1
RESPIRATORY SYSTEM
Dr.Firdous
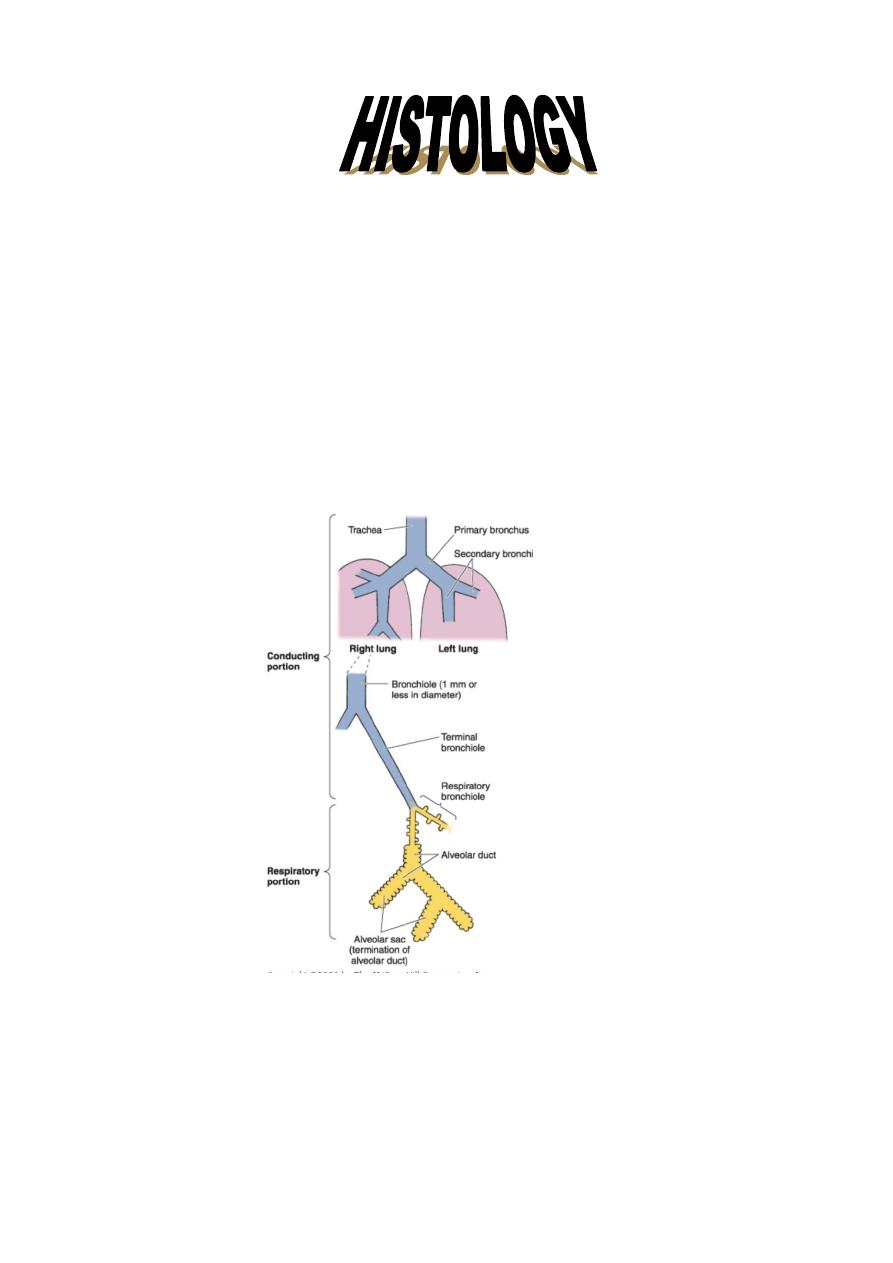
It consists of two regions:
1-Conducting portion: The main conducting airways in the upper part of the respiratory
tract have walls that are reinforced with bone or cartilage to keep them open, and their
mucosal lining is adapted for cleaning and conditioning air on its way to the lungs. The
incoming air passes through a succession of cavities and passageways, namely the nasal
cavities, nasopharynx, larynx, trachea, and next enters several generations of progressively
smaller bronchi, followed by a larger number of different orders of bronchioles.
2- Respiratory portion: includes: respiratory bronchioles, alveolar ducts, sacs, and
alveoli.
The main functions of the conducting part are:
1- Act as a conduit (pathway) to transport air to and from lungs. This is achieved by the
presence of cartilage, to support the walls, and prevents the collapse of its lumen. The
walls are richly supplied with elastic fibers for the flexibility, while smooth muscles
regulate air flow during inspiration and expiration, by their contraction.
2
2- Conditioning of air: through:
a- Vibrissae: they are specialized hair which is thick and short, present in the inner
surface of the nostrils, to remove coarse dust particles.
b- Layer of mucous and serous secretion in the nasal fossae traps the particles and gas
impurities, and moistens the air.
c- Presence of conchae, where the air pass through them, to increase the surface area,
and turbulence of air flow.
The main function of the respiratory portion is the exchange of oxygen and carbon dioxide
between inspired air and blood.
RESPIRATORY EPITHELIUM
Pseudostratified columnar ciliated epith., with goblet cells. It lines most of the
conducting part. It consists of five types of cells:
1- Ciliated columnar cells: represent the most common type. Each cell has
about 300 cilia on the apical surface. Beneath these cilia, there is a basal body, and
small mitochondria, to supply ATP for ciliary beating.
Ciliary movement transports a continuous layer of mucous to the pharynx. Foreign
particles will be traped in this mucous, so this will protect lungs from any particulate
matter and any bacteria.
Immotile cilia syndrome, a disorder that causes infertility in men and chronic
respiratory tract infections in both sexes, is caused by immobility of cilia and flagella
induced, in some cases, by deficiency of dynein; protein normally present in the cilia.
Dynein participates in the ciliary movement .
2- Mucous goblet cells: they are global in shape, and their apical part contains mucous
droplets composed of glycoproteins.
3- Brush cells: they have numerous microvilli on their apical surface. They are considered
as sensory receptors due to the presence of afferent nerve endings on their basal
surface.

3
4- Basal(short) cells: small, rounded cells, lie on the basal lamina, but do not extend to
the luminal surface of the epithelium. They are believed to be the generative cells for
other cell types.
5- Small granule cells: small, rounded cells, with numerous granules, 100-300 nm in
diameter, with dense core. They are part of the diffuse neuro endocrine system
(DNES),also known as Kulchtsky cells. They produce calcitonin, somatostatin,
serotonin, and bombesin. These cells are demonstrated by using silver stain, which
react with their granules. With the use of EM, granule cells show fine tapering
cytoplasmic processes towards the lumen. The function of granule cells is still not
understood well, but they may function in reflexes regulating the air-way or vascular
caliber.
Respiratory epithelium a- Brush cell b- Small granule cell
From the nasal cavity through the larynx, portions of the epithelium are stratified
squamous. This type of epithelium is evident in regions exposed to direct airflow or
physical abrasion (eg, oropharynx, epiglottis, vocal folds); it provides more protection
from attrition than does typical respiratory epithelium. If airflow currents are altered or
new abrasive sites develop, the affected areas can convert from typical ciliated
pseudostratified columnar epithelium to stratified squamous epithelium. Similarly, in
smokers, the proportion of ciliated cells to goblet cells is altered to aid in clearing the
increased particulate and gaseous pollutants (eg, CO, SO 2 ). Although the greater
numbers of goblet cells in a smoker's epithelium provide for a more rapid clearance of
pollutants, the reduction in ciliated cells caused by excessive intake of CO results in
decreased movement of the mucous layer and frequently leads to congestion of the
smaller airway.

4
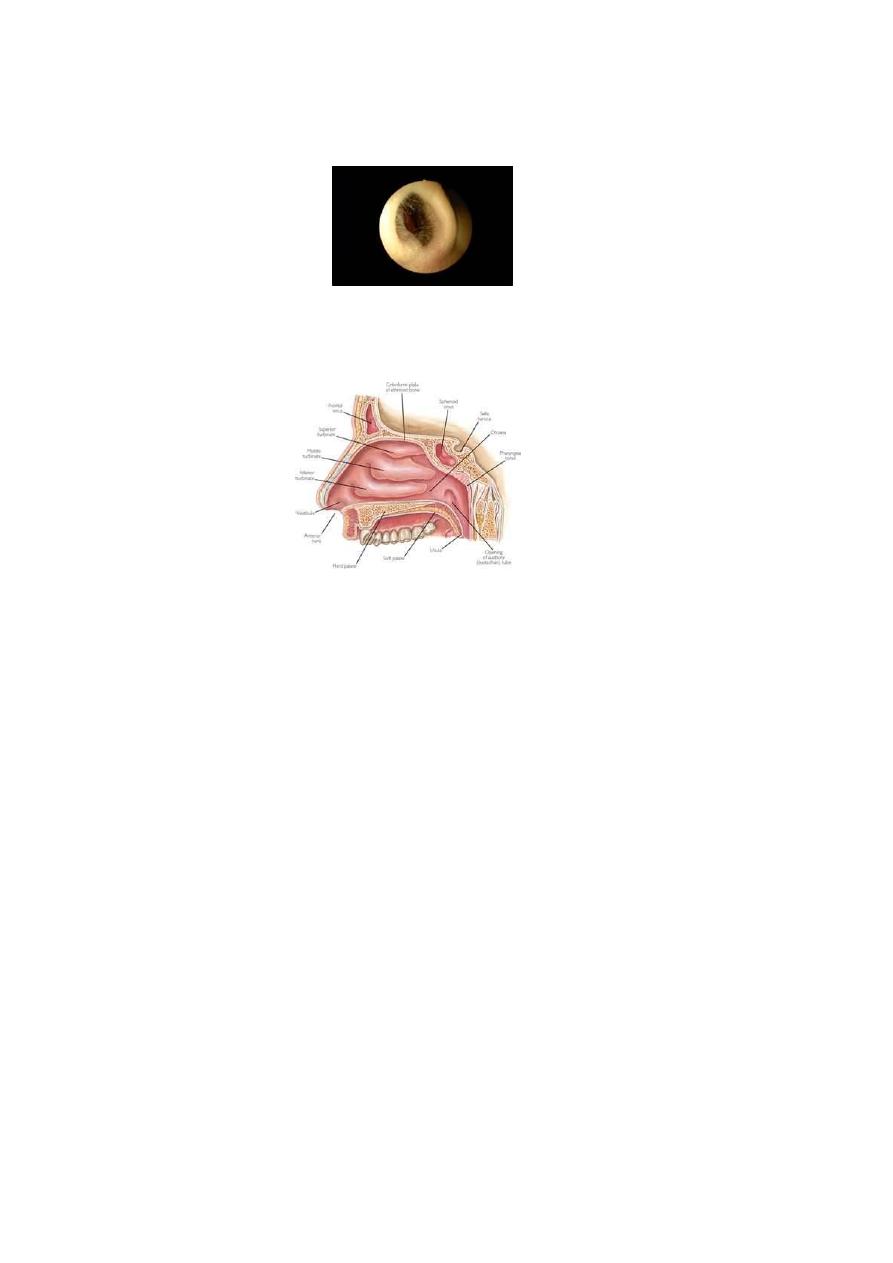
NASAL CAVITY
It is opened anteriorly into the nares, and posteriorly into the nasopharynx, at the
choanae.
Its wall is well supported by bone and cartilage. Naasal cavity consists of two
structures:
1- Vestibule: it is the most anterior and dilated part of the nasal cavity. The nares(nostrils)
are the anterior openings and are covered by skin(stratified seq. keratinized ), which is
rich in sebaceous and sweat glands, in addition to the thick short hair, or vibrissae.
Inside the vestibule, the epith. will change into respiratory epith.
2- Nasal fossae: They are two cavernous chambers within the skull, separated by nasal
septum. From each lateral wall projects three boney shelf-like projections; the
chonchae, or turbinates. The middle and inferior ones are lined by respiratory epith.
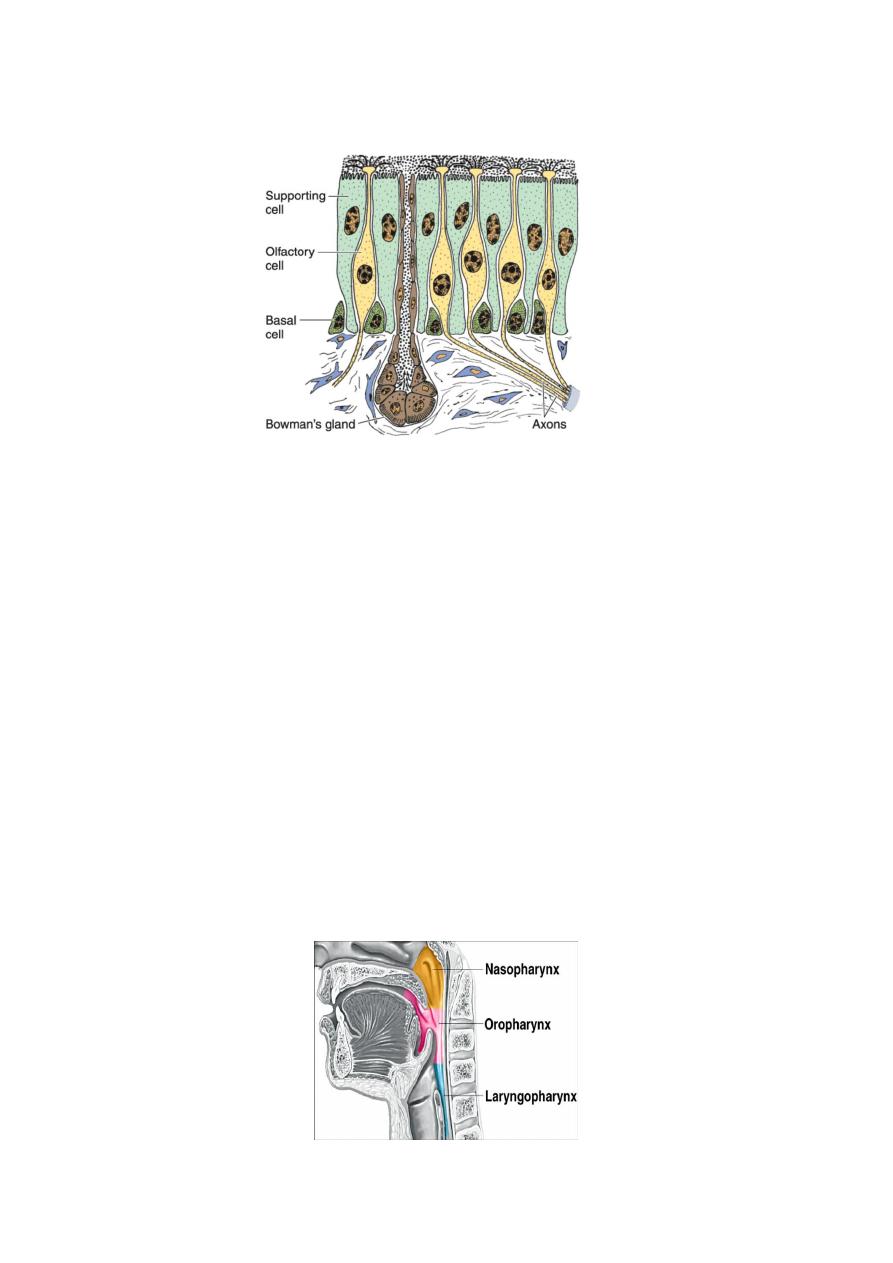
Superior choncha is covered by a specialized olfactory epith. It is about 10 cm
3
in area,
and up to 100µm in thickness. It is composed of three types of cells:
a- Supporting cells: they have broad cylindrical apices with narrow bases.
On their free surface, are microvilli which are covered by fluid layer. Well developed
junctional complexes bind these cells to the adjacent olfactory cells. The nucleus lies in
the upper half of the cell. The cytoplasm contains RER, SER, and mitochondria. A
yellow pigment is found in the cytoplasm similar to lipofuscin. Theses cells act as glial
cells, providing both metabolic and mechanical support.
b- Basal cells: small, spherical or cone shaped cells, rest on the basement membrane.
Their cytoplasm contains few organells, and they act as stem cells for other
respiratory cells.
c- Olfactory cells: Bipolar neurons. Their nuclei lie in a level bellow that of the
supporting cells. The apices have elevated and dilated areas; the olfactory vesicle,
from which arise 6-8 non motile long cilia,(although some research suggest some
limited motility). The plasma membrane of cilia contains odorant-binding protein
that act as receptors for smell sensation.These cilia extend radially in a plane parallel
to the surface epithelium. The afferent axons of bipolar cells unite to form the
olfactory nerve, which traverse the cribriform plate of ethmoid bone, then enter
olfactory bulbs of olfactory cortex. Olfactory cells have a life span of one month, and
they are replaced if injured, so they are the only neurons that replaced during postnatal
life.
Lamina propria of the olfactory epith.contains the glands of Bowman, a branched
tubuloalveolar serous glands, which secretes a fluid around the olfactory cilia to
facilitate the dissolve of odoriferous substances to stimulate olfactory cells. The lamina
propria of the concha contains large venous plexuses known as the swell bodies. Every
20-30 minutes the swell bodies on one side of the nasal fossae become engorged with
blood, resulting in distention of the conchal mucosa, and decrease in the flow of air.
These periodic intervals of occlusion reduce the air flow, allowing the respiratory epith.
to recover from dryness.
5
Allergic reactions and inflammation can cause abnormal engorgement of swell bodies
in both fossae, severely restricting the air flow.
PARANASAL SINUSES
They are closed cavities in the frontal, maxillary, ethmoidal, and sphenoid bones.
They are lined by thin respiratory epith., with few goblet cells. Their lamina propria
contains small glands. They communicate with nasal cavity through small openings.
Mucous produced in the sinuses is swept into nasal cavity by ciliated cells.
Sinusitis is an inflammatory process of the sinuses that may persist for long periods of
time, mainly because of obstruction of drainage orifices. Chronic sinusitis and
bronchitis are components of immotile cilia syndrome, which is characterized by
defective ciliary action.
NASOPHARYNX
It is the first part of the pharynx, lined by respiratory epith. at the contact with soft
palate. It communicates with middle ear by Eustachian tube. Its wall is rich in diffuse
and nodular lymphatic tissue.
6
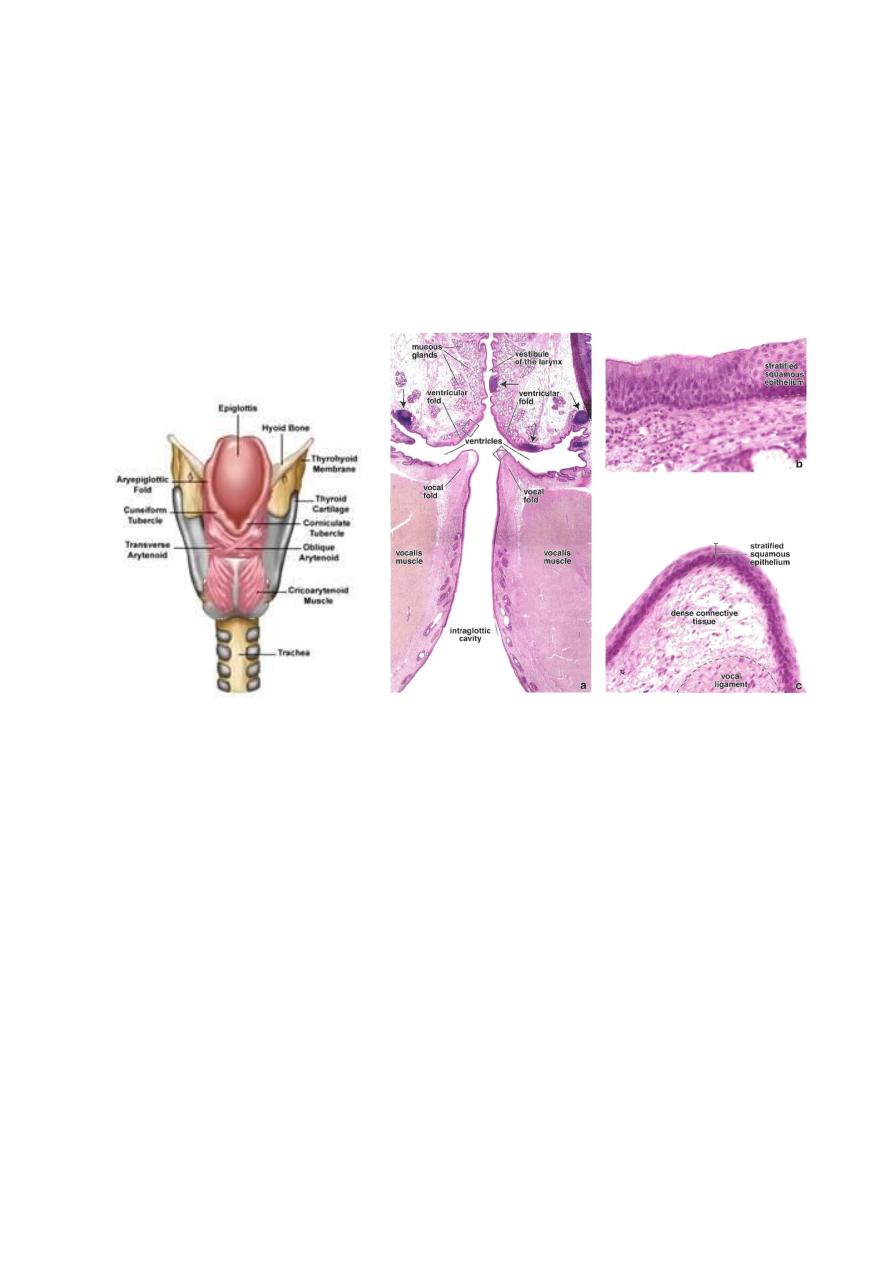
LARYNX
An Irregular tube that connects the pharynx to the trachea. The skeleton of the
larynx is made of cartilage within the lamina propria. The large cartilages are hyaline,
while the small ones are elastic. These cartilages support the larynx to maintain an open
air way, and prevent swallowed food from entering the trachea, also they participate in
sound production(phonation). Larynx also counteract obstruction or irritation by
coughing.
Larynx Epiglottis
Epiglottis: is one the small elastic cartilages that projects from the anterior wall of
the larynx. It has both lingual and laryngeal surfaces. Lingual surface(anterior surface),
and the apical part of epiglottis is covered by stratified seq.non keratinized epith. The
lower part of the laryngeal surface (posterior surface)is covered by respiratory epith.
Bellow the epith., the lamina propria contains both mucous and serous glands.
Bellow the epiglottis, the mucosa forms two pairs of folds that projects into the lumen
of the larynx. The upper pair constitutes the false vocal folds, which are covered by
respiratory epith. The lower pair represents the true vocal cords, and lined by stratified
seq. epith. These folds are oriented in an antero-posterior direction, and define the
lateral boundaries of the opening of the larynx; rima glottis. Within these folds, there is
large bundles of parallel elastic fibers composing the vocal ligament. The tention and
length of vocal ligament determines the kind of sounds produced. Parallel to this
ligament, are bundles of skeletal muscle fibers; the vocalis muscle.

7
TRACHEA
Thin walled tube, about 10cm length, and 2.5 cm diameter, extends from the
larynx into the thorax where it bifurcates into two primary bronchi. The wall consists of
three layers:
1- Mucosa: consists of respiratory epith. and lamina propria of loose connective
tissue, with diffuse lymphatic tissue, some times of nodular form.
2- Submucosa: loose connective tissue, rich in lymphatic tissue. It is separated
from lamina propria by an elastic membrane. Muco-serous glands; tracheal
glands also present that produce mucous fluid.
3- Cartilage layer: there are 16-20 C- shaped hyaline cartilage to keep tracheal
lumen opened.
A fibro-elastic ligament binds the open ends of the cartilage to prevent over
distention of the lumen. Deep to this ligament, a band of smooth muscle;
trachealis muscle regulates the lumen of trachea. The more flexible area
between the cartilages is supported by dense fibroelastic connective tissue
continuous with the perichondrium, to facilitate the extension of trachea if the
head is tilted back, or during respiration.
4- Adventitia: loose connective tissue rich in blood vessels and nerves.
8
BRONCHEAL TREE
The trachea divides into two main bronchi, each enters the lung through the hilum,
where arteries, veins, and lymphatics enter and leave the lungs, where they are nvested by
dense connective tissue.
Each primary bronchus course downwards dividing into three bronchi in the right
lung, and two in the left lung, each supply a pulmonary lobe. These lobar bronchi divide
repeatedly into bronchioles, then 5-7 terminal bronchioles.
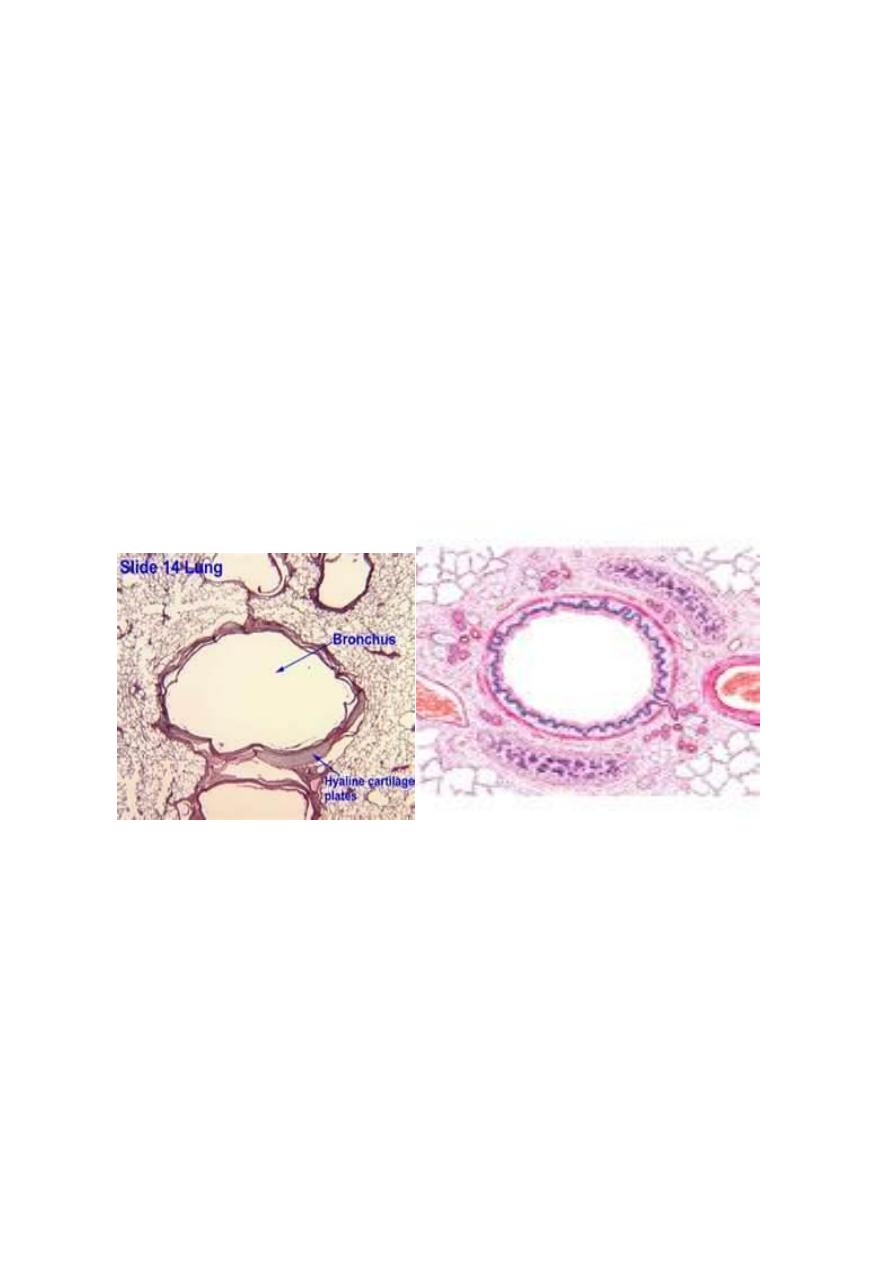
Bronchus:
Primary bronchus has the same histological structure as trachea, except that the
cartilage is a complete ring. At the level of secondary bronchus, the cartilage become as
an isolated plates.
Lamina propria is rich in elastic fibers, mucous and serous glands, lymphocytes, and
lymphatic nodules. Well developed smooth muscle fibers also present.
Primary bronchus Secondary bronchus
Bronchioles:
They are an intralobular air ways with a diameter of 1-5mm or less. They are lined by
respiratory epith., with few goblet cells. No glands and no cartilage present in their wall.
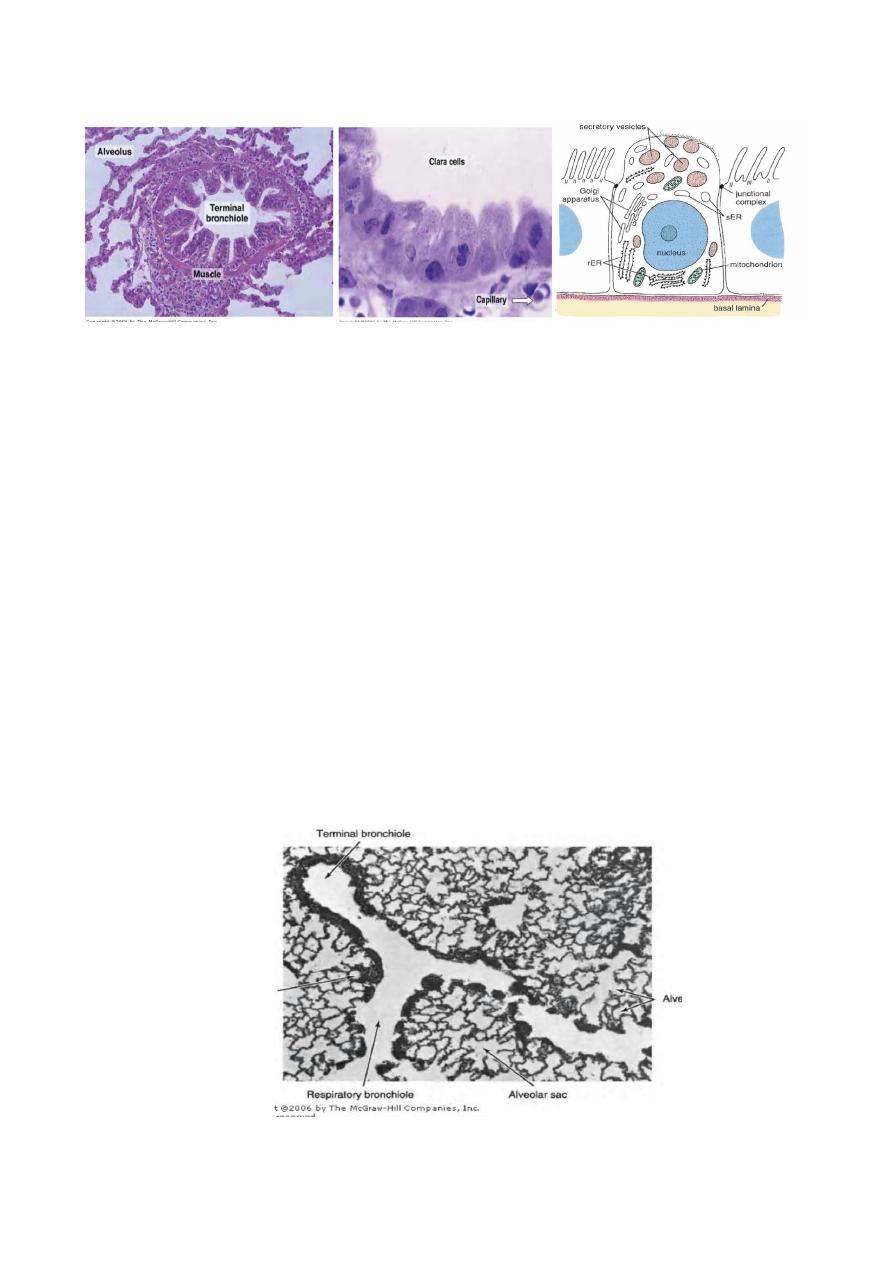
Terminal bronchioles:
They are lined by simple columnar or simple cuboidal cells, ciliated with Clara cells.
Clara cells are non ciliated, and have an apical secretary granules that secrete
glycosaminoglycans, which has a protective function against oxidative agents and
inflammation, and has a detoxifying effect on noxious inhaled particulate matters. Goblet
cells disappear above the level where ciliated cells disappear.
Lamina propria has smooth muscle fibers and elastic fibers arranged in a helical
crisscrossing pattern.
9
Terminal bronchiole Clara cell Clara cell
Bronchioles also exhibit specialized regions called neuroepithelial bodies. These are
formed by groups of 80-100 cells that contain secretory granules and receive cholinergic
nerve endings. Their function is poorly understood, but they are probably chemoreceptors
that react to changes in gas composition within the airway. They also may involved in
the reparative process of airway epithelial cell renewal after injury.
The increase in bronchiole diameter in response to stimulation of the sympathetic
nervous system explains why epinephrine and other sympathomimetic drugs are
frequently used to relax smooth muscle during asthma attacks. When the thickness of the
bronchial walls is compared with that of the bronchiolar walls, it can be seen that the
bronchiolar muscle layer is more developed. Increased airway resistance in asthma is
believed to be due mainly to contraction of bronchiolar smooth muscle.
Respiratory bronchioles:
Each terminal bronchiole gives two or three respiratory bronchioles. These are lined
by simple ciliated cuboidal cells, with non ciliated Clara cells.
Lamina propria is rich in smooth muscle fibers and elastic fibers. The wall of
respiratory bronchioles is interrupted by the alveolar sacs and alveolar ducts, where the
epith. changes into simple seq. epith.

11
Alveolar duct:
It is a tubular structure that is connected to the respiratory bronchioles. It is lined by
simple seq. epith.
Lamina propria has smooth muscles which disappear distally
, and replaced by
elastic and reticular fibers.
Alveolar sac:
It is a space where a group of alveoli open at each other. It is lined by simple seq. epith.,
and invested by elastic and reticular fibers. The elastic fibers are for the expansion and
contraction, while reticular fibers prevent over distention
.
Alveoli:
Sac like evaginations of respiratory bronchioles, alveolar ducts, and sacs. They are
about 200µm in diameter, and are specialized for O
2
and CO
2
exchange between air and
blood.
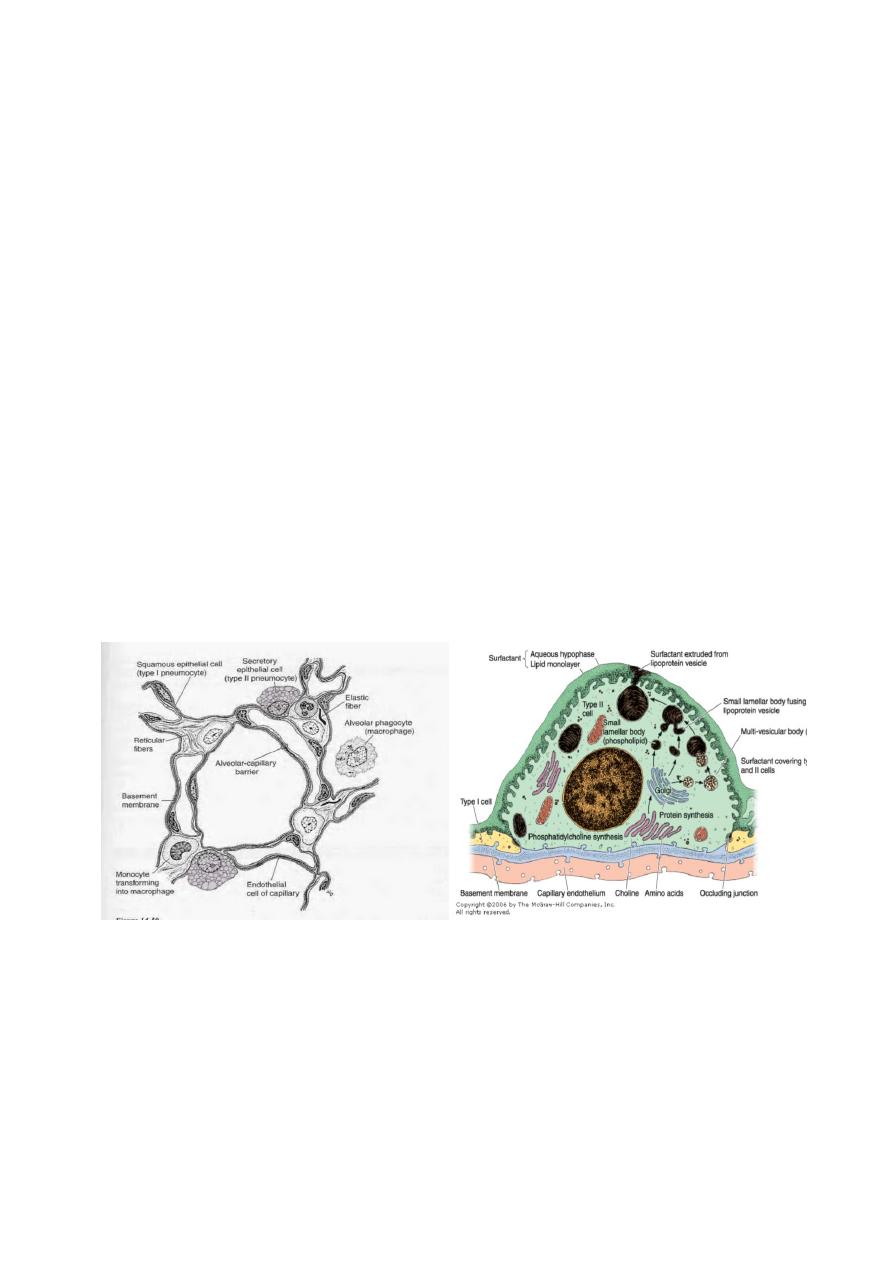
Each alveolus is lined by simple seq. epith., and is separated from adjacent alveolus
by the inter-alveolar septum. Within this septum, we have the Blood- Air Barrier which
separates the air in the alveolus from blood in the capillaries.
Blood-Air barrier consists of the following structures:
1- Cytoplasm of the alveolar cell wall.
2- Fused basal laminae of alveolar and capillary endothelial cells.
3- Cytoplasm of endothelial cells.
This barrier is about 0.1-1.5 µm in thickness.
There are four types of cells in the inter-alveolar septum:
1- Endothelial cells: extremely thin, where the nucleus and organelles are clustered in
one side to increase the efficiancy of gas exchange. It is of the continuous type, with
no fenestrae. The cytoplasm contains large number of pinocytotic vesicles.
11
2- Type Ι (sequamus alveolar cell): extremely thin cells, and constitute about 97% of the
alveolar surface. The organells are grouped around the nucleus, leaving large area of
free cytoplasm with large number of pinocytotic vesicles, to remove contaminants.
These cells act as a barrier with minimal thickness.
3- Type ΙΙ (great alveolar cells) or septal cells: they form only 3% of the alveolar
surface, found in between type Ι cells, and connected to them by desmosomes and
occluding junctions. They are cuboidal in shape, and found in groups at the angles of
alveolar wall. These cells are rich in mitochondria, RER, well developed Golgi
apparatus, with microvilli on their apical surface. Their cytoplasm contains lamellar
bodies of 1-2µm in diameter, that contain concentric or parallel lamellae limited by a
membrane. These bodies contain phospholipids, glycosaminoglycans, and proteins,
which are continuously synthesized and released at the apical surface. The lamellar
bodies produce the pulmonary surfactant, which spread over the alveolar surface as a
coating to lower their surface tention, so, less inspiratory force is needed to inflate the
alveoli, and also to prevent alveolar collapse during expiration. Type ΙΙ cells divide
by mitosis to replace their own type and typeΙ cells.
4- Macrophage: They are called dust cells, and seen on the surface of alveoli, also in the
connective tissue around major blood vessels or in the pleura. These cells phagocytize
debries that passed from alveolar lumen by pinocytotic vesicles of typeΙ cells.
Macrophages that found on the outer surface of the surfactant are carried to the
pharynx and swallowed. These macrophages originate from circulating monocytes in
adjacent capillaries.
Type ӀӀ alveolar cell
In congestive heart failure, the lungs become congested with blood, and erythrocytes
pass into the alveoli, where they are phagocytosed by alveolar macrophages. In such
cases, these macrophages are called heart failure cells when present in the lung and
sputum; they are identified by a positive histochemical reaction for iron pigment
(hemosiderin).
12
Alveolar pores: These are pores of 10-15µm diameter, found at the inter-alveolar
septum. They equalize the pressure between alveoli and act as collateral of air if a
bronchiole is obstructed.
Pulmonary blood vessels
They include two systems:
Systemic circulation: is the nutrient circulation for the lung. The vessels follow the
bronchial tree up to the respiratory bronchioles, where they will anastamose with small
branches of the pulmonary artery.
Pulmonary circulation: represents the functional circulation. Pulmonary arteries are
thin walled, because of the low pressure(25mmHg/5mmHg). Within the lungs, these
arteries branch, up to the level of alveolar ducts, where they will give off capillary
network in the inter-alveolar septum. Venules collect blood from capillaries. They have
thin wall of connective tissue, and they follow the bronchial tree towards the hilum.
Pulmonary lymphatic vessels
Superficial network: present at the visceral pleura, and it drains lymph into hilum.
Deep network: follow the bronchi and pulmonary vessels, drain into the hilar lymph
nodes. Lymphatic vessels are absent in the terminal bronchioles and alveolar ducts.
Pleura
Serous membrane that covers the lungs. It consists of two layers; parietal and
visceral. Pleura consists of mesothelial cells that rest on fine connective tissue layer of
collagen and elastic fibers. There is a cavity between parietal and visceral pleurae which
is lined by mesothelial cells, called pleural cavity. It contains a thin film of liquid act as a
lubricant for smooth sliding during respiration.

13
Lungs lie protected by the thoracic cage. Each lung is invaginated into its own pleural
cavity, which is accordingly reduced to a narrow potential space . This cavity is lined
with simple squamous serosal mesothelium, which together with a subserosal layer of
dense fibroelastic connective tissue constitutes a lining layer known as the pleura. At the
hilum of the lung, the site at which major blood vessels, air passages, lymphatics, and
nerves enter or emerge, the parietal pleura lining the walls of the pleural cavity is
continuous with the visceral pleura investing the lung.