1
Forth stage
Surgery
Lec-2+3
د
.ا
ح
م
د
أ
ب
ر
ا
ه
ي
م
4/10/2015
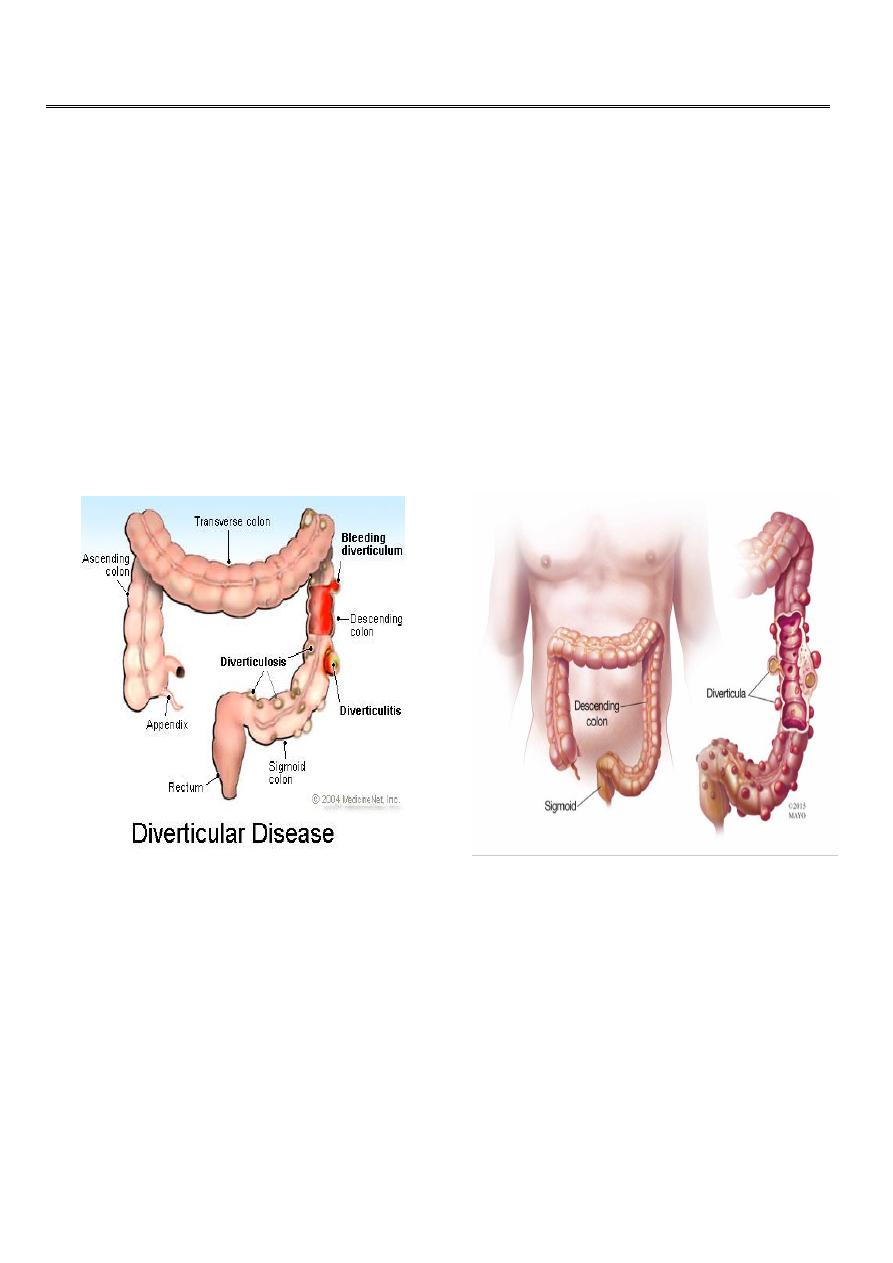
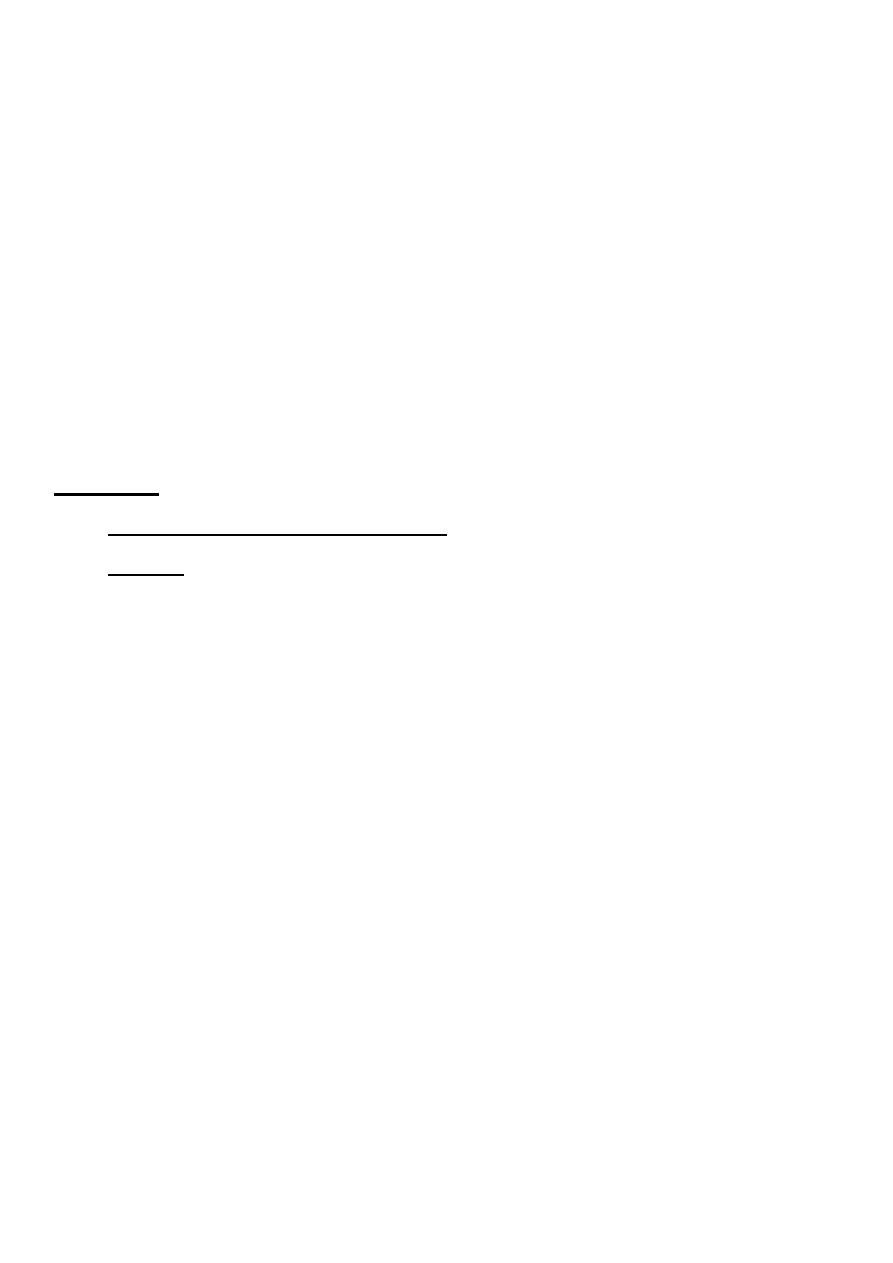
Diverticulitis Disease of the Large Intestine II
Found around 75% of over seventy year olds in western world.
Mostly affect sigmoid colon, but can occur in the caecum or the whole colon (but not
the rectum).
Diverticula are most often asymptomatic (diverticulosis) and found incidentally, but can
present clinically with sepsis or haemorrhage
.
Aetiology: western diet deficient in dietary fibre
Complications of diverticulitis disease:
1. Diverticulitis
2. Perforations, leading to peri colic abscess occasionally generalized peritonitis.
3. Intestinal obstruction lead to fibrosis can cause stenosis or loops of small bowel
4. Adhere to inflamed sigmoid.
5. Haemorrhage, diverticulitis may cause haemorrhage.
6. Fistula, colovesical , colocutanous , colovajnal, enterocutaneous.
2
Classification of contamination:
The major of sepsis impact on the outcome in acute diverticulitis .
The most commonly used system of classification is: Hinchey
Classification of complicated diverticulitis.
Grade
i. Mesenteric or pelvic abscess.
ii. Pelvic abscess.
iii. purulent peritonitis
iv. faecal peritonitis.
Radiology:
• Plain chests and abdominal radiograph can demonstrate pneumoperitonium.
• Spiral CT,identifying the bowel wall.
• On identifying of abscess in stable patient ,drainage maybe carried out per
cutaneously.
• Barium enemas and colonoscopy,avoided in acute cases.How can be used after the
attack has settled to exclude a co existing carcinoma.
• Colovesical fistula evaluated with cystoscopy and biopsy in addition.
The differential diagnosis for colovesical fistula includes:
• Cancer
• Radiation injury
• Crohn's disease
• Tuberculosis
• Actinomycosis .

3
Management
Conservative
1. Nothing by mouth, rest to the bowel.
2. I.v.fluid and antibiotics for gram negative bacilli and anaerobes.
3. CT. scan can confirm the diagnosis and assess the complications.
Principles of surgical management:
• *Hartman's procedure ,safest option in emergency surgery
• ** primary anastamosis in selected patients
• *** elective resection
• **** colovesical fistula requires resection.
Tumours of the large Intestine III
Benign:
• Polyp: is protrusion of the mucosa.
Classification of intestinal polyps:
• Inflammatory. Inflammatory polyps ( pseudopolyposis in ulcerative colitis)
• Meta plastic. Meta plastic or hyperplastic polyps
• Hammartomatous.
Peutz- jet hers polyp
Juvenile polyp
Adenoma.
Neoplastic.
Tubular ,tubulovillous ,villus
Adenocarcinoma ,carcinoid tumor
4
Adenomatous polyp:
• Varies from tubular to villus.may be solitary and the cause of rectal bleeding or
sometimes villous and the cause of hypo Kalaemia and Hypoalbuminaemia .the risk
of malignancy increases with their size .
• Familial adenomatous polyposis: defined to have more than 100 polyps and multiple
extra intestinal manifestation like endodermal( adenomas of duodenum,stomach) or
ectodermal like epidermoid cysts ,brain tumours . And mesodermal like
desmoid,dental problems,or osteomas.
• Gardener's syndrome: familial polyps with epidermoid cyst and desmoid tumours.
Features of familial adenomatous polyposis:
1. Autosomal dominant
2. More than 100 colonic adenomas
3. Prophylactic surgery
4. Polyps and malignant tumours can develop in the duodenum and small bowel.::
5. Treatment
6. Colectomy with ileorectal anastamosis
7. Restorative proctocolectomy with ileal pouch
8. Total removal with end ileostomy.
Lynch syndrome: characterised by increased risk of colorectal cancer and also cancer of
endometrium,ovary,stomach and small intestine.

5
Malignant:
• Epidemiology in UK colorectal cancer is the second most common cause of cancer
death .
• Aetiology: the accepted model arises from adenomatous polyps after genetic
mutation influenced by environmental factors . The p53 gene mutated in carcinomas.
• Linkage between diet and colon cancer
• Ulcerative colitis
• Suggested after cholecystectomy increase risk
• Also increased risk after ureterosigmoidostom
Pathology:
Macroscopic
• Four types; annular,tubular,ulcer,cauliflower.
Microscopic
• It is adenocarcinoma originating in the colonic epithelium
A.L.Y