IsosporabelliIsospora belli is an intestinal protozoan that causes Isosporiasis ( is a human intestinal disease caused by this parasite. Isospora belli cause diarrhea,especiallyin innunocomprpmised patients,eg, those with AIDS
It is world wide, especially in tropical and
subtropical area. Its life cycle parallels that of other members of the coccidia. The organism is acquired by fecal – oral transmission of oocysts from either human or animal sources.CausalAgentThe coccidian parasite Isospora belli infects the epithelial cells of the small intestine, and is the least common of the three intestinal coccidia that infect humans (Toxoplasma, Cryptosporidium, and Isospora
LifecycleAt time of excretion, the immature oocyst contains usually one sporoblast (more rarely two). In further maturation after excretion, the sporoblast divides in two, so the oocyst now contains two sporoblasts. The sporoblasts secrete a cyst wall, thus becoming sporocysts
and the sporocysts divide twice to produce four sporozoites each. Infection occurs by ingestion of sporocyst-containing oocysts: the sporocysts excyst in the small intestine and release their sporozoites, which invade the epithelial cells and initiate schizogony.
Upon rupture of the schizonts, the merozoites are released, invade new epithelial cells, and continue the cycle of asexual multiplication. Trophozoites develop into schizonts which contain multiple merozoites.
After a minimum of one week, the sexual stage begins with the development of male and female gametocytes. Fertilization results in the development of oocysts that are excreted in the stool. Isospora belli infects both humans and animals
Unsporulated oocysts of Isospora belli (human feces; acid fast stain)

Isospora belli. Wet mount preparation. When passed in feces

ClinicalFeaturesInfection causes acute, non-bloody diarrhea with crampy abdominal pain, which can last for weeks and result in malabsorption and weight loss.
In immunodepressed patients, and in infants and children, the diarrhea can be severe. Eosinophilia may be present (differently from other protozoan infections).
LaboratoryDiagnosisMicroscopic demonstration of the large typically shaped oocysts is the basis for diagnosis.
Because the oocysts may be passed in small amounts and intermittently, repeated stool examinations and concentration procedures are recommended.
If stool examinations are negative, examination of duodenal specimens by biopsy or string test (Enterotest) may be needed. The oocysts can be visualized on wet mounts by microscopy with bright-field, differential interference contrast (DIC), and epifluorescence. They can also be stained by modified acid-fast stain
Typicallaboratoryanalyses include:MicroscopyMorphologic comparison with otherintestinalparasitesBench aids for Isospora
TreatmentTrimethoprim-sulfamethoxazole is the usual treatment choice. See recommendations in The Medical Letter (Drugs for Parasitic Infections) for complete information.
Sarcocystis:(Sarcocysts were first isolated by the Swiss scientist Friedrich Miescher in 1843. When examining a house mouse, Miescher discovered white, “threadlike” structures (sarcocysts) in its muscle tissue.
These cysts came to be called “Miescher’s tubules” for many years after their discovery. Over the next few decades, similar cysts were found in other animals such as pigs, but it was not until 1889 when they were finally given a name – Sarcocystis miescheriana .
As much was still unknown about the organism, scientists were unsure whether to classify the species as protozoa or as fungi, since only the sarcocyst stage had been identified at that time. However, in 1967 through the use of electron microscopes,
bradyzoites (crescent-shaped structures found in several protozoa) were found in sarcocyst cultures, and the debate was resolved
Sarcocystis species are intracellular protozoan parasites with an intermediate-definitive host life cycle based on a prey-predator relationship.
Asexual stages develop in intermediate hosts after they ingest the oocyst stage from definitive-host feces and terminate with the formation of intramuscular cysts (sarcocysts).
Sarcocysts in meat eaten by a definitive host initiate sexual stages in the intestine that terminate in oocysts excreted in the feces. Most Sarcocystis species infect specific hosts or closely related host species.
For example, humans and some primates are definitive hosts for Sarcocystis hominis and S. suihominis after eating raw meat from cattle and pigs, respectively. The prevalence of intestinal sarcocystosis in humans is low and is only rarely associated with illness, except in volunteers who ingest large numbers of sarcocysts
We have 3 species that infect man:S hominis causes coccidiosis hominis.S suihominis causes coccidiosis suihominis.S lindemanni causes sarcocytosis
Specificity for Definitive Hosts Similar specificity relationships have been found for definitive hosts of some species. Dogs and coyotes serve as definitive hosts for S. cruzi, but humans and cats do not .
Humans, baboons, and rhesus monkeys can serve as definitive hosts for S. hominis, and humans, chimpanzees, and rhesus and cynomolgus monkeys can serve as definitive hosts for S. suihominis . No other definitive hosts have been identified for S. hominis or S. suihominis.
The infective stage of these parasites to man is:1-bradyzoites or cystizoites within cyst or true cyst ( sarcocyst), we have larger number of these bradyzoites which are fusiform, elongated& cylindrical with a cystic wall, either smooth or striated & divided into many compartments ( the infective stage reach the man by eating undercooked meats).
The infective stage of man is called mieschers tube which are elongated , fusiform or cylindrical bodies forming the encapsulated cystic intramascular of the protozoan Sarcocystis


(the white threadlike sarcocysts were once called Miescher's tubules)
B-mature oocyst: containing the sporocyst with 4 sporozoites.Sometimes upon rupture we may find feces with free sporocyst each containing 4 sporoziotes, these are found in stool of infected man ( as final host).TRANSMISSION FROM ANIMALS TO HUMANSEating raw or undercooked beef and pork containing mature oocysts of S. hominis and S. suihominis. respectively, has resulted in humans acquiring intestinal sarcocystosis
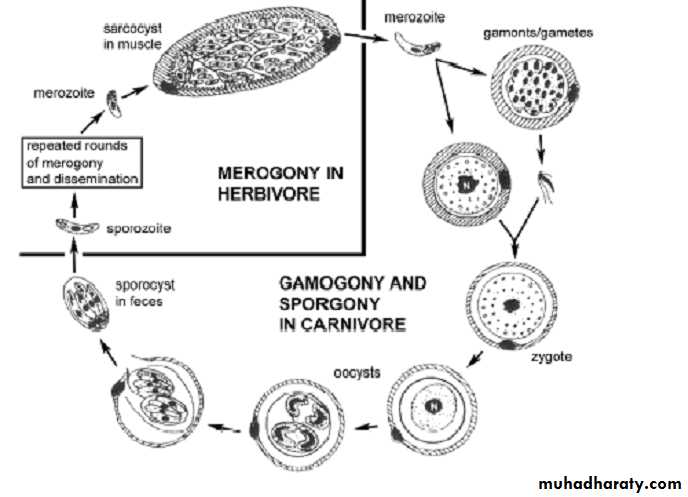
LIFECYCLESSarcocystis species are intracellular protozoan parasites with a requisite two-host life cycle based on a prey-predator (intermediate-definitive) host relationship.The life cycle involve 2 obligatory hosts, bearing the sexual & asexual cycles is completed in man or predator ( carnivorous) while the asexual stage take place in prey ( herbivorous
or intermediate host In the small intestine of man ( final host) the bradyzoites are released & they migrate to sub – epithelial lining of small intestine & develop to male & female gametocytes.
One male gametocytes fertilize the female gametocyte (ovum) to form immature oocyst. But this maturation occurs within the tissue of intestine & pass with feces & some of them are ruptured, so we may see within the stool free sporocyst or mature oocyst.
When intermediate host get these sporocyst it infect endothelial cells of blood vessels and schizogony ( asexual reproduction by multiple fission, found in some protozoa especially parasitic sporozoan),
these schizonts rupture releases merozoites infect blood vessels & go to striated muscle & develop into tissue cyst ( sarcocyst). But in case of Sarcocystis lindmani is similar to this life cycle but differ in that asexual cycle in the muscle of man while the sexual cycle is the unknown final host, so the sexual cycle is a blind end.
Characteristic
Muscular infectionIntestinal infection
Source of infection
Water or food contaminated with feces from unknown carnivore or omnivore
Raw or undercooked meat
Infective stage
Oocyst or free sporocysts
Sarcocyst containing bradyzoites
Developmental stages
Intravascular schizonts (not seen); intramuscular sarcocysts
Sexual stages in lamina propria; oocysts excreted in feces
Time from ingestion of infective stage to symptoms
Weeks to months, lasting months to years
3-6 h, lasting 36 h
• TABLE 1. Symptoms of sarcocystosis are summarized in Table 1.
Characteristic
Muscular infection
Intestinal infection
Source of infection
Water or food contaminated with feces from unknown carnivore or omnivore
Raw or undercooked meat
Infective stage
Oocyst or free sporocysts
Sarcocyst containing bradyzoites
Developmental stages
Intravascular schizonts (not seen); intramuscular sarcocysts
Sexual stages in lamina propria; oocysts excreted in feces
Time from ingestion of infective stage to symptoms
Weeks to months, lasting months to years
3-6 h, lasting 36 h
• TABLE 1. Symptoms of sarcocystosis are summarized in Table 1.
Time from ingestion of infective stage to symptoms
Weeks to months, lasting months to years
3-6 h, lasting 36 h
Symptoms
Musculoskeletal pain, fever, rash, cardiomyopathy, bronchospasm, subcutaneous swelling
Nausea, loss of appetite, vomiting, stomach ache, bloat, diarrhea, dyspnea, and tachycardia
Diagnosis
Biopsy specimen containing sarcocyst; antibodies to bradyzoites
Oocysts or sporocysts in feces, beginning 5-12 days after ingestion
Therapy (none approved)
Co-trimoxazole, furazolidone, albendazole, anticoccidials, pyrimethamine, anti-inflammatories
None
DIAGNOSISPresumptive diagnosis of human intestinal sarcocystosis is based on symptoms and a history of recently having eaten raw or undercooked meat. Definitive diagnosis, requiring identification of sporocysts in feces,
might require several stool examinations beginning several days after having eaten the meat. Sporocysts of S. hominis are first excreted 14 to 18 days after ingesting beef, and those of S. suihominis are excreted 11 to 13 days after ingesting pork
Sporocysts can be seen by bright-field microscopy in a fecal flotation wet mount just beneath the coverslip. Flotation based on high-density solutions incorporating sodium chloride, cesium chloride, zinc sulfate, sucrose, Percoll, Ficoll-Hypaque, and other such density gradient media is preferred to formalin-ethyl acetate and other sedimentation methods.
Because sporocysts of different species overlap in size and shape, species cannot be distinguished from one another solely by microscopy.
TreatmentThere is no known prophylaxis or therapeutic treatment for intestinal sarcocystosis. Infections are self-limiting, of short duration, and often asymptomatic.
The efficacy of co-trimoxazole or furazolidone remains to be demonstrated. For six persons in Thailand with segmental necrotizing enteritis associated with sexual stages of Sarcocystis and gram-positive bacilli, surgical resection of the small intestine was followed by antibiotic treatment. This extremely aggressive course of treatment has not been applied in other cases.