


Acute flaccid paralysis
Dr Nebal WaillCWTH / Pediatric neurology department
Definition
Acute Flaccid Paralysis (AFP) occurs when there is rapid evolution of motor weakness (< than 4 days), with a loss of tone in the paralysed limb. This excludes weakness due to trauma and spastic paralysis.AFP is a medical emergency as unnecessary delays can result in death and disability
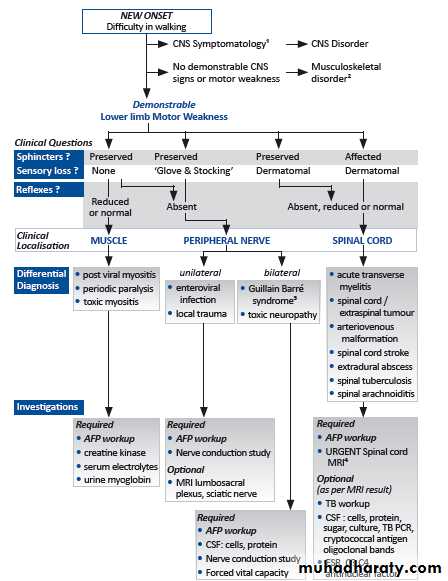
The list of underlying causes of AFP is broad, and there is substantial variation by age, ethnicity, and geographic area.
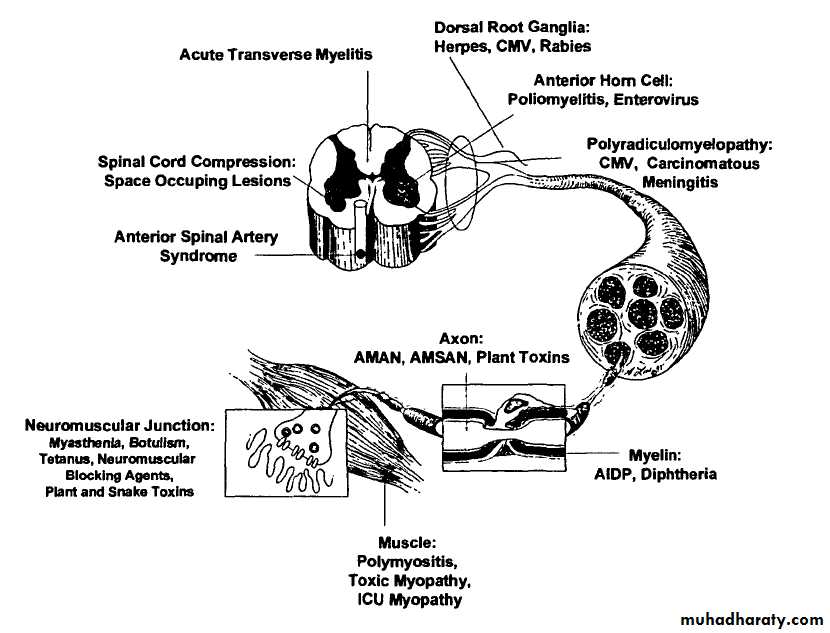
In the absence of wild virus-induced poliomyelitis, the acute demyelinating form of Guillain-Barre syndrome (AIDP) accounts for at least 50 percent of AFP cases globally followed in frequency by paralytic non-polio enterovirus infection, the motor axonal form of Guillain-Barre syndrome (AMAN), traumatic neuritis, and acute transverse myelitis.
Background
• • 1916- Guillian, Barre and Strohl described 2 French soldiers with motor weakness, areflexia, and “albuniocytological dissociation” in the cerebrospinal fluid. They recognized the peripheral nature of the illness.•
•
Guillian
BarreAndre Strohl
Epidemiology
• Annual incidence of GBS = 1-3/ 100000 persons annually.• Rare in infants.
• Male & female have similar risk
• Any age but most frequent at 4-9 years
GBS subtypes
• Sporadic AIDP• AMSAN
• AMAN
• MFS
Pathology
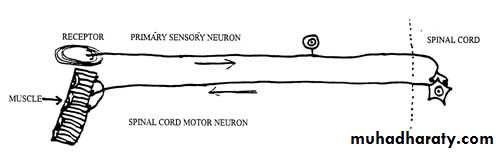
Both motor and sensory fibers are affected
AIDP
Segmental demyelination occurs at all levels of peripheral nervous systemCNS alterations are secondary to axonal degeneration and affect
Segmental demylinationAxonal degeneration ( less extensive )
Anterior + posterior rootsSympathatic chain and ganglia
peripheral nerves
Anterior horn cells in spinal grey matter
Neurons of motor cranial nerves neucli in brainstem
Pathogenesis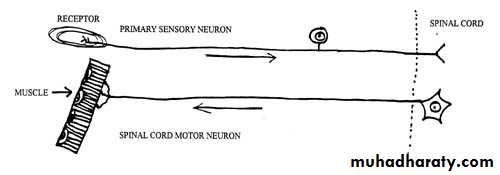
Pathogenesis
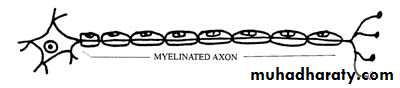
node of Ranvier
myelin sheathmyelin sheath
Antecedent Events
Documented in 2/3 of casesAgents :
Campylobacter jujeniCMV
EBV
HSV
H.Influenzae
Mycoplasma
Vaccines :
Rabies
Swin-flu
Tetanus
Mumps
Measles
Rubella
Hepatitis A
Hepatitis B
H. Influenzae type b
Trauma
Sugrical procedures
C.Jujeni accounts for 1/3 of GBS because of mimicry between gangliosides and lipopolysaccharides of the bacteria
Clinical features
• AIDP
Infection (GIT: Campylobacter, Respiratory: Mycoplasma) within 2 weeks of onset
Weakness(lower extremities then ascend up to the trunk then upper limbs and bulbar weakness.
May start in the arms and move downward
May begin in the arms and legs at the same time
May occur in the nerves of the head only
In mild cases, weakness or paralysis may not occur
This weakness is symmytrical ( minor sides differences may occure), proximal and distal
9% is asymmetricalprogress slowly over days or weeks Or abrupt and rapid
Clinical features• Child becomes irritable .
• Parasthesia may occur, 89% pain accompany weakness
• 50% bulbar involvement .
• Facial nerve involved. also VI,III,XII,IX,X
• Some show viral meningitis or meningoencephalitis.
• Papillodema ( unexplained pathogenesis )
• Respiratory muscules : reduced vital capacity CO2 retention even in absence of respiratory symptoms
Clinical features
• Features required for diagnosis
• Progressive motor weakness of more than one limb.
• Areflexia or hyporeflexia (loss of ankle jerks and diminished knee and biceps reflexes will suffice if other features are consistent with the diagnosis.
Clinical features
• Featrues supportive of diagnosis• Progression :weakness may develop rapidly but cease to progress after 4wk . Roughly 50%will plateau within 2 wks , 80% by 3wks,and 90%by 4wks.
• Relative symmetry .
• Mild sensory symptoms and signs.
• Cranial nerve involvements like facial weakness develops in about 50% of patients.
• Autonomic dysfunction.
• Absence of fever at the onset of neurological symptoms.
• Recovery without specific therapy, begins 2-4wks after progression ceases, occasionally delayed for months.
Clinical features
• Features casting doubt on the diagnosis• Marked persistent asymmetry in motor function.
• persistent bowel or bladder dysfunction at onset of symptoms .
• Discrete sensory level .
• Progressive phase longer than 4wks .
• CSF pleocytosis ( > 50wcc/mm3).
• Complete ophthalmoplegia (internal or external).
Clinical Phases
Guillian-barre can be divided into five distinct clinical phases :
Phase 1- first 24 hr from presentationPhase 2- disease progression
Phase 3- plateau phase
Phase 4- initial recovery
Phase 5- rehabilitation
Dx
• Clinical
• CSF
• Electrophysiologic
• MRI
Investigation
• MRI of the brain and spinal cord• Should be considered in all patients ,usually done if :
• The presentation is acute or rapidly progressive
• There are predominantly sensory symptoms (including back pain)
• There is predominant sphincter disturbance of presentation
• There is a clear sensory or marked motor level
Investigation
• Lumber puncture
• Elevated CSF protein without pleocytosis is a supportive diagnostic finding ,however the CSF may be normal within seven days of onset of symptoms
• Protein level :elevated (>45mg/dl ) after the first week of symptoms , peak 4-5 wks
• WCC <10/mm3 , occasionally up to 50 mm3
• Glucose level normal
Investigation
NeurophysiologyNormal nerve conduction studies in the first week does not exclude the diagnosis of GBS
In AIDP nerve conduction impairment = conduction block , decrease compound action potential amplitude
Investigation
Since the median duration of excretion of Campylobacter in stools of infected persons is only 16 days and because of the 1- to 3-week lag time between infection and the onset of GBS, many GBS patients with preceding Campylobacter infection might have falsely negative stool cultures.multiple stool samples (or rectal swabs) should be obtained from GBS patients immediately upon admission to the hospital, preferably 3 over a 3-day period.
Investigation
Other investigationsFull blood count, blood culture ( if pyrexial )
Urea and electrolytes ( hypokalemia )
Creatine kinase (myositis)
Chest x-ray , ECG
Abdominal x-ray ( palpable bladder , constipation )
Treatment
• Admission
• IVIG
• Plasma exchange
• Supportive treatment
• Rehabilitation
treatment
• Symptomatic treatment is an essential part of the management of GBS.• Children should admitted to the pediatric intensive care unit if they have one or more of the following :
• Flaccid tetraparesis
• Severe rapidly progressive course
• Reduced vital capacity at or below 20 ml/kg
• Bulbar palsy with symptoms
• Autonomic cardiovascular instability that is persistent hypertension or labile blood pressure or arrhythmias.
Plasma exchange
Plasmapheresis has remained the gold standard treatment for GBS over the last 20 years.Should be used within 4 weeks of onset of neuropatic symptoms in non-ambulatory patients
Should be used within 2 weeks of onset of neuropathic symptoms in ambulatory patients
treatment
• Plasmapheresis is generally safe in children who weigh 10 kg or more . A series of exchange with a cumulative total of approximately 250 ml/kg volume exchange or roughly a triple volume exchange .
• Disadvantages of Plasmapheresis include its rare complications, such as sepsis, risk of acquiring viral infections such as hepatitis and HIV.
treatment
• IVIG treatment has advantages over plasmapheresis because• it is easier to administer,
• has significantly fewer complications,
• and is more comfortable for the patient.
• Side effects of IVIG
• expands the plasma volume so it must be administered with caution in patients with congestive heart failure and renal insufficiency
• fever, myalgia, headache, nausea, and vomiting, but these "influenza-like" symptoms are self-limiting.
• aseptic meningitis, neutropenia, and hypertension
• Anaphylaxis
• Thromboembolic events
• risk of serious hepatitis C infection transmission has been reduced
IVIG should be used within 2 weeks
Corticosteroid not recommendedSequential treatment with PE then IVIG not recommended
PE & IVIG recommended for the severe disease
treatment• Pain management
• Pain of discomfort is present in 50-80%of children with GBS at the time of presentation .
treatment
Managing pain by:Opioids
Non steroidal anti-inflammatory drugs ( ibuprofen)
Anti-epileptic drugs ( carbamazepine, gabapentine)
Tricyclic antiderpessants (amitryptine)
Prevention of pain:
Air matressesTurning patients and carful positioning of limbs
Continuation of enteral feeding ,effective antacids as omeprazole
Preventing constipation
Prevent and treat urinary retention.
treatment
• Supportive treatment directed to:
• Hypertension , hypotension
• Cardiac arrhythmia
• Pulmonary embolism (Prophylaxis for deep venous thrombosis should be provided because patients frequently are immobilized for many weeks).
• Bladder and bowel
• Psychological support
• Nutrition , fluid , electrolytes
• Pain
• Skin
• Cornea
• Joints
• Infection
• communication
prognosis
• 40% bed bound• 15% require ventilation
• 90-95% complete recovery within 6-12months
• Remainder ambulatory with minor residual deficit
• 4% mortality rate
• Antecedents C.jujeni infection correlates with poor Px
• Causes of death :
• Autonomic (bradycardia , tachycardia , hypertension)
• Respiratory failure
• Pulmonary embolism
• Complication of ventilation
• Cardiovascular collapse
prognosis
• Chronic relapsing or chronic unremitting (7%)
• Features suggestive relapsing are:
• Severely weak
• Flaccid tetraplagia
• Bulbar and respiratory muscle involvement
• One or more relapses over 2mo.- years = CIDP
• Congenital GBS
• Weakness , areflexia , hypotonia .
• CSF and electrophysical studies suggestive of GBS .
• No treatment , gradual improvement.
Poliomyelitis
poliovirusesRNA viruses, Picornaviridae family, enterovirus
3 genetically distinct serotypes
Spread from intestinal tract to CNS
90 – 95 % inapperant infections
Transmission: human is the only reservoir
Fecal – oral route
Isolated from stool for 2 weeks before paralysis to several weeks after onset of symptoms
Pathogenesis
Wild type and vaccine strains
Gain host entry through GIT
Pass to the regional lymph nodes
Goes to the blood causing viremia
Wild type access the CNS through peripheral nerves
Incubation period 8-12 days
Clinical manifestions
Wild type follow one of the following courses :• 90 -95 % inapparent infection (no disease & no sequelae
• 5% inabortive disease (influenza – like syndrome 1-2 wk after infection, fever, malaise, anorexia , headache +/- vomiting) then recovery complete
3- Non-paralytic poliomyelitis
1%Signs of abortive type, fleeting paralysis of bladder and constipation.
This is first phase (minor) then symptoms-free period then major phase
O/E: nuchal rigidity, changes in the deep and superficial reflexes (impending paralysis). No sensory defects
4- Paralytic poliomyelitis
0.1%Spinal type : major phase , sensory (paresthesia, hypersthesia), motor( fasiculation and spasms) progress to
Asymmetric paralysis of one leg, then 1 arm
DTR initially active then diminished and absent
Variable course: some progress, some recover
5- Bulbar type
+/- spinal cord involvement
Nasal voice or cry
Difficulty in swallowing
Accumulated pharyngeal secretion
Absence of effective coughing
Nasal regurgitation
Deviation of palate, uvula, tongue
Involvement of vital centers in the medulla
Paralysis of vocal cords … hoarseness, aphonia
Sometimes culminate into ascending paralysis (Landry type)
6- polioencephalitis
RareSeizures , coma , spastic paralsysis , increased reflexes
Respiratory insufficiency
7- Paralytic polio with respiratory insufficiency
Anxious expressionInability to speak without frequent pauses
Increased RR
Movement of ala nasi, accessory muscles
Inability to cough or sniff
Paradoxical abdominal movement
Relative immobility of intercostal space
Diagnosis
Should be considered in any unimmunized or incompletely immunized child with paralytic disease
Or any child with paralytic disease occurring 7-14 days after receiving the oral vaccine
Diagnosis
Stool : Isolate the virus in 2 stool specimen collected with 24 – 48 hr apartCan isolate polio virus in 80 – 90 % in the first week and less than 20% within 3-4 wk
CSF : normal in minor disease
Cells 20 -200 / mm3 initially then reducedProtein : increase to reach 50 -100 mg/dl by 2nd week
CSF serology : seroconversion or 4 folds rise in antibody titers
Treatment
No specific treatmentSupportive: Limit progression, prevent skeletal deformities, prepare child and family for prolonged treatment
Abortive poliomyelitis
Analgesics, sedativesAttractive diet
Bed rest until temperature normalize
Avoidance of exertion for ensuing 2 wks
Careful neurologic and musculoskeletal examination
Non paralytic poliomyelitis
Same as abortive
Relief muscle tightness
Analgesics
Hot packs for 15-30 min every 2-4 hr
Hot tub baths
Firm bed
Footboard or splint to keep feet at right angle to legs
Later gentle physical therapy
Paralytic poliomyelitis
HospitalizationPhysical rest
Suitable body alignment to prevent deformity
Change position every 3-6 hr
Active and passive movement indicated as pain disappear
Moist hot packs
Opiates and sedatives
Treat constipation
Parasympathetic stimulant for bladder paralysis
Adequate dietary and fluid intake
Orthopedist, physiatrist should see them
Bulbar
Maintain airway
Avoid risk of inhalation
Gravity drainage of accumulated saliva
Nursed in lateral or semi-prone position
Aspirators with rigid tips for oral pharyngeal secretion or flexible catheter for nasopharyngeal
Fluid and electrolytes equilibrium
Blood pressure taken at least twice
Impaired ventilation signs should be noticed to decide tracheostomy
Prognosis
Inapparent, abortive and aseptic meningitis = good outcomeParalytic = depends on the extent and severity of CNS involvement, recovery phase last 6 months
Severe bulbar = MR 60%
30 – 40 % of persons survived paralytic polio… may experience muscle pain and exacerbation of exisiting weakness after 30 -40 yrprevention
VaccinationHygienic mearures
Thank you