
1
Dr. Hawa Al-Dhahir (M.B.Ch.B., M.Sc., Ph.D.-United Kingdom)
Department of physiology / College of medicine – Baghdad University.
THE PHYSIOLOGY OF THE GASTROINTESTINAL TRACT
INTRODUCTION
The main function of the gastrointestinal tract is to provide the cells and tissues of the body with
continual supply of water, electrolyte and various nutrients.
The gastrointestinal tract (GI tract) is a coiled hollow tube which passes right through the body
and opened to the outside at both ends(mouth and anus), so that the lumen of the tube can be
considered as an internal continuation of the external environment. Technically speaking the
contents of the digestive tract are not truly inside the body until they are absorbed across the
cells that line the digestive tract.
Food and fluids will enter at the top end (the mouth) and during their passage through the tract
the food will be subjected to various mechanical and chemical changes. It will be chopped and
grounded by the teeth, propelled forward through the tract by contraction of its muscular wall,
and it will be broken down by chemical reactions performed by the digestive enzymes, into
smaller and simpler compounds.
The digested food along with water and electrolytes will be absorbed by the intestinal mucosa to
enter the blood or lymph and will be utilized either to build up the body structure or to provide
energy. The undigested food will pass at the lower end (the anal canal).
The GI tract is divided into successive compartments starting with:
1- Oral cavity.
2- Pharynx.
3- Esophagus.
4- Stomach.
5- Small intestine. - Duodenum
- Jejunum
- Ileum
6- large intestine -Caecum -Ascending colon -Transverse colon -Descending colon
-Sigmoid -Rectum and anal canal
2
The accessory organs are:
1- Salivary glands. 2- Pancreas. 3- Liver.
ORAL CAVITY
There are 3 main structures in the oral cavity these are:
1- Teeth.
2- Tongue.
3- Salivary glands.
TEETH: they are important for the process of mastication (chewing). Mastication is vital
because
1-the process of mastication will result in the opening or destruction of the cellulose
covering of most fruits and raw vegetables since most fruits and vegetables have
indigestible cellulose membranes that must be broken down before the food can be
utilized. Cooking and steam also breaks the cellulose covering.
2-chewing aids in the digestion of food because the digestive enzymes act only on the
surface of the food particles. Therefore chewing will help in digestion by cutting the large
food particles into smaller ones with larger total surface area being exposed to the
intestinal secretion.
3-with proper mastication the bolus formed will be reduced into a paste form. This will
prevent excoriation or damage of the mucus membrane of the esophagus, stomach and
small intestine, and will facilitate the movement of food from one segment of the GI tract
to the succeeding segment of the gut.
After understanding the importance of chewing one can understand why people without
teeth or dentures will have difficulty in swallowing dry food and they often complain of
indigestion in addition they may complain of painful contraction of the esophagus upon
swallowing because the food bolus hasn’t been turned into a paste.
TONGUE: this is an extremely mobile mass of striated muscle covered with a mucus
membrane. It helps greatly in mastication and swallowing.
SALIVARY GLANDS:
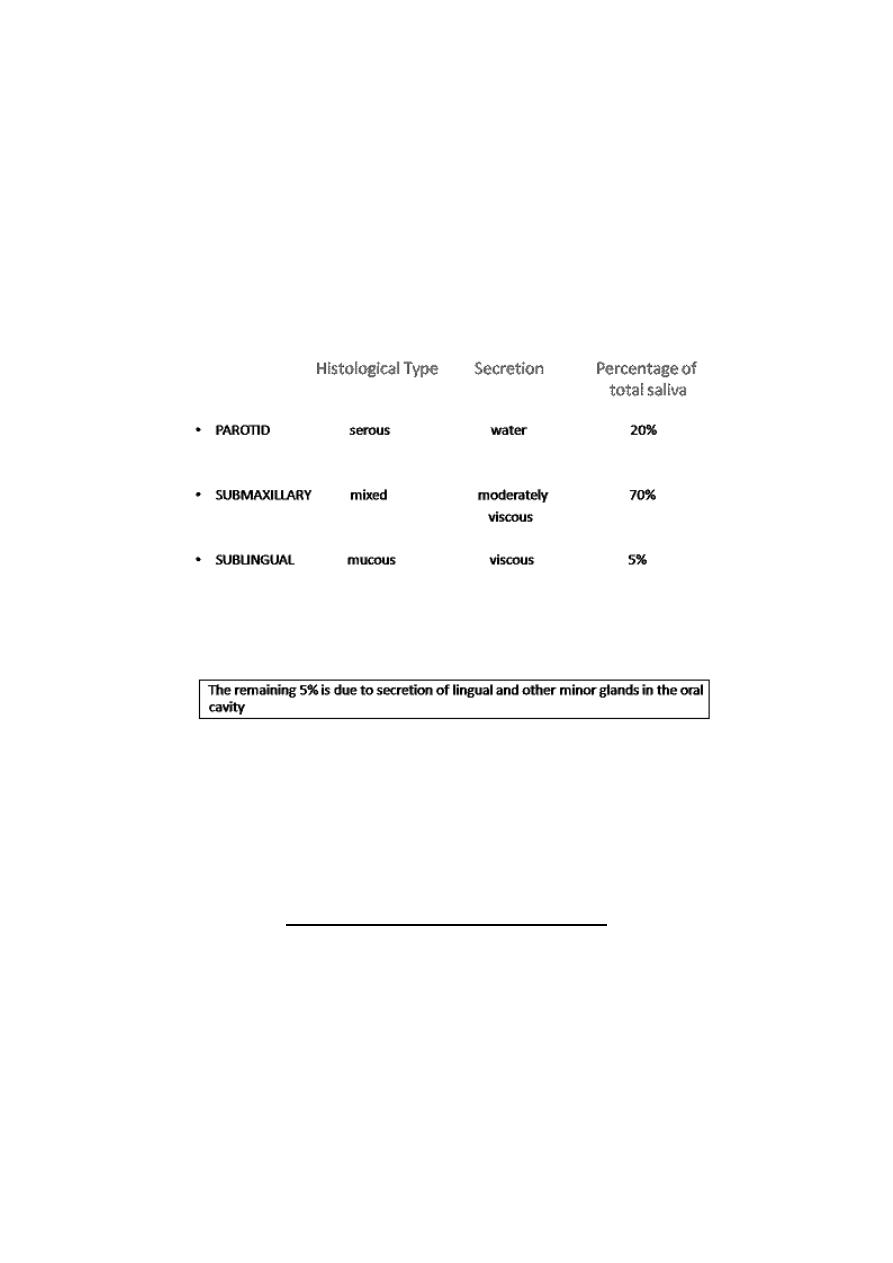
There are 3 chief paired salivary glands these are:
1- Parotid.
2- Submandibular (submaxillary).
3- Sublingual.
In addition there are many small salivary glands scattered in the lining of the oral cavity
and are named according to their position.
3
Labial -------- lips
Buccal -------- cheeks
Palatal -------- palate
Lingual -------- lingual tonsils
There are 2 types of secretory cells in the salivary glands.
1- Serous cells: these cells secret the serous secretion that provide the enzyme
ptyalin
(salivary α- amylase) for the digestion of starch, and the secretion of these cells is thin
and watery.
2- Mucus cells: these cells secret mucus secretion which contains
mucin
and the
secretion is viscid(thick).
COMPOSITION OF SALIVA
The daily secretion of saliva is about 1-1.5 liter per day. A large proportion of this 24 hours
volume is secreted at meal time. Ordinary mixed saliva contains:
1- Water 99.5%.
2- Solids 0.5%.
The solid materials are:

4
A- Organic
B- Inorganic
Organic constituents of saliva:
1- Protein mucin.
2- Ptyalin or α-amylase for the digestion of starch.
3- Lingual lipase this enzyme is secreted by Ebner’s gland on the dorsal surface of the tongue. It
plays an important role in the hydrolysis of triglycerides. It differs from pancreatic lipase in that
it does not need a detergent for its action. It is also very hydrophobic and so has a great ability
to bind to dietary triglycerides. The enzyme is active over a wide range of PH and has an acidic
PH optimum. And it is very stable; its action starts in the mouth and continues in the stomach
and even in the upper intestine. It can digest as much as 30% of dietary triglycerides.
4- Urea, uric acid & creatinine.
5- Kallikrein which is an enzyme that acts on plasma protein to produce a very powerful
vasodilator polypeptide called kinin.
6- Specific blood group antigen (ABO system).
Blood groups substances agglutinogens (ABO system) are present in 80% of the people we call
them (secretors). The activity of saliva of secretors is several hundred times greater than that of
the red blood cells which make them of medico-legal significance because it may make it
possible to determine an individual blood group from a recently used drinking vessel or glass or
discarded cigarettes.
7- Somatostatin, glucagon, renin and several growth factors.
8- Lysozyme which can destroy the bacteria by lysis.
9- Lactoferrin which binds to iron and deprive organisms of nutrient iron and it is bacteriostatic.
10- Proline-rich protein that protects tooth enamel and binds toxic tannins.
11- Immunoglobulin A which can destroy the bacteria including those that cause the dental
caries.
12- Glucose is absent from saliva.
Inorganic constituents of saliva:
Saliva contains different ANIONS such as chloride, phosphate, bicarbonate, Floride and CATIONS
such as calcium, sodium and potassium.
5
Floride is important to prevent dental caries, calcium salts might be the source of tartar deposits
on the teeth.
The concentration of sodium and chloride in the saliva is less than that in the plasma, while
potassium concentration in the saliva is higher than that in the plasma.
PLASMA SALIVA
Na⁺ 146 mEq/liter 10
Cl⁻ 110 mEq/liter 10
K⁺ 5 mEq/liter
25
Glucose 80-120 mg/dl
zero
The low sodium concentration of the saliva and the absence of glucose in the salivary secretion
might be of significance in that it will help in the taste of sweet and salty substances.
Aldosterone increases the absorption of Na⁺ and Cl⁻ from the saliva and the secretion of K⁺ to
the saliva similar to the kidney. In Addison disease there is a high Na⁺/K⁺ ratio in saliva.
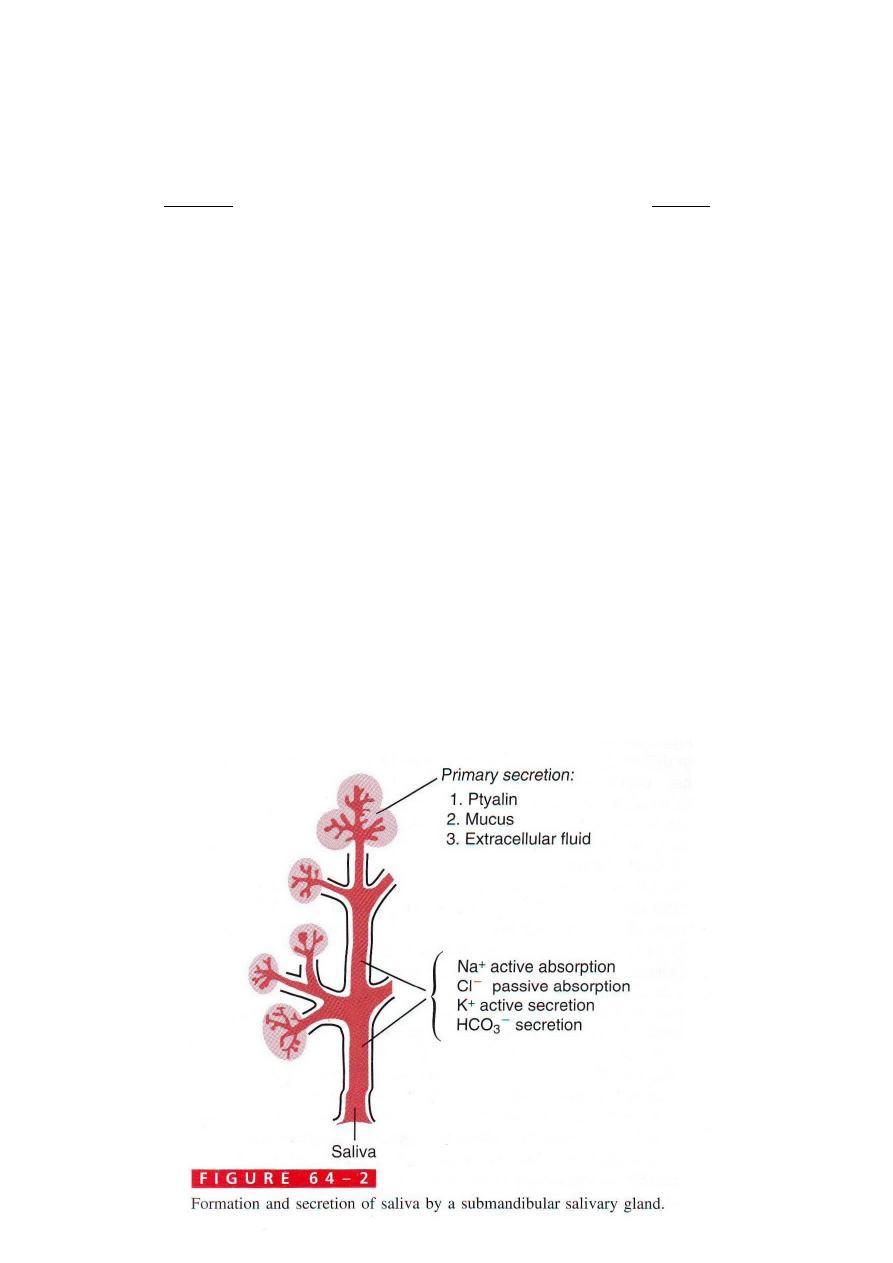
The rate of salivary secretion is determined mainly by the end piece secretion while the
composition is determined mainly by the ducts. The ductal epithelium is very impermeable to
water. The absorption of sodium and chloride occurs at a faster rate than the secretion of the
potassium thus saliva becomes hypotonic. When salivary flow rates are high, there is little time
for re-absorption so saliva contains more of the normally reabsorbed and less of the normally
secreted ions. The PH of the saliva is between (6-7.4). This PH is quiet favorable for the action of
the enzyme ptyalin. At PH 7 the saliva is saturated with calcium so that the teeth do not lose
calcium to the saliva. On the other hand at more acidic PH the calcium will be lost from the teeth
to the saliva.
6
INNERVATION OF THE SALIVARY GLANDS
The salivary glands are supplied with efferent fibers from both the parasympathetic and
sympathetic division of the autonomic nervous system.
The
parasympathetic stimulation
causes:
1- Increase salivation (copious secretion).it produces a rapid flow of large amount of watery
saliva from the gland.
2- Vasodilatation which is mediated by non-adrenergic non-cholinergic (NANC) vasodilator
nerve fibers and these nerves might secrete VIP (vasoactive intestinal polypeptide).
VIP is a co-transmitter with acetylcholine in some of the post ganglionic parasympathetic
neurons.
Also increase salivation will increase Kallikrein secreted by the activated salivary cells
which in turn causes additional vasodilatation.
The stimulation of the
SYMPATHETIC NERVE SUPPLY
causes:
1- Mainly vasoconstriction.
2- Some secretory response which is more variable than that of the parasympathetic and
depends on the species and the gland, for example in human stimulation of the
sympathetic nerve supply to the submandibular gland causes the secretion of small
amounts of thick viscid saliva rich in organic constituents while it has no effect on parotid
secretion.
3- Contraction of the myoepithelial cells.
REGULATION OF SALIVARY SECRETION
Salivary secretion is brought about reflexly:
1- Unconditioned salivary reflex due to stimulation of the nerves within the mouth
such as by the presence of food or other substances. Materials placed in the mouth
will cause secretion after a short latent period of 2-3 seconds; the secretion of
saliva varies in quantity and quality with the physical and chemical nature of the
substance introduced. The most palatable food or those that cause great taste
sensation will produce greater salivary secretion. Material such as acid will cause
profuse salivary secretion because it stimulates the taste buds, this stimulus is
chemical in nature e.g. stimulation of salivary secretion by lemon or sweets.
7
Material such as dry sand or powder with no taste (inedible powder) will stimulate
secretion by acting as a physical stimulus. The mere movements of the jaws and of
the tongue over the mucosa of the mouth will have such an effect. Also grinding of
the teeth and manipulation of the dentist will cause salivary secretion.
2- Conditioned reflex the stimulus which initiates such a reflex is not applied to the
nerves of the mouth but is received by one or other of the organs of special senses
other than that of taste particularly those of sight, smell, hearing, or even thought
of palatable food. The conditioned reflex requires previous training and experience
e.g. Pavlov experiment on dogs.
3- In abnormal situations, salivation can occur in response to reflexes originating from
the esophagus, stomach and the small intestine by stimulation of the vagal afferent
fibers. Thus when a person eats a very irritating food or is nauseated there will be
an increase salivation which might act as a neutralizing or diluting agent for the
irritating substance.
FUNCTIONS OF SALIVA
1- Saliva helps to moisten, lubricate and soften food, mixes it up and makes it
possible to be swallowed.
2- It keeps the mouth wet and facilitates speech.
3- Saliva is important for the taste sensation because it acts as a solvent. Taste is
chemically mediated and therefore any substance must be dissolved in order to
stimulate the taste buds.
4- Saliva contains 3 buffering systems and these are bicarbonate, phosphonate, and
mucin. The bicarbonate is the most important. These buffers in saliva help in
maintaining the oral PH around 7 so that the teeth do not lose calcium to the oral
fluid.
5- Saliva has a digestive function through its enzyme ptyalin and lingual lipase.
6- Oral hygiene this is one of the very important functions of the saliva. The flow of
saliva plays a very important role in maintaining healthy oral tissues. The mouth is
loaded with many harmful bacteria that can cause tissue damage or dental caries.
Salivary secretion helps in preventing these harmful effects by several ways:
1) Mechanical: the flow of saliva will wash away the pathogenic bacteria and
also the remaining food particles and debris that can act as a metabolic
support for the bacteria.
2) Thiocyanate ions which can act as bactericidal.
3) Lysozyme.
4) Lactoferrin.
5) Proline-rich proteins.
6) Immunoglobulin A.
*the last 4 were mentioned previously regarding their action.

8
The salivary secretion is very important for oral hygiene that’s why wounds in the mouth rarely
become infected. Thus in patients with deficient salivary secretion there are higher than normal
incidence of dental caries, oral ulcers and infections. In patients with fever when salivary
secretion is suppressed the lips, teeth and mouth becomes coated with a mixture of food
particles, dry mucus and dead epithelium which if not removed mechanically might become the
site of bacterial infection.
Disturbance of salivary secretion
:
Deficiency of salivary secretion (xerostomia) can occur after
:
- Emotional state such as fear or anxiety.
- Dehydration.
- Fever.
- Anticholinergic drugs.
Hyper salivation (sialorhoea) occurs during:
- Pregnancy.
- Tumours of the mouth or tongue or even a carious tooth (reflex stimulation of salivary
secretion due to local irritation).
- Diseases of the esophagus, stomach, pancreas such as tumor of the esophagus or spasm,
gastric or duodenal ulcer, pancreatitis, (esophago-salivary reflex).
Esophageal secretion:
Mucus only, in the upper esophagus to prevent excoriation and in the lower esophagus to
protect from acid.
9
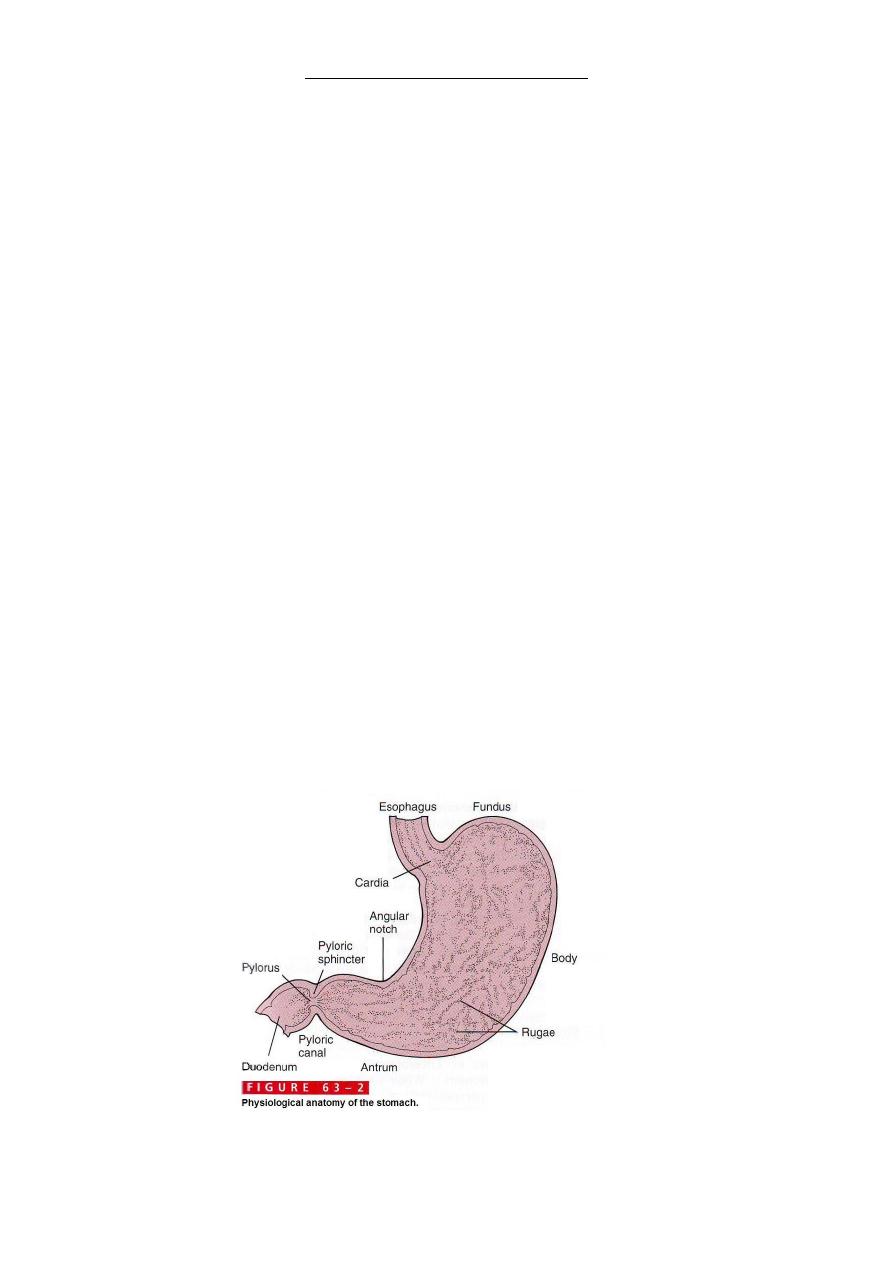
FUNCTIONS OF THE STOMACH
1- As a reservoir to store the food, we can eat food faster than we can digest, so some
degree of storage is needed within the digestive tract. The stomach is specialized to
meet this need the human stomach is a pouch like enlargement of the gut tube
that stores food as it is eaten and gradually releases it into the intestine for
complete processing. Because of its storage function, the tunica mucosa and tunica
sub mucosa of the stomach are specialized for distention as food enters the
stomach. These 2 layers of the stomach show longitudinal fold or rugae that can
flatten as the stomach is stretched. The tunica muscularis of the stomach is also
specialized for distention. The smooth muscle of this layer can be stretched
without increasing its contraction strength or tone. This allows the stomach to hold
large quantities of food without increasing the pressure of its contents.
2-
Mechanical degradation and liquification of the food, the stomach mixes the food
with gastric secretion until it forms a semi-fluid mixture called
chyme.
3- Small role as a digestive function by hydrochloric acid and pepsin. Hydrochloric acid
cause hydrolysis of food and also activates pepsinogen into pepsin and pepsin
begins protein digestion.
4- Antibacterial action, the high acidity of the gastric juice will render the gastric juice
sterile. If the gastric acid secretion is reduced by diseases, drugs or surgery, there is
an increased likelihood of bacterial growth.
5- Absorption, no nutritionally important absorption occurs in the stomach, only
alcohol, some water and lipid soluble drugs are absorbed across the stomach
mucosa.
6- Haemopoiesis, the secretion of intrinsic factor in the body of the stomach is
necessary for the normal absorption of vitamin B12 in ileum.

10
GLANDS OF THE STOMACH
In addition to mucus secreting cells that line the entire surface of the stomach we have
other glands, in the narrow zone about 1 cm. wide that surrounds the esophageal orifice this
area contains the cardiac glands, the cardiac glands consist of mucus secreting cells and few
pepsinogen secreting cells.
In the pyloric antrum, the pyloric glands are located. These glands consist of mucus
secreting cells and also they secrete some pepsinogen and in the deeper portions of these glands
there are the G-cells or the gastrin secreting cells which secrete the hormone gastrin.
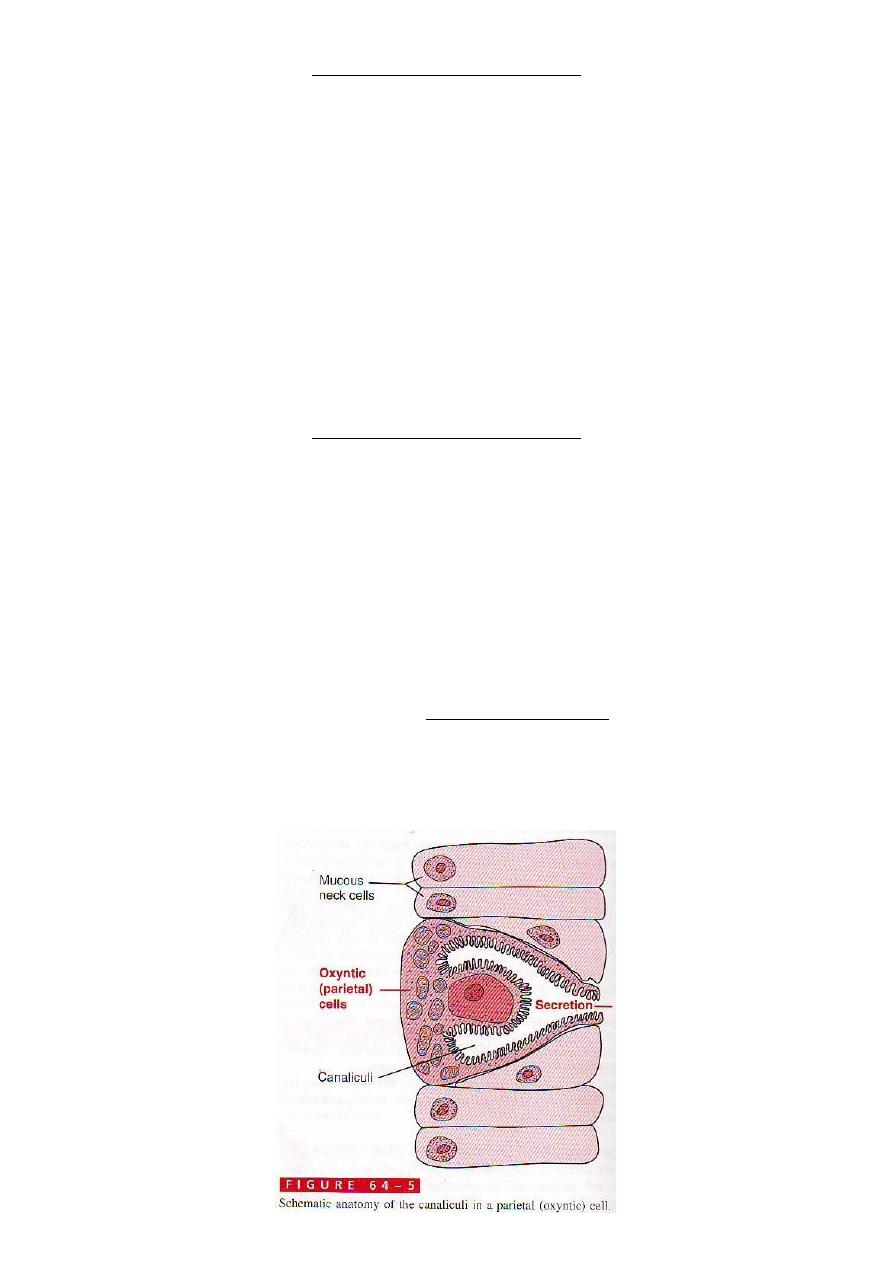
In the body and fundus of the stomach we have the main gastric gland or the oxyntic
gland or the gastric gland proper. There are 35 millions of these glands in the body and fundus of
the stomach, the gastric gland proper is composed of 3 different types of cells:
1- Mucus neck cells: these cells secret mainly mucus with some pepsinogen.
They divide and the new cells which migrate both to the surface to become mucus
cells or down into the gland to become parietal cells. Peptic cells are capable of
mitosis but they may also come from mucus neck cells.
2- Peptic or chief cells: these cells secrets pepsinogen.
3- Parietal or oxyntic cells: these cells secrete hydrochloric acid and also the intrinsic
factor.
11
COMPOSITION OF GASTRIC JUICE
Daily secretion 2-3 liters, the PH is about 0.9-1.0.
Gastric juice consists of water and different organic and inorganic constituents:
1- Electrolytes like sodium, potassium, magnesium, calcium, chloride, phosphate,
sulphate and bicarbonate.
2- HCL.
3- Mucus.
4- Pepsins.
5- Lipase.
6- Gelatinase.
7- Intrinsic factor.
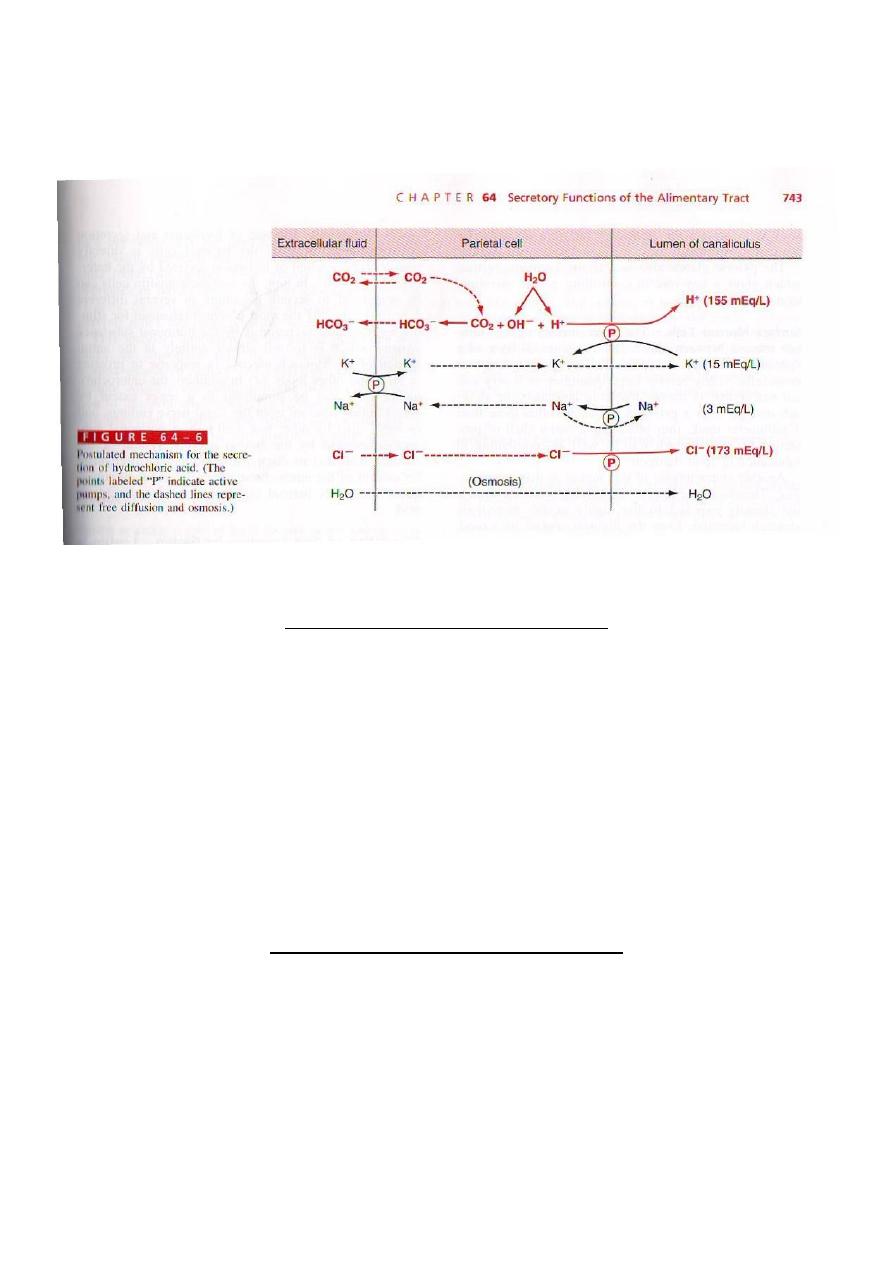
HYDROCHLORIC ACID SECRETION
HCL is secreted by the parietal or oxyntic cells which are found in the main gastric gland or
oxyntic gland, the PH of acid solution is about 0.9 and thus it is extremely acidic. To reduce the
PH to this level the hydrogen ion concentration of this solution is about 3 million times that of
the arterial blood.
Plasma Juice
0.00004 mEq/liter. 150 mEq/liter.
To concentrate the hydrogen ion to this tremendous amount, a great amount of energy is
needed. The hydrochloric acid formed and released by the parietal cells is not formed inside the
protoplasm of the cells but it is formed in the intracellular canaliculi that are small channels that
communicate with the lumens of the gastric gland. If the parietal cells are stained with certain
indicator dyes, the inside of the cells like that of the other body cells has a PH 7-7.2 while the
canaliculi has an extremely acid reaction. HCL is formed at the membrane of these canaliculi and
then conducted through openings to the outside.

12
Although the mechanism behind the formation of HCL is not completely understood however
one of the suggestive mechanisms is the following:
The hydrogen ion (H⁺) comes from H
2
CO
3
and
by the hydration of C
O2.
This reaction is catalyzed
by carbonic anhydrase and the parietal cells are particularly rich in this enzyme. Diamox which is
a carbonic anhydrase inhibitor inhibits acid secretion. H⁺ is pumped out of the parietal cells in
exchange for potassium and this is carried out by the enzyme H⁺-K⁺ ATPase which transports
hydrogen against a concentration gradient of this great magnitude. Omeprazol inhibits H⁺-K⁺
ATPase and thus inhibit acid secretion and is very effective in the treatment of peptic ulcer.
The bicarbonate HCO
3
⁻ formed by the dissociation of H
2
CO
3
is extruded into the interstitial fluid
in exchange for Cl⁻. Because of the efflux of HCO
3⁻ into
the blood the stomach has a negative
respiratory quotient i.e. the amount of CO
2
in the arterial blood is greater than the amount in
the gastric venous blood. When gastric acid secretion is elevated after a meal (which stimulates
acid secretion) sufficient H⁺ may be secreted to raise the PH of the systemic blood and make the
urine alkaline (because the amount of bicarbonate ions diffusing to the blood will depend on the
amount of hydrogen ions secreted into the juice). This is the probable explanation of the high PH
of the urine excreted after a meal the so called
post-prandial alkaline tide
.
Pumping hydrogen out of the parietal cells in exchange for potassium requires appreciable
energy and this is provided by hydrolysis of ATP, inhibition of ATP generation prevents H⁺
secretion.
Cl⁻ is extruded to the lumen, the concentration gradient is inward but the electrical gradient is
outwardly directed and is much greater so Cl⁻ is extruded outwards.
Water moves passively from cell to juice and the gastric juice is isotonic with plasma.
13
Other suggested mechanism for the formation of HCL is that H⁺ comes from the dissociation of
water into H⁺ and OH⁻. And that Cl⁻ is actively secreted into the lumen of the canaliculus.
FUNCTIONS OF HYDROCHLORIC ACID
The main functions of HCL are:
1- It causes activation of pepsinogen into pepsin. Pepsin is an active proteolytic enzyme in a high
acid medium (PH-2) but above a PH of 5, pepsin has little proteolytic activity and soon becomes
completely inactivated.
2- This acidity has some antibacterial or antiseptic action against some virulent organisms. The
gastric acid will damage these bacteria before they reach the small intestine, thus in normal
healthy individuals the duodenal contents are relatively sterile.
3- Reduce iron from ferric to ferrous state.
MUCUS SECRETION BY THE STOMACH
Two types of gastric mucus are secreted by the stomach:
1- Soluble mucus this is secreted by the cells of the pyloric and cardiac gland and also
by mucus neck cells of the main gastric gland. These cells secrete large quantities of
thin mucus which is soluble and helps in protecting the stomach wall from damage
by peptic digestion.
14
2- Visible mucus this is secreted by the surface epithelial cells of the gastric mucosa
and its more alkaline, thick, viscid and even jelly-like. It forms a thick coat (2-3 mm
thick) that covers the surface of the gastric mucosa. This mucus will act as an
important factor of protection for the stomach wall. The mucus secretion from the
surface epithelium is stimulated by various chemical and tactile stimuli. Mucus
secreted by neck cells and surface mucus cells in the body and fundus of the
stomach and similar cells form a
FLEXIBLE GEL
that coats the mucosa.
The surface mucosal cells also secrete HCO
3⁻.
The HCO
3⁻
and the mucus form an
UNSTIRRED LAYER
that has a PH around 7.
The unstirred layer plus the surface membrane of the mucosal cells and the tight junctions
between them constitute the
MUCOSAL BICARBONATE BARRIER
that protects the mucosal
surface from damage by gastric acid.
PROSTAGLANDINS:
Act as cyto-protector to gastric mucosa by:-
1) Stimulate mucus production.
2) Increase bicarbonate secretion.
3) Inhibit acid accumulation.
4) Increase mucosal blood flow.
Misoprostol is a prostaglandin analogue is effective in the treatment of duodenal
ulcer it has both acid inhibitory and cyto-protective properties. Especially when
used in patients with arthritis and duodenal ulcer (DU).
Substances that tend to disrupt the barrier (mucosal bicarbonate barrier) and cause
irritation include:
H-pylori (helicobacter pylori) – Aspirin – NSAID’S (non-steroidal anti inflammatory
drugs) – ethanol – vinegar – bile salts.
NSAID’S inhibit prostaglandin, the older types are non specific inhibitors of both
cyclooxygenase 1 (COX1) which is involved in the production of prostaglandins in
the normal GI and cyclooxygenase 2 (COX2) which induce prostaglandin production
at inflammatory site. So COX2 specific inhibitor like rofecoxib is used in treating
arthritis.
Some of the resistance of the gastric mucosa is provided by the presence of
TREFOIL PEPTIDES
in which there are several types of these peptides and they
are acid resistant.
PEPSIN:
secreted as pepsinogen and activated by HCL. Also pepsin itself can
activate pepsinogen into pepsin → autocatalytic positive feedback process.
Optimum PH for pepsin is 2, At PH 5 it will be blocked.
15
Group
I
pepsinogen: only present in acid secreting region i.e. secreted by peptic
and mucus neck cells of the oxyntic gland.
Group
II
pepsinogen: from pyloric, Brunner’s and oxyntic gland.
Maximal acid secretion correlates with pepsinogen
I
level. Patients with
congenitally elevated circulating pepsinogen
I
levels have a 5 folds greater
incidence of peptic ulcer than normal levels.
Gastric lipase:
weak lipolytic enzyme acts mainly on butter fat.
Gelatinase:
liquefies the protein gelatin.
Intrinsic factor:
secreted by the parietal cells, it’s a glycoprotein that combines
firmly with vitamin B12→protect vitamin B12 from digestion and also this complex
will become bound to specific receptors in the ileum and from there vitamin B12 is
absorbed by endocytosis.
Trypsin is required for the process of absorption to be efficient and absorption
might be decreased in patients with pancreatic insufficiency. If the acid producing
cells of the stomach are destroyed such as after chronic gastritis then the person
will develop achlorhydia and also pernicious anaemia due to the failure of
maturation of RBC in the absence of Vitamin B12 stimulation of the bone marrow.
REGULATION OF GASTRIC SECRETION
The regulation of the gastric secretion is by both nervous and hormonal mechanisms. Thus it is
different from that of salivary secretion which is controlled by nervous mechanism only. Gastric
secretion associated with a meal can be divided into 3 phases:-
1- Cephalic phase.
2- Gastric phase.
3- Intestinal phase.
1)
Cephalic phase:
also called
nervous or appetite phase
. Gastric secretion can occur
even before the food reaches the stomach and it is controlled by the vagus nerve. It can be
divided into to 2 types:
A-unconditioned reflex: the secretion results from the taste of the food. The presence of food in
the mouth will stimulate gastric secretion after five minutes and the secretion may persist for
half to two hours. The sham feeding technique by Pavlov proves the mechanism of production of
appetite juice.
16
B-conditioned reflex: the cephalic phase of gastric secretion can be brought about not only by
the taste of the food but also by the sight, smell or thought of food that’s to say by conditioned
reflex.
The neural pathway for the cephalic phase is through the vagus and can be abolished by:
-Atropine.
-Vagatomy (cutting the vagi).
Gastric secretion in response to this vagal stimulation is highly acidic and high in pepsin.
Cephalic phase accounts for 1/3 to ½ of total gastric acid secretion associated with a meal.
Cephalic phase can be studied by some drugs for e.g. hypoglycaemia introduced by insulin or
glucose analogue such as 2 deoxyglucose which activates hypothalamic centers that stimulates
secretion through the vagus nerve.
Emotional states
:
anger and hostility is associated with hyper secretion of the gastric mucosa.
This is mediated principally by the vagi. Fear and depression decrease gastric secretion.
2)
Gastric phase:
presence of food in the stomach stimulates gastric secretion by both
A-Nervous. B-Hormonal.
A-Nervous:
1-Local reflexes in the intrinsic nerve plexus of the stomach (chemoreceptor and stretch).
2-Vagovagal reflexes that passes from the stomach to the brainstem and back to the stomach.
B-Hormonal:
→
Gastrin
Gastrin is produced by G-cells in the antrum. A second type of gastrin producing cells the TG-cells
found throughout the stomach and small intestine. Gastrin is also found in pancreatic islets in
fetal life, but not certain if in normal adult life, but it is present in gastrin secreting tumours of
the pancreas (Gastrinomas).
The G-cells are flask shaped and have a small apex which contains micro villi which is in contact
with the lumen. This apical portion may serve some type of receptor function.
MOLECULAR FORMS OF GASTRIN:
1- G-17 with 17 amino acids mainly in tissues.
2- G-34 (big gastrin) with 34 amino acids mainly in blood.
3- G-14 (mini gastrin) found in both blood and tissues.
G-17 is the principle form to do with respect to gastric acid secretion.
The presence of food in the stomach causes the release of gastrin by:
1-distention→the bulk of food distends the pyloric antrum and this causes the release of gastrin
2-certain substances such as peptides and amino acids (meat extract-partially digested proteins)
3-however gastrin is also released in response to vagal stimulation which release gastrin-
17
releasing peptide (GRP) or Bombesin to produce gastrin.
Vagal nerve stimulation will inhibit somatostatin which inhibits the G-cells. Thus the nervous
and humeral stimulation of gastric secretion interact and are not merely additive but are
markedly synergistic.
Gastrin stimulates gastric juice highly acidic but it does not contain high peptic activity.
The gastric phase of secretion accounts for ½ -
2/3
of total gastric acid secretion associated with a
meal.
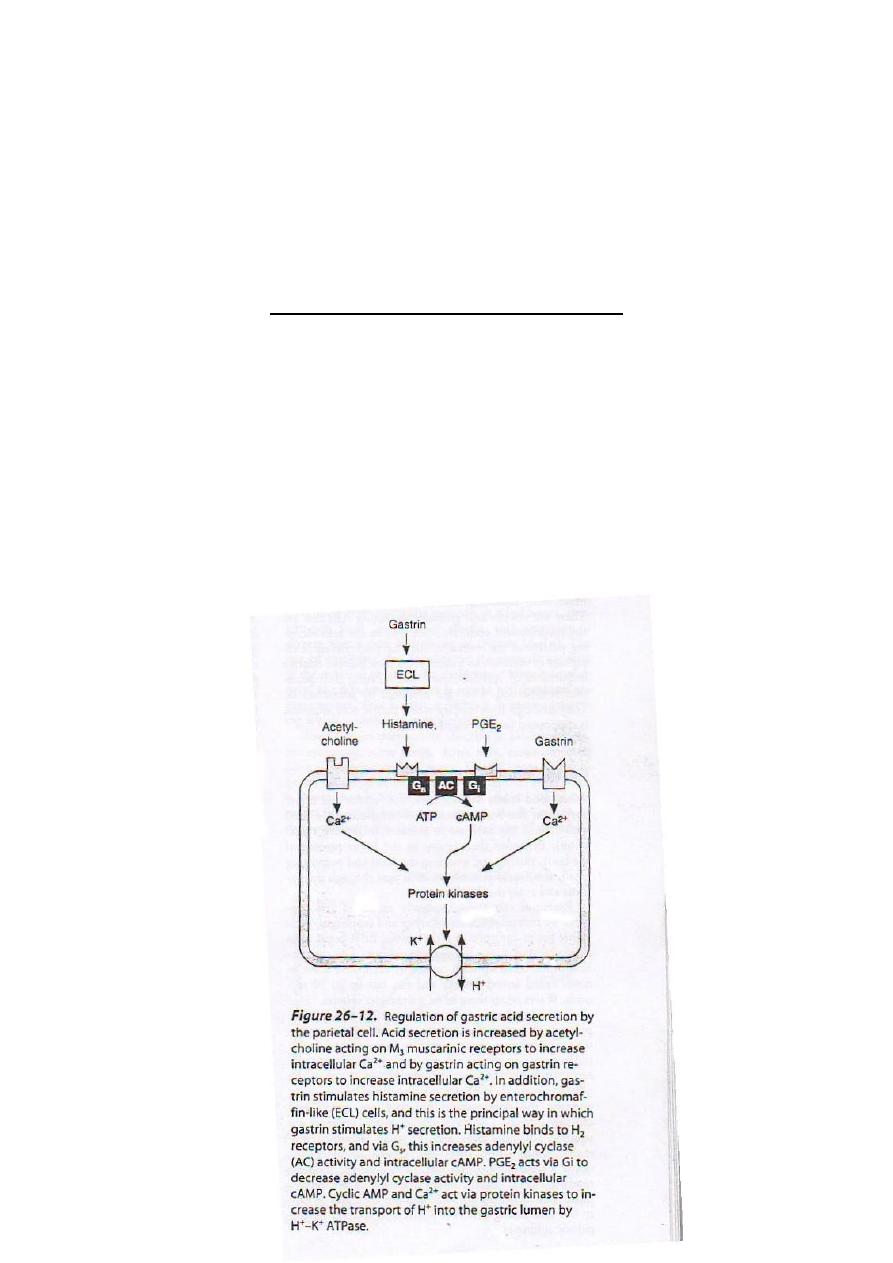
ROLE OF HISTAMINE IN ACID SECRETION
Histamine is a powerful stimulant of acid secretion. There are 3 receptors for histamine
H1 – H2 – H3
H2-receptors mediate the stimulatory effect of histamine on acid secretion. So H2-receptors
antagonist such as cimitidine – ranitidine – famotidine – e.t.c. are very useful drugs in the
treatment of peptic ulcer.
It is believed that there are separate receptors for acetylcholine-gastrin and histamine but they
interact synergistically i.e. histamine facilitate the action of gastrin and acetylcholine. It is
believed that the stimulatory effect of gastrin on acid secretion is mediated by the release of
histamine which in turn stimulates the oxyntic cells to produce acid secretion.
18
ECL (Enterochromaffin like cells or chromaffin)
Present in acid-secreting part of the stomach. Gastrin acts mainly by stimulating these cells to
release histamine which acts quickly to stimulate gastric acid secretion. These cells have Ach
receptors but?? Importance.
These cells are inhibited by somatostatin.
FEEDBACK INHIBITION OF GASTRIC ACID SECRETION BY ANTRAL FACTORS:
If the PH in the antrum falls to 1.5 or 2 (highly acidic) then there will be inhibition of the gastrin
mechanism and thus there will be inhibition of acid secretion induced by gastrin. This will
protect the stomach against very high acid secretion. When the PH rises gastrin will be secreted
again. Acid in the antrum inhibit gastric secretion partly by direct inhibition of the G-cells and
partly by somatostatin which inhibits the G-cells.
3)
Intestinal phase:
The presence of certain substances in the upper small intestine will stimulate the secretion of
gastric acid. Certain food in the small intestine will cause small release of enteric or intestinal
gastrin from duodenal mucosa which will cause small increase in acid secretion. The intestinal
phase accounts for the least of the total acid gastric secretion.
Inhibition of gastric secretion by intestinal factors:
gastric secretion can be inhibited also by
certain substances in the upper small intestine for e.g. 1-Acid. 2-Fat. 3-Hyper/Hypo-osmotic
fluids. 4-Any irritating substance in the upper small intestine.
The inhibition of gastric secretion can be brought about in 2 ways:
1) Enterogastric reflex: reflex nervous signals are transmitted from the duodenum
back to the stomach to cause inhibition of gastric secretion and gastric emptying.
This reflex is stimulated by many factors for e.g. acid in the duodenum will
stimulate this reflex. If the PH in the duodenum falls to 3.5 or 4 this will stimulate
this reflex to inhibit gastric secretion and thus protects the duodenal mucosa from
high acidity.
2) Inhibitory hormones: the presence of acids, fat, hypo/hyper osmotic fluids, e.t.c.
causes the release of several intestinal hormones that are:
-
Secretin.
-Gastric inhibitory peptide (GIP).
-Vasoactive intestinal polypeptide (VIP).
-Somatostatin.
-Peptide YY.
19
Enterogastrone: refers to the inhibitory hormones that inhibit gastric acid secretion. Peptide YY
is a good candidate to be Enterogastrone. Fat causes its release from the jejunum and it is an
effective inhibitor of gastrin-stimulated acid secretion.
Gastric secretion is increased following the removal of a large part of the small intestine, due to
the removal of the source of these inhibitory hormones. The purpose of inhibition of gastric
secretion and emptying is to slow the release of chyme from the stomach to the small intestine
when the small intestine is already filled. So high acidity reduces gastric secretion and motility
and high fat reduce gastric secretion and emptying and so on.
Secretion of the stomach during the interdigestive period
The stomach secrets only a few milliliters of gastric juice per hour during the interdigestive
phase when little or no digestion is occurring anywhere in the gut. The secretion is usually of the
non-oxyntic type i.e. composed mainly of mucus, little pepsin and almost no acid and sometimes
it is usually slightly alkaline with sodium bicarbonate. During emotional stress there will be an
increase of the interdigestive secretion up to 50 ml. or more per hour like that of the cephalic
phase. So emotional stimuli is believed to be one of the factors for the development of peptic
ulcer.
Total Gastrectomy and its effect:
1-Componsate for the intrinsic factor deficiency by paranternal injection of cyanocobalamine
(vit.B12).
2-Protein digestion is normal in the absence of pepsin.
3-Iron deficiency anaemia will occur. Gastric secretions dissolve the iron and permit it to form
soluble complexes with ascorbic acid (vit. C) and other substances that aid its reduction to the
fe⁺⁺ ferrous form. That’s why iron deficiency anaemia is a troublesome and frequent
complication of Gastrectomy.
4-They must eat small, frequent meals because of the dumping syndrome. Dumping syndrome
occurs due to:
A-Rapid absorption of glucose from the intestine and the resulted hyperglycaemia and abrupt
rise in insulin secretion will cause in turn hypoglycaemic symptoms about 2 hours after a meal.
B-Rapid entry of hyper osmotic meals to the intestine, this provokes the movement of so much
water into the gut and this will cause hypovolaemia and hypotension.

20
PANCREAS
Another part of the GI that is present outside the GI but connected to it by a duct. The pancreas
has two components
1- Endocrine: produces hormones such as insulin, glucagon.
2- Exocrine: produces several digestive enzymes that help in the digestion of protein, fat and
carbohydrates (CHO). The enzymes are secreted by the acini of the pancreas.
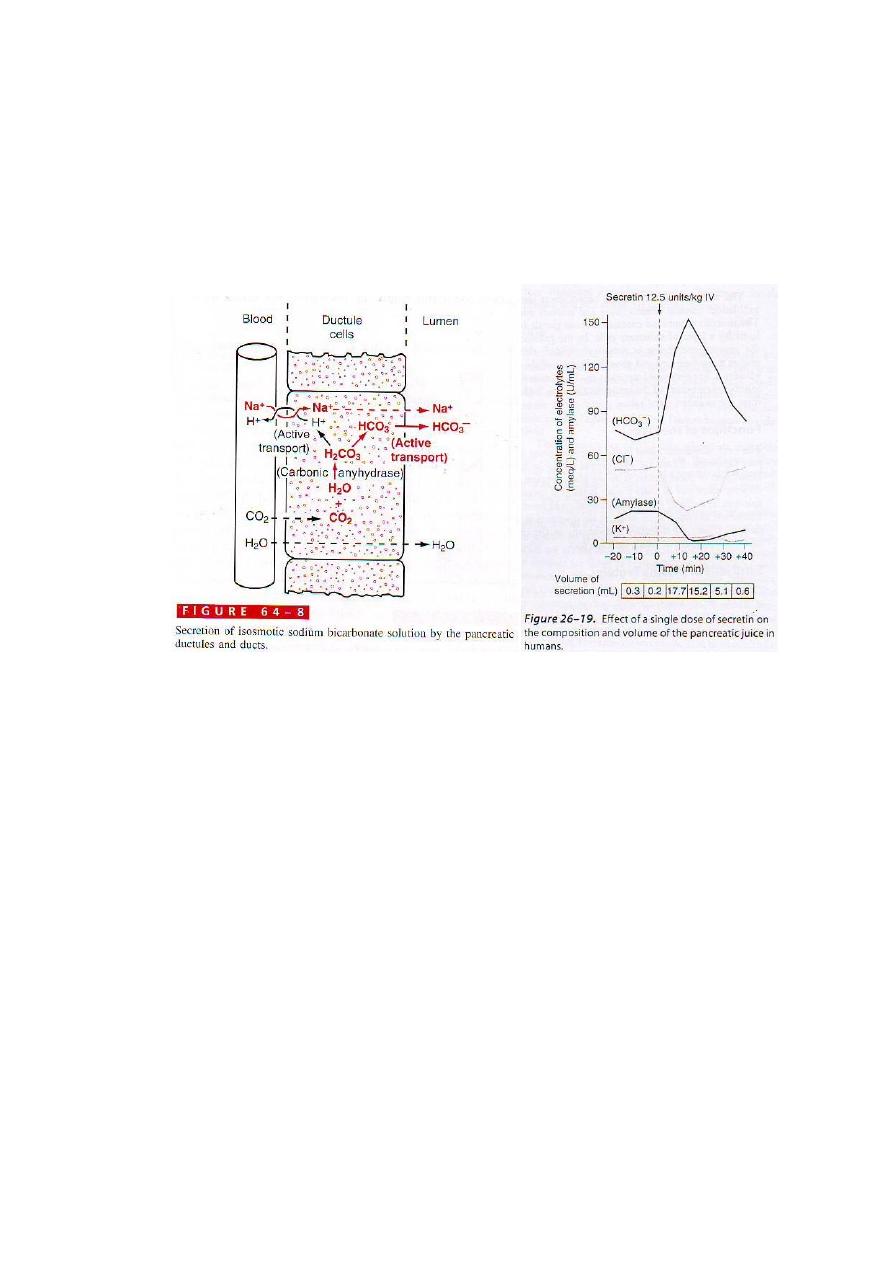
In addition the epithelial cells lining the ducts will secret an electrolyte solution that
contains large amounts of water and bicarbonate ions which is important in neutralizing
the acid chyme emptied by the stomach, into the small intestine. Thus the alkaline
pancreatic secretion as well as bile and intestinal juice which are also neutral or alkaline
will raise the PH of the duodenal contents to 6-7.
Composition of the pancreatic juice:
The volume is 1-1.5 liter per day.
PH is 8
It contains water and different electrolyte - CATIONS (Na⁺, K⁺, Ca⁺⁺, Mg⁺⁺)
- ANIONS (HCO
3⁻
, Cl⁻, SO4
⁼,
HPO4
⁼
)
The organic constituents: different digestive enzymes for the digestion of protein, fat and
CHO.
Protein digesting enzymes:
1- Trypsin.
2- Chymotrypsin.
3- Elastase.
4- Carboxypeptidase.
These enzymes are secreted from the pancreas in an inactive form. Thus trypsin is
secreted as trypsinogen, chymotrypsin as chymotrypsinogen, elastase as proelastase, and
carboxypeptidase as procarboxypeptidase.
These enzymes will become activated only after they are secreted into the intestinal tract
and not while they are present in the pancreas. Trypsinogen is activated by an enzyme
called enterokinase or enteropeptidase secreted by the intestinal mucosa when chyme
comes in contact with mucosa. Enterokinase will convert the inactive trypsinogen into
active trypsin. The active trypsin can also activate trypsinogen into trypsin. Thus once
trypsin is formed it can cause autocatalytic chain reaction by which more trypsinogen is
activated into trypsin. Trypsin will also activate chymotrypsinogen into chymotrypsin,
procarboxypeptidase into carboxypeptidase, and proelastase into elastase.
Trypsin and chymotrypsin will digest whole or partially digested protein into peptide
level.
Carboxypeptidase will digest peptides into amino acids. Elastase will act on the protein
elastin found in yellow connective tissue such as in ligaments.

21
Enzymes for the digestion of nucleic acids:
5-
Ribonuclease:
which acts on RNA.
6-
Deoxyribonuclease:
which acts on DNA.
Enzymes for the digestion of carbohydrates:
7- α-amylase:
the pancreas secrets an α-amylase similar to that of salivary secretion. It
splits starches and glycogen into disaccharides such as maltose and isomaltose.
Fat splitting enzymes:
8-
Lipase.
9-
Bile salts-activated lipase:
In adults pancreatic lipase is 10 to 60 times more active,
but unlike pancreatic lipase, bile salt-activated lipase catalysis the hydrolysis of
cholesterol esters, fat soluble vitamins and phospholipids as well as triglycerides. A
very similar enzyme is found in human milk.
10-
Procolipase (colipase):
it is secreted from the pancreas as procolipse (inactive form)
and activated into active form by trypsin. Colipase is a protein that binds to the
surface of the fat droplet displacing the emulsifying agents and anchoring lipase to the
droplet, because lipase cannot act on the fat droplets covered by emulsifying agents
without colipase.
11-
Cholesterol ester hydrolase.
12-
Phospholipase A2
secreted as inactive form (prophospholipase A2) and activated by
trypsin into phospholipase A2, phospholipase A2 acts on lecithin and normally causes
complete hydrolysis of lecithin. In acute pancreatitis prophospholipase A2 is activated
inside the pancreas and the active enzyme will cause partial digestion of lecithin into
lysolecithin and a fatty acid. Lysolecithin has a damaging effect on cell membrane and
causes damage of the pancreatic tissue and necrosis of the surrounding fat.
13-
Trypsin inhibitor:
This substance is secreted by the same cells that secrete the
proteolytic enzymes and at the same time. It surrounds the enzyme granules and
prevents its activation both inside the acini or the ducts of the pancreas. In the small
intestine it will be diluted and loss its effect.
Q: why the pancreas does not digest itself?
A: 1- The enzymes are secreted in an inactive form.
2- Trypsin inhibitor.
3- Flow (no stagnation). The amount of enzyme secreted will flow, if there is any
blockage in the ducts then the autocatalytic cycle will start in the pancreas which leads to
pancreatitis and the result will be the digestion of the pancreas by its own enzymes.
22
One of The main causes of acute pancreatitis is obstruction of papilla of vater by a gall
stone. This blocks the pancreatic duct and also the common bile duct, therefore large
quantities of pancreatic enzymes accumulate in the pancreatic tissue and will eventually
overcome the trypsin inhibitor in the secretion and thus a small amount of trypsinogen
will be activated into trypsin and this in turn will activate more trypsinogen and the other
proteolytic enzymes and also will activate prophospholipase A2, and the result will be the
digestion of the pancreas.
DEFICIENCY OF PANCREATIC ENZYMES:
This occurs after chronic pancreatitis or damage to the pancreas. If effects mainly the
digestion of fat. Protein digestion will also be effected and thus protein loss will be
significant. However carbohydrates digestion is little effected. So deficiency of pancreatic
lipase will result in deficiency in the digestion of fat → this will lead to steatorrhoea. The
stool will be bulky, pale, greasy and of bad odour and floats on water.
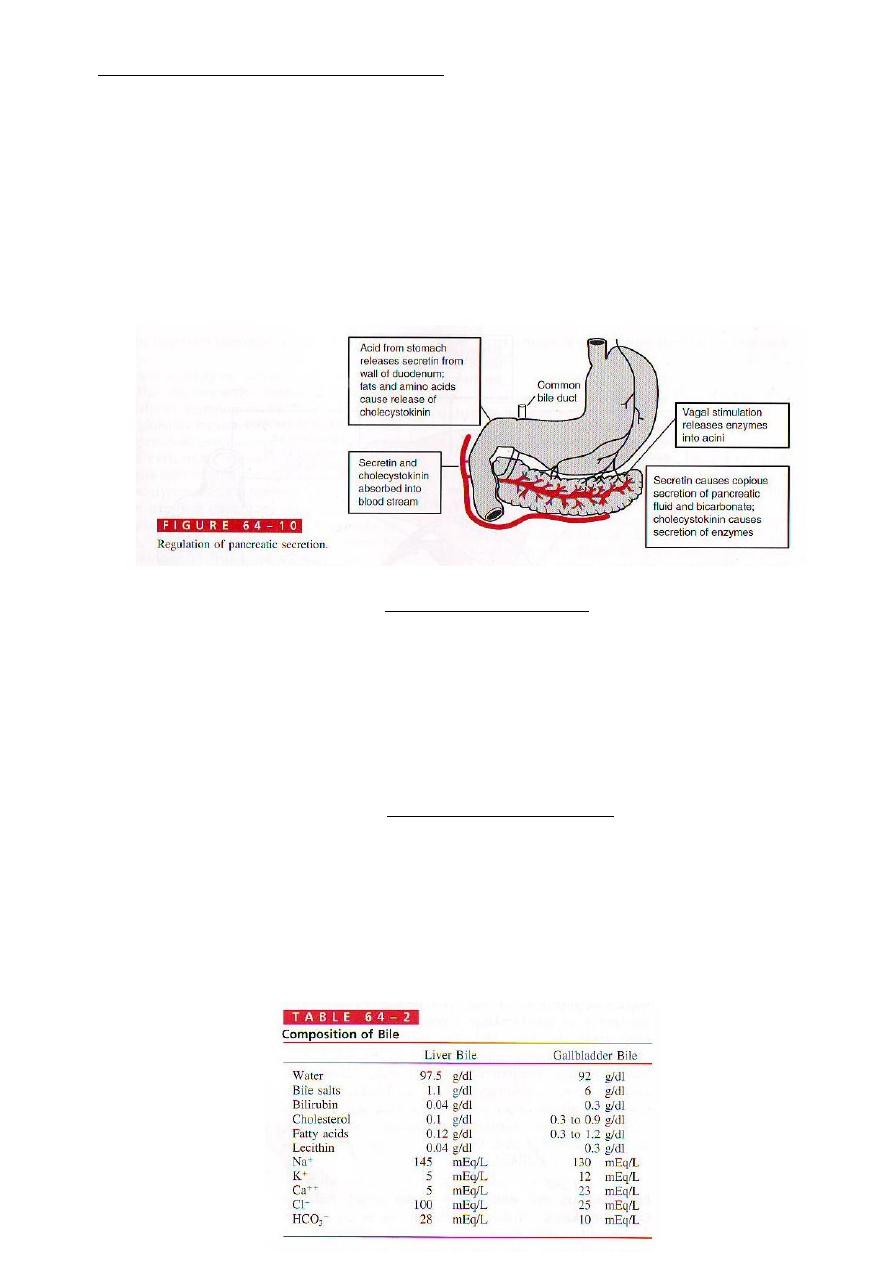
REGULATION OF PANCREATIC SECRETION:
1- Nervous by the vagus and other cholinergic nerves in the enteric nervous system.
2- Hormonal a- Cholecystokinin-pancreozymin CCK.
b- Secretin.
PHASES OF PANCREATIC SECRETION:
1- Cephalic and Gastric phase:
The same nervous signals that cause the secretion in the stomach also cause acetylcholine
release by the vagal nerve endings in the pancreas. It will cause moderate amount of
enzymes to be secreted into the pancreatic acini and ducts, so the pancreatic juice
secreted is rich in enzymes and poor in water and bicarbonate.
As the amount of water secreted is little then the pancreatic secretion to the intestine is
small because there is no fluid medium to transport the enzymes to the intestine. So most
of the enzymes are temporarily stored in the pancreas itself. This phase accounts for 20%
of the total secretion of pancreatic enzymes after a meal.
2- Intestinal phase:
After the chyme enters the small intestine, it will cause copious secretion mainly in
response to secretin. Also CCK causes more increase in the secretion of enzymes.
SECRETIN:
Secretin is present in the mucosa of the upper small intestine and it’s
secreted when chyme enters the intestine. The most important factor in chyme that
causes the release of secretin is:
23
ACID→
hydrochloric acid → causes release of secretin → absorbed by blood → to the
pancreas.
Secretin causes copious secretion of pancreatic juice that contains little enzymes and
chloride ions. Secretin acts on the epithelial cells lining of the small ducts and not on the
acinar cells (that secrete the enzymes) and the duct cells will secrete water and
bicarbonate ions thus the response of the pancreas to secretin is a watery, alkaline juice
poor in enzymes and chloride.
Importance of the secretin mechanism:
1- Secretin is released in large quantities from the mucosa of the small intestine
whenever the PH of the duodenal contents falls below 4.5-5. This will cause the
secretion of large amounts of watery-alkaline pancreatic juice which will neutralize the
acid in the duodenum.
HCL + NaHCO
3
→ NaCl + H
2
CO
3
The carbonic acid will then dissociate into CO
2
+ H
2
O and CO
2
will be absorbed by blood
and expired through the lungs leaving a neutral solution of NaCl in the duodenum. Thus:
a- Excessive acidity is neutralized.
b- Peptic activity of gastric juice is stopped.
This is a protective mechanism against the development of peptic ulcer in the
duodenum.
2- The bicarbonate ions will provide a suitable PH for the action of the pancreatic
enzymes, since all these enzymes act optimally in a slightly alkaline or neutral medium
at a PH of 7-8.
3- Secretin will also provide the fluid medium to wash out the enzymes that are secreted
into the acini without large accompanying osmotic equivalent of water.
24
CHOLECYSTOKININ-PANCREOZYMIN (CCK):
This hormone is released from the mucosa of the upper small intestine in response to
fat and partial byproducts of protein digestion such as proteoses and peptones and also to
a lesser extent in response to acid (HCL). CCK when released will be absorbed by the blood
and then will go to the pancreas to cause the secretion of pancreatic juice rich in enzymes
but poor in water and bicarbonate. this effect similar to vagal nerve stimulation but even
more pronounced, however vagal stimulation of pancreatic secretion is blocked by
atropine while that of CCK is not blocked by atropine.
CCK accounts for about 70-80% of the total secretion of pancreatic digestive enzymes after
a meal.
SECRETION OF BILE
Bile serves two important functions:
1- Very important for the digestion and absorption of fat although it does not contain
any digestive enzymes.
2- Bile serves as a mean for excretion of several waste products from blood e.g.
bilirubin (end product of haemoglobin destruction) and excess of cholesterol.
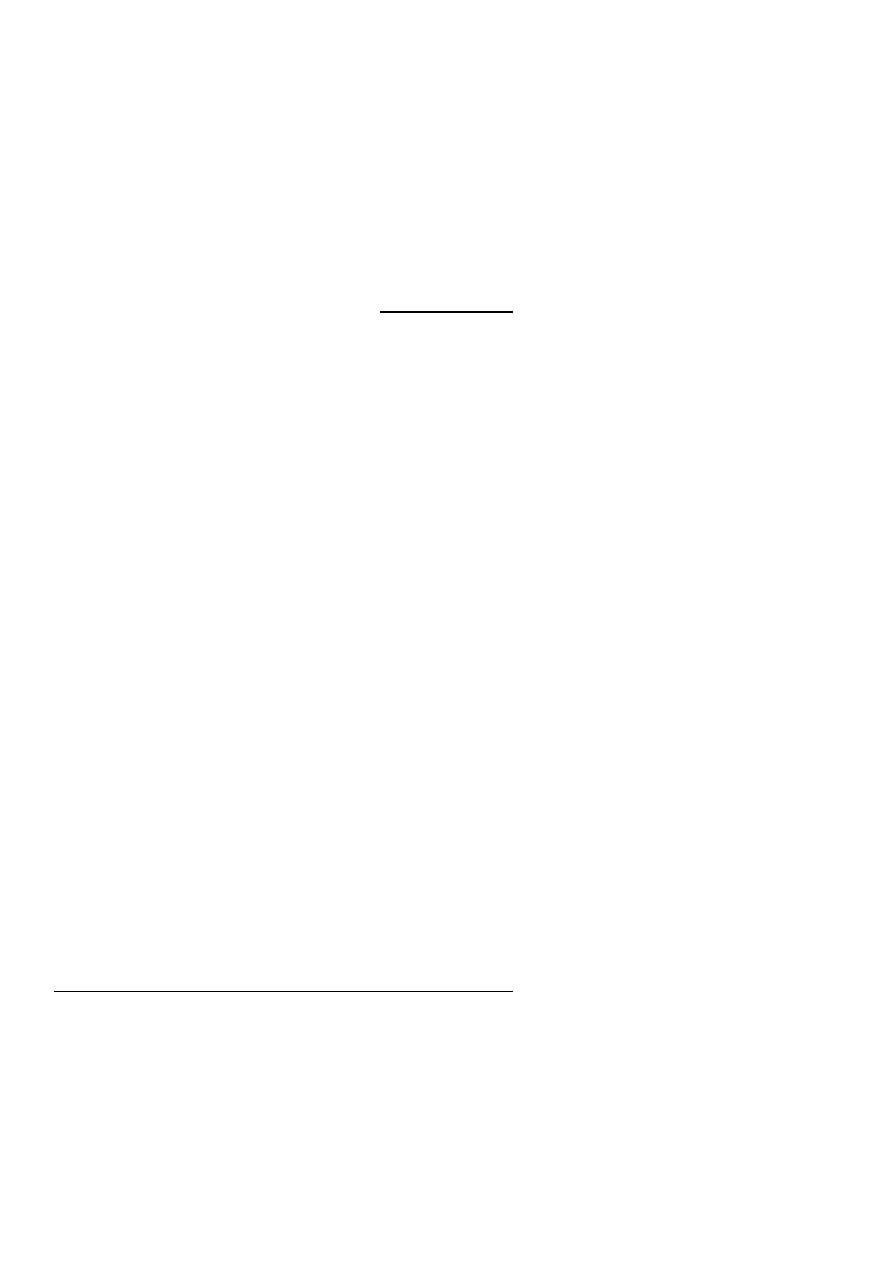
COMPOSITION OF BILE
The daily secretion of bile from the liver is 500-1000 ml. however the gall bladder
has the capacity of 40-50 mills only so the hepatic bile is concentrated in the gall
bladder by the absorption of water and electrolytes. So we have two types of bile:
1- Hepatic bile → secreted by the liver.
2- Gall bladder bile → which is the hepatic bile that has been stored and
concentrated by the gall bladder.
25
PH of the hepatic bile 7.8-8.6
PH of gall bladder bile 7-7.4 more acidic.
In the gall bladder bile will be concentrated about 5 -10 times.
So in the gall bladder water and electrolytes will be absorbed while other
constituents especially calcium, bile salts, lipid substances, cholesterol and lecithin
are not reabsorbed, and therefore become highly concentrated in the gall bladder.
BILE SALTS
These are the sodium and potassium salts of bile acids. The bile acids are formed by the liver
cells from cholesterol. The human bile contains 4 types of bile acids and these are:
1- Cholic acid 50%.
2- Chenodeoxycholic acid 30%.
These 2 are formed by the liver cells and are the primary bile acids.
3- Deoxycholic acids 15%.
4- Lithocholic acid 5%.
The last 2 are formed by the action of colonic bacteria on the primary bile acids. So Cholic acid is
converted by bacterial flora into deoxycholic acid and Chenodeoxycholic acid into lithocholic
acid. Deoxycholic acid and lithocholic acids are called secondary bile acids.
Bile acids will be conjugated in the liver with either glycine or taurine to form glycol or tauro-
conjugated acid.
Cholic acid + glycine → glycocholic acid.
+ Taurine → taurocholic acid.
Chenodeoxycholic acid + glycine → glycochenodeoxycholic acid.
+ Taurine → taurochenodeoxycholic acid.
The bile acids will form sodium and potassium salts in alkaline medium.
Main functions of bile salts in the intestinal tract:
1- Detergent function (emulsification).
Bile salts through their detergent effect will decrease the surface tension of fat particles in
the food and allow the agitation in the intestine to break the fat globules into smaller
sizes thus it will increase the total surface area of fat particles exposed to the action of the
digestive enzymes, this emulsification function is very important for the digestion of fat.

26
2- Formation of micelles.
This is a very important effect by which bile salts help in the absorption of fatty acids,
monoglycerides, cholesterol and other lipids from the intestinal tract. Bile salts will form
small complexes with lipids particles called micelles; they are highly soluble in the water
of the digestive fluid. The lipids are then ferried (transported) to the mucosa to be
absorbed. Without the presence of bile salts 40-50% of lipids are lost in the stool, and
there is important loss of fat soluble vitamins such as vitamin A, D, E, and K.
3- Activate lipases in the intestine.
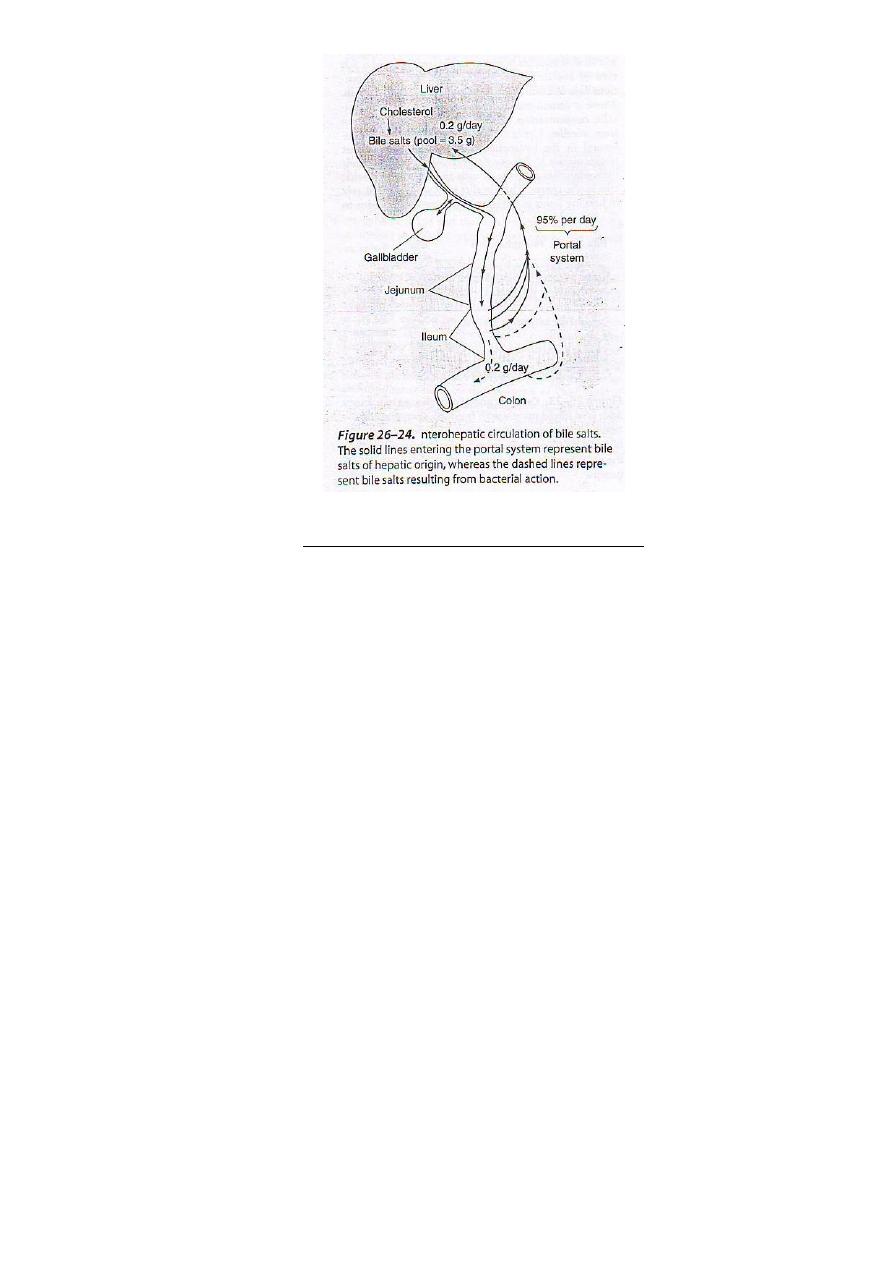
FATE OF BILE SALTS
95% of bile salts are reabsorbed from the terminal ileum through mainly active transport
process (Na+ -bile salts co transport) but some by non-ionic diffusion in upper small
intestine. Then the bile salts will enter the portal circulation → to the liver → re-secreted
again into the bile. This re-circulation of bile salts is called ENTEROHEPATIC CIRCULATION
of bile salts. Total bile salts pool which is about 3.5 grams recycles repeatedly via the
enterohepatic circulation and the entire pool recycles twice per a meal and 6-8 times per
day. The remaining 5% of the bile salts will enter the colon and will be subjected to
bacterial action of the colon; these bacteria will convert the primary bile salts to
secondary bile salts i.e. deoxycholic acid from Cholic acid and lithocholic acid from
Chenodeoxycholic acid. Deoxycholic acid is relatively soluble and will be absorbed from
the colonic mucosa to the circulation and back to the liver.
Lithocholic acid is relatively insoluble and thus will be mostly excreted in stool.
When bile salts absorption is prevented by resection or disease of the terminal ileum,
steatorrhoea can occur by interruption of the enterohepatic circulation of bile salts and
the liver cannot increase the rate of bile salt production to a sufficient degree to
compensate for the loss (0.2-0.4 grams / day).
27
REGULATION OF BILIARY SECRETION
Bile is continuously formed by the liver and is stored and concentrated by the gall bladder until it
is needed. Any agent that causes an increase in the production of bile by the hepatic cells is
called CHOLERETICS. The most important choleretic substances:
1-Bile salts: They are the most important choleretic substance. The presence of large amount of
bile salts in the blood increase the rate of liver secretion proportionately. Thus the efficient
enterohepatic circulation of bile salts will ensure a continuance of biliary secretion. So the
amount of bile salts secretion is controlled by the concentration of bile salts in the blood. The
greater the plasma concentration of bile salts, the greater is the stimulus for their secretion.
Thus between meals when there is little bile salts in the intestine and little absorbed , the
plasma concentration of bile salts is low and there is little bile salts available to be transported
into the bile ducts i.e. the enterohepatic cycling of bile salts is minimal. During a meal the higher
plasma concentration of absorbed bile salts leads to an increased rate of bile salts secretion. The
liver synthesizes new bile salts to replace the bile salts that escaped absorption in the small
intestine (0.2-0.4 grams/day). The uptake by hepatocyte of bile salts from the plasma inhibits
the synthesis of bile salts.
2-Vagal stimulation: increases the flow??
3-Secretin: increases the bile secretion. This is due mainly to the stimulation of the small bile
ducts to secret sodium bicarbonate solution, the same effect that secretin has on the pancreas.
The bicarbonate ions in the bile help to neutralize the acid in the duodenum. This electrolyte

28
solution is stimulated by secretin in response to the presence of acid in the duodenum (just like
the pancreas), so secretin does not stimulate the secretion of the bile salts by the hepatocyte.
Control of gall bladder Contraction and emptying
Substances that cause contraction of the gall bladder and expulsion of bile from the gall bladder
are called CHOLAGOGUES, for example CCK. The contraction of gall bladder is under control of
two types of control: 1- Nervous.
2- Hormonal.
The hormonal mechanism is more important.
Nervous mechanism: is by parasympathetic (vagus nerve) which causes contraction of the gall bladder
and relaxation of the sphincter of Oddi.
Hormonal mechanism: CCK is secreted from the duodenal mucosa in response mainly to fat and
byproducts of protein digestion such as proteoses and peptones and to a lesser extent to acid. CCK will
be absorbed to the blood then to the gall bladder and will cause emptying of the gall bladder
(contraction of the gall bladder and relaxation of the sphincter of Oddi).
Effect of cholecystectomy:
The periodic discharge of bile from the gall bladder helps digestion but it is not essential for it.
Cholecystectomized patients maintain good health and nutrition with a constant flow of bile into the
duodenum, although eventually bile ducts becomes dilated and more bile tends to enter the duodenum
after eating than other times.
29
SMALL INTESTINE
The small intestine consists of the duodenum, jejunum, and ileum. The small intestine is the
major site for digestion and absorption. Within the small intestine the hydrolysis of every major
type of food molecules is completed and the resulting smaller molecules are absorbed into the
circulating blood or lymph. The secretion of 2 major accessory glands, that’s to say the pancreas
and the liver enter the small intestine and help in the digestive process,. We have two types of
glandular secretions in the small intestine:
1- Brunner’s gland secretion.
2- Crypts of Lieberkühn secretion.
Both these secretions contain almost no digested enzymes. In the duodenum there are extensive
numbers of mucus secreting glands called Brunner’s glands. They are only present in the
duodenum and are located mainly in the first few cm. of the duodenum between the pylorus
and the duodenal papillae (where the bile and pancreatic juice empty in the duodenum).
Brunner’s gland secrete special type of mucus which is thick, viscid, alkaline and helps in
protecting the duodenum against the acid chyme emptied by the stomach. There is also an
appreciable secretion of HCO
3⁻
that is independent of Brunner’s gland. Decreased duodenal
HCO
3⁻
secretion may play a role in the genesis of duodenal ulcer.
The secretion of Brunner’s gland can be stimulated by:-
1- Direct tactile or irritating stimuli of the overlying mucosa.
2- Vagal stimulation.
3- Intestinal hormones: Especially secretin.
These glands are inhibited by sympathetic stimulation, and therefore sympathetic stimulation
over a long time might leave the duodenal bulb unprotected and is perhaps one of the reasons
for the development of peptic ulcer.
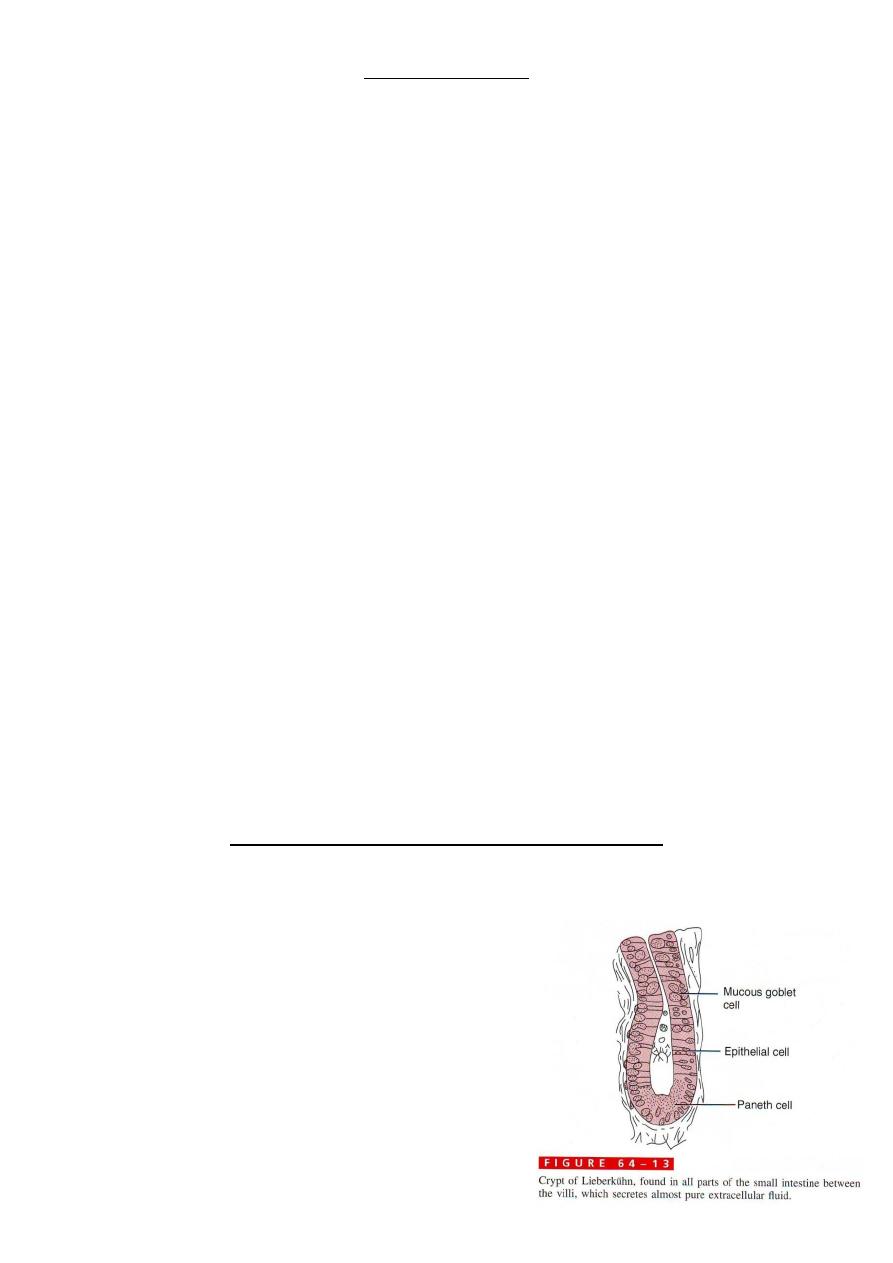
INTESTINAL GLANDS→CRYPTS OF LIEBERKüHN
Throughout the whole length of the small intestine (except the Brunner’s gland area) there are
many simple tubular intestinal glands called crypts of
Lieberkühn. The crypts are situated between the
intestinal villi. The villi are the small finger like projection
(about 1 mm. long) of the intestinal mucosa.
Crypts of Lieberkühn contain different types of cells:
1- Epithelial cells: the epithelial cells at the bottom of
the crypts are undifferentiated and these cells
undergo active mitosis. The new cells formed will
30
migrate gradually upward towards the tip of the villi to replace the cells shed or
desquamated from the tips of the villi. The lining of the small intestine is replaced in
average 3 days (2-5days) by this rapid turnover of cells. This rapid growth of new cells in
the intestinal epithelial cells will allow rapid repair of any excoriation that occurs in the
mucosa.
There is about 50-200 grams of human gastrointestinal mucosa renewed daily. The no. of cells
shed daily is about 17 billion in human and the amount protein secreted in this fashion is about
30 grams per day.
2- Goblet cells: these are mucus secreting cells. The mucus coats and protects the mucosa
and acts as a lubricant.
3- Paneth cells: these are situated at the base of the crypts. They might have an endocrine
function. Quanylin is secreted by Paneth cells. Stimulation of guanylyl cyclase increases
the concentration of intracellular cGMP→increase activity of cystic fibrosis-regulated Cl⁻
channel →increase secretion of Cl⁻ into the intestinal lumen.
Paneth cells also secrete DEFENSINS, naturally occurring peptide antibiotics that are also
secreted elsewhere in the body.
COMPOSITION OF THE INTESTINAL JUICE OR SUCCUS ENTERICUS
The crypts of Lieberkühn secrets the intestinal juice or succus entericus. This intestinal juice is
secreted at a rate of about 1-2 liters by day. It is similar to extracellular fluids and has a PH
slightly alkaline 7.5-8. The secretion is rapidly reabsorbed by the villi. The circulation of fluid
from the crypts to the villi will provide a fluid medium for the absorption of substances from the
chyme as it comes in contact with the villi.
If the secretion of small intestine is collected without cellular debris there will be almost no
enzymes except the enterokinase. If we collect any enzymes in the juice then it’s from
desquamated epithelial cells. The epithelial cells of the mucosa contain digestive enzymes on the
Brush border
of the epithelial cells. These enzymes will digest the food as they come in contact
with the microvilli prior to the absorption of the end products of digestion.
The enzymes are:-
1- Peptidases: there are several peptidases which act on peptides→ amino acids.
2- Disaccharidases: there are
-Maltase acts on maltose and gives two molecules of glucose.
-Isomaltase acts on isomaltose and gives two molecules of glucose.
-Sucrase acts on sucrose (cane sugar) to give glucose + fructose.
-Lactase acts on lactose to give glucose + galactose.
31
3- Lipase acts on triglycerides → glycerol + fatty acids.
4- Nucleases: will breakdown nucleic acids
into pentoses and purine + pyrimidine bases.
EFFEECT OF CHOLERA TOXIN ON INTESTINAL SECRETION:
Cholera toxin increases greatly the flow of fluids from the crypts of Lieberkühn especially in the
jejunum. As much as 15 liters of fluids can be lost from the bowel in the first day→ this will lead
to dehydration→ circulatory shock if not treated promptly.
Treatment by administration of large amounts of saline and glucose either intravenously or by
mouth. Cholera toxin seems to have a specific effect in increasing active transport of Cl⁻ ions into
the crypts. This will lead to massive loss of fluid into the intestinal tract.
Several other bacteria can also increase Cl⁻ transport but are much less severe, such as colon
bacillus and dysentery bacillus.
REGULATION OF SECRETION OF THE SMALL INTESTINE
1- local stimuli→ local nervous reflexes: this is the most important regulatory mechanism.
Thus local nerve reflexes initiated by various stimuli will cause the secretion of the small
intestinal juice. Of these stimuli are:-
A-Tactile B-Irritative C-Distension.
Therefore the secretion of the small intestine occurs mainly in response to chyme, the greater
amount of chyme→ the greater response.
2- hormonal regulation: some hormones that increase secretion in other parts of the
gastrointestinal tract will increase the small intestinal secretion of these hormones:
A-Secretin
B-CCK
C-VIP (vasoactive intestinal polypeptide).
Vagal stimulation has probably No effect on intestinal glands.
LARGE INTESTINE
The main function of the large intestine is to absorb water and electrolytes from the chyme, and
to store the faecal matter until it can be expelled by defaecation.
The mucosa of the large intestine contains No villi. There are crypts of Lieberkühn but they are
composed largely of goblet cells that secrete mucus. Also there are no enzymes in the epithelial
32
cells. Thus the most important secretion in the large intestine is mucus. The main functions of
mucus secreted by the large intestine are:
1- Provide an adherent medium to hold the faecal mass together.
2- Protect the mucosa against excoriation or damage, against bacterial activity inside the
faecal mass, against the acid formed deep in the faeces (PH 8 caused by large amount of
sodium bicarbonate in colonic secretion) and thus neutralize the acid formed by the
bacterial activity in the large intestine.
REGULATION OF SECRETION OF THE LARGE INTESTINE:
1- Direct tactile stimulation of the goblet cells.
2- Local nerve reflexes through the intrinsic nerve plexus to the goblet cells.
3- Parasympathetic nerve stimulation through stimulation of Nervi erigentes (pelvic
nerve). This nerve supplies the distal half of the large intestine and stimulation of this
nerve will cause marked increase in mucus secretion and also it causes an increase in
motility. Therefore during excessive parasympathetic stimulation such as after
emotional stress there might be frequent bowel motions with a large amount of ropy
mucous quality→ psychogenic or emotional diarrhea.
ABSORPTION
In the mouth and esophagus no significant absorption of food stuff occurs, although some
drugs are absorbed through the oral mucus membrane such as trinitrin, morphine and steroids.
In the stomach absorption is very limited to a small
amount of water, alcohol and aspirin. The stomach has no
villi and has tight junctions so little absorption.
The major site of absorption is the intestine and
particularly the small intestine. In the small intestine there
will be almost complete absorption of the digestive
products. In the colon absorption is confined to water and
some electrolytes such as Na⁺, K⁺, Cl⁻ and glucose;
however it cannot absorb protein, fat?? Or calcium.
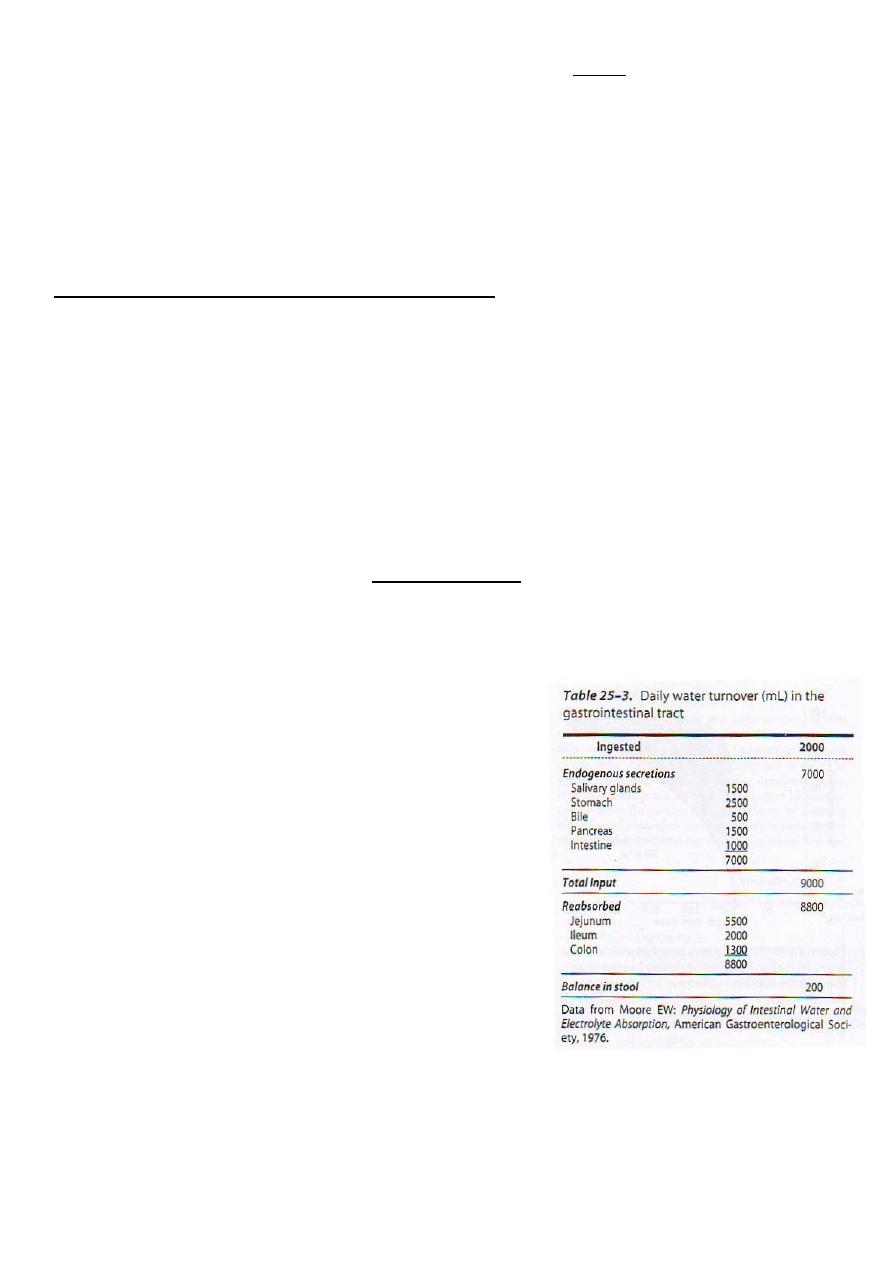
The total quantity of fluids presented to the intestine each
day is about 9 liters and is equal to ingested food(2liters)
plus that secreted in various gastrointestinal secretions (7
liters). Of this fluid about 7.5 liters are absorbed by the
small intestine and only 1-1.5 liters of fluid pass through the ileo-caecal valve to the large
intestine.
Absorption of fluid is completed in the colon so that only about 200 mills pass to the faeces.

33
THE INTESTINAL VILLI
(THE ABSORPTIVE SURFACE OF THE INTESTINAL MUCOSA)
There are many folds in the intestinal mucosa called VALVULAE CONNIVENTES which increase
the surface area of the absorptive mucosa to about 3
folds.
Over the entire surface of the mucus membranes of
the small intestine, there are about 5 millions of small
finger-like projections called villi. The presence of
these villi will increase the mucosal absorptive area
by about 10 folds. Each villus is 1 mm long and is
covered by a single layer of columnar epithelium and
contains an artery, vein and central lacteal. The
vascular system is for the absorption of fluid and
dissolved materials into the portal blood, while the
central lacteal is for the absorption of lipids materials
into the lymphatic system.
The free edge of intestinal epithelial cells is
characterized by the presence of BRUSH BORDER consisting of about 600-1000 microvilli. The
microvilli increase the absorptive area at least by 20 folds. Thus the absorptive area of the small
intestine is increased by about 600 folds by the valvulae conniventes, villi and microvilli. The
total area of the mucosa is about 250 square meters for the entire small intestine, about the
surface area of a tennis court.
STRUCTURE OF THE CELL MEMBRANE
Cell membrane is a very thin structure composed almost entirely of protein and lipids (only 3%
of CHO). The lipid layer of the cell membrane makes the membrane very permeable to lipid
soluble substances such as O
2,
CO
2,
alcohol, fatty acids, phospholipids and cholesterol. While it is
impermeable to water soluble substances such as ions, glucose and urea. However the cell
membrane contains many pores so substances that have a small size will pass through these
pores such as water and urea molecules.
Basic mechanisms of absorption:
1- Diffusion: means the transport of substances through the membrane as a result of electrical
or chemical gradient. This process is passive and does not require energy. Diffusion can be:
34
a) Diffusion through the lipid layer: if the substance is soluble in the lipid layer of the cell
membrane, then it will diffuse through the cell membrane e.g. O
2
, CO
2
, alcohol, fatty
acids, cholesterol and phospholipids.
b) Facilitated diffusion: some substances are very insoluble in lipid; however they can pass
the lipid matrix or layer by a process called facilitated diffusion. This is how some of the
sugars pass through the membrane. The substance will combine with a carrier substance
at the outer surface of the membrane and this combination is soluble in the lipid, so that
it can diffuse to the other side of the membrane where the substance will break away
from the carrier and passes to the inside of the cell. Thus the carrier will make the
substance soluble in lipid.
c) Diffusion through the membrane pores: some lipid insoluble substances can pass through
the cell membrane pores. Substances with molecules of small size can diffuse through
these pores. Of these substances water, urea and chloride ions.
2-Active transport: the substance is transported against an electrical or chemical (concentration)
gradient. This mechanism requires the expenditure of energy and carriers.
3-Pinocytosis: this occurs when some substances with large molecular weight such as proteins
can enter the cell. Pinocytosis is similar to phagocytosis. An invagination occurs in the cell
membrane that will surround and then completely envelope or close over the material to be
ingested. Thereafter the membrane breaks away from the surface of the cell forming a pinocytic
vesicle that will enter the cytoplasm.
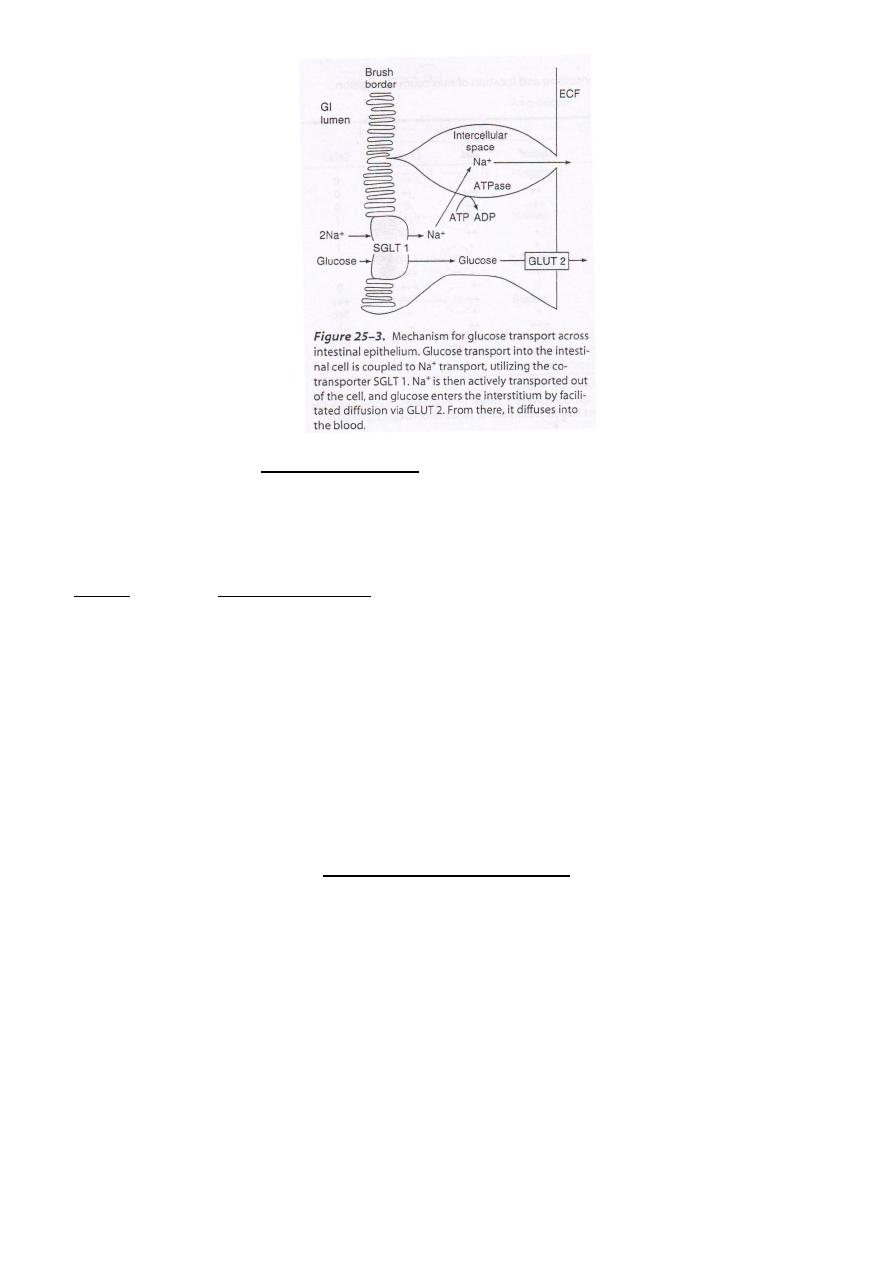
ABSORPTION OF CARBOHYDRATES
Almost all the CHO are absorbed in the form monosaccharides and little as disaccharides and
non as large carbohydrates compounds. Most of the monosaccharides absorption occurs by
active transport and particularly for glucose and galactose; Fructose is absorbed by facilitated
diffusion. Very little absorption of monosaccharides occurs by simple diffusion through the
pores.
The transport of galactose and glucose is affected by the amount of sodium ions in the intestinal
lumen. A high sodium ion contents will increase absorption, while low sodium ion contents will
inhibit it. The reason for this is that the carrier for the transport of glucose (and this applies also
to galactose) has a receptor sites for both glucose molecules and sodium ions and the carrier will
not transport either of these to the interior of the epithelial cells until both receptor sites are
filled at the same time. This is the physiological bases for the treatment of Na⁺ and water loss in
diarrhea by oral administration of solution containing NaCl and glucose. This treatment is also
useful in the treatment of cholera.
35
Fructose absorption is by facilitated diffusion. It is independent of sodium ions and utilizes a
different carrier and does not require energy for its transport.
Deficiency either inherited or acquired of disaccharidases which digest disaccharides into
monosaccharides will lead to malabsorption of the corresponding sugar. For example deficiency
in lactase will cause intolerance to milk which contains lactose. The patient will develop diarrhea
after the ingestion of milk. The diarrhea is caused by the presence of large amount of
osmotically active molecules that remain in the intestinal lumen, and this in turn will cause
osmosis of water to the lumen and thus the volume of intestinal contents will increase. In
addition the fermentation of the disaccharides by the colonic bacteria will result in distension
and flatulence. The problem of milk intolerance can be relieved by administration of commercial
lactase preparations but this is expensive. Yogurt is better tolerated than milk in intolerant
patients because it contains its own lactase.
ABSORPTION OF PROTEIN
Some of the proteins that are absorbed every day are exogenous (supplied by the diet) which is
about 50%. And some endogenous i.e. protein contained in gastrointestinal secretions 25%, and
the desquamated epithelial cells of the gut 25%.
The proteins are absorbed in the form of amino acids, although some might be absorbed as
dipeptides and tripeptides. Very small amounts of whole protein can sometimes be absorbed by
Pinocytosis which is not the usual absorptive mechanism.
There are at least 7 different transport systems to transport amino acids into the enterocyte. 5
of them require Na⁺ and co transport amino acids and Na⁺ similar to the co transport of Na⁺ and

36
glucose. In two systems transport is independent of Na⁺. Separate system transport di and tri
peptides. Very small amounts of whole protein can be absorbed by Pinocytosis and particularly
in infants. The absorption of protein antibodies from the mother colostrum by the new born
child can be explained by this process (colostrum contributes to passive immunity against
infection). In addition, the absorption of some proteins which act as antigen and provoke the
formation of antibodies in the body can be explained by this mechanism. The protein is antigenic
(that’s to say they stimulate an immunological response) only if it is in the form a relatively large
molecule. The digestion of the protein will destroy its antigenicity. Thus for a protein to produce
an immunological response it must be absorbed as large molecule and this occur most probably
by Pinocytosis.
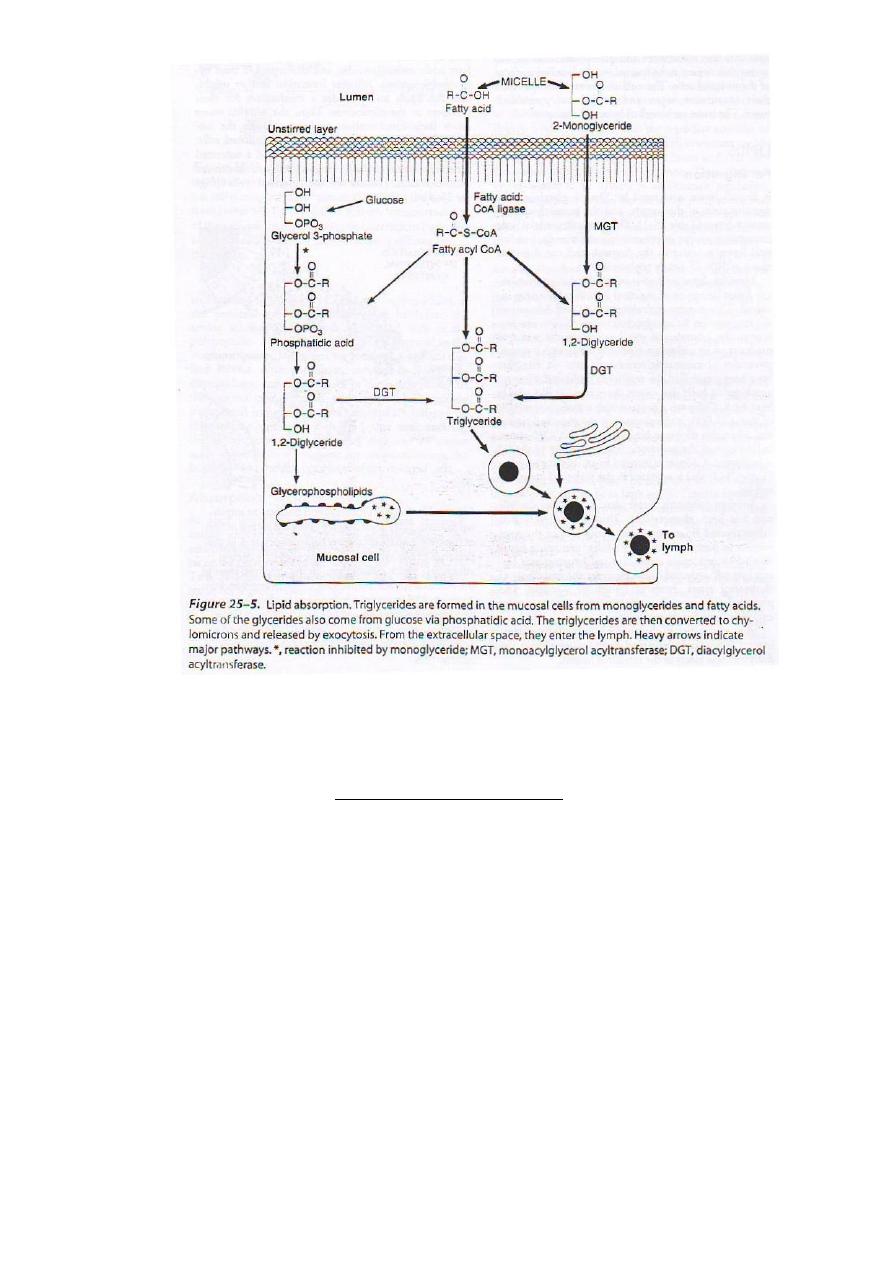
ABSORPTION OF FAT
The monoglycerides, cholesterol, fatty acids are absorbed by passive diffusion through the lipid
matrix of cell membrane. However there is some evidence that carriers are involved. The
monoglycerides cholesterol and fatty acids will interact with bile salts to form micelles and in
this way the lipids are turned soluble in intestinal fluids and the micelles formation will provide
a way for transporting these lipids to the mucosal cells. When the micelles reach the brush
border of the mucosal cells, the lipids will diffuse out of the micelles to enter the cells by passive
diffusion. Most of the monoglycerides during entry into the epithelial cells will be further
digested into glycerol and fatty acids by an epithelial cell lipase.
FATE OF FATTY ACIDS:
The subsequent fate of fatty acids depends on their size:
1- If the fatty acid contains less than 10-12 carbon atoms (short and medium chain fatty
acids) → then it will be transported to the portal blood. Thus it will not be re-esterified
into triglycerides.
2- If it is a long chain fatty acid (with more than 10-12 carbon atoms) then it will be re-
esterified into triglycerides by the smooth endoplasmic reticulum of the mucosal cells.
Some of the absorbed cholesterol is esterified. The triglycerides and cholesterol esters are
then coated with a layer of protein, cholesterol and phospholipids to form
CHYLOMICRONS which leave the cell by exocytosis to enter the lymphatic. 80-90% of all
fat absorbed from the gut is by this way i.e. as chylomicrons.
The protein coat → is ß lipoprotein which is essential for cellular exocytosis of the
chylomicrons to occur, because this protein provides a mean for attaching the fatty
globule to the cell membrane, before it is extruded. In genetic deficiency of ß lipoprotein,
the epithelial cells become engorged with fatty products that cannot precede the rest of
the way to be absorbed.
37
ABSORPTION OF WATER
Water can move in and out of the intestine entirely by diffusion following the osmotic pressure,
so that the chyme becomes is osmotic with plasma. Thus if the duodenal chyme is hypotonic,
then water will be absorbed by the intestinal mucosa until the chyme becomes iso osmotic with
plasma. If the chyme is hypertonic (particularly in the duodenum) then water will be transferred
to it to make it iso osmotic with plasma. Therefore the chyme will be iso osmotic with plasma
throughout its whole passage through the small and large intestine. As dissolved substances are
absorbed from the chyme into the blood, then an iso osmotic equivalent of water is absorbed in
order to maintain the osmolality of the chyme.

38
ABSORPTION OF ELECTROLYTES
Sodium ions (Na⁺)
The basic mechanism for sodium absorption is by the secondary active transport of sodium from
inside the epithelial cells through the side walls of
these cells into the paracellular space. This active
transport will result in lowering the sodium
concentration inside the cell to a lower value than
that in chyme (50 mEq/liter inside the cell and 142
mEq/liter in the chyme). This will result in diffusion
of sodium from the chyme into the epithelial cell
cytoplasm. This will replace the sodium that has
been actively transported out of the epithelial cells
into the paracellular space. Sodium plays an
important role in the absorption of sugars and
amino acids. 20-30 grams of sodium are secreted into intestinal secretion each day. In addition
the person eats 5-8 grams of sodium daily. So the intestine absorbs 25-35 gram of sodium each
day which is about 1/7 of all the sodium that is present of the body. Thus if the intestinal
secretions are lost to the outside such as in severe diarrhea → then the sodium reserves of the
body can be depleted to a lethal level within hours. Normally this sodium is secreted and re-
absorbed continuously with only 1mEq lost in the faeces each day.
Chloride ions (Cl⁻)
In the upper small intestine chloride is absorbed by passive diffusion mainly following the
movement of sodium ions. In the distal part of the ileum and in the large intestine, chloride is
absorbed actively. This is coupled to active secretion of bicarbonate ions. The secretion of
bicarbonate is important in neutralizing the acidic product formed by bacteria in the large
intestine.
Potassium ions (K⁺)
Transport of potassium ions is believed to be passive by diffusion following potential
differences. However sometimes it can be active.
Calcium ions (
Ca⁺⁺
)
Is mainly absorbed actively and the absorption is controlled by vit D and parathyroid hormone.
The parathyroid hormone will activate vit D in the kidney and the activated vit D in turn will
increase Calcium absorption, this is because the activated vit D will induce the synthesis of a
calcium binding protein in the mucosal cells.
39
Generally speaking, the monovalent ions are absorbed with ease and in great quantity while
bivalent ions are normally absorbed in only small amounts. For instance the max. Absorption of
calcium ions is only 1/50 as great as the normal absorption of sodium ions. However only small
quantities of bivalent ions are normally needed by the body.
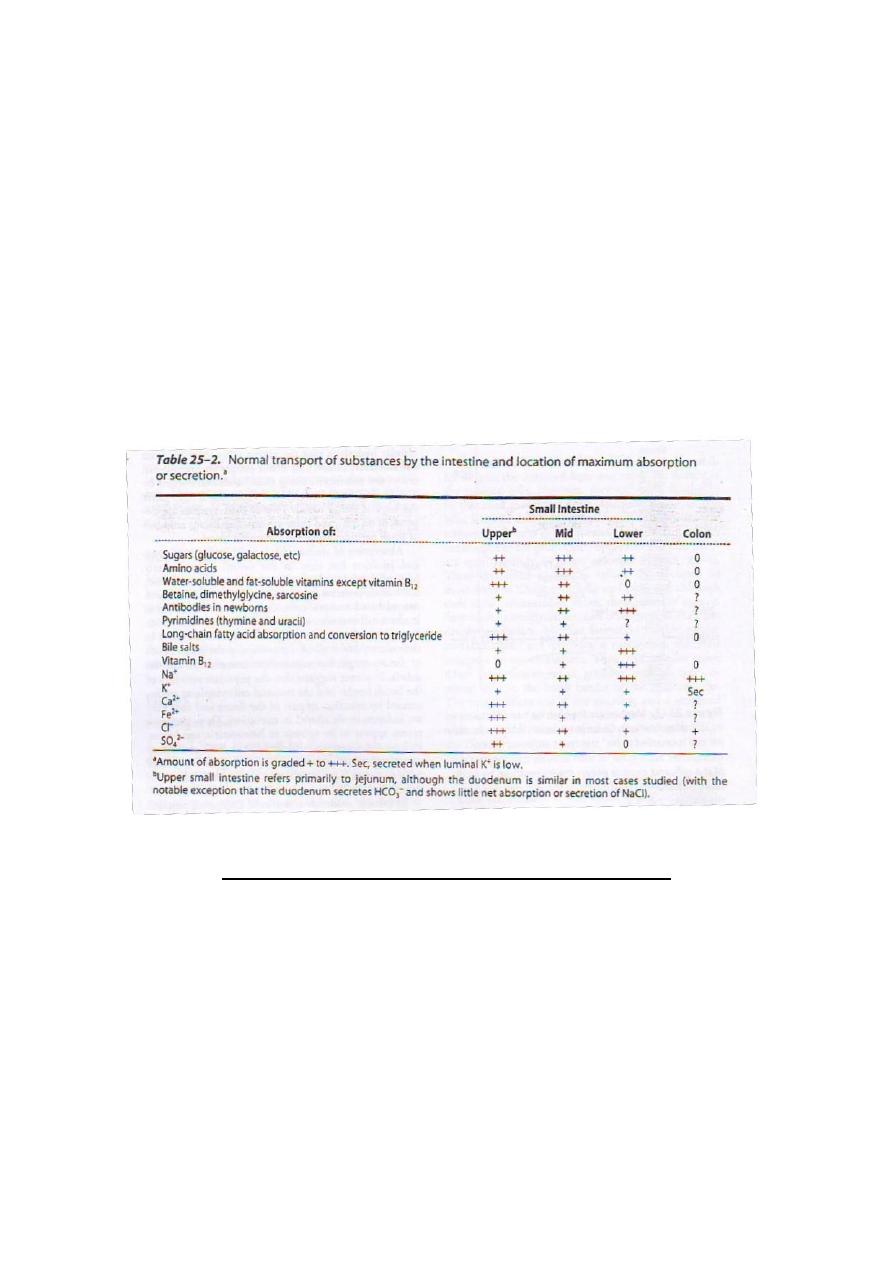
SITE OF ABSORPTION OF MAJOR NUTRIENTS:
Iron and calcium absorbed primarily in duodenum. The jejunum is the major site of absorption of
fat, sugars, amino acids, folic acid and bulk of water and electrolytes.
Bile salts re-absorbed across ileal mucosa by active transport process. The ileum is also the site
where vit B12 is absorbed. Site of absorption is not absolutely specific for individual nutrients and
in health, functional reserve of the small intestine is great with exception of specific site of vit B12
and bile salts absorption in the terminal ileum.
REGULATION OF GASTROINTESTINAL FUNCTION
Some of the mechanisms that regulate the gastrointestinal functions depend on:
1- Intrinsic properties of intestinal smooth muscles.
2- Nervous A-Extrinsic.
- Parasympathetic
- Sympathetic
B-Intrinsic
-Auerbach or myenteric plexus
-Meissner’s or sub mucosal plexus
3- Hormones.
40
ELECTRICAL ACTIVITY OF THE G.I. SMOOTH MUSCLES:
The smooth muscle of the G.I. tract is excited by almost continual slow intrinsic electrical
activity along the membranes of the muscle fibers. This activity has two basic types of
electrical waves.
1- Slow waves
2- Spikes.
SLOW WAVES: these waves are slow undulating changes in the resting membrane
potential. Their intensity ranges between
5-15 mille volts, and their frequency range
between 3-12 per minute (3 in the body of
the stomach and 12 in the duodenum).
The cause of the slow waves is unknown
→ might result from slow undulation of
the pumping activity of sodium-potassium
pump. The slow waves do not by
themselves cause muscle contractions,
but they mainly control the appearance of
intermittent spike potentials and the
spike potentials in turn actually excite
most of muscle contractions.
SPIKE POTENTIALS: they are true action potentials. They occur automatically when the
resting membrane potential of the G.I. smooth muscle becomes more positive than about
-40 mille volt (normal resting membrane potential of the gut is -50 to -60 mille volt). Thus
each time the peaks of the slow waves rises temporarily above -40 mille volt level
(becomes less negative than -40 mille volt), spike potentials appear on peaks. The higher
the slow wave potential rises above this level, the greater the frequency of spike
potentials (1-10 spikes per second). The slow waves do not cause muscle contraction by
themselves, but the spike potentials generated at the peak of the slow waves, cause most
of the contraction.
Q: why?
Smooth muscle contractions occur in response to entry of calcium ions into the muscle
fibers. The slow waves do not cause calcium ions to enter the smooth muscle → cause no
muscle contraction. Spike potentials causes large quantities of calcium ions to enter the
fibers → causes muscle contraction.
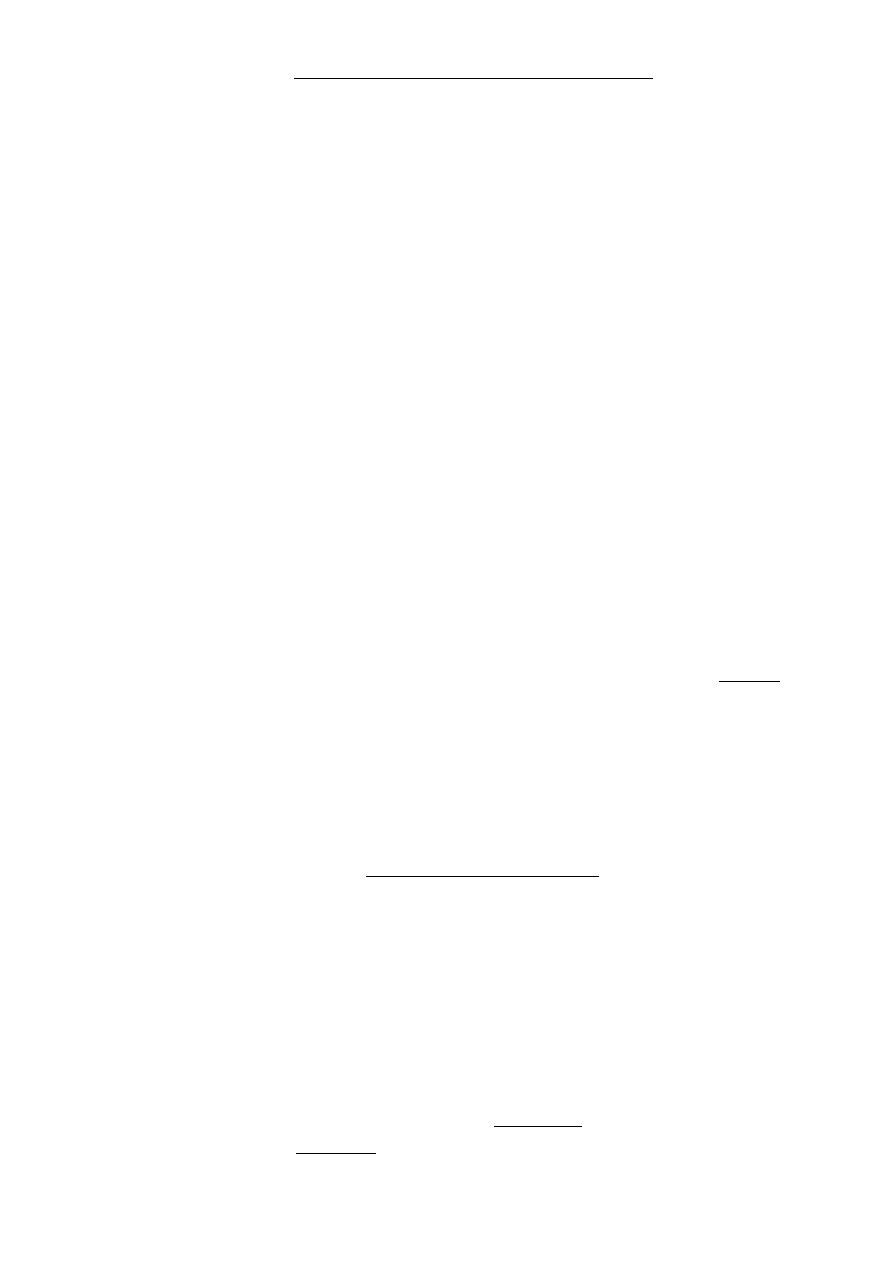
41
AUTONOMIC INNERVATION (extrinsic)
A) Parasympathetic innervation:
Come from the cranial and sacral divisions. The cranial division is through the vagus which is
the main parasympathetic nerve supply to the gut. The parasympathetic nerve supply in the
vagus provides extensive innervations to the oesophagus, stomach, pancreas and first half of
the large intestine. But to a lesser extent to the small intestine. The sacral outflow is through
the pelvic or Nervi erigentes and comes from 2, 3, 4
th
sacral segments of the spinal cord. It
supplies the distal half of the large intestine. The preganglionic parasympathetic nerves will
end on ganglion cells in the enteric plexus (Meissner and Auerbach). The post ganglionic fibers
will pass then to the muscles of the muscular coat and to the muscularis mucosae to control
contraction of the smooth muscles. Some fibers pass to the secretory cells to control secretion
of mucus or different juices. Stimulation of parasympathetic nerves generally speaking
increase the activity of the gastrointestinal tract i.e. increases the motility and increases the
secretion.
B) Sympathetic innervation:
Sympathetic outflow which originates from the thoraco-lumbar part of the spinal cord. The
preganglionic fibers after leaving the cord will end in the celiac and various mesenteric ganglia.
From there the post ganglionic fibers will pass to all parts of the G.I. tract. Some post
ganglionic fibers will end on the myenteric plexus of Auerbach’s to inhibit its activity. In
addition to these axons, other postganglionic sympathetic fibers pass to the circular and
longitudinal muscle to produce relaxation. There are also some fibers going to the blood
vessels to cause vasoconstriction. Some fibers pass to the Meissner plexus to inhibit its
activity. Thus generally speaking stimulation of the sympathetic nervous system inhibits
activity in the G.I. tract causing an opposite effect for that of the parasympathetic stimulation.
This inhibition is carried out by two ways:
1- Direct inhibitory effect of nor-epinephrine on the smooth muscle (except the muscularis
mucosae which it excites).
2- By inhibiting the neurons of the enteric nervous plexus.
INTRINSIC INNERVATION
The whole gut from the oesophagus to the anus is supplied by intrinsic nerves which
consist of two plexuses.
A) Meissner’s plexus in the submucosa.
B) Auebach’s or myenteric plexus. In between the circular and longitudinal muscle layer
of the muscular coat.
Together these plexuses are called
ENTERIC PLEXUSES. T
hese plexuses are composed
of groups of ganglionic cells interconnected by a network of fibers. This system control
most gastrointestinal functions and particularly movement and secretion. Auerbach’s
plexuses control mainly the gastrointestinal movement, while the Meissner’s plexus
controls mainly the secretion, and also has many sensory functions. The intrinsic
42
nervous system is responsible for many neurogenic reflexes that occur locally in the
gut, such as reflexes from the mucosal epithelium to increase the activity of the gut
muscles or to cause localized secretion of digestive juice by the gastrointestinal glands.
The enteric nervous system, some investigators add to the sympathetic and
parasympathetic divisions as a third division of the autonomic nervous system. There
are about 100 million neurons in this system. They contain not only Ach and nor-
epinephrine but other mediators.
Mediators:
1- Ach.
2- Nor-epinephrine.
3- Nitric oxide (NO).
4- Carbon monoxide (CO).
5- Vasoactive intestinal polypeptide (VIP).
6- Serotonin.
7- CCK.
8- Enkephalin.
9- ATP.
10- GRP.
11- Neuropeptide y.
12- Peptide yy.
13- Neurotensin.
14- Somatostatin.
15- Substance P
16- Endothelin -2. e.t.c………..
The way the peptides- secreting and other neurons interact to regulate G.I. function is unsettled.
However coordinated motor activity occurs in the total absence of extrinsic innervation and it is
clear that this is mediated by intrinsic neurons. It also plays a role in regulating secretion.
HORMONAL CONTROL
There are two major families of gut hormones according to their chemical structure.
1- Gastrin family which includes GASTRIN and CCK.
2- Secretin family which includes SECRETIN, GLUCAGON, GLICENTIN (GLI), VIP, GIP.
Other hormones include Motilin, substance P, Bombesin (GRP), Somatostatin,
Neurotensin, e.t.c………
GASTROINTESTINAL MOTILITY:
Smooth muscle of the gut exhibits two types of movements
1- Tonic contraction.
2- Rhythmic contraction.
1) Tonic contraction: is continuous contraction lasting for minutes or hours and increasing or
decreasing in intensity but the contraction is on. The intensity of tonic contraction in each
segment of the gut determines the amount of steady pressure in the segment. Tonic

43
contractions of the sphincters will determine the amount of resistance offered by the
sphincters to the movement of intestinal contents. Examples of tonic contractions of
sphincters are 1-Pyloric. 2-ileocaecal. 3-internal anal sphincter.
Length of the small intestine from pylorus to the ileo-caecal valve is 285 cm in living
human, at autopsy 700 cm. the colon length is 100 cm in living human adults and 150 cm
at autopsy.
2) Rhythmic contraction: can occur as rapid as 9-12 per minute in the intestine or as slow as
3 per minute in the stomach. It is the frequency of the slow wave in these segments that
sets the frequency. Rhythmic contraction is important for:
1- Mixing the food.
2- Peristaltic propulsion of food.
Peristalsis
Peristalsis is a reflex response that is initiated when the gut wall is stretched by the
contents of the lumen, and it occurs in all parts of the gastrointestinal tract from the
esophagus to the rectum. The stretch initiates a circular contraction behind the stimulus
and an area of relaxation in front of it. The wave of contraction then moves in an oral to
caudal direction, propelling the contents of the lumen forward at rates that vary from 2 to
25 cm/s. Peristaltic activity can be increased or decreased by the autonomic input to the
gut, but its occurrence is independent of the extrinsic innervation. Indeed, progression of
the contents is not blocked by removal and resuture of a segment of intestine in its
original position and is blocked only if the segment is reversed before it is sewn back into
place. Peristalsis is an excellent example of the integrated activity of the enteric nervous
system. It appears that local stretch releases serotonin, which activates sensory neurons
that activate the myenteric plexus. Cholinergic neurons passing in a retrograde direction
in this plexus activate neurons that release substance P and acetylcholine, causing smooth
muscle contraction. At the same time, cholinergic neurons passing in an anterograde
direction activate neurons that secrete NO, VIP, and ATP, producing the relaxation ahead
of the stimulus
Migrating Motor Complex
During fasting between periods of digestion, the pattern of electrical and motor activity in
gastrointestinal smooth muscle becomes modified so that cycles of motor activity migrate
from the stomach to the distal ileum. Each cycle, or migrating motor complex (MMC),
starts with a quiescent period (phase I), continues with a period of irregular electrical and
mechanical activity (phase II), and ends with a burst of regular activity (phase III)). The
MMCs migrate aborally at a rate of about 5 cm/min, and they occur at intervals of
approximately 90 minutes. Their function is unsettled, although gastric secretion, bile
flow, and pancreatic secretion increase during each MMC. They may clear the stomach
and small intestine of luminal contents in preparation for the next meal. They are
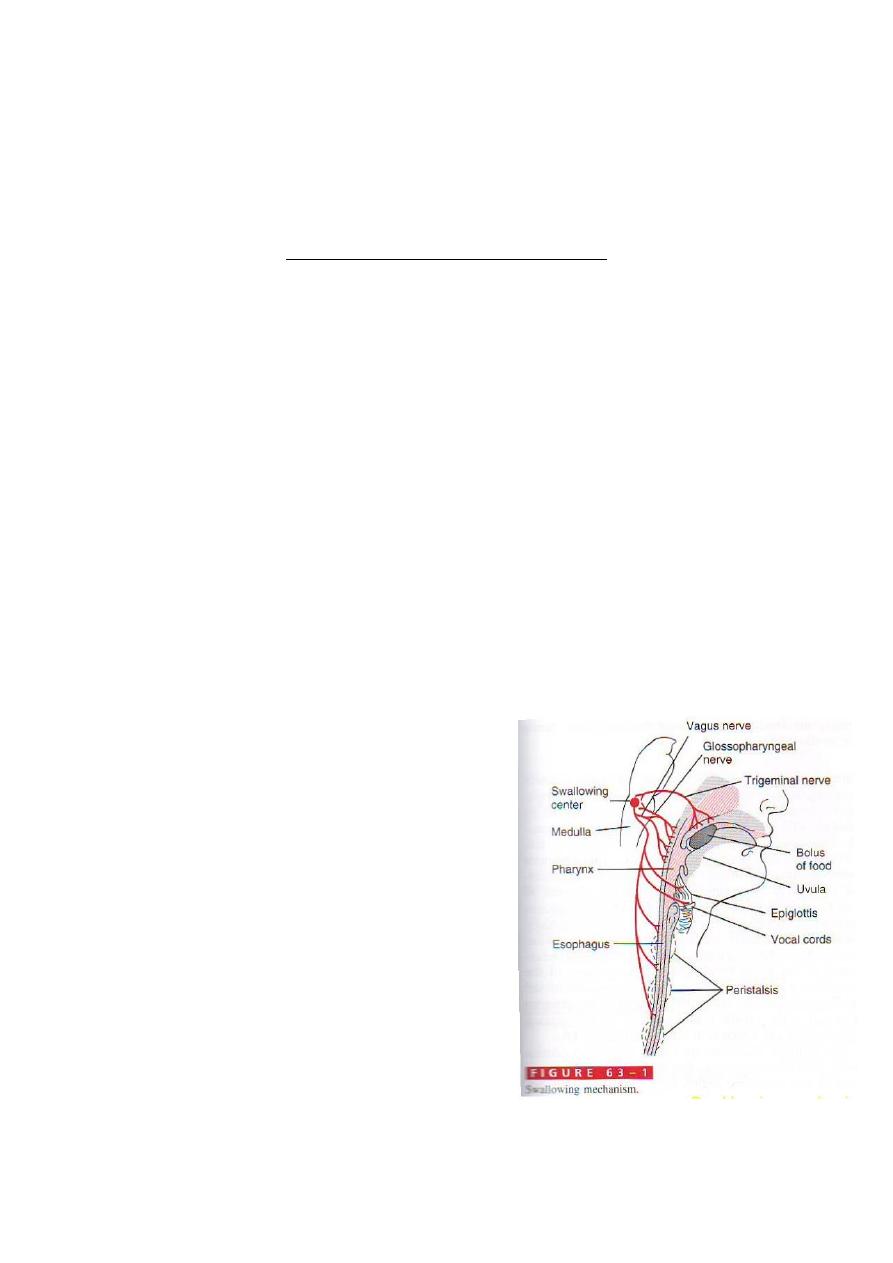
44
immediately stopped by ingestion of food, with a return to peristalsis and the other forms
of BER and spike potentials.
MASTICATION OR CHEWING:
The incisors for cutting and the molars for grinding action.
DEGLUTITION OR SWALLOWING
Deglutition or swallowing is a highly complicated process because it requires the simultaneous
activity of a number of structures. Any delay in any one of these structures will cause difficulty in
swallowing and the condition is called Dysphagia. Swallowing can be divided into 3 stages:
1- Oral stage.
2- Pharyngeal stage.
3- Oesophageal stage.
The oral stage is voluntary while both the pharyngeal and oesophageal stages are involuntary.
1- ORAL STAGE: swallowing starts by closing the mouth and the bolus will be maneuvered or
moved to the postero-dorsal surface of the tongue, and the tongue will squeeze or roll the
bolus against the hard palate in an upward and backward direction. Thus the bolus will be
forced into the pharynx. Saliva is necessary for normal swallowing.
2- PHARYNGEAL STAGE: when the bolus is pushed
backwards in the mouth, it stimulates the
swallowing receptor areas all around the
opening of the pharynx and particularly on the
tonsillar pillars. From there impulses will be
transmitted through the sensory branch of the
trigeminal (5
th
) and glossopharyngeal (9
th
)
nerves to the brainstem where the swallowing
or the deglutition center is situated. From the
swallowing center motor impulses will be sent
to the pharynx through 5
th
, 9
t
, 10
th
and 12
th
cranial nerves. These motor impulses will
produce a series of automatic pharyngeal
muscular contractions.

45
To understand the complexity of the second stage of swallowing, it will be easier if we
kept in mind the fact that the alimentary tract crosses the respiratory tract in the region
of the pharynx, so the swallowing movements have to serve two quiet different functions:
1) First is to propel the food through the pharynx and into the oesophagus.
2) Second is to protect the airways both above and below form the possible entrance of
food particles.
The pharyngeal movements that occur in the second stage of swallowing are the
followings:-
1- The soft palate will be pulled upwards in order to close the posterior nares, so that
no food or fluid will enter the nasal cavity (protective).
2- The palate-pharyngeal folds of mucus membranes on either side of the pharynx will
be pulled medial wards so that they are approximated. This will change the
pharyngeal opening into a slit through which the bolus must pass to the posterior
pharynx. This slit will have a selective action allowing the passage of properly
masticated food easily while impeding the passage of large objects. This is a
protective phenomenon.
3- Vocal cords of the larynx are approximated in order to prevent the passage of food
to the trachea. This is a protective mechanism. Damage to the vocal cords or the
muscles that approximate them can cause strangulation.
4- Epiglottis will swing backwards over the superior opening of the larynx, in order to
prevent the food from getting as far as the vocal cords. This is a protective
phenomenon.
5- The larynx will be elevated by muscles attached to the hyoid bone. This will elevate
the glottis out of the main stream of food flow so that the food passes on either
side of the epiglottis rather than on its surface. Thus it is another protective
mechanism against the passage of food to the trachea.
6- The upper oesophageal sphincter will relax to allow the food to pass from the
posterior pharynx to the oesophagus. This sphincter (made from crico-pharyngeus
muscle) is in a state of tonic contraction normally between swallows and thus it
prevents the air form going to the oesophagus during respiration.
7- Simultaneously will the elevation of the larynx and relaxation of the upper
oesophageal sphincter there will be a contraction of the superior constrictor muscle
of the pharynx which will initiate a rapid peristaltic wave passing downward from
the pharynx to the oesophagus.
8- The process of respiration will be inhibited temporarily. The swallowing center will
inhibit the respiratory center whether in the process of inspiration or expiration.
This is a protective mechanism also.
46
The entire pharyngeal stage of swallowing will take less than 2 seconds, so that temporary
inhibition of respiration will take only a small fraction of the respiratory cycle. So in
summary of the pharyngeal stage:
a- The trachea is closed.
b- The oesophagus is open.
c- Rapid peristaltic wave originate in the pharynx, will force the bolus of food into the
upper oesophagus.
Swallowing can be greatly affected or prevented by:
1- Any damage to the cranial nerves (5
th
, 9
th
, 10
th
)
2- Or to the swallowing center such as in poliomyelitis or encephalitis.
3- Or to the swallowing muscle as in muscle dystrophy
4- Failure of neuromuscular transmission as in myasthenia gravis.
One of the most important conditions of paralysis of the swallowing mechanism
occurs when the patient is under deep anesthesia.
Most anesthetic agents used are emetic in nature (they cause vomiting). Thus the
patient vomits materials from the stomach into the pharynx, however the
swallowing act is paralysed but respiration stays. Therefore instead of swallowing
the material again, the material will pass to the trachea. These patients will often
chock to death by their own vomitus, or they inhale the vomited material and this
will cause chemical of bacterial pneumonia.
3- OESOPHAGEAL STAGE: the oesophageal stage of swallowing begins with the relaxation of
the upper oesophageal sphincter. Immediately after the bolus has passed, the sphincter
closes, the glottis opens and breathing returns. Once in the oesophagus the bolus is
moved towards the stomach by a progressive wave of muscle contraction which is known
as peristaltic wave. Swallowing can occur while a person is upside down since it is not
primarily gravity but the peristaltic wave which moves the bolus to the stomach. In
upright position liquids and semi-solids foods generally fall by gravity to the lower
oesophagus ahead of the peristaltic wave. The oesophagus has two types of movements:
1- Primary peristalsis: is the continuation of the peristaltic wave that started higher up in
the pharynx. It will take about 8-10 seconds to pass from the pharynx to the stomach.
The vagus nerve is the main nerve that controls this primary peristalsis. If this primary
peristalsis fails for some reason to move all the food then secondary peristalsis will
start.
2- Secondary peristalsis: it will be stimulated by the distension of the oesophagus by the
retained food. The myenteric plexus of the oesophagus are responsible for these
secondary peristalsis.
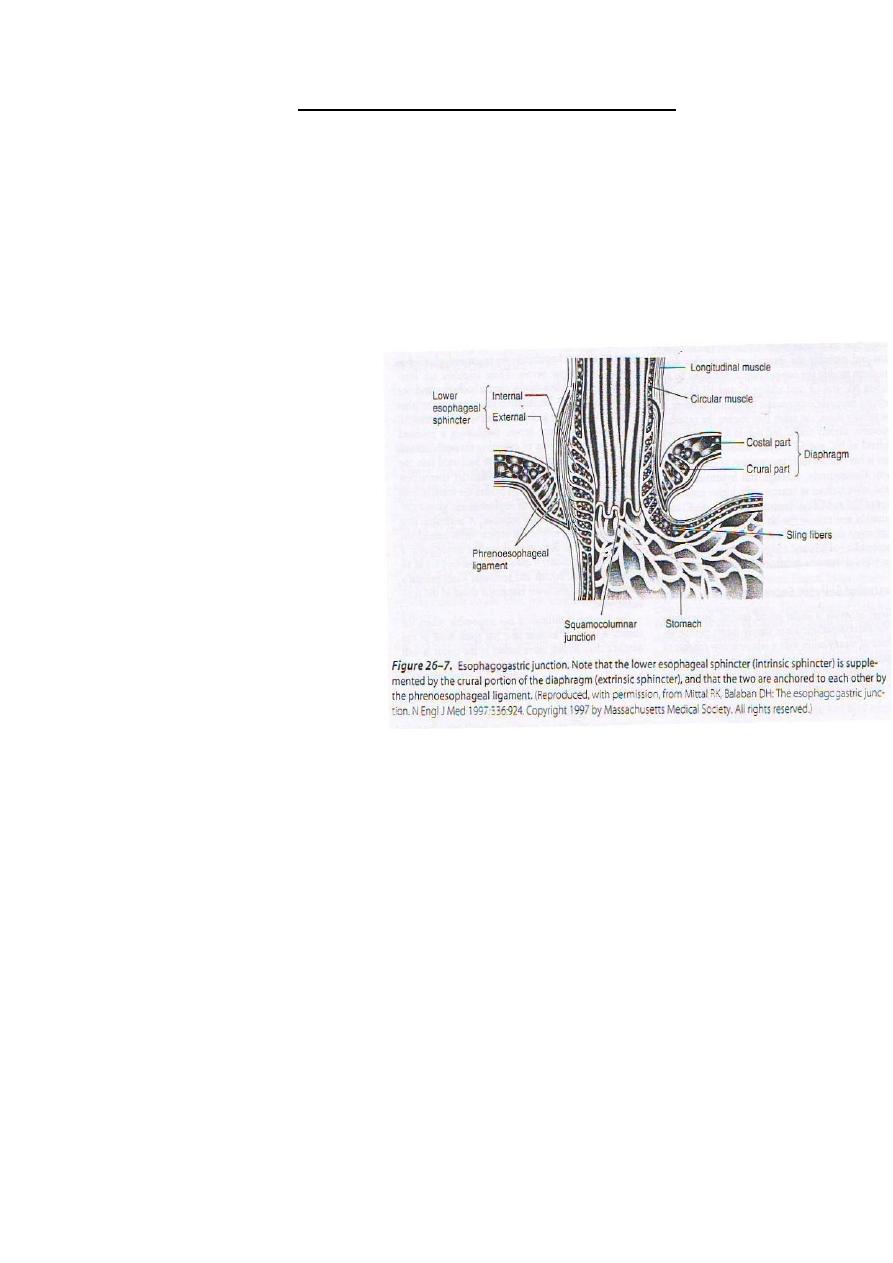
47
LOWER OESOPHAGEAL SPHINCTER (LOS)
The lower Oesophageal sphincter (LOS) is a physiological sphincter rather than an
anatomical sphincter. When there is no swallowing the sphincter is in state of tonic
contraction and thus there is no reflux of food from the stomach to the oesophagus.
During swallowing, this sphincter will relax to allow the food to enter the stomach.
LOS is controlled by both nervous and hormonal mechanisms.
1- Nervous: Ach from vagal endings cause increase in tonic contraction. Nitric oxide
(NO) and VIP released
from interneurons
innervated by other
vagal fibers causes it to
relax (non-adrenergic
non-cholinergic NANC).
2- Hormonal: some
hormones increase the
tone of the sphincter
such as gastrin, and
some decrease the tone
of this sphincter such as
secretin and
progesterone. Because
progesterone decreases
the tone of LOS, thus reflux is well documented in the 3
rd
trimester of pregnancy,
and in women taking birth control pills containing progesterone. Thus the common
problem of heart burn occurring during pregnancy appears to be primarily due to
hormonal influence on LOS pressure which will allow a gastro-esophageal reflux to
occur particularly when there is an enlarged uterus with increased abdominal
pressure.
Several mechanisms operate to prevent reflux of food and fluid from
the stomach into the lower oesophagus. The most important are:-
1- Lower oesophageal sphincter just above the oesophago-gastric junction. 2-The
position of this sphincter just below the diagram so that it is reinforced by intra-
abdominal pressure and the 3-The angle of entry of the oesophagus into the
stomach.
48
Thus reflux is prevented by this flutter valve closure of the distal end of the
oesophagus which is a valve-like mechanism of that portion of the oesophagus
that lies immediately beneath the diaphragm. Greatly increased intra-
abdominal pressure caves the oesophagus inward at the same time that the
abdominal pressure also increases the intra-gastric pressure. This flutter-valve
closure of the lower oesophagus prevents the high pressure in the stomach
from forcing stomach contents into the oesophagus. The later two mechanisms
are lost when the oesophago-gastric junction slides through the diaphragm. This
proximal displacement is usually sufficient to allow reflux although the lower
oesophageal sphincter may remain operative.
ACHALASIA
Due to increase in resting LOS tension and incomplete relaxation of this
sphincter upon swallowing and motor disorder in the lower 2/3 of the
oesophagus. The myenteric plexus of the oesophagus is deficient in NO and VIP.
And the patient usually complains from dysphagia. If the condition becomes
sever, the emptying of food from the oesophagus to the stomach may take a
long time (many hours instead of the normal time of few seconds) and the
oesophagus will be greatly dilated (mega-oesophagus).
Lower Esophageal sphincter incompetence
This is opposite to Achalasia, the incompetence will cause reflux of gastric
contents and acids to the oesophagus. This will lead to inflammation of the
oesophagus→Oesophagitis by the irritating gastric contents. This can lead to
ulceration of the oesophagus and then scarring and stricture of the oesophagus.
49
RECEPTIVE RELAXATION OF THE STOMACH:
The normal tonic contraction of the stomach is inhibited by the arrival of food,
mediated by a vagal reflex. This allows the stomach to accommodate greater
quantities of food up to 1-1.5 liter. This large increase in volume is accompanied by
only a small rise in pressure within the lumen.
BASIC ELECTRICAL RHYTHM (BER) OR GASTRIC SLOW WAVE:
Consisting of electrical slow wave that occur spontaneously in the stomach wall.
The BER is a wave of depolarization of smooth muscle cells proceeding from
circular muscle of the fundus of the stomach to the pylorus every 15-20
seconds. This wave is the pacemaker for the mixing and peristaltic movement of
the stomach.
MOVEMENTS IN THE STOMACH
1- MIXING movement: when the stomach is filled, weak constrictor waves move
towards the antrum at a rate of 3-4/min. these waves usually start near midpoint of
the stomach when it is filled and they progress from the body of the stomach to the
antrum. When they reach the antrum, they become more intense in order to mix the
food.
2- PROPULSIVE OR PERISTALTIC waves: strong peristaltic waves occur in the antrum with
a rate of 3-4/min. these are really an extension of the mixing waves that have
become more intense as they spread from the body of the stomach to the antrum.
They start at the incisura angularis and spread as strong peristaltic ring-like
constriction through the antrum in the direction of the pylorus and duodenum. They
are about 6 times as powerful as the usual mixing waves. The peristaltic waves help in
propulsion and mixing of food.
3- HUNGER contractions: this is an intense contraction that occurs in the stomach when
it has been empty for a long time. They are usually
rhythmic peristaltic
contraction
which are very strong and they may fuse together to cause a continuing
TETANIC
CONTRACTION
lasting 2-3 minutes. It happens in young healthy persons with high
degree of gastrointestinal tonus and usually after fasting for 12-24 hours, when the
blood sugar is low. The strong hunger contractions causes pain in the area of the
stomach called Hunger pangs and it is relieved by ingestion of food.
50
EMPTYING OF THE STOMACH
The emptying of the stomach is opposed by the resistance of the pylorus to the
passage of food and is promoted by peristaltic waves in the antrum of the stomach.
ROLE OF THE PYLORUS IN THE STOMACH EMPTYING:
The pylorus is usually tonically contracted. This tonic contraction is weak enough so
that water and fluid can empty with ease. While it is great enough to prevent
movement of semisolid food (chyme) into the duodenum, except when strong antral
peristaltic wave force the chyme through the pylorus. The degree of constriction of
the pyloric sphincter can increase or decreases under the influence of signals from the
stomach and duodenum. Gastrin and distension of the stomach by food by (nervous
mechanism) will inhibit the pylorus. While signals from the duodenum depress the
pyloric pump and increase pyloric tone by both nervous (enterogastric) and hormonal
(secretin-GIP-VIP-CCK-peptide YY….e.t.c).
ROLE OF ANTRAL PERISTALSIS IN THE STOMACH EMPTYING:
Antral peristalsis sometimes become so intense and spread as strong peristaltic ring-
like constriction. Each antral peristaltic wave forces several milliliters of chyme into
the duodenum, thus peristaltic waves provides a pumping action that is frequently
called pyloric pump.
FACTORS AFFECTING GASTRIC EMPTYING
The rate at which food leaves the stomach is determined by various factors:-
1- Total volume of gastric contents.
2- Consistency.
3- Chemical composition.
4- Osmolar concentration.
5- PH.
1) The total food volume → the amount evaluated in a unit of time is related to
the volume of the gastric contents. Stretch of the stomach wall elicits VAGAL
and local MYENTERIC reflexes in the wall that increase the emptying.
2) Consistency: liquid more than solids, inert liquids that do not stimulate the
stomach chemically or osmotically leave the stomach rapidly such as water.
Solids are not evacuated until they are reduced to a fluid or semi-fluid
consistency.
3) Chemical composition: CHO leave more rapidly followed by protein and lastly
fat. Fat especially if eaten in large quantities remain in the stomach for a long
time and in animal experiments up to 24 hours.
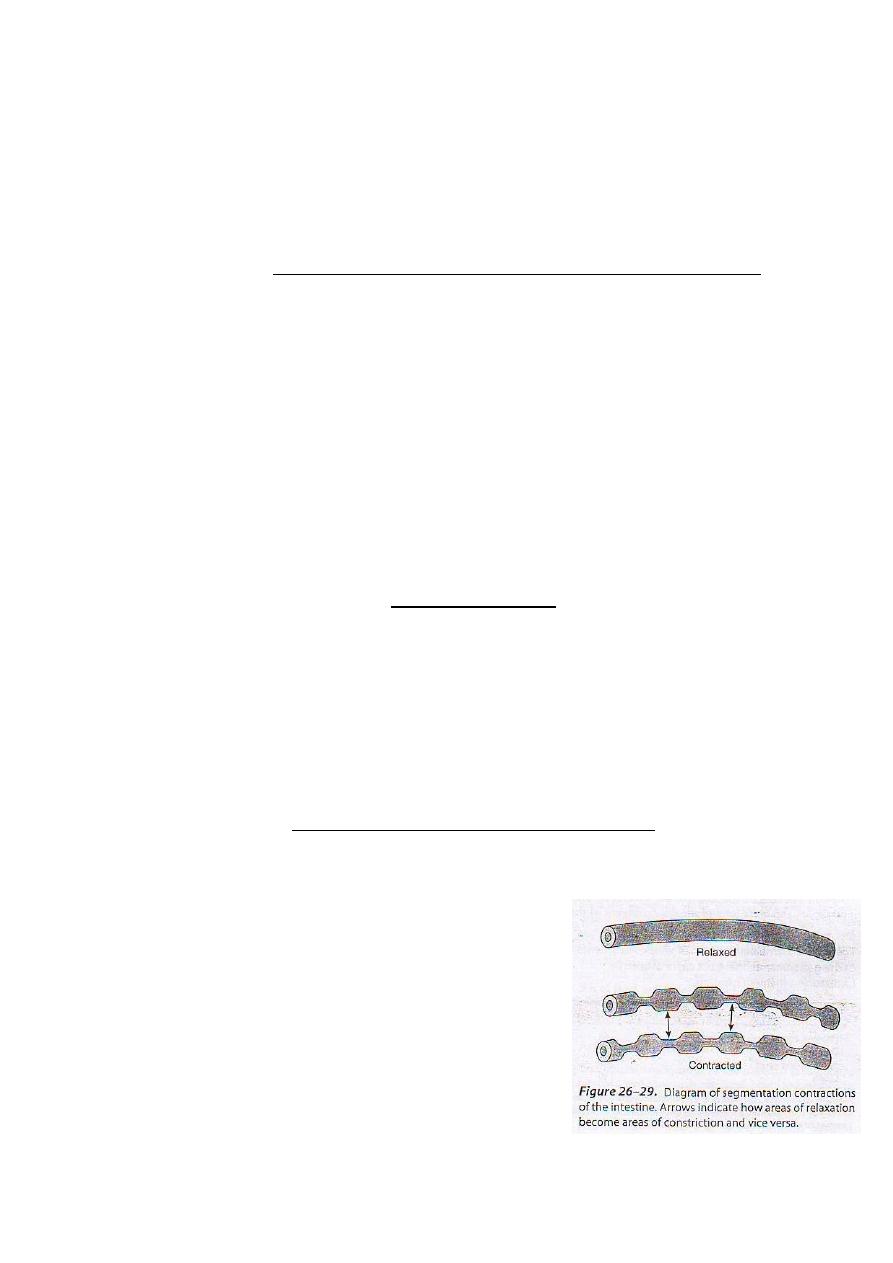
51
4) Osmolar concentration of the gastric contents → saline in a physiological
concentration leaves the stomach more rapidly than do salt solution of either
greater or lesser concentrations.
5) Acid: strong acid solution in the stomach leaves the stomach slowly and the
rate of emptying of such solution can be accelerated by neutralizing the acid.
REGULATION OF GASTRIC MOTILITY AND EMPTYING
1- NERVOUS
- Local reflexes through myenteric plexus.
- Vagal nerve.
*the above are in the stomach and they increase gastric motility and
emptying.
- Enterogastric reflex → inhibits activity.
2- Hormonal
- Gastrin in the stomach and small intestine → increase emptying.
- INTESTINAL: Enterogastrone, GIP, VIP, Secretin, CCK, Peptide YY…e.t.c.→
inhibit gastric motility and emptying.
SMALL INTESTINE
BER : Basic electrical rhythm in the small intestine. They are initiated by pacemaker
cells located in the outer circular muscle layer near the myenteric plexus. It is about
12/min. in the duodenum and falls to about 8/min. in the distal ileum, thus enabling the
proximal small bowel to override more distal areas. It is thought that the myenteric
plexus and the enteric hormones determine the local response to the slow wave so the
contraction may or may not occur depending on the state of the affairs in the lumen at
any one time.
MOVEMENTS IN THE SMALL INTESTINE
1- Mixing or segmentation contraction: they are ring-like contractions that occur
throughout the length of the small intestine. These
ring-like contractions appear at regular or irregular
intervals. The length of each segment is about 1 cm.
these ring-like contractions causes segmentation of
the gut (a chain of sausage). As a set of contraction
disappear, a new set appears in the segment
between the previous contractions.
2- Tonic contractions: are relatively prolonged
contractions that in effect isolate one segment of
the intestine from another. The segmentation contractions and the tonic contractions
52
slow transit in the small intestine to the point that the transit time is actually longer in
the fed than in the fasted state. This allows longer contact of the chyme with the
enterocyte and enhances absorption.
3- Propulsive or peristaltic movement: these will propel the chyme through the small
intestine, being faster in the proximal small intestine than in the distal small intestine.
4- Peristaltic rush: very strong peristaltic waves not seen normally but in intestinal
obstruction or severe diarrhea.
5- Movements caused by muscularis mucosae and muscle fiber of the villi:
Muscularis mucosae contract → making mucosal fold → increase absorption.
Muscle fiber of the villi contract intermittently, thus the villi will shorten and elongate
and shorten again. This will help in MILKING the villi so that lymph flow is increased
from central lacteal to the lymphatic system.
Movements in the colon:
The movements of the colon are coordinated by BER of the colon.
The frequency of this wave, unlike the wave in the small intestine, increases along the
colon from about 2/min. at the ileo-caecal valve to 6/min. at the sigmoid.
Types of movements of the colon:
The motor activities in the colon are designed to either:
a- Mix colonic contents and facilitate absorption.
b- Propulsion.
1- Mixing movement → Haustration.
It is similar to segmentation movement of the small intestine. Large circular
constriction occurs in the large intestine. These circular constrictions are due to
the contraction of circular muscles and also the longitudinal muscles. The
longitudinal muscles in the colon are aggregated into three longitudinal strips
called TAENIA COLI. The contraction of these longitudinal and circular muscles
will result in that the unstimulated portion of the large intestine to bulge
outwards into bag-like sacs called Haustration. The Haustral contraction mixes
the colonic contents and exposes them to the mucosa. Thus it facilitates
absorption by colonic mucosa of water and electrolyte.
2- Peristaltic movement: propel the contents towards the rectum.
3- Mass peristalsis: most of the peristalsis in the colon is the mass peristalsis. It
occurs only in the colon. It is not like the slow peristalsis in the small intestine.
Mass peristalsis occurs only a few times every day and they occur mostly after
eating breakfast. The mass peristalsis occur when a point in the colon is
distended or irritated, then this will cause a constrictive contraction around this
point and simultaneously there will be contraction of 20 cm or more of the
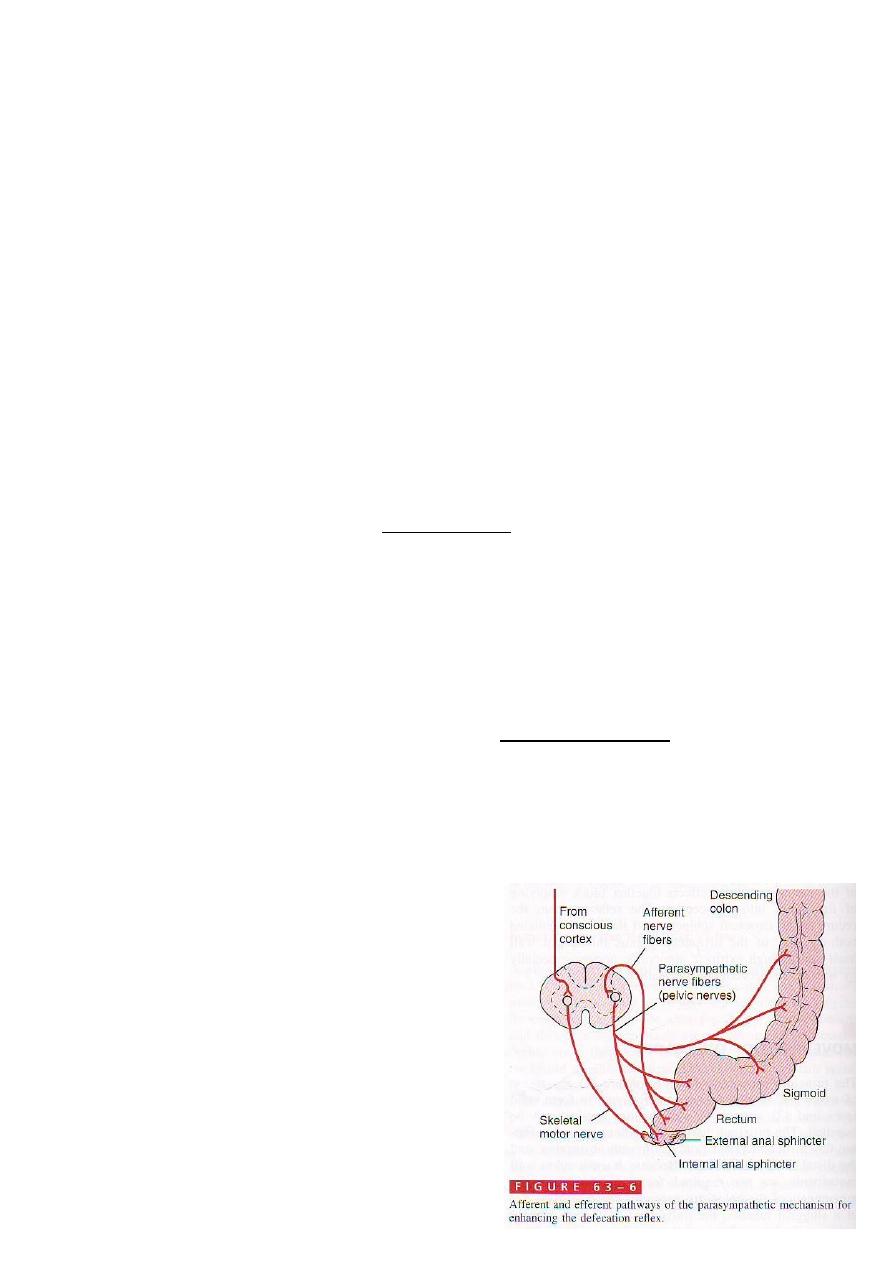
53
colon distally. This will force the faecal contents in this colonic segment
enmasse
down the colon. The mass peristalsis can occur anywhere in the colon
although they often occur in the transverse or descending colon. If mass
peristalsis has forced a mass of faeces into rectum, then the desire for
defaecation will be felt. However not all mass peristalsis result in the desire to
defaecate because sometimes the movements of the colonic contents stops
before emptying the colonic contents into the rectum.
Mass movements occur usually after meal and particularly after breakfast,
drinking a glass of coffee, warm water, orange juice or lemon juice in the
morning. This is at least due to Gastro-colic and Duodeno-colic reflexes.
These reflexes occur when the stomach or duodenum is distended after eating
or drinking. The mechanism behind these reflexes might be due to both nervous
and hormonal. The nervous pathway might be through the autonomic nervous
system. The hormonal mechanism might be due to release of the hormone
gastrin from the antral mucosa in response to distension.
Defaecation
The rectum is usually empty from faeces and the faecal masses are stored in the sigmoid colon
and not in the rectum. The desire to defecate occurs when the faeces enter the rectum as a
result of mass peristalsis. An increase in the intra-luminal pressure of the rectum by 18 mmHg
will usually cause the desire to defecate. The desire to empty the rectum is experienced if the
rectum is filled with solid faeces, liquid or gas. The receptors in the rectal wall are not only able
to detect increase in pressure inside the rectum, but they can also differentiate whether the
increase in pressure is due to faeces, liquid or gas. This discriminating ability of these receptors
will be lost in patients with infectious diarrhea or proctitis due to ulcerative colitis or other
inflammatory conditions.
Defaecation will happen as a result of the defaecation reflexes:-
1-Intrinsic defaecation reflex: this occurs when afferent signals spreading to the myenteric
plexus will cause peristaltic waves in the descending
colon, sigmoid and rectum, and relaxation of the
internal anal sphincter (which is a circular mass of
smooth muscle lying immediately inside the anus)
and if the external anal sphincter is relaxed then
defaecation will occur. However this reflex is very
weak and in order to be effective it must be
supported by the second defaecation reflex →
54
2-Parasympathetic defaecation reflex: this occurs when afferent signals will pass to the sacral
portion of the spinal cord and impulses will be sent back through Nervi erigentes or pelvic
nerve to cause contraction of the descending colon, sigmoid and rectum and relaxation of
internal anal sphincter. This parasympathetic reflex will greatly intensify the intrinsic reflex.
However the defaecation reflexes will not produce defaecation unless the external anal
sphincter is relaxed. This sphincter is composed of striated voluntary muscles and it is under
voluntary control from the cerebral cortex through the somatic nerve which is the pudendal
nerve. Contraction of this sphincter will counteract the defaecation reflex. Except in babies ,
in the normal adults the conscious mind will take the control of the external anal sphincter
and will either cause relaxation of the external anal sphincter if the time is suitable, or will
cause contraction of the external anal sphincter to prevent defaecation. Thus if the time is
suitable then from cerebral cortex, efferent impulses will be sent through the pudendal nerve
to cause relaxation of the external anal sphincter. At the same time impulses from higher
centers will facilitate defaecation by:
1) Taking a deep breath
2) Closure of the glottis
3) Contraction of the abdominal muscles
*all these will increase the intra-abdominal pressure and force the faeces downward.
If the time was not suitable, then the external anal sphincter will remain contracted and the
reflex will die out after a short time and will not return until an additional amount of faeces
enter the rectum.

55
Large intestinal bacteria
The large intestine of the newborn child is bacteriologically sterile. This sterility will last
for a few days only and thereafter the intestine will be invaded and colonized by ingested
bacteria. The bacteria will flourish mainly in the large intestine, while the small intestine
contains much less bacteria. The reasons why the small intestine contains less bacteria
than the large intestine might be due to:
1. Acid gastric secretion.
2. Rapid transit time in the small intestine will allow less time for the growth of
bacteria.
Effect of intestinal bacteria
Intestinal bacteria have a complex effect on their host (man). Some of these effects are
useful and others are harmful:
1. Antibiotics improve growth rates in a variety of species including man, that’s the
reason why antibiotics are frequently added to the diets of domestic animals and
the reason is unsettled?.
2. Nutritionally important substances such as vitamin C and cyanocobalamine and
choline are utilized by some intestinal bacteria. On the other hand some bacteria
synthesize vitamin K and some B-complex vitamin. Folic acid was shown to be
absorbed in significant amounts.
3. Intestinal bacteria form a number of amines such as indole – skatole, which
contribute to the odor of the faeces, as do sulfides.
4. Change primary bile acids in to secondary bile acids.
5. Partly responsible for the formation of gases in the large intestine .the amount of
gases entering or forming in the large intestine each day is about 7 – 10 liters where
as the average amount expelled is only 0.6 liters. The reminder is absorbed through
the intestinal mucosa. Most often the person expels large amount of gases not
because of excessive bacterial activity but because of excessive motility of the large
intestine, the gases being moved on through the large intestine before they can be
absorbed.
6. Intestinal bacteria appear to play a role in cholesterol metabolism, since the poorly
absorbed antibiotic neomycin that modifies the intestinal flora lowers plasma LDL
and cholesterol levels.
7. Colonic bacteria produce short chain fatty acids (SCFA) by acting on undigested
complex carbohydrates from fruits and vegetables, and the major site of their
56
production and absorption is the colon. They appear to be trophic to the colonic
mucosa and they promote the absorption of Na⁺ by Na⁺ - SCFA coupled absorption.
SCFAs when absorbed will be metabolized and make a significant contribution to
the total caloric intake.
SCFAs combat inflammation. SCFAs are absorbed in part by exchange for H⁺ helping
to maintain acid – base equilibrium.