1
PHYSIOLOGY
Dr. Basim Mohamad Awan
Lecture 21
MEMORY
Memory is the ability of the brain to store information and
retrieve it at a later time. The storage capacity of the human
brain is limited. So, the information that flow into the brain is
classified into significant one that will stored and insignificant
one that is ignored and not stored. The most important ones (less
than 1%) are selected and stored, but all the rest are neglected
and forgotten.
STORAGE CAPACITY OF THE BRAIN
The information unit is the "bit", which is the simplest form of
sensory experience; i.e. a letter, a line, a color, a tone, a smell...etc.
The capacity of all the sensory system to send information to the
brain is less than 50 bits/s. An average rate of information flow is
about 20 bits/s. Ten neurons are required to store one bit of
information. The total storage capacity of the human brain is
about 3x 10
8
bits.
TYPES OF MEMORY :
Four different types of memory:
[I] SENSORY MEMORY (Immediate memory).
[II] PRIMARY MEMORY (Short-term memory)
2
[III] SECONDARY MEMORY (Long-term memory)
[IV] TERTIARY MEMORY (permanent memory)
[I] SENSORY MEMORY (Immediate memory)
Any sensory signal is automatically stored in the sensory memory
for few seconds. This memory can accommodate 15-20 bits.
Forgetting
starts
spontaneously
immediately
after
the
information is acquired. The spontaneous gradual decline in the
amount of stored information is called "fading" of information.
The spontaneous disappearance of information from the memory
is called "extinction" of information. The information in
sensory memory can be transferred to the secondary memory.
[II] PRIMARY MEMORY (Short-term memory)
This is a memory that lasts for few minutes to few hours. The
information enters this memory by verbalization; i.e. through
spoken or written words. The primary memory is not found in
young infants or animals as they would not understand the
meaning of spoken or written words.
The capacity of primary memory is small. Bits of information
are introduced into it in chronological order, one after the other.
The new information replaces the old ones. The latter are then
forgotten.
The access to the primary memory stores is rapid; one can retrieve
the information rapidly.
3
[III] SECONDARY MEMORY (Long-term memory)
This is a memory that lasts for several hours up to several years.
The information is introduced into this memory from the sensory
and primary memories by two mechanisms:
1. Stimulation of the reward or punishment systems.
2. Repeated practice or rehearsal of the experience.
The capacity of the secondary memory is large. The information
is stored according to its significance. The bits of information of
related significance are stored together. The access to the
secondary memory stores is slow; it takes some time to remember
the wanted information.
Forgetting of information in the secondary memory occurs when
a new information conflicts with an old stored one. In this case,
one information cancels the other either by repulsion or by
replacement. If the 'old information repels the new one; the
process is called "proactive inhibition" and if the new
information replaces the old one, the process is called
"retroactive inhibition".
In this way, the more we have learned, the greater the liability to
forget the new information by proactive inhibition. The old
information inhibits the acquisition of new ones. Therefore, the
blame for most of our forgetting must be placed on what we
have learned before.
4
[IV] TERTIARY MEMORY (Permanent memory)
This is the permanent memory. The information stored in this
memory are never forgotten; e.g. one's name or the ability to
read and write. Information in the tertiary memory comes from
the secondary memory by years of practice, which strongly
consolidates the memory. The stored information in the tertiary
memory remains available for retrieval even if information in
other memories is erased by brain injury or disease. This is
because information in the tertiary memory occupies large areas
of the brain and more than one "copy" of the information is
stored in different regions of the brain.
The access to the ternary memory is very rapid, e.g. one
immediately remembers his name if he is asked about it.
MECHANISMS OF MEMORY
[I] SENSORY MEMORY
Sensory memory is made by prolonged after discharge in the
neuronal circuits. Three mechanisms are involved:
(a) Activation of reverberating circuits leading to repeated
reactivation of neurons.
(b) Short term synaptic potentiation by multiple successive
stimulation of input neurons.
(
C
)
Synaptic sensitization by coupling the sensory experience
with intense or noxious stimulus.
5
[II] PRIMARY MEMORY
The primary memory is made by the formation of temporary
memory traces. A memory trace is a newly developed pathway
for signal transmission resulting from facilitation of new
synapses. This leads to the creation of new circuits in the brain
that keeps the memory of the experience. Activation of these
circuits brings the memory up to one's mind. There are two
possible mechanisms for the formation of the new memory
traces:
(a) Long term potentiation of synapses. During verbalization
the brain catches the new interesting information and rehearses it
several times.
(b) Changes in the physical properties of the postsynaptic
membrane leading to enhanced sensitivity to the chemical
transmitter.
[III] SECONDARY MEMORY
Secondary memory is made by formation of "memory
engrams". A memory engram is a long-lasting memory trace
formed by structural changes in presynaptic terminals. These
changes include:
(a) Increase in the total area of the specific release sites in
the cell membrane. Transmitter vesicles get attached to these
sites before they rupture and release their transmitter into the
synaptic cleft. The increase in the release sites increases the
6
amount of transmitter released at the presynaptic terminal, thus
facilitating synaptic transmission.
(b) Increase in the number of transmitter vesicles in the
presynaptic terminal.
(c) Increase in the number of presynaptic terminals by
formation of new terminals.
The memory engrams remain for a long time, up to several
years. Formation of memory engrams requires protein synthesis.
Antibiotics which inhibit protein biosynthesis interfere with the
formation of memory engrams. They prevent the consolidation
of memory but do not affect the primary memory.
[IV] TERTIARY MEMORY
Tertiary memory is made by the formation of permanent
memory traces (permanent engrams). These permanent
engrams are made by structural changes in the neurons. The
changes are similar to those in secondary memory. Tertiary
memory may be considered as an advanced stage of secondary
memory.
CONSOLIDATION OF MEMORY
Consolidation of memory means the transfer of information
from the Sensory and primary short-term memories to the
secondary long-term memory. This process takes from 5 minutes
for minimal consolidation to two hours for maximal
7
consolidation. Consolidation of memory could be interrupted by
deep anesthesia, brain concussion or electroconvulsive
therapy (ECT). Accordingly, if a sensory impression is made,
then followed within 5 minutes by brain concussion or ECT or
anesthesia, the experience gets extinct. This explains why
patients who had brain concussion in accidents cannot remember
what happened at the time of the accident. If the concussion
occurs 2 hours after" the sensory experience, the information
remains unaffected. If it occurs within two hours, the memory is
affected proportionately.
Consolidation occurs to the information which attracts the
attention of the mind. The brain automatically rehearses this
information. A wide awake person consolidates memories far
better than a person with mental fatigue. This is because the
wide awake brain is more attracted by the new information and
is capable of making rapid and more frequent rehearsals that
would consolidate memory more effectively. Normal quiet sleep
consolidates the memory of information received before the
onset of sleep.
ENCODING OF MEMORY
Encoding of memory is the classification, then placing each memory
item with other related items in the proper memory store; i.e.
memory archiving. It is part of the consolidation process. The
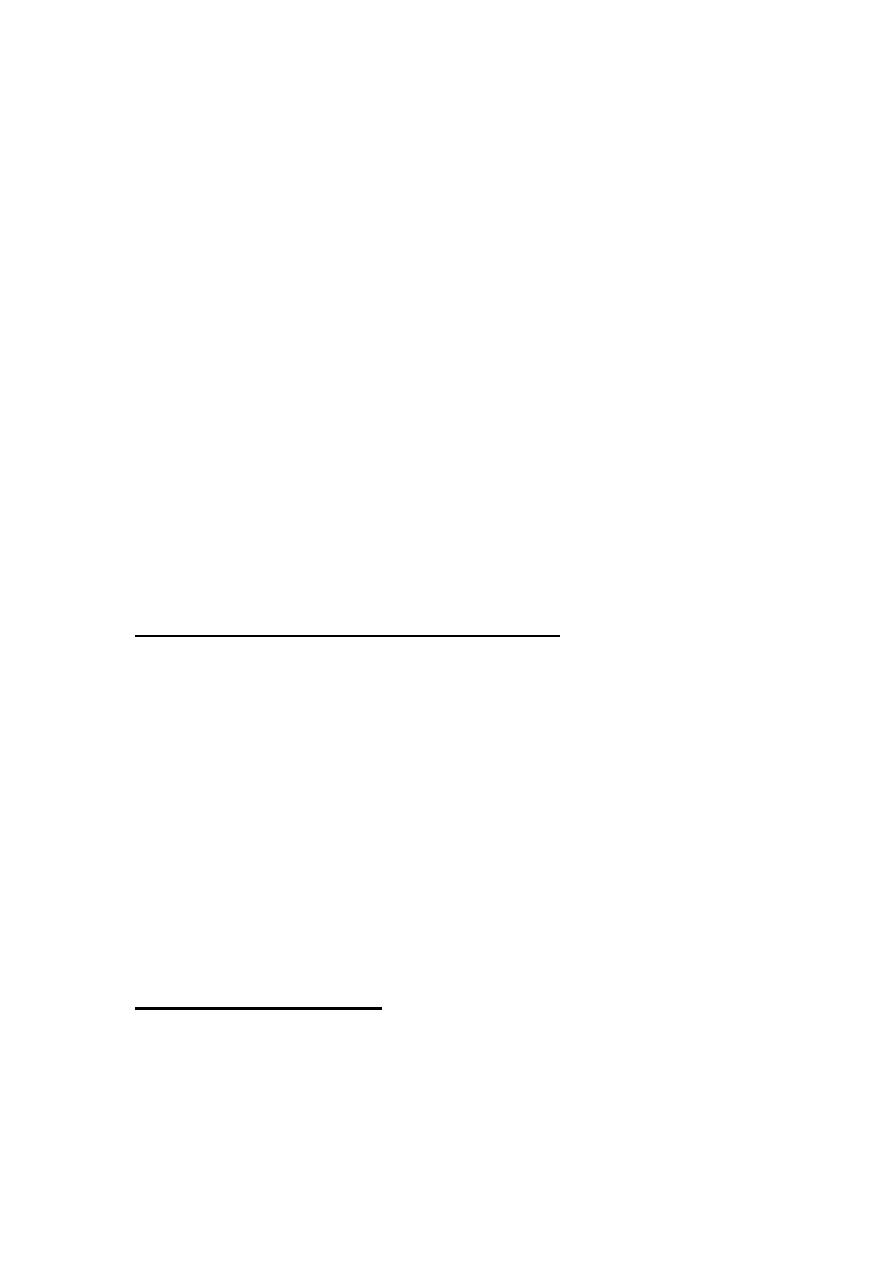
hippocampus plays a central role in this function. All bits of
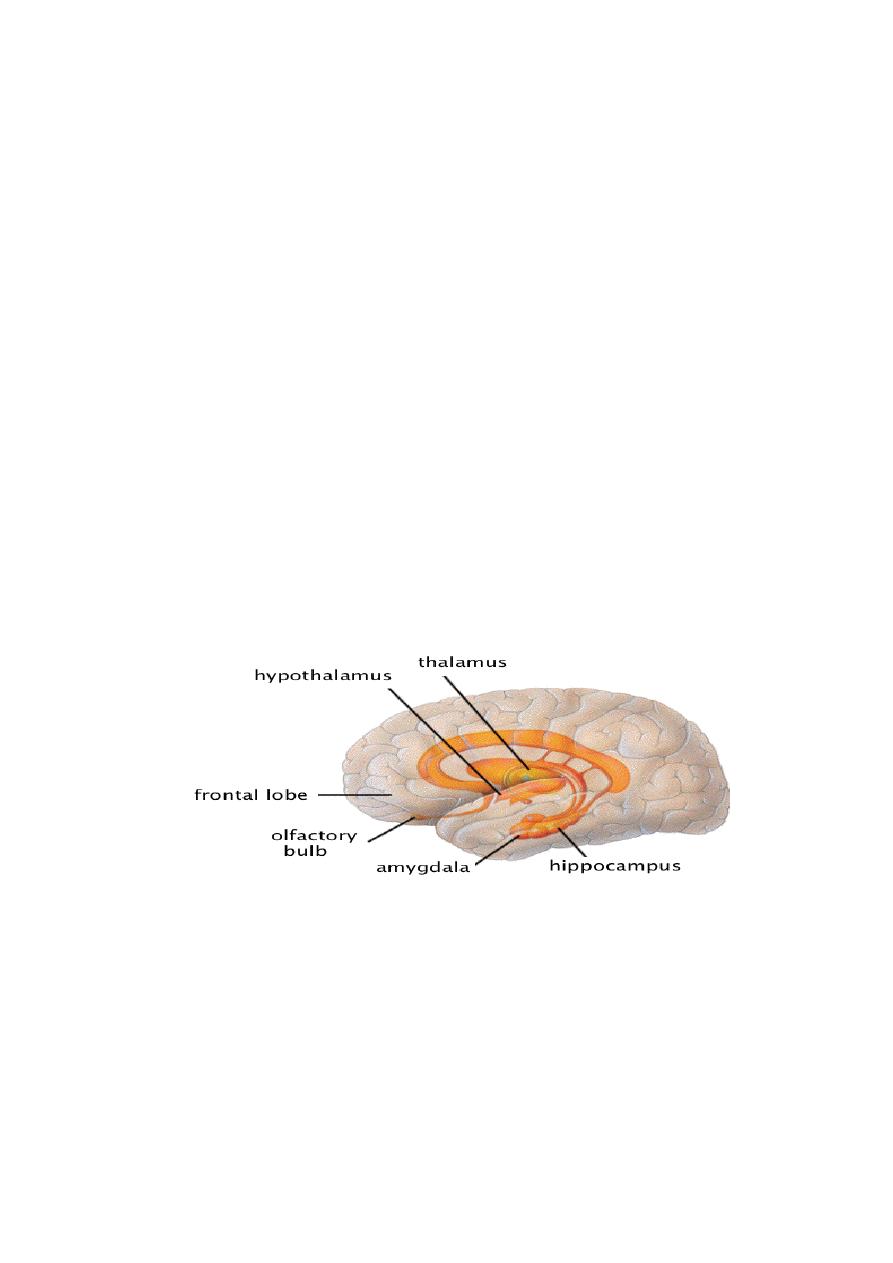
8
information go first to the hippocampus where they are sorted out
as significant or insignificant. If the information is classified as
significant, signals are sent to the mamillary bodies of the
hypothalamus. From the hypothalamus signals proceed on to the
orbitofrontal cortex, then to the basal forebrain (Fig. 19-1).
From the basal forebrain (nucleus basalis of Meynert) there are
diffuse cholinergic projections to the memory stores which are
found in all parts of the neocortex, the amygdala and the
hippocampus. The amygdala associates the memories formed
through different senses, then through its connections with the
hypothalamus (the amygdalohypothalamic pathways) it is
responsible for the emotional and autonomic responses to
memories.
Figure 21-2:
Brain areas concerned with encoding of long term
memory
Long-term memories are stored in the form of engrams in
different regions of the brain. To retrieve a certain memory item,
one should get an access to the specific engrams of this item and
activates them. This can be done by different associations. For
example the word "Egypt" could be accessed and activated by
9
other words as "the pyramids", "the Nile" or hearing part of the
opera "Aida" or seeing a photo of a pharaoh with his
characteristic features and head dress. Each of these methods of
access is considered as a specific "key" which "unlocks " and
activates the specific engrams of the stored item.
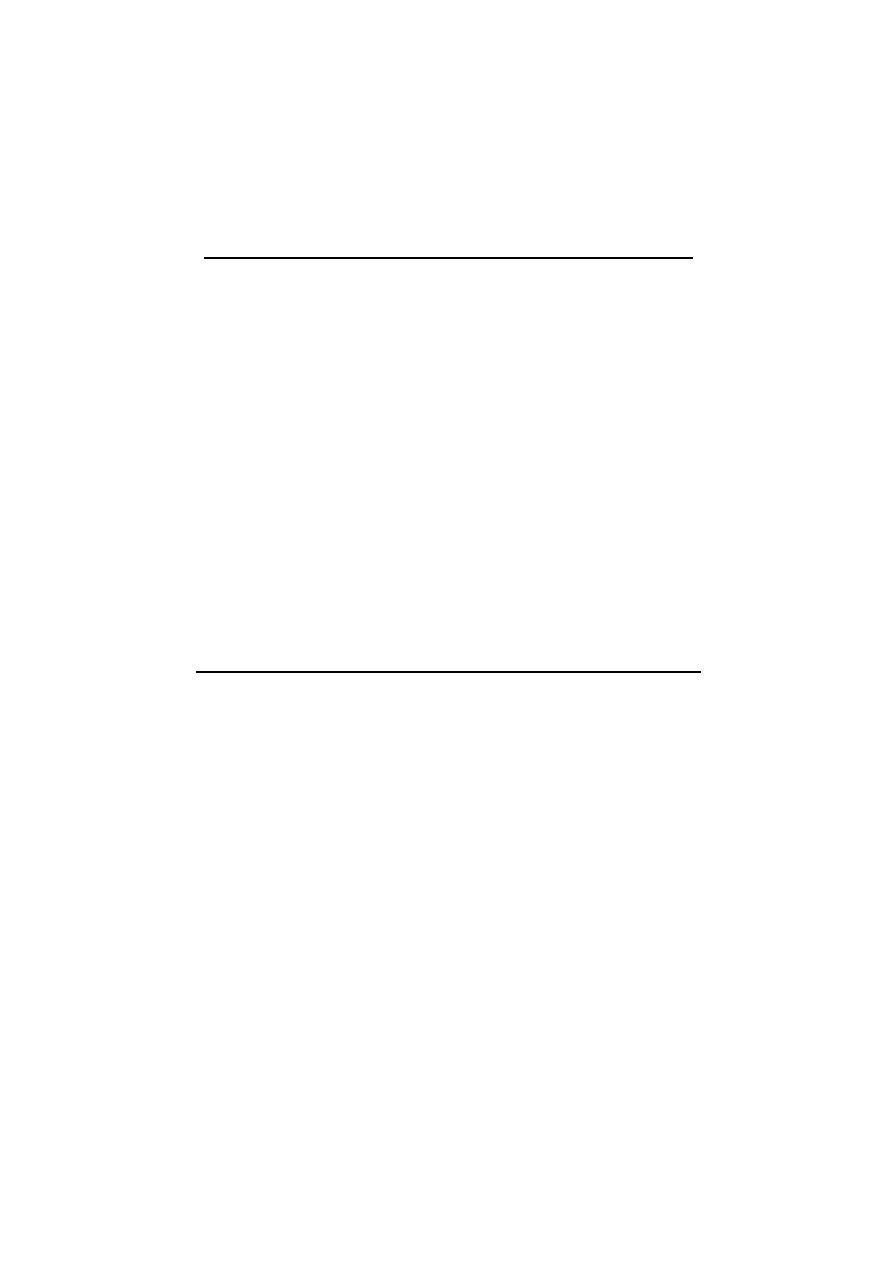
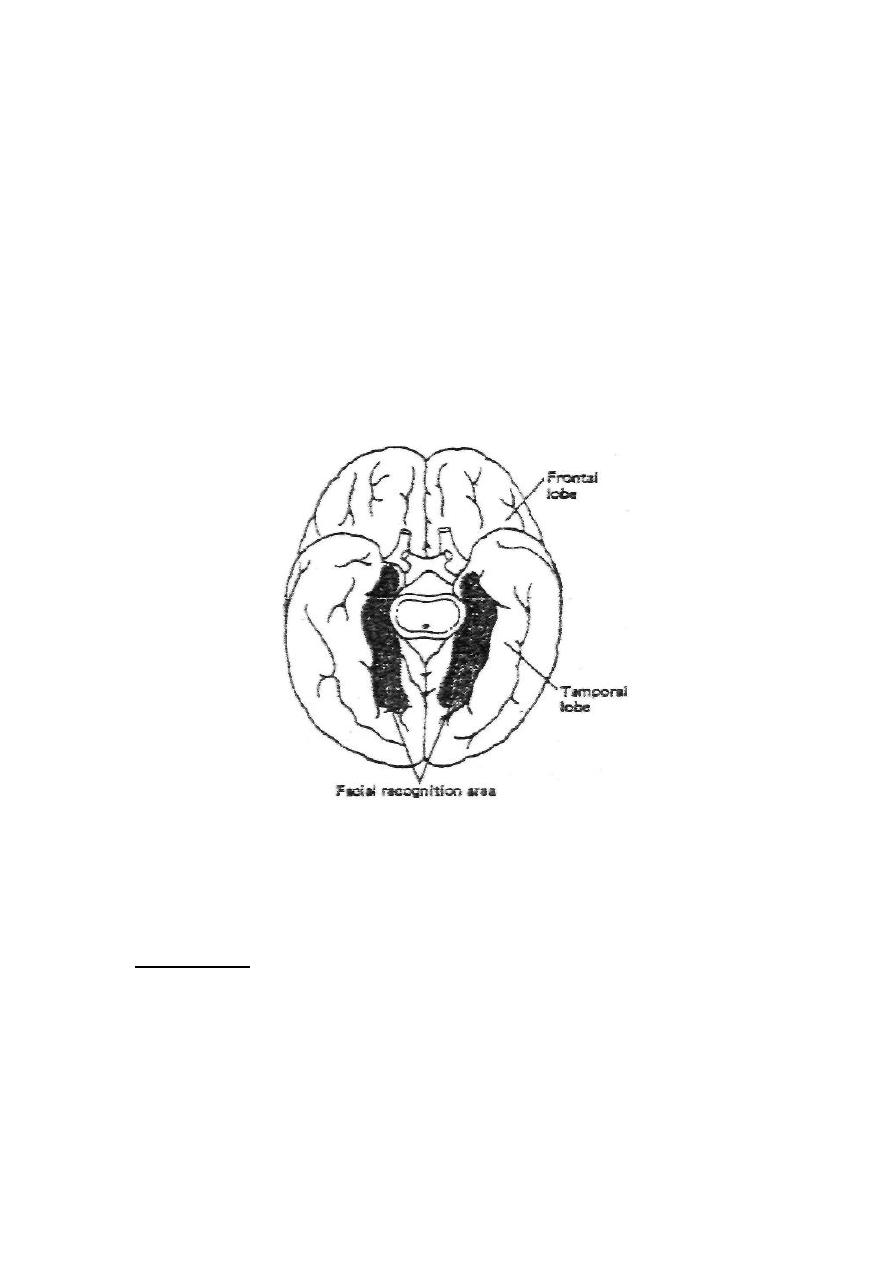
FACIAL RECOGNITION AREA
The impression of faces is stored in the "facial recognition
area" in the neocortex of the undersurface of the temporal and
occipital lobes (Fig. 21-3). In right-handed persons and some of
the left handed ones, the facial recognition area is much better
developed in the right (representational) hemisphere than in the
left (categorical) hemisphere.
Bilateral lesion in this area leads to "prosopagnosia" which is'
inability to recognize people by their faces. In this case, the
patient can recognize persons by their voices. A prosopagnostic
patient develops emotional and autonomic reactions on seeing a
familiar face, but he wouldn't identify the person until he hears
him speaking.
NAMING OF OBJECTS AREA
This is the function of an area in the most lateral portion of
both the anterior occipital and posterior temporal lobes. In
this area, the names of different objects are stored. Like the
facial recognition area, it is better developed on the right side
10
than in the left side. Damage of this area leads to inability to
name objects, although the patient is able to know what the
object is, its value or its use. Only the name is lost from memory.
This is probably the brain area which gave Adam the advantage over
angels. According to the holy Qur'an, after the creation of Adam,
angels failed to name objects when Allah asked them to do, Adam by
the command of Allah, preceded and told the names of objects.
Figure 21-3: Basal view of the human facial recognition
area.
AMNESIA
Amnesia (Gr. = forgetfulness) means the inability to remember
past experience. There are several types of amnesia:
1. RETROGRADE AMNESIA
It is the inability to recall events that occurred shortly before the

11
onset of brain malfunction without affecting memories of the
remote past. Retrograde amnesia occurs with brain concussion
(post-traumatic amnesia), anesthesia, electric shock (therapeutic
ECT or accidentally). In these conditions, a transient brain
malfunctioning erases the memories of events over a long period
before the onset of malfunctioning. During recovery, the length
of the period of amnesia shrinks progressively till it involves only
several minutes.
2. ANTEROGRADE AMNESIA
It is the inability to form new memories. The memories
consolidated before the onset of amnesia are retained. The
sensory and primary memories are functional but cannot be
consolidated.
Anterograde amnesia occurs with bilateral lesions in the
hippocampus or other structures involved in the encoding of
memory.
3. PSYCHOGENIC OR HYSTERICAL AMNESIA
This is a rare condition characterized by sudden loss of memory
for usually all information in the secondary and tertiary
memories. This usually follows a severe psychological trauma or
it may be an unconscious response to internal conflict or an
intolerable life situation. It is a purely functional disorder
without any organic disease. It can be differentiated from
12
amnesia caused by damage or disease in the brain tissue by three
characteristics:
(I) All the personal data are forgotten, including the patient's
own name.
(ii) The amnesia is not affected by key stimuli; seeing members
of his family, his friends or his personal effects.
(iii) The inability to remember past events persists although the
patient can make new memories.
Complete recovery of memory almost always occurs.
ALZHEIMER DISEASE AND SENILE DEMENTIA
Alzheimer disease is caused by degeneration of the cholinergic
nerve fibers which project from the nucleus basalis of
Meynert to the neocortex, the amygdala and the
hippocampus. The disease is characterized by deterioration of
intellectual abilities as impairment of memory, lack of judgment
and inattentiveness. The disease may occur at any age. In old
age, it is called senile dementia. It is the commonest cause of
dementia in old age (found in 10-15% of the population above
the age of 65). The anticholinesterase drug eserine
(physostigmine) produces some improvement but it does not
stop the progress of the disease.