1
Fifth stage
Radiology
Lec-10
اسم الدكتور
5/4/2016
MAGNETIC RESONANCE IMAGING
…..
Why we use MRI when we have ct scan?
1. Because of higher tissue contrast resolution so it is more sensitive to detect brain
lesion.
2. beam hardening artifact is not present so visualization of posterior fossa is better on
MRI than on ct scan.
3. direct coronal & sagittal section are taken.
4. Lack of ionizing radiation.
MRI:employs radiowaves & magnetic fields.
- The patient is placed in a magnet & radiowave sent in, the transmitters is turned of & the
patient re-emits radiowaves , which are received & used for reconstruction of the image.
WHAT IS THE TYPE OF NUCLEI WHICH ABSORB & emit the radiofrequency energy?
It is the nuclei of hydrogen atoms in water & fat which absorb & emit the radiofrequency
energy.
WHAT IS THE MAGNETIC FIELD STRENGTH ?
The magnetic field strength has a set value between 0.5-2.0 tesla (T), depending on the
machine.
e.g.1T = this is some 20 000 times greater than the earth's magnetic field.
TISSUE CONTRAST
-The MR image maps two properties (T1 ,T2 ) of tissue & is controlled by two parameters
set by the operator TE (time to echo) & TR (time to repeat ).

2
T1 WEIGHTED IMAGE ( LONGITUDINAL RELAXATION TIME): the maximum contrast
differences between tissues of different T1 is produced by a short TR ( 300-600ms) , a short
TE (30 MS ).
+the shorter T1 , the stronger the signal & the brighter the pixel.
+ fat is bright as is fatty bone marrow , white matter & csf are dark.
T2 WEIGHTED IMAGE ( TRANSVERCE RELAXATION TIME): the maximum contrast
differences between tissues of different T2 is produced by a longer TE ( 90-140ms) , a long
TR(1000-2000 ms).
+the long T2 , the stronger the signal & the brighter the pixel , water & csf appear brighter
than fat.
T1 T2
3
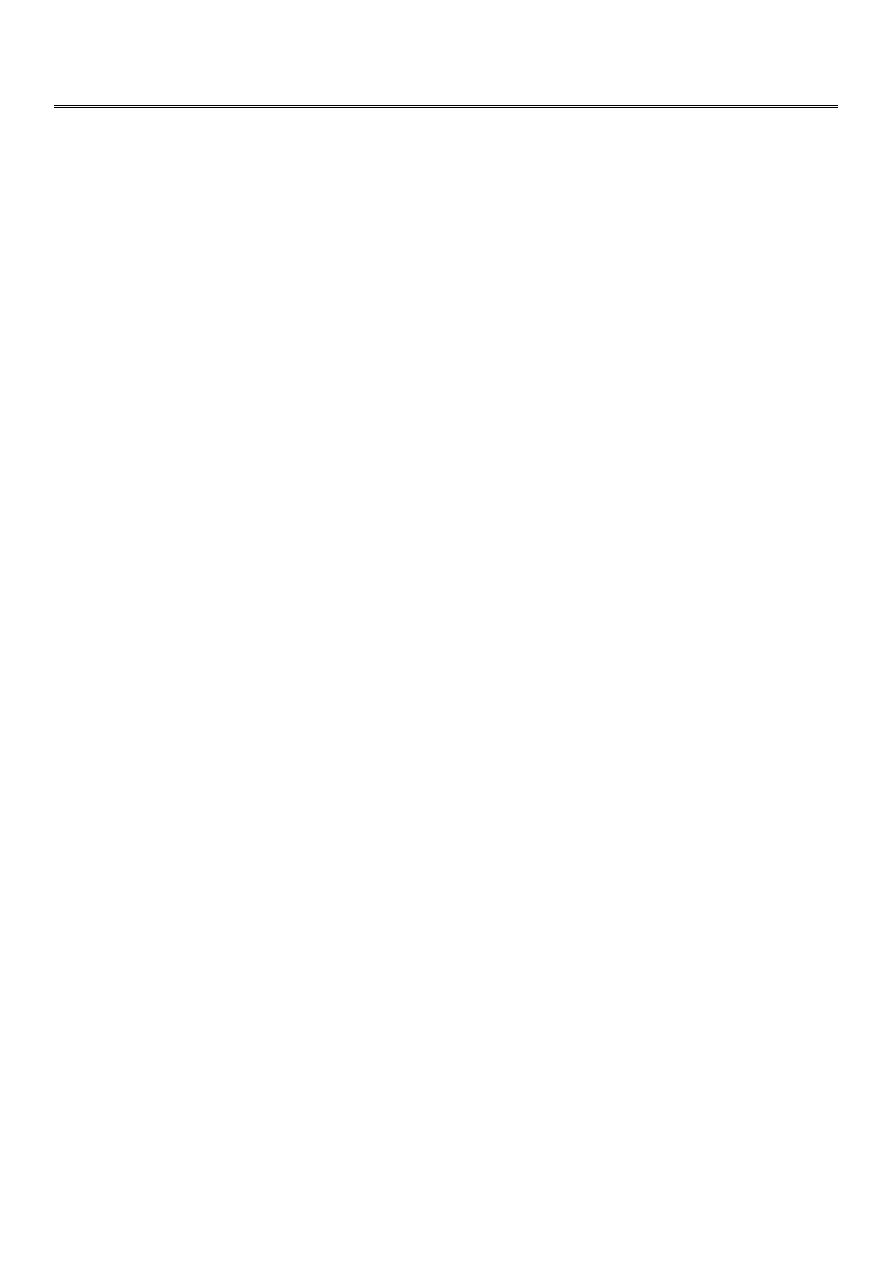
T 2/ FLAIR SEQUENCE: fluid attenuation inversion recovery T 1w + GADOLINEUM INJECTION
/ SAGITAL SECTION
Sagital section of brain ( T1 w post contrast injection)
CORONAL SECTION OF BRAIN ( T1w post contrast injection)

4
CONGENITAL LESION OF BRAIN
Congenital lesion of brain are well seen by MRI & CT scan but MRI has the advantage of
absence of ionizing radiation so can be used safely in children.
Congenital hydrocephalus:
Congenital hydrocephalus: Congenital hydrocephalus in infant & young children can be
classified as communicating & non – communicating.
Communicating Congenital hydrocephalus :
1-free communication between ventricles & basal cisterns.
2- obstruction to flow of csf is in the subarachnoid space or basal cisterns.
3- this is due to meningeal irritation by hemorrhage ,infection or trauma .
4- all ventricles are enlarged & basal cisterns may be prominent.
NON- Communicating Congenital hydrocephalus
:
CSF flow is obstructed within the ventricular system , usually at 3rd ventricle , aqueduct or
4th ventricular level.
The ventricles are dilated above the level of obstruction.
AQUIDUCT STENOSIS:
AQUIDUCT STENOSIS: It is the most common cause of NON- Communicating Congenital
hydrocephalus , it is congenital obstruction or stenosis of the aqueduct which result in
hydrocephalus involving the 3rd & lateral ventricles.
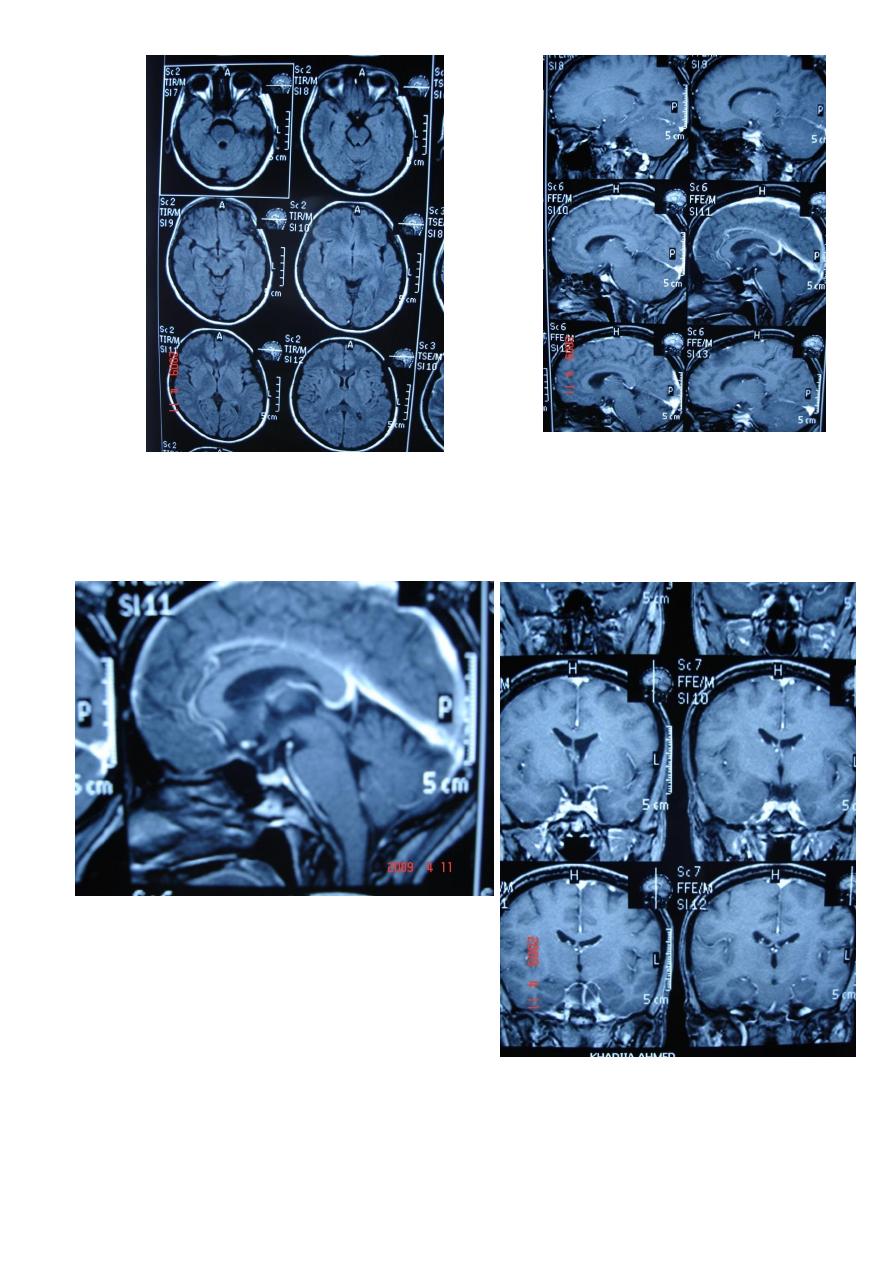
ARNOLD CHIARI MALFORMATION
1-Donward herniation of cerebellar tonsil & medulla oblongata beneath level of foramen
magnum.
2- elongation of 4th ventricle.
3- associated with aqueduct stenosis.
4- associated with myelomeningocele.
5
ARACHNOID CYST :
ARACHNOID CYST :
-clear csf filled cyst.
- occur due to congenital splitting of the arachnoid membrane.
- they are intracranial but extracerebral.
-cam be seen in middle ,posterior cranial fossa , suprasellar region & behind the 3rd
ventricle.
- they can be large enough to produce mass effect or obstructive hydrocephalus.
- there may be Hypoplasia of underlying cerebral tissue such as the temporal pole.
6
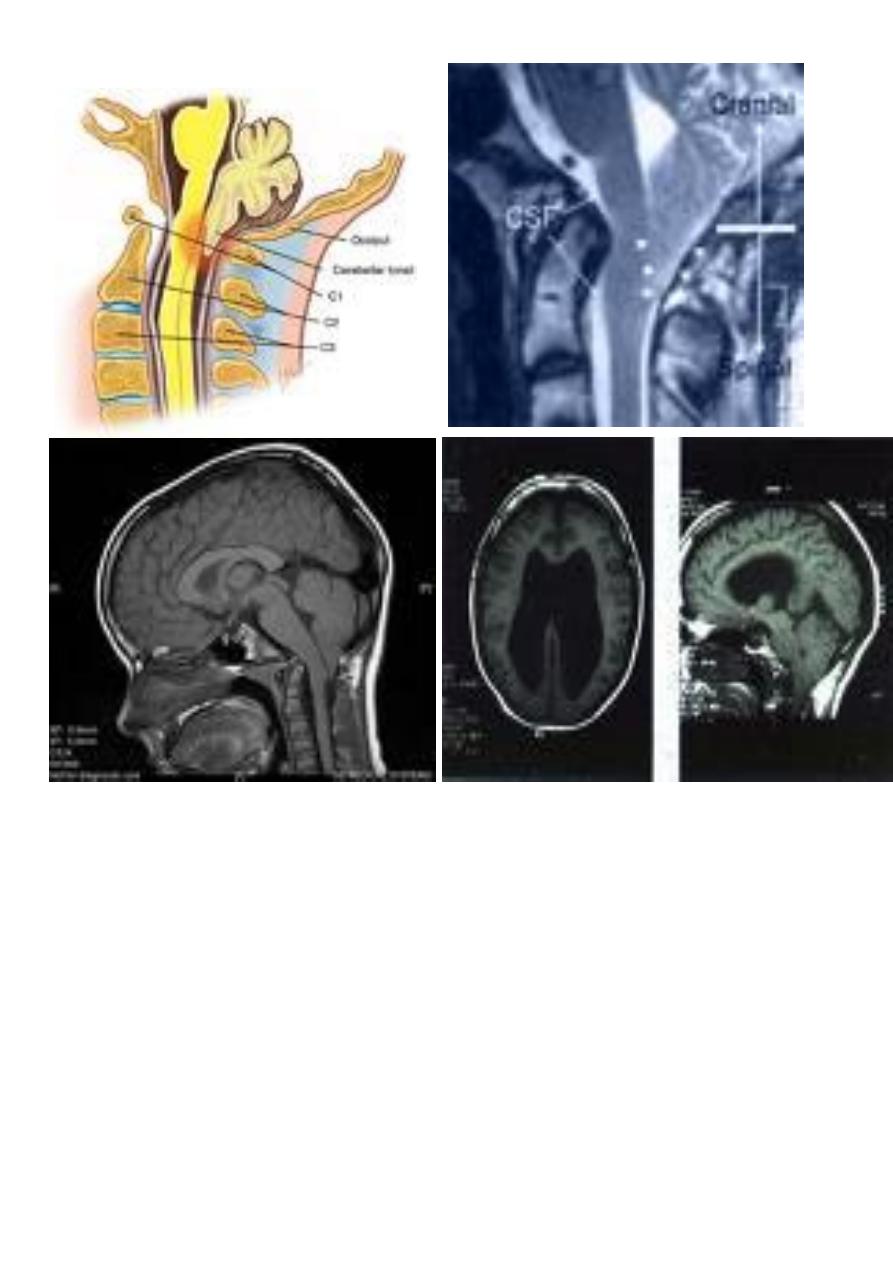
Coronal T1-weighted MRI image through a brain lesion
showing homogeneity of the lesion, lack of a perceptible
wall, lack of internal complexity, and CSF signal intensity.
There is associated remodeling of the adjacent calvarium
and brain displacement. These imaging features are typical
of an arachnoid cyst .
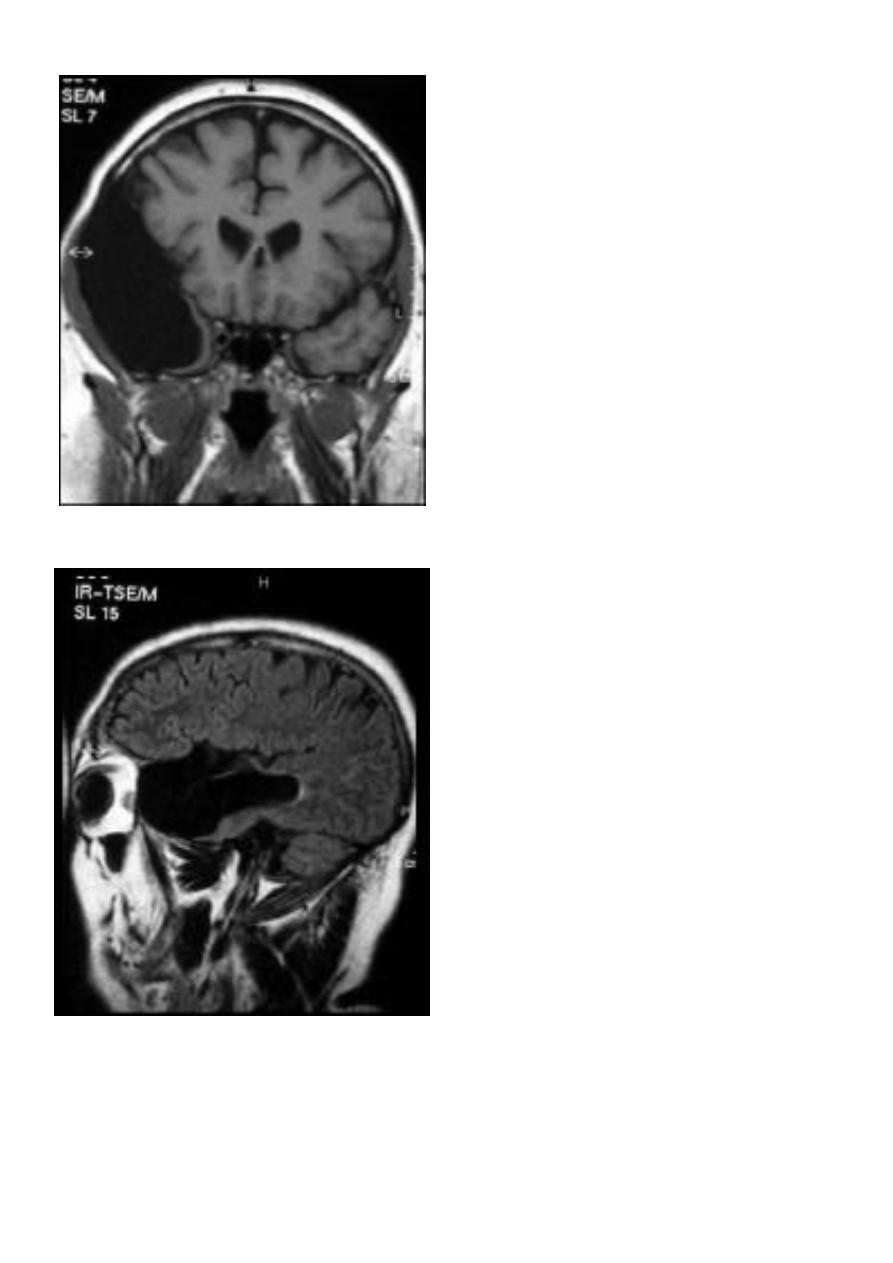
Sagittal fluid-attenuated inversion recovery
(FLAIR) weighted image through a brain lesion), showing
homogeneity of the lesion, lack of a perceptible wall, lack
of internal complexity, and CSF signal intensity. There is
associated brain displacement. These imaging features are
typical of an arachnoid cyst.
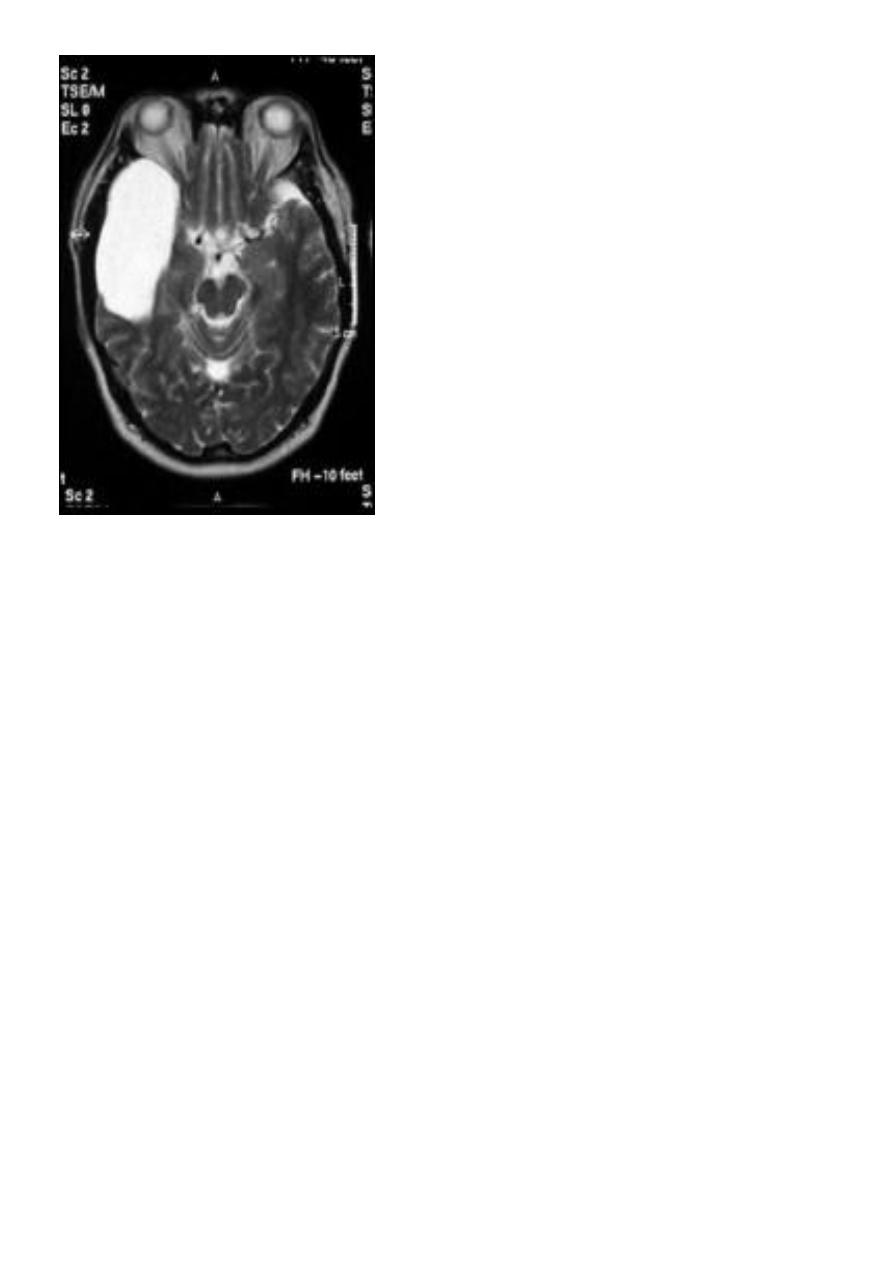
7
Axial T2-weighted MRI image through the midbrain,
showing a right middle cranial fossa homogeneous lesion) with CSF
signal intensity and no perceptible wall or internal complexity.
There is associated remodeling of the adjacent sphenoid bone and
brain displacement. .
WHITE MATTER DISORDER:
White matter disease have been classified as:
1-dysmyelinating: there is abnormal formation of myelin e.g. leukodystrophies , metabolic
disorders.
2-demylinating: there is destruction of normally formed myelin e.g. multiple sclerosis.
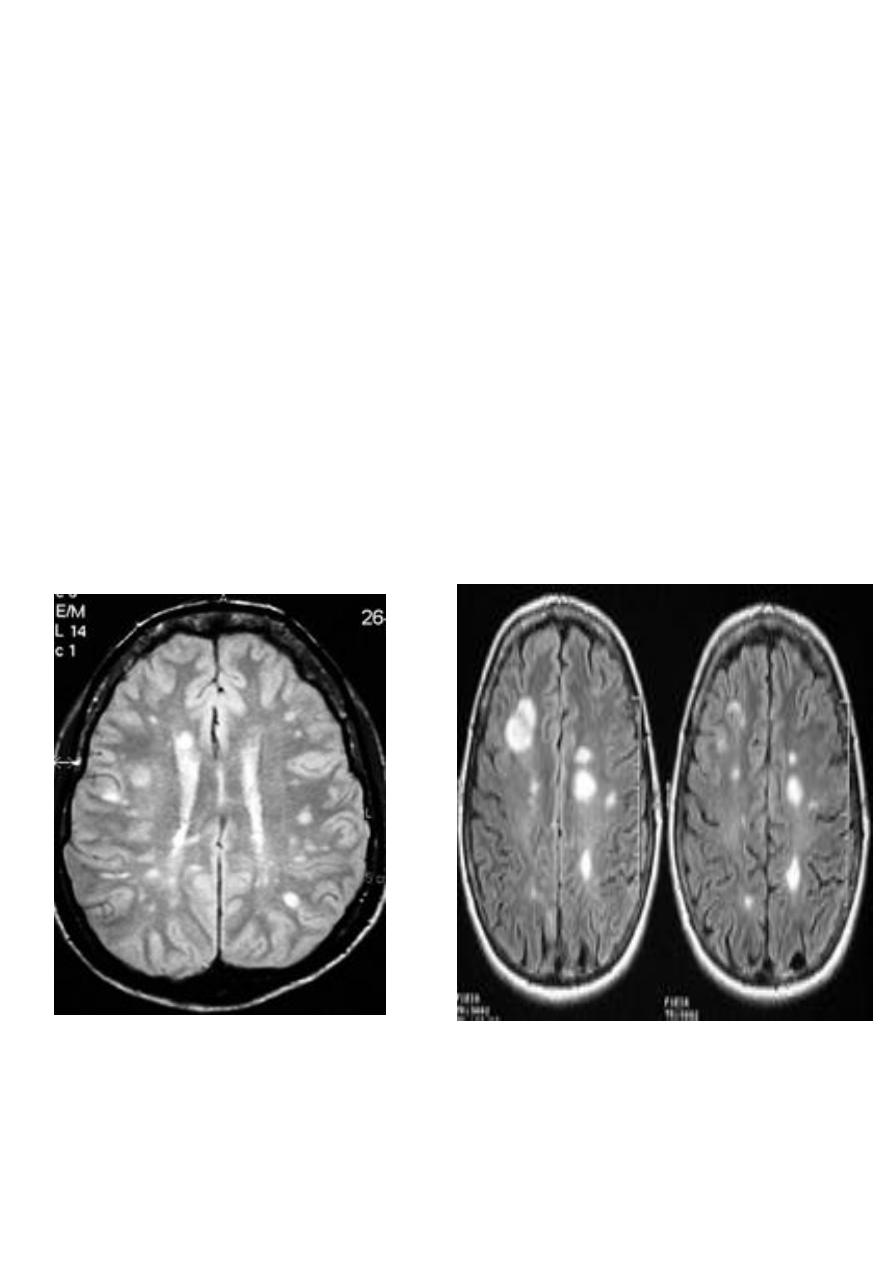
MULTIPLE SCLEROSIS:
-common neurological disorder.
-characterized by disseminated plaques of demyelination & gliosis throughout the neuraxis.
-the sites of election are:
1.periventricular.
2.optic pathways.
3.brainstem.
4.cerebellar white matter & peduncles.
5.spinal cord.
8
-young adults are primarily affected.
-MRI is more sensitive than CT in the demonstration of MS plaques.
- the most characteristic appearance is that of peri ventricular nodular Hyper intense
lesions on T2 weighted images.
-the plaques are also well seen at the gray- white matter interfaces.
-MRI can even image lesions in the spinal cord , brainstem & cerebellum.
-multiple cerebral lesions are seen in over half the patient presenting with a single episode
of optic neuritis.
-some lesion may show a central area of greater signal intensity , resembling a target.
-contrast enhancement after giving gadolinium occurs in the acute phase indicating activity
& in the chronic phase doesn't enhance.
-differential diagnosis :1-ischaemic lesions ,2-following radiotherapy , 3-
in encephalomyelitis.
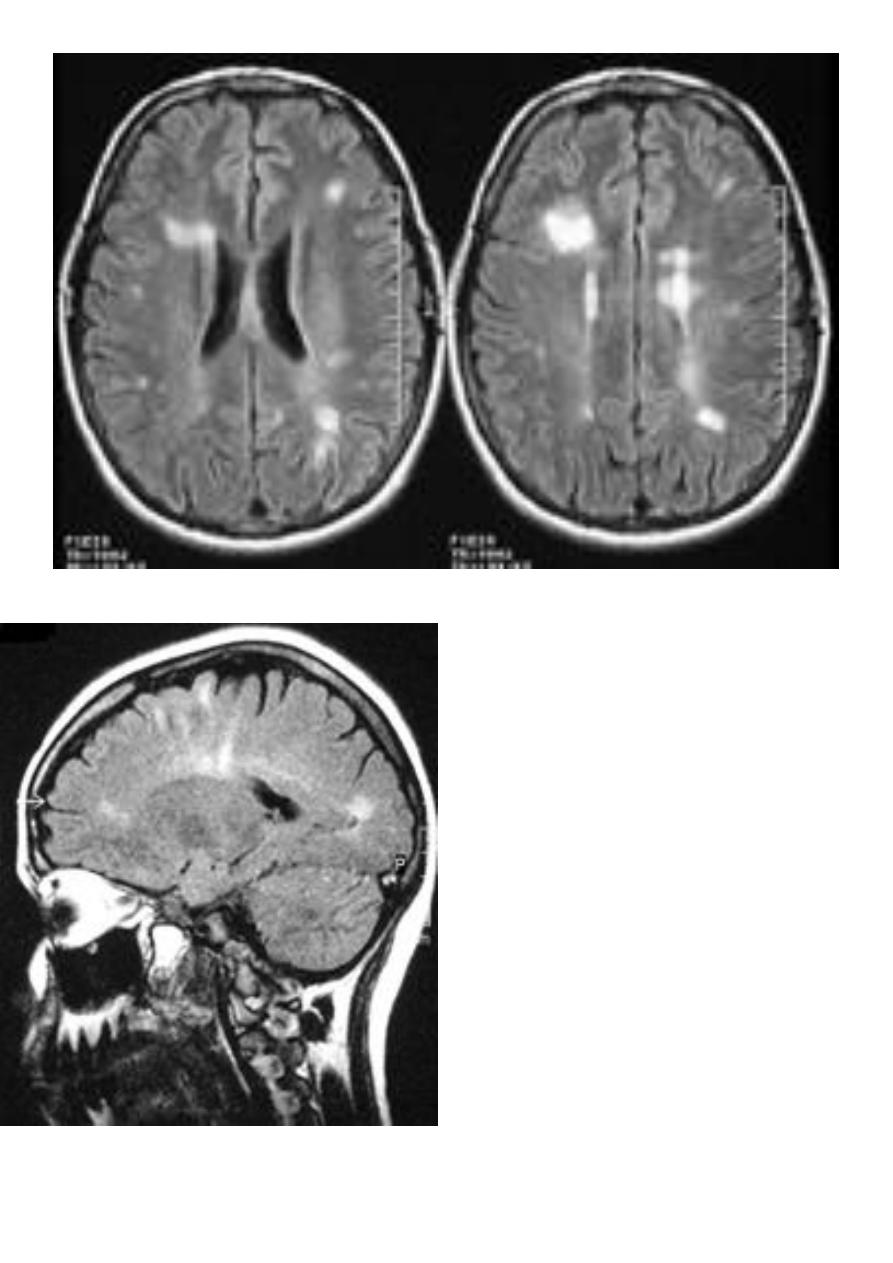
9
SAGITAL FLUID ATTENUATION INVERSION RECOVERY
SEQUENCE: OVOID PLAQUES ( HIGH SIGNAL INTENSITY) ,
WHICH ARE PERPENDICULAR TO LATERAL VENTRICLE.