4th stage
SurgeryLec-4
Dr.Ahmed
3/4/2016
TongueAnomalies of the tongue :
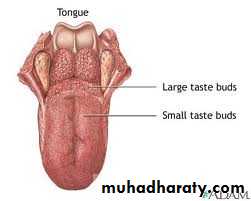
Aglossia
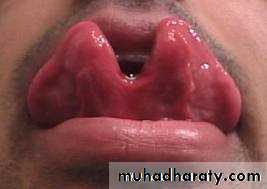
Tongue tie.Bifid
Lingual thyroid
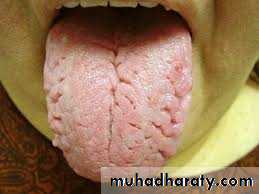
Congenical fissured tongue
Geographic tongue
Macroglossia




Congenital causes of macroglossia :
Cavernous haemangioma
A-V fistulaeLymphangioma
Neurofibromatosis
Aquired causes:
Muscular hypertrophy
Amyloidosis
Acromegaly
Diffuse carcinoma ,sarcoma

TONGUE INJURIES :
Mechanism of injury :Tongue biting (epileptic fit )
Fracture jaw
C/F: bleeding ,if unconscious may be sever
Rx : arrest bleeding (pressure )
Suturing UGA
Haematoma may need tracheostomy

Inflammation of tongue :
Acute : superficial (red, painful) or deep due to streptococcal infection or angioneurotic edema may need tracheostomy
Chronic : Due to irritation by smoking, denture ,sharp tooth.(erythroplakia then leukoplakia)

Treatment :
Stop irritationWash with antiseptic
Excisional biopsy
Diathermy coagulation
Tuberculer glossitis
Syphilitic glossitis at any stage of the disease 1ry ,2ry and 3ry.
Candida glossitis (oral thrush)
Apthus ulcer
Tongue ulcer :
Traumatic e.g. dentureInflammatory :
Acute : apthus painful 2 weeks spontaneous healing,lichin planus ,herpetic.
Chronic : tubercular ulcer (undermined edge +submandibular L.N )
Treatment: anti TB +antiseptic wash +anesthetic jelly.
Syphilitic ulcer.
Chronic superficial glossitis.
Neoplastic :Scc (commonest),lymphoma.

The lip
Common lesions :Herpis simplex infection :
- Fever
- Trauma
Malignant :carcinoma
Carcinoma of the lip :
Commonly in the lower lip away from the contact with the upper lip.Only 5%in the upper lip .
Spread :
Laterally rather than deeply.If uncontrolled it can spread to ant. Triangle of neck and invade the mandible.
L .n. metastasis late.
Treatment :
Both surgery and radiotherapy are highly effective with cure rate 90%
Up to one third of the lip can be removed with primary suture
Larger tumor needs facial flap.