Coronary Artery Disease
Prof Hassan Yousif AlnajjarBaghdad Nov..2014
Introduction
Coronary Artery Disease is the most common cause of Morbidity and mortality worldwideIn Iraq it is very common
Coronary artery disease is caused by atherosclerosis in almost all cases
Atherosclerotic lesion causes Ischaemia of the myocardium hence it is called schaemic Heart Disease
Aim of lectures
1- Discuss etiology and Risk Factors of Aherosclerosis its prevention2-Discuss the pathophysiology of the ischaemic syndromes
3- Try to link the symptoms of the Ischaemic syndrome to the underlying pathology
Atherosclerosis
1- Increased atherogenic lipoproteins levels favour t their subendothelial accumulation where they undergo chemical alteration such as oxidation rendering them unclearable, and resulting In the trigger of self-perpetuating inflammatory process2- They will be taken by macrophages to form foam cells that will attracts more inflammatory cells such as fibroblasts. Myofibrils migrates from the media to the intima an multiply.
3- Eventually atheromatous plaque forms in the subendothelium starting with fatty streaks ending with large plaque that impinge on the lumen
Site of atherosclerosis
Probably affect the whole arterial tree but not uniformly ie patchy and selective
Affects the medium size arteries eg the coronaries, the femorals and the carotids
More at bifurcation.
More at jet site when the artery curve around
Can be concentric or eccentric
Etiology of Ayherosclerosis
Etiology is Unknown but there areRisk Factors. They are multiplicative
1- Age and Sex Not M
2- Smoking M
3- HTN M
4- DM ? M
5- Dyslipidaemia M
6-Family h. Not M
7-Obesity M
8-Inactivity M
New risk factors
HyperinsulinaemiaGlucose intolerance
Hyperfibrinogenaemia
Anti phospholipids' syndrome
The last two factors are associated with recurrent arterial thrombosis in total agreement with the new name of
Atherothrombosis
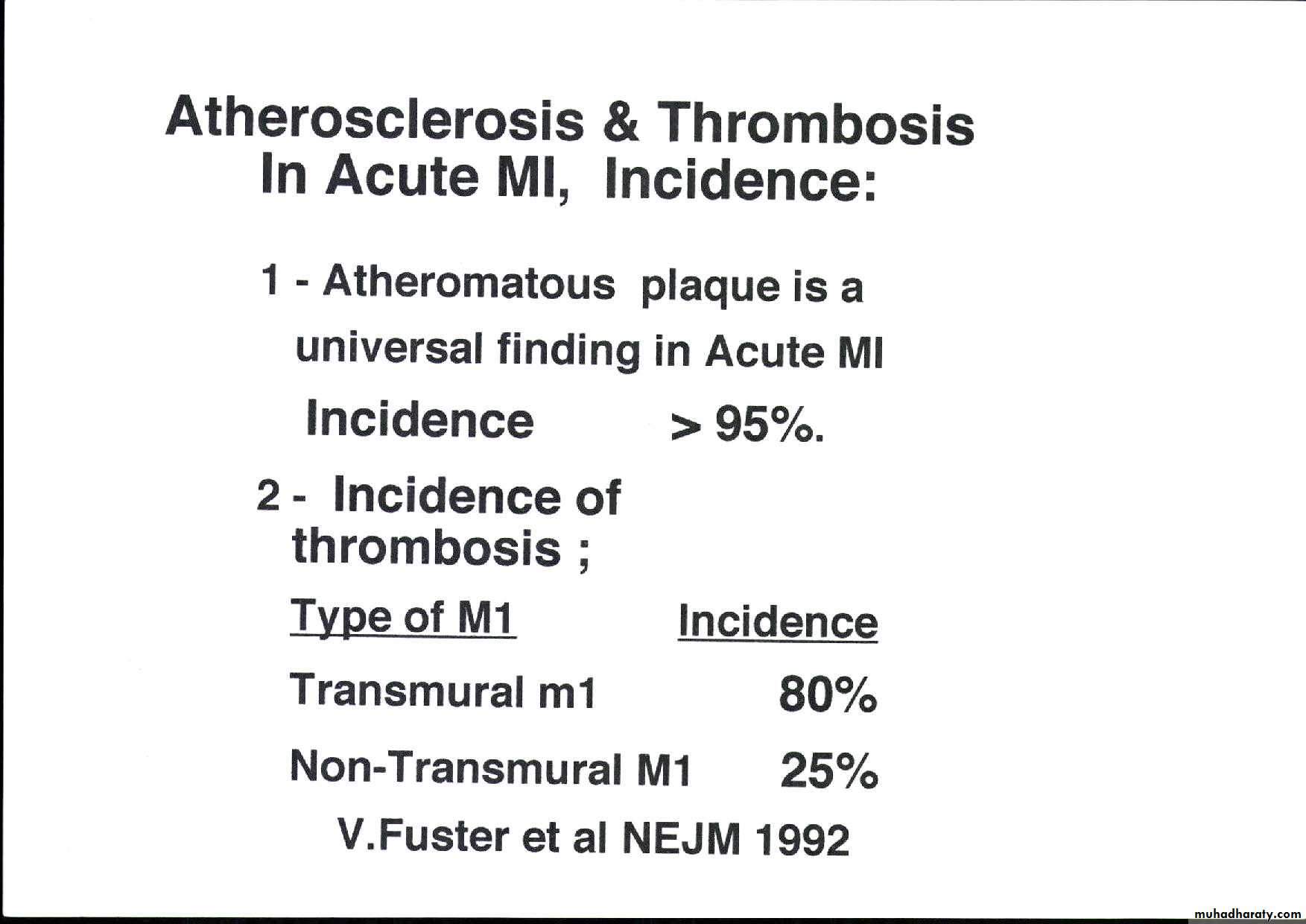
Atherosclerosis and Thrombosis
Plaque fissuring, cracking or even rupture
Exposure of subendothelium
Activation of thrombin and platelets leading toThrombosis hence the new name
Atherothrombosis
Manifestation of atherosclerosis
Atherosclerosis is a pan-arterial disease hence it affects almost all systems but the effects on the CVS and the brain is far disastrous where it causesStable and Unstable Angina and Myocardial Infarction ;
Heart Failure
Arrhythmia
Sudden death
Valvular heart disease; Acute or Ch. MR
Peripheral Vascular disease
Aneurysm of the Aorta
Dissection of the Aorta
TIA and Stroke
Determinant of Outcome of atherosclerotic plaque
Depends on
1-Stability of plaque
2- Structure and territory supplied.
3 Severity of Stenosis -
Stability of PLAQUE
The whole mark of atherosclerosis is theAtherosclerotic plaque which impinges on arterial the lumen and can impair flow
The plaques are mainly two types
1- Cellular and less fibrotic with thin cap hence unstable and susceptible to rupture
Leading to Unstable Angina or Infarction
2-Less cellular more fibrotic with thick cap ie Stable plaque ; may cause Angina Pectoris
Outcome of atheroma plaque
A -Stable plaque Outcome depends on severity1- Mild stenosis is asymptomatic
2- Moderate- total occlusion may cause
1-Silent Ischaemia
2- Ch. Stable angina.
3-Formation of Collaterals will be induced Chronic Ischaemia. Pt may remain asymptomatic
B- Unstable plaque can rupture then thrombose. Outcome depends on whether it led to
1- Partial occlusion Unstable Angina or
2-Total occlusion Acute MI
Pathophysiology of Angina :- is chest pain caused by imbalance between O2 supply and O2 demand
physics law;- Flow in a narrowed tube depends o
1- Severity of narrowing ; degree of stenosis
2- Pressure gradient across the stenosis
In coronary artery stenosis significant reduction of flow occur when the narrowing is 70%+ .
A70% Stenotic plaque causes significant reduction of O2 supply to the myocardium
This reduction is worsened by increased demands by increased heart rate ; causing pain : ie angina
Other causes of Angina :-
A Other Important factors that reduce O2 SUPPLY1- Coronary thrombus
2- -coronary spasm
3- Anaemia
B-Other Important factors that increase DEMAND
LVH due to HTN, AS, or HOCM
Chronic stable angina; Angina pectoris
Episodes of chest pain that is usually triggered by exertion. and relieved within 5 min of by rest or sublingual Nitroglycerine. The reproducibility and the predictability , and its relationship to exertion is most important features. The duration of the symptom is important. Recent onset angina is more risky than longstanding stableCriteria of ischaemic chest pain
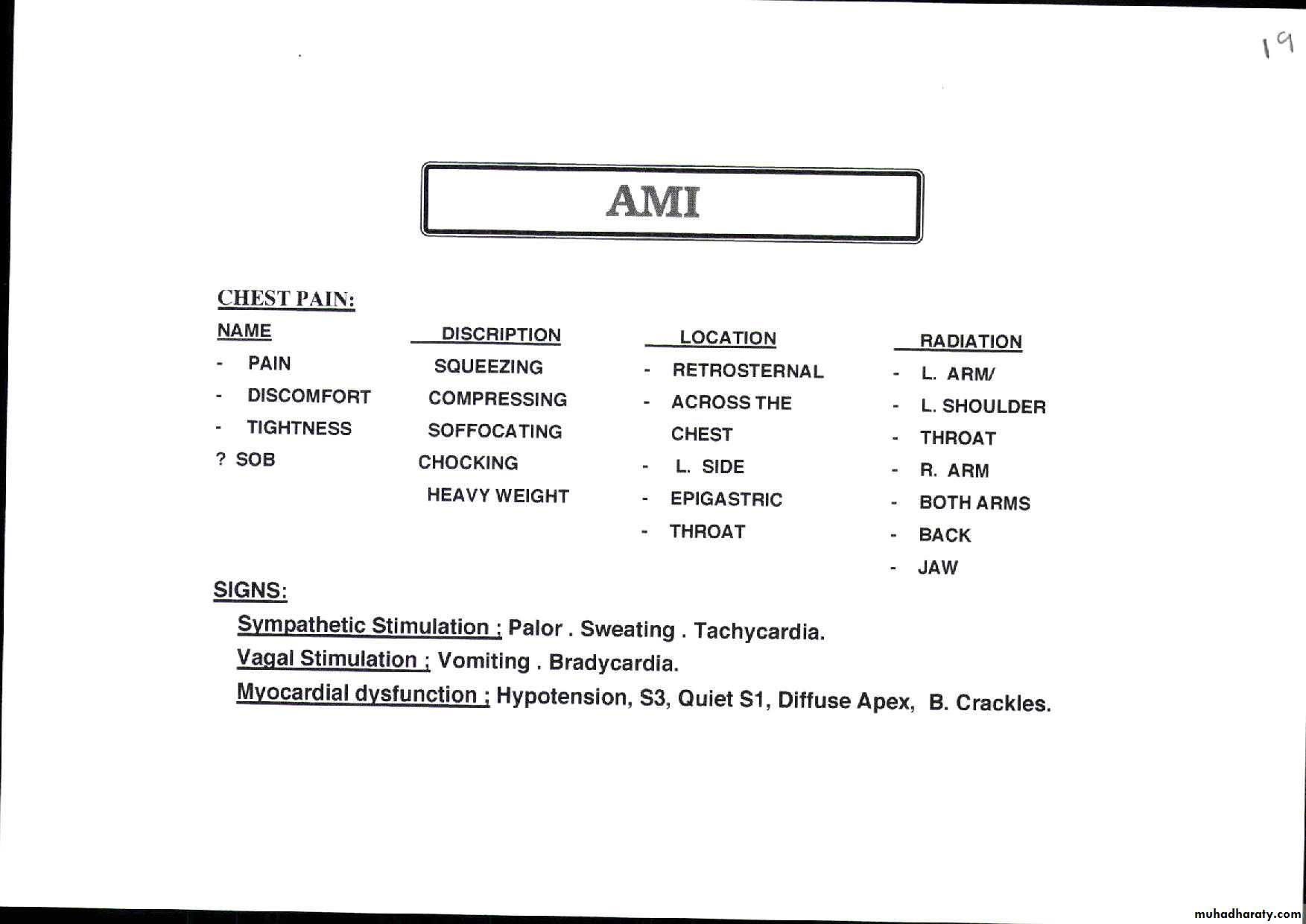
Type
Dull Constricting
Chocking
Squeezing crushing Burning or
Heavy weight Suffocating
Aching
Location
Retrosternal
Across the
chest
In the left arm
Others
Radiation
Left arm
Left shoulder
throat
others
Other Criteria of ischaemic pain
symptomcriteria
Ischaemic sydrome
Duration
Severity
Courseshort ; few min.
few -30 min
>30 min
mild
moderate
Severe
Episodic
Fiactauting
Continous
Ch Stable Angina
Unstable Angina
Acute Myo. Inf.
CSA
UA
AMI
CSA
UA
AMI
Associated symptoms
NO sym.
MildMODERATE
SEVERE
Nausea / vomiting
CSA or UA
AMI
AMI
AMI
Sweating
CSA
??
UA or AMI
UA or AMI
Or Cadiogenic shock
Cold periphery
CSA
??
UA
AMI
Or Cardiogenic Shock
Case no. 1
A 50 yrs old hypertensive and diabetic teacher complained of constricting retrosternal chest pain for three months. The pain occur while walking across the bridge in the morning against the wind and is relieved by rest. He denies SOB, Palpitation, or Syncope.
He has no similar illness before His father had died suddenly at the age of 60 yrs.
His examination is unremarkable
His ECG is normal. His lipids are elevated
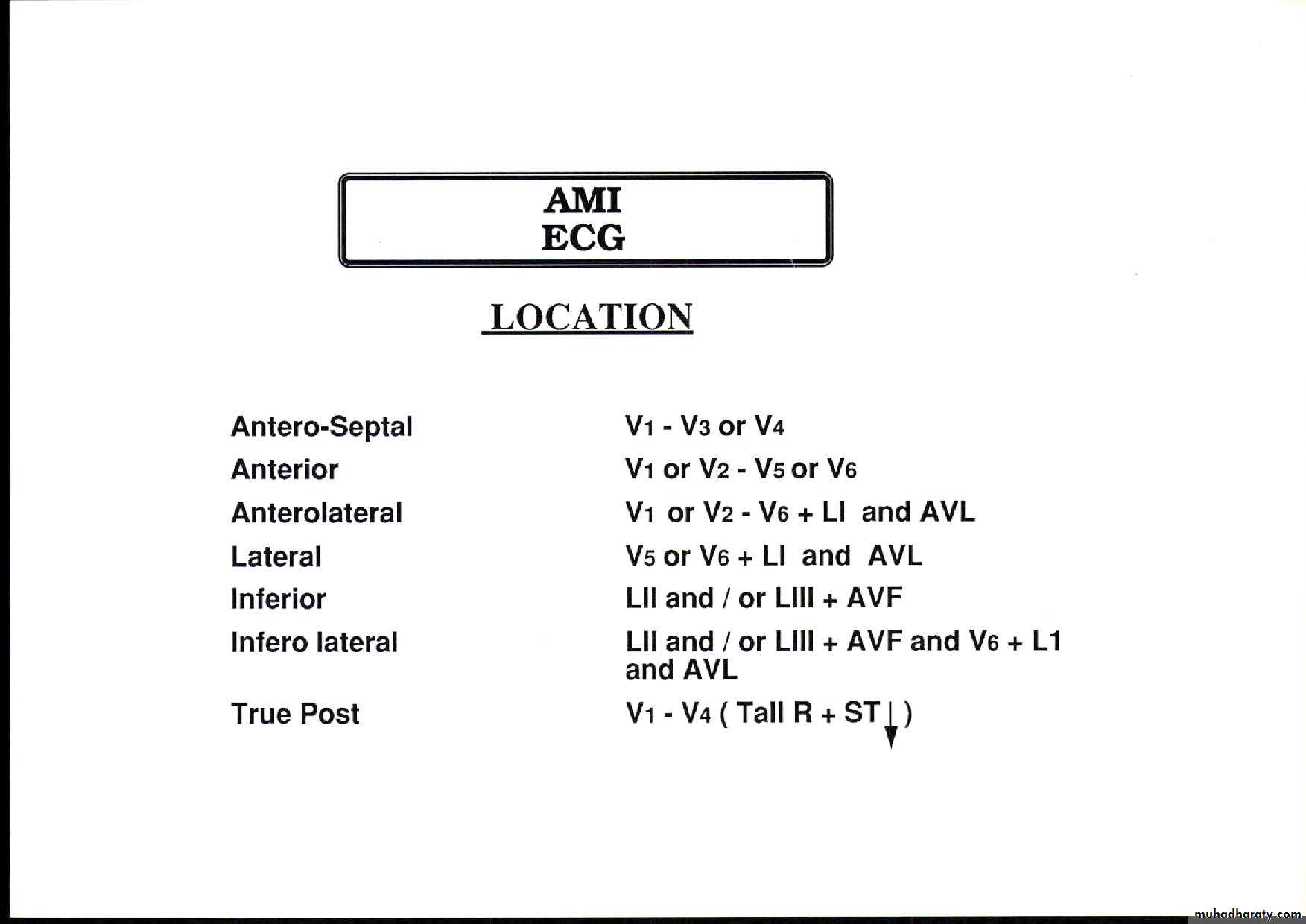
InvestigationsECG
Usually normal unless done during pain wherehorizontal or down slopping ST segment depression T wave inversion on resting ECG
2- Stress Test
Ischaemia is revealed by stressing myocardium through inducing tachycardia . It is used to:-
a- Reveal ischaemia in atypical chest pain
b- Asses the extent of CAD
c- Identify high risk ISCHAEMIC pts pts
d- can reveal the Ischaemic cause of L.V. Dysfunction, Heart Failure arrhythmia, or syncope
Types of Stress test
Type depends on the way of stressing to induce Tachycardia and how to demonstrate IschaemiaTwo ways of inducing tachycardia
a- Walking on treadmill or
b- Dobutamine infusion
Three ways of of demonstrating ischaemia
a- ST depression on ECG
b- filling defect on nuclear test
c- hypokinesia on ECHO
.
Types of Stress Tests
-1 1-
1- Exercise test ; Exercise ECG test :-
Exercise induces tachycardia and if Ischaemia occur it manifests as ST- Depression or hypotension .
IF pt is unable to Exercise use dobutamine or e pacing
2- Dobutamine Stress Thallium test ( Myocardial perfusion scan) ;- used to demonstrate ischaemia if
a- Exercise ECG is equivocal
b- The baseline ECG shows LBBB
c- Pt. is unable exercise
Radioactive Thallium is taken by viable perfused myocardium. Transient Ischaemia causes transient filling defect while a scar causes a permanent one
3- Stress Echo:- induced Ischaemia causes transient hypokinesia while scar causes permanent akinesia
Investigations of CSA:- CT angiography and calcium score
Used to exclude ischaemia rather diagnosing it
Hence more useful for atypical chest pain and no risk factors where the test is likely to be negative and calcium score is low
New version with thinner cuts may increase the accuracy and may enable a positive diagnosis
Coronary Angiography
Gold standard to diagnose I.H.D. until nowDemonstrates the anatomy of the artery. By showing
1- severity of stenosis and type of the lesion
a- non-significant stenosis (<70%)
b- Mod or severe (Critical) lesion ( >70% )
2- Extent of the disease:-
single, two ,three vessel disease, Left main
stem disease (> 50%)
3- L.V angiography if done will assess L.V. function
4- If suitable intervention can be done
Indicated for the diagnosis of atypical chest pain
and before revascularization
Diagnosis
1-Typical history is diagnostic.
In young pts Risk factors are essentials for DX
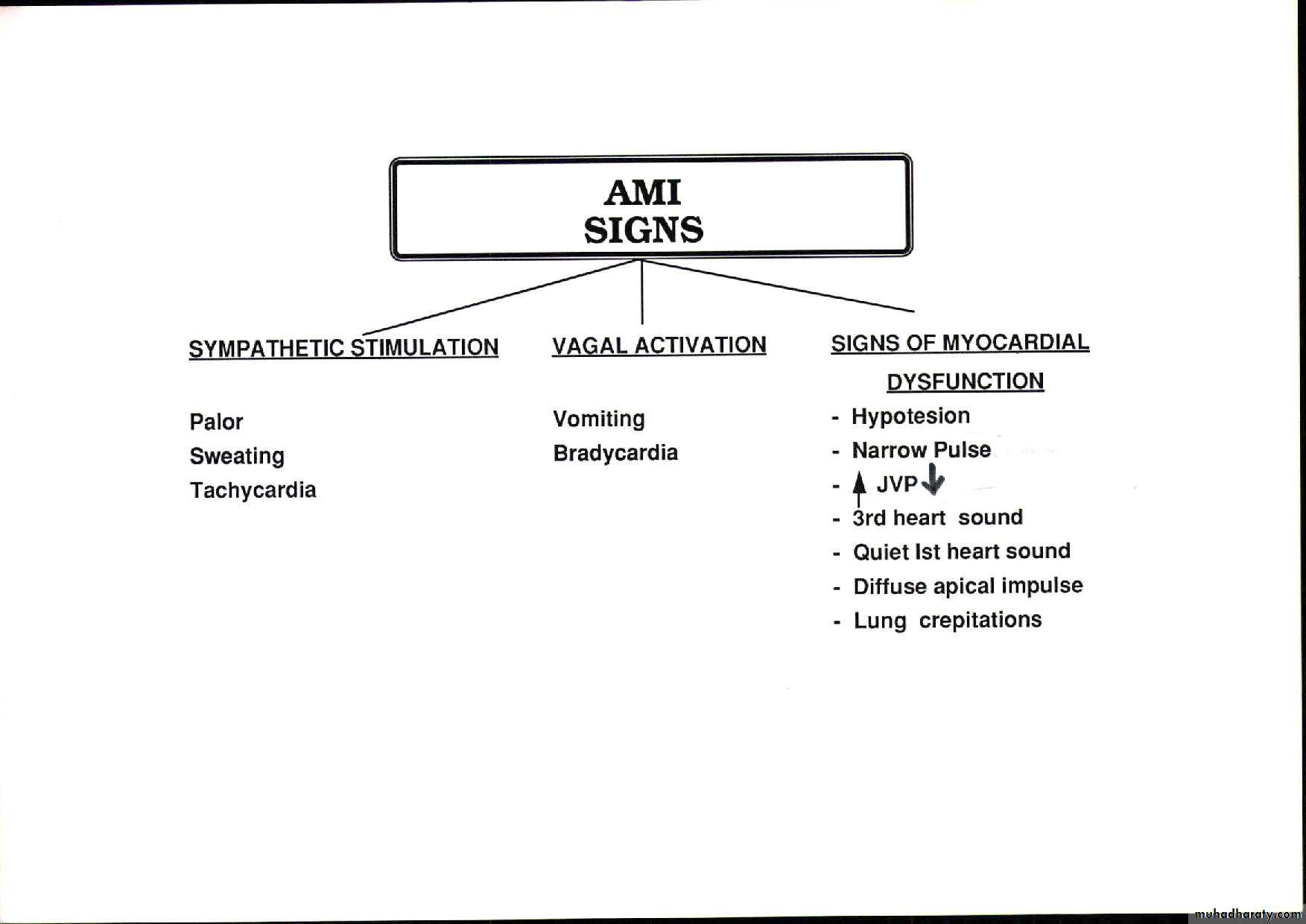
2-Examination
is usually normal
Some pts may have signs related to :-
A- Risk factors e.g. nicotine stain in smokers, xanthomara in hyperlipdaemia, and Retinopathy in D.M and in HTN
B-Peripheral Vascular Dis. :- absent pulses, carotid bruits. Also abd. Bruit in Renal artery stenosis
C- Other causes of increased demand such as
Aortic Stenosis or HOCM
or reduced supply e.g. ; Anaemia
Differential diagnosis of Chest Pain
Ischaemic pain but without atheromatous coronary stenosis ; e g:-1- Microvascular angina
2– CA artery spasm
Non-ischaemic Chest pain; Atypical chest pain
Frequent causes Rare Causes
1- Musculoskeletal pain 1- Herpes zoster
2- Oesophageal spasm 2- Tietze disease
3 – Mitral valve prolapse
4- Pleuretic chest pain
5- pericarditis chest pain
Ischaemic pains without atheromatous CA stenosis
1--Micro vascular angina ( Cardiac syndrome X)
Due to defective O2 supply at the microcirculation ; No epicardial coronary stenosis
more common in women.
Pain usually occurs at night
The patient has evidence of Ischaemia on investigation such as ST depression during pain or on Exercise test
But has normal coronary angiogram.
2- CA spasm
Causes transient Ischaemia which can be transmural hence the ECG reflect that ;Transient ST-elevation
usually more common in women. May occur on the top of atheromatous epicardial CA stenosis
Atypical chest pain
Not typical for Ischaemia ; Usually has some characters for ischaemia such location and some other criteria but lacks that of duration and its relation to exertion1- Musculoskeletal pain;-
Far more common than anginal pain usually nagging more in the L. arm and related to moving arm or turning over. Numbness is common as well as neck pain.
Longer duration ie hours or dayes
Atypical chest pain
2- A-Oesophagyeal spasm:-Ultra short ; lasts for seconds , pricking ,sharp rather than compressive in nature. It is usually associated with dyspepsia and emotional stress but not related to exersion
B-Oesophageal reflux pain causing oesophagitis which is dull pain ,felt at the xiphi sternum ,above , or below it.
Dyspepsia is common and worse in when pt. lie dow. There might be a sharp element i due spasms
ATYPICAL CHEST PAIN
3- Mitral valve prolapse;-
Commoner in young and thin girlsPricking or soffocating feeling with SOB
Unrelated to exrtion associated with palpitations and numbness of left arm Has no risk factors for IHD
Migrain or Irritable bowel syndrome are common
Examination, ECG and CXR are usually normal .
Rarely M.V prolapse is significant leading to Mitral regurgitation with Systolic click and late or pan-systolic murmur. This leads to L.V dilatation which if severe
cause SOB and EVEN LV failure
Atypical Chest Pain
3- Mitral Valve Prolapse;-Commoner in young and thin girls
Pricking or suffocating feeling with SOB
Unrelated to exertion associated with palpitations and numbness of left arm Has no risk factors for IHD
4- Migraine or Irritable bowel syndrome are common
Examination, ECG and CXR are usually normal .
Rarely M.V Prolapse is significant leading to Mitral regurgitation with Systolic click and late or pan-systolic murmur. This leads to L.V dilatation which if severe cause SOB and even LV failure
Atypical CHEST PAIN
4-- Pleuretic pain : It is due to pleurisy
Pain is sharp
More lateral and
Related to breathing and coughing.
5- Acute Pericarditis Usually due to viral infection
Pain usually dull or sharp
Worse on lying and relieved by sitting up
Pericardial rub is the diagnostic
Rare causes of Chest pain
6-Costo-Chondritis (Tietze disease)Dull or sharpe pain at those joints.
Tenderness on pressing the joint
7- Herpes Zoster of the left thoracic nerve
Severe burning pain like fire along the intercostal space
Rash with the vesicles will be diagnostic.
LATER This might cause Post herpetic neuralgia
Management of chronic stable angina
It involves1- Life style changes
2- Control of symptoms
3- Control of Risk Factors
4- Assessment of severity and Extent CAD
5-Identify high risk pts who may need revascularization
Life style changes
Take Exercises
Aim at ideal weight
Avoid Smoking
Avoid strenuous or competitive tasks
GTN prior to angina-precipitating exertion
Control of symptoms and Lipids Quadruple therapy
1- Nitrates2- Betablockers
3-Antilipids
4-Antiplateles
Plus
Ca antagonists
K Channel activators
I channel antagonists
Quadruple Therapy
1- Nitrates reduce demand and increase supplyGTN 0. 5 mg tab S.L. on need up to 12 tab.s daily
Isosrbide Dinitrate 10-20 mg 8 hrly
Long acting ; Mononitrates 2o-60 mg 12hrly
Nitratess free zone to reduce tolerance.
headackes needs analgesics initially
2- Betablockers Cornerstone of RX
Reduce Demands; reduce HR, BP, Contractility
Be carful in Asthma by monitoring PFR
Be careful in L.V failure start small dose
Quadruple therapy 3-- Anti lipids
A -Cholesterol Lowering Agents
Statins Act by blocking HMG CoA Reductaze in the liver hence effectively reduce LDL
Start Statin therapy ((start with Atorvastatin 20 m daily) irrespective of serum level to all pts
The new guideline use high intensity Statin therapy to cut LDL to < 50% of its baseline if it was is higher than 190mg /dl or < 30% if it was 70-190 mg/dl
Ezetimibe 10 mg BID if intolerant to statin
Quadruple therapy Antilipids and anti-platelets
Triglycerides (TG) lowering agents;Fibrates reduce synthesis and enhance catabolism 1-Gimfirozil 600mg BID is used
2-Fish oil 6.0 grams daily if needed
Side effects of Statin and Fibrates include Myopathy and arthropathy
4- Antiplatelets
1- Aspirin tab. 100m daily is effective.
2- Clopidogrel 75 mg /d is an alternative if pt. is Aspirin intolerant
OTHER Anti anginal therapy
A- Calcium antagonists Inhibits Ca influx leading to reduced BP. and Contractility. lowers O2 Demand1- Nifedipine 10-20mg TID it induces
tachycardia hence Betablocker is necesary
2- Diltaizem 60 mg TID if betablocker is not used
B- K channel Activator arterio-venous dilator such as Nicorandil 10-20 mg TID.
C- Ion channel antagonist. Inhibits the Sinus Node leading to Bradycardia; without affecting the L.V. Function. Itlowers O2 Demand
IVABRADINE 10- 30 mg BID is the only one
ACE or ARB for L.V. Dysfunction
Angiotensin Converting Enzyme (ACE) Inhibitor
OR Angiotensin Receptor blocker (ARB) in pts with L.V dysfunction
An important addition to this Quadruple therapy is An ACE inhibitor such Captopril is necessary.
Or an ARB such as Valsartan 80 mg / d
is a good alternative if cough ( a side effect)
is distressing Unfortunately both are contraindicated during pregnancy
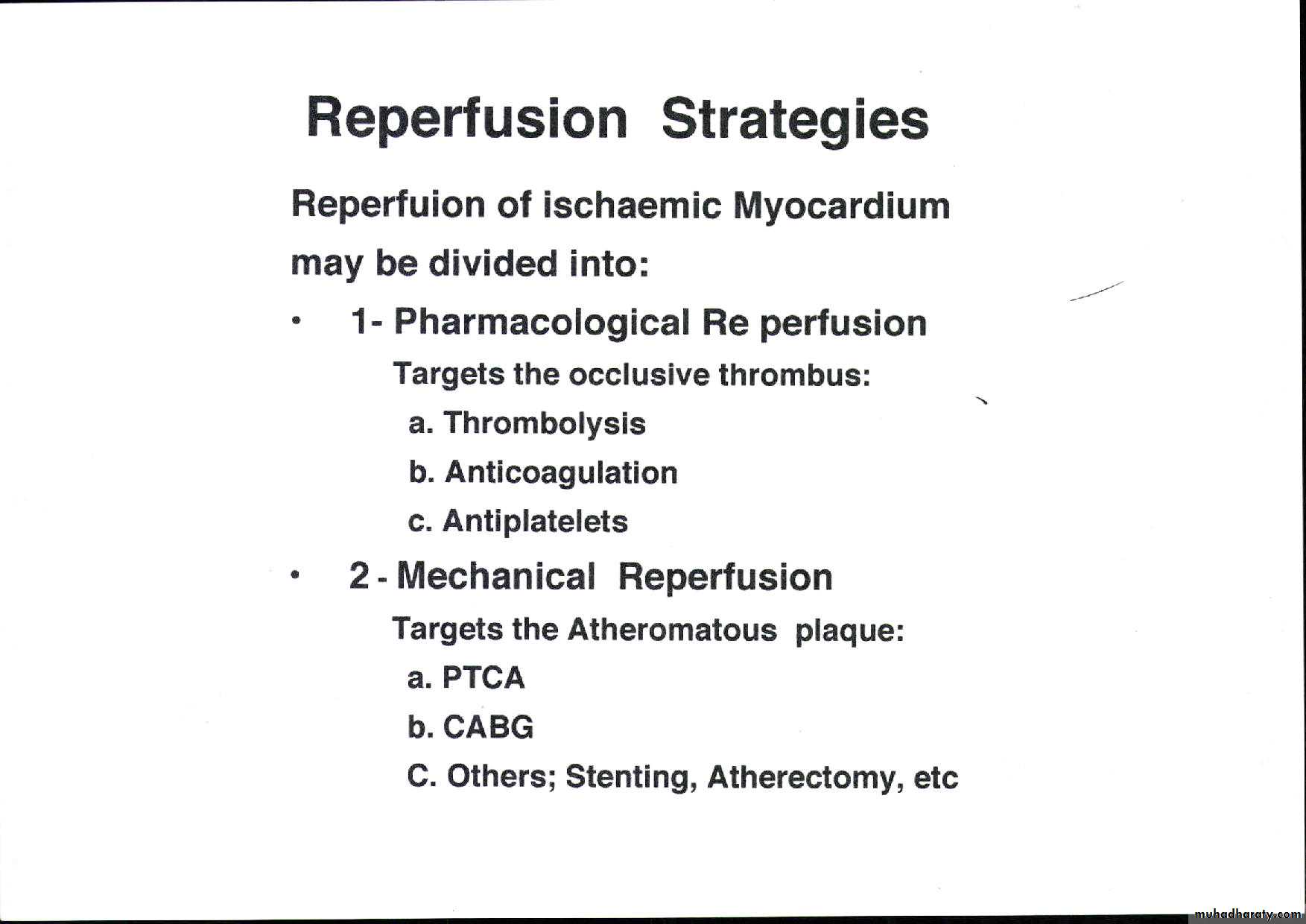
RevascularizationPercutanous C. Intervention (PCI) or C.A Bypass Grafting (CABG)
PCI which include Balloon Angioplasty + - Stenting Is indicated in discrete single vessel or two vessel lesions except that of the Proximal Left Anterior Descending artery LADCABG is for Left Main Stem lesion , Three Vessel Disease, and proximal LAD 1-2 vessels Disease
Especially diabetic pts and also those with LV dysfunction
Benefits and drawbacks of PCI
PCI benefitsImproves symptoms only (no evidence it improve survival ) and used for stenosis of native CA or graft .
PCI drawbacks ( related to lesion morphology, operator skills, and co morbidity ( page 588 Davidson)
1- Dissection and or Thrombosis ( 2-5%) Usually corrected by stenting
2- Restenosis occur in up to 33% in Angioplasty and reduced by Stenting with Bare Metal Stent ( BMS ) and reduced further by using Drug Eluting Stents (DES). Restenosis still occur in 10%. Dual antiplatelets needed
3- Late stent thrombosis occur in 0.6 % every yr.
CABG benefits and drawbacks
CABG benefits
1- Relives symptoms in 90% 1yr and 60% in 5 yrs
2- improve survival.
More benefits in total arterial Bypass and Off-pump
CABG drawbacks
1- Op. Mortality is 1.5% and higher in the elderly
and those with co morbidity.
2- Repeat Revascularization 2% in 2yrs
3- Stroke in 1-5%
3- Cognitive impairment (30-80%) mostly resolve at 6
months. Reports of a long term one (30% at 5 yrs)
Primary PreventionPopulation strategy and Targeted Strategy
A- Population strategy :-Life style changes:-1- Exercise. 2- Diet to maitain ideal weight, 3- no smoking
Regular Exercise Brisk such as Brisk walking or
Cycling or Swimming for 20 min. 3 times/week
Healthy Diet Less fat ;- down to 10% of calories
Rich in fish vegetables and fruits
B- Targeted Strategy
Calculate the composite Risk Score to identify pts with risk factors ( high risk) and advise-treat them
Secondary Prevention
Life style of Primary prevention
AspirinStatin irrespective serum cholestrol and High intensity statin for high cholestrol
ACE inhibiyor even in normal L,V. Function
Control BP. Below 140/90
Good control of D.M
The teacher’s story
He was put on ISMN 20 mg/d, Atenolol 50 mg /d Atorvastatin 20 mg /d, and Aspirin 100mg /dHe stopped smoking He became asymptomatic
and lost to follow up
Two years later his pains returned but became more frequent and occurring even at rest.
Then he came to casualty when he developed much longer pain for 20 min with sweating but with no nausea or vomiting. He confessed that he stopped his Statins tab and he was smoking
Acute Coronary syndrome
ACS encompasses wide spectrum of Acute Ischaemic syndromes starting with Unstable Angina through Acute Non ST-elevation MI to Acute ST-Elevation MI.It extends from Recurrent Angina at one end , to include sudden death due to extensive MI and Cardiogenic shock.
If the chest pain and the RFs are classical ACS and its clinical subtypes can confidently diagnosed by history only. Investigations will assess the severity and also confirm the diagnosis of Non classical cases
The chest pain in ACS is similar to that of CSA, It can be mild in UA and severe, excruciating in AM
UA Clinical Classification
UA is divided into four categories depending on the clinical Characteristics of the pain of
1- New onset Angina
2-Rapidly deteriorating Angina
3- Angina at rest
4- Long episode of angina Up to 30 min but without cardiac damage.
The pain can be recurrent or variable in intensity (wax and wane) and dictated by the coronary flow which is determined by stenosis severity, the underlying thrombus , and the possible spasm
UA other symptoms
SOB depends on the amount of the LV dysfunction which becomes worse with pain reaching the feelong of suffocation. If the amount of Ischaemia is large it may lead to transient acute LV failure.Palpitation and syncope can occur and are more frequent in extensive underlying disease.
UA is usually not associated by Enzyme leak
UA investigations
ECG and EchoLike CSA both ECG and Echo can show evidence of Ischaemia during pain.
Cardiac enzymes as markers of myocardial damage are normal.
Troponins
Troponins are usually negative except in small minority of pts and is regarded as high risk group
Diagnosis
1-Classical pains in a susceptible pt is diagnostic2-Investigations may confirm or exclude the diagnosis
3-if the case is doubtful the pt must be labeled as suspected UA and managed like a certain UA case until the diagnosis is clear.
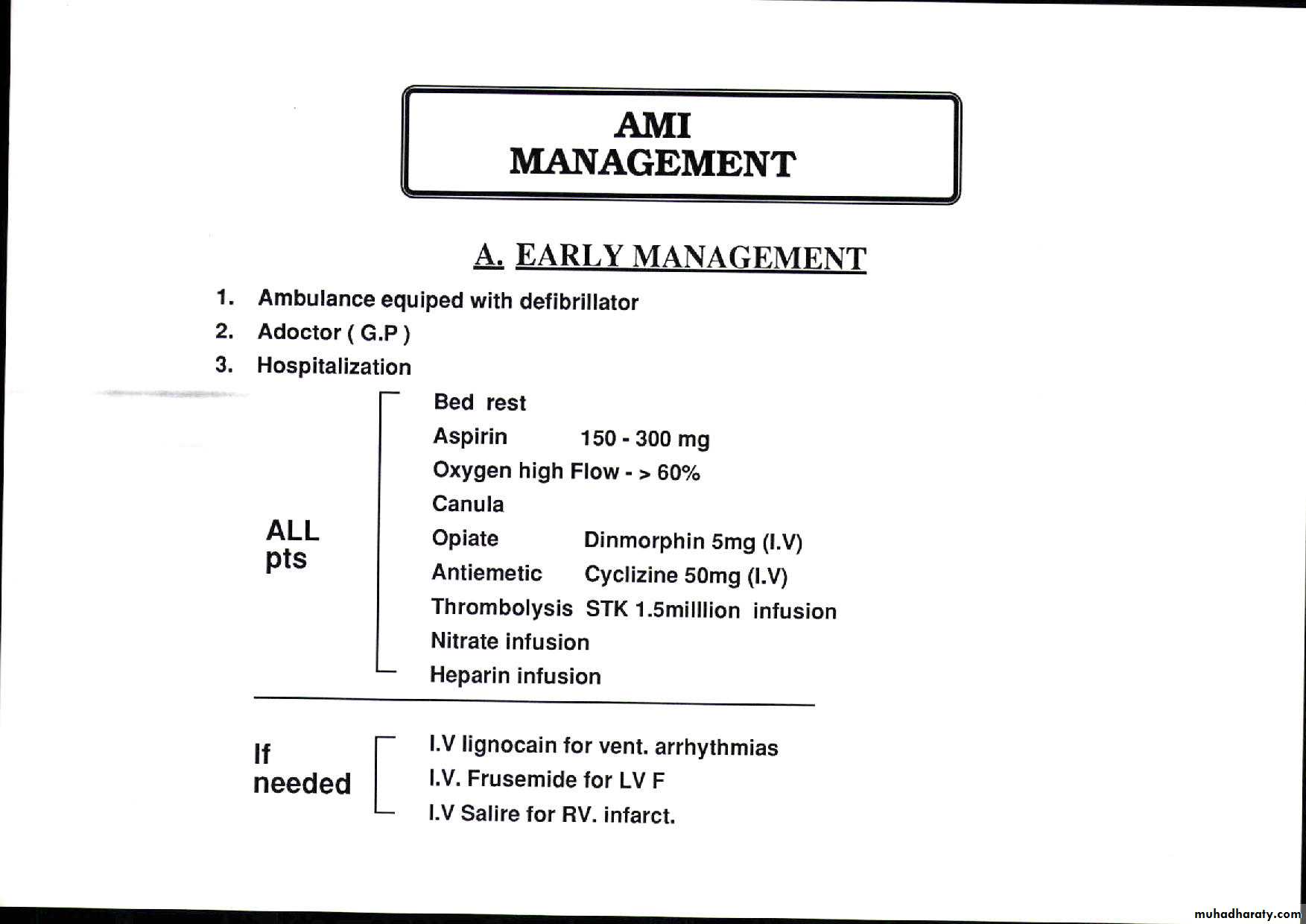
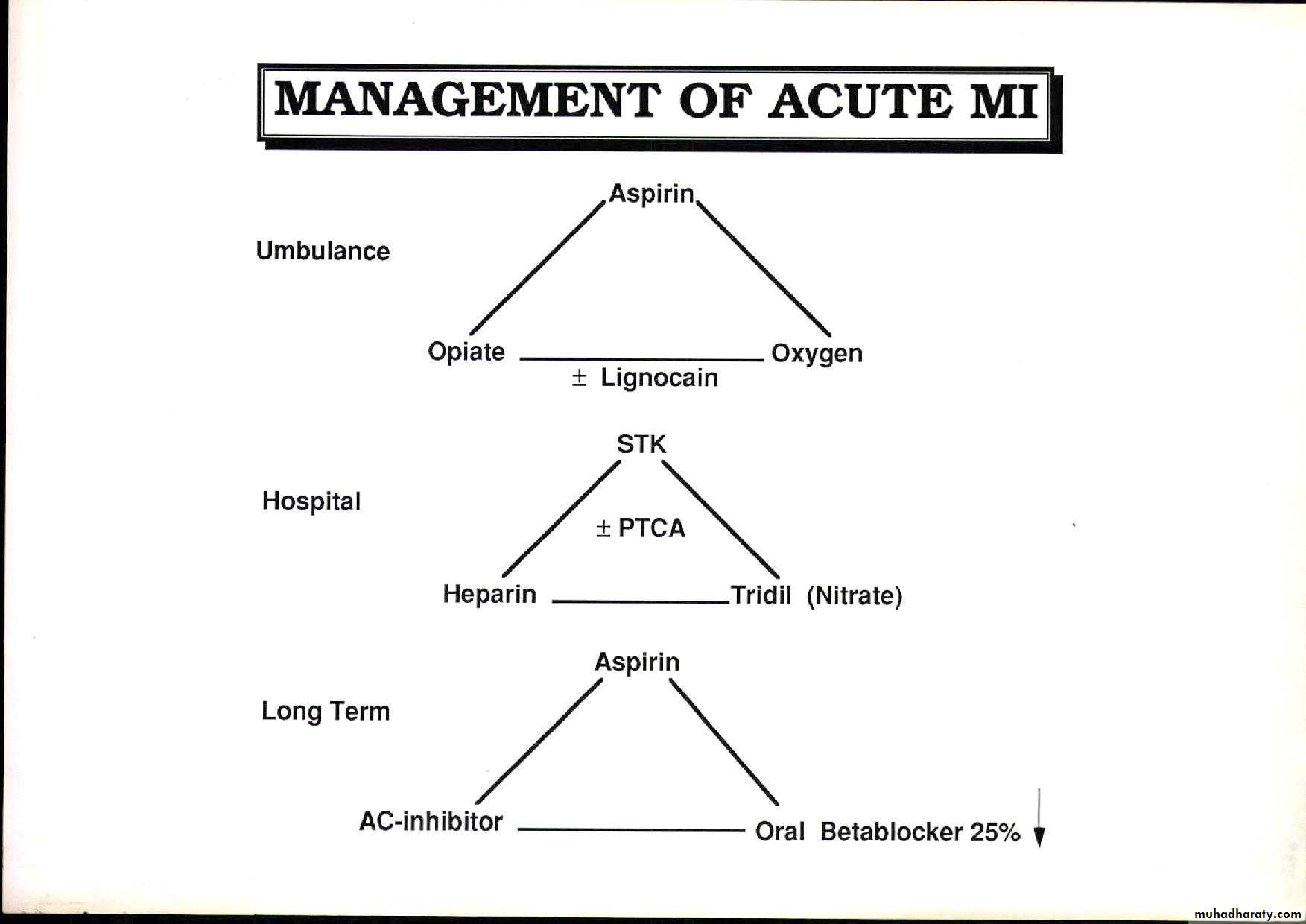
Management
1- Hospital Admission. Obviously A CCU is better
2-Close clinical evaluation + cardiac monitoring
3- serial ECG ,Troponins. and cardiac enzymes.
4--Calculating Grace Risk score
It is calculated to identify high risk pts (; high risk of death or MI) . It is based of recording admission clinical findings :- Age HR, BP, RFT, CCF, STE, C arrest , Troponins. Medium score (1-9), and High score ( >9 ) scors pts need invasive approach ie Coronary angiography and Revascularization Low Risk pts ( score <1 ) go for Conservative Rx
UA management
5- Oxygen 60%6- Aspirin 100 mg or Clopidogril 75 mg
7- Nitroglycerine infusion 0.6-1.2 mg/hr or ISDN 1-2 mg/hr is given it can relive pain if maximal dose fail to relieve pain then Narcotic analgesics may be used
8-The Pentasaccharide Fondaparinux 2.5 mg s.c or The LMW heparin Enoxaparin 1.0 mg/kg 12 hrly i
9- I.V. Betablocker Atenolol 5-10mg or Metoprolol 5-15m every 5.0 min followed by oral Atenolol 50mg daily or Metoprolol 50mg twice aday
Invasive therapy for UA
Give High dose Clopidojril 600mgGP 11b/111a Receptors Blockers such Tirofiban or Abciximab a powerful antithrombotic agent will be infused before and during the Intervention .
It is used for high risk pts such as pts with
1- recurrent ischaemia
2- High Troponins
3- Diabetics.
Intervention is aimed at the culprit lesion
Teacher’s chest pains
He was treated as a case of Unstable Angina He was labeled as high risk pt. And scheduled for Invasive strategy. His pains settled . He felt better. He refused catheterization and went home . Few weeks later he presented with severe retrosternal pain increasing in severity over 3 hrs the pain was constrictive associated with profuse sweating ,nausea and vomiting . His ECG showed ST depression on t V2-5 His BIOMARKERS were Up. He was labeled as NSEMI
He was admitted to the CCU
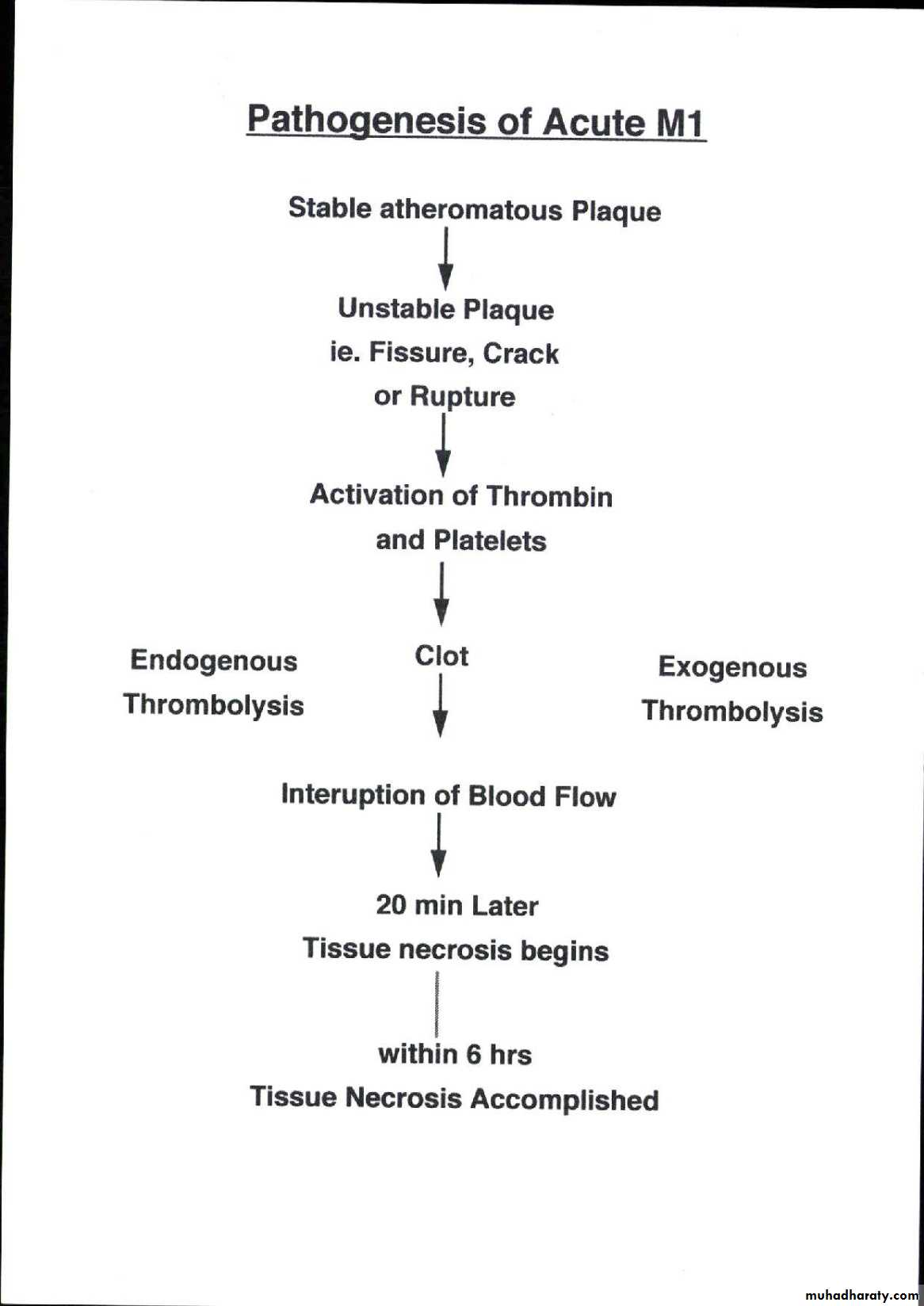
Outcome of Unstable Plaque
1- Fissures, cracks, or ruptures leading to the formation of a thrombus2- Outcome depend on severity of occlusion
a- Partial occlusion …. …….Unsatble Angina
b- Total occlusion …Acute Myocardial Infarction (MI)
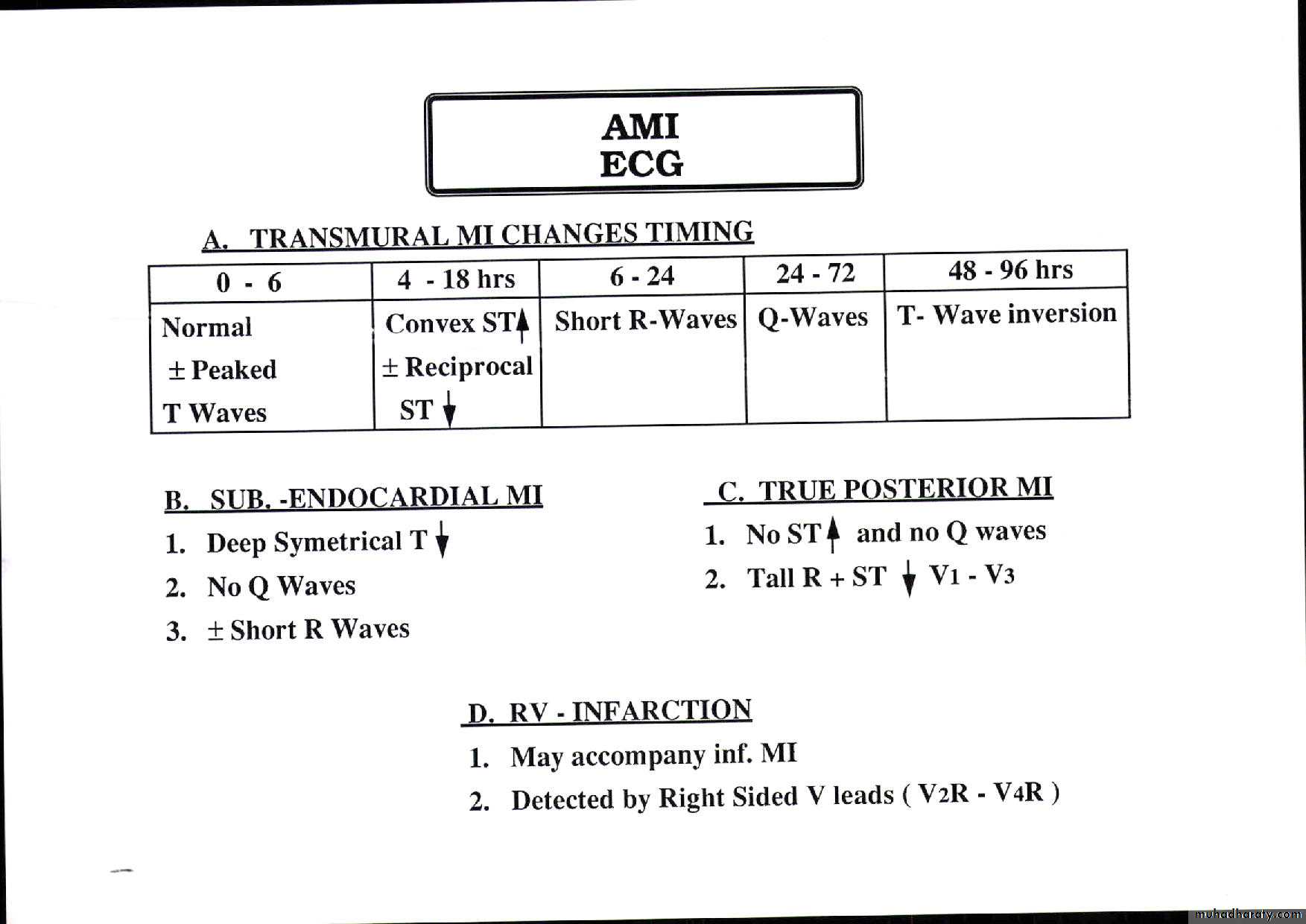
ACUTE MI are two types
Full thickness necrosis …. Acute STE MI
Partial thickness necrosis… Acute NSTEMI
Manifestation of Ischaemic heart disease
Manifetaed as1- Ch. Stable Angina
2- Acute Coronary Syndrome
A– Unsable Angina
B- Acute M MI Either STEMI or NSTEMI
C- Ischaemic Cardiomyopathy
D- Arrghhythmia
E-Sudde Death
Determinant ot outcome of plaque
Severity of Stenosis
A- Mild asymptomatic unless it is unstable
B-Moderate or severe impairs blood flow if 70% + ; significant lesion leading to ischaemia
C- Total occlusion stable plaque that has increased gradually leading to formation of collaterals
Pathophysiology
Reduction of blood flow that lead to shortage of O2 recieved by myocardiumUsually due to Athermatous plaque that occupies 70%% of one of the three epicardial arteries ( or 50% in the left main coronary artery). Since O2 requirement increases with tachycardia that accompanies exercise the ischaemia is directly related to exertion
Determinant of O2 requirement
In human Physiology O2 requirement of the myocardium depends on1-Supply ; amount O2 delivered to myocardium
2- Demand; amount O2 needed myocardium
Supply is mostly determined by stenosis
Demand is mostly determined by Heart Rate and myocadial thickness ; LVH
Cont’d pathophysiology
Angina either wholeley or partially caused by increase demand due to Tachyarrhythmia (Sinus Tachycardia AF , SVT ) or due to Hypertrophy (HTN, HOCM, or Aortic stenosis)Also it may be due to reduced carrying capacity of the blood leading to shortage of O2 supply such as Anaemia, or CO poisoning
Angina pectoris ;
1- The most common cause of Reduced SUPPLY is atheromatous Plaque
2- The most common cause of increased DEMAND is Tachycardia
3- The most frequent scenario is
Exercise induced tachycardia of a patient with a 70% plaque stenosis .
4- This transient ischaemia makes the syndrome of
Chronic stable angina
Symptoms of IHD
FOUR Cardinal Symptoms1- Chest pain
2- SOB Shortness Of Breath
or breathlessness
or Dyspnoea
3- Palpitations
4- Syncope
CARDINAL cardiac SYMPTOMS
• 1-Chest pain• 2-SOB on severe exersion in CSA
• mild exersion………….. in LVF
• at rest ; Orthopnea …… in LVF
• during sleep ; PND ……. in LVF
• 3-Palpitation :- regular . Irregular ..in AF
• 4-Syncope:- on severe exersion especially with aortic stenosis