Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
Hernia:
is the protrusion of viscus or part of a viscus through an abnormal
opening. The external abdominal hernia is the commonest form. The common
types being inguinal, femoral and umbilical. The most frequent of these inguinal
which occurs in 73% of cases, then comes femoral in 17% of cases, followed by
umbilical which occurs in 8.5%.this leaves 1.5% for the rarer forms.
Etiology in most cases no cause can be elucidated. It is probable than
indirect inguinal hernia occur in a congenital performed sac, the remains of
processus vaginalis.
Sometimes a powerful musculature efforts or strain occasioned by lifting a
heavy weight will cause such a hernia. Any condition which raise the
inraabdominal pressure is liable to be followed by hernia, whooping cough
in childhood
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
Straining at micturation because of urethral obstruction in prostatisim,
straining at defecation due to constipation may precipitate hernia, stretching
of abdominal musculature because of increase in contents as in obesity and
pregnancy can be another factor.
Pathological anatomy: hernia consists of three parts. The sac, the content of
the sac, and the covering. The sac consists of a diverticulum. The sac
consists of a diverticulum of a peritoneum which is divided in to mouth,
neck, body, and fundus.
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
Usually the neck is well defined, but in certain directs inguinal hernia and in
much incisional hernia there is no actual neck. The body varies greatly in
size and not necessarily occupied.
Contents:
it can be
1- Omentum ----- omentocele.
2- Intestine ------- enterocele.
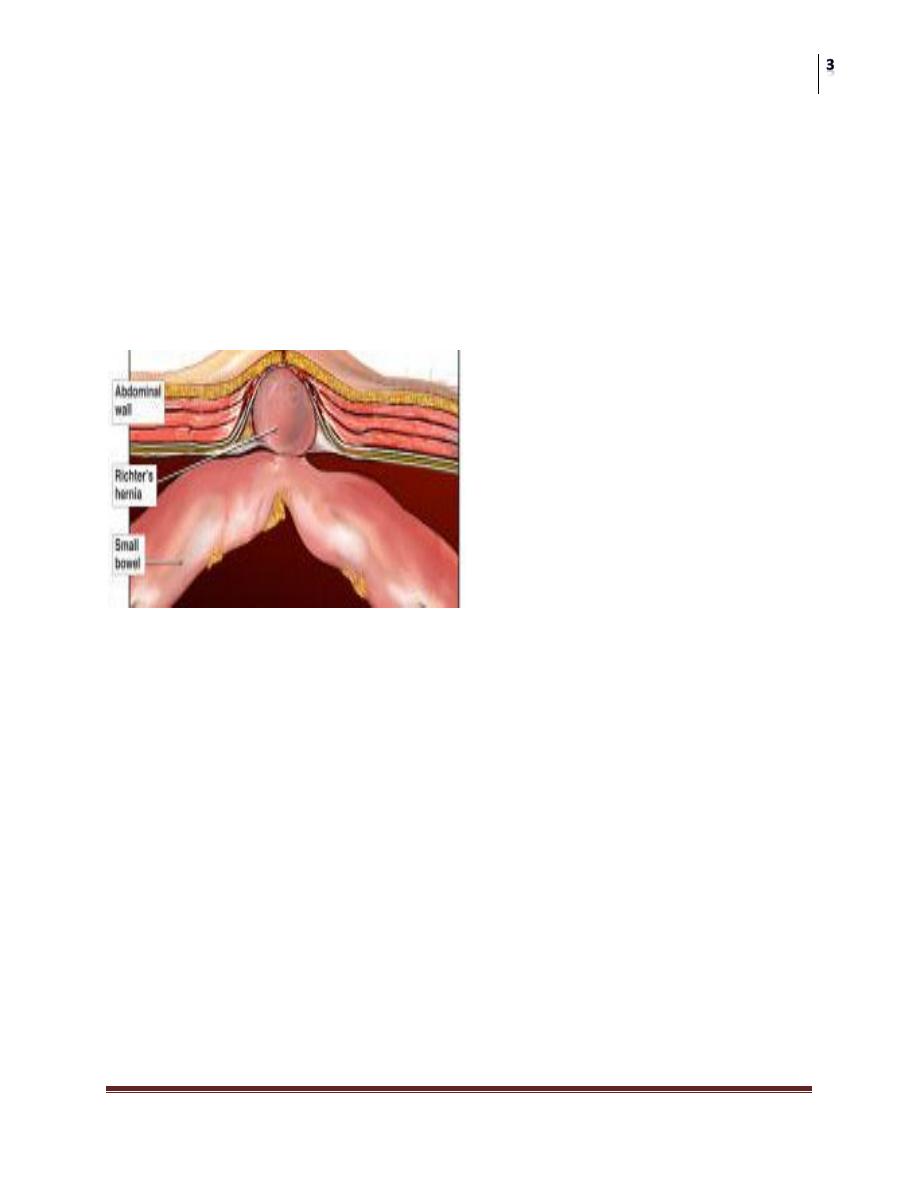
3- A portion of circumference of intestine called Richter's hernia.
4- A portion of bladder or diverticulum of bladder as in direct inguinal hernia,
sliding hernia, femoral hernia.
5- Ovary with or without fallopian tube.
6- Meckel,s diverticulum called Littre,s hernia.
7- Fluid as part of ascites or blood stained fluid in accompanies strangulation.
Coverings:
derived from the layers of the abdominal wall through which the sac
passes.
Classification: irrespective of their site as follow:
1- Reducible. 2- Irreducible. 3- Obstructed. 4- Strangulated. 5- Inflamed.
Reducible hernia
either reduces itself when the patient lies down, or can be
reduced by the patient or by the surgeon. The physical signs of reduction vary
somewhat with the nature of the contents of the sac. Intestine gurgles on reduction,
and the first portion is more difficult tom reduces than the last. Omentum is

Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
doughy and the last portion is more difficult to reduce than the first. A reducible
hernia imparts an expensile impulse on coughing.
Irreducible hernia:
a hernia is said to be irreducible when its contents
cannot be returned to the abdomen, and there is no evidence of other
complications. Usually such a condition is brought about by adhesions between the
sac and its contents or from overcrowding within the sac. Irreducibility without
other symptoms is almost diagnostic of an omentocele. Femoral and umbilical
hernias are most often complicated in this manner. Any degree of irreducibility
predisposes to strangulation.
Obstructed hernia:
an obstructed hernia is an irreducible hernia containing
intestine the lumen of which is obstructed from without or from within, but there is
no interference to the blood supply to the bowel. The symptoms are less severe and
the onset more gradual than is than the case in strangulation. Usually no clear
distinction can be made between obstruction and strangulation in hernias, so the
safe course is to assume that strangulation is imminent and treat the case
accordingly.
Incarcerated hernia:
the term incarceration is often used loosely as an
alternative to obstruction or strangulation. It should be employed only when the
lumen of that portion of the colon occupying a hernial sac is blocked with feces.
Strangulated hernia:
a hernia become strangulated when the blood supply
of its contents is seriously impaired, rendering gangrene imminent. Gangrene may
occur as early as 5-6 hours after the onset of the first symptom of strangulation. A
femoral hernia is more likely to strangulate than inguinal hernia.
Clinical feature of strangulated hernia: pain comes on suddenly and is at
first situated over the. Generalized abdominal pain soon supervenes, it is
paroxysmal in character and it is often located mainly at umbilicus.
Vomiting is forcible and usually oft-repeated. The patient often says that the
hernia has recently become larger.
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
On examination, the hernia is tense, extremely tender, and there is no
extensile impulse on coughing. The patient is seriously ill and the treatment
is vitally urgent. Unless the strangulation is relived the paroxysms of pain
continue until peristaltic contractions cease with the onset off gangrene
when paralytic ileus and endtoxin shock develops. Spontaneous cessation of
pain is therefore of grave significance.
Inguinal hernia:
it can direct or indirect.
Indirect inguinal hernia:
is the most common of all forms of
hernia. It is due to performed sac which is partially or completely patent processus
vaginalis. Normally, shortly before birth, the processus vaginalis becomes
obliterated, at first at the deep inguinal ring, and a little later immediately above
the upper pole of epididymis; the tunnel of peritoneum between these two points
becomes a fibrous cord. In the first decade of life inguinal hernia is more common
on the right side in the male.
This is no doubt associated with later descent of right testis. After the second
decade left inguinal hernia are as frequent as right. The hernia is bilaterally
in nearly 30% of cases.
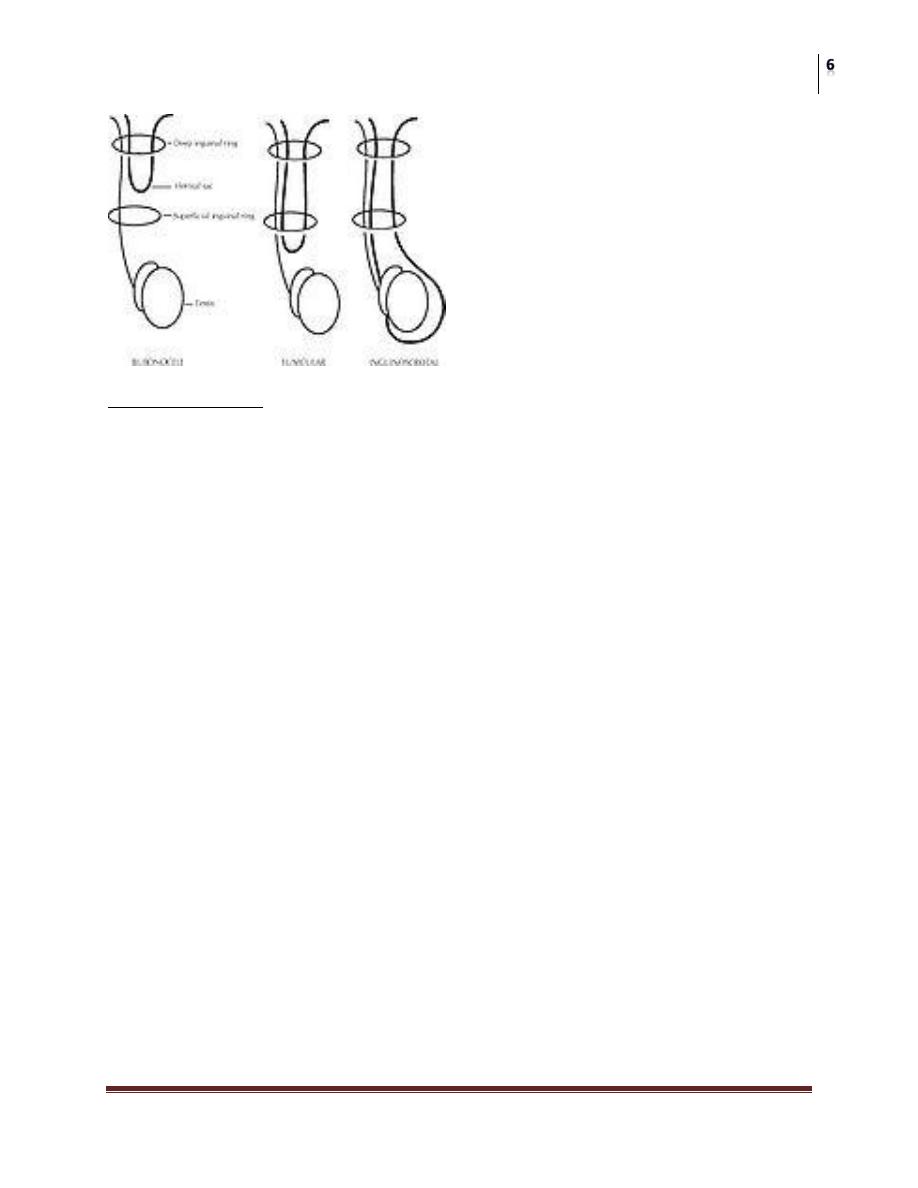
There are three types of oblique inguinal hernia:
1- bubonocele: the hernia is limited to inguinal canal, the processus vaginalis
having been obliterated at the superficial inguinal ring, seen mainly in young adult.
2- Funicular: the processus vaginalis is closed only at its lower end, just above the
epididymis, the content of the sac can be felt separately from the testis.
3- Complete: there is a persistence of prenatal condition before the processus
vaginalis becomes obliterated; nevertheless, a complete inguinal hernia is rarely
present at birth. Commonly encountered in infancy, it may not appear until
adolescent or adult life. The testis appears to l8e within the lower part of the
hernia.
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
Clinical features: an oblique hernia can appear at any age. Males are twenty times
more commonly affected than females. In the early stages of the development of
the, hernia when the sac is still limited to inguinal canal, the diagnosis presents
some difficulty. Often the patient complains of pain in the groin or pain referred to
the testicle when he is performing heavy work or taking strenuous exercise. The
patient is asked to cough and small transient bulging may be seen and felt with
expensile impulse.
Often the patient complains of pain in the groin or pain referred to the
testicle when he is performing heavy work or taking strenuous exercise. The
patient is asked to cough and small transient bulging may be seen and felt
with expensile impulse. Often the bulge may be better seen by observing the
inguinal region from the side or even looking down the abdominal wall
while standing slightly behind the respective shoulder of the patient. When
oblique inguinal hernia has become larger it produces a swelling that appears
at first intermittently.
In these circumstances the swelling often become apparent when the patient
coughs, and it persists until it is reduced usually by the act of lying down.
Local pain is unusual unless complications have occurred. As the time goes on the
hernia comes down as soon as the patient assumes the upright position. In large
hernia there is a sensation of weight and dragging on the mesentery may produce
epigastric pain.
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
If the contents of the sac are reducible, the inguinal canal will be found to be
commodious. In infants the swelling appears when the child cries. An
inguinal hernia may be translucent in infancy and early childhood, but never
in an adult. In girls an ovary may prolapsed in to the sac.
Differential diagnosis in the male: 1- vaginal hydrocele. 2- An encysted hydrocele
of the cord. 3- Spermatocele. 4- A femoral hernia. 5- An incompletely descended
of the testis in inguinal canal. 6- A lipoma of the cord.
Differential diagnosis in the female: 1- a hydrocele of the canal of Nuck. 2- A
femoral hernia.
Treatment of indirect inguinal hernia: operation is the treatment of choice. In
infant by herniotomy and in adult by herniorrhaphy and hernioplasty. The main
point is exploration of the sac and then excision, this is called herniotomy, if there
is association with reconstruction or strengthening of the posterior abdominal wall
by suturing of the inguinal ligament with the conjoint tendon by nylon or using a
piece of mesh
Direct inguinal hernia:
between 10%-15% of inguinal hernia are
direct. Over half of the hernia is bilateral. A direct inguinal hernia is always
acquired. The sac passes through a weakness or defect of the transversalis fascia in
the posterior wall of inguinal canal. In some cases the defect is small and closely
related to the insertion of the conjoint tendon, while in others there is a generalized
bulge.
Often the patient has a poor lower abdominal musculature as shown by the
presence of elongated bulging called Malgaigne,s bulge.
Women in generally never develop direct inguinal hernia.
Predisposing factors are a chronic cough, straining and a heavy work.
Direct inguinal hernia rarely attains a large size or descends into scrotum.
The content mainly of extraperitonial fat and it is rarely obstructed or
strangulate.
Treatment by herniorrhaphy and hernioplasty.
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
Strangulated inguinal hernia:
occurs at any time during life,
and in both sexes. Indirect hernia strangulates more due to narrow neck, usually the
content is small intestine, and the next most common frequent is omentum or both.
Treatment is usually by emergency operation.
If dehydration and collapse are present, intravenous fluid replacement and gastric
aspiration by nasogastric tube and parental antibiotics with evacuation of the
bladder by a Folly's catheter. The operation done by releasing the content of sac
and check the availability of the bowel if it is not vital, resection of gangrenous
bowel should be done with anastomosis.
Femoral hernia:
is the third most common type of hernia. It account
for about 20% of hernia in women and 5% in men. The overriding importance of
femoral hernia lies in the facts that it cannot control by truss and that it is the most
liable to become strangulated.
Clinical feature: femoral hernia is very rare before the fifteen year. Between
twenty and forty years of age the prevalence rises, and continues to old age. The
right side affected twice often as the left and 20% of cases the condition is
bilateral. The symptoms to which femoral hernias gives rise are less pronounced
that those of inguinal hernia, indeed, a small femoral hernia may be unnoticed by
the patient or disregarded for years.
Differential diagnosis:
1- Inguinal hernia.
2- Saphena varix. Is a saccular enlargement of the termination of the long
saphenous vein and usually accompanied by other sign of varicose vein.
3- Enlarged femoral lymph node.
4- Lipoma.
5- Femoral aneurysm.
6- Psoas abscess.
7- A distended psoas bursa. 8- Rupture of adductor longus with hematoma. It
cannot be emphasized too strongly that not only does a femoral hernia
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
become strangulated frequently, but often gangrene develops rapidly. This is
accounted for by the narrow unyielding femoral ring.
Treatment:
by operative measures.
Umbilical hernia:
in children, this hernia comes through a weak
umbilical scar usually the result of neonatal sepsis. The ratio of males to females
2:1. The hernia is often symptomless but increase in the size of the hernia by
crying causes pain which make the infant cry the more. Small hernia is spherical,
that increases in size tend to assume a comical shape and present apart from crying.
Obstruction or strangulation below the age of years is extremely uncommon.
Treatment; conservative treatment by masterly inactivity is successful in
about 93% of cases. When the hernia is symptomless reassurance of the
parents is all that necessary, for in a very high percentage of cases the hernia
will be found to disappear spontaneously during the first few months of life.
Cure may be hastened by pulling the skin and abdominal musculature
together by adhesive strapping placed across the abdomen.
Paraumbilical hernia:
it should be noted that in adults the hernia does
not occur through the umbilicus scar. It is protrusion through the lina alba just
above the umbilicus or occasionally just below that structure.
Clinical feature: women are affected five times more frequently than men. The
patient is usually corpulent and between the ages of thirty –five and fifty.
Increasing obesity, with flabbiness of the abdominal muscles and repeated
pregnancy are important factors.
These hernias soon become irreducible because of omental adhesions within
the sac. A large umbilical hernia causes a local dragging pain by its weight.
Gastro-intestinal symptoms are common and are probably due to traction on
the stomach or transverse colon. Often there are transient attacks of
intestinal colic due to subacute intestinal obstruction. Treatment: untreated,
the hernia increases in size, and more of its contents become irreducible.
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
Eventually, strangulation may occur. Therefore without undue delay
operation should be advised in nearly all cases. If the patient is obese and the
hernia is symptomless, operation can be postponed with advantage until
weight has been reduced.
Incisional hernia:
usually starts as a symptomless partial disruption of
the deeper layers of a laparotomy wound during immediate or very early
postoperative period. It occurs more frequently in obese patients and a persistence
postoperative cough and postoperative abdominal distension. There a high
incidence of incisional hernia following operation for peritonitis as the result of
wound infection.
Clinical feature: incisional hernia presents no difficulty in diagnosis. There is
great variation in the degree of herniation. The hernia may occur through a small
portion of the scar often the lower end. More frequently there is a diffuse bulging
of the whole length of the incision.
A postoperative hernia especially one through a lower abdominal scar
usually increases steadily in size and more and more of its content becomes
irreducible. Sometimes the skin overlying it is so thin and atrophic that
normal peristalsis can be se3en in the underlying coils of intestine.
Attacks of subacute intestinal obstruction are common and strangulation is
liable to occur at the neck of a small sac or in a loculus of a large one.
Palliative by abdominal belt in patient cannot do the operation, but the
treatment should be surgical repair. Weight reduction preoperatively must be
done because there is a risk of failure of hernial repair or there is possibility
of paralytic ileus from visceral compression and pulmonary complication
from elevation of diaphragm.
Epigastric hernia:
occurs through the lina alba anywhere between the
xiphoid process and the umbilicus usually mid-way between these structures. It
commences as protrusion of extraperitonial fat through the lina alba where the
latter is pierced by a small blood vessel. A swelling the size of a pea. The mouth of
the scar is rarely large enough to permit a portion of a hollow viscus to enter it;
consequently either the sac is empty or it contains a small portion of greater
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
omentum. The patient is usually manual worker between thirty and forty-five years
of age.
Clinical feature: symptomless---a small fatty hernia of the lina alba can be felt
well than it can be seen, and may be symptomless being discovered only in the
course of routine abdominal palpation. Or4 it can be painful as local pain or tender
to touch and tight clothes. Or it has referred pain as gastric or duodenal ulcer.
Treatment by surgical repair.
Umbilicus:
Inflammation of the umbilicus:
Infection of the umbilical cord: in over 50% of babies born in maternity
hospitals the stump of the umbilical cord is found to be carrying
staphylococci by the third or fourth day post-delivery. Less commonly the
stump of the cord harbors streptococci and epidemics of puerperal sepsis in
maternity hospitals have been traced to the umbilical cord of one infant in
the nursery thus infected. E. coli and clostridium tetani (causing neonatal
tetanus) are other possible invaders. The chief prophylaxis is strict asepsis
during severance of the cord and he use of 0.1% chlorhexidine locally for a
few days.
Omphalitis:
the incidence of an infected umbilicus is much higher in
communities that do not practice aseptic servence of the umbilical cord. When the
stump of the umbilical cord becomes inflamed, antibiotic therapy usually localize
the inflammation. By employing warm, moist dressing, the crusts separate, giving
exit to pus. Exuberant granulation tissue requires a touch of silver nitrate. I9n more
serious cases infection is liable to spread along the defunct hypo gastric arteries or
umbilical vein when, in all probability, one or other of the following complications
will supervene:
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
1- Abscess of the abdominal wall: if gentle pressure is exerted above the naval
and a bead of pus exudes at the navel, a deep abscess associated with one of
the defunct umbilical vessels is present. This must be opened. A probe is
passed in to sinus to determine its direction and this is followed by a
grooved director on to which the skin and overlying tissues are incised in the
midline.
2- Extensive ulceration of the abdominal wall: extensive ulceration of the
abdominal wall due to synergistic infectionis treated in the same way as
postoperative subcutaneous gangrene.
3- Septicemia: can occur from organisms entering the blood stream via the
umbilical vein. Jaundice is often the first sign. An abscess in the abdominal
wall above the umbilicus should be sought. In other respects, the treatment
of this grave complication follows the usual line.
4- Jaundice in the newborn: infection reaching the liver via the umbilical vein
may cause a stenosing intrahepatic cholangitis appearing some 3-6 weeks
after birth.
5- Portal vein thrombosis and subsequent portal hypertension.
6- Peritonitis carries a band prognosis.
7- Umbilical hernia.
Umbilical granuloma:
it is a chronic infection of the umbilical cicatrix
that continues for week’s cause’s granulation tissue to pout at the umbilicus. There
is no certain means of distinguishing this condition from adenoma. Usually,
umbilical granuloma can be treated by one application of silver nitrate followed
by dressing, but adenoma soon recurs in spite of these measures.
Dermatitis of and around the umbilicus:
fungus and parasitic infections
are more difficult to eradicate from the umbilicus than from the skin of the
abdomen. Sometimes the dermatitis is consequent upon a discharge from the
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
umbilicus as is the case when umbilical fistula or a sinus is present. In overweight
women, intertrigo occurs.
Pilonidal sinus of the umbilicus:
pilonidal sinus is sometimes
encountered. It should be excised.
Umbilical calculus (umbolith):
this is often black in color and is composed
of desquamated epithelium, which becomes inspissated and collects in the deep
recess of the umbilicus. The treatment is to dilate the orifice and extract the
calculus but, to prevent recurrence, it may be necessary to excise the umbilicus.
Umbilical fistulae:
as the umbilicus is a central abdominal scar it is
understandable that a slow leak from any viscus is liable to track to the surface at
this point. Added to this, very occasionally, the vitellointestinal duct or the urachus
remains patent; consequently, it has been aptly remarked that the umbilicus is a
creek into which many fistulous streams may open. For instance, an enlarged,
inflamed gall bladder perforating at its fundus may discharge gall stones through
the umbilicus.
An unremitting flow of pus from a fistula at the umbilicus of middle aged women
led to the discovery of a length of gauze overlooked during a hysterectomy 5 years
previously. Anomalies connected with the vitellointestinal duct (a) umbilical
fistula (b) intraabdominal cyst (c) intraabdominal band (d) meckel,s diverticulum
with a band adherent to the sac of the congenital umbilical hernia.
Neoplasm of the umbilicus:
umbilical adenoma or raspberry tumor: this is
commonly seen in infants but only occasionally later in life. It is due to partially or
completely unobliterated Vitellointestinal duct. Mucosa prolapsing through the
umbilicus gives rise to raspberry like tumor which is moist and tends to bleed.
Treatment: if the tumor is pedunculated. A ligature is tied around it and in few
days the polypus drop off. Should the tumor reappear after this procedure,
umbilectomy is indicated. Vitellointestinal band will be associated with a Meckel,s
Surgery
Abdominal Wall Hernias and Umbilicus
Dr. Tariq E. Al-Aubiadi
Lec. 19
diverticulum. The meckel,s diverticulum and the attached cord or duct should be
excised at the same time as the umbilicus. Histologically the tumor at the
umbilicus consists of columnar epithelium rich in goblet cells.
Endometrioma can also be present in the umbilicus and bleed at each menstrual
cycle. Treatment is by excision of the umbilicus.
Malignant tumors:
as secondary carcinoma or called Sister Joseph's
nodule is quite common but is always a late manifestation of the disease. The
primary neoplasm is often situated in the stomach, colon, or ovary but metastasis
from the breast probably transmitted along the lymphatic of the round ligament of
the liver is sometimes located here.