Tumours Of The Respiratory Tract
CarcinomaAdenoma
Benign Tumor( carcinoid)
Secondary Tumor

Bronchial carcinoma accounts for 95% of all primary tumours of the lung.
Alveolar cell carcinoma accounts for 2% of lung tumours
other less malignant or benign tumours account for the remaining 3%.
Secondary (metastasis)
1.Bronchial Carcinoma
most common malignant tumor with 1.3 million deaths annually.It is the 3rd most common cause of death in the UK after heart disease & pneumonia.
The strength of cigarette smoking & bronchial carcinoma overshadows any other aetiological factors:- e.g.
Passive smoking increases the risk of bronchial carcinoma by a 1.5.
Occupational factors include exposure to asbestos, contact with arsenic, chromium, iron oxide, petroleum products and oils, coal tar, products of coal combustion, radiation.
Tumours associated with occupational factors are mostly adeno carcinomas & appear to be less related to cigarette smoking
Cell types
Based on the characteristics of the disease & its response to treatment
bronchial carcinoma is divided in to:-
small-cell carcinoma (SCC)
non-small-cell carcinoma (NSCC).
Studies of mean doubling times of carcinomas from the initial malignant change to presentation takes About:
15 years for adenocarcinoma,
8 years for squamous carcinoma3 years for small-cell carcinoma.
Small-cell carcinoma (Oat)
accounts for 20–30% of all lung cancers.It arises from endocrine cells (Kulchitsky cells).
These cells are members of the APUD* system, which explains why many polypeptide hormones are secreted by these tumours.
spreads early
almost always inoperable at presentation
The tumors is rapidly growing & highly malignant.
It responds to chemotherapy & radiotherapy
but the overall prognosis remains poor
* APUD amine precursor uptake & decarboxylation) cells
Non-small-cell carcinoma
Squamous (epidermoid) carcinoma ( 40% ) .
Most present as obstructive lesions, leading to infection.
It occasionally cavitates (10%) at presentation.
The cells are usually well differentiated but occasionally anaplastic.
Local spread is common but widespread metastases occur relatively late.
Large cell carcinomas (25%) are less-differentiated forms of squamous cell & adenocarcinomas ,account for about & metastasize early.
Bronchoalveolar cell carcinoma (1–2%) ( bronchiolar )
occurs either as a peripheral solitary nodule or as diffuse nodular lesions ( expectoration of very large volumes of mucoid sputum.)
Adeno carcinoma
Adenocarcinoma arises from mucous cells in the bronchial epithelium.Invasion of the pleura &the mediastinal lymph nodes is common, as are metastases to the brain, adrenal glands and bones.
It accounts for 10% of all bronchial carcinomas.
It is the most common bronchial carcinoma associated with:-
In asbestosin non-smokers,
in women,
in the elderly,
in the Far East.
Common Cell Types Of Bronchial Carcinoma
comment
%Cell type
• obstructive lesions of the bronchus
35
Squamous
• Asbestos,non smoker
• 30
• Adenocarcinoma• polypeptide hormones secreted tumours
• 20• Small-cell
• adenocarcinomas. sequmouse, metastasize early
15
• Large-cell
expectoration of very large volumes
of mucoid sputum.• 1-2
• Bronchoalveolar cell carcinomaClinical features
Lung cancer presents in many different ways, reflecting:-local, metastatic or paraneoplastic tumour effects.
•Cough. This is the most common early symptom
Chest pain & discomfort are often described as fullness & pressure, may be pleuritic owing to invasion of the pleura or ribs.physical signs
Often there are no abnormal physical signs.
Enlarged supraclavicular lymph nodes .
signs of a pleural effusion or of lobar collapse.
Signs of an unresolved pneumonia
associated underlying disease(e.g. diffuse pulmonary fibrosis in asbestosis
Finger clubbing, Overgrowth of the soft tissue of the terminal phalanx, leading to increased nail curvature and nail bed fluctuation) .
The frequency of the common presenting symptoms of bronchial carcinoma
(%)
Symptom Frequency
41 (changing smoker) cough
Cough
22
Chest pain
15 dry but secondary infection may cause purulent sputum
Cough and pain
7 (haemoptysis) mild to massive
Coughing blood
5
Chest infection
5
Malaise
5
Weight loss
5 (collapse, mediastinal displacement)
Shortness of breath
5
Hoarseness
5
Distant spread
5
No symptoms
spread
1. Direct spread
The tumour may directly involve the pleura & ribs.
in the apex of the lung can erode the ribs and involve the lower part of the brachial plexus (C8, T1 & T2), causing severe pain in the shoulder and down the inner surface of the arm (Pancoast’s tumour).
The sympathetic ganglion can also be involved, producing Horner’s syndrome.
Hilar tumours may involve the left recurrent laryngeal nerve, causing unilateral vocal cord paresis with hoarseness and a bovine cough.can also directly invade the phrenic nerve, causing paralysis of the ipsilateral hemidiaphragm.
oesophagus, producing progressive dysphagia, &
pericardium, producing pericardial effusion & malignant dysrhythmias.
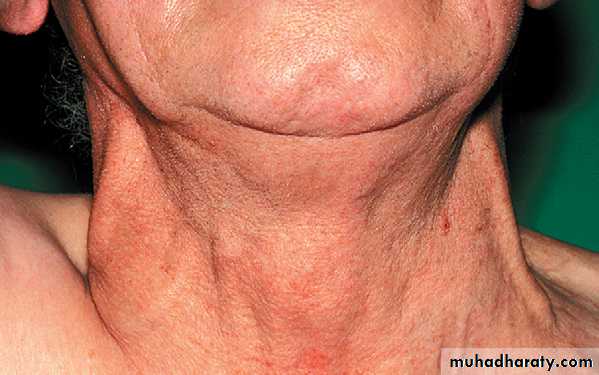
Superior vena caval obstruction :-causes early morning headache, facial congestion and oedema involving the upper limbs; the jugular veins are distended, as are the veins on the chest that form a collateral circulation with veins arising from the abdomen.
2.Metastatic complications
Bony metastases are common, giving rise to severe pain & pathological fractures.There is frequent involvement of the liver.
Secondary deposits in the brain present as a change in personality, epilepsy or as a focal neurological lesion.
Spinal cord compression is not uncommon and requires urgent treatment
Secondary deposits in the adrenal gland are frequently found at post mortem but are often asymptomatic
3.Non-metastatic extra-pulmonary manifestations of bronchial carcinoma
%
• Rarer:
manifestations
Type(universal at some stage)
Loss of weight, Lassitude
AnorexiaMetabolic
(10%)
• hypoglycaemia,, gynaecomastia
thyrotoxicosis
Ectopic adrenocorticotrophin syndrome
appropriate secretion of anti diuretic hormone (SIADH)
Hypercalcaemia
Endocrine(in small-cell carcinoma)
(in squamous cell carcinoma)
(2–16%)
Neuropathies – peripheral sensorimotor neuropathy
Muscular disorders – polymyopathy, myasthenic syndrome
(Eaton–Lambert syndrome)
Encephalopathies – including subacute cerebellar degeneration
Myelopathies – motor neurone disease
Myasthenia (Lambert–Eaton syndrome,Neurological
Other Manifestations
• (%)• Rarer:
Common
type(rare)
Disseminated intravascular coagulopathy (DIC )
Thrombotic thrombocytopenic purpura(TTP)
Haemolytic anaemia Syndrome (HUS)
Thrombo-phlebitis migrans
Non-bacterial thrombotic endocarditis
Microcytic and normocytic anaemia
Vascular and haematological
(3%)
Clubbing (30%),
Hypertrophic,osteoarthropathy ,gynaecomastia
Skeletal
(rare)
Dermatomyositis
Acanthosis nigricansHerpes zoster
Cutaneous