Chest X-ray:
Used In:A -Preoperatively. B- Pre-employment .
C - Patient complains from respiratory symptoms.
D - Patient complains from cardiovascular symptoms.
INVESTIGATIONS:
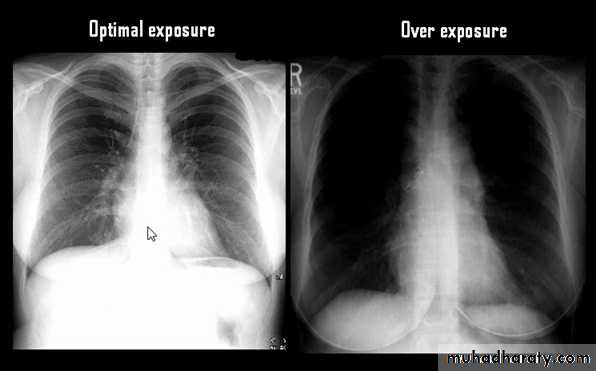
Techniques - Projection
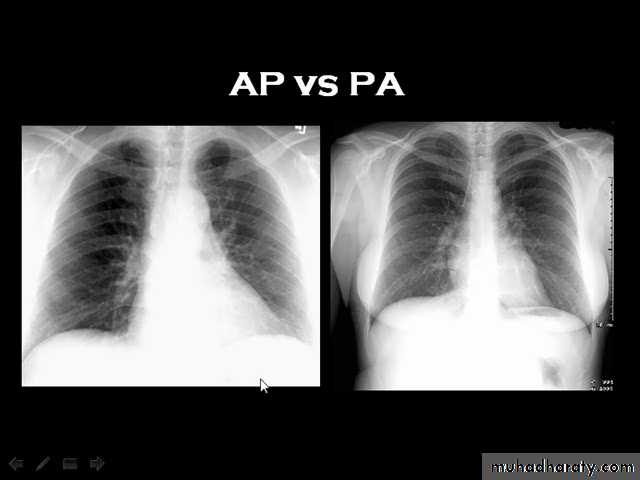
P-A (relation of x-ray beam to patient)
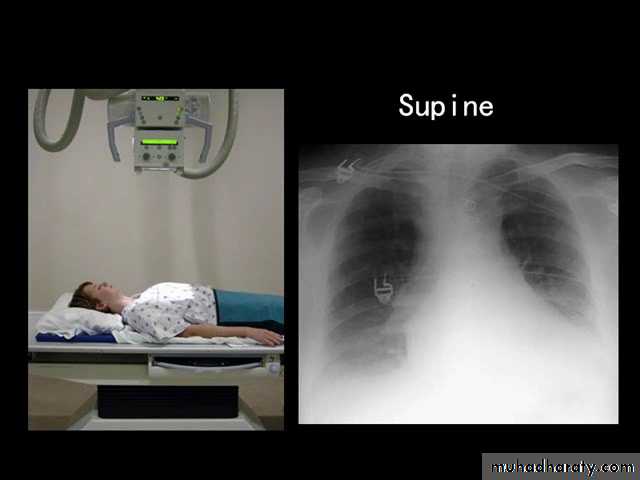
Supine view (AP)
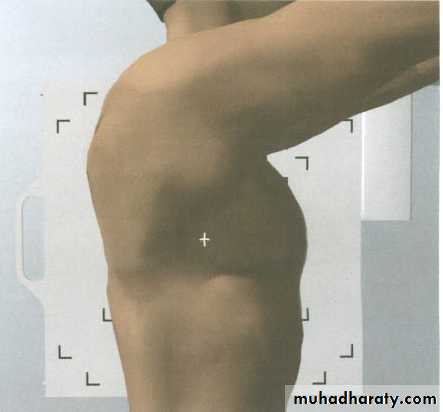
Lateral view .
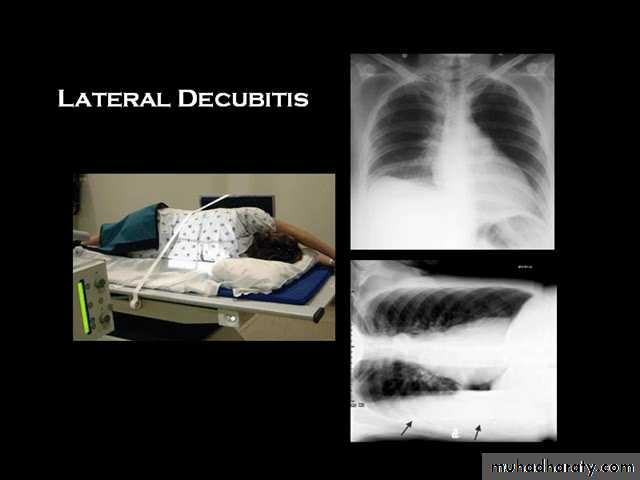
lateral decubitus .(in which the pt put on the suspected side & X-ray is taken (such as in pleural effusion).
LORDOTIC VEIW

Thoracic inlet view : to see hilar shadows, cardiophrenic angle shadow & right middle lobe collapse.
Routine Examination includes
P-A view , Other supplementary views are done according to the case. So all Patients admitted to hospital should have P-A X-ray In standing erect view in complete inspiration

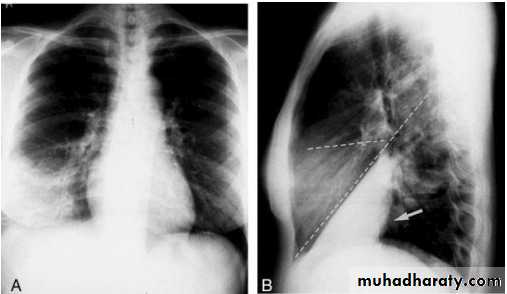
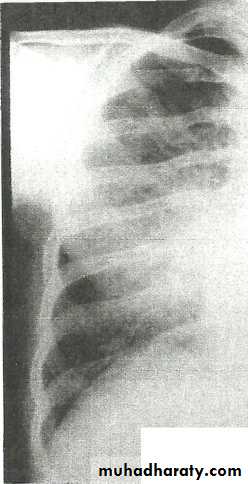
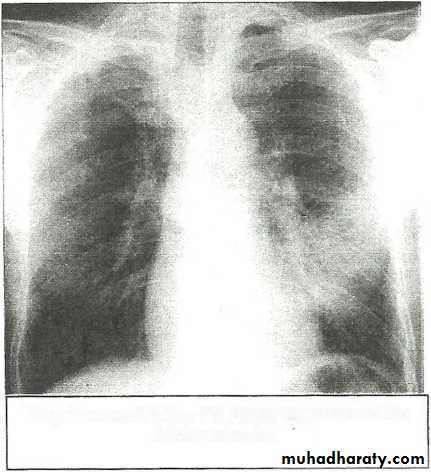
• LOBAR PNEUMONIA
Right lower lobe consolidation - PA. Dense opacification in the right lower zone with effacement of the outline of the right hemidiaphragm.
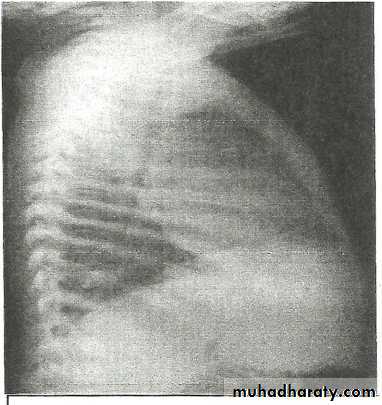
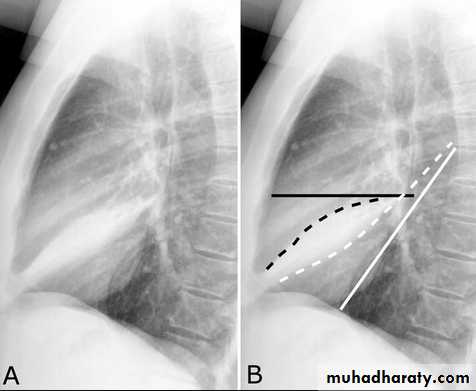
• Right lower lobe consolidation - Lat.
• The density lies posterior to fthe oblique issure- the position of the lower lobe.
BRONCHOPNEUMONIA
Mycoplasma pneumonia. A 35 year old man presents with nonproductive cough and fever
• Alveoiar oedema (‘Bat’s wings’)
• Kerlev B lines (interstitial oedema)• Prominent upper lobe vessels
• Cardiomegaiy
• Pleura
• effusion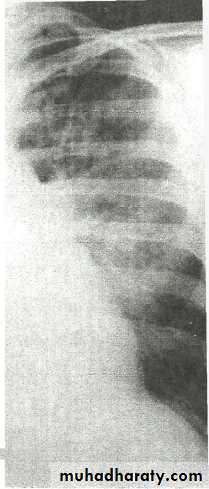
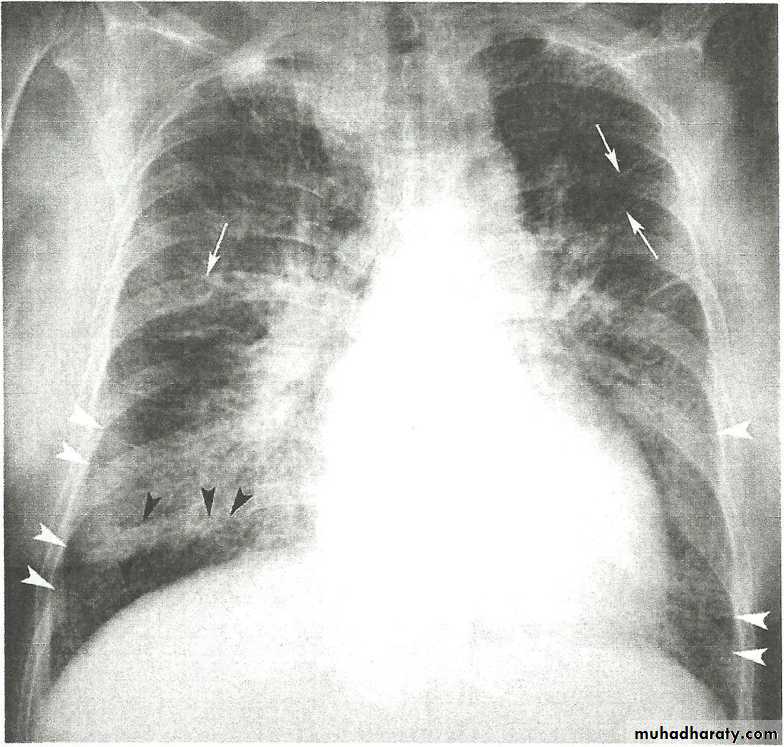
Kerley A lines (Arrows), Kerley B lines (arrowheads)
Lingular consolidation-PA. Patchy effacement of the left heart border.
Left upper lobe consolidation-Lat.
The opacification is sited anterior to the obliq- fissure-the position of the upper lobe.
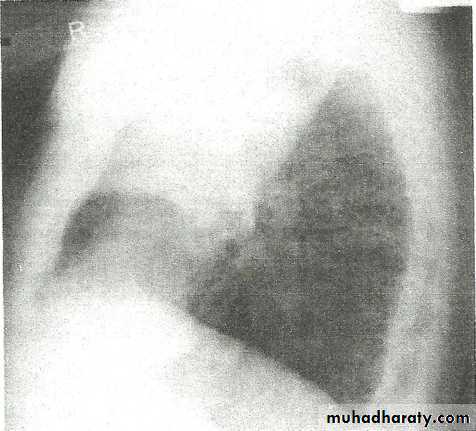
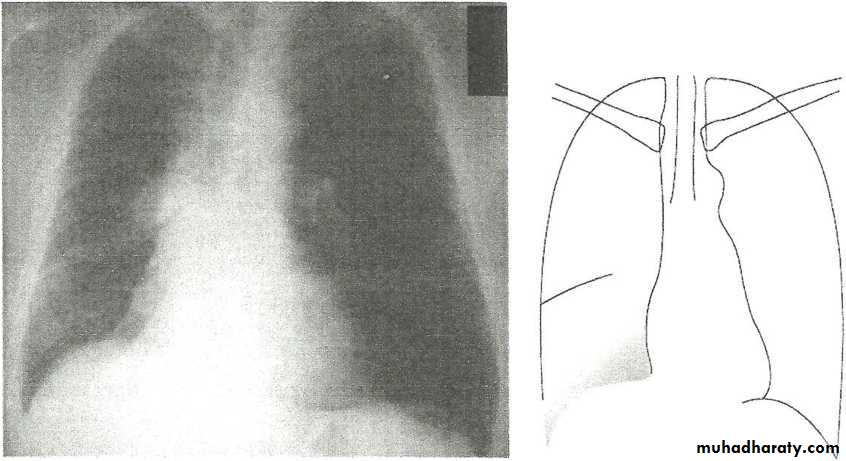
RLL collapse - PA.
•
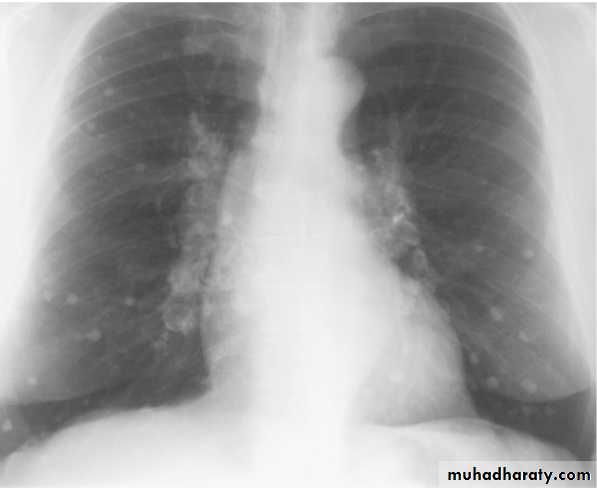
Nodular (coin) lesion in the left upper lung with irregular edge (most probably cancinoma
•
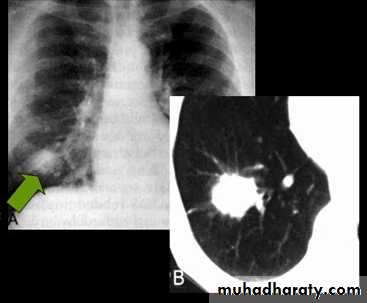





Differential diagnosis of multiple spherical lesions:
1 - Metastasis.2-Hydatid cyst.
3- Sarcoidosis.
4- Rheumatoid nodules.
5 – pneumoconiosis
6- Histoplasmosis
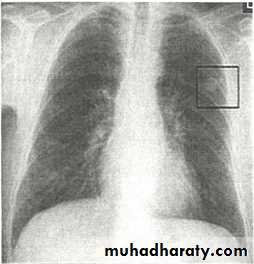
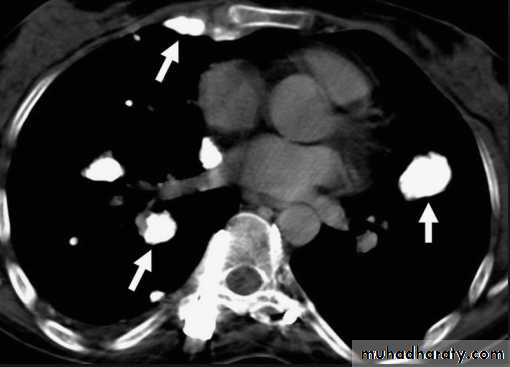
Chest X-ray shows radio-opaque (white) nodular lesion in the right mid-lung field.
Dx:x chicken pox , Histoplasmosis (calcified granuloma).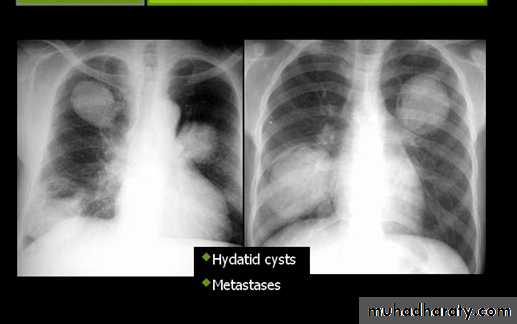
CAVITARY LESIONS
Abscess: necrosis of lung parenchyma +\-bronchial communication
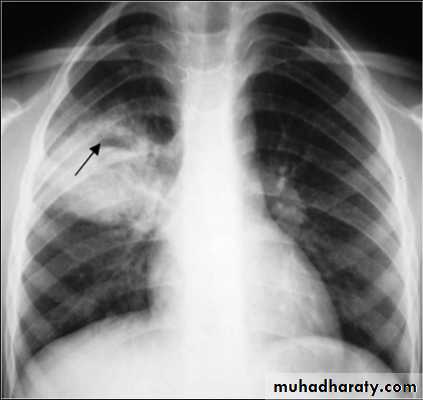
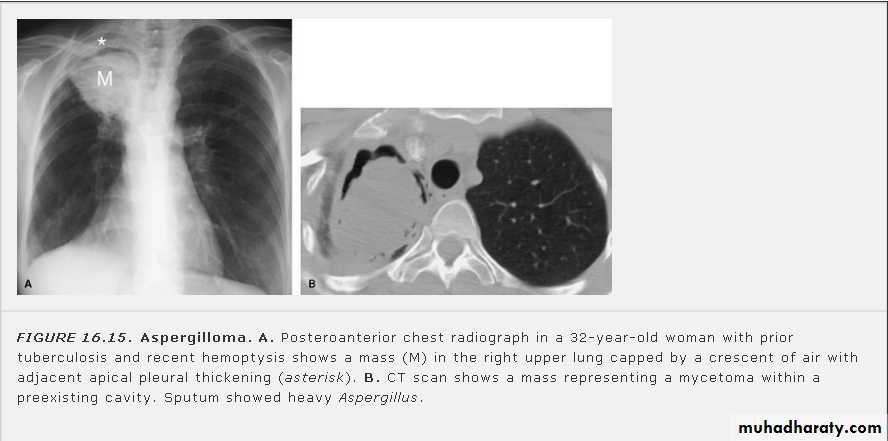
Fungus ball (air crescent sign)
Ruptured hydatid cyst (water lily sign)
Pneumatoceles due to air leak into
pulmonary interstitium (S. aureus)

CAVITARY LESIONS ( lung abcess)
A PA chest radiograph demonstrates a thick-walled cavity with fliud level adjacent to heterogeneous opacities in the left upper lobe.Necrotizing pneumonias and abscess formation .
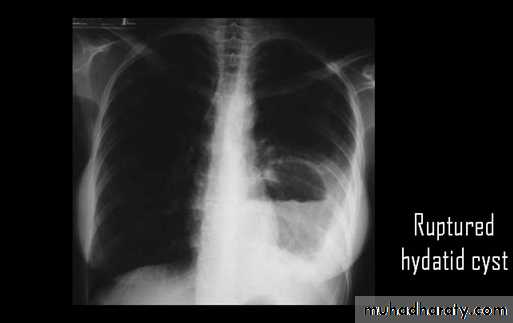
Ruptured H.C. With water lily sign .



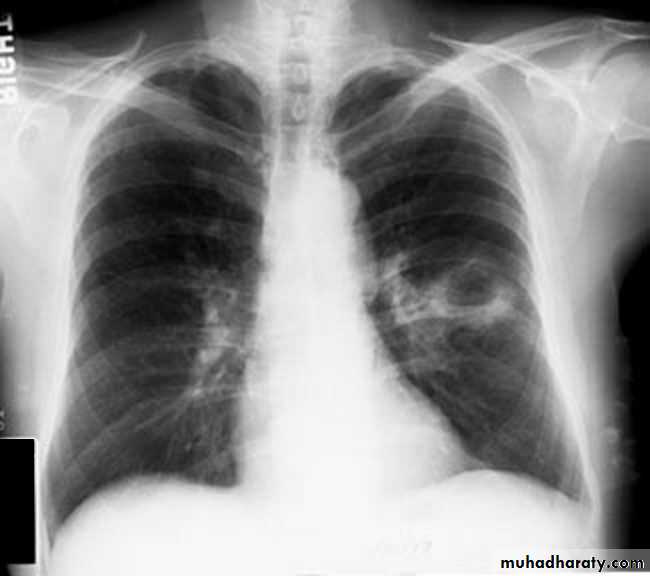
Un complicated Hydatid cyst of th lung , cuased by echenococus granulosis seen as well defined nodule or mass lesion .
Early rupture is sen as a cresnt air sign .ddx aspergillus ball
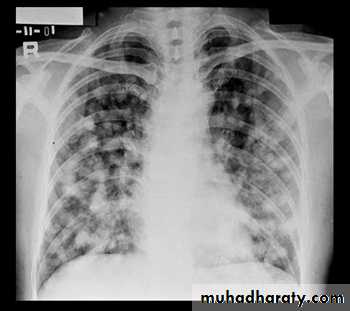
Miliary Tuberculosis. A cone-down view of a frontal radiograph demonstrates innumerable micronodular opacities characteristic of micronodular (miliary)
interstitial disease.
Transbronchial biopsy demonstrated caseating granulomas containing acid-fast bacilli.

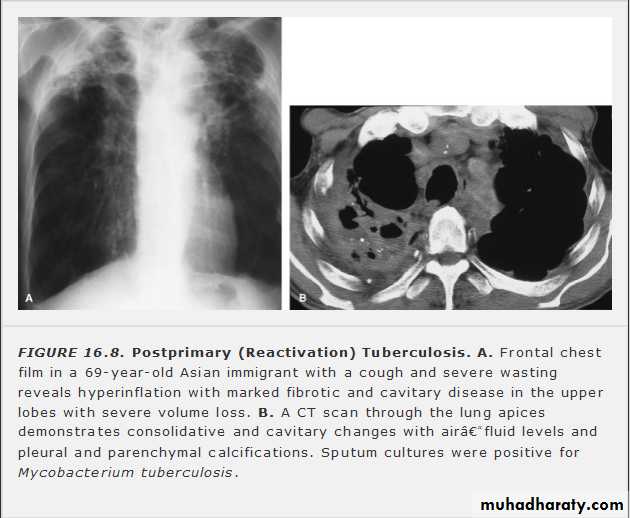
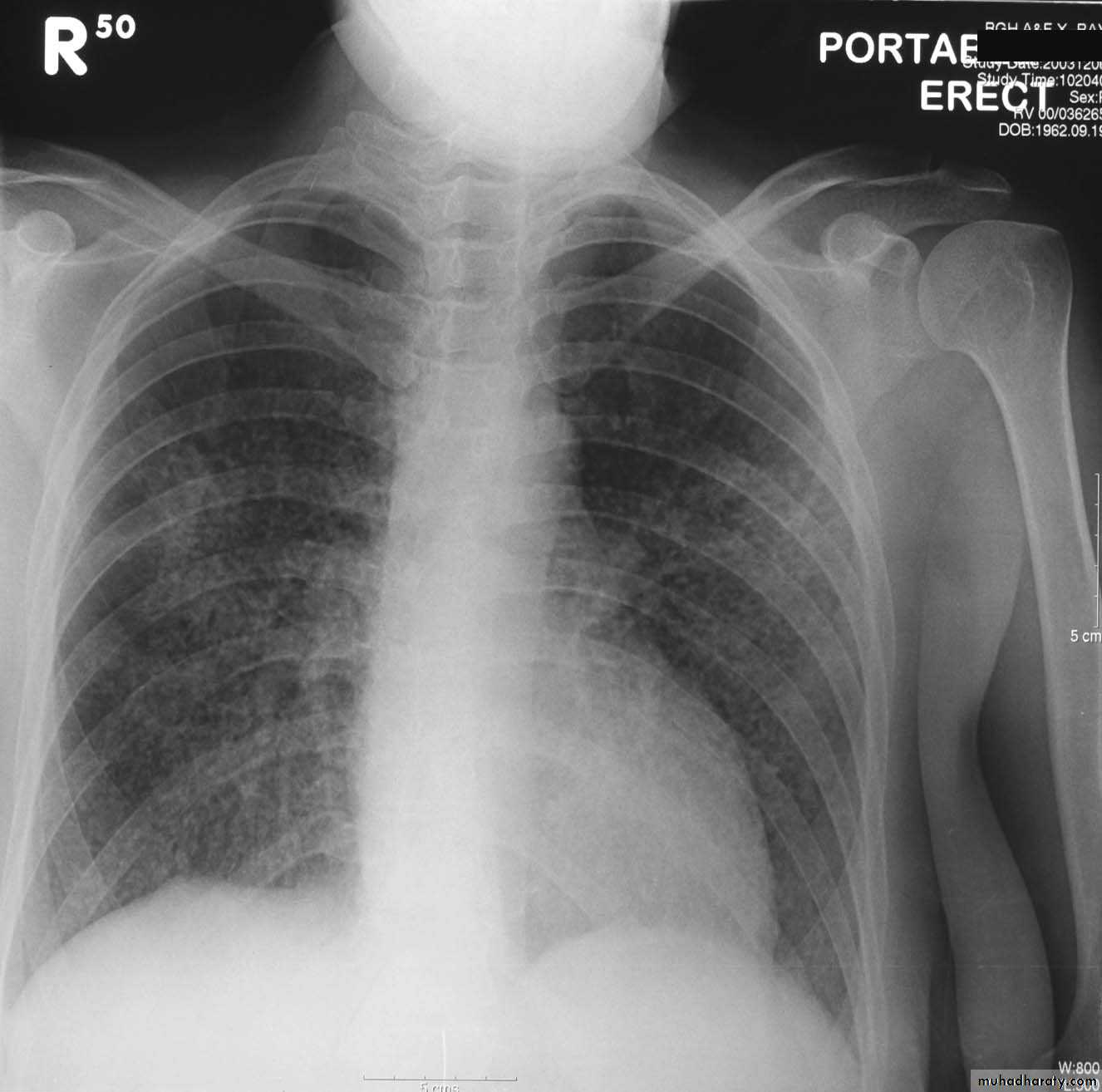
Miliary TB
a frontal radiograph demonstrates innumerable micronodular opacities characteristic of micronodular (miliary) interstitial disease. Transbronchial biopsy demonstrated caseating granulomas containing acid-fast bacilli.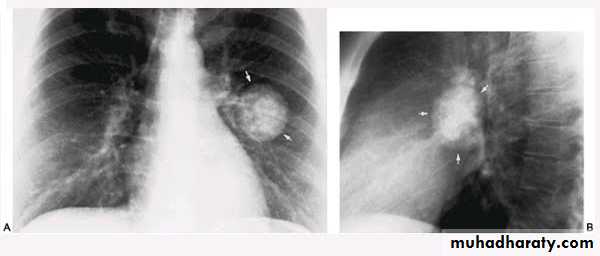
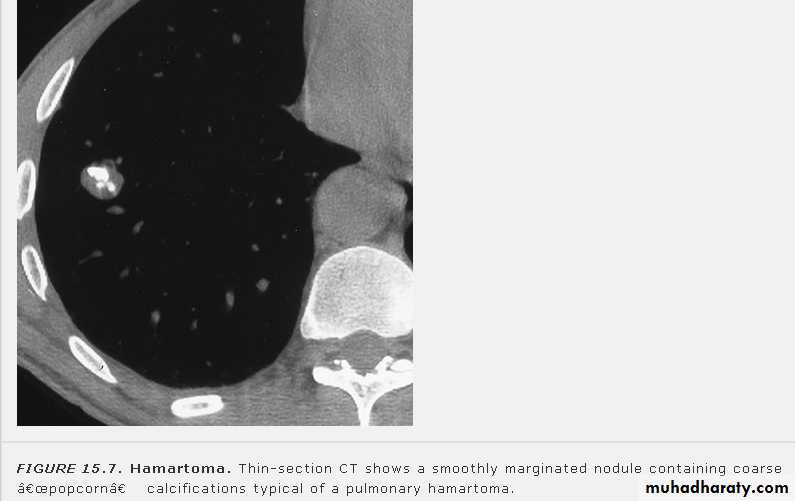
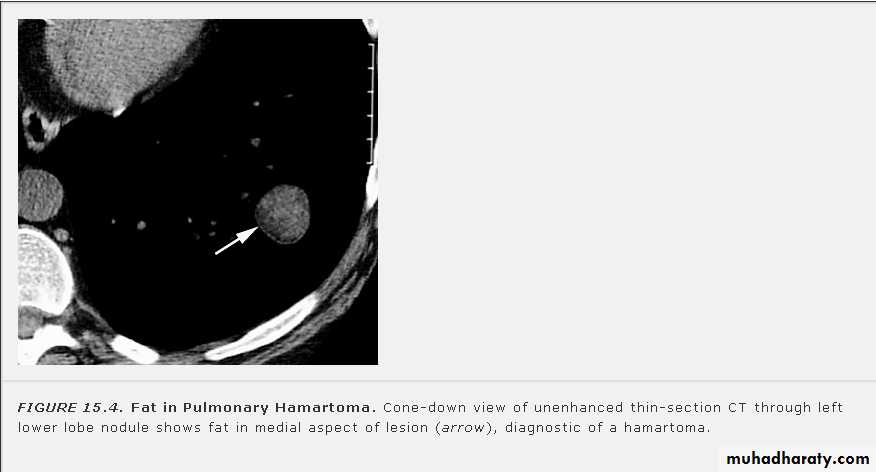
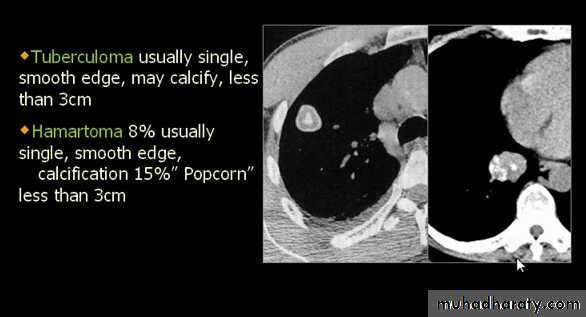
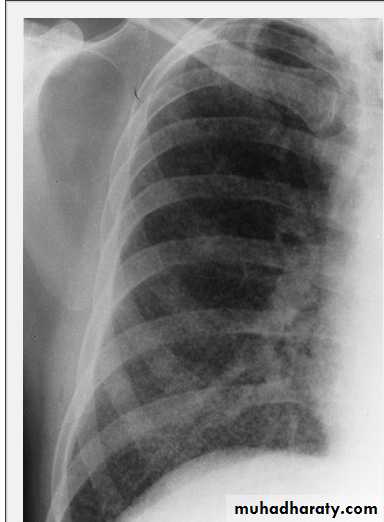
Tuberculoma
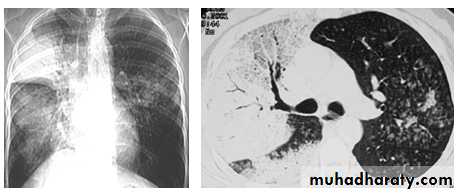
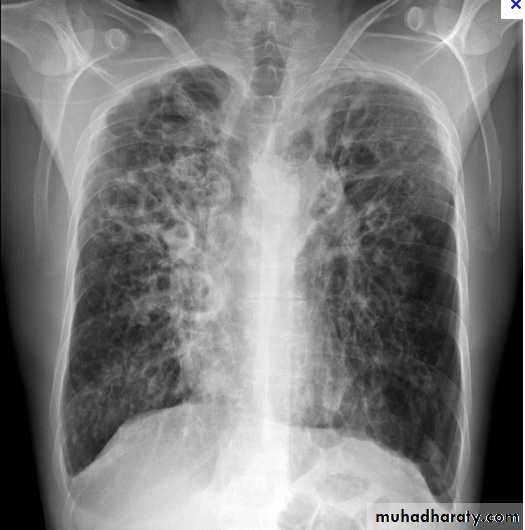
Plain film* Tramline: horizontal, parallel lines corresponding to (cylindrical ) thickened, dilated bronchi
* Bronchial wall thickening (best seen end-on) as honey comb appearance ( cystic ) .
* Indistinctness of central vessels due to peribronchovascular inflammation
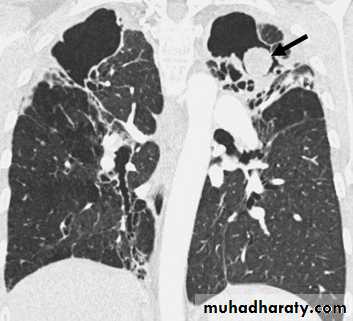
Atelectasis
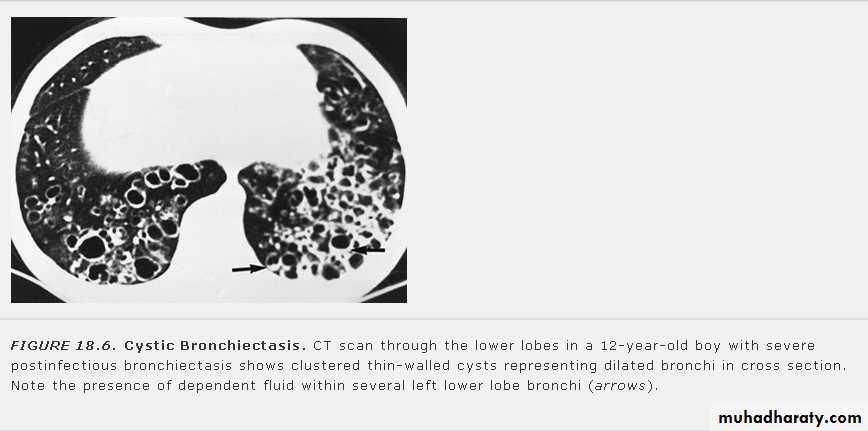
HRCT is more senstive , modality .of choice now adays
Signet ring sign : focally thickened bronchial wall adjacent to pulmonary artery branch .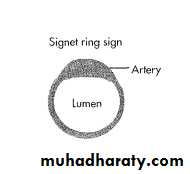

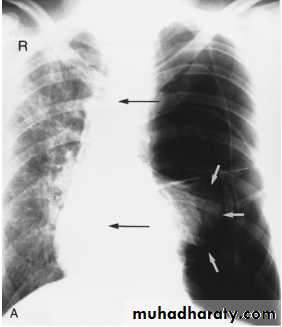
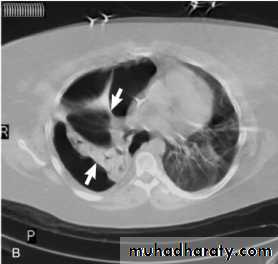
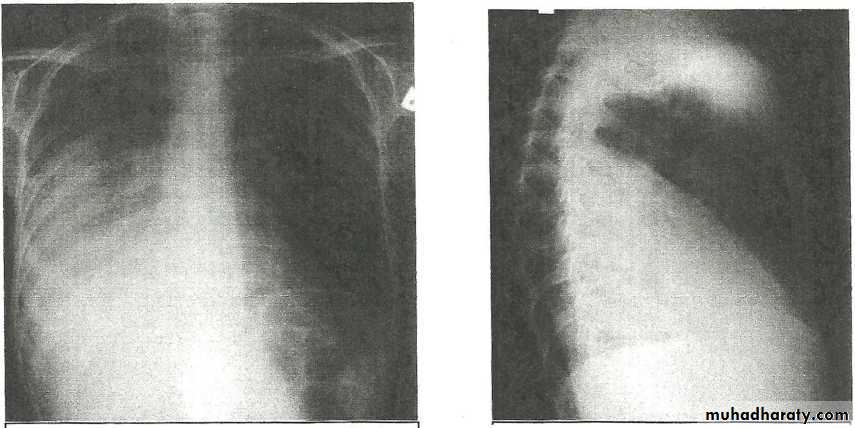
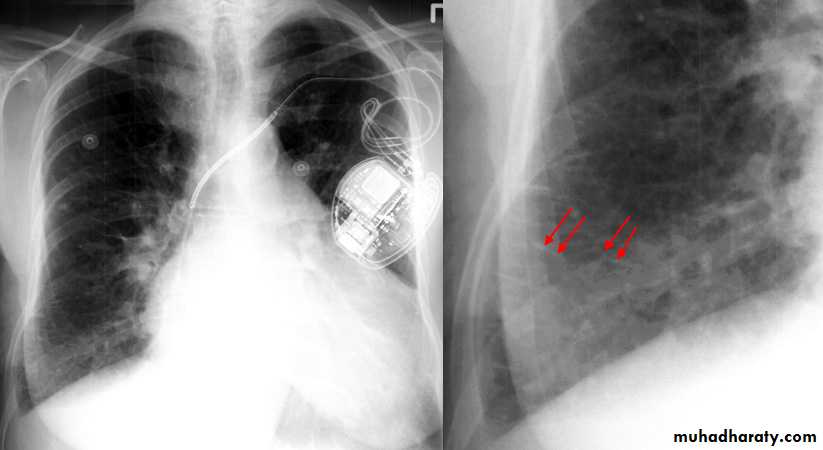
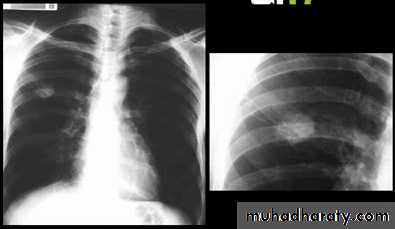
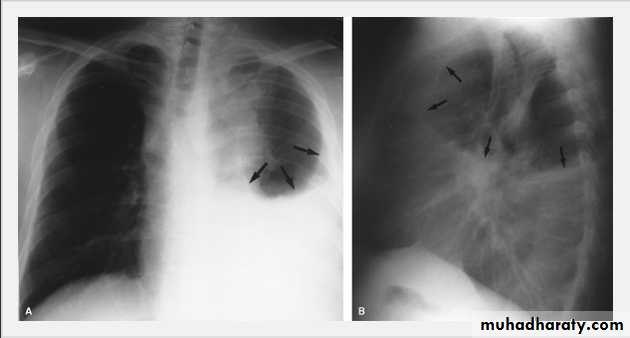
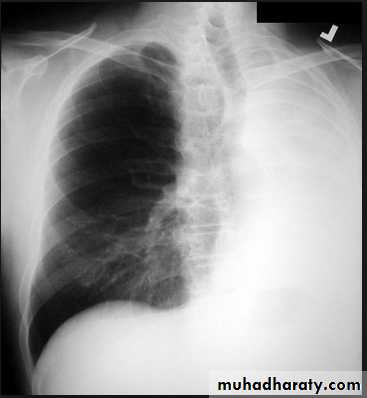
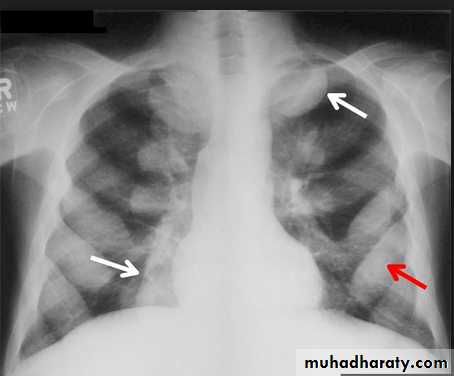
Tension pneumothorax.
On a posteroanterior chest x-ray (A), the left hemithorax is very dark or lucent because the left lung has collapsed completely (white arrows).The tension pneumothorax can be identified because the mediastinal contents, including the heart, are shifted toward the right, and the left hemidiaphragm is flattened and depressed. A computed tomography scan done on a different patient with a tension pneumothorax (B) shows a completely collapsed right lung (arrows) and shift of the mediastinal contents to the left.

Tension Pneumothorax. Portable chest film in a 43-year-old woman with ARDS shows a large right pneumothorax with mediastinal shift and ipsilateral diaphragmatic depression, suggesting tension.
Air was evacuated under pressure during emergent placement of a right chest tube.
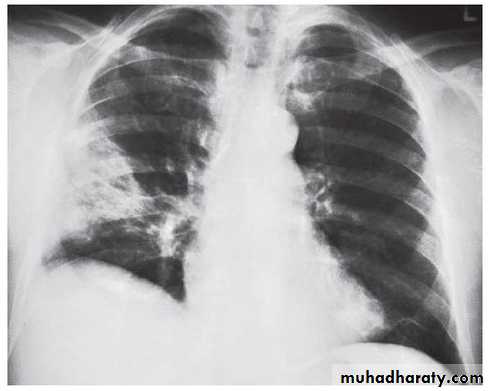
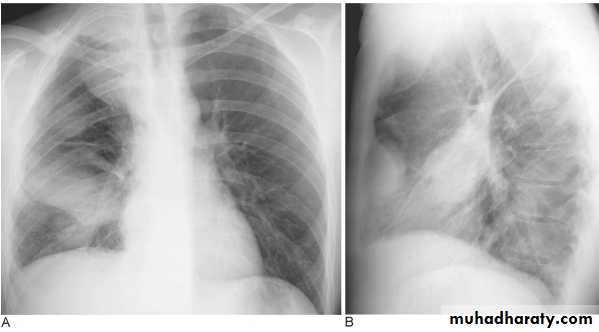
Pleural Effusion on Chest Radiographs.
Posteroanterior (A) and lateral (B) chest radiographs demonstrate the typical meniscoid appearance (arrows) in a patient with a left pleural effusion
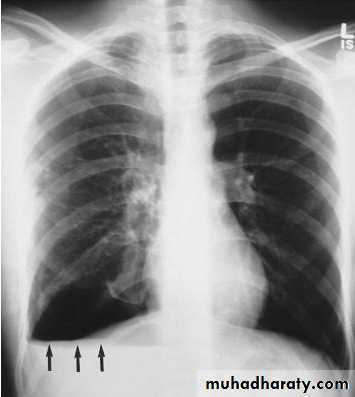
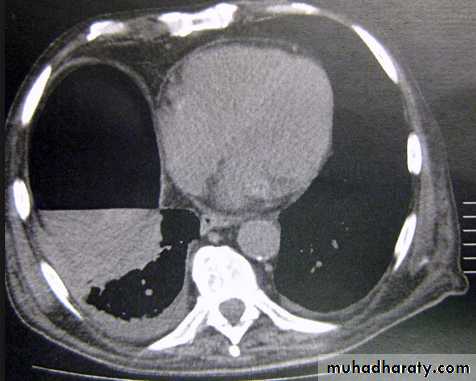
Hydropneumothorax.
When fluid and air are present in the pleural space on an upright chest x-ray, a perfectly straight horizontal line will extend all the way from the spine to the edge of the pleural cavity. In this patient, a loculated right basilar hydropneumothorax is present.The air/fluid interface is easily seen (arrows). If this were a lung abscess, the air/fluid level would be very unlikely to extend all the way from the medial to the lateral aspect of the hemithorax.
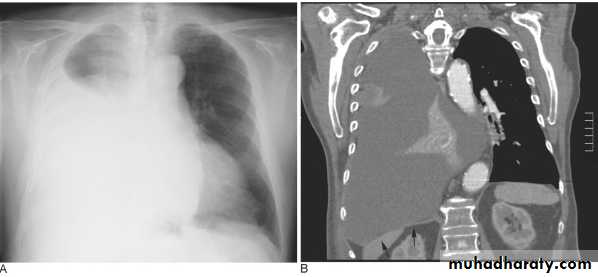
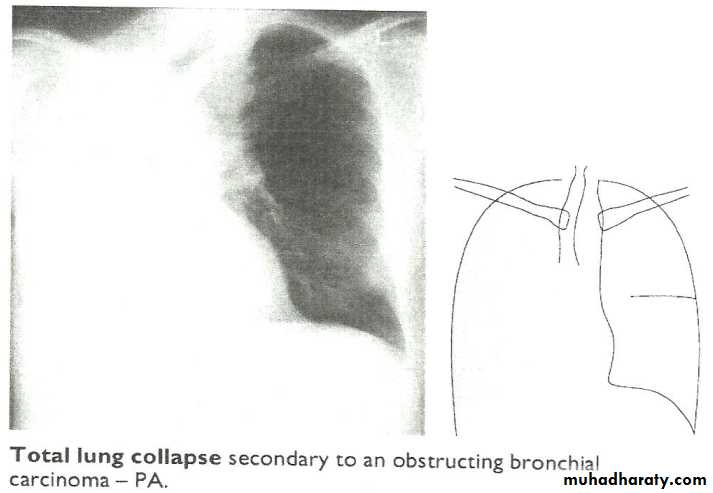
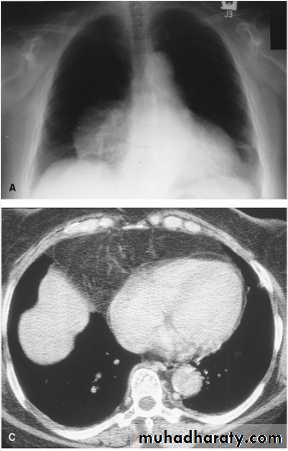
Massive pleural effusion with mediastinal shift to the left.
(A) Chest radiograph(B) CT coronal reconstruction. A massive effusion displaces the mediastinum to the left. CT shows the important pleural effusion together with the enhanced atelectatic left lung.
Note also the depression of the right hemidiaphragm (arrows).
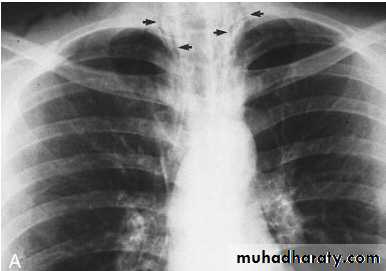
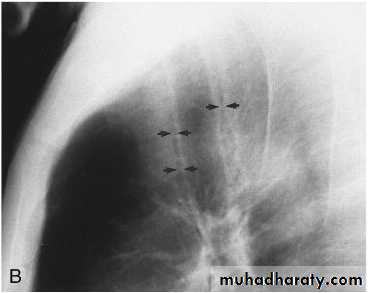
Pneumomediastinum.
Vertical dark (lucent) lines representing air within the mediastinum are usually seen at or above the level of the aortic arch.On the posteroanterior view (A), these can be seen extending up into the lower cervical soft tissues (arrows).
On the lateral view (B), dark linear air collections can be seen in front of and behind the trachea.
Encapsulated fluid
(A) PA and (B) lateral chest radiographs. Pleural fluid is encapsulated in the major fissure and against the anterior chest wall. These encysted fluid collections can mimic a lung tumour.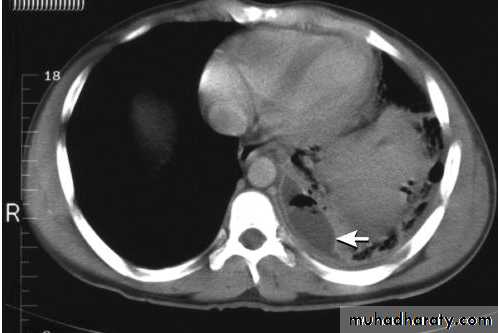
Empyema.
A computed tomography scan shows a posterior left pleural fluid collection (arrow) containing air (dark) and surrounded by thickened pleura.
The thickened pleura appears to be split by the lenticular fluid collection.
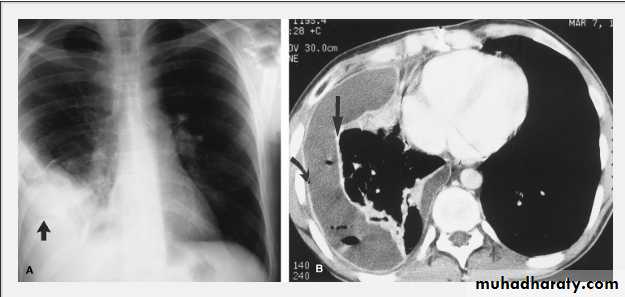
Empyema on Chest Radiograph and CT.
A. Posteroanterior chest film in a patient with a recent right lower pneumonia demonstrates an oval opacity in the right lateral costophrenic sulcus containing gas (arrow).B. An enhanced CT scan shows a circumferential pleural fluid collection with enhancing visceral (straight arrow) and parietal (curved arrow) pleural layers representing an empyema.
Note the contained gas pockets, indicating loculations within the collection itself.

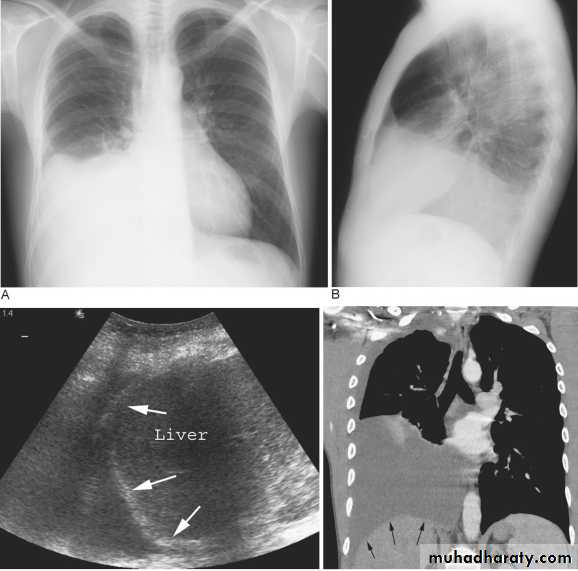
Subpulmonary pleural effusion. On the (A) erect PA and (B) lateral radiograph the effusion simulates a high hemidiaphragm. (C) Ultrasound and (D) CT clearly show that the effusion is located above the diaphragm. Arrows = diaphragmatic area.
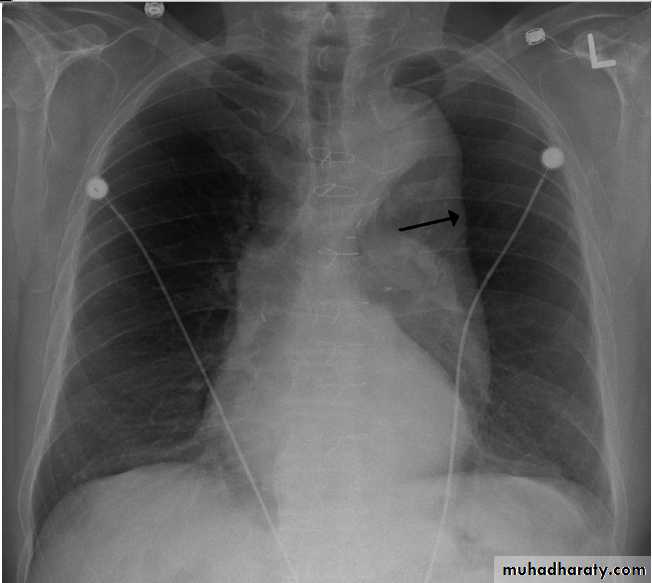

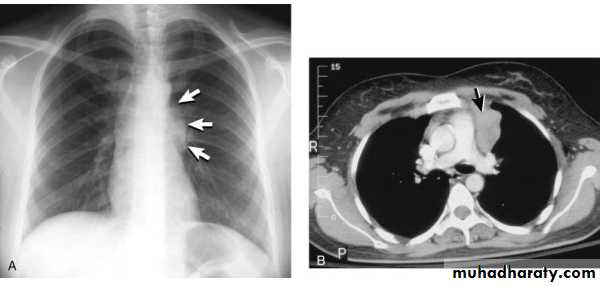
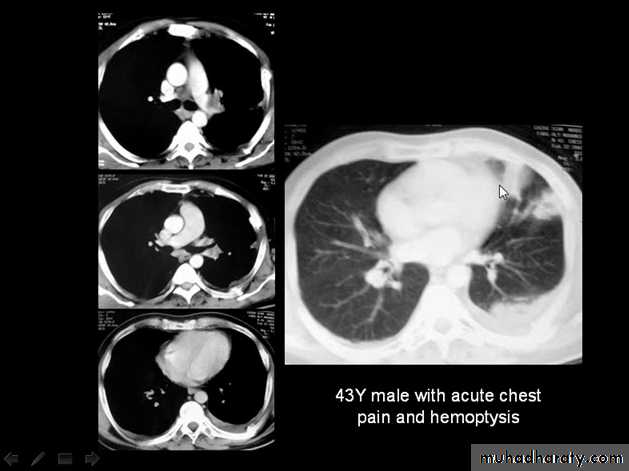
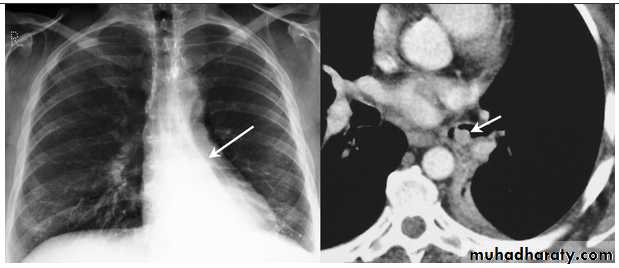
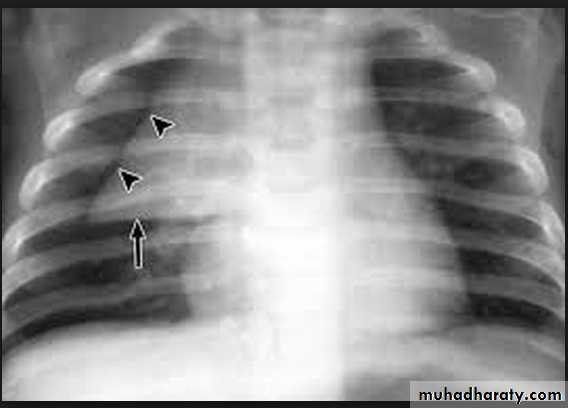
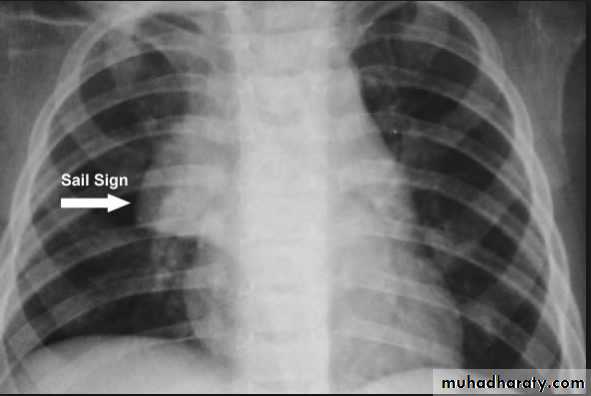
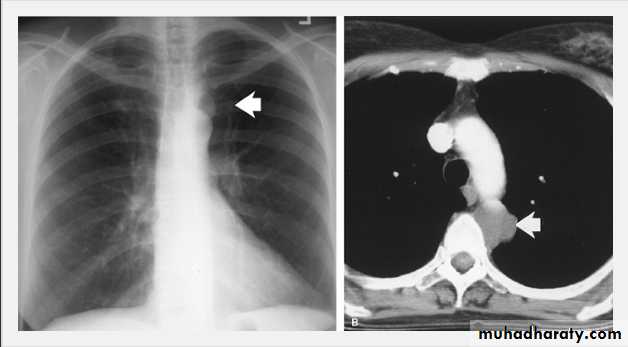
Thymoma.
A chest x-ray (A) reveals an unusual contour over the left hilum (arrows). That the hilum is not obscured (no silhouette sign) indicates that the mass must either be in front of or behind the hilum. A computed tomography scan (B) reveals a soft tissue mass (arrow) just to the left of the aorta. This is the most common location of a thymoma.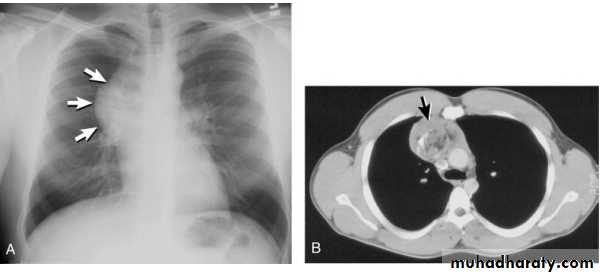
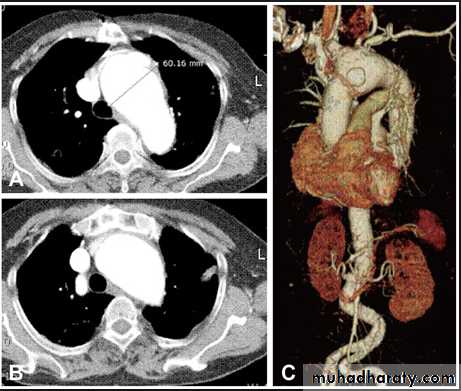
Mediastinal teratoma. A chest x-ray (A) shows a large upper right mediastinal mass (arrows), but no specific internal structure is apparent. A computed tomography scan (B) reveals that the mass contains multiple types of tissue elements including fat (dark), soft tissue (gray), and calcium (white). This is essentially diagnostic of a teratoma.
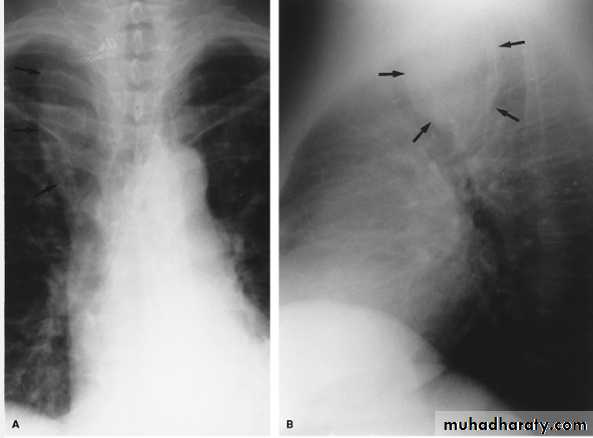
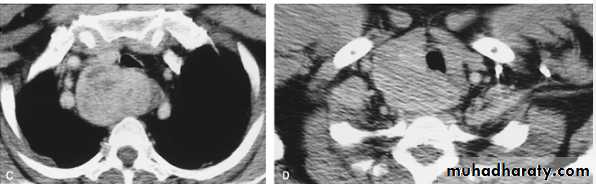
Thyroid Goiter. Posteroanterior (A) and lateral (B) radiographs show a right superior mediastinal mass (arrows) compressing the trachea from the posterior. C. Contrast-enhanced CT at the level of the sternoclavicular joints shows inhomogeneous increased attenuation and enlargement of the thyroid gland that extends retrotracheally. D. More superiorly, the mass is contiguous with the right lobe of an enlarged gland.
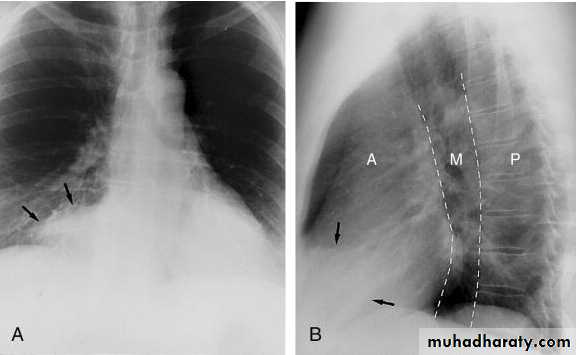
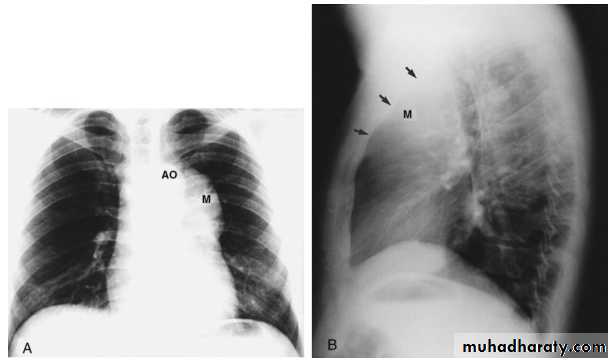
Pericardial fat pad. A, A soft tissue mass (arrows) is seen in the right cardiophrenic angle on the frontal chest x-ray. B, It also is seen in the anterior mediastinum on the lateral view. On this view, the anterior (A), middle (M), and posterior (P) portions of the mediastinum have been identified.

Foramen of Morgagni Hernia. Frontal (A) and lateral (B) chest radiographs in a 60-year-old woman reveal a large mass in the right cardiophrenic angle. C. CT scan at the level of the diaphragm shows a fatty pericardiac mass containing omental vessels
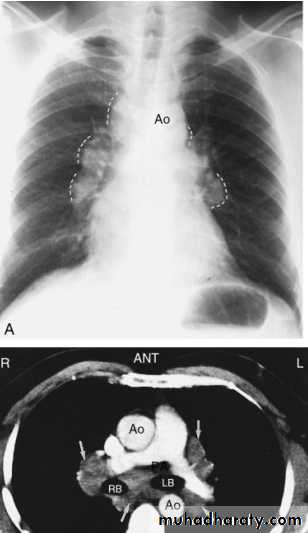
Sarcoid.
Marked lymphadenopathy (dotted lines) is seen in the region of both hila in the right paratracheal region (A).The transverse contrast-enhanced computed tomography scan of the upper chest (B) clearly shows the ascending and descending aorta (Ao) as well as the pulmonary artery (PA) and superior vena cava. The right and left main-stem bronchus area also is seen. Arrows, the extensive lymphadenopathy.
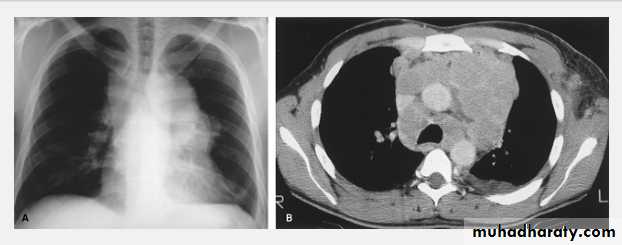
Hodgkin Lymphoma. A. Posteroanterior chest radiograph in a 35-year-old man shows a large, lobulated mediastinal mass. B. Contrast-enhanced CT at the level of the aortic arch shows bulky anterior and middle mediastinal lymphadenopathy
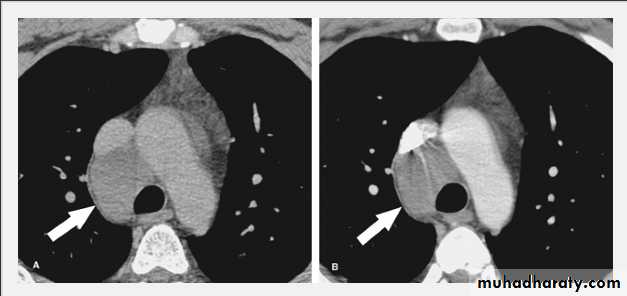
Bronchogenic Cyst. Unenhanced (A) and enhanced (B) CT scans in a 38-year-old man demonstrate a smooth, low-attenuation paratracheal mass (arrows) that fails to enhance, consistent with a bronchogenic cyst.
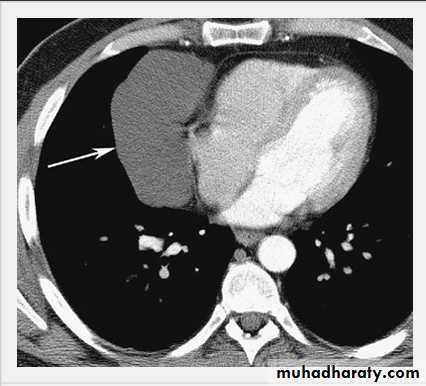
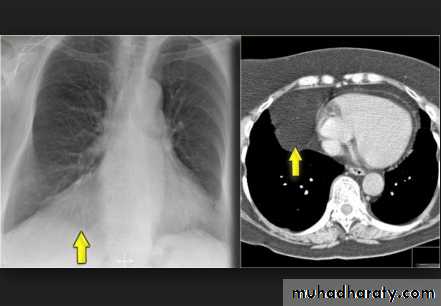
Pericardial Cyst.
Enhanced CT scan through heart shows a smooth, sharply marginated, low-attenuation mass (arrow) in the right cardiophrenic angle, consistent with a pericardial cyst.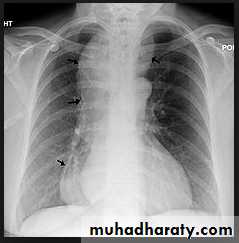

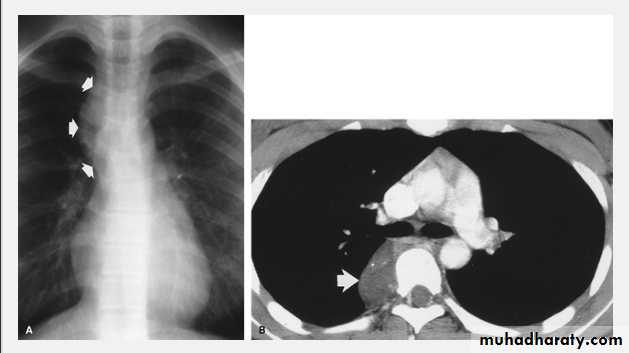
Neurofibroma.
A. Frontal chest radiograph shows a left upper mediastinal mass (arrow).B.Contrast-enhanced CT confirms the presence of a left paravertebral soft tissue mass (arrow). Surgical resection confirmed a neurofibroma.
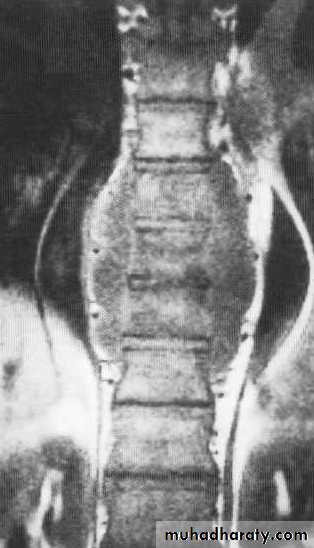
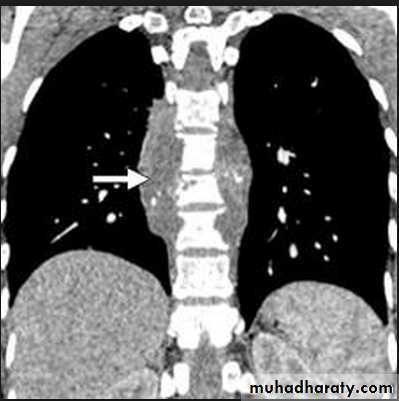
The plain film shows features which are typical for spinal tuberculous disease.
There is an extensive paraspinal soft-tissue mass.Detail in the underlying spine is poor but there is early crowding of ribs posteriorly, indicating early vertebral collapse.
(B) Coronal MR image of the thoracic spine demonstrates destruction of the intervertebral disc at the point where the paraspinal widening is maximal and this change is associated with alteration of signal from the vertebrae.

Ganglioneuroma.
Posteroanterior radiograph in a 15-year-old woman reveals an oval, vertically oriented, right-sided mediastinal mass (arrows).B. Contrast-enhanced CT shows a low-attenuation posterior mediastinal mass (arrow) with calcification. This was surgically proven to be ganglioneuroma

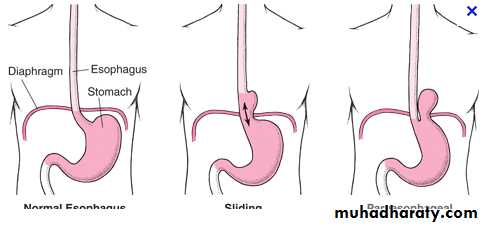
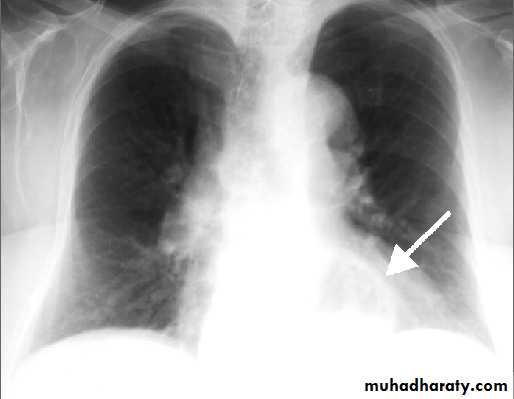
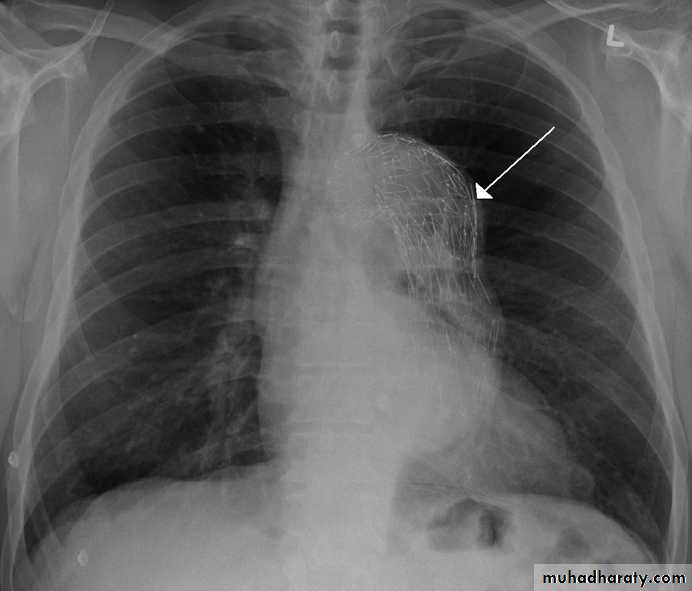
PA chest X-ray: A smooth-contoured cavity of 5 cm diameter, containing gas fluid level, is visible behind the heart shadow (arrow). This lesion is the gas-containing fornix protruding into the chest cavity through the esophageal hiatus.

A barium swallow study demonstrates a large hiatal hernia with the majority of the stomach in the chest, not in the abdomen where it belongs.
