Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
Incidence & Epidemiology
• BPH is the most common benign tumor in men, and its incidence is age
related.
• Symptoms of prostatic obstruction are also age related.
• At age 55, approximately 25% of men report obstructive voiding symptoms.
• At age 75, 50% of men complain of a decrease in the force and caliber of
their urinary stream.
BPH?
• BPH to the pathologist is a microscopic diagnosis characterized by cellular
proliferation of the stromal and epithelial elements of the prostate .
• The radiologist makes the diagnosis of BPH on the basis of an enlarged
prostate either on ultrasound or with three-dimensional diagnostic imaging
studies of the male pelvis.
• BPH to the practicing urologist represents a constellation of signs and lower
urinary tract symptoms (LUTS) that develop in the male population in
association with aging and prostatic enlargement.
• The patient is typically concerned about the impact of BPH on quality of life
rather than the presence of cellular proliferation, prostatic enlargement, or
elevated voiding pressures.
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
Etiology
• The observed increase in cell number may be due to epithelial and
stromal proliferation or to impaired programmed cell death leading to
cellular accumulation.
• Androgens, estrogens, stromal-epithelial interactions, growth factors, and
neurotransmitters may play a role, either singly or in combination, in the
etiology of the hyperplastic process.
Hyperplasia
• In a given organ, the number of cells, and thus the volume of the organ, is
dependent upon the equilibrium between cell proliferation and cell death .
The Role of Androgens
• Although androgens do not cause BPH, the development of BPH requires
the presence of testicular androgens during prostate development, puberty,
and aging .
• In the prostate, however, the nuclear membrane bound enzyme steroid 5α-
reductase converts the hormone testosterone into DHT, the principal
androgen in this tissue .
• The prostate, unlike other androgen-dependent organs, maintains its ability
to respond to androgens throughout life .
The Role of Estrogens
• The role of estrogens in the development of human BPH, however, is less
clear.
• In the dog, where estrogens act synergistically with androgens to produce
experimental BPH, estrogen appears to be involved in induction of the AR
(androgen receptors).
Regulation of Programmed Cell Death
• Programmed cell death (Apoptosis) is a physiologic mechanism crucial to
the maintenance of normal glandular homeostasis.
• An organ can enlarge not only by an increase in cell proliferation but also by
a decrease in cell death.
• Following castration, active cell death is increased.
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
Growth Factors
• Interactions between growth factors and steroid hormones may alter the
balance of cell proliferation versus cell death to produce BPH.
The Potential Role of Inflammatory Pathways and Cytokines in BPH.
• Studies suggested a link between inflammation and BPH-related growth
reported extensive infiltration of human BPH tissues by activated T cells.
Genetic and Familial Factors
• Relative Risk of Clinical BPH =4.4 %
• Autosomal dominant inheritance pattern.
• Familial BPH was characterized by large prostate size, with a mean prostate
volume of 82.7 mL in men with hereditary BPH compared with 55.5 mL in
men with sporadic BPH.
Pathology
• BPH develops in the transition zone.
• It is truly a hyperplastic process resulting from an increasein cell number.
• Microscopic evaluation reveals a nodular growth pattern that is composed
of varying amounts of stroma and epithelium.
• Stroma is composed of varying amounts of collagen and smooth muscle.
Anatomic Features
• One of the unique features of the human prostate is the presence of the
prostatic capsule, which plays an important role in the development of
LUTS.
• The size of the prostate does not correlate with the degree of obstruction.

Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
Pathophysiology
• Prostatic hyperplasia increases urethral resistance, resulting in
compensatory changes in bladder function.
• The elevated detrusor pressure required to maintain urinary flow in the
presence of increased outflow resistance occurs at the expense of normal
bladder storage function.
• Obstruction-induced changes in detrusor function, compounded by age-
related changes in both bladder and nervous system function, lead to urinary
frequency, urgency, and nocturia, the most bothersome BPH-related
complaints.
SYMPTOMS
• The symptoms of BPH can be divided into obstructive and irritative
complaints.
• Obstructive symptoms include: hesitancy, decreased force and caliber of
stream, sensation of incomplete bladder emptying, double voiding, straining
to urinate, and post-void dribbling.
• Irritative symptoms include urgency, frequency, and nocturia.
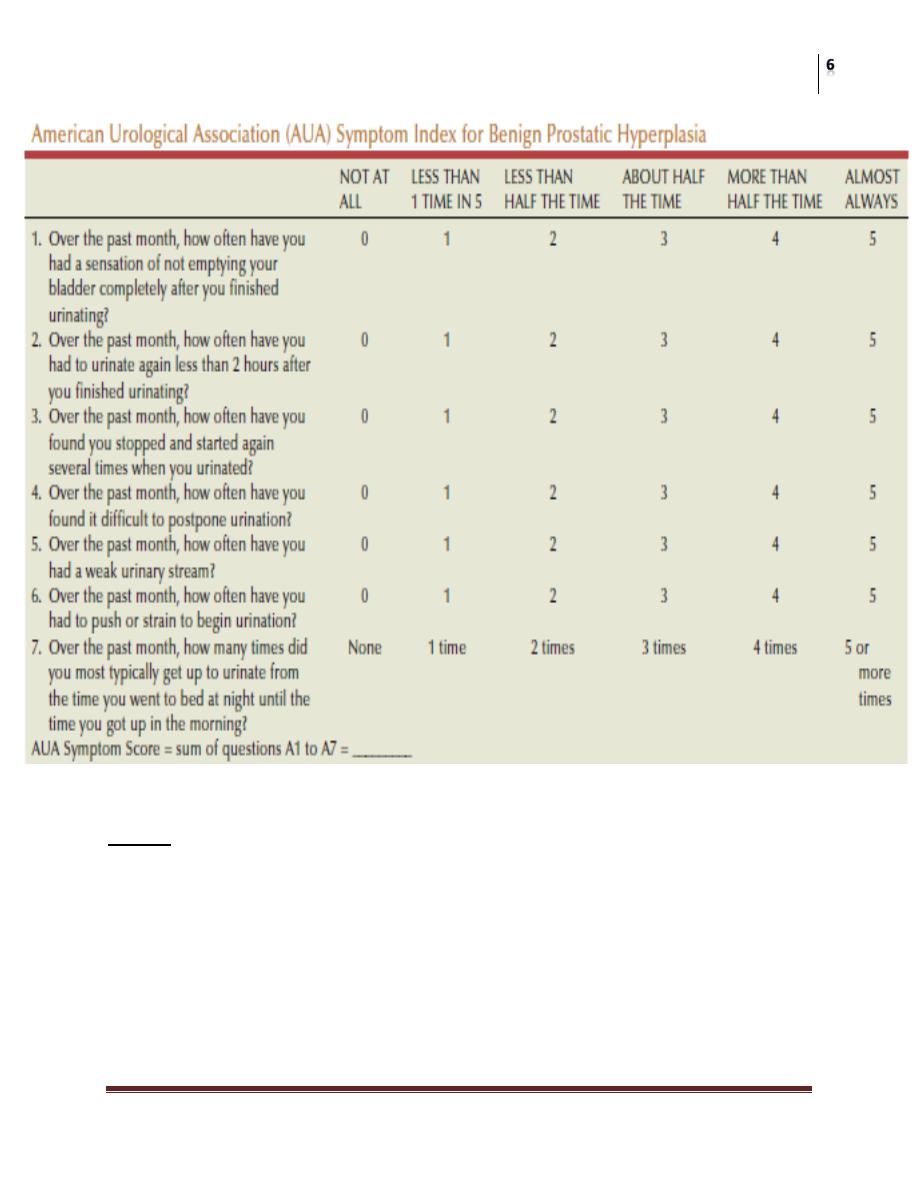
Symptom Assessment
• The International Prostate Symptom Score (IPSS), is recommended as
the symptom scoring instrument to be used for the baseline assessment
of symptom severity in men presenting with LUTS.
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
SIGNS
• A physical examination, DRE, and focused neurologic examination are
performed on all patients.
• BPH usually results in a smooth, firm, elastic enlargement of the
prostate.
• Induration, if detected, must alert the physician to the possibility of
cancer and the need for further evaluation.
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
LABORATORY FINDINGS
• A urinalysis to exclude infection or hematuria
• Serum creatinine measurement to assess renal function are required.
• Serum PSA is considered optional, but most physicians will include it in the
initial evaluation.
• PSA, compared with DRE alone, certainly increases the ability to detect
CAP.
IMAGING
• Upper-tract imaging (intravenous pyelogram or renal ultrasound) is
recommended only in the presence of concomitant urinary tract disease or
complications from BPH (eg, hematuria, urinary tract infection, renal
insufficiency, history of stone disease).
CYSTOSCOPY
• Cystoscopy is not recommended to determine the need for treatment but may
assist in choosing the surgical approach in patients opting for invasive
therapy.
ADDITIONAL TESTS
• Cystometrograms and urodynamic profiles are reserved for patients with
suspected neurologic disease or those who have failed prostate surgery.
• Measurement of flow rate, determination of post-void residual urine, and
pressure flow studies are considered optional.
Differential Diagnosis
• Other obstructive conditions of the lower urinary tract, such as urethral
stricture, bladder neck contracture, bladder stone, or CaP,must be
entertained when evaluating
• men with presumptive BPH: A history of previous urethral instrumentation,
urethritis, or trauma should be elucidated to exclude urethral stricture or
bladder neck contracture.
• Hematuria and pain are commonly associated with bladder stones.
• Ca.Prostate may be detected by abnormalities on the DRE or an elevated
PSA.
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
• A urinary tract infection, which can mimic the irritative symptoms of BPH,
can be readily identified by urinalysis and culture.
• Patients with neurogenic bladder disorders may have many of the signs and
symptoms of BPH, but a history of neurologic disease, stroke, diabetes
mellitus, or back injury.
Treatment
• After patients have been evaluated, they should be informed of the various
therapeutic options for BPH.
• It is advisable for patients to consult with their physicians to make an
educated decision on the basis of the relative efficacy and side effects of the
treatment options.
A. WATCHFUL WAITING
Watchful waiting is the appropriate management of men with mild symptom scores
(0–7).
Patients in the placebo arm of the study had a 7% risk of developing urinary
retention over 4 years.
Timed voiding, Decrease Fluid intake…
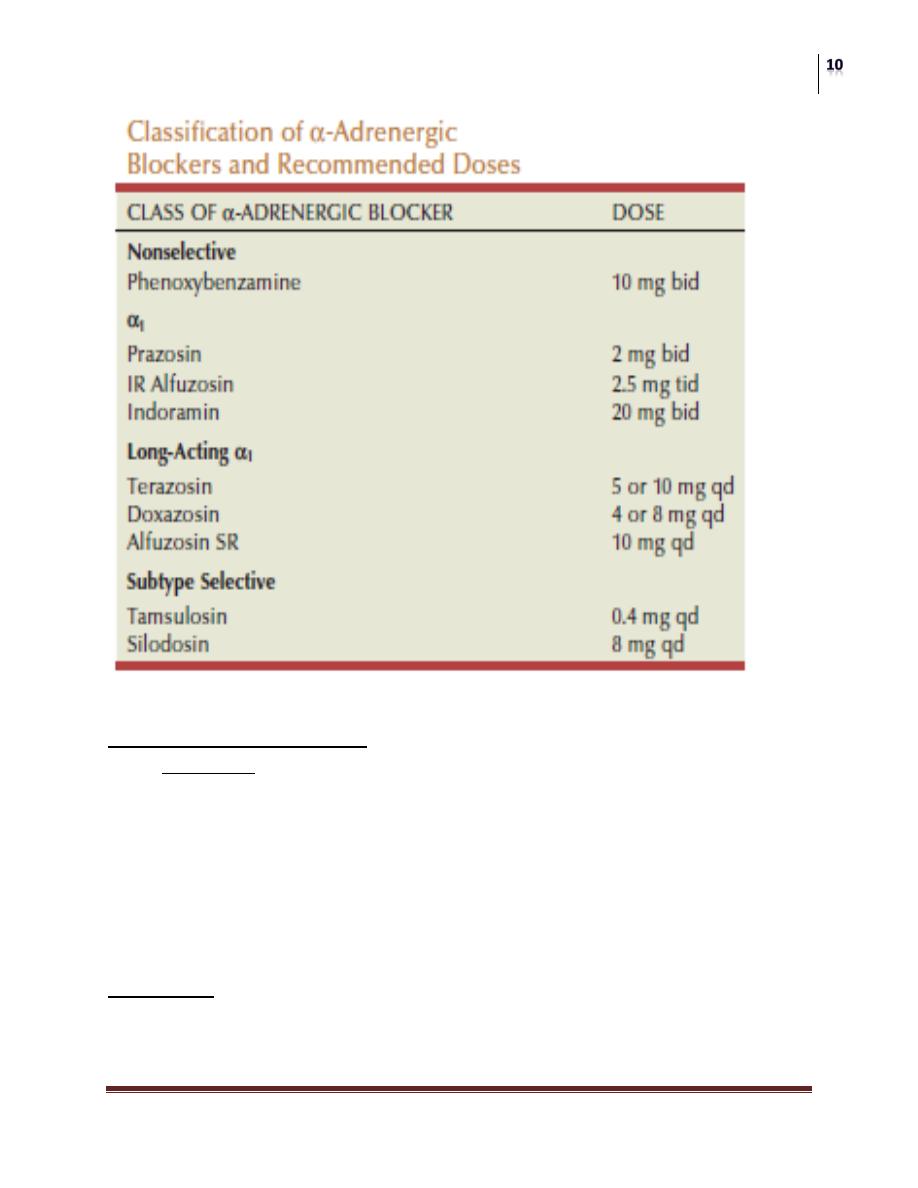
B. MEDICAL THERAPY
• Medical therapies investigated for BPH include :
• α-adrenergic blockers,
• 5α-reductase inhibitors,
• aromatase inhibitors, and
• numerous plant extracts .
• Anticholinergics
• Phosphodiastrase inhibitors.
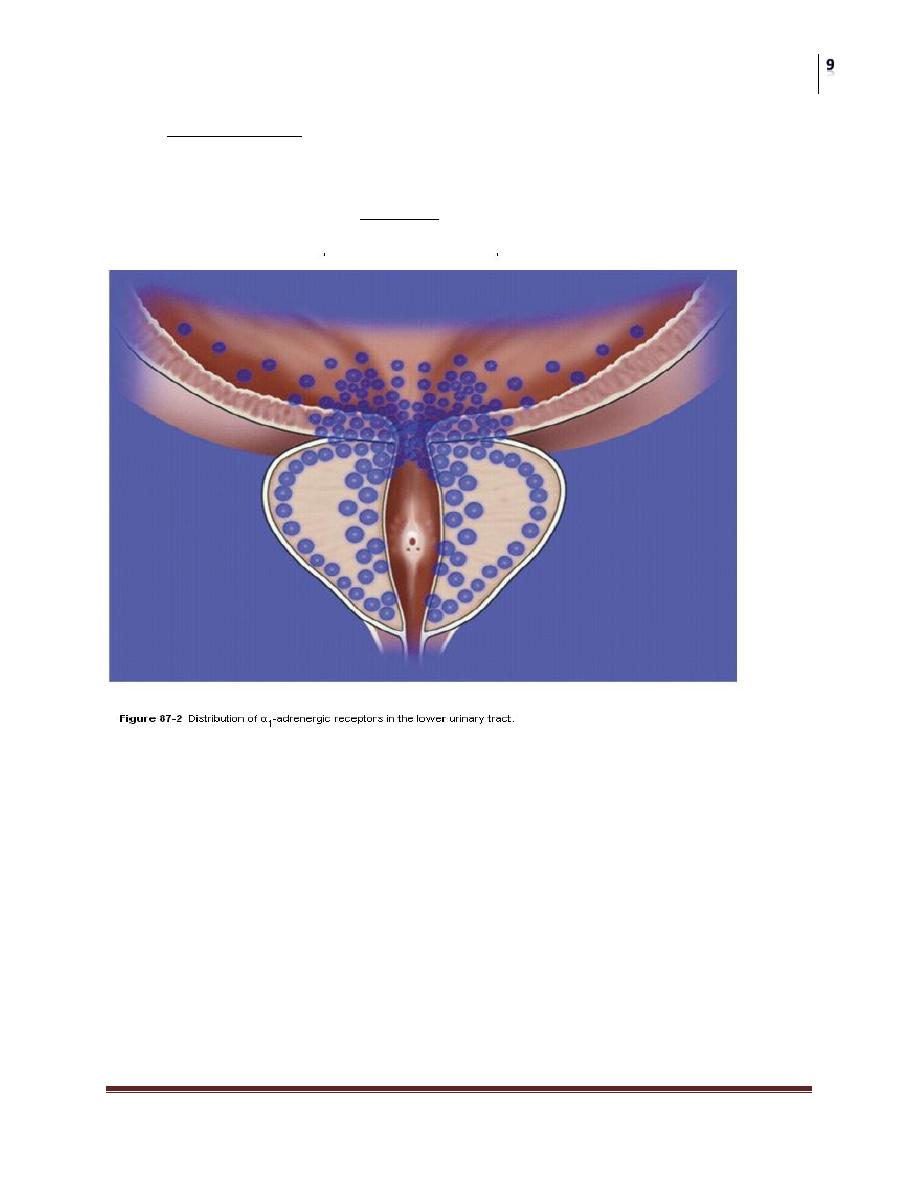
1. Alpha-blockers
• The human prostate and bladder base contains alpha-1-adrenoreceptors, and
the prostate shows a contractile response to corresponding agonists.
• The contractile properties of the prostate and bladder neck seem to be
mediated primarily by the subtype alpha-1a receptors.
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
• Alpha-blockade has been shown to result in both objective and subjective
degrees of improvement in the symptoms and signs of BPH in some
patients.
• Alpha blockers can be classified according to their receptor selectivity as
well as their half-life.
• The most recent advance in alpha-blocker therapy is related to the
identification of subtypes of alpha-1-receptors.
• Selective blockade of the alpha-1a receptors, which are localized in the
prostate and bladder neck, results in fewer systemic side effects (orthostatic
hypotension, dizziness, tiredness, rhinitis, and headache), thus obviating the
need for dose titration.
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
5-Alpha-reductase inhibitors
• Finasteride is a 5- alpha-reductase inhibitor that blocks the conversion of
testosterone to dihydrotestosterone.
• This drug affects the epithelial component of the prostate, resulting in a
reduction in the size of the gland and improvement in symptoms.
• Six months of therapy are required to see the maximum effects on prostate
size (20% reduction) and symptomatic improvement.
• However, Symptomatic improvement is seen only in men with enlarged
prostates (>40 cm3).
Side effects include decreased libido, decreased ejaculate volume, and impotence.
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
• Serum PSA is reduced by approximately 50% in patients being treated with
finasteride, but individual values may vary.
• Dutasteride differs from finasteride as it inhibits both isoenzymes of 5-
alpha-reductase.
• Similar to finasteride, it reduces serum prostatic specific antigen and total
prostate Size.
Combination therapy: The reduction in risk associated with combination therapy
(risk reduction) was significantly greater than that associated with alpha-blocker or
finasteride alone.
Phytotherapy:
• Phytotherapy refers to the use of plants or plant extracts for medicinal
purposes.
• The use of phytotherapy in BPH has been popular in Europe for years, and
its use in the United States is growing as a result of patient-driven
enthusiasm.
Others
• Flutamide :Flutamide is an orally administered nonsteroidal antiandrogen
that inhibits the binding of androgen to its receptor.
• Cetrorelix :Cetrorelix is the only gonadotropin-releasing hormone
antagonist that has been investigated for BPH.
• Atamestane: is a highly selective aromatase inhibitor that lowers both
serum and intraprostatic levels of estradiol and estrone.
• Anti cholinergics: Decrease storage symptoms.
• Phosphodiastrase inhibitors: investigational.
Surgical treatment for BPH
• Absolute surgical indications include :
• Refractory urinary retention (failing at least one attempt at catheter
removal),
• Recurrent urinary tract infection from BPH,
• Recurrent gross hematuria from BPH,
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
• Bladder stones from BPH, renal insufficiency from BPH, or large bladder
diverticula.
Types and indiccations of surgical techniques:
A- CONVENTIONAL SURGICAL THERAPY
Types:
• 1. Transurethral resection of the prostate.(TURP).
• 2. open prostatectomy.
A-Trans vesical
B- retropubic
Indications for open prostatectomy
• TURP is a gold standard. BUT:
• When the prostate is too large to be removed endoscopically, an open
enucleation is necessary.
• Open prostatectomy may also be initiated when concomitant bladder
diverticulum or a bladder stone is present or if dorsal lithotomy positioning
is not possible.
• Open prostatectomies can be done with either a suprapubic(trans vesical) or
retropubic approach.
• Transvesical approach used when there is intra vesical pathalogy like stone
or diverticulum.
B- MINIMALLY INVASIVE THERAPY
Indications: For patient with moderate symptoms score or unfit for surgery.
1. Laser therapy: Many different techniques of laser surgery for the prostate have
been described. See later.
2. Transurethral electrovaporization of the prostate: Transurethral
electrovaporization uses the standard resectoscope but replaces a conventional loop
with a variation of a grooved rollerball.
3. Hyperthermia: Microwave hyperthermia is most commonly delivered with a
transurethral catheter. Some devices cool the urethral mucosa to decrease the risk
of injury.
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
4. Transurethral needle ablation of the prostate.
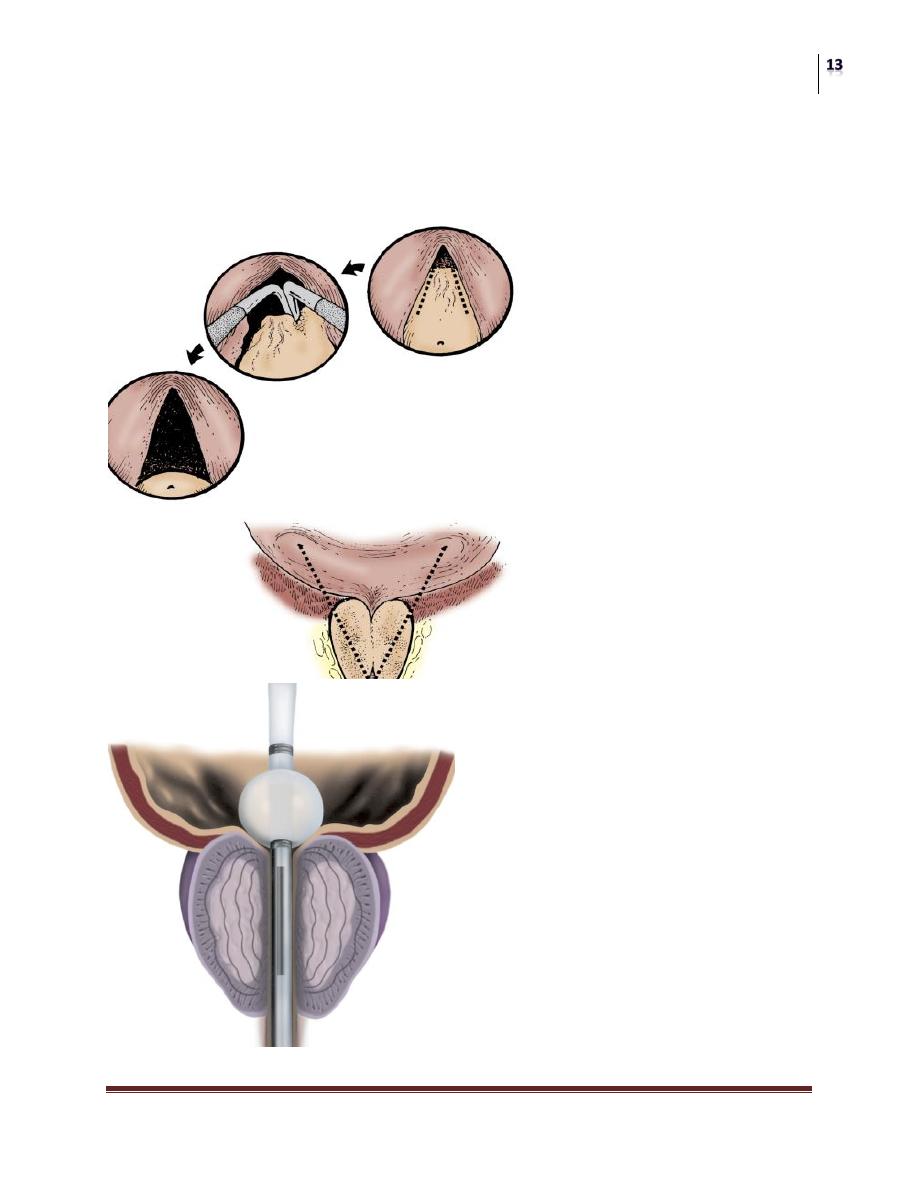
5. Transurethral incision of the prostate.
6. High-intensity focused ultrasound.
7. Intraurethral stents.
Surgery
Benign Prostate Hyperplasia
Dr. Saad Dakhil
Lec. 46
C- Laser Prostatectomy
• There are four types of laser that can be used to treat the prostate.
• 1-Neodymium:Yttrium-Aluminum-Garnet Laser
• 2-Potassium Titanyl Phosphate Laser
• 3-Diode Laser .
• 4-Holmium:Yttrium-Aluminum-Garnet Laser.
• Procedures:
• Prostatectomy with Holmium Laser : Now considered the standard care in
many centre it has the advantage of being less blood loss and urethral
catheterization and hospitalization time.