Ear
Prof. Dr. Malak A. Al-yawer
Learning objectives
At the end of this lecture, the medical student will be able
to
List the embryonic origin of the different parts of the ear
Describe how the otic placode gives rise to coclea, saccule,
utricle, endolymphatic duct & semicircular ducts
Describe the embryonic origin of the different components
of the middle ear
Describe the embryonic origin of the different components
of the external ear
List the embryonic origin of the ear drum
State some clinical correlates
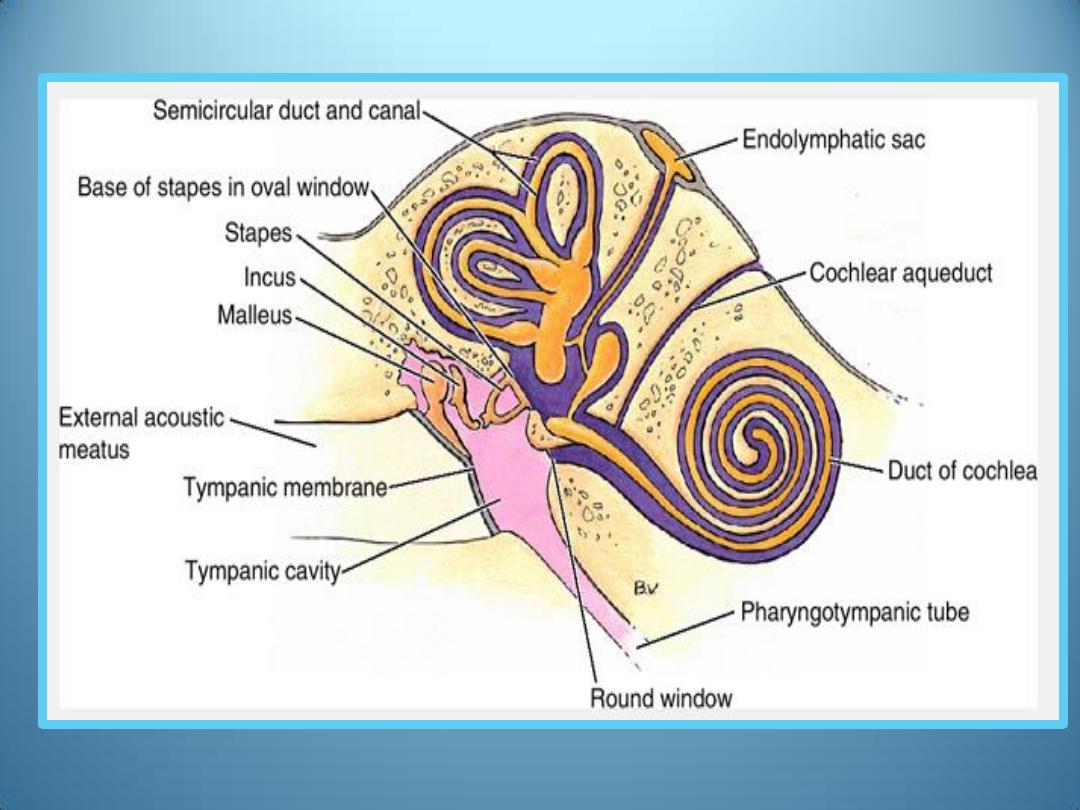
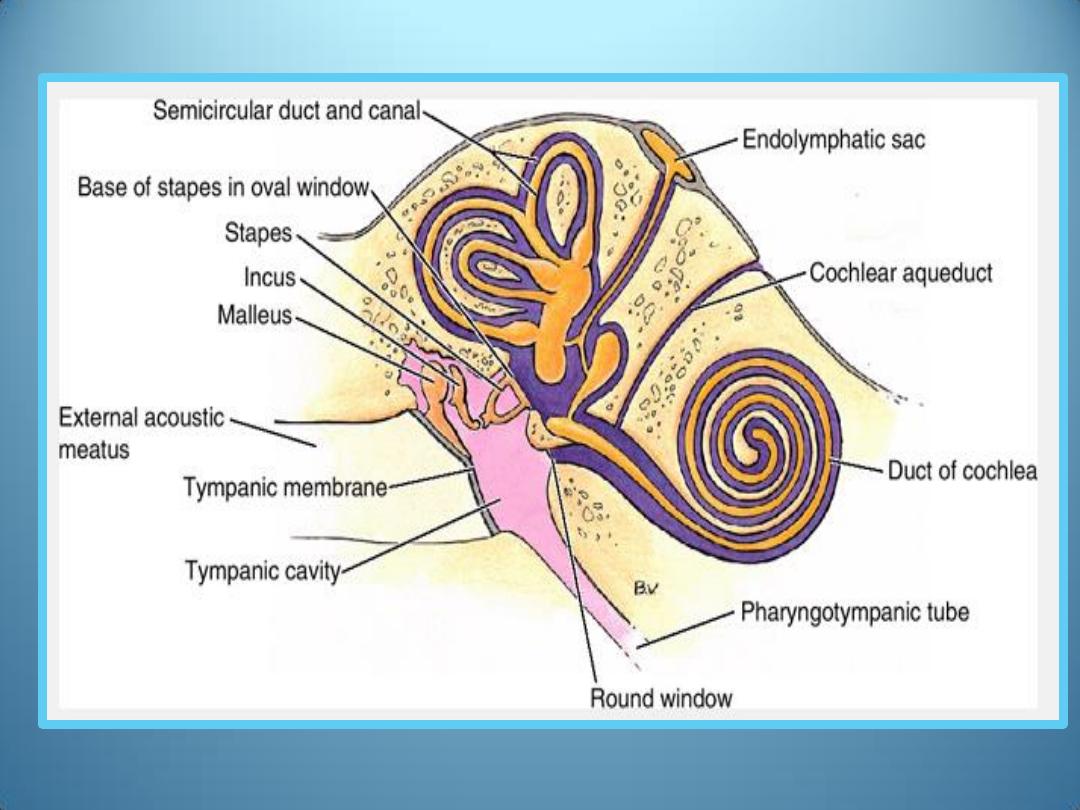
Internal Ear
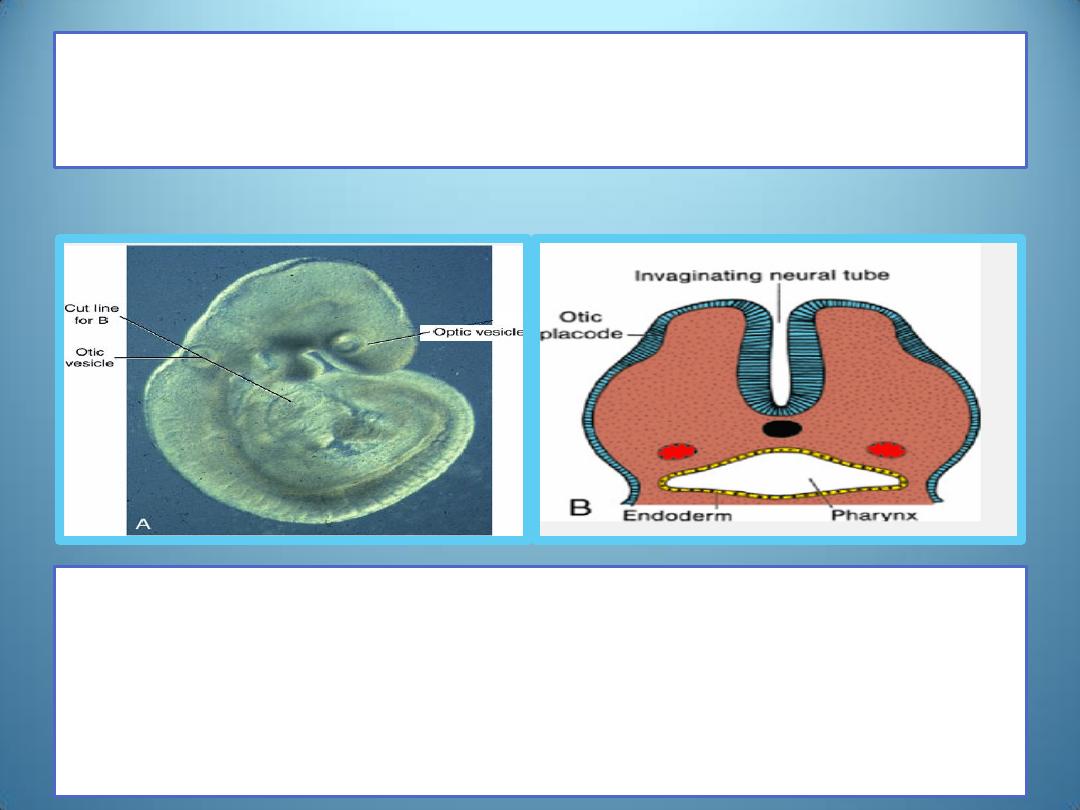
Otic placodes
• The first indication of the developing ear can be
found in embryos of approximately 22 days as a
thickening of the surface ectoderm on each side of
the rhombencephalon (otic placodes)
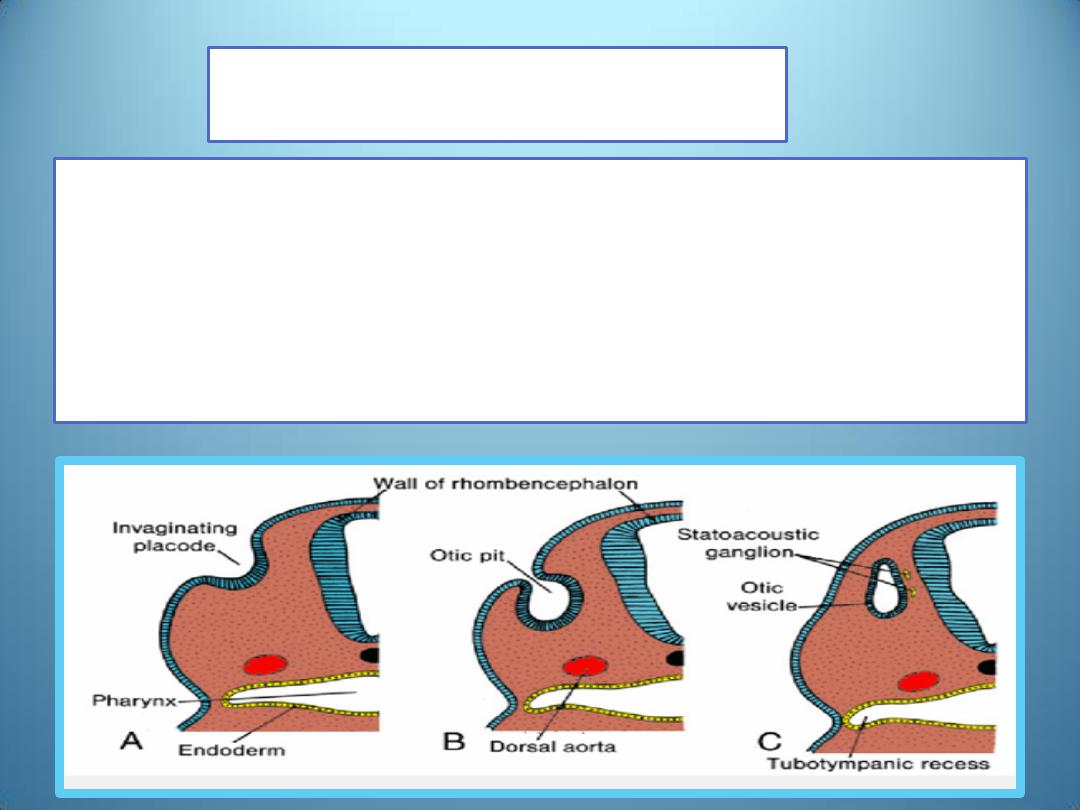
otic vesicles
• Each otic placode soon invaginates into the under-lying
mesenchyme and forms an otic pit.
• The edges of the otic pit soon come together and fuse to
form an otic vesicle.
• The otic vesicle then loses its connection with the surface
ectoderm
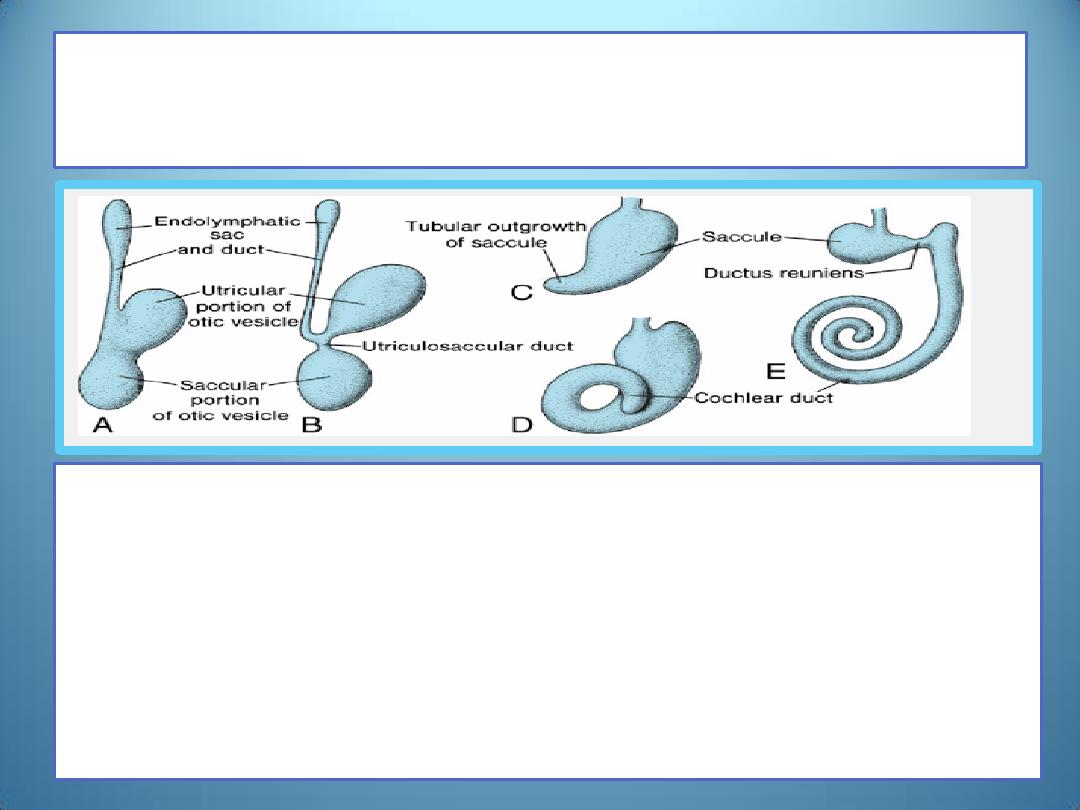
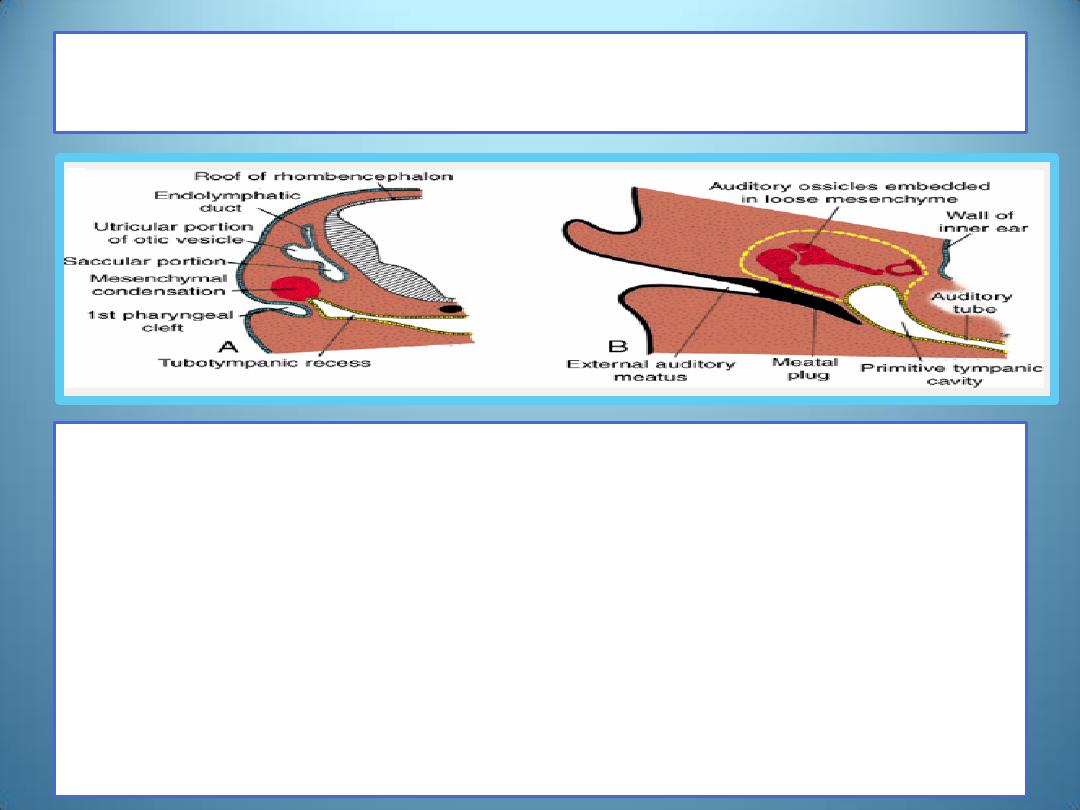
During later development, each vesicle
divides into
1.
a ventral component (saccular portion) that gives rise to the
saccule and cochlear duct
2.
a dorsal component (utricular portion with the
endolymphatic duct) that forms the utricle, semicircular
canals ,and endolymphatic duct .
•
Together, these epithelial structures form the membranous
labyrinth .
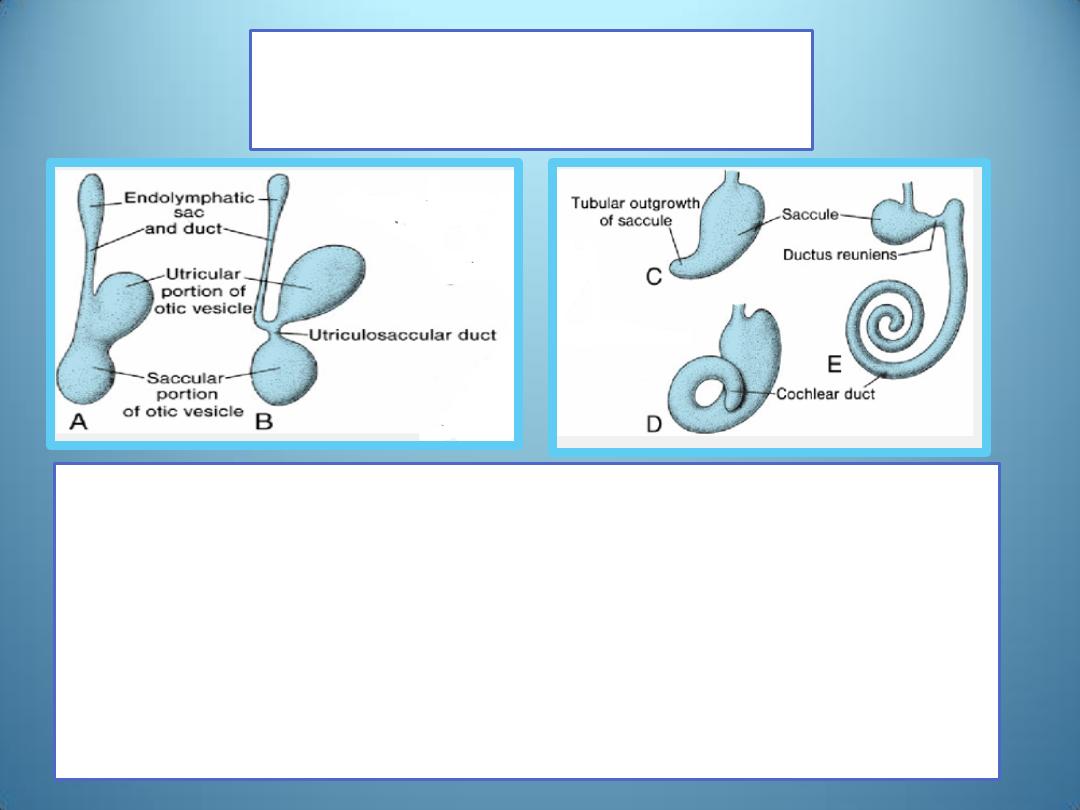
Saccule
(Cochlear duct)
• In the 6
th
week of development, the saccule forms a tubular
outpocketing (the cochlear duct) at its lower pole .
• This outgrowth, penetrates the surrounding mesenchyme in
a spiral fashion until the end of the 8
th
week, when it has
completed 2.5 turns .
• Its connection with the remaining portion of the saccule is
then confined to a narrow pathway, the ductus reuniens.
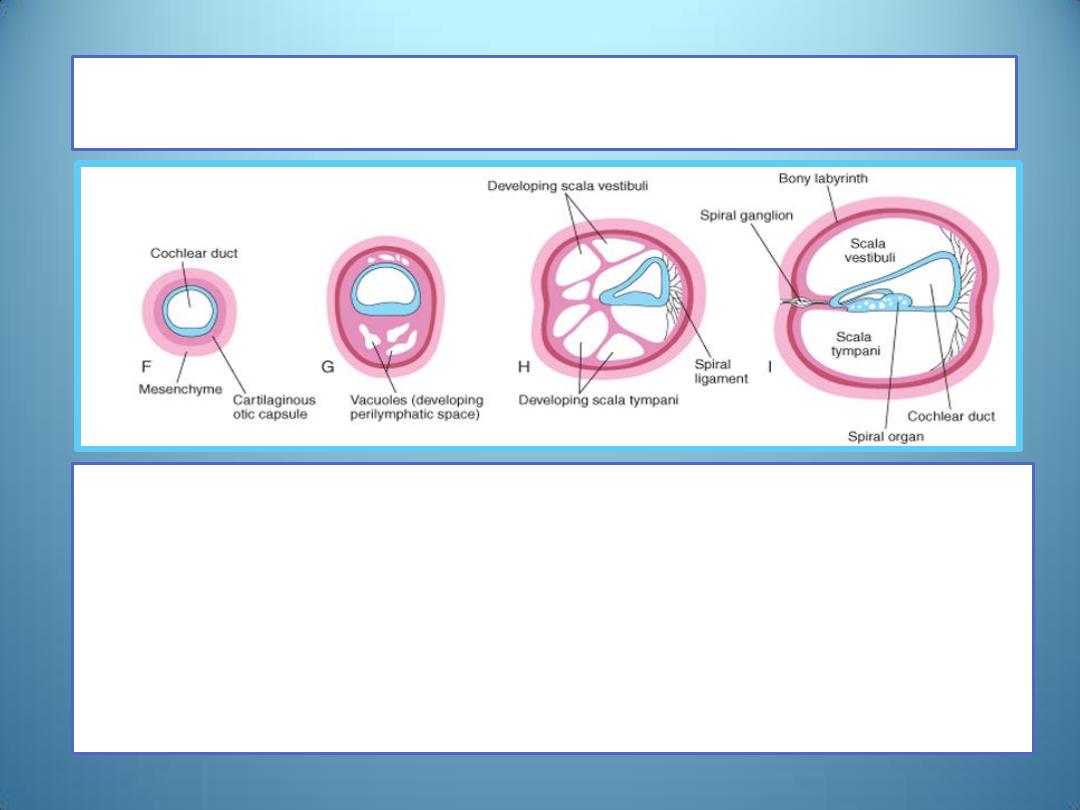
Scala tympani and Scala vestibuli
• Mesenchyme surrounding the cochlear duct soon
differentiates into cartilage.
• In the 10th week, this cartilaginous shell undergoes
vacuolization, and two perilymphatic spaces, the scala
vestibuli and scala tympani are formed.
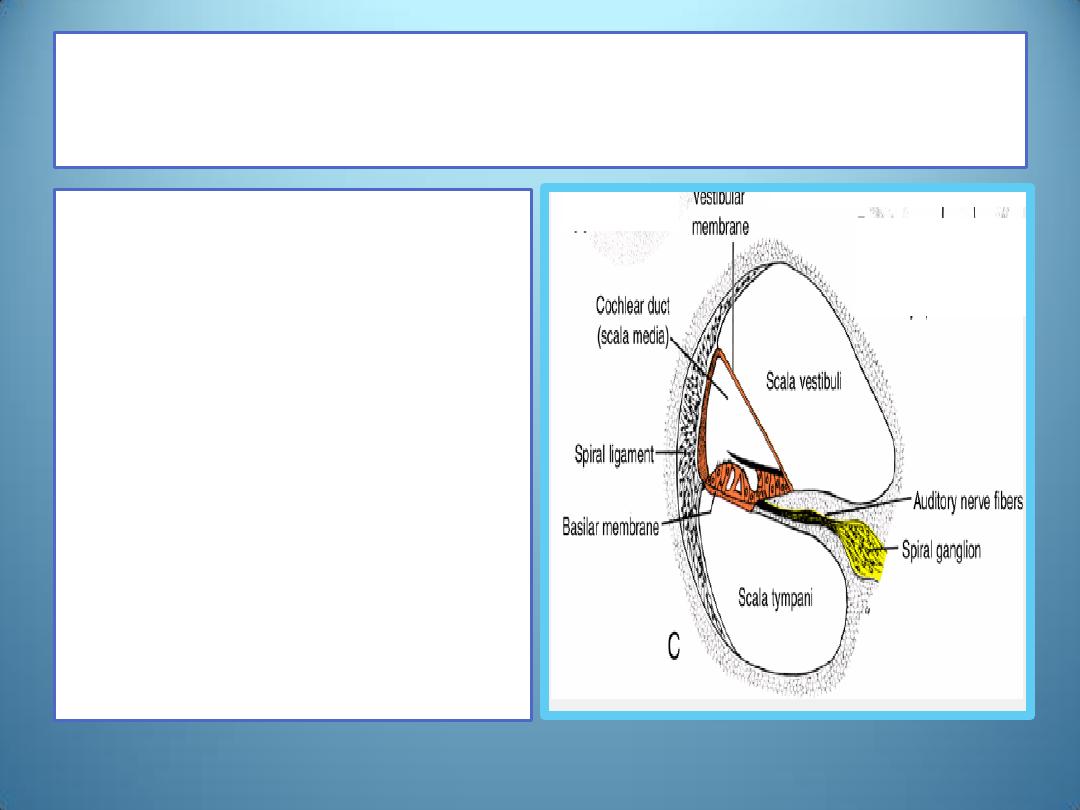
Vestibular membrane and Basilar
membrane
• The cochlear duct is
then separated from
the scala vestibuli by
the vestibular
membrane and from
the scala tympani by
the basilar membrane.
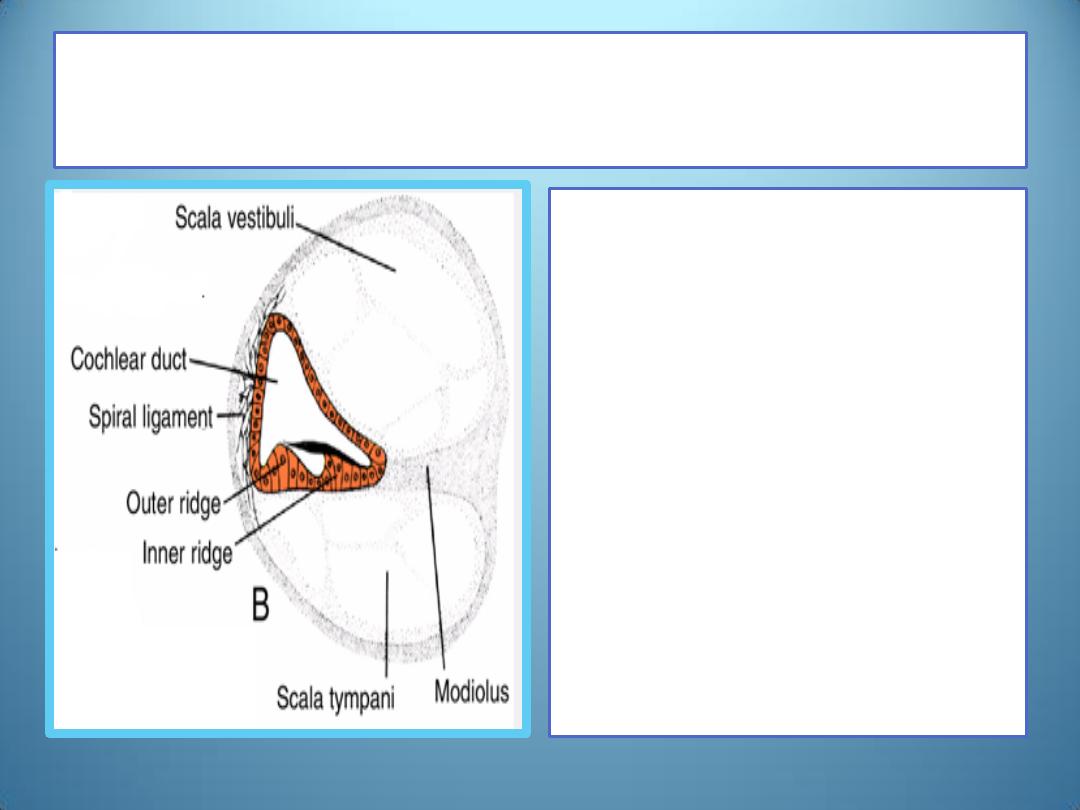
Spiral ligament and Modiolus
• The lateral wall of the
cochlear duct remains
attached to the surrounding
cartilage by the spiral
ligament ,whereas its
median angle is connected
to and partly supported by a
long cartilaginous process,
the modiolus ,the future
axis of the bony cochlea.
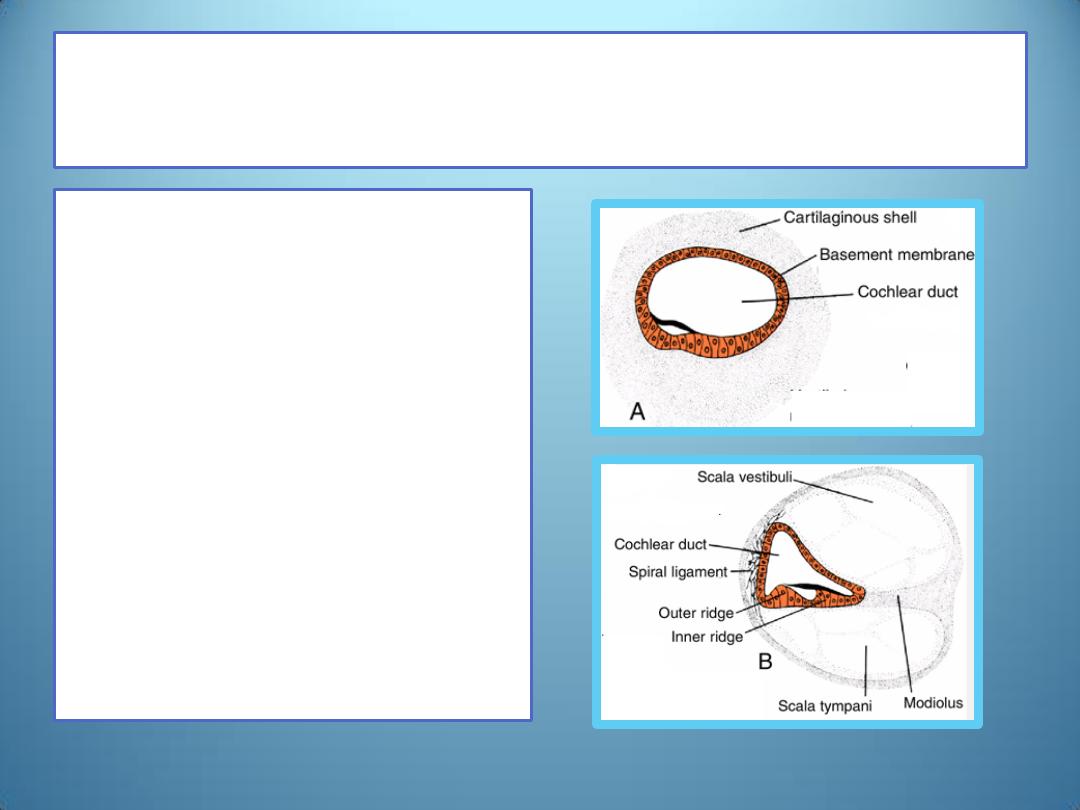
The inner ridge and the outer ridge
• Initially, epithelial cells
of the cochlear duct are
alike.
• With further
development, they form
two ridges:
the inner ridge( the
future spiral limbus)
the outer ridge.
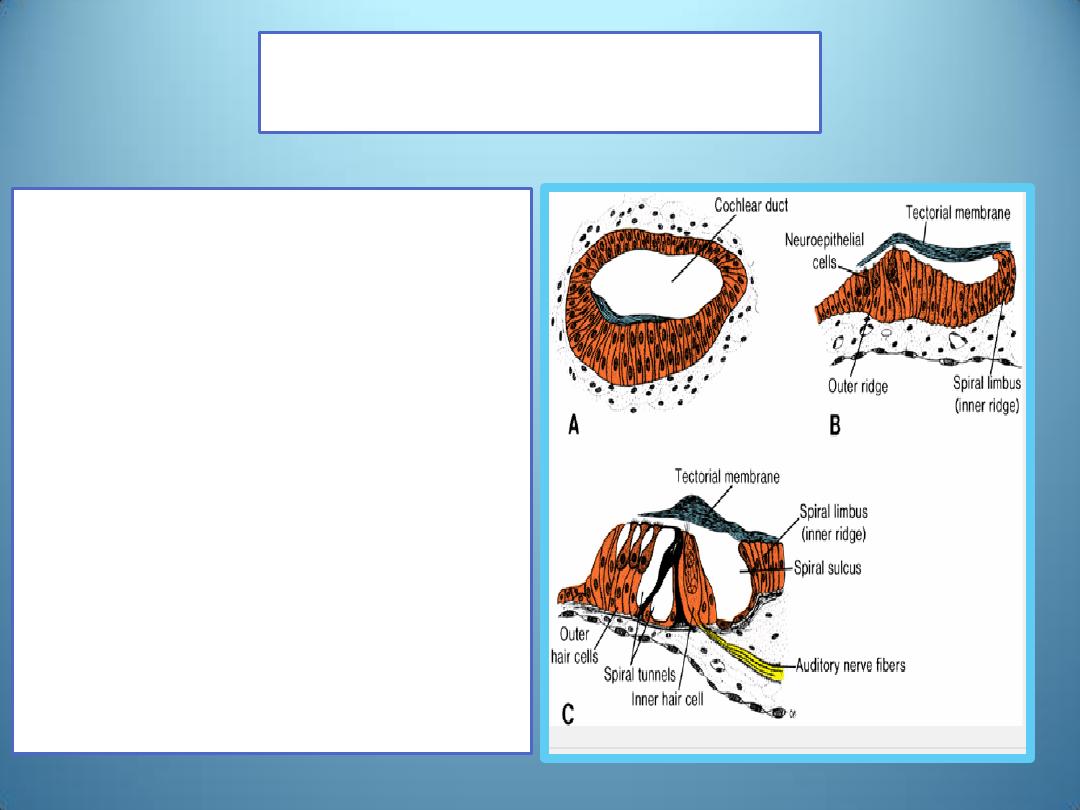
Organ of Corti
• The outer ridge forms one row
of inner and three or four rows
of outer hair cells ,the sensory
cells of the auditory system.
• They are covered by the
tectorial membrane ,a fibrillar
gelatinous substance attached
to the spiral limbus that rests
with its tip on the hair cells
• The sensory cells and tectorial
membrane together constitute
the organ of Corti .
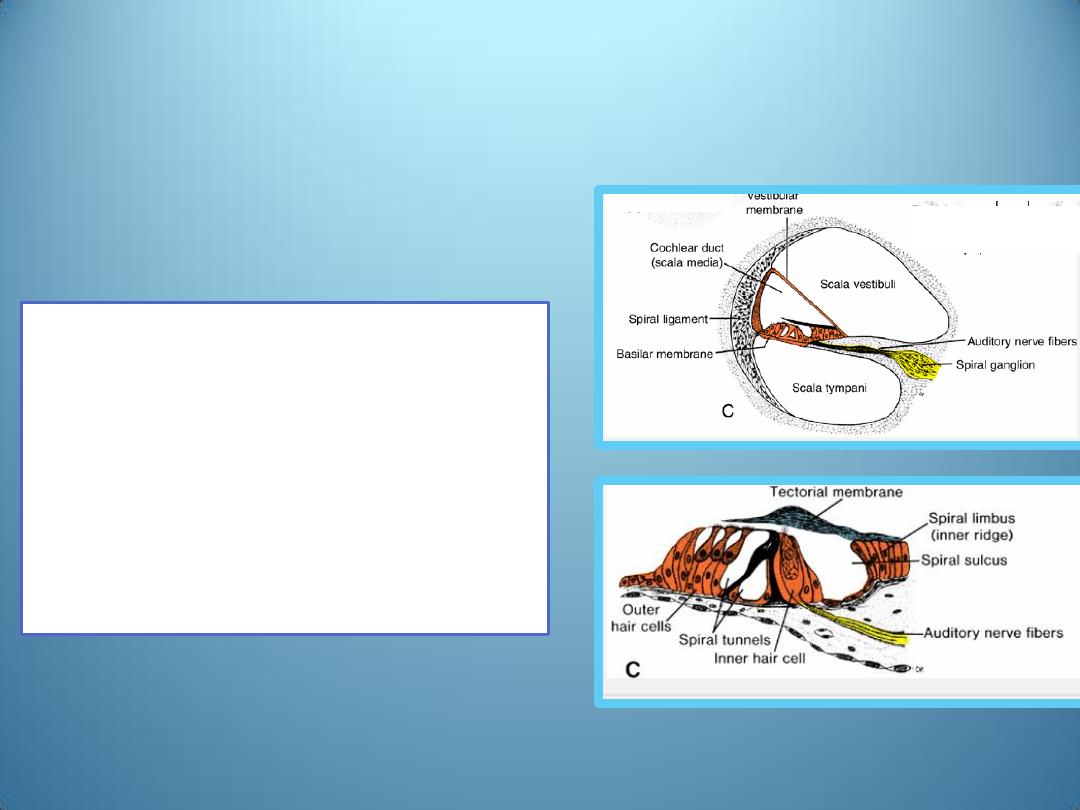
• Impulses received by this
organ are transmitted to
the spiral ganglion and
then to the nervous
system by the auditory
fibers of cranial nerve VIII
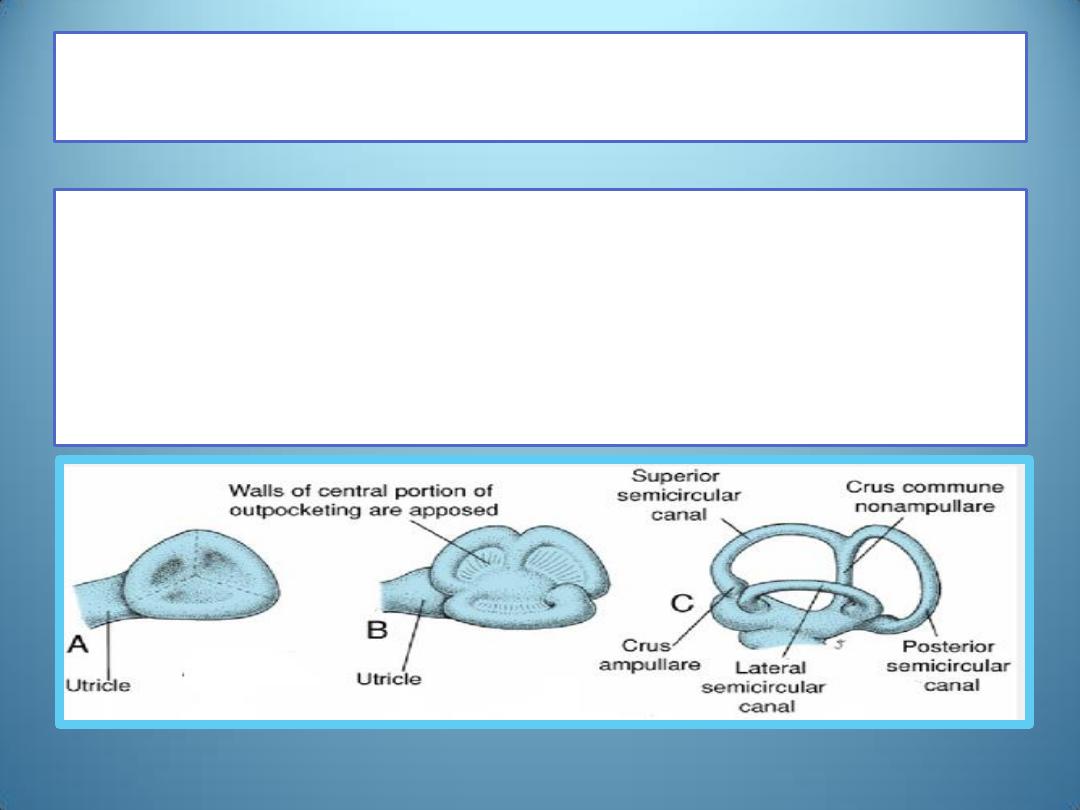
Utricle and Semicircular Canals
• During the 6
th
week of development ,semicircular canals appear as
flattened outpocketings of the utricular part of the otic vesicle.
• Central portions of the walls of these outpocketings eventually
appose each other and disappear, giving rise to three semicircular
canals
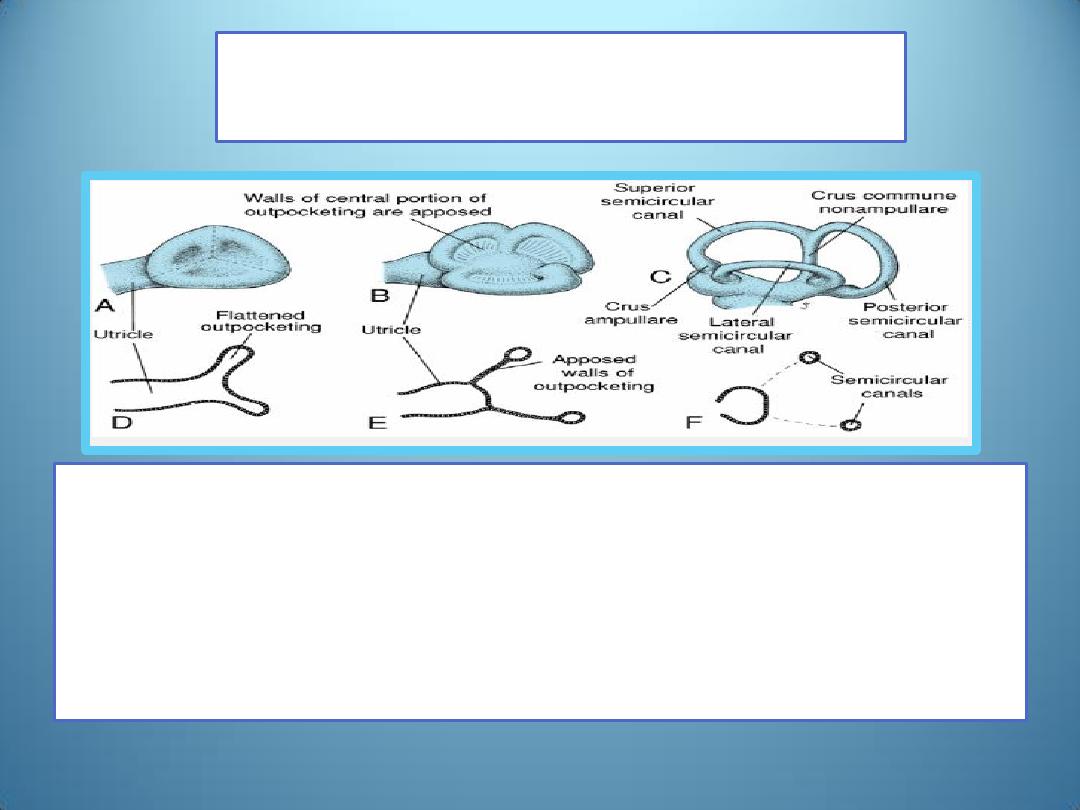
Semicircular Canals
• Whereas one end of each canal dilates to form the crus
ampullare ,the other, the crus nonampullare ,does not widen
• Since two of the latter type fuse, however, only five crura
enter the utricle, three with an ampulla and two without.
Crista ampullaris & Maculae acusticae
• Cells in the ampullae form a crest, the crista
ampullaris ,containing sensory cells for maintenance
of equilibrium.
• Similar sensory areas, the maculae acusticae ,
develop in the walls of the utricle and saccule.
• Impulses generated in sensory cells of the cristae and
maculae as a result of a change in position of the
body are carried to the brain by vestibular fibers of
cranial nerve VIII.
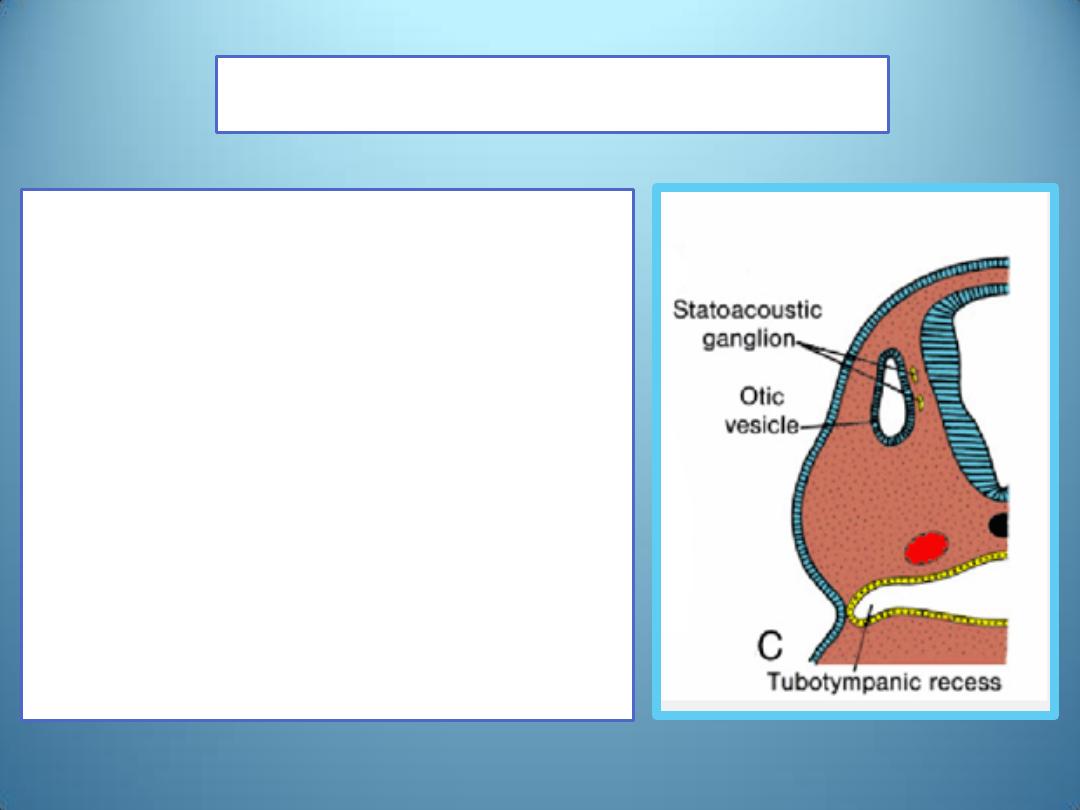
Statoacoustic ganglion
• During formation of the otic
vesicle, a small group of cells
breaks away from its wall and
forms the statoacoustic ganglion
• Other cells of this ganglion are
derived from the neural crest.
• The ganglion subsequently splits
into cochlear and vestibular
portions, which supply sensory
cells of the organ of Corti and
those of the saccule, utricle, and
semicircular canals, respectively
.
Middle Ear /The tympanic cavity
• originates in the endoderm,
• is derived from the first pharyngeal pouch
• This pouch expands in a lateral direction and comes in contact
with the floor of the first pharyngeal cleft.
• The distal part of the pouch, the tubotympanic recess ,
widens and gives rise to the primitive tympanic cavity, and
• the proximal part remains narrow and forms the auditory
tube
( eustachian tube, through which the tympanic cavity
communicates with the nasopharynx.
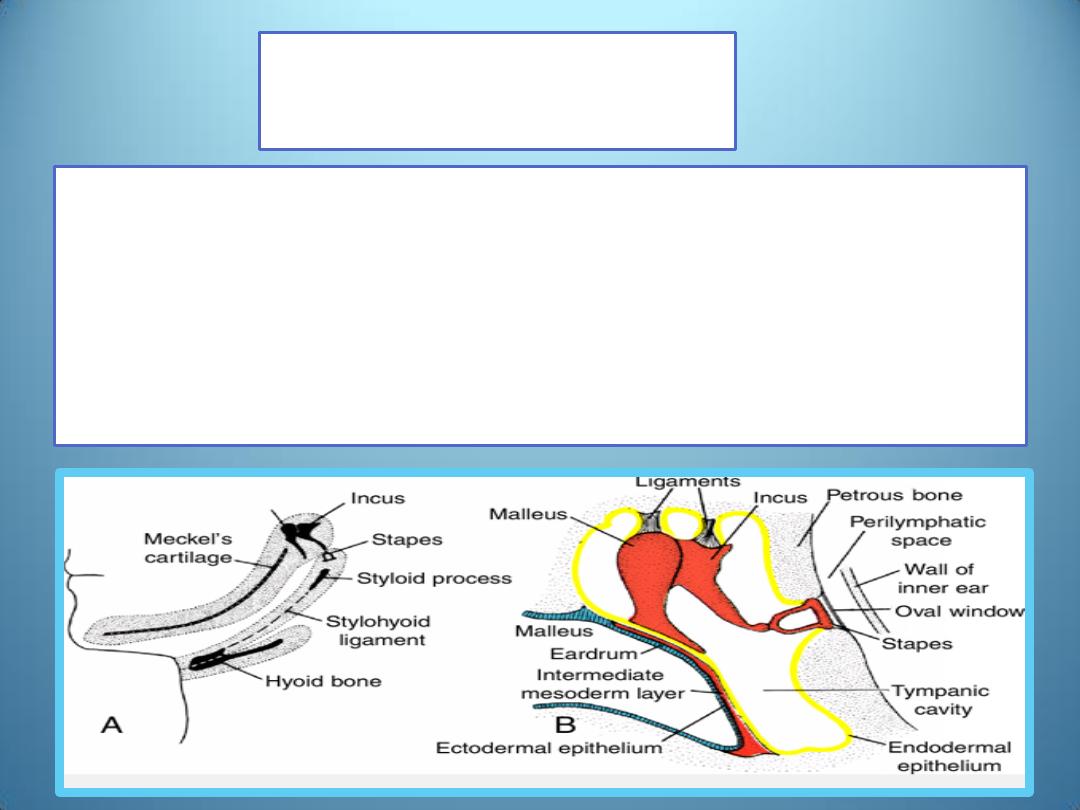
Ossicles
• The malleus and incus are derived from cartilage of the first
pharyngeal arch, and the stapes is derived from that of the
second arch
• Although the ossicles appear during the first half of fetal life,
they remain embedded in mesenchyme until the 8
th
month
when the surrounding tissue dissolves.
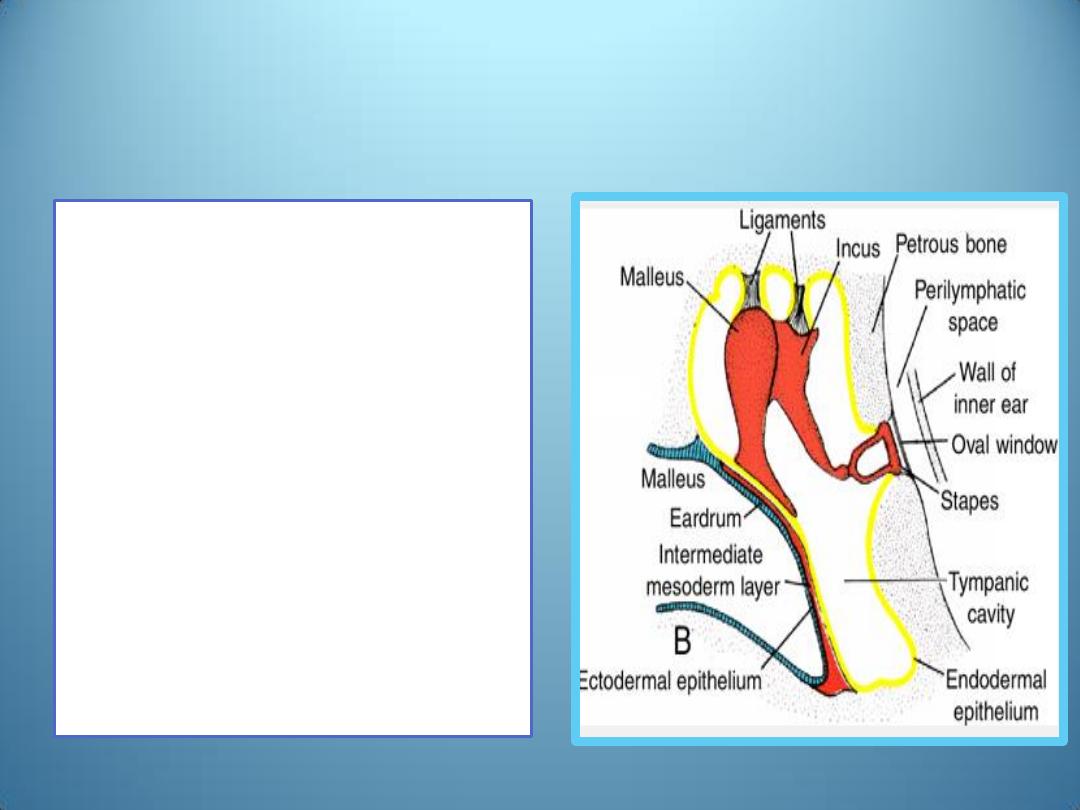
• The endodermal epithelial lining
of the primitive tympanic cavity
then extends along the wall of
the newly developing space.
• The tympanic cavity is now at
least twice as large as before.
• When the ossicles are entirely
free of surrounding mesenchyme,
the endodermal epithelium
connects them in a mesentery-
like fashion to the wall of the
cavity .
• The supporting ligaments of the
ossicles develop later within
these mesenteries .
• Since the malleus is derived from the 1
st
pharyngeal arch, its muscle, the tensor
tympani ,is innervated by the mandibular
branch of the trigeminal nerve
• The stapedius muscle ,which is attached to
the stapes, is innervated by the facial nerve ,
the nerve to the 2
nd
pharyngeal arch.
Mastoid antrum
• During the late fetal period,
expansion of the tympanic
cavity gives rise to the
mastoid antrum, located in
the petromastoid part of the
temporal bone.
• The mastoid antrum is
almost adult size at birth;
however, no mastoid cells are
present in newborn infants.
• By 2 years of age, the
mastoid cells are well
developed and produce
conical projections of the
temporal bones, the mastoid
processes.
• The middle ear continues to
grow through puberty.
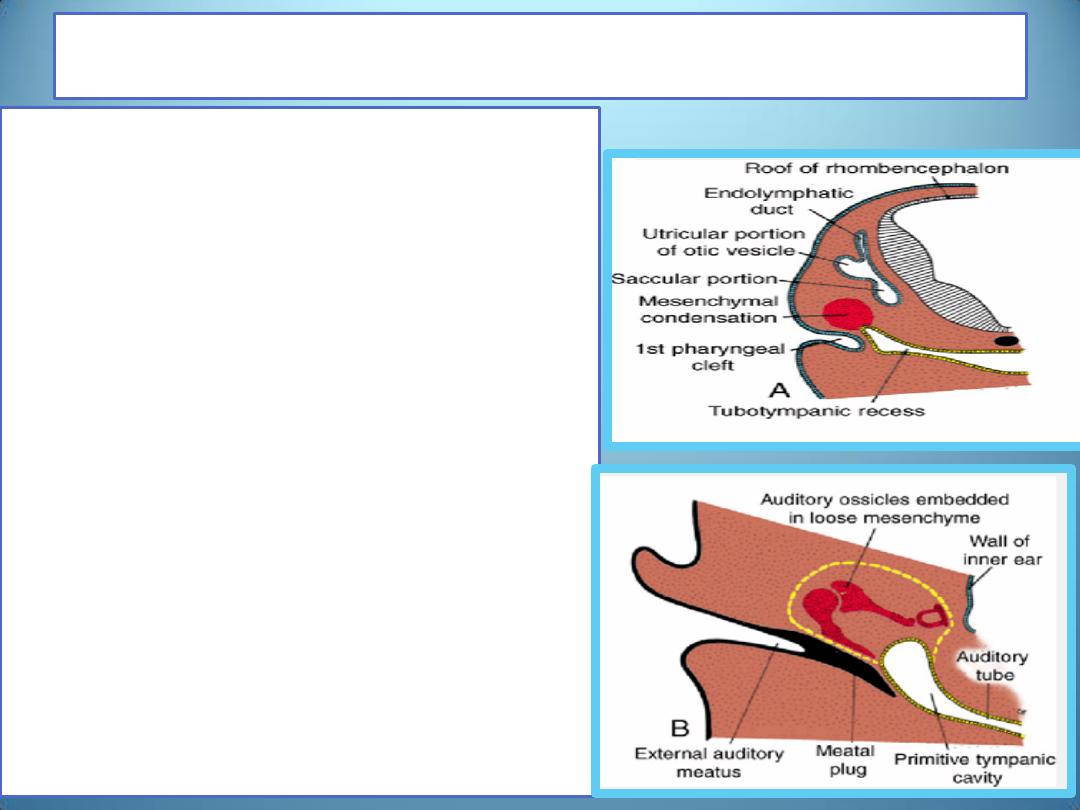
The external auditory meatus
• develops from the dorsal portion of
the 1
st
pharyngeal cleft
• At the beginning of the 3
rd
month,
epithelial cells at the bottom of the
meatus proliferate, forming a solid
epithelial plate, the meatal plug
• In the 7
th
month, this plug dissolves
and the epithelial lining of the floor
of the meatus participates in
formation of the definitive eardrum.
• Occasionally, the meatal plug
persists until birth, resulting in
congenital deafness.
• The external acoustic meatus,
relatively short at birth, attains its
adult length in approximately the 9
th
year.
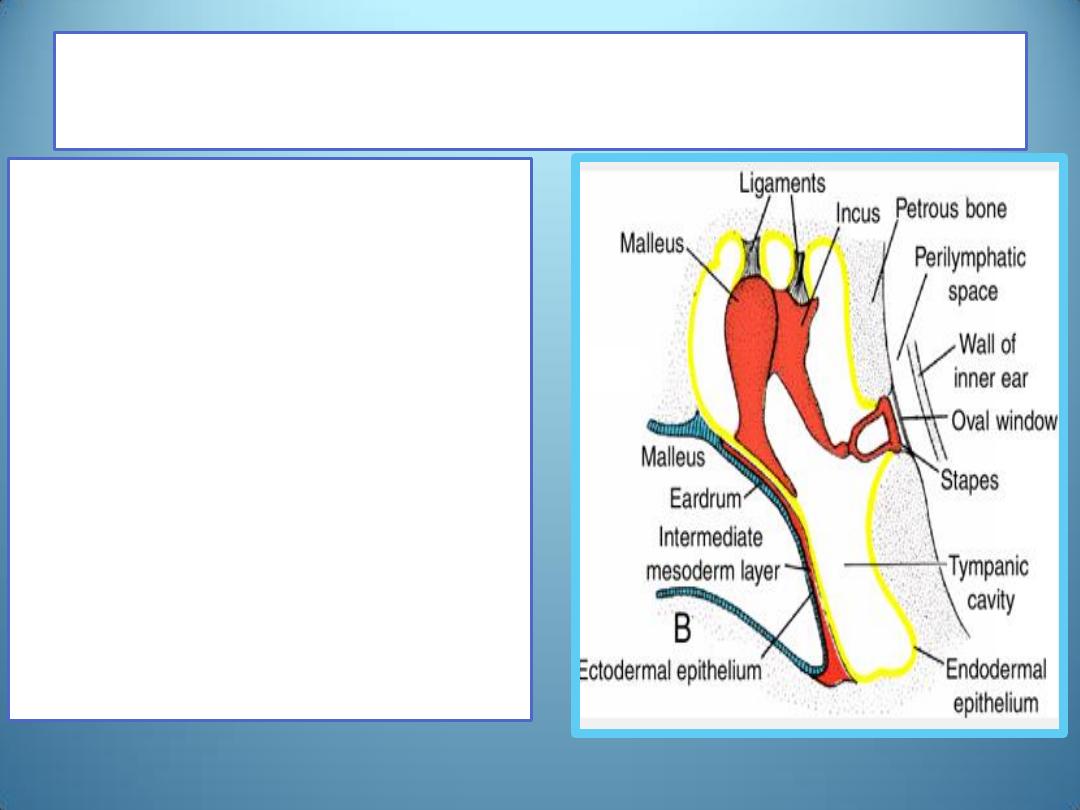
Eardrum or Tympanic Membrane
•
The eardrum is made up of
1. ectodermal epithelial lining at
the bottom of the auditory
meatus ,
2. endodermal epithelial lining
of the tympanic cavity, and
3. an intermediate layer of
connective tissue that forms
the fibrous stratum.
•
The major part of the
eardrum is firmly attached to
the handle of the malleus and
the remaining portion forms
the separation between the
external auditory meatus and
the tympanic cavity.
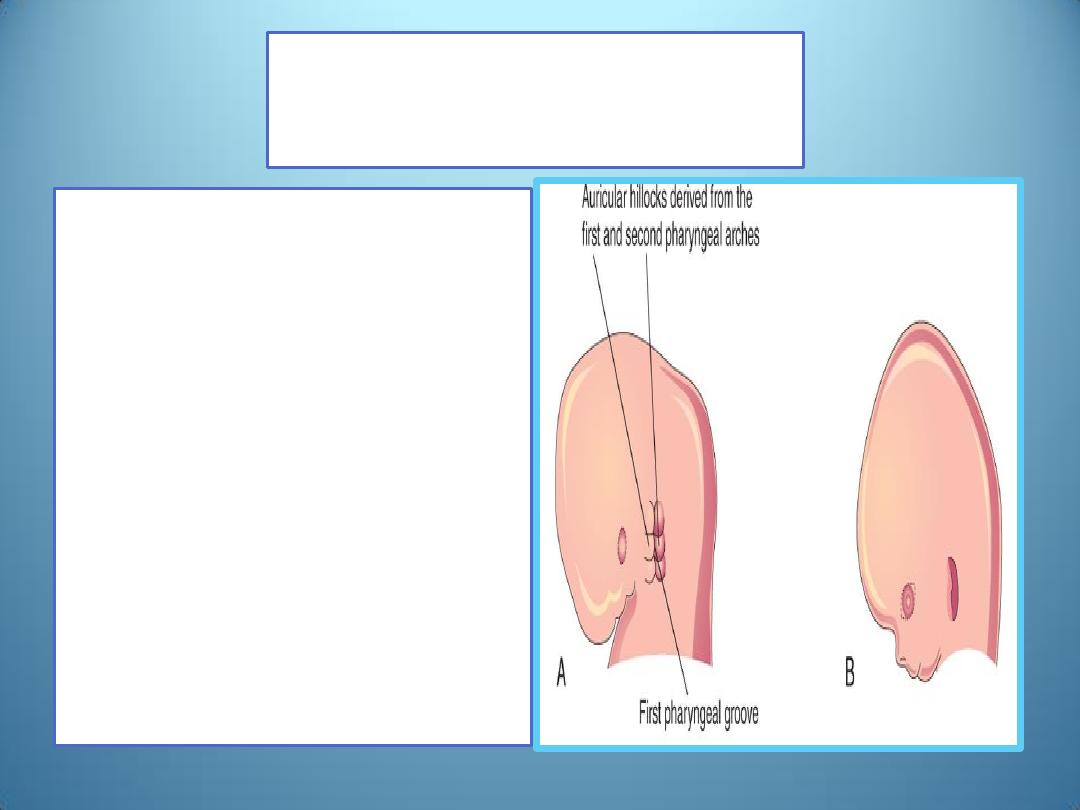
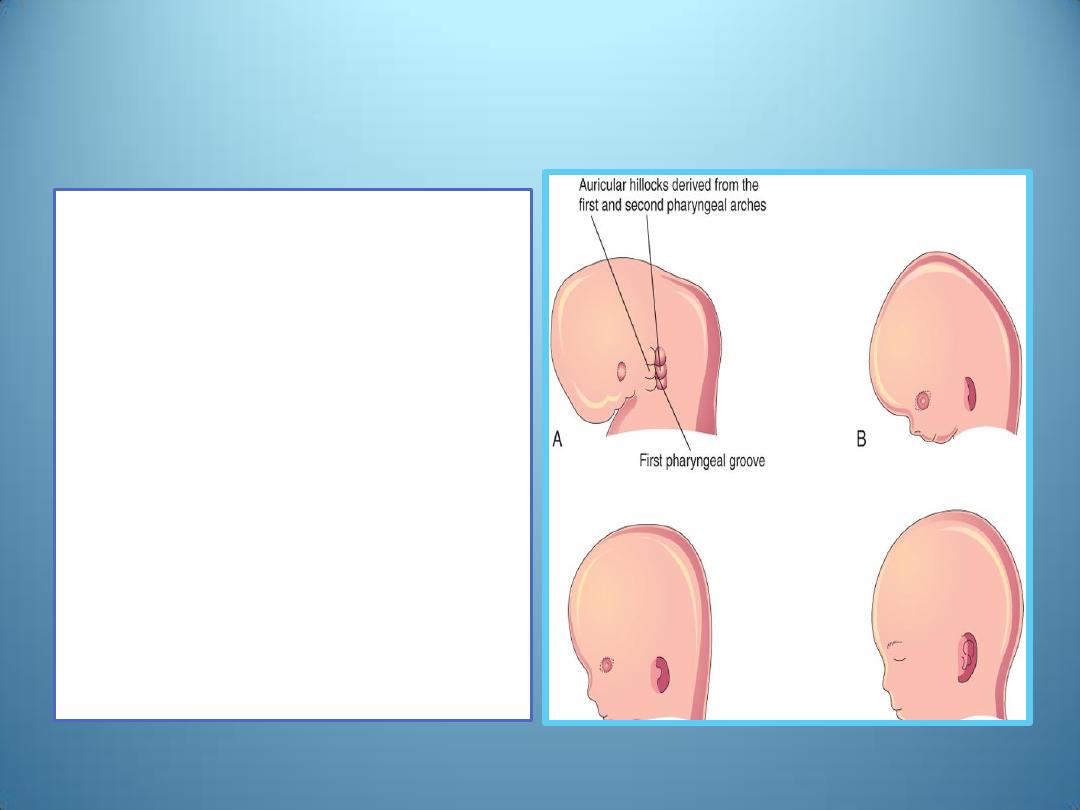
Auricle
• develops from six
mesenchymal
proliferations at the
dorsal ends of the first
and second pharyngeal
arches ,surrounding the
1
st
pharyngeal cleft.
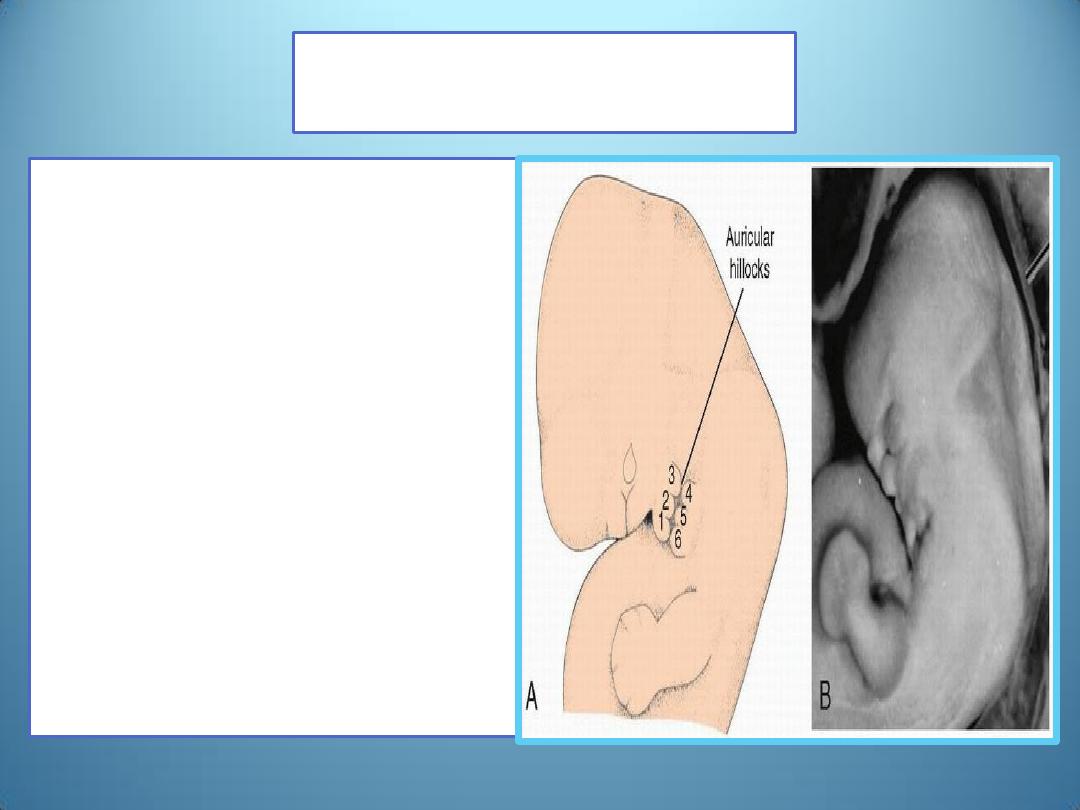
Auricle
Note that
hillocks 1, 2, and 3 are part
of the mandibular portion of
the 1
st
pharyngeal arch
the ear lies horizontally at
the side of the neck. At this
stage, the mandible is small.
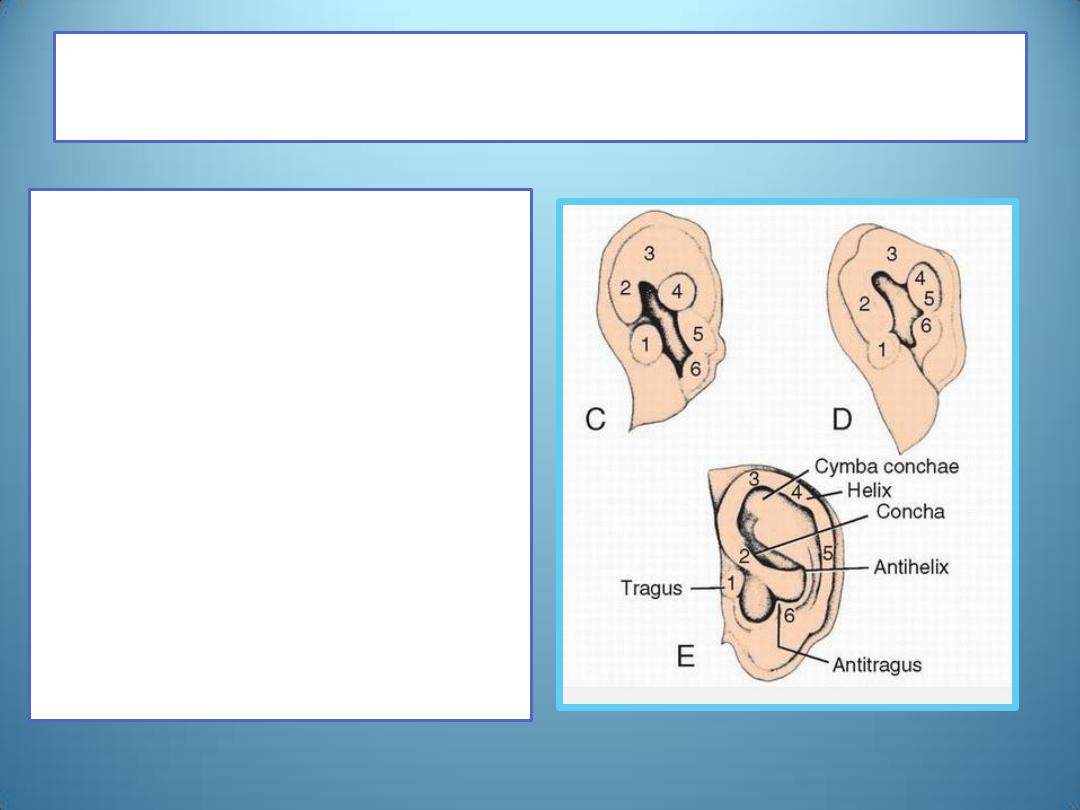
Auricular hillocks
• These swellings (auricular
hillocks) ,three on each
side of the external
meatus, later fuse and
form the definitive
auricle.
• As fusion of the auricular
hillocks is complicated,
developmental
abnormalities of the auricle
are common.
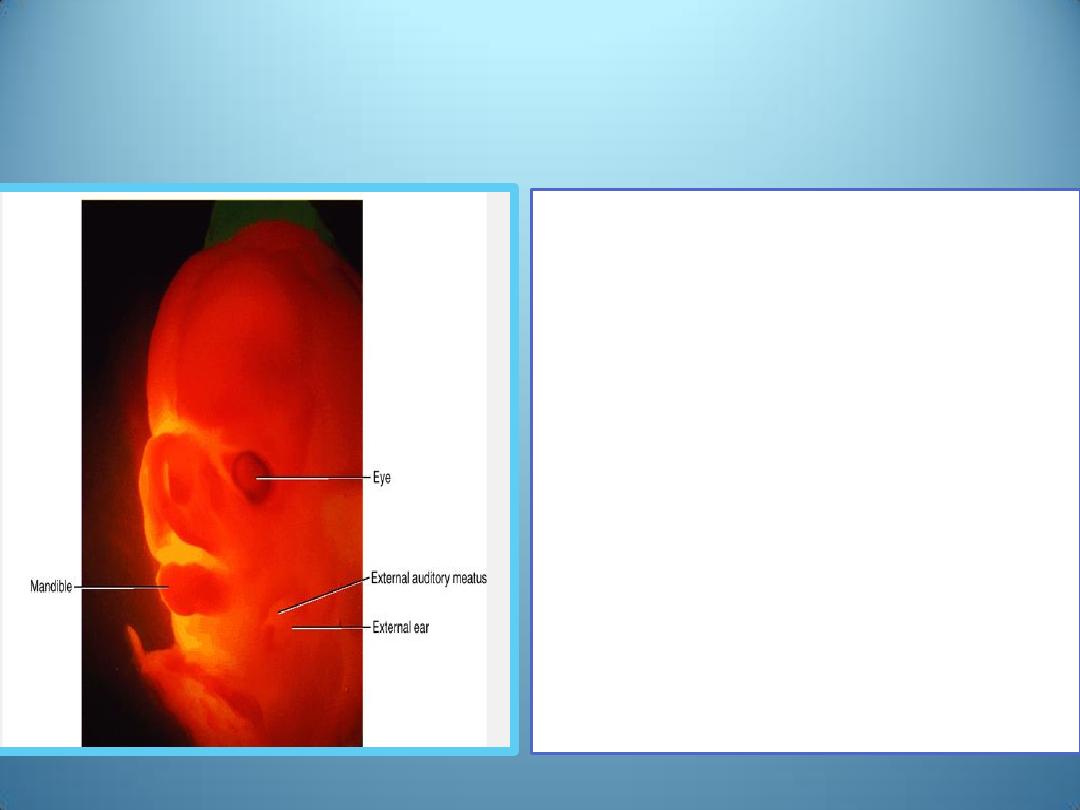
• Initially, the external ears
are in the lower neck region
but with development of
the mandible, they ascend
to the side of the head at
the level of the eyes.
•
The parts of the auricle derived from
the first pharyngeal arch are supplied
by its nerve, the mandibular branch
of the trigeminal nerve ;
•
the parts derived from the second
arch are supplied by cutaneous
branches of the cervical plexus,
especially the lesser occipital and
greater auricular nerves
•
The facial nerve of the second
pharyngeal arch has few cutaneous
branches; some of its fibers
contribute to the sensory innervation
of the skin in the mastoid region and
probably in small areas on both
aspects of the auricle .
Congenital deafness
may be caused by
1. abnormal development of the
membranous and bony
labyrinths or
2. by malformations of the
auditory ossicles and eardrum.
3. In the most extreme cases, the
tympanic cavity and external
meatus are absent.
• Most forms of congenital
deafness are caused by
1. genetic factors, but
2. environmental factors may
also interfere with normal
development of the internal
and middle ear.
• Rubella virus, affecting the
embryo in the seventh or
eighth week, may cause
severe damage to the organ of
Corti.
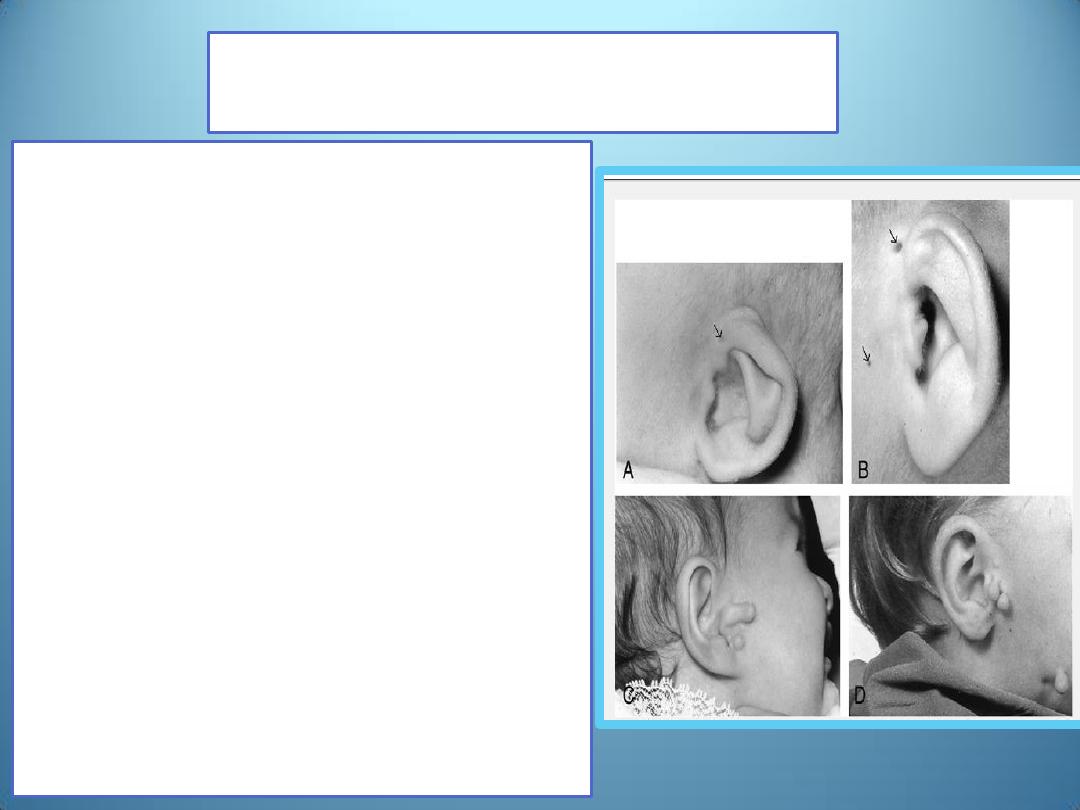
External ear defects
• are common; they include minor
and severe abnormalities
• They are significant
1. from the standpoint of the
psychological and emotional
trauma they may cause and
2. for the fact they are often
associated with other
malformations.
• Thus, they serve as clues to
examine infants carefully for other
abnormalities .All of the frequently
occurring chromosomal syndromes
and most of the less common ones
have ear anomalies as one of their
characteristics.
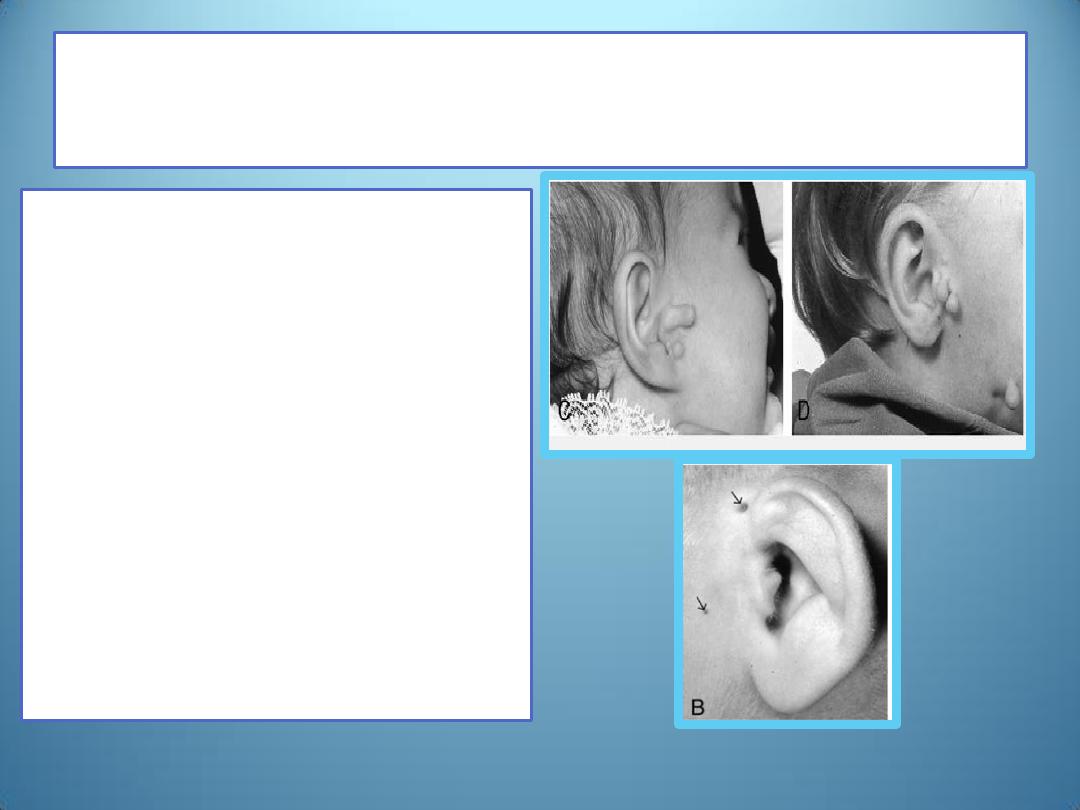
Preauricular appendages and pits
• are skin tags and shallow
depressions, respectively,
anterior to the ear.
• Pits may indicate abnormal
development of the auricular
hillocks, whereas appendages
may be due to accessory
hillocks. Like other external
ear defects, both are
associated with other
malformations.
Summary
• The internal ear originates from the otic vesicle, which in
the fourth week of development detaches from surface
ectoderm.
• This vesicle divides into a ventral component, which gives
rise to the saccule and cochlear duct and a dorsal
component, which gives rise to the utricle, semicircular
canals, and endolymphatic duct
• The middle ear(tympanic cavity and auditory tube) is
derived from the first pharyngeal pouch.
• The ossicles are derived from the first (malleus and incus)
and second (stapes) pharyngeal arches
• The external auditory meatus develops from the first
pharyngeal cleft
• The auricle develops from six mesenchymal hillocks along
the first and second pharyngeal arches.