CONGENITAL ADRENAL HYPERPLESIA(CAH)
By the end of these lectures, the student will be able to:Define (CAH).
State the etiology and list the types of (CAH).
Describe the clinical presentation of (CAH).
List the diagnostic tests of (CAH).
Identify the treatment options of (CAH).
Define pheochromocytoma and outline its etiology.
Describe the clinical features of pheochromocytoma.
List the diagnostic tests and state the treatment plan of pheochromocytomas.
Objectives
(CAH) is a group of inherited autosomal-recessive disorders in which a genetic defect results in the deficiency of an enzyme essential for synthesis of cortisol and, at times, aldosterone.
Most common and clinically important Enzymes deficiency are:
21-Hydroxylase
11-β-Hydroxylase
17-α-Hydroxylase
Reduction in end-products, accumulation of hormone precursors, impaired negative feedback and increased ACTH production and adrenal hyperplasia.
The C/F reflects the effects of:
1- Inadequate production of cortisol & aldosterone
2- Increased production of androgens & steroid metabolites.
Most common type, accounts for 90- 95% of cases.
Incidence is 1:5000 to 1:15000 live birth.Gene is located on the short arm of chromosome 6 near the C4 locus in close association with HLA genes.
21-Hydroxylase Deficiency
21-Hydroxylase Deficiency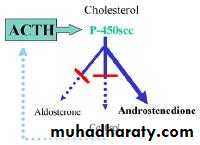
It is characterized by reduced production of cortisol and aldosterone and increased production of adrenal androgen.
Diagnostic markers: serum (and urine)
17-OH-progesterone, pregnanetriolone, and
17-hydroxypregnanolone.
2 forms, classic early virilization type with or without salt-losing crisis and non-classic type with late-onset virilization.
In one third of cases of 21-OH deficiency, pat have severe salt wasting from reduced aldosterone. If not diagnosed at birth, the neonate will develop a life-threatening hyponatremia, hyperkalemia, and hypovolemia by day 10-14 of life (adrenal crisis).
Mass neonatal screening using filter paper blood sample from the heal for 17-OH-Progesterone is used in the USA.
The excess androgens causes virilization of girls & ambiguous genitalia & dark scrotum in boys.
The other two third of cases have adequate mineralocorticoid and will present later with premature adrenarche (pubic hair development), accelerated growth velocity, advanced bone age, acne, and hirsutism.
Gene is located on the long arm of chromosome 8.
It is characterized by:Glucocorticoid deficiency, mineralocorticoid excess, adrenal androgen excess
low plasma renin activity
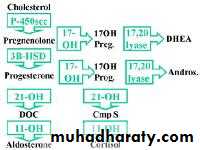
elevation of serum 11-Deoxycortisol and 11-deoxycorticosterone (DOC) which exerts mineralocorticoid activity.
- salt retention, hypertension & hypokalemic alkalosis.
11-b-Hydroxylase Deficiency
Genetic defect is on chromosome 10.Presents with similar features of those of 11-Hydroxylase deficiency except that androgens are low, so no virilization in girls & genitalia is ambiguous in boys.
17-a-Hydroxylase deficiency
17α-hydroxylase is necessary to convert pregnenolone to 17-hydroxypregnenolone (17-OH Preg) and progesterone to 17-hydroxyprogesterone (17-OH Prog). Thus, absence of this enzyme impairs all sex steroid and cortisol production. This results in increased secretion of pregnenolone, progesterone, (DOC), and corticosterone.
17-a-Hydroxylase deficiency
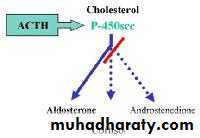
Increased linear growth with advanced bone age and eventual short stature
Pseudohermaphorditism in girls due to androgen virilizing effectSexual precocity in boys with small infantile testes.
DIAGNOSIS
Adrenal crisis with salt-loss or Hypertension & hypokalemic alkalosis.
Low cortisol with high androgens, ACTH and steroid precursors e.g. 17-OH-Progest. or 11-Deoxycortisol.Diagnosis is confirmed by measurement of ACTH, Cortisol, Aldosterone, 17-OH-progesterone, Testosterone & urinary 17-ketosteroids.
Needs alertness for the possibility in all babies with Diarrhea & Vomiting, hypoglycemia or BP.
In 21-hydroxylase deficiency:
very high serum 17-hydroxyprogesteronevery high urinary pregnanetriol (metabolite of 17-hydroxyprogesterone).
Laboratory Findings
11-b-hydroxylase deficiency is characterized by: -high serum 11- (DCS) and 11-deoxycortisol, elevation of its urinary metabolites (tetrahydrocompound-S).
Both are accompanied by elevated 24-hour urinary 17-ketosteroids.
In salt wasting forms of adrenal hyperplasia:
low serum aldosterone,- hyponatremia, hyperkalemia
- elevated plasma renin activity (hypovolemia)
In (11-b-hydroxylase deficiency and 17-a-hydroxylase deficiency):
HTsuppressed plasma renin activity
hypokalemia.
Treatment is life-long
Treatment goals are:to maintain growth velocity & skeletal maturation.
to normalize electrolytes & hormone levels using the smallest dose of glucocorticoids that will suppress the ACTH to normal. Mineralocorticoid replacement may be needed to sustain normal electrolyte homeostasis.
TREATMENT PRINCIPLES
Steroid replacement
Supportive therapy when neededPlastic surgery for ambiguous genitalia at early age
Genetic counseling
Psychological support
MODES OF TREATMENT
Glucocorticoids Replacement
For children, hydrocortisone 10-15 mg/m2/day divided in 3 oral doses. Dose should doubled during crisis & stressful conditions. The goals of therapy are:
To replace the body's requirement under normal conditions and during stress.
To suppress ACTH secretion.
For adults, predinsolone is used
Long Term Therapy
Mineralocorticoids Treatment
Fludrocortisone acetate 0.05-0.2 mg once daily orally is indicated for patients who have salt-wasting forms of CAH. It will restore the sodium- potassium balance.A New approach therapy is the combined use of 4 drugs:
glucocorticoid (to suppress ACTH and adrenal androgen production),mineralocorticoid (to reduce angiotensin II concentrations),
aromatase inhibitor (to slow skeletal maturation),
flutamide (an androgen blocker to reduce virilization)
New Trends of treatment
Done by chorionic villus sampling at 8-12 wk & amniocentesis at 18-20 wk.
HLA typing in combination with measurement of 17-OH-progesterone & androstenedion in amniotic fluid is used for antenatal diagnosis.Prenatal diagnosis
Pheochromocytoma
Are catecholamine- producing tumors derived from the sympathetic or parasympathetic nervous system.
They may arise sporadically or be inherited as features of MEN type 2.
It is estimated to occur in 2–8 of 1 million persons/ year, and about 0.1% of hypertensive patients harbor a pheochromocytoma.
The mean age at diagnosis is about 40 y.
The "rule of tens" for pheochromocytomas states that about 10% are bilateral, 10% are extraadrenal, and 10% are malignant.
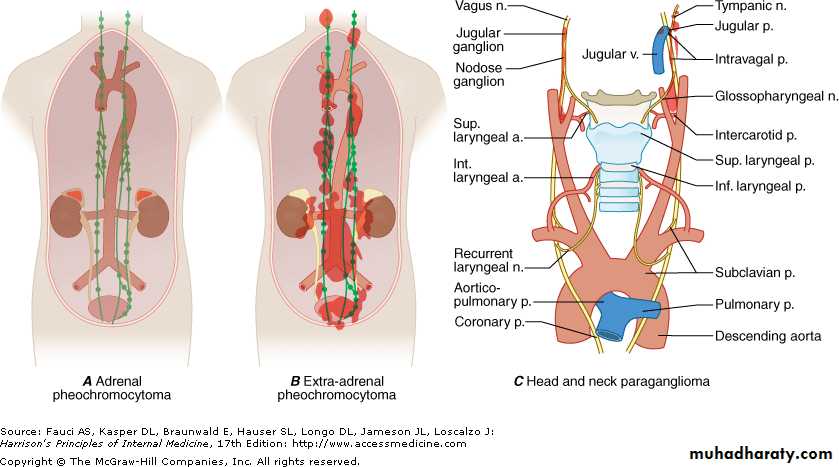
Well-vascularized tumors that arise from cells derived from the sympathetic (e.g., adrenal medulla) or parasympathetic (e.g., carotid body) paraganglia.
They are catecholamine-producing tumors, including those in extra-adrenal retroperitoneal, pelvic, and thoracic sites
Etiology
Episodes of palpitations, headaches, and profuse sweating are typical (triad), in association with HT (sustained or paroxysmal).
It can be asymptomatic for years, and some tumors grow to a considerable size before symptoms.
Other CF associated with pheochromocytoma:
Anxiety and panic attacks, Pallor, Nausea, Abdominal pain, Weakness, Weight loss, Constipation, Orthostatic hypotension, Dilated cardiomyopathy, glucose intolerance.
Clinical Features
The dominant sign is hypertension
Catecholamine crises can lead to HF, pulmonary edema, arrhythmias, and intracranial hemorrhage.The paroxysms last less than an hour and may be precipitated by surgery, positional changes, exercise, pregnancy, and various medications (e.g., tricyclic antidepressants, opiates, metoclopramide).
Biochemical testing and localization of the tumor by imaging.
Elevated plasma and urinary levels of catecholamines and the methylated metabolites, (metanephrines) are the cornerstone for the diagnosis.Urinary tests for (VMA), metanephrines (total or fractionated), and catecholamines are used commonly for initial testing.
The fractionated metanephrines and catecholamines are the most sensitive.
Plasma tests are the most sensitive.
Suppression test using clonidine may be valuable (3 h after oral administration of 300 g of clonidine).
Diagnosis
Abdominal CT or MRI.
MIBG scintigraphy.Somatostatin receptor scintigraphy.
Dopa (dopamine) PET.
(A) Anterior (left) and posterior (right) whole-body images of 51-y-old woman with right adrenal tumor on CT, confirmed as pheochromocytoma at surgery. Gregory A. Wiseman et al. J Nucl Med 2009;50:1448-1454

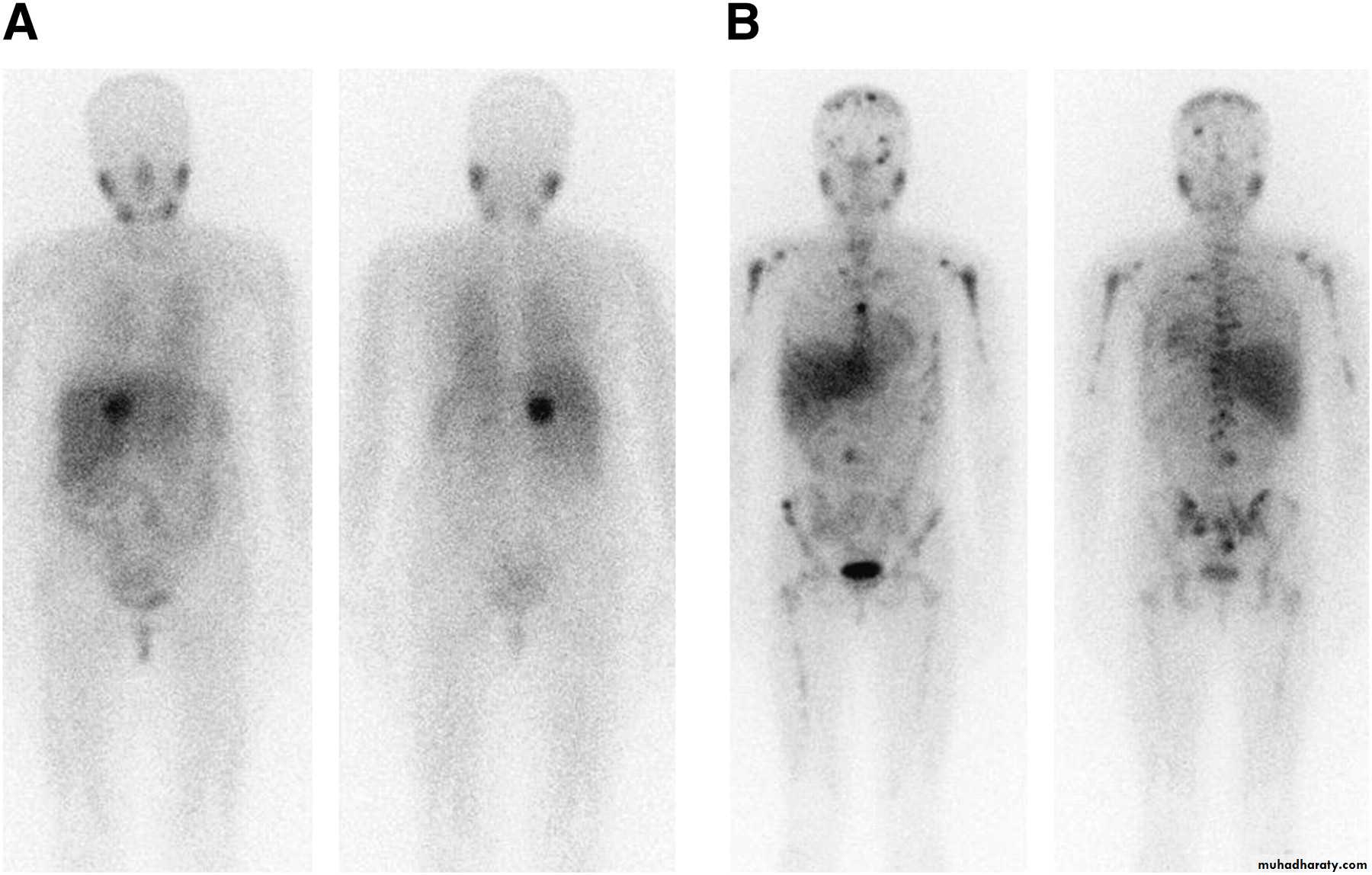
• (c) Copyright 2014 SNMMI; all rights reserved
Complete tumor removal is the goal.Preoperative preparation for 6w is essential before surgery. α-Adrenergic blocker (phenoxybenzamine) should be initiated at relatively low doses (5–10 mg orally 3X per day) and increased every few days up to
20–30 mg 3X/d.
Good hydration is necessary to avoid orthostasis.
Treatment
Intravenous phentolamine can be used to manage paroxysms while awaiting adequate alpha blockade. It is also used during surgeryBefore surgery, BP should be below 160/90 mmHg.
Beta blockers (10 mg propranolol 3-4 times daily) can be added if tachycardia persists.
Nitroprusside infusion is useful for intraoperative hypertensive crises.