Skeletal System
Prof. Dr. Malak A. Al-yawer
Department of Anatomy/Embryology Section
At the end of this lecture, the medical student will
be able to
•
State the embryonic origin of skeletal system
•
Define Mesenchyme (embryonic connective tissue)
•
Distinguish between the two types of ossification
•
Describe the embryonic development of the skull( neurocranium and
viscerocranium)
•
State the embryonic origin of sutures
•
State the characteristic of new born skull
•
Describe the embryonic development of the vertebrae
•
State the significance of re segmentation in development of vertebral column
•
State the embryonic development of ribs and sternum
•
State the embryonic development of limbs
•
Define apical ectodermal ridge and progress zone
•
Distinguish between the embryonic development of the forelimbs and hindlimbs
•
Define the embryonic origin of joints
•
State the significance of appearance of ossification centers in determination of
bone age
•
State some clinical correlates
The skeletal system develops from
• paraxial mesoderm
• lateral plate (parietal layer)
mesoderm
• neural crest.

Somites differentiate into
Sclerotome
dermomyotome.
At the end of the fourth week,
sclerotome cells form a loosely
woven tissue, the
Mesenchyme, or embryonic
connective tissue.
Mesenchymal cells may
become
fibroblasts
chondroblasts,
osteoblasts
Mesenchyme in the parietal layer of the lateral
plate mesoderm of the body wall forms bones of
the
pelvic and shoulder girdles
limbs
sternum
Neural crest cells in the head region differentiate
into mesenchyme and participate in formation of
bones of the face and skull.
Occipital somites and somitomeres contribute to
formation of the cranial vault and base of the
skull.
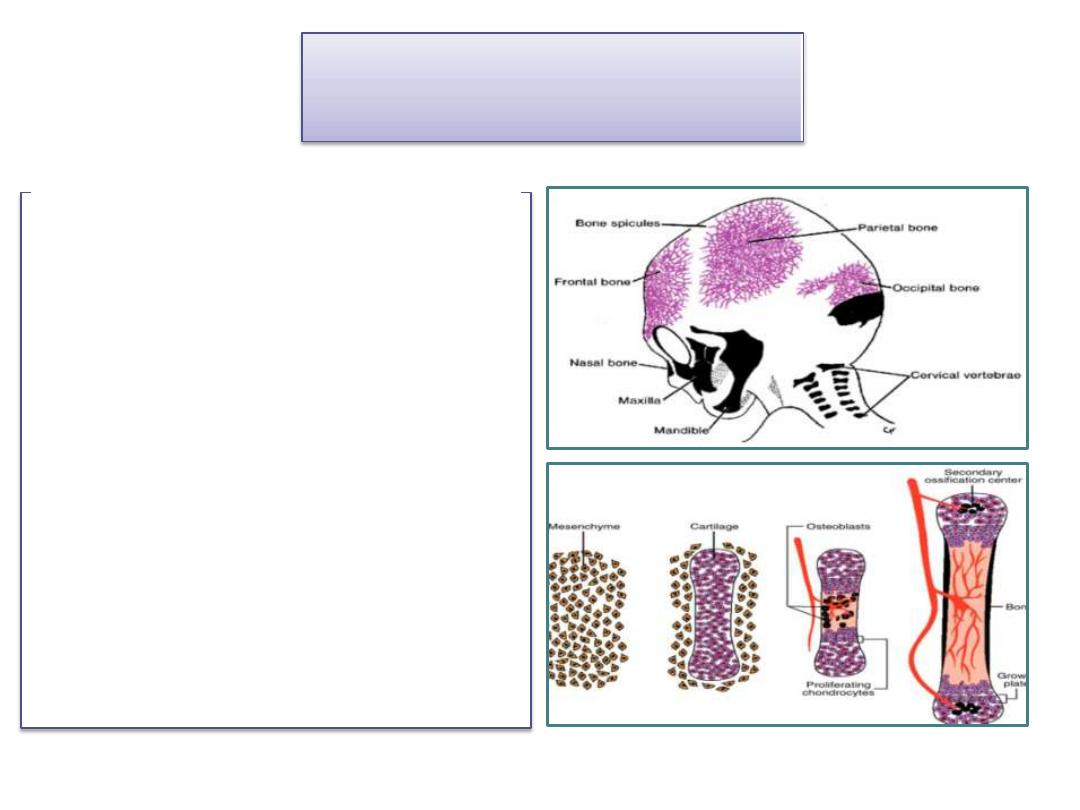
Bone formation
Intramembranous ossification
• Mesenchyme in the dermis
differentiates directly into
bone such as the flat bones of
the skull
Endochondral ossification
• Mesenchymal cells first give
rise to hyaline cartilage
models, which in turn become
ossified . Most bones formed
by this way
The skull can be divided into two parts:
• the Neurocranium
around the brain
• the Viscerocranium forms the skeleton of the
face.
forms a protective case
Neurocranium
is divided into two portions :
Membranous Neurocranium , consisting of flat
bones ,which surround the brain as a vault
Cartilaginous Neurocranium (Chondrocranium)
which forms bones of the base of the skull
.
Membranous Neurocranium
• Mesenchyme from
neural crest cells and
paraxial mesoderm
invests the brain and
undergoes
Membranous
ossification.
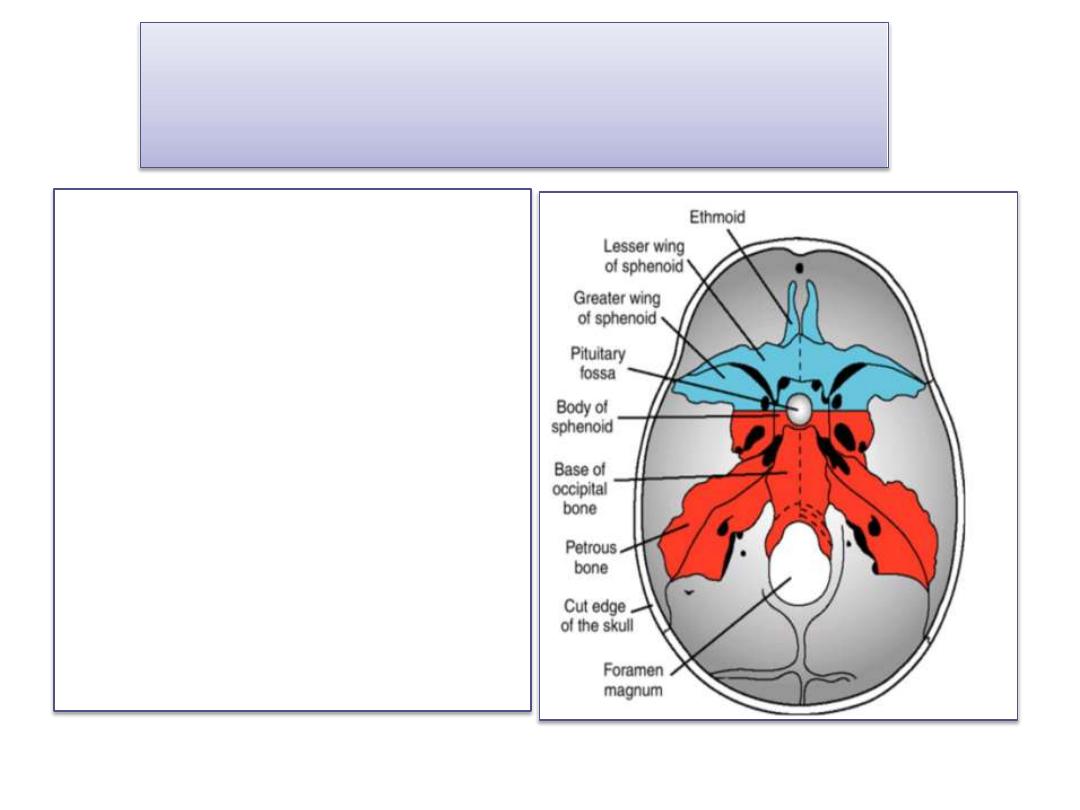
Cartilaginous Neurocranium or
Chondrocranium
• initially consists of a number of
separate cartilages.
Prechordal chondrocranium
Those that lie in front of the
rostral limit of the notochord,
they are derived from neural
crest cells.
Chordal chondrocranium Those
that lie posterior to rostral limit
of the notochord .They arise
from occipital sclerotomes
formed by paraxial mesoderm.
• The base of the skull is formed
when these cartilages fuse and
ossify by endochondral
ossification
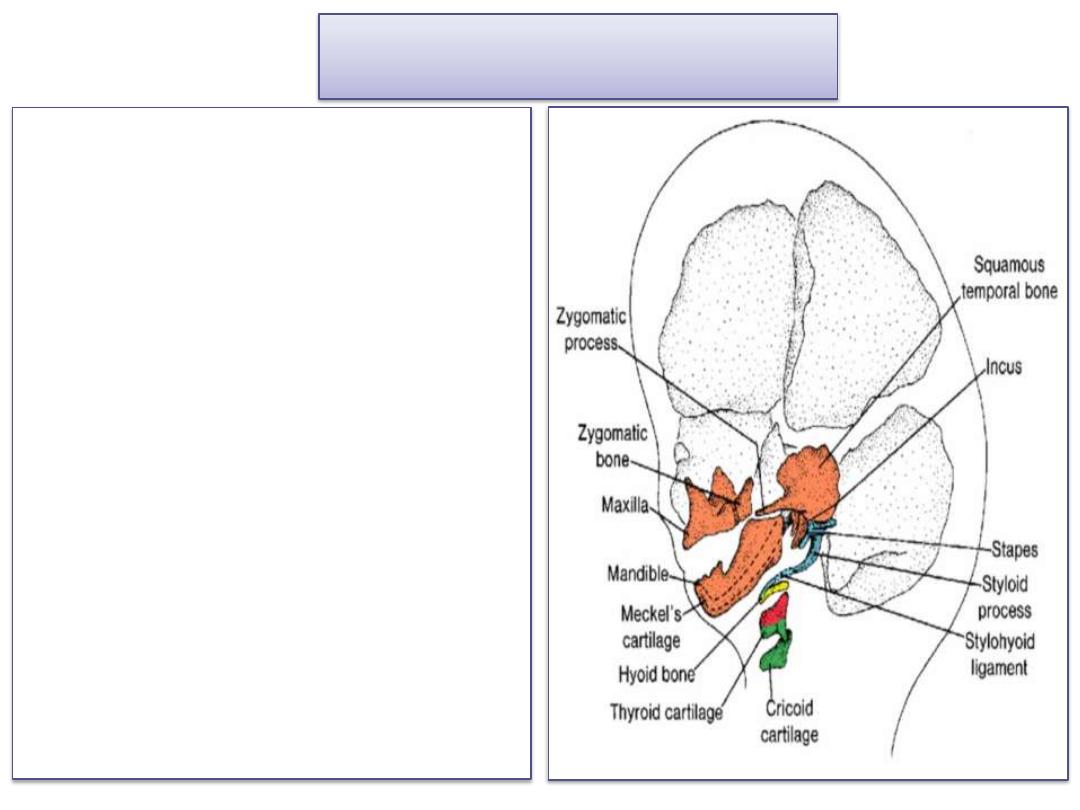
Viscerocranium
bones of the face which is formed
mainly from the first two pharyngeal
arches.
The first arch gives rise to
A dorsal portion ( the maxillary
process) gives rise to the maxilla, the
zygomatic bone, and part of the
temporal bone
A ventral portion(the mandibular
process) contains the Meckel
cartilage. Mesenchyme around the
Meckel cartilage condenses and
ossifies by membranous ossification
to give rise to the mandible.
The dorsal tip of the mandibular
process, along with that of the
second pharyngeal arch gives rise to
the incus, the malleus, and the
stapes
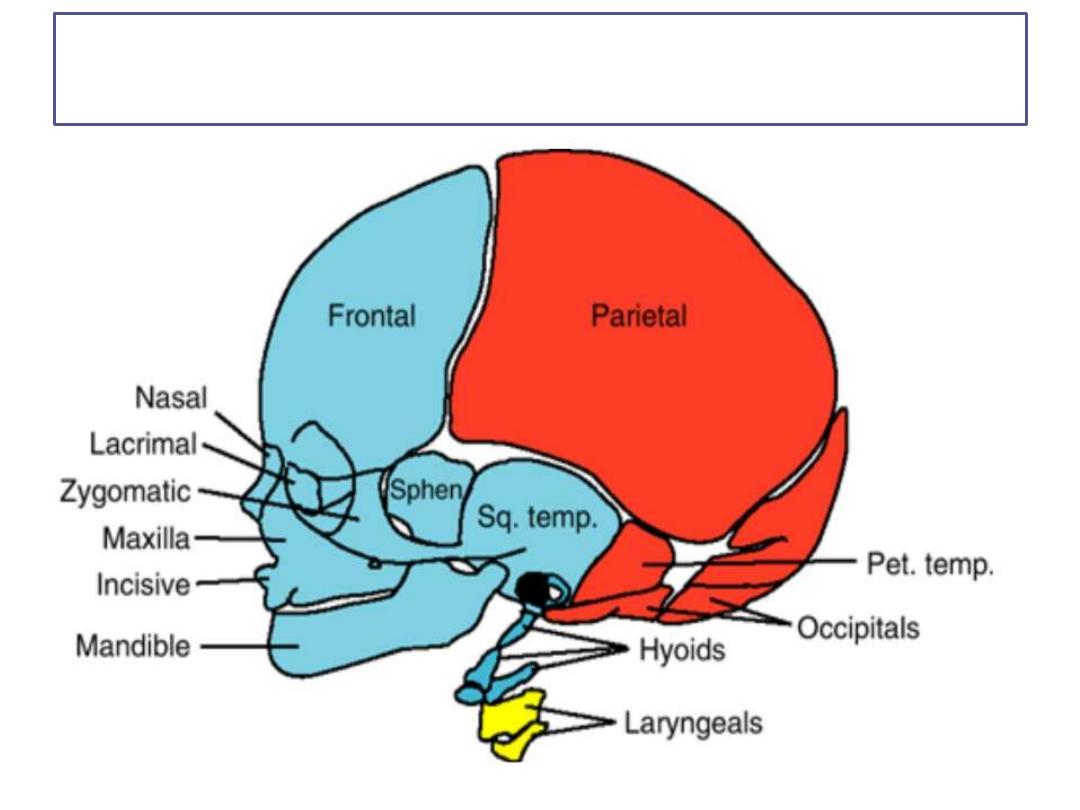
Skeletal structures of the head and face Mesenchyme for formation of the bones of the face is
derived from neural crest cells, including the nasal and lacrimal bones (blue), paraxial
mesoderm (somites and somitomeres) (red), and lateral plate mesoderm (yellow).
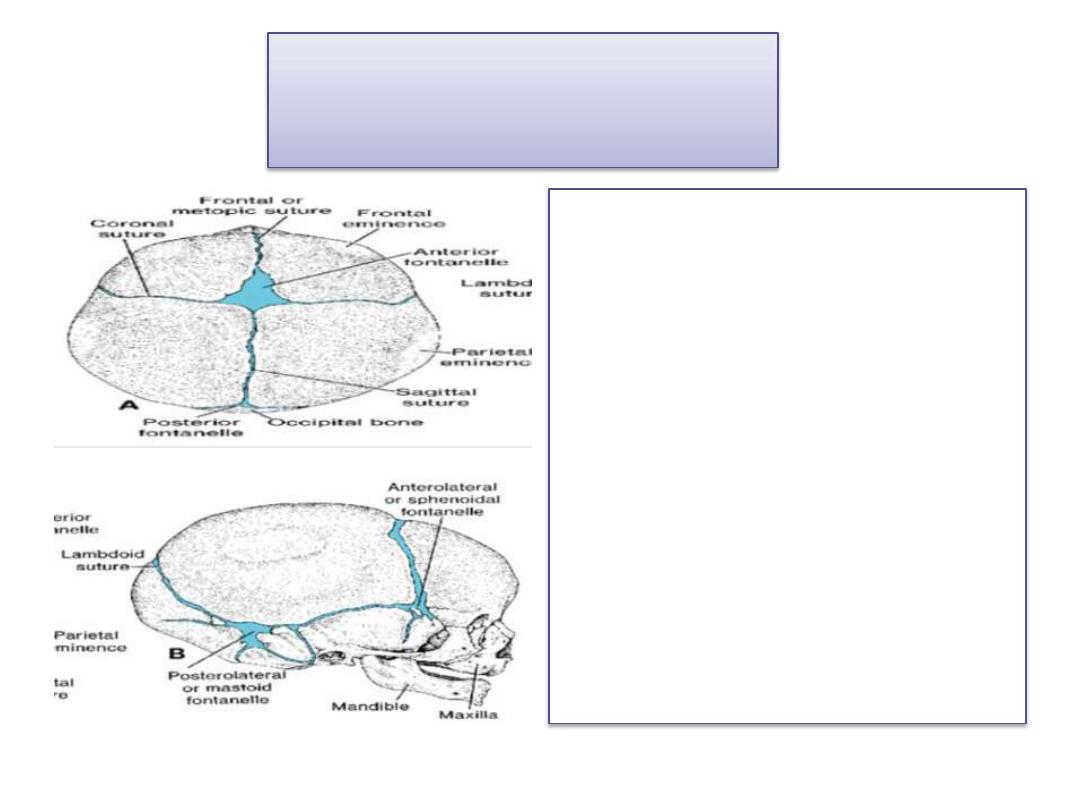
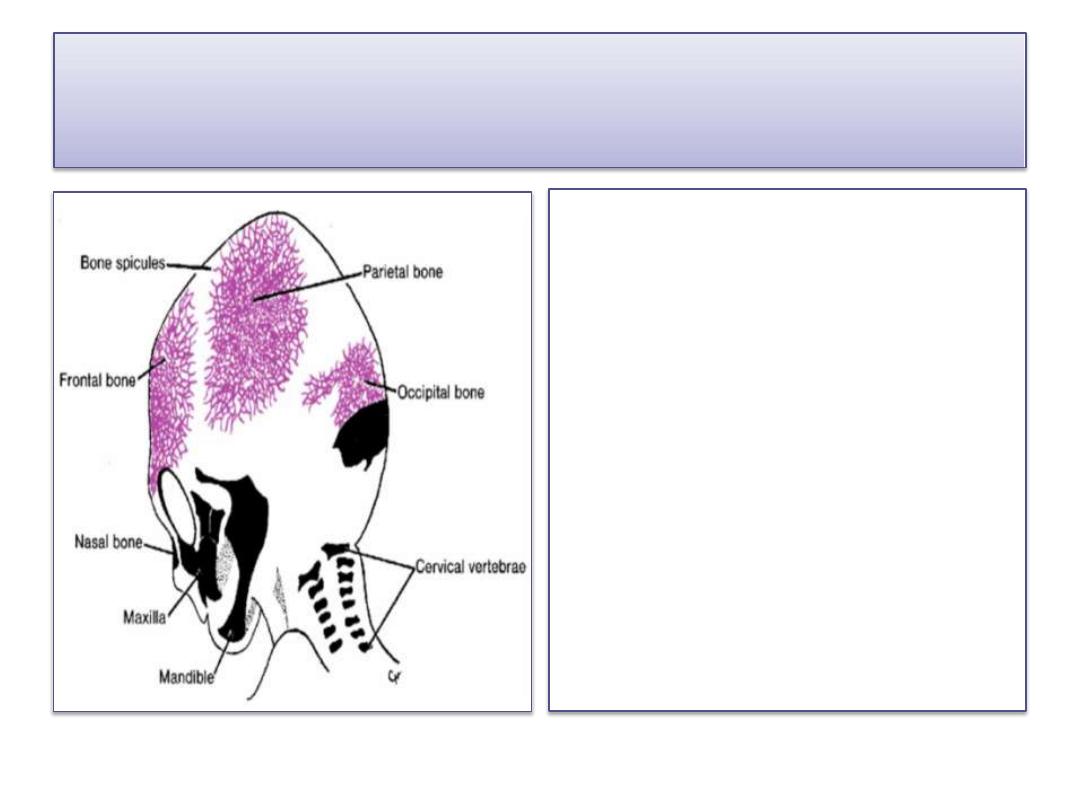
Newborn Skull
• At birth, the flat bones of the
skull are separated from each
other by narrow seams of
connective tissue, the sutures,
which are also derived from
two sources: neural crest cells
(sagittal suture) and paraxial
mesoderm (coronal suture )
.
• Several sutures and
fontanelles remain
membranous for a
considerable time after birth.
• The posterior fontanelle closes
by 1to 2months of age
• The anterior fontanelle closes
by 18months of age
• Many of the sutures disappear
during adult life.
Newborn Skull
• The bones of the vault
continue to grow after
birth because the brain
grows.
• Although a 5- to 7-year-
old child has nearly all
of his or her cranial
capacity, some sutures
remain open until
adulthood.
After birth, palpation of
the anterior fontanelle
may give valuable
information about
ossification of the skull
intracranial pressure
At first, the face is small in comparison
with the neurocranium because of the
(a)virtual absence of the paranasal air sinuses
(b)the small size of the bones, particularly the
jaws.
With the appearance of teeth and development
of the air sinuses, the face loses its babyish
characteristics.
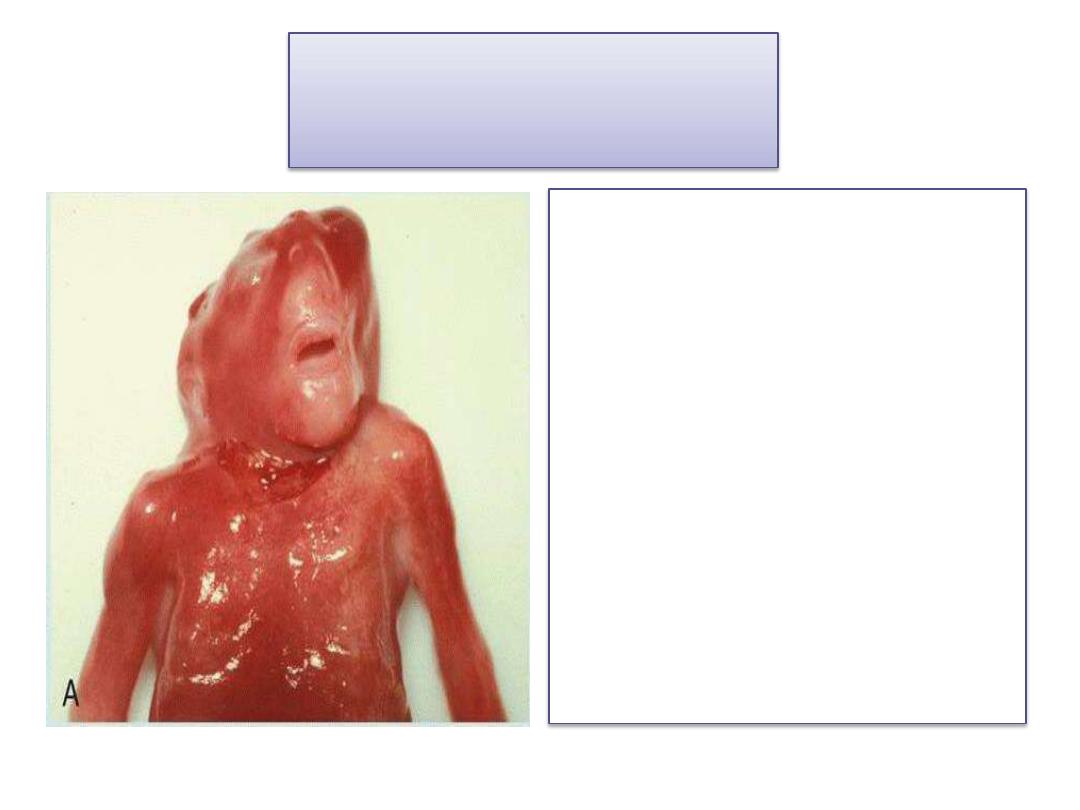
Cranioschisis
• is due to failure of the
cranial neuropore to close
• The skull never forms, and
brain tissue degenerates.
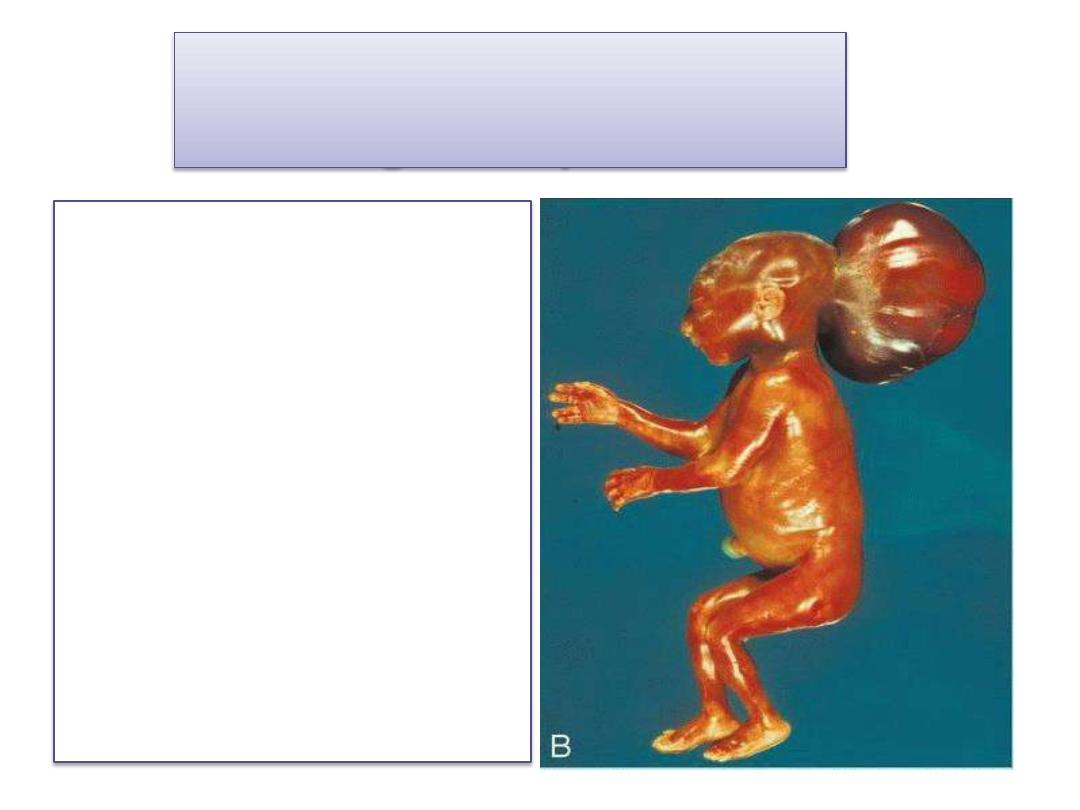
Cranial meningocele and
meningoencephalocele
• Small defects in the
skull through which
meninges and/or brain
tissue herniate.
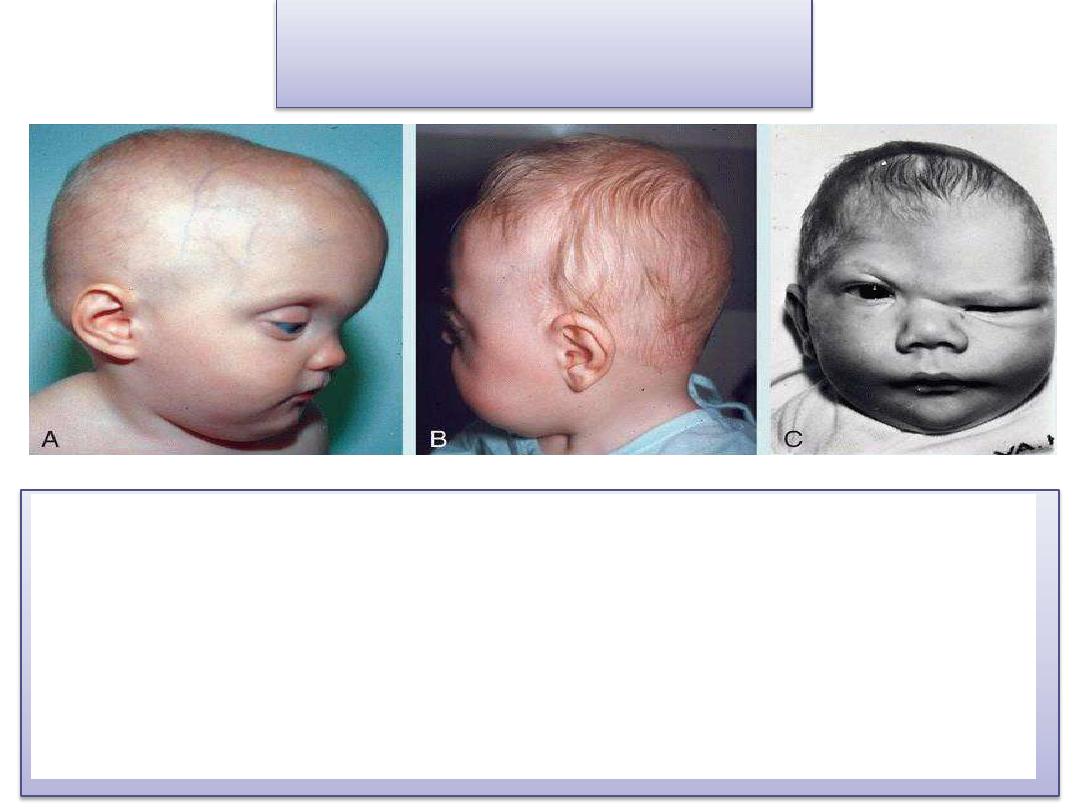
Craniosynostosis
• A. Child with scaphocephaly caused by early closure of the
sagittal suture. Note the frontal and occipital bossing.
• B. Child with brachycephaly caused by early closure of
both coronal sutures.
• C. Child with plagiocephaly resulting from premature
closure of the coronal suture on one side of the skull.
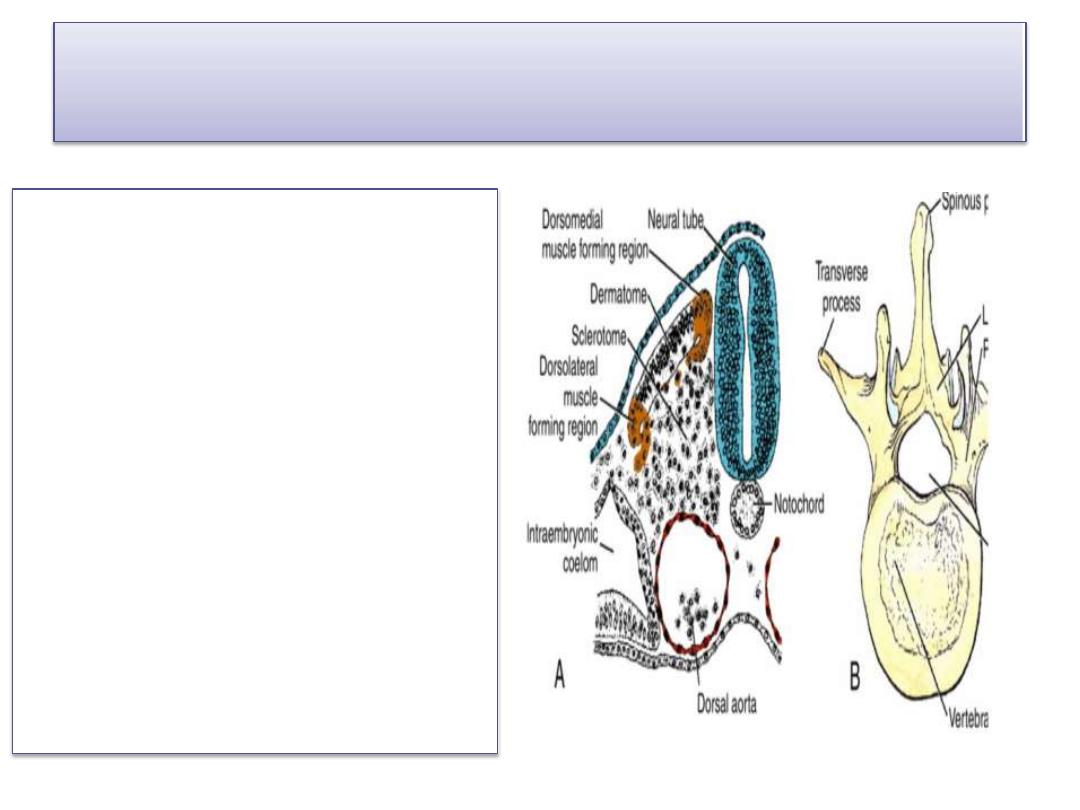
Vertebrae and the Vertebral Column
• Vertebrae form from the
sclerotome portions of
the somites.
• During the 4
th
week,
sclerotome cells migrate
around the spinal cord and
notochord to merge with
cells from the opposing
somite on the other side of
the neural tube
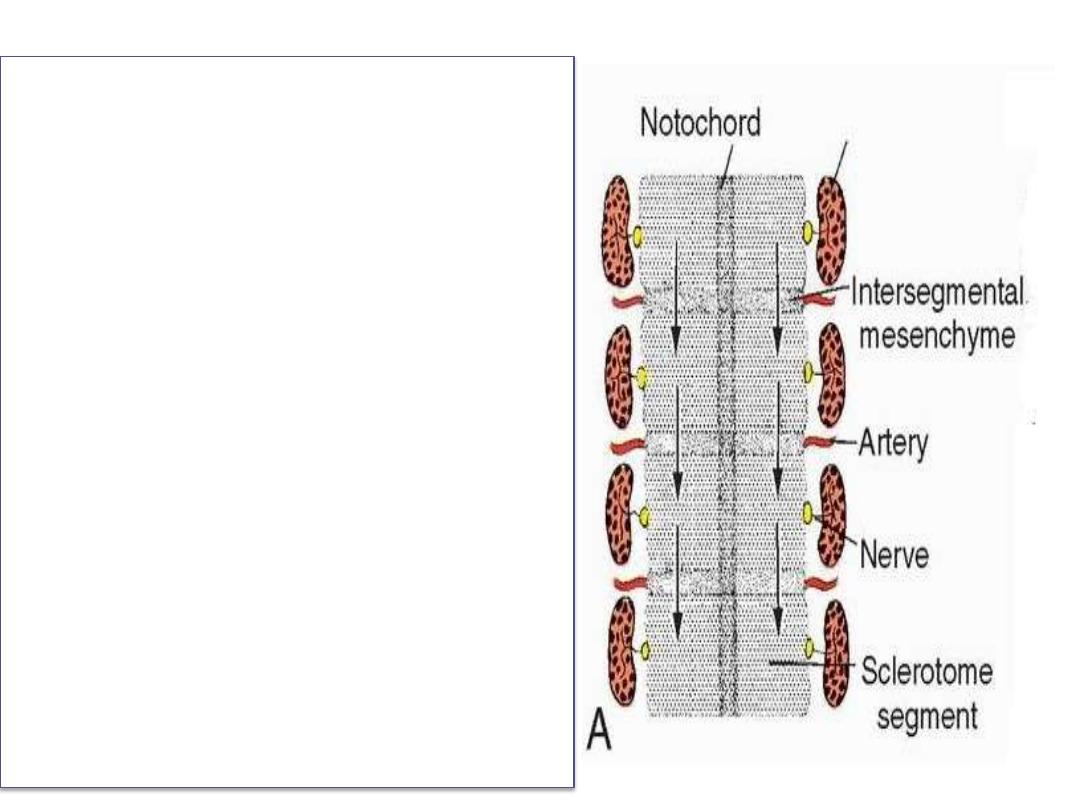
• A definitive vertebra is
formed by condensation of
the caudal half of one
sclerotome and fusion with
the cranial half of the
subjacent sclerotome
through a process known as
Re segmentation
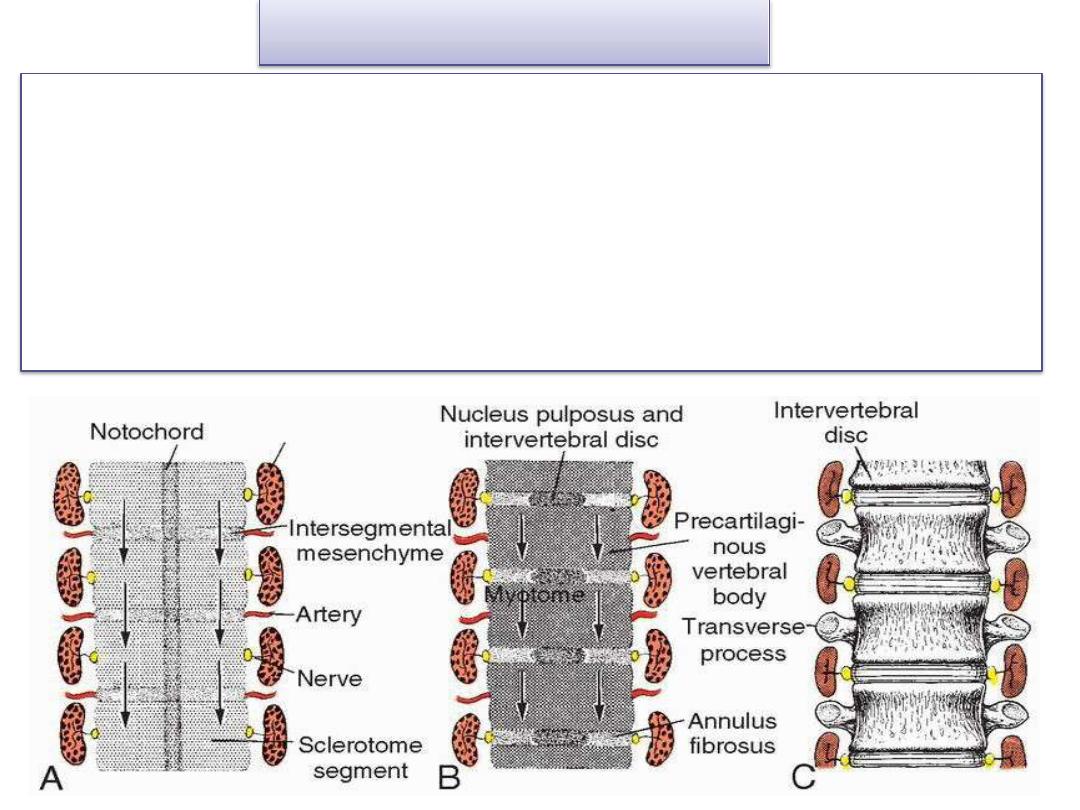
• Mesenchymal cells between cephalic and caudal parts of
the original sclerotome segment do not proliferate but fill
the space between two precartilaginous vertebral bodies.
• Although the notochord regresses entirely in the region of
the vertebral bodies, it persists and enlarges in the region of
the intervertebral disc.
• Here it contributes to the Nucleus pulposus, which is later
surrounded by circular fibers of the annulus fibrosus.
Combined, these two structures form the Intervertebral disc
Intervertebral disc
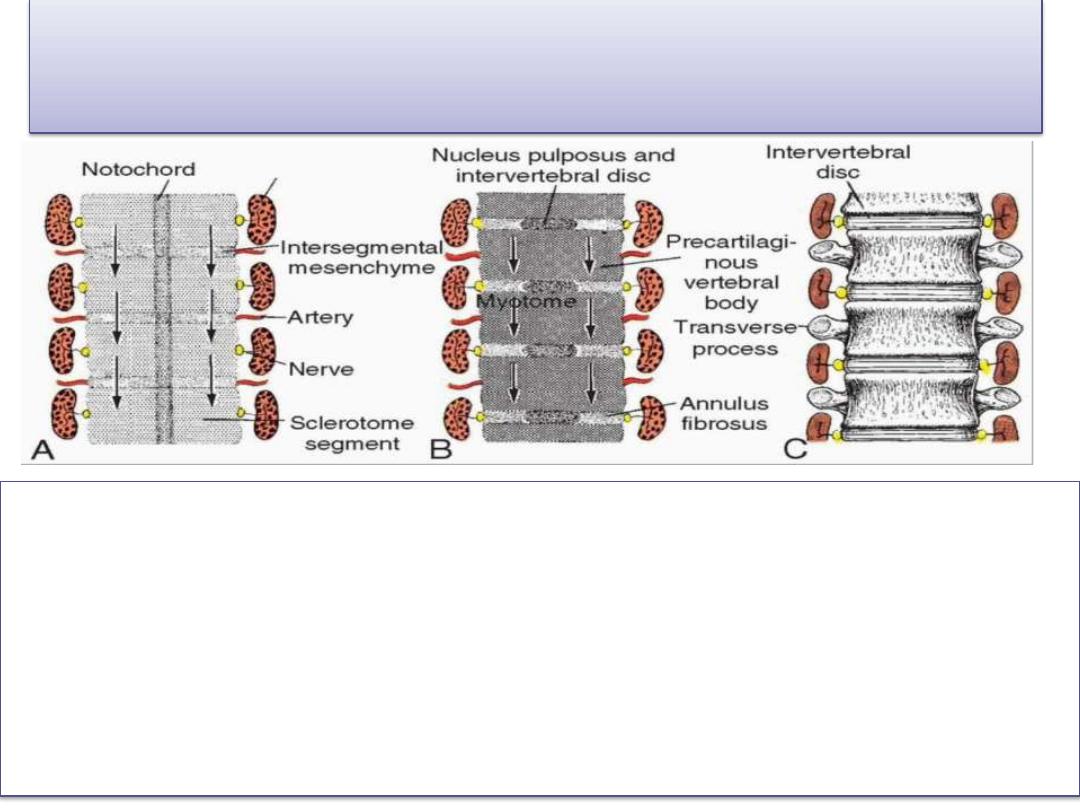
Re segmentation of sclerotomes into
definitive vertebrae causes :
• The myotomes to bridge the intervertebral discs, and this
alteration gives them the capacity to move the spine
• Intersegmental arteries, at first lying between the
sclerotomes, now pass midway over the vertebral bodies.
• Spinal nerves come to lie near the intervertebral discs and
leave the vertebral column through the intervertebral
foramina.

As the vertebrae form, two primary curves of the
spine are established:
thoracic curvature
sacral curvature
Later, two secondary curves are established:
the cervical curvature, as the child learns to hold
up his or her head
the lumbar curvature, which forms when the
child learns to walk.
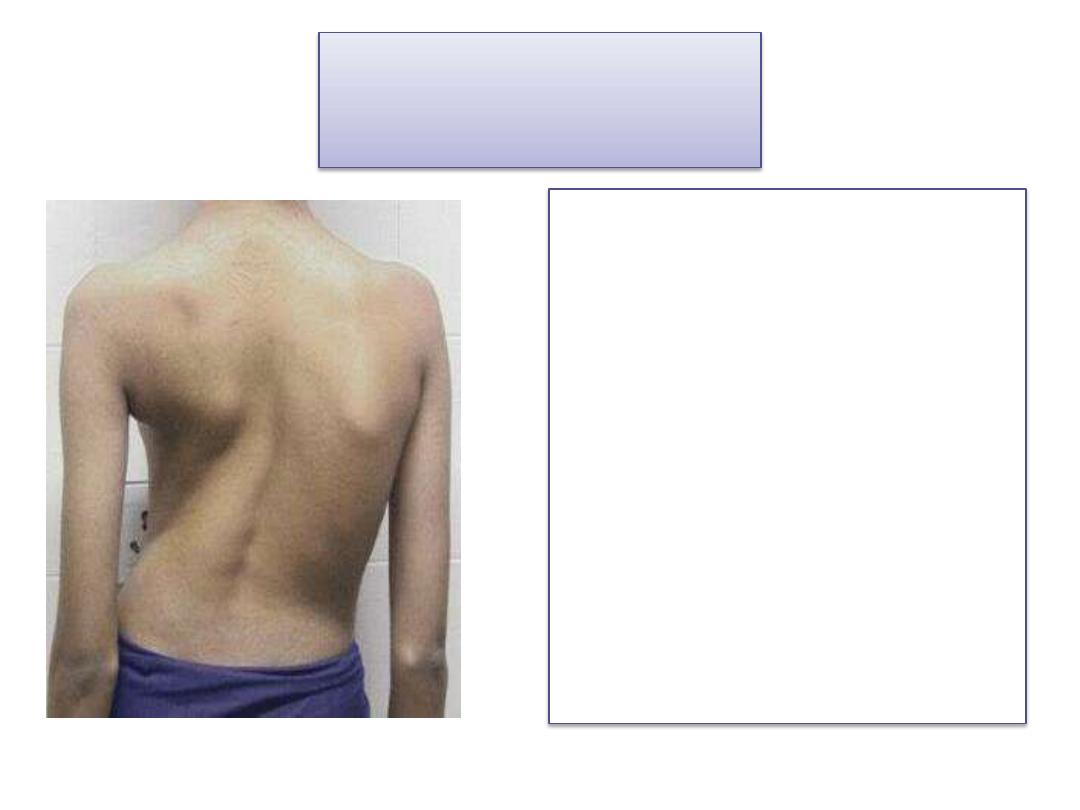
Scoliosis
• Scoliosis (lateral curving
of the spine): two
successive vertebrae fuse
asymmetrically or have
half a vertebra missing
• A photograph of a patient
with scoliosis taken from
behind. The curvature is
seen between the
shoulder blades (thoracic
spine.)
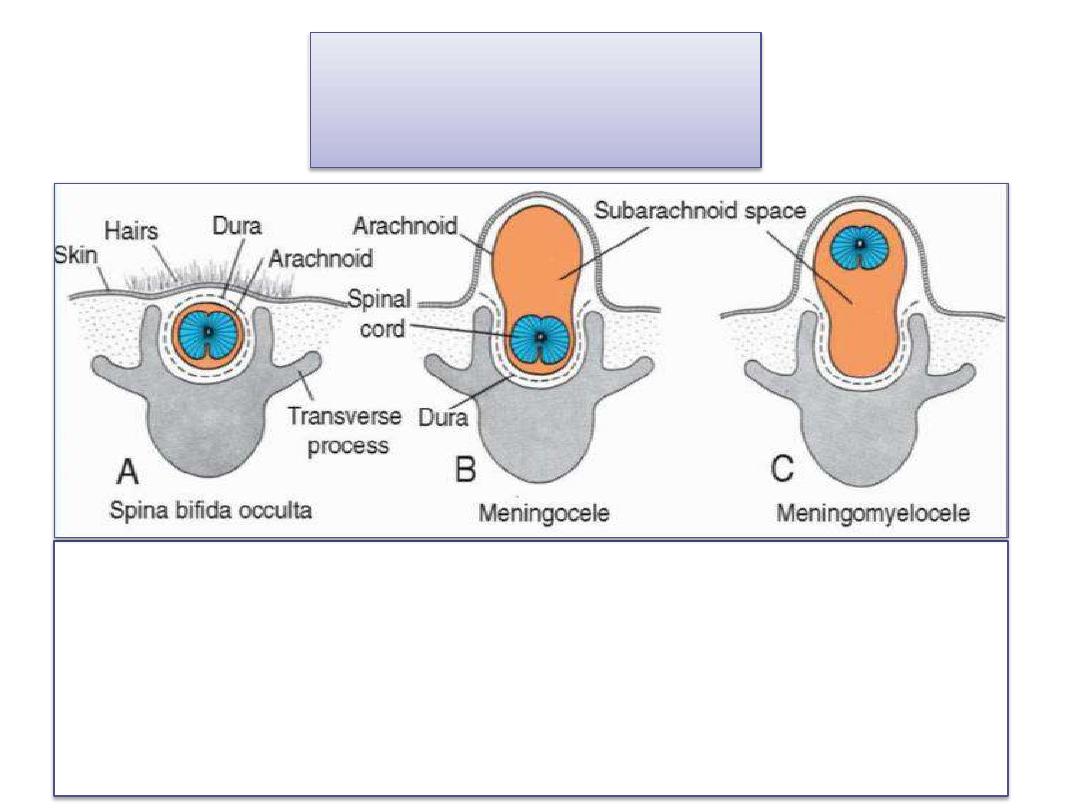
Spina bifida
• imperfect fusion or nonunion of the vertebral arches.
• (a) spina bifida occulta may involve only the bony
vertebral arches, leaving the spinal cord intact.
• (b)spina bifida cystica in which the neural tube fails to
close, vertebral arches fail to form, and neural tissue is
exposed.
Ribs and Sternum
The bony portion of each
•
rib is derived from
sclerotome cells that
remain in the paraxial
mesoderm and that grow
out from the costal
processes of thoracic
vertebrae.
Costal cartilages are
formed by sclerotome
cells that migrate across
the lateral somitic frontier
into the adjacent lateral
plate mesoderm
The sternum develops
independently in the
parietal layer of lateral
plate mesoderm in the
ventral body wall.
• Two sternal bands are
formed in the parietal layer
of lateral plate mesoderm
on either side of the
midline, and these later
fuse to form cartilaginous
models of the manubrium,
sternebrae, and xiphoid
process.
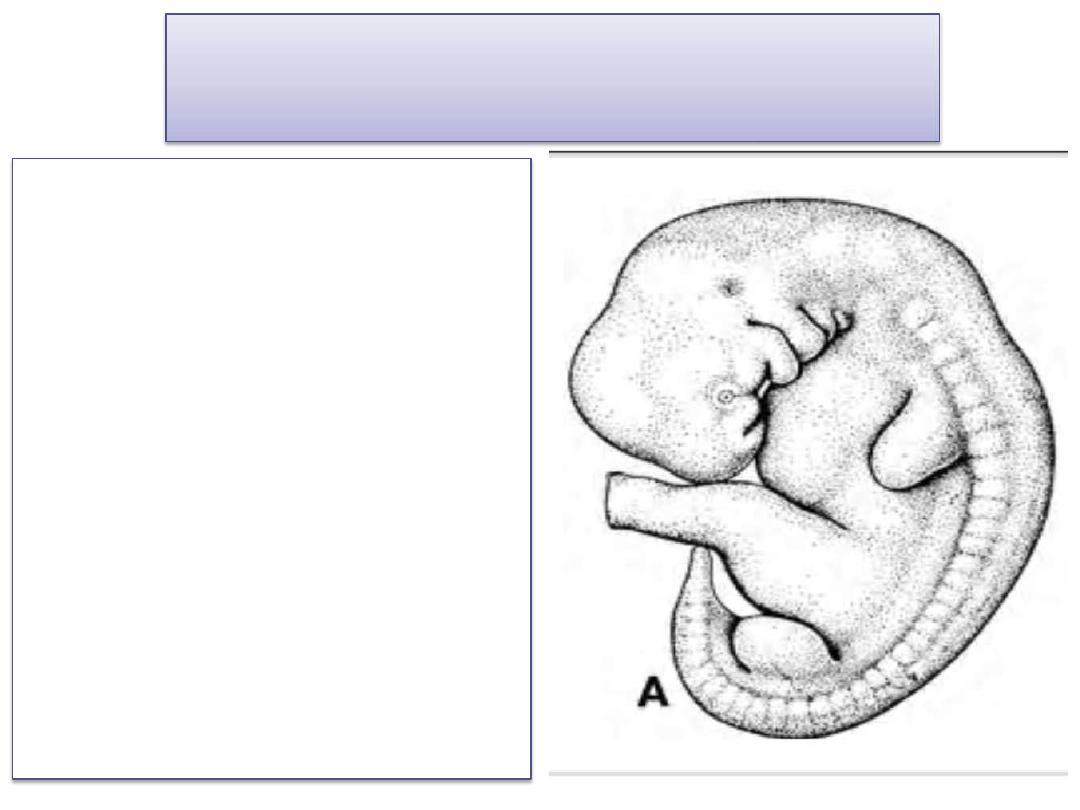
Limbs
Limb Growth and Development
• At the end of the 4
th
week of
development, limb buds
become visible as
outpocketings from the
ventrolateral body wall
• The forelimb appears first
followed by the hindlimb 1 to
2 days later.
• Initially, the limb buds consist
of a mesenchymal core derived
from the parietal layer of
lateral plate mesoderm that
will form the bones and
connective tissues of the limb,
covered by a layer of cuboidal
ectoderm.
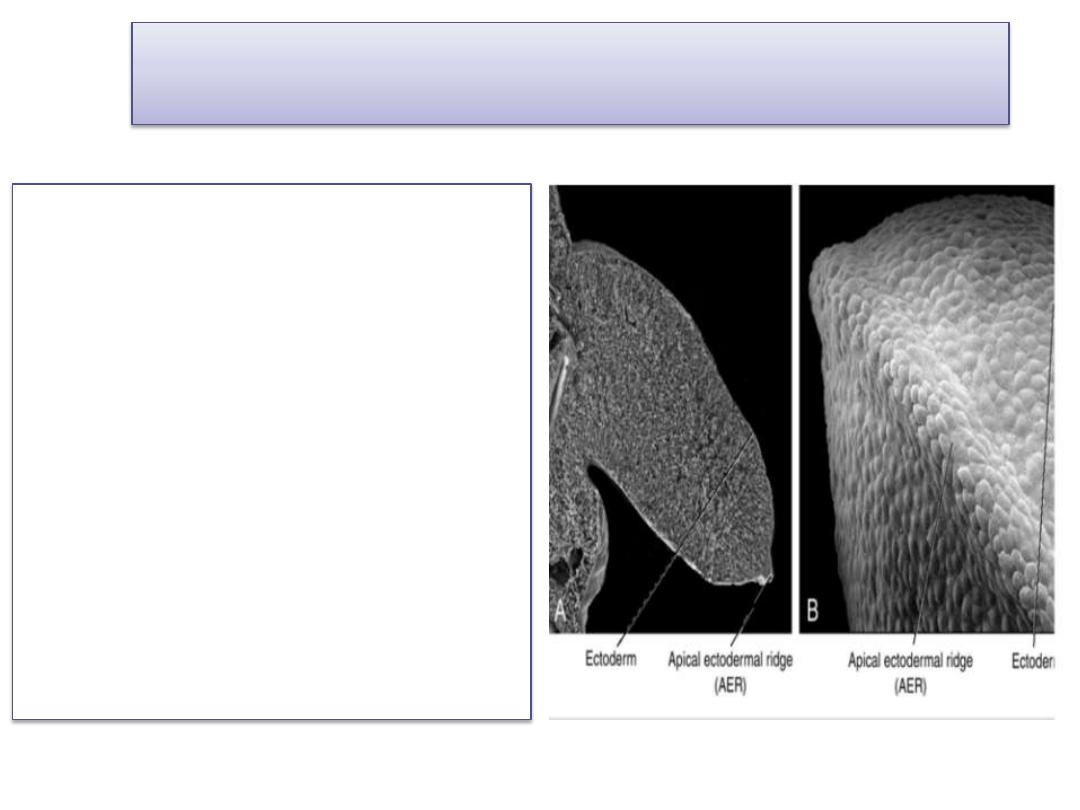
Apical ectodermal ridge (AER)
• Ectoderm at the distal border of
the limb thickens and forms the
Apical ectodermal ridge (AER) .
• This ridge exerts an inductive
influence on adjacent
mesenchyme, causing it to
remain as a population of
undifferentiated, rapidly
proliferating cells, the progress
zone.
• As the limb grows, cells farther
from the influence of the AER
begin to differentiate into
cartilage and muscle. In this
manner, development of the
limb proceeds proximodistally
.
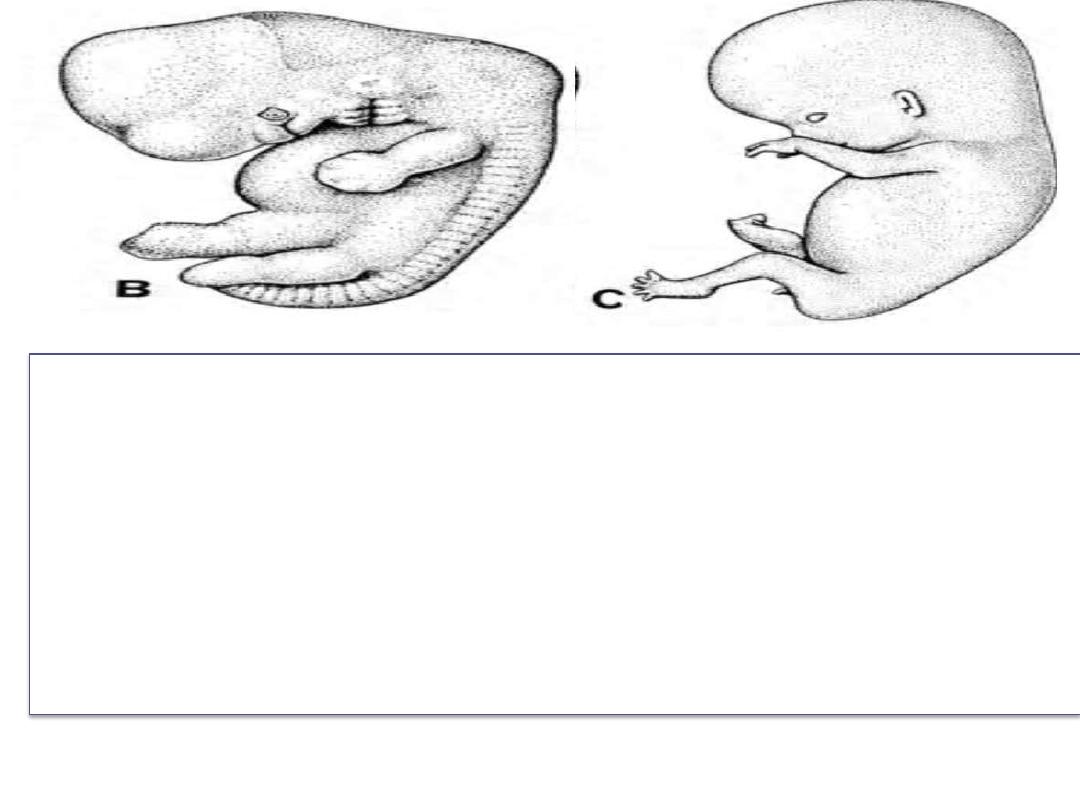
• In 6
- week-old embryos, the terminal portion of the limb
buds becomes flattened to form the hand- and footplates
and is separated from the proximal segment by a circular
constriction.
• Later, a second constriction divides the proximal portion
into two segments, and the main parts of the extremities
can be recognized.
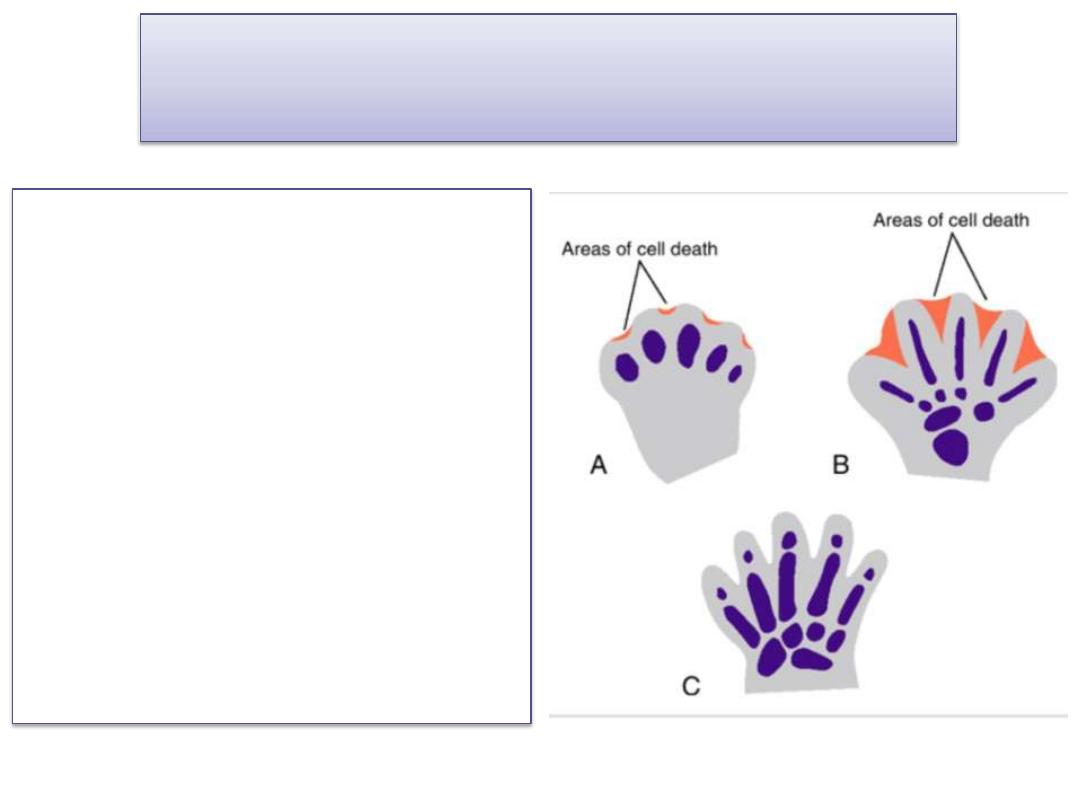
Fingers and toes are formed
• A. At 48 days. Cell death in the
apical ectodermal ridge
creates a separate ridge for
each digit.
• B. At 51 days. Cell death in the
interdigital spaces produces
separation of the digits.
• C. At 56 days. Digit separation
is complete
Development of the upper and lower
limbs is similar except that
• Morphogenesis of the lower limb is approximately 1
to 2 days behind that of the upper limb.
• During the 7
th
week of gestation, the limbs rotate in
opposite directions.
• The upper limb rotates 90 degrees laterally, so that
the extensor muscles lie on the lateral and posterior
surface and the thumbs lie laterally
• The lower limb rotates approximately 90 degrees
medially, placing the extensor muscles on the
anterior surface and the big toe medially.
Joints
• Joints are formed in the cartilaginous condensations
when chondrogenesis is arrested, and a joint
interzone is induced.
• Cells in this region increase in number and density,
and then a joint cavity is formed by cell death.
• Surrounding cells differentiate into a joint capsule.
Bone Age
• Radiologists use the appearance of various
ossification centers to determine whether a child
has reached his or her proper maturation age.
• Useful information about bone age is obtained from
ossification studies in the hands and wrists of
children.
• Prenatal analysis of fetal bones by ultrasonography
provides information about fetal growth and
gestational age.
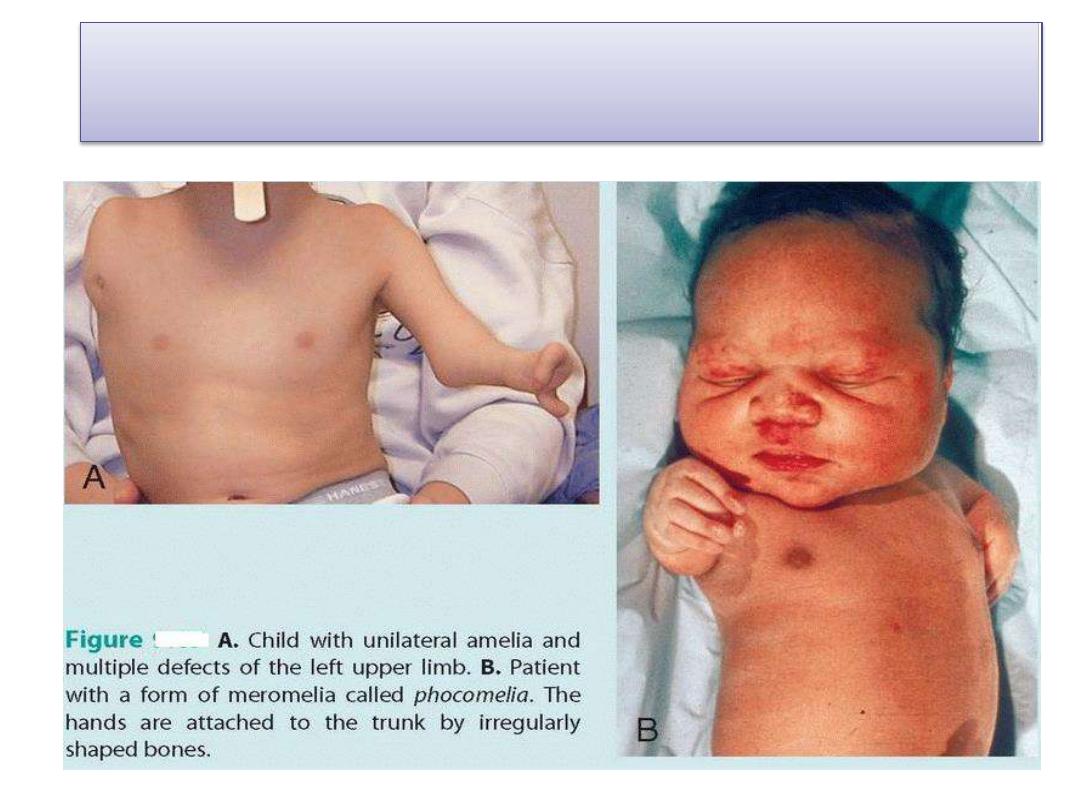
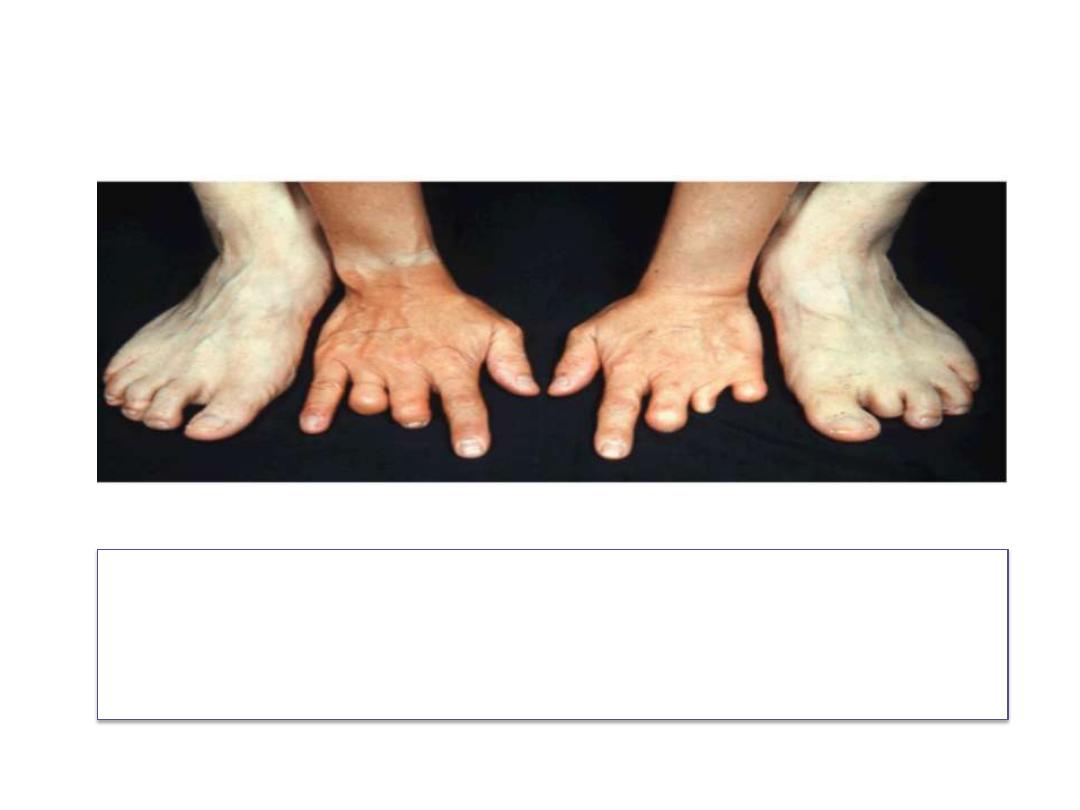
Partial (meromelia) or complete absence (amelia) of
one or more of the extremities

A. Brachydactyly the digits are shortened.
B. Syndactyly If two or more fingers or toes are fused.
C. Polydactyly are usually bilateral, whereas absence of a digit (ectrodactyly), such
as a thumb, usually occurs unilaterally
D. Cleft hand and foot (lobster claw deformity). consists of an abnormal cleft
between the second and fourth metacarpal bones and soft tissues. The third
metacarpal and phalangeal bones are almost always absent, and the thumb and
index finger and the fourth and fifth fingers may be fused. The two parts of the
hand are somewhat opposed to each other and act like a lobster claw.
Amniotic bands
• may cause ring constrictions and amputations of the
limbs or digits.
Congenital hip dislocation
• consists of underdevelopment of the acetabulum
and head of the femur. It is rather common and
occurs mostly in female newborns.
• Although dislocation usually occurs after birth, the
abnormality of the bones develops prenatally.
• Since many babies with congenital hip dislocation
are breech deliveries, it has been thought that
breech posture may interfere with development of
the hip joint. It is frequently associated with laxity of
the joint capsule.
Summary
• Skeletal system derives from paraxial mesoderm,
parietal layer of lateral plate mesoderm and neural
crest cells
• Bone ossification is of two types: intramembraneous
ossification and endochondral ossification
• Skull is divided into 2 parts: neurocranium and
viscerocranium which have different embryonic origin
• Vertebrae is derived from sclerotomes which undergo
re segmentation
• Apical Ectodermal ridge play an important role in
development of limbs