


Pediatric Hematologic Malignancy5th Year Medical Students
Dr. Salma AL-HadadApril 12th 2016
Objectives
To list the most common pediatric malignanciesDefine leukemia and lymphoma & list their classifications
To list the signs and symptoms of leukemia and lymphoma
To outline the steps for diagnosis of leukemia and lymphoma
Epidemiology
Pediatric cancer is rare - 2% of all cancerMost often occur before 15 years of age
Accounts for 10% of childhood deaths
Most common cause of death from disease
Second to accidents
Leukemia, Lymphoma and CNS Tumors are the most common
Predisposing Factors
Genetic
• Syndromes (trisomy 21), bone marrow failure
Hereditary
• Wilms Tumor, Retinoblastoma
Environmental
• Radiation, toxins
Case Study
5 year old girl presented with 1 week history of fatigue, pain that began in her feet and progressed to legs; and a petechial rash over her arms and legs with some bruising.She had a brief episode of epistaxis one day prior to appointment.
They also felt that her abdomen is prominent for the past 2 weeks.
Differential Diagnosis
Viral Illness?Idiopathic Thrombocytopenic Purpura (ITP)?
Aplastic Anemia?
Leukemia?
Case Study
Case Study
Initial labs at admission:
CBC
Hb: 4.9 g/dl (11.5-13.5)
Platelets: 6,000/cmm (150,000-400,000)
WBC: 27,000/cmm
Blasts: 34%
Neutrophils 1%
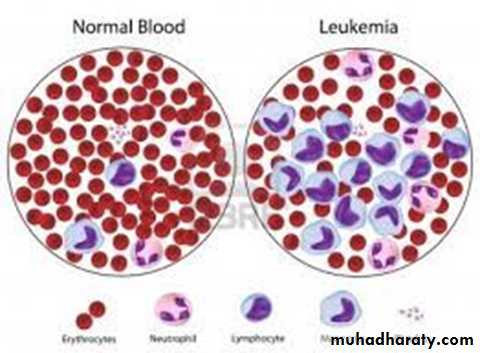
Introduction to leukemia
Leukemia is a malignant disease characterized by unregulated proliferation of one cell typeLeukemias are classified into 2 major groups
Chronic in which the onset is insidious, the disease is usually less aggressive, and the cells involved are usually more mature cells
Acute in which the onset is usually rapid, the disease is very aggressive, and the cells involved are usually poorly differentiated with many blasts.
Introduction to leukemia
Both acute and chronic leukemia are further classified according to the prominent cell line involved in the expansion:If the prominent cell line is of the myeloid series it is a myelocytic leukemia
If the prominent cell line is of the lymphoid series it is a lymphocytic leukemia
Classification of leukemia
AcuteChronic
Myeloid origin
Lymphoid origin
Acute Myeloid Leukemia (AML)
17%
Acute Lymphoblastic Leukemia (ALL)
80%
Chronic Myeloid
Leukemia (CML)
3%
Chronic Lymphocytic
Leukemia (CLL)
Virtually none
Bone marrow
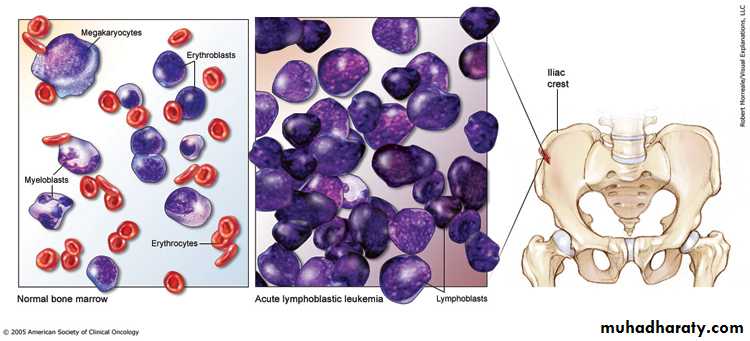
Normal Leukemic (ALL)

Hematopoietic
stem cell

Neutrophils
Eosinophils
Basophils
Monocytes
Platelets
Red cells
Myeloidprogenitor
Lymphoid
progenitor
B-lymphocytes
T-lymphocytes
Plasmacells
germinal center
naïve
ALL
AML
Introduction to leukemia
Leukemic proliferation, accumulation, and invasion of normal tissues, including the liver, spleen, lymph nodes, central nervous system, and skin, cause lesions ranging from rashes to tumors.A humoral mediator from the leukemic cells may inhibit proliferation of normal cells.
Failure of the bone marrow and normal hematopoiesis may result in pancytopenia with death from hemorrhage and infections.
Introduction to leukemia
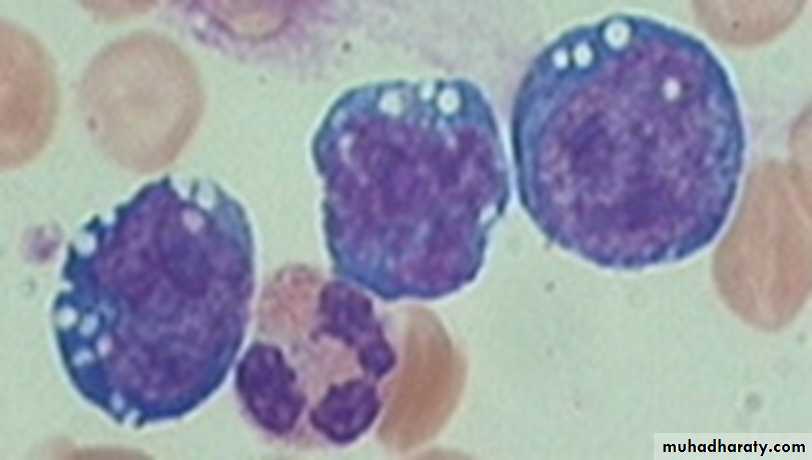
The lab diagnosis is based on two thingsFinding a significant increase in the number of immature cells (blasts), >30% blasts is diagnostic (normally <5%)
Identification of the cell lineage of the leukemic cells
Clinical manifestations
Symptoms due to:Marrow failure
Tissue infiltration
Leukostasis
Constitutional symptoms
Other (DIC)
Usually short duration of symptoms
Marrow failure
Neutropenia: Infections, sepsis
Anemia: Fatigue, pallor
Thrombocytopenia: Bleeding
Enlargement of liver, spleen, lymph nodes
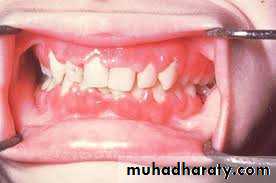
Gum hypertrophy
Bone pain
Other organs: CNS, skin, testis, any organ
Leukostasis
Accumulation of blasts in microcirculation with impaired perfusion• Only seen with WBC > 50 x 109/L
• Lungs: Hypoxemia, pulmonary infiltrates
• CNS: Stroke
Diagnosis: Symptoms
FatiguePallor
Anorexia
Bruising/Bleeding
Fever
Bone/joint pain
Diagnosis: Exam Findings
Pallor
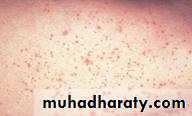
Bruises & Petechiae
Lymphadenopathy
Hepatosplenomegaly
Cranial Nerve Palsies
Testicular enlargement
Chloromas & Leukemia Cutis
Mediastinal Mass
Superior Vena Cava Syndrome
Leukemia Cutis
Petechiae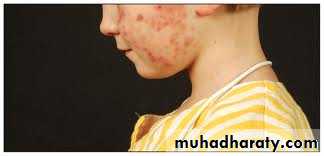
Gum hypertrophy
Differential Diagnosis
Viral Illness lymphadenopathyITP bleeding tendency
Aplastic Anemia anemia and bleeding tendency
Arthritis Joint swelling
SLE Joint swelling
Diagnostic Studies
Complete Blood CountBone marrow aspirate:
• Morphology & Immunohistochemistry examination using FAB classification: ALL L1-L3, AML M0-M7
Flowcytometry
Cytogenetics
Diagnostic Studies
CBCWBC usually elevated, but can be normal or low
Blasts in peripheral blood
Normocytic anemia
Thrombocytopenia
Neutropenia
Laboratory tests:
To detect infiltration of the disease; CXR, CSF, Ultrasound for kidneyTo assess the function of other organs; LFT, RFT, viral titers, LDH, uric acid
Auer rods in AML
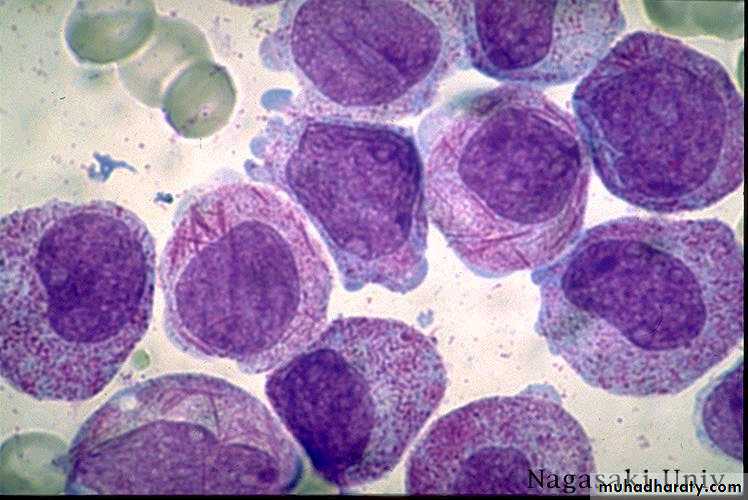
ALL

Principles of treatment
Combination chemotherapyFirst goal is complete remission,
Further treatment to prevent relapse
Supportive medical care
transfusions, antibiotics, nutrition
Psychosocial support
patient and family
Prognosis
Leukemia is now a curable disease in developed world
ALL 80% - 90%
AML 65%
Childhood lymphoma
Lymphomas are malignant neoplasms of lymphoid lineage.Major types include Hodgkin's and Non-Hodgkin's lymphoma
60% are Non-Hodgkin's lymphoma (NHL)
40% Hodgkin’s Lymphoma (HL)
Hodgkin’s lymphoma
Six year old boy presented with painless right sided cervical swellingnot responding to antibiotics
How do they present?


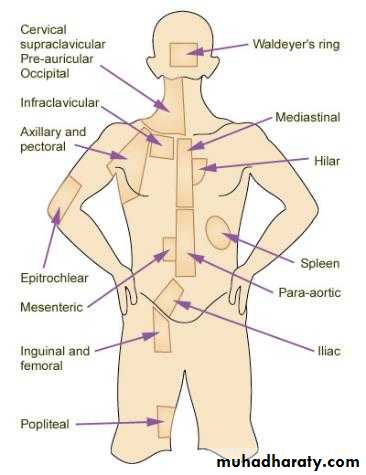
Clinical Presentation
The onset is typically subacute & prolonged for HLMost common presentation in children is asymptomatic cervical lymphadenopathy in 90% of cases
Painless, firm or rubbery, not inflammatory
Extension from one lymph node group to another
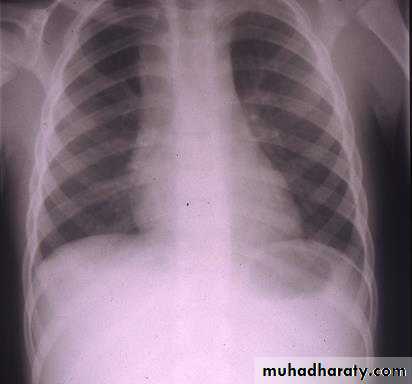
Asymptomatic mediastinal mass discovered by CXR
mediastinal adenopathy at presentation occurs in 60% of patients
Cough or SOB if significant compression
Systemic symptoms, classified as B symptoms
Unexplained fever >39°CWeight loss >10% total body weight over 3 months
Drenching night sweats
Infrequently presents as axillary or inguinal adenopathy
Clinical PresentationCase Study
A 13-y-old boy presented with malaise, night sweats, loss of weight and intermittent fever dating from a flu-like illness 3 months ago. O/E, he had bilateral, cervical & axillary LAP; the glands were 2-5cm in diameter, firm, rubbery, discrete and fairly mobile. His liver and spleen were not enlarged.
Investigation showed that his hemoglobin was low (11.3g/dl) and the WBC was normal but his ESR was 78mm/h; the blood film did not show any abnormal cells.
No enlargement of the hilar glands was seen on chest X-ray,
A cervical L.N. was removed for histology: the tissue consisted of giant cells known as Reed-Sternberg cells. These large binucleated cells are characteristic of Hodgkin's disease.
A BM examination was normal and CT showed no involvement of other lymph nodes.
This patient had stage IIB Hodgkin's disease.
In view of his symptoms, the suffix 'B' was added to the stage.
Case Study
Diagnostic Workup
Tissue is needed for definitive histologic diagnosisSample the node that is most accessible
Labs needed for evaluation (not for diagnosis)
CBC with blood film
ESR
LFT, Renal function
Alkaline phosphatase; ferritin,copper elevated
Immune response decreased,
Cytokines IL 1,6,TNF, IL 2 elevated - B symptoms,
Diagnostic & Staging Workup
Cervical area US/CT/MRI
Thoracic imaging
• Chest X-ray, CT scan of chest (ant/middle mediastinum) for best visualization of lung parenchyma, pleura
Abdominal imaging
• US/CT/MRI
Diagnostic & Staging Workup
Gallium Scan/ PET scanBone marrow biopsy
Bone scan
The pathologic hallmark of HD is the identification of Reed – Sternberg cells in tumor tissue.
Reed-Sternberg cells are giant binucleated cells with prominent nucleoli, classically a single giant nucleolus in each nucleus
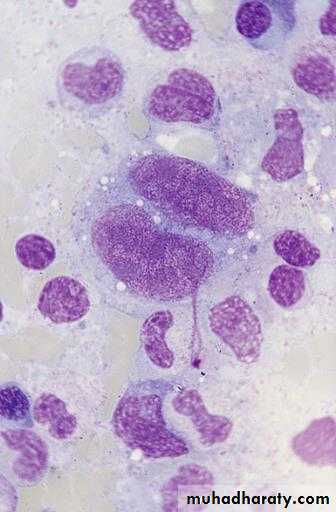
HL Histology
Hodgkin’s Disease TreatmentBalance ensuring the best opportunity for long-term, disease free survival and the lowest risk of severe treatment toxicity
With appropriate treatment about 85% of patients with Hodgkin’s disease are curable with Combination Chemo + Radiotherapy
NHL Clinical Presentation
Depend primarily on pathological subtype and sites of involvement.
70% present with advanced stages III or IV including extra nodal disease as GIT, bone marrow, and central nervous system (CNS) involvement.
Burkitt’s Lymphoma (B-Cell) commonly presents with abdominal or head and neck masses with involvement of the bone marrow or CNS.
Lymphoblastic Lymphoma (T Cell) commonly presents with an intra thoracic or mediastinal mass, and may spread to the bone marrow and CNS.
Contrast and compare
Hodgkin’s LymphomaIndolent, unifocal
Cervical, mediastinal, supraclavicular LAD
B- symtoms common
Non-Hodgkin’s Lymphoma
Rapid (tumor lysis), multifocalAbdominal, mediastinal masses and LAD
Abdominal pain common
Intussusception
High Risk for NHL
Familial casesInherited immune deficiencies
Acquired immune deficiencies: HIV, organ transplant, post-BMT
EBV
malaria
Chemicals: Pesticides and solvents
NHL(Burkitt’s subtype) Jaw Mass
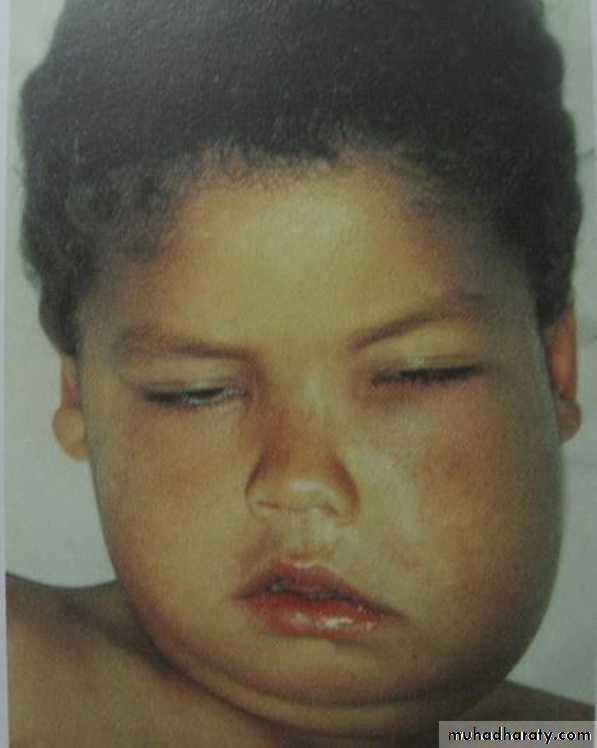

NHL(lymphoblastic subtype) mediastinal LAP
DiagnosisLymph node or tissue biopsy is mandatory for histologic diagnosis for appropriate:
Immunohistochemical,
Molecular studies,
Culture,
Cytogenetic analysis
Diagnostic Evaluation
Complete history and physical examination
Complete blood count with differential count, ESR
Chemistries: renal and hepatic function tests, serum electrolytes
Serum lactate dehydrogenase(LDH) and uric acid; alkaline phosphatase
Imaging studies: CXR, computed tomography (CT) of neck and chest, CT, etc.
Bone marrow examination
Cerebrospinal fluid examination (cytology)
Supportive
Chemotherapymulti-agent
intensive
Radiotherapy in special cases
Treatment Options
ComplicationsTumor related
• SVC syndrome
• Spinal cord compression
• Pleural and pericardial effusions
• Obstructive uropathy
• Pharyngeal/ airway obstruction
Metabolic
• Tumor lysis
GI
• Obstruction
Cytokine mediated
• Cachexia, fever, malaise
Hematologic
• BM infiltration
• Pancytopenia
Therapy
Chemotherapy
Surgery only for abdominal emergency
Radiation for SVC obstruction, or paraspinal compression
NHL - Treatment Response
Before Rx.
After Rx.
Prognosis of Lymphomas
Overall survival 70-80%Different sub-group survival