also modulate their own contractility through the
production of nitric oxide and other local mediators. Transport in the
thoracic & right lymphatic ducts is also depends upon intrathoracic
(respiration) & central venous (cardiac cycle) pressures. Therefore,
cardiorespiratory disease may have an adverse effect on lymphatic
function.
The Lymphatic System Dr. Bassim Rassam
25-11-2014
3
In summary, in the healthy limb, lymph flow is largely due to intrinsic
lymphatic contractility, although this is augmented by exercise, limb
movement and external compression. However, in lymphoedema, when
the lymphatics are constantly distended with lymph, these external forces
assume a much more important functional role.
Acute Lymphangitis
It is infection spreading from a skin (wound, abrasion, laceration) through the
draining superficial lymphatic vessels to the draining lymph nodes. It is usually
seen in the extremities (upper and lower limbs).
Causative Microorganisms :
1. Group A B-haemolytic streptococci (streptococcus pyogenes),
2. Staphylococcus aureus.
Clinical Presentation :
1- Red blushes or streaks in the skin (correspond to inflamed lymphatics)
extending from the source of infection to the regional LNs.
2- Regional LNs are enlarged and tender and may suppurate with abscess
formation, occasionally the infection bypasses one group to affect another
at a higher level (e.g, if the point of infection is the foot, an abscess may
form in the external iliac group of LNs rather than the superficial (lower)
and deep inguinal groups and because the point of infection may have
healed and been forgotten, by the time the mass appears it may be mistaken
for an (appendix abscess).
Treatment :
1- Bed rest (to reduce lymphatic drainage) with elevation of the affected limb
(to reduce swelling).
2- Antibiotics. Failure to improve within 48 hours suggest inappropriate
antibiotic therapy, or the presence of undrained pus, or the presence of
an underlying systemic disorder (malignancy, immunodeficiency).
3- Drainage of an abscess if it has formed.
The Lymphatic System Dr. Bassim Rassam
25-11-2014
4
Complications :
1- Post lymphatic oedema due to permanent lymphatic obstruction after
resolution of acute lymphangitis leadind to persistent oedema. These
patients are prone to so-called acute inflammatory episodes (AlEs).
2- Chronic lymphangitis. Follows repeated attacks of acute lymphangitis.
3- Bacteraemia or Septicaemia.
LYMPHOEDEMA
It is abnormal limb swelling due to the accumulation of increased amounts of
high protein ISF secondary to defective lymphatic drainage in the presence of
(near) normal net capillary filtration. So it is accumulation of fluid in the
interstitial spaces (extracellular fluid compartment), in the limbs it accumulates
mainly in the subcutaneous tissues.
Clinical Presentation :
1. Gradually increasing circumference of the affected limb (huge enlargement)
with multifolding of the skin.
2. In the early stages the lymphoedema is pitting on pressure thus it
simulates ordinary oedema, but with time lymphoedema characteristically
becomes Non-pitting lymphoedema due to subcutaneous thickening with
fibrous tissue being worsened by recurring low grade lymphangitis and
cellulitis. (Recurrent acute infective episodes). In the early stages,
lymphoedema will ‘pit’ and the patient will report that the swelling is down
in the morning. This represents a reversible component to the swelling, which
can be controlled. Failure to do so allows fibrosis, dermal thickening and
hyperkeratosis to occur.
3. Unlike other types of oedema, Iymphoedema characteristically involves the
foot. The contour of the ankle is lost through infilling of the submalleolar
depressions, a ‘buffalo hump’ forms on the dorsum of the foot, the toes appear
‘square’ due to confinement of footwear, and the skin on the dorsum of
the toes cannot be pinched due to subcutaneous fibrosis (Stemmer’s
sign) Lymphoedema usually spreads proximally to knee level and less
commonly affects the whole leg.
The Lymphatic System Dr. Bassim Rassam
25-11-2014
5
4. Lymphangiomas are dilated dermal lymphatics that ‘blister’ onto the
skin surface. The fluid is usually clear but may be bloodstained and, in the
long term, they thrombose and fibrose, forming hard nodules and raising
concerns about malignancy. If lymphangiomas are < 5 cm across,
they are termed lymphangioma circumscriptum, and if they are more
widespread, they are termed lymphangioma diffusum. If they form a
reticulate pattern of ridges then it has been termed lymphoedema ab igne.
Lymphangiomas frequently weep (lymphorrhoea, chylorrhoea), causing skin
maceration and they act as a portal for infection.
5. Lymphangiosarcoma was originally described in post-mastectomy oedema
(Stewart—Treves syndrome) and affects around 0.5% of patients at a mean
onset of 10 years. However, lymphangiosarcoma can develop in any
longstanding lymphoedema, but usually takes longer to manifest (20
years). It presents as single or multiple bluish/red skin and subcutaneous
nodules that spread to form satellite lesions that may then become confluent.
6. Ulceration, non-healing bruises, and raised purple-red nodules should
lead to suspicion of malignancy.
7. Constant dull ache, even severe pain or Burning and bursting sensations or
pins and needles.
8. Sensitivity to heat.
9. General tiredness and debility.
10. Skin problems, including dehydration, flakiness, weeping, excoriation and
breakdown. Chronic eczema, fissuring, verrucae and papillae (warts) are
frequently seen in advanced disease. Ulceration is unusual, except in
the presence of chronic venous insufficiency.
11. Immobility, leading to obesity and muscle wasting.
12. Backache and joint problems.
13. Fungal infection of the skin (dermatophytosis) and nails (onychomycosis)
Athlete’s foot.
Pathophysiology :
The 1SF compartment (10-12 litres in a 70-kg man) constitutes 50% of the
The Lymphatic System Dr. Bassim Rassam
25-11-2014
6
wet weight of skin and subcutaneous tissues and, in order for oedema to
be clinically detectable, its volume has to double. About 8 litres (protein
concentration approximately 20-30g/L, similar to ISF) of lymph is produced
each day and travels in afferent lymphatics to lymph nodes. There, the volume is
halved and the protein concentration doubled, resulting in 4 litres of
lymph re-entering the venous circulation each day via efferent
lymphatics. In one sense, all oedema is lymphoedema in that it results from
an inability of the lymphatic system to clear the ISF compartment. However, in
most types of oedema this is because capillary filtration rate is pathologically
high and overwhelms a normal lymphatic system, resulting in the accumulation
of low-protein oedema fluid. In contrast, in true lymphoedema, when the primary
problem is in the lymphatics, capillary filtration is normal and the oedema fluid
is relatively high in protein. Of course, in a significant number of patients with
oedema there is both abnormal capillary filtration and abnormal lymphatic
drainage. Lymphoedema results from lymphatic 1-aplasia, 2- hypoplasia, 3-
dysmotility (reduced contractility with or without valvular insufficiency), 4-
obliteration by inflammatory, infective or neoplastic processes, or 5-surgical
extirpation. Whatever the primary abnormality, the resultant physical and/or
functional obstruction leads to lymphatic hypertension and distension, with
further secondary impairment of contractility and valvular competence.
Lymphostasis and lymphotension lead to the accumulation in the ISF of
fluid, proteins, growth factors and other active peptide moieties,
glycosaminoglycans and particulate matter, including bacteria. As a
consequence, there is increased collagen production by fibroblasts, an
accumulation of inflammatory cells (predominantly macrophages and
lymphocytes) and activation of keratinocytes. The end result is protein-rich
oedema fluid, increased deposition of ground substance, subdermal fibrosis and
dermal thickening and proliferation. Lymphoedema, unlike all other types of
oedema, is confined to the epifascial space. Although muscle compartments may
be hypertrophied owing to the increased work involved in limb movement, they
are characteristically free of oedema.
The Lymphatic System Dr. Bassim Rassam
25-11-2014
7
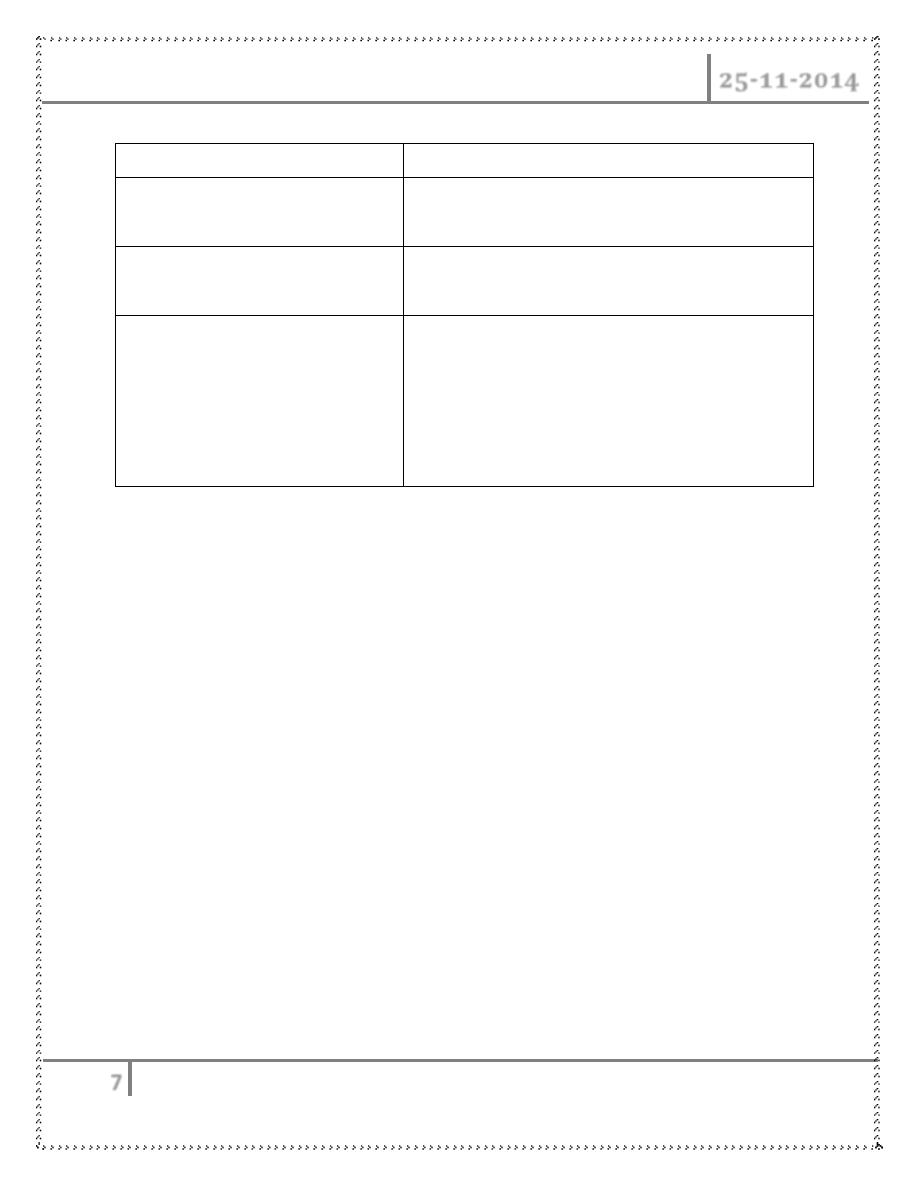
Ordinary Oedema
Lymphoedema
Pitting.
Nonpitting (due to excessive collagen
deposition).
Involves epifascial, subfascial
and
muscle compartments.
Is confined to the epifascial space only.
Capillary filtration rate is
pathologically high and
overwhelms a normal lymphatic
system, resulting in the
accumulation of low-protein
oedema fluid.
capillary filtration is normal but there is an
abnormal lymphatic drainage system and the
oedema fluid is relatively high in protein.
Classification
In general, primary lymphoedema progresses more slowly than secondary
lymphoedema. Two main types of lymphoedema are recognized :
1- Primary lymphoedema, in which the cause is unknown (or at least
uncertain and unproved), but often presumed to be due to (congenital
lymphatic dysplasia), Primary lymphoederna is usually further subdivided
on the basis the presence of family, age of onset and lymphangiographic
findings :
a- Congenital (onset < 2 years old).
Sporadic.
Familial (Milroy’s disease).
b- Praecox (onset 2 - 35 years old).
Sporadic.
Familial (Meige’s disease).
c- Tarda (onset after 35 years old).
2- Secondary lymphoedema, in which there is a clear underlying cause, such as
inflammation, malignancy or surgery.
1- Infection.
Parasitic infection (filariasis).
Fungal infection (tinea pedis).
The Lymphatic System Dr. Bassim Rassam
25-11-2014
8
2- Exposure to foreign body material (silica particles).
3- Malignancy.
Primary lymphatic malignancy.
Metastatic spread to lymph nodes.
4- Surgery. Excision of LNs.
5- Radiotherapy. to groups of lymph nodes.
6- Trauma. (particularly degloving injuries).
7- Venous complications.
Superficial thrombophlebitis.
Deep venous thrombosis.
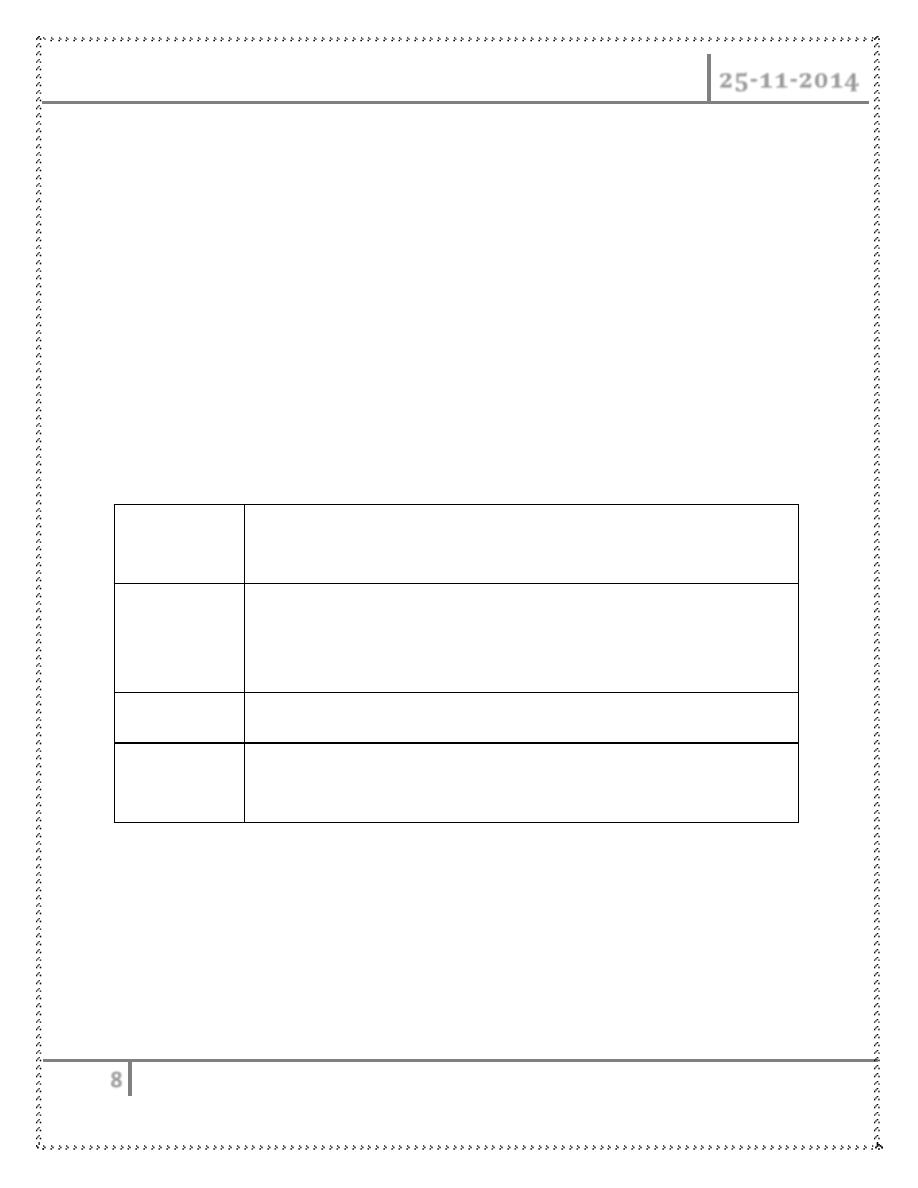
Clinical classification of lymphedema
Grade
(Brunner)
Clinical features
Subclinical
(latent)
I
Oedema pits on pressure and the swelling largely, or
completely disappears on elevation and bed rest.
II
Oedema does not pit and does not significantly reduce upon elevation.
Ill
Oedema is associated with irreversible skin changes, i.e. fibrosis,
papillae.
Differential diagnosis of the swollen limb
1) Non-vascular or lymphatic :
1- General disease states
Cardiac failure from any cause
Liver failure
Hypoproteinaemia due to nephrotic syndrome, malabsorption,
protein- losing enteropathy.
The Lymphatic System Dr. Bassim Rassam
25-11-2014
9
Hypothyroidism (myxoedema)
Allergic disorders, including angioedema and idiopathic cyclic
oedema.
Prolonged immobility and lower limb dependency.
2- Local disease processes. (Ruptured Baker’s cyst, Myositis ossificans,
Bony or soft-tissue tumours, Arthritis, Haemarthrosis, Calf muscle
haematoma, Achilles tendon rupture).
3- Retroperitoneal fibrosis.May lead to arterial,venous and lymphatic
abnormalities
4- Gigantism. (Rare, all tissues are uniformly enlarged)
5- Drugs. Corticosteroids (oestrogens, progestagens), Monoamine
oxidase inhibitors (phenylbutazone, methyldopa, hydralazine,
nifedipine)
6- Trauma. Painful swelling due to reflex sympathetic dystrophy
7- Obesity. (Lipodystrophy, Lipoidosis)
2) Venous :
1- Deep venous thrombosis.(There may be an obvious predisposing
factor, such as recent surgery,The classical signs of pain and redness
may be absent)
2- Post-thrombotic syndrome. (Swelling, usually of the whole leg, due to
iliofemoral venous obstruction,Venous skin changes, secondary
varicose veins on the leg and collateral veins on the lower abdominal
wall ,Venous claudication may be present)
3- Varicose veins. Simple primary varicose veins are rarely the cause of
significant leg swelling
4- Klippel—Trenaunay syndrome and other malformations. (Rare) Present
at birth or develops in early childhood, Comprises an abnormal lateral
venous complex, capillary naevus, bony abnormalities, hypo(a)plasia of
deep veins and limb lengthening, Lymphatic abnormalities often coexist
5- External venous compression. Pelvic or abdominal tumour including
the gravid uterus, Retroperitoneal fibrosis
The Lymphatic System Dr. Bassim Rassam
25-11-2014
10
6- lschaemia—Reperfusion. Following lower limb revascularisation for
chronic ischaemia
3) Arterial :
1- Arteriovenous malformation. May be associated with local or
generalised swelling
2- Aneurysm. (Popliteal, Femoral, False aneurysm following (iatrogenic)
trauma)
Malignancies associated with lymphedema
1- Lyrnphangiosarcoma (Stewart—Treve’s syndrome)
2- Kaposi’s sarcoma (human immunodeficiency virus, HIV).
3- Squamous cell carcinoma.
4- Liposarcoma
5- Malignant melanoma
6- Malignant fibrous hisfiocytoma
7- Basal cell carcinoma
8- Lymphoma
INVESTIGATION OF LYMPHOEDEMA
1) Routine tests :
1- Full blood count,
2- Urea and electrolytes, creatinine
3- Liver function tests
4- Chest radiography
5- Blood smear for microfilariae
2) Lymphangiography :
1- Direct lymphangiography involves the injection of contrast medium into a
peripheral lymphatic vessel and subsequent radiographic visualisation of
the vessels and nodes. It remains the ‘gold standard’ for showing structural
abnormalities of larger lymphatics and nodes. However, it can be
technically difficult, it is unpleasant for the patient, it may cause further
The Lymphatic System Dr. Bassim Rassam
25-11-2014
11
lymphatic injury and, largely, it has become obsolete as a routine method of
investigation. Few centres now perform this technique and those that do
generally reserve it for preoperative evaluation of the rare patient with
megalymphatics who is being considered for bypass or fistula ligation
2- Indirect lymphangiography involves the intradermal injection of water-
soluble, non-ionic contrast into a web space, from where it is taken up by
lymphatics and then followed radiographically, It will show distal lymphatic
but not normally proximal lymphatics and nodes
3) Isotope Lymphoscintigrcaphy :
This has largely replaced lymphangiography as the primary diagnostic
technique in cases of clinical uncertainty. Radioactive technetium-labelled
protein or colloid particles are injected into an interdigital web space and
specifically taken up by lymphatics, and serial radiographs are taken with a
gamma camera. The technique provides a qualitative measure of lymphatic
function rather than quantitative function or anatomical detail.
4) Computerised Tomography
A single, axial computerised tomography (CT) slice through the midcalf has
been proposed as a useful diagnostic test for lymphoedema (coarse, non-
enhancing, reticular ‘honeycomb’ pattern in an enlarged subcutaneous
compartment), venous oedema (increase volume of the muscular
compartment), and lipoedema (increased subcutaneous fat). CT can also be
used to exclude pelvic or abdominal mass lesions .
5) Magnetic resonance imaging
Magnetic resonance imaging (MRI) can provide clear images of lymphatic
channels and lymph nodes, and can be useful in the assessment of patients with
lymphatic hyperplasia. MRI can also distinguish venous and lymphatic causes
of a swollen limb.
6) Ultrasound
Ultrasound can provide useful information about venous function.
The Lymphatic System Dr. Bassim Rassam
25-11-2014
12
MANAGEMENT OF LYMPHOEDEMA
1) Relief of pain
On initial presentation, 50% of patients with lymphoedema complain of
significant pain. The pain is usually multifactorial and its severity and
underlying cause(s) will vary depending on the aetiology of the
lymphoedema. For example, following treatment for breast cancer, pain may
arise from the swelling itself, (radiation and surgery induced) nerve
(brachial plexus and intercostobrachial nerve), bone (secondary depositis,
radiation necrosis) and joint disease (arthritis, bursitis, capsulitis), and
recurrent disease.
Use of (1)non-opioid(NSAIDs) and (2)opioid analgesics, (3)corticosteroids,
(4)tricyclic antidepressants, (5)muscle relaxants, (6)anti-epileptics,
(7)nerve blocks, (8)physiotherapy, (9)adjuvant anti-cancer therapies
(chemo-, radio- and hormonal therapy).
2) Control of swelling
Physical therapy for lymphoedema comprising 1-bed rest, 2-elevation,
3-bandaging, 4-compression garments, 5-massage and 6-exercises. The
current preferred term is decongestive lymphoedema therapy (DLT) and
comprises two phases. The first is a short intensive period of therapist-led
care and the second is a maintenance phase in which the patient uses a self-
care regimen with occasional professional intervention. The intensive phase
comprises skin care, manual lymphatic drainage (MLD) and multi-layer
lymphoedema bandaging (MLLB), and exercises.
3) Skin care
1- Protect hands when washing up or gardening; wear a thimble when
sewing.
2- Never walk barefoot and wear protective footwear outside.
3- Use an electric razor to depilate.
4- Never let the skin become macerated.
5- Treat cuts and grazes promptly (wash, dry, application of
antiseptic and a plaster).
The Lymphatic System Dr. Bassim Rassam
25-11-2014
13
6- Use insect repellent sprays and treat bites promptly with antiseptics and
antihistamines.
7- Seek medical attention as soon as limb becomes hot, painful or more
swollen.
8- Do not allow blood to be taken from, or injections to be given into the
affected arm (and avoid blood pressure measurement).
9- Protect the affected skin from sun (shade, high factor sun block).
10-
Consider taking antibiotics if going on holiday.
4) Manual lymphatic drainage
Aim to evacuate fluid and protein from the 1SF space, and stimulate
lymphangion contraction. The therapist should perform MLD daily; they
should also train the patient (and/or carer) to perform a simpler, modified
form of massage, termed simple lymphatic drainage (SLD). In the intensive
phase, SLD supplements MLD and, once the maintenance phase is entered,
SLD will carry on as daily massage.
5) Multilayer lymphoedema bandaging and compression garments
Elastic bandages provide compression, produce a sustained high resting
pressure and ‘follow in’ as limb swelling reduces. However, the sub-bandage
pressure does not alter greatly in response to changes in limb circumference
consequent upon muscular activity and posture. By contrast, short-stretch
bandages exert support through the production of a semi-rigid casing where
the resting pressure is low but changes quite markedly in response to
movement and posture. It is generally believed that non-elastic multilayer
lymphoedema bandaging (MLLB) is preferable (and arguably safer) in
patients with severe swelling during the intensive phase of DLT, whereas
compression (hosiery, sleeves) is preferable in milder cases and during the
maintenance phase. Whether the aim is to provide support or compression,
the pressure exerted must be graduated (100% ankle/foot, 70% knee,
50% midthigh, 40% groin) and, of course, the adequacy of the arterial
circulation must be assessed.
Compression garments form the mainstay of management in most clinics.
The Lymphatic System Dr. Bassim Rassam
25-11-2014
14
The control of lymphoedema requires higher pressures (30—40 mmHg arm,
40—60 mmHg leg) than are typically used to treat CVI. The patient should
put the stocking on first thing in the morning before rising. Donning and
doffing lymphoedema grade stockings is difficult and many patients find
them intolerably uncomfortable, especially in warm climates.
Pneumatic compression devices, Unless the device being used allows the
sequential inflation of multiple chambers up to > 50 mmHg, it will probably
be ineffective for lymphoedema.
6) Exercise
Lymph formation is directly proportional to arterial inflow and 40% of lymph
is formed within skeletal muscle. Vigorous exercise, especially if it is
anaerobic and isometric, will tend to exacerbate lymphoedema and patients
should be advised to avoid prolonged static activities, for example carrying
heavy shopping bags or prolonged standing. In contrast, slow, rhythmic,
isotonic movements (e.g. swimming) and massage will increase venous and
lymphatic return through the production of movement between skin and
underlying tissues (essential to the filling of initial lymphatics) and
augmentation of the muscle pumps. Exercise also helps to maintain joint
mobility. Patients who are unable to move their limbs benefit from passive
exercises.
7) Limb Elevation
When at rest, the lymphoedematous limb should be positioned with the
foot/hand above the level of the heart. A pillow under the mattress or blocks
under the bottom of the bed will encourage the swelling to go down
overnight.
8) Drugs
The benzpyrones are a group of several thousand naturally occurring
substances, ( flavonoids) they reduce capillary permeability, improve
microcirculatory perfusion, stimulate interstitial macrophage proteolysis,
The Lymphatic System Dr. Bassim Rassam
25-11-2014
15
reduce erythrocyte and platelet aggregation, scavenge free radicals and
exert an anti-inflammatory effect. Oxerutins (paroven).
Diuretics are of no value in pure lymphoedema. Their chronic use is
associated with side-effects, including electrolyte disturbance, and should be
avoided.
9) Surgery
Only a small minority of patients with lymphoedema benefit from surgery.
1- Bypass procedures
The rare patient with proximal ilioinguinal lymphatic obstruction and
normal distal lymphatic channels might benefit, from lymphatic bypass.
Methods :
1. Omental pedicle
2. Skin bridge (Gillies)
3. Anastomosing lymph nodes to veins (Neibulowitz)
4. Ileal mucosal patch (Kinmonth)
5. Direct lymphovenous anastomosis
2- Limb reduction procedures
These are indicated when a limb is so swollen that it interferes with
mobility and livelihood. These operations are not ‘cosmetic’ in the sense
that they do not create a normally shaped leg and are usually associated
with significant scarring
1. Sistrunk. A wedge of skin and subcutaneous tissue is excised and the
wound closed primarily.
This is most commonly carried out to reduce the girth of the thigh.
2. Homans. First skin flaps are elevated, to allow the excision of a wedge
of skin and a larger volume of subcutaneous tissue down to the deep
fascia from beneath the flaps, which are then trimmed to size to
accommodate the reduced girth of the limb and closed primarily. This
is the most satisfactory operation for the calf. The main complication
is skin flap necrosis. There must be at least 6 months between
The Lymphatic System Dr. Bassim Rassam
25-11-2014
16
operations on the medial and lateral sides of the limb and the flaps
must not pass the midline to avoid skin flap necrosis. This procedure
has also been used on the upper limb, but is contraindicated in the
presence of venous obstruction or active malignancy.
3. Thompson One denuded skin flap is sutured to the deep fascia and
buried beneath the second skin flap (the so-called ‘buried dermal
flap’). This procedure has become less popular as pilonidal sinus
formation is common. The cosmetic result is no
better than that obtained with the Homans’ procedure and there is no
evidence that the buried flap establishes any new lymphatic connection
with the deep tissues.
4. Charles This operation was initially designed for filariasis and
involved circumferential excision of all the skin and subcutaneous
tissues (lymphoedematous tissue) down to and including the deep
fascia, with coverage using split-skin grafts. This leaves a very
unsatisfactory cosmetic result and graft failure is not uncommon.
However, it does enable the surgeon to reduce greatly the girth of a
massively swollen limb(allows the surgeon to remove very large
amounts of tissue and is particularly useful in patients with severe skin
changes).
DONe by
Ali Kareem