1
Fifth stage
ENT
Lec-18
د.سعد
4/4/2016
Chronic Suppurative Otitis Media (CSOM)
CSOM is a long-standing infection of a part or whole of the middle ear cleft characterized by painless
ear discharge and a permanent perforation with hearing loss. A perforation becomes permanent
when its edges are covered by squamous epithelium and it does not heal spontaneously.
Classification of chronic suppurative otitis media
1.
Classification based on
anatomical
considerations
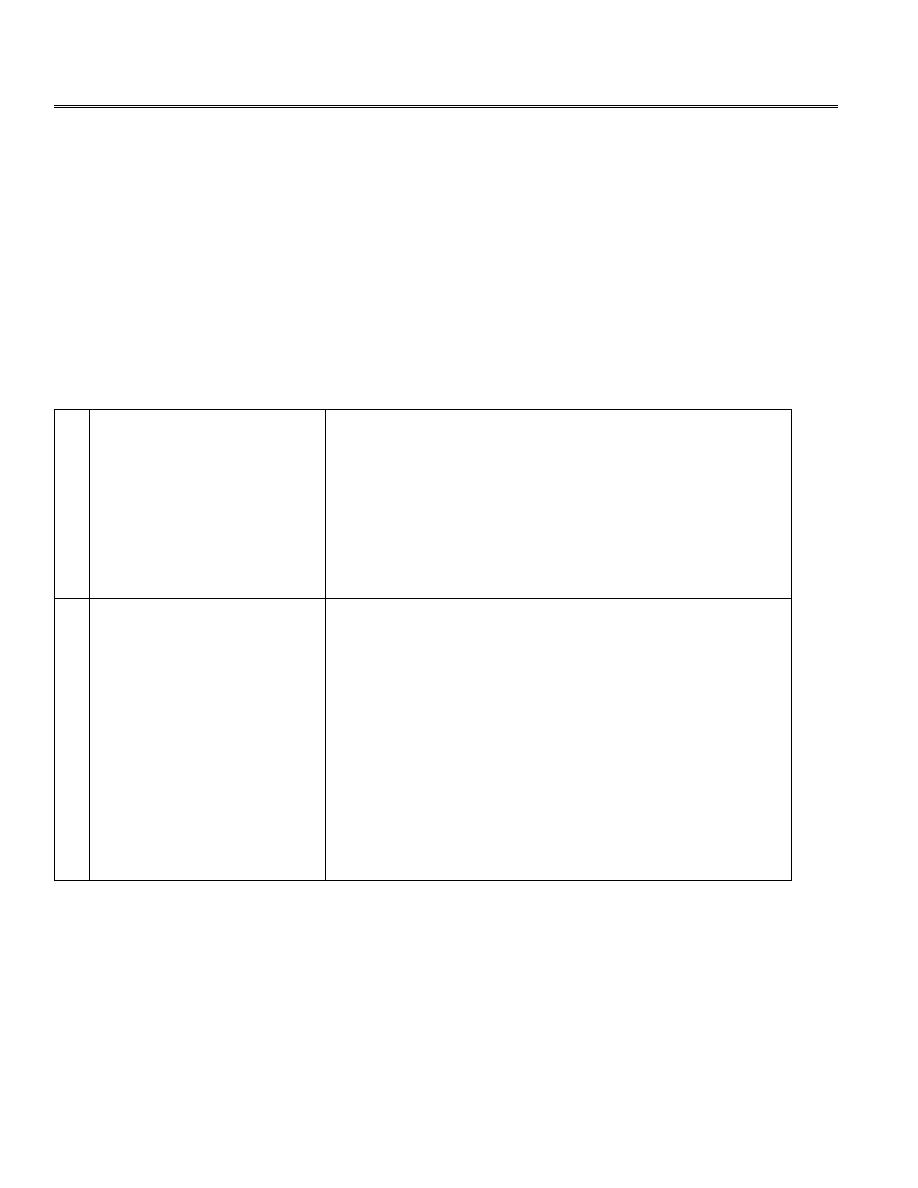
a. Tubotympanic disease =’ safe’ disease;
perforation is central and
non-marginal.
b.Atticoantral disease=’unsafe’ disease: perforation
is marginal or in attic: cholesteatoma.
2.
Classification based on
pathological
consideration
A. Healed otitis media: adhesive otitis media,
tympanosclerosis.
B. Inactive mucosal chronic otitis media:
permanent perforation.
C. Active mucosal chronic otitis media: chronic
suppurative otitis media, aural polyp.
D. Active squamous epithelial chronic otitis
media: cholesteatoma with discharge.
E. Inactive squamous epithelial chronic otitis
media: retraction pocket.
2
Tubotympanic Disease
Also called the safe or benign type; it involves the anteroinferior part of the middle ear cleft, i.e.
Eustachian tube and mesotympanum and is associated with central perforation. There is no risk of
serious complication.
Aetiology
It is virtually always a complication of AOM where there is persisting perforation of the TM. It
therefore usually starts in infancy and early childhood. Reinfection either through the nasopharynx
(tonsillitis, adenoid hypertrophy and sinusitis) or through the perforation allows active infection to
persist or to recur.

3
Bacteriology
There is high incidence of gram negative infection like proteus and pseudomonas aeroginosa.
Anaerobic infection can be found as well.
Pathology
The main pathological condition is a central perforation of the TM resulting from AOM. Repeated
infection may cause polyp formation which consists of oedematous middle ear mucosa prolapsing
through the perforation.
Clinical picture
1.
Mucoid or mucopurulent discharge which may be intermittent or persistent.
2.
CHL Its degree varies with the size and position of the perforation.
Examination
1.
Otoscopy:
a. Central TM perforation in the pars tensa.
b. Middle ear mucosa It is seen when the perforation is large. Normally, it is pale pink and moist;
when inflamed it looks red, oedematus and swollen. Occasionally, a polyp may be seen.
2.
Tuning fork tests: CHL.
Investigations
1.
PTA: CHL.
2.
X-ray and CT scan shows sclerosis with clouding of the mastoid air cells.
3.
Swab of the aural discharge for c/s.
Treatment
1.
Elimination of URTI: Treatment of sinusitis, adenoidectomy and tonsillectomy.
2.
Medical Treatment
a)
Aural toilet: suction clearance and mopping with cotton-wool wicks at home. The patient
should be warned not to get water into the ear when washing or swimming.
b)
Local antibiotic /steroid drops e.g. Ciprofloxacin, Neomycin or Gentamycin. These drops
are instilled after mopping the ear and the head should be on the side so that the affected
ear is upper most. After that the tragus is pressed inwards to assist the drops to pass into
the middle ear.
c)
Systemic antibiotics has little role in treatment.
4
3.
Surgical treatment
a)
Removal of polyps and granulation tissue.
b)
Myringoplasty: repair of TM perforation by temporalis fascia is indicated when there is
recurring discharge or there is disabling deafness.
Atticoantral Disease
In this type of infection the bone of the attic, mastoid antrum and air cells are involved as well as
the mucosa of the middle ear cleft. It is therefore referred to as atticoantral disease. As erosion of
bone may extend to adjacent vital structures there is always a danger of serious complications; both
intra- and extracranial. This type of infection is usually associated with cholesteatoma.
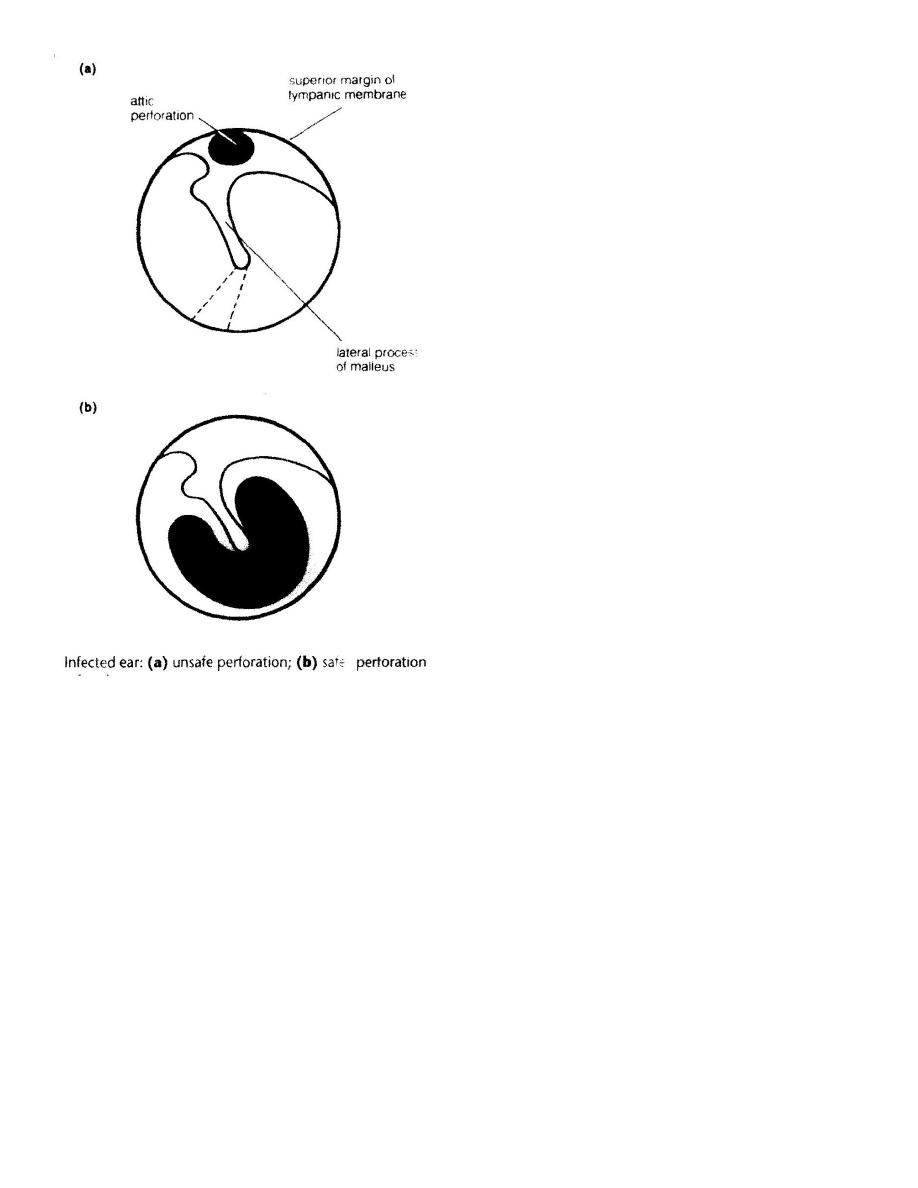
Cholesteatoma
Definition: Cholesteatoma is a sac of keratinizing squamous epithelium containing keratinous debris
and surrounded by granulation tissue (i.e. it is a skin in a wrong place). The surface layers of epithelium
keep producing keratin and this result in the appearance of a thin-walled sac containing cheesy
material. The granulation tissue on the outside of the sac produces lysozymes and this gradually
erodes the ossicles, ear drum and mastoid bone.
The suffix “oma” may suggest that it is a tumour, this is not the case, though if untreated it will
continue to expand and destroy surrounding structure.
Theories of origin of cholesteatoma
I Congenial: This is unrelated to CSOM as it arises from embryonic epithelial tissue and occurs in
the temporal bone and in the middle ear.
II Acquired

5
1.
Invagination theory: Cholesteatoma starts
as a retraction pocket of the TM due to ET
obstruction. The TM tends to be retracted
in attic region where the pars flaccida is
thin. If the retraction pocket is more
marked, a cholesteatoma sac may be
formed inside the middle ear.
2.
Emigration theory: cholesteatoma arise from extension of squamous epithelium into the middle ear
through a marginal TM peroration.
3.
Metaplasia theory: Squamous metaplasia of the middle ear mucosa in response to chronic
infection.
Clinical picture
The onset of symptom is insidious so that the patient may be unaware of the starting point.
1. Persistent or recurrent purulent aural discharge. The discharge however, is purulent rather than
mucopurulent and is frequently scanty and foul smelling.
2. CHL: Usually marked hearing loss because of involvement of the ossicular chain.
3. Bleeding from the ear if granulation tissue is present.
4. Headache, vertigo and facial paralysis all indicate complications.
Examination
1. Otoscopy: Attic (unsafe perforation) situated in the pars flaccida. Cholesteatoma may be seen a
grayish substance projecting from an attic perforations. Granulation tissue may be seen as well
occupying such perforation.
2. Tuning fork test: CHL.
3.
Fistula sign: cholesteatoma can cause erosion of the lateral semicircular canal leading to fistula. If
such fistula is present, any change in pressure in the middle ear e.g. by
Siegle`s pneumatic speculum
will probably produce vertigo and nystagmus. If the test is positive, it is an indication of urgent
surgery because of the risk of labyrinthitis.
Investigations
1. PTA: CHL.
2. X-ray and CT scan of mastoid; Cholesteatoma appear as an area of translucency with a clearly out
lined bony margin.
3. Swab of the aural discharge for c/s.
6
Treatment
1. Conservative: it’s used when no complications are suspected and if the cholesteatoma is small and
accessible. It includes removal of cholesteatoma and granulation tissue by fine crocodile forceps
and suction clearance under magnification. Other measures like ear drops and dry ear precaution
are also recommended.
2. Surgical: In most cholesteatoma surgical treatment is required.
Complications of Otitis Media
Occurs when the infective process spreads beyond the confines of the middle ear.
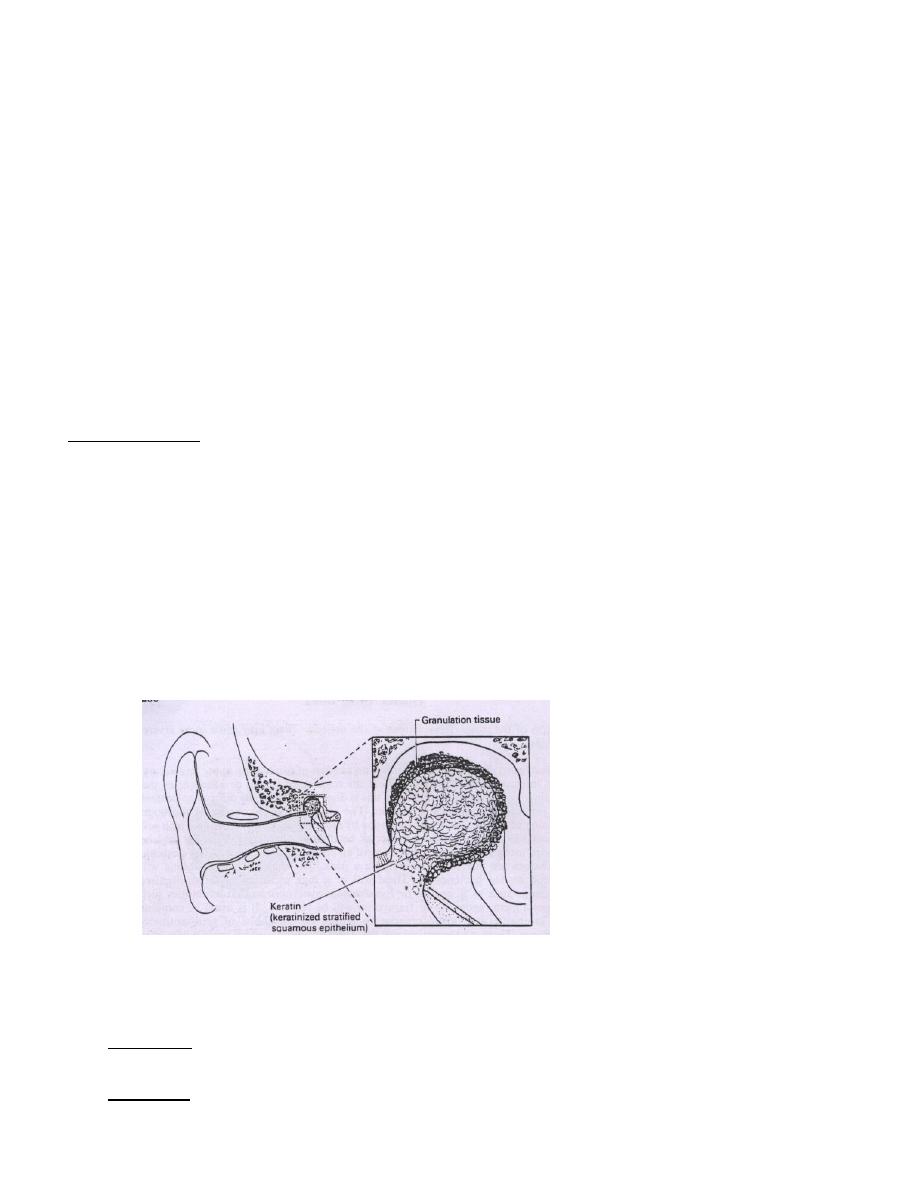
Routes of infection
a) Medially to the labyrinth, through the oval
window, round window, or by erosion of
the LCC.
b) Superiorly to the middle cranial fossa
through the tegmen tympani.
c) Posteriorly to the posterior cranial fossa.
d) Inferiorly through the floor of the
tympanum producing a septic thrombosis
the bulb of the internal jugular vein.
Extracranial complications of otitis media
1. Mastoiditis.
2. Labyrinthitis.
3. Petrositis.
4. Facial nerve paralysis.
Intracranial complications of otitis media
1. Extradural abscess.
2. Subdural abscess.
3. Lateral (sigmoid) sinus thrombosis.
4. Meningitis.
Primarily the objective of surgical treatment is
Eradication of potentially dangerous disease by
mastoidectomy.
Reconstruction of hearing mechanism ( tympanoplasty): i.e.
Reconstruction of TM (Myringoplasty) + Reconstruction of the sound
conducting ossicular chain (Ossiculoplasty).
7
5. Brain abscess.
6. Otitic hydrocephalus.
Features indicating complication in COSM
1. Pain (Extradural or brain abscess and OE )
2. Vertigo ( erosion of lateral semicircular canal and labyrinthitis)
3. Persistent headache ( Intracranial complication)
4. Facial weakness ( erosion of facial canal )
5. A listless child refusing to take feeds and easily going to sleep ( extradural abscess)
6. Fever, nausea and vomiting ( Intracranial infection)
7. Irritability and neck rigidity ( Meningitis)
8. Diplopia ( petrositis with involvement of CN VI )
9. Ataxia ( Labyrithitis and cerebellar abscess)
10. Abscess round the ear ( Mastoiditis)
8
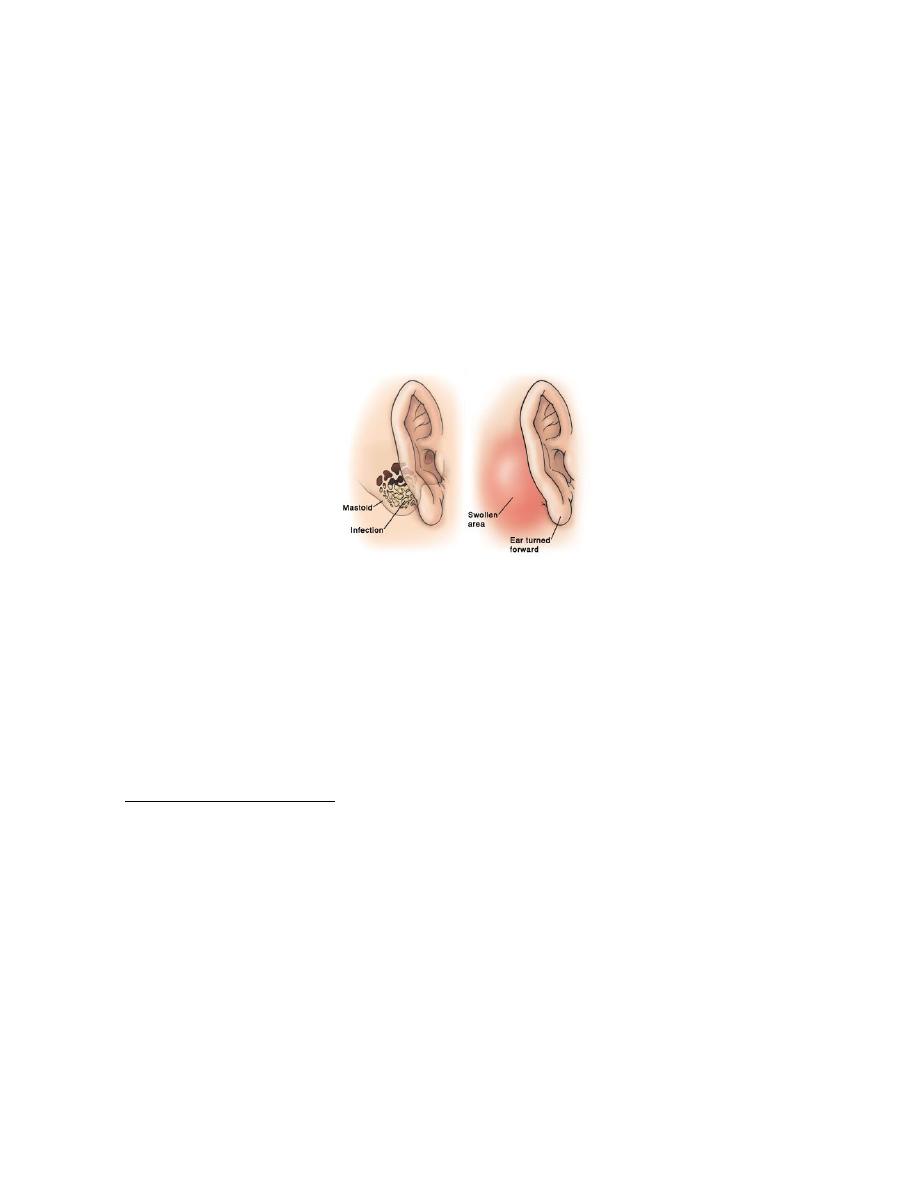
Acute Mastoiditis
Inflammation of mucosal lining of antrum and mastoid air cell system is an invariable accompaniment
of acute otitis media and forms part of it. The term "mastoiditis" is used when infection spreads from
the mucosa, lining the mastoid air cells, to involve bony walls of the mastoid air cell system. The
production of pus under tension and with the hyperaemic decalcification and osteoclastic resorption of
bone will cause destruction and coalescence of mastoid air cells, converting them into a single irregular
cavity filled with pus (Empyema of mastoid). Pus may break through the mastoid cortex leading to
subperiosteal abscess which may even burst on the surface leading to a discharging fistula.
Aetiology
1. It can complicate AOM if it has been either untreated or given incorrect or inadequate antibiotic
therapy.
2. Acute mastoiditis can be superimposed on a chronic atticoantral disease in which the cholesteatoma
has invaded the mastoid bone.
Clinical picture
It is more common in children than adults and is often seen in mastoid with well developed air
system.
1. The patient generally looks ill with fever and tachycardia.
2. Earache followed by aural discharge with relief of pain. This is followed by cessation of discharge
and recurrence of pain with pyrexia.
3. If the disease continues uncontrolled the pus may break through the superficial cortex and forms
postauricular abscess.
Examination
1. Retroauricular swelling and tenderness over the mastoid area with fluctuation if postauricular
abscess forms.
9
2. Soft tissue oedema with displacement of the auricle downwards and outwards. The postauricular
sulcus tends to be retained.
3. Narrowing of the EAM due to sagging of the posterosuperior meatal wall.
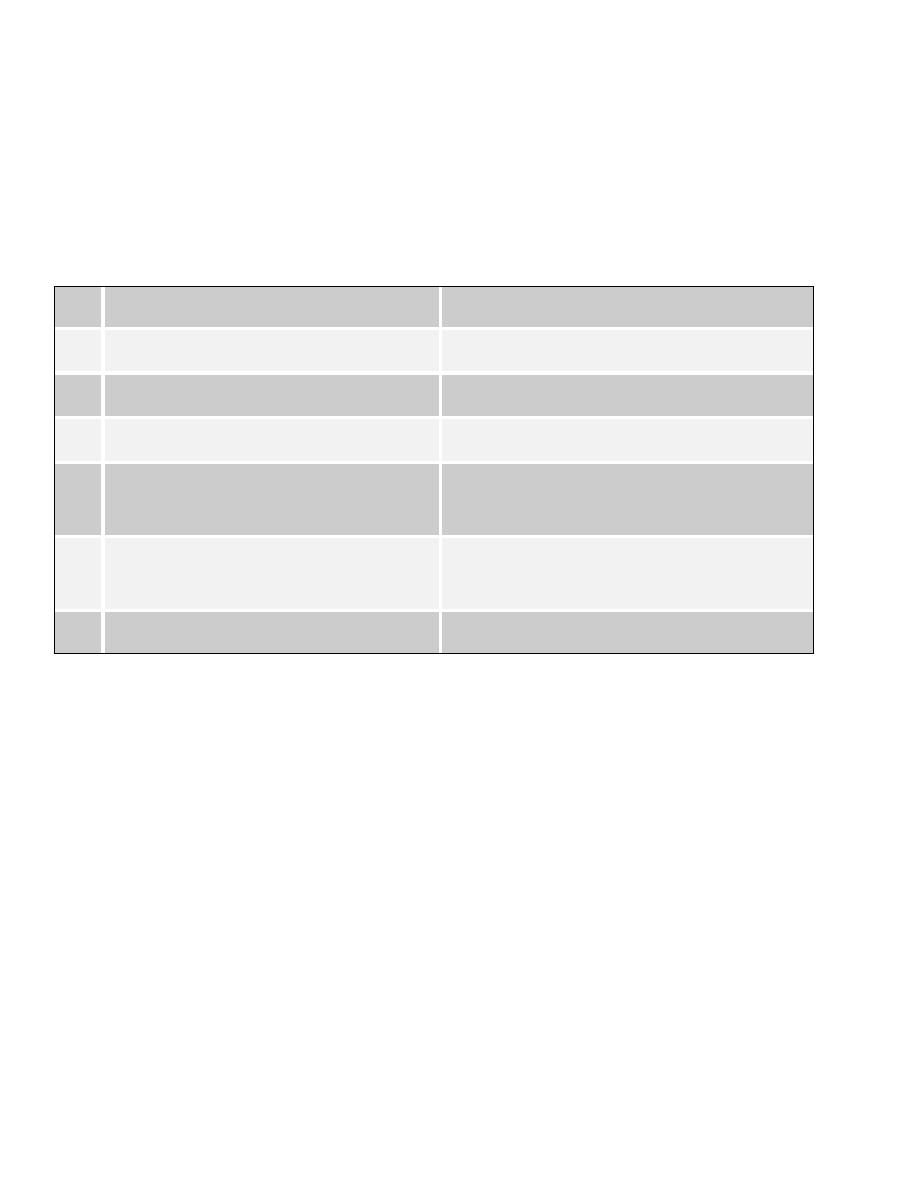
Differential diagnosis
Frunculosis.
Infected sebaceous cyst.
Mastoiditis
Furuncle
1.
Preceding history of OM
No such history
2. Deafness is present
No deafness until the canal is occluded
3. TM shows signs of OM
TM is normal
4. Tenderness on pressure over the
mastoid
Tenderness on moving the auricle
5. Postauricular sulcus tends to
remain
Postauricular sulcus tends to be
obliterated with forward displacement.
6. Radiographic changes in mastoid
No radiographic changes in mastoid
Investigations
X-ray and CT scan shows opacity of the mastoid air cells.
Treatment
Medical
1. Admission to hospital
2. Antibiotic (in full dose): Intravenous antibiotic therapy according to c/s if there is discharge. If not
IV penicillin for 48 h whether there is an abscess or merely periosteal thickening, then followed by
oral antibiotic for a week.
Surgical
Indications:
1. The skin remains red over a fluctuant area.
2. Pyrexia and tenderness continue.
And this includes abscess drainage with or without cortical mastoidectomy with c/s of the aspirate
followed by a course of appropriate antibiotic for a week.